Embed Size (px)
Citation preview
APPROACH TO CHRONIC
DIARRHOEADR.D.RASIKAPRIYA
1 st YEAR PEDIATRICS

OBJECTIVESINTRODUCTION DEFINITIONETIOLOGYPATHOPHYSIOLOGYRISK FACTORAPPROACH TO CHRONIC DIARRHOEA History Examination Red flags Investigation ManagementTAKE HOME MESSAGE

INTRODUCTION
• a stool output that exceeds 10 mL/kg/day is considered diarrhoea.
• Practical definition - diarrhoea is present when stools increase in frequency, fluidity (water content), or volume, in comparison with the previously established “normal” pattern.
• Major burden of childhood deaths globally, with an estimated 2.5 million deaths.

DEFINITION
• Defined as diarrhoea which exceeds 2 to 3 weeks.PERSISTENT DIARRHOEA CHRONIC DIARRHOEA• Diarrhoea that begins acutely
and last for 14 days or more• Usually infective in origin
• Usually non infective in origin.
WHY????
As per WHO in 201110% of total diarrhoea 35% of diarrheal deaths For every 100 children, 7 suffers PD in Malnutrition – 20% 60% < 6 months 90% < 1 year

ETIOLOGY <2YR >2YR
Infection
Bacterial- Enteroaggregative E.coli, Atypical E.coli, Shigella, Heat stable/labile enterotoxin producing E.coliViral- RotavirusParasites- Cryptosporidium, Giardia
Post infection Post enteritis diarrhoea syndrome
Abnormal digestive processes
Schwachman-Diamond syndrome, Primary bile acid malabsorption
Cystic fibrosis
Nutrient malabsorption
Congenital lactase deficiency, Glucose-galactose malabsorption.
Short bowel
Immune/Inflammatory
Immunodeficiencies, Food allergy-cow’s milk protein.
Celiac disease, IBD, Eosinophilic gastroenteritis.
Structural defects Microvillus inclusion disease, Tufting enteropathy
Rare
Defects in electrolyte and metabolism transport
Congenital chloride diarrhoea, Abetalipoprotinemia, Acrodermatitis enteropathica
Late onset chloride diarrhea.

ETILOGY < 2YRS >2YRS
Motility disorder Hirsch sprung disease, Intestinal pseudo obstruction
Thyrotoxicosis
Diarrhoea associated with exogenous substances
Excessive intake of carbohydrate, foods or drinks containing mannitol or sorbitol
SAME
Chronic nonspecific diarrhea Functional diarrhea IBS
Neoplastic diseases Neuroendocrine hormone secreting tumors.
SAME
CONTD….

COMMON CAUSES
INFANCY Post gastroenteritis malabsorption syndrome (persistent) Cows milk/soy protein intolerance Secondary disaccharidase deficiencies and Cystic fibrosisCHILDHOODChronic nonspecific diarrhoeaSecondary disaccharidase deficienciesGiardiasis and Post gastroenteritis malabsorption syndromeCeliac disease and Cystic fibrosis ADOLESCENCEIrritable bowel syndromeInflammatory bowel diseaseGiardiasisLactose intolerance

