Embed Size (px)
DESCRIPTION
Dr Rachel Perrin's presentation at Meningitis Research Foundation's 2014 Meningitis Symposium http://www.meningitis.org/symposium2014
Citation preview

MRF’s healthcare and awareness initiative in Malawi
MRF Meningitis Symposium 11 June 2014

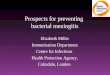
Barriers to recognition and treatment of meningitis at Primary Health Level
Primary health level
misdiagnoses
High numbers of patients
Erratic consultation systems
Unsystematic & informal triage
Desmond et al 2013 PLOSone
Desmond et al 2013 PLOSone
• Negative perceptions of health services
• Low level of awareness of meningitis
• Gender and age-based decision making in community
• Financial constraints
Barriers to seeking timely treatment for meningitis at community level
Desmond et al 2013 PLOSone
Action Meningitis
• Improved recognition of severe illness• Appropriate referral
Primary Health Level
Community Level
• Community recognition & awareness of meningitis and triage system
• Initiation of timely treatment
Triage system
Theatre
Radio

‘Health Talk’ Radio

Theatre for Development
• Partnering with local theatre group
• Establish a community-level intervention to encourage recognition and response to illness
Primary Health Clinics: Blantyre
Primary Health Level Triage system
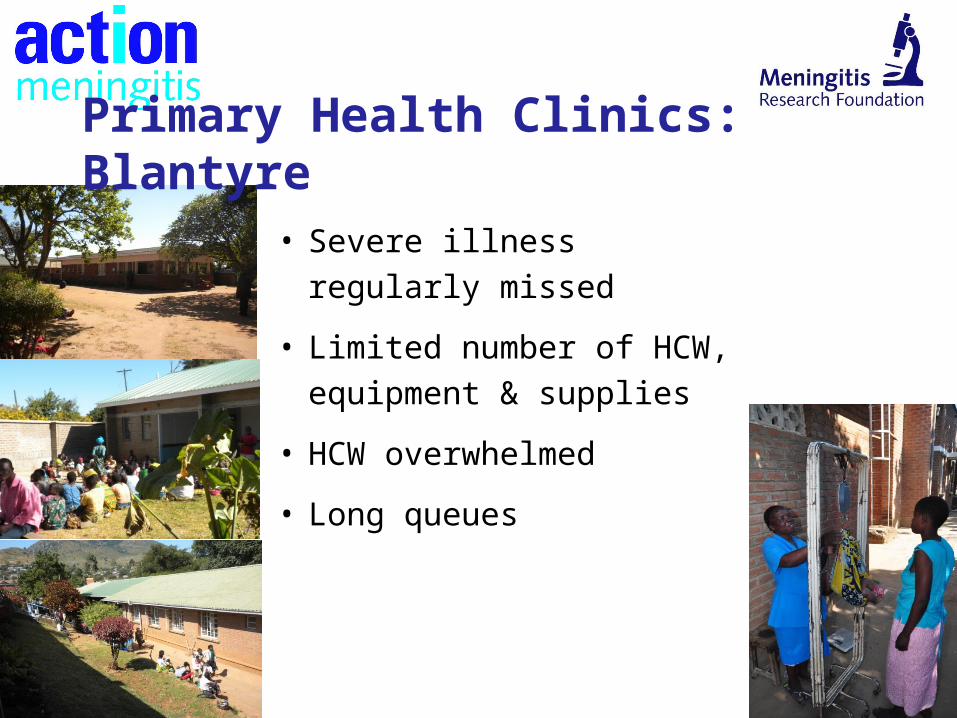
• Severe illness regularly
missed
• Limited number of HCW,
equipment & supplies
• HCW overwhelmed
• Long queues
Primary Health Clinics: Blantyre
Aims:
1. To develop a triage system, tailored for PHCs
2. To implement this system within 5 PHCs in Blantyre
3. To encourage appropriate referral decisions to
hospital & track referrals
4. To monitor, evaluate and refine this system
Implementation of Triage System
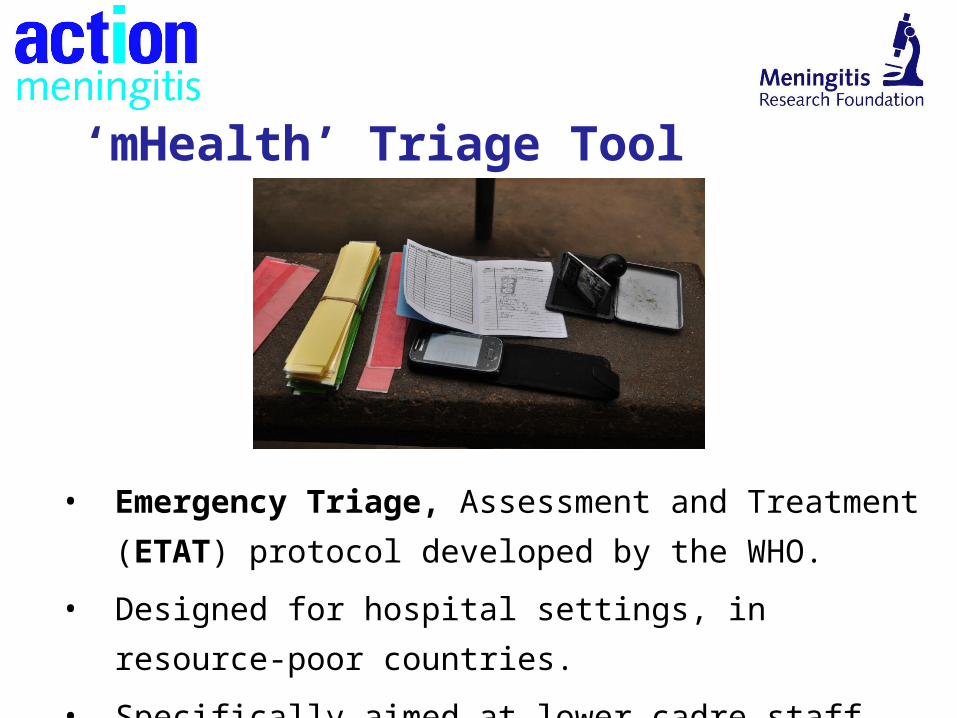
‘mHealth’ Triage Tool
• Emergency Triage, Assessment and Treatment (ETAT)
protocol developed by the WHO.
• Designed for hospital settings, in resource-poor countries.
• Specifically aimed at lower cadre staff.
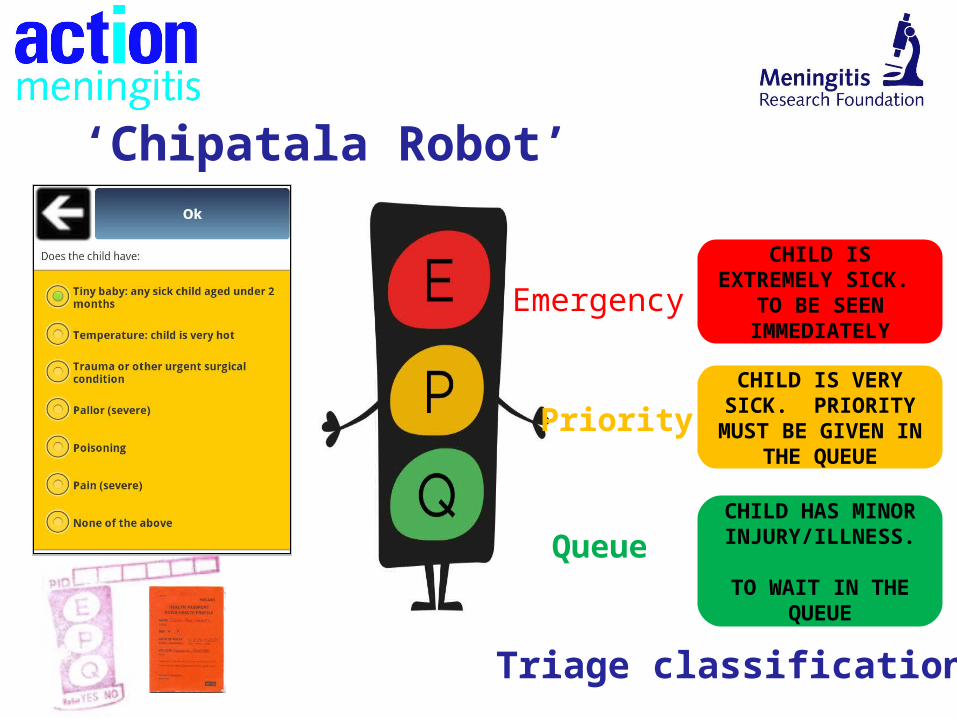
Emergency
PriorityCHILD IS VERY
SICK. PRIORITY MUST BE GIVEN IN THE QUEUE
Queue
CHILD HAS MINOR
INJURY/ILLNESS.