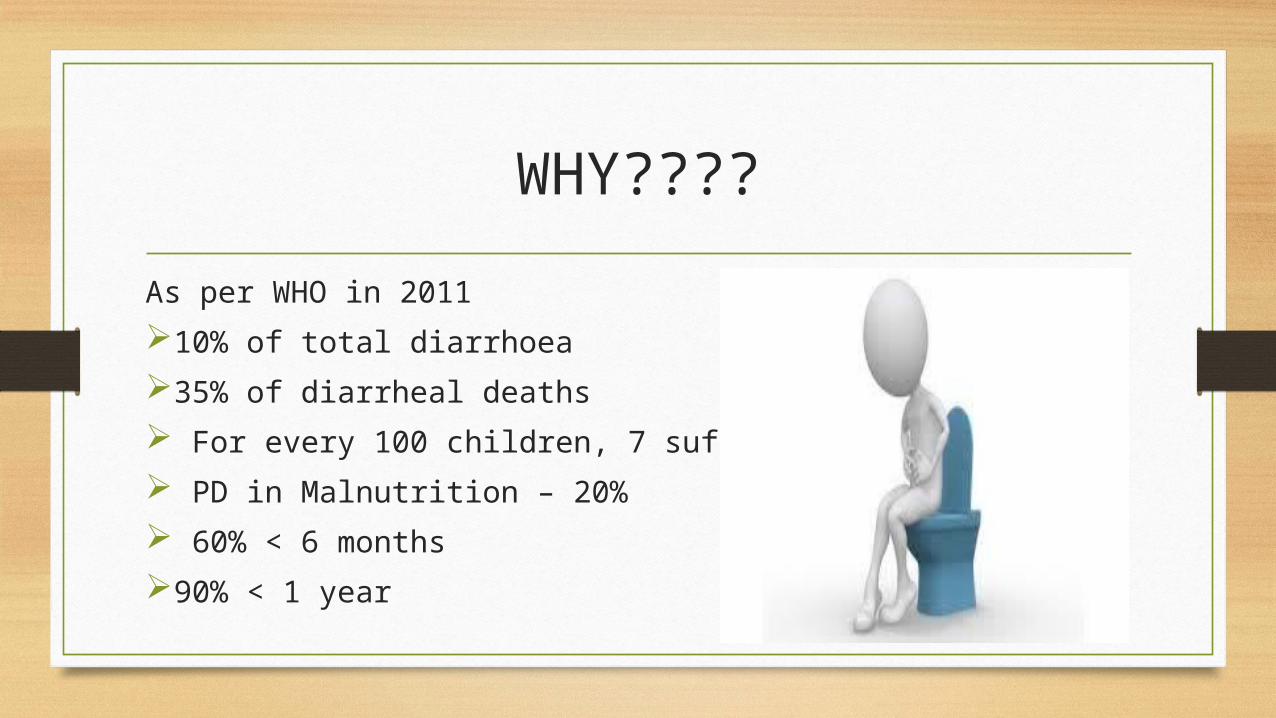
PATHOPHYSIOLOGY• Osmotic diarrhoea • Secretory diarrhoea,• Mutations in apical membrane transport proteins,• Reduction in anatomic surface area• Alteration in intestinal motility, • Inhibition of transport of electrolytes by inflammatory mediators

RISK FACTORS• Repeated enteric infections• Malabsorption of CHO & fats • Malnutrition • Very young age • Recent introduction of animal milk • Irrational usage of antibiotics • Lack of breast feeding/ bottle feeding • Improper therapy of ADD • Protein dietary intolerance

APPROACH TO A CHRONIC DIARRHOEA CHILD
HISTORY
• History is the most important step, it usually makes the DD narrow and gives clues to the cause of chronic diarrhoea.
• Personal history Age
• Sex :- IBD in paediatrics is common in MALE. • HISTORY OF THE PRESENT ILLNESS Onset:- just before 6m of age- coeliac disease. After 1 year- cow’s milk allergy. Preceded by gastroenteritis- post infectious diarrhoea. Course and duration is important. Most patients were completely free before this episode. Stool character is extremely important:- differentiate - secretory and osmotic diarrhoea.

STOOL HISTORY
Odourless blood tinged stools - shigellosis Frequent mucoid stools in a healthy child without blood -
IBS Nocturnal diarrhoea is usually associated with organic
disease rather than IBS. Infant having chronic diarrhoea, with a history of delayed
passage of meconium and if constipation preceded diarrhoea- Hirschsprung's disease

Associated symptoms• No symptoms, well child- toddlers diarrhoea.• Abdominal distension and weakness- Coeliac disease.• Severe abdominal pain, Bloody diarrhoea and oral ulcers - IBD.• Vomiting and rash- Eosinophilic enteritis. • Attacks of constipation - Hirsch sprung and IBS. • Infant with severe napkin dermatitis resistant to most treatment -
Acrodermatitis enteropathica.
NON GI SYMPTOMS• Recurrent respiratory tract infections- CF. • Weakness, fatigue and weight loss- IBD,
Addison and HIV. • Headache and mood changes - IBS. • Eczema- cow’s milk allergy and
Eosinophilic enteritis.• Generalized lymphadenopathy- HIV.• Recurrent fever and weight loss-TB.