TO WAIT IN THE QUEUE
CHILD IS EXTREMELY SICK. TO BE
SEEN IMMEDIATELY
Triage classification
‘Chipatala Robot’
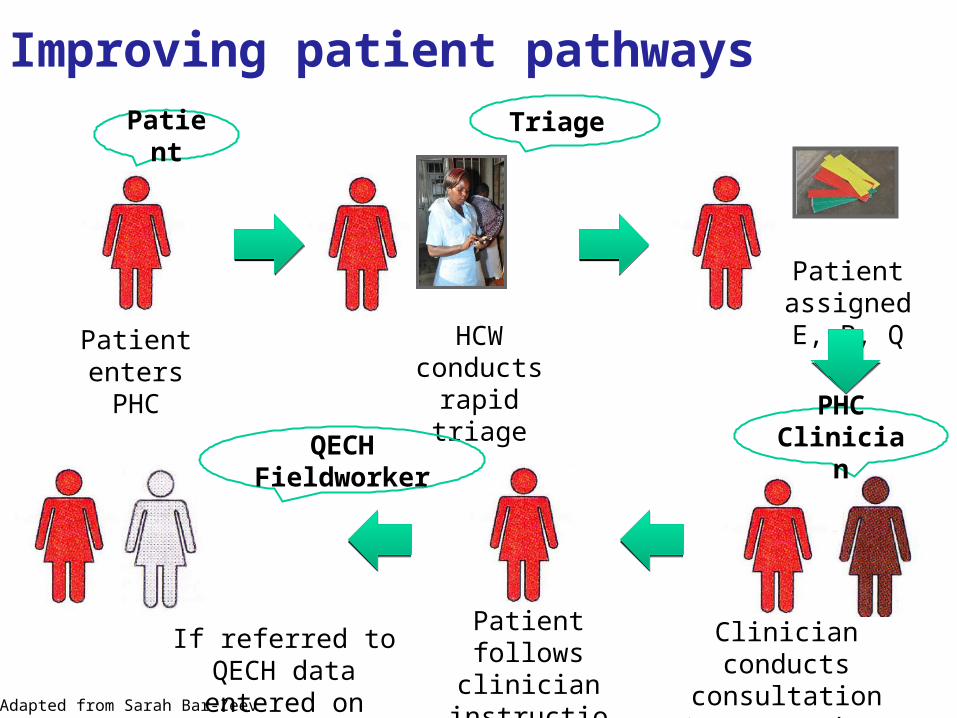
Improving patient pathways
Patient enters PHC
HCW conducts rapid triage
Patient assigned E, P, Q
Clinician conducts consultation &
enters dataAdapted from Sarah Bar-Zeev (2012)
Patient follows clinician
instructions
Patient Triage
PHC ClinicianQECH
Fieldworker
If referred to QECH data entered on arrival
Bangwe clinic
Evaluation
• Measured agreement between HSA triage assessment and clinician triage assessment.
• Above chance agreement for concordance between triageand clinician assessment (kappa = 0.71)
Accuracy of triage
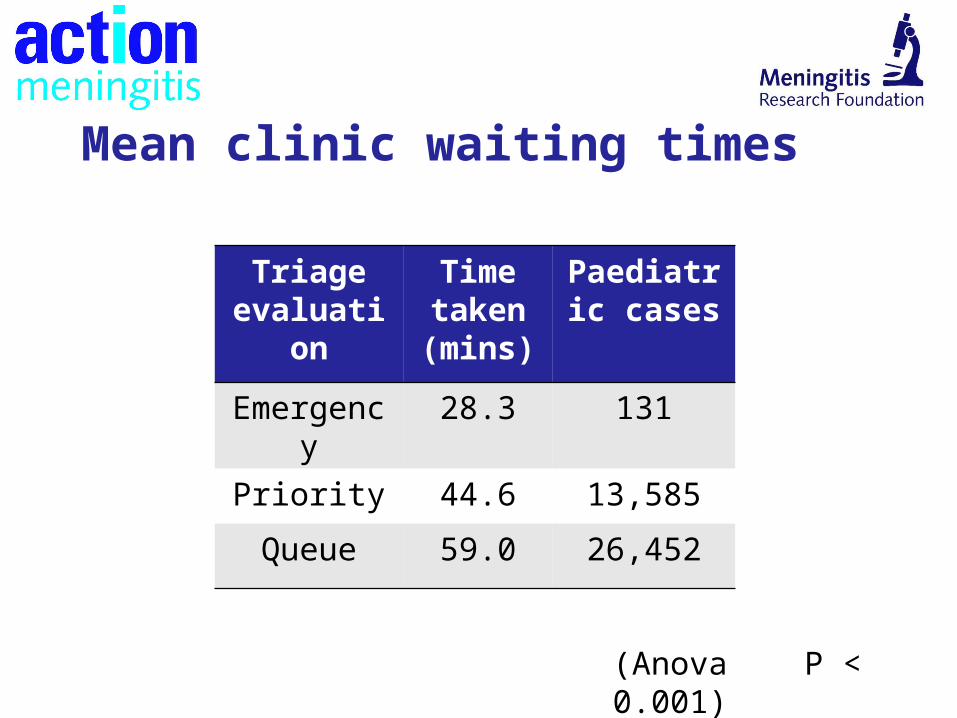
(Anova P < 0.001)
Triage evaluation
Time taken (mins)
Paediatric cases
Emergency 28.3 131
Priority 44.6 13,585
Queue 59.0 26,452
Mean clinic waiting times
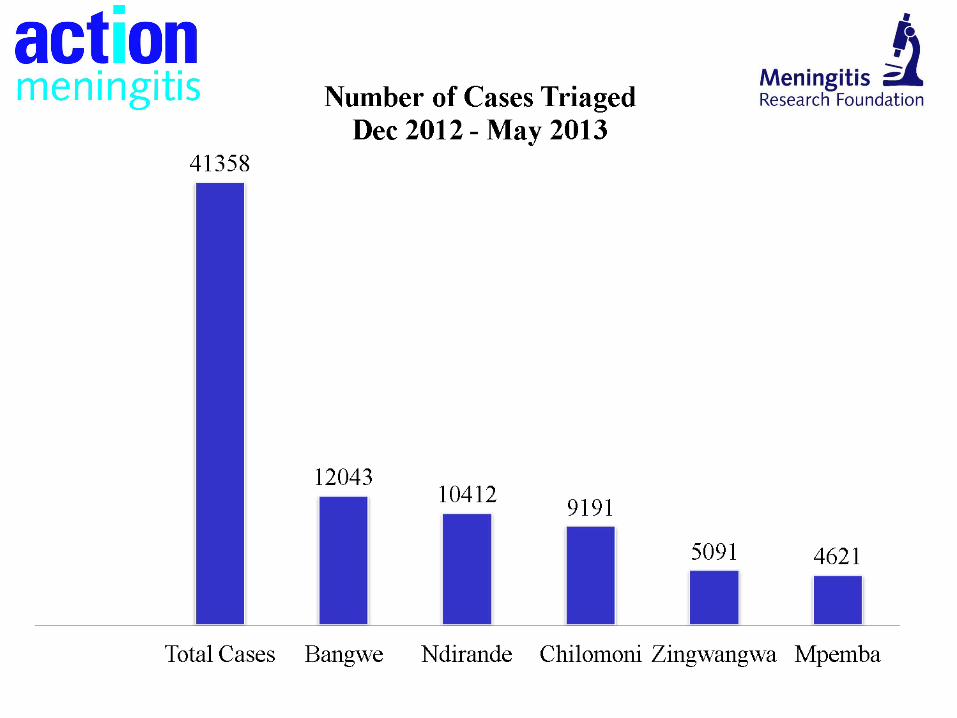
• Out of 41,358 children triaged 1.6% (644) were referred to QECH
• From the 644 referrals 37.3% (240) arrived at QECH
• Overall mean time to QECH 5.5hrs
• 62.7% (404) of referrals from PHCS did not reach QECH
Referrals
“At Bangwe we are now working together as a team. It is helping us manage the children so much better. We are seeing them far more quickly than before”
“At Bangwe we are now working together as a team. It is helping us manage the children so much better. We are seeing them far more quickly than before”
Medical Assistant, 2013
Qualitative findings
Chikhwawa District• Rural setting, 2.5hrs outside Blantyre• Chipatala Robot triage system at two additional
Primary Clinics• Also in District Hospital• 40 HCW trained
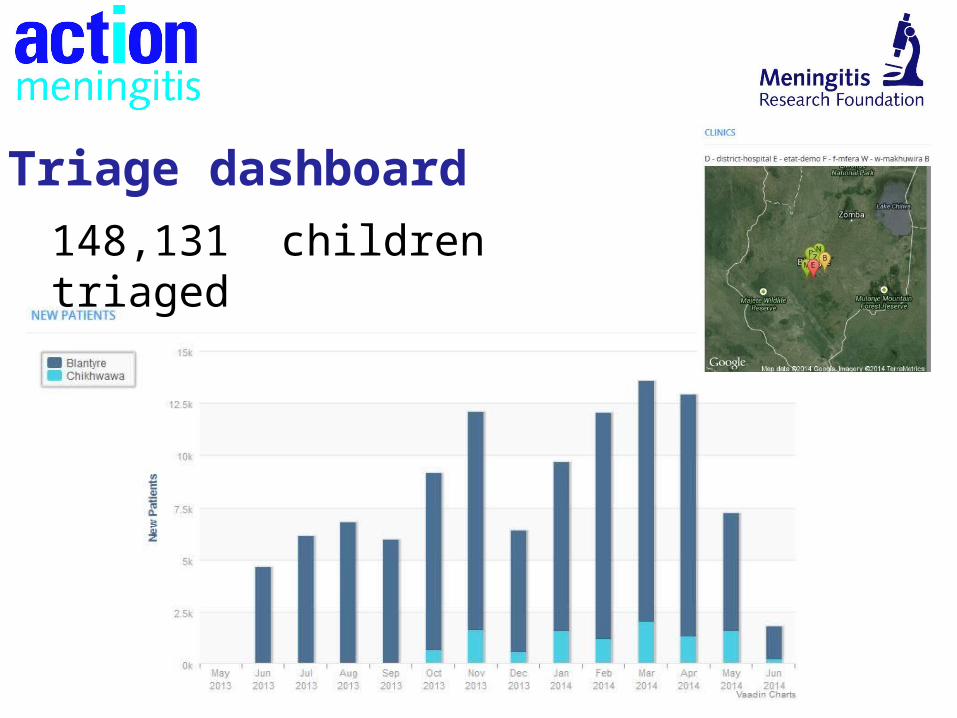
148,131 children triaged
Triage dashboard
Next steps