Family and other history Same illness or respiratory problems- CF. IBD and IBS.
Dietetic history: Record a detailed history of feeding, prior to the onset of the disease and during the disease. Provide vital clues to the aetiology, e.g., cow's milk protein intolerance, lactose intolerance, gluten enteropathy. Soy protein intolerance, egg protein enteropathy. Overfeeding, concentrated formula feeds> osmotic diarrhoea.
Drug history: History of prolonged course of antibiotics- pseudomembranous colitis.

EXAMINATION• GENERAL EXAMINATION: Weight and height should be
measured and put on the appropriate charts.
• Weight loss is seen in many disorders like CF, Coeliac disease, IBD. weight and height are usually normal in toddlers diarrhoea.
• Pallor - CF, Coeliac disease.
• Fever- Infection, TB, CF and HIV.
• Clubbing- CF

• Hyperpigmentation- Addison’s disease, Coeliac disease
• Generalized lymphadenopathy- Lymphoma, HIV.
• Periorificial and acral vesicular and scaly lesions- Acrodermatitis enteropathica.
• Stomatitis and Perianal fistula- Crohn’s disease.
• Hepatomegaly -lymphomas, metastatic carcinoid, IBD and Whipple’s disease.
• Ascites - TB and lymphoma

• Poor weight gain or weight loss.• Continuous diarrhoea. • Night stools. • Acid stools- burning sensation with severe
inflammation and crying. • Blood and mucous in stool.• Failure to thrive.• Associated symptoms of systemic diseases like
fever, rash and arthritis.
DIAGNOSTIC WORK UPSTEP 1 Intestinal microbiology Stool- culture/parasite/electrolytes. Screening test for celiac disease( transglutaminase 2 autoantibodies) Non invasive test Intestinal function/inflammation Pancreatic function and sweat test Test for food allergy(prick/patch test)

STEP 2 INTESTINAL MORPHOLOGY•BIOPSY
STEP 3 SPECIAL INVESTIGATIONS• Intestinal immunohistochemistry • Anti-enterocyte antibodies • Serum chromogranin and catecholamine• Autoantibodies 75SeHCAT measurement• Brush border enzymatic activities • Motility and electrophysiological studies

DIAGNOSIS IN INDIATYPE TEST DIAGNOSIS in INDIAOsmotic vs Secretory Stool pH, Reducing
substances(Good)Stool electrolyteStool osmotic gapBreath hydrogen test
Based only on stool pH/reducing substance and response to keeping child nil orally.
Fatty diarrhoea Sudan stain(Good)Acid steatocrit72hr stool fat
Based on fat globules in normal microscopy and Sudan stain at some centers
Protein losing enteropathy Fecal Alpha 1 antitrypsin Based on clinical picture, low serum albumin and by exclusion
Pancreatic insufficiency Fecal elastase/chymotrypsinSecretin test
Based on ruling out other cause of fatty diarrhea.

SPECIFIC ETIOLOGY
• Cow’s milk protein allergy- colitis with blood and mucus in stools.
• Celia disease- Response to gluten free diet by 8-12 weeks. • Giardiasis/Amebiasis- stool microscopy• Immunodeficiency associated diarrhea• Cystic fibrosis- clinical picture and Sweat test• Intractable diarrhea of infancy-with/without villous atropy

PROBLEM AREAS IN MANAGEMENT
• Awareness – CMPA, Celiac disease and Immunodeficiency associated diarrhoea.
• Lack of availability of many specific diagnostic tests and cost in most part of country.

TREATMENT
• General supportive measures • Replacement of fluids & electrolytes • Nutritional rehabilitation • Elimination diet • Treat the cause

• CMPA- need extensively hydrolysed 100% bovine casein infant formula or Elemental amino acid formula
• Celiac disease- gluten free diet
• Lactose intolerance- Lactose free formula
• Intractable diarrhea of infancy- Elemental formula

PREVENTION
• Improvement in nutrition and hygiene status of infants and children.
• Cost effective intervention• Promotion of breast feeding, Promotion of safe drinking
water• Low osmolality ORS and Zinc supplementation• Avoid unnecessary antibiotics and continued feeding
during diarrhoea.