• Continue triage system in 8 centres.
- High drop-out between primary level referral and arrival at tertiary (63%).
- How best to adapt triage for primary setting?
- Provide evidence that triage can be successfully implemented in a sustainable and cost-effective way.
Primary Health Level
Community Level
• Continue to develop theatre and radio interventions.

Mphatso Cheonga, 2012
“I only wish the primary health centres could
improve on diagnosis and recognising
symptoms quicker...”
“I only wish the primary health centres could
improve on diagnosis and recognising
symptoms quicker...”
Acknowledgments MLWNicola DesmondRob HeydermanDeborah NyirendaQueen DubeElizabeth MolyneuxRob Heyderman
MRFLinda GlennieChris HeadThomasena O’ByrneZione KalvosiMeliya KwelepetaBernadetta Payesa
MoHNorman LufesiDr Owen MalemaDr Amber Manjidu
ETAT RegistrarsDr Zondiwe MwanzaDr Thembi ChirwaDr Yabwile MulambiaMtisunge Gondwe
D-Tree InternationalDr Marije GeldofDr Marc MitchellPhidelis Suwedi
Primary ClinicsBangwe: Tinkhani BophaniChilomoni: Dalitso NamasaniNdirande: Francis PhiriMpemba: Rodgers KuyokwaZingwangwa: Margaret Chingona
All photos reproduced by kind permission of participants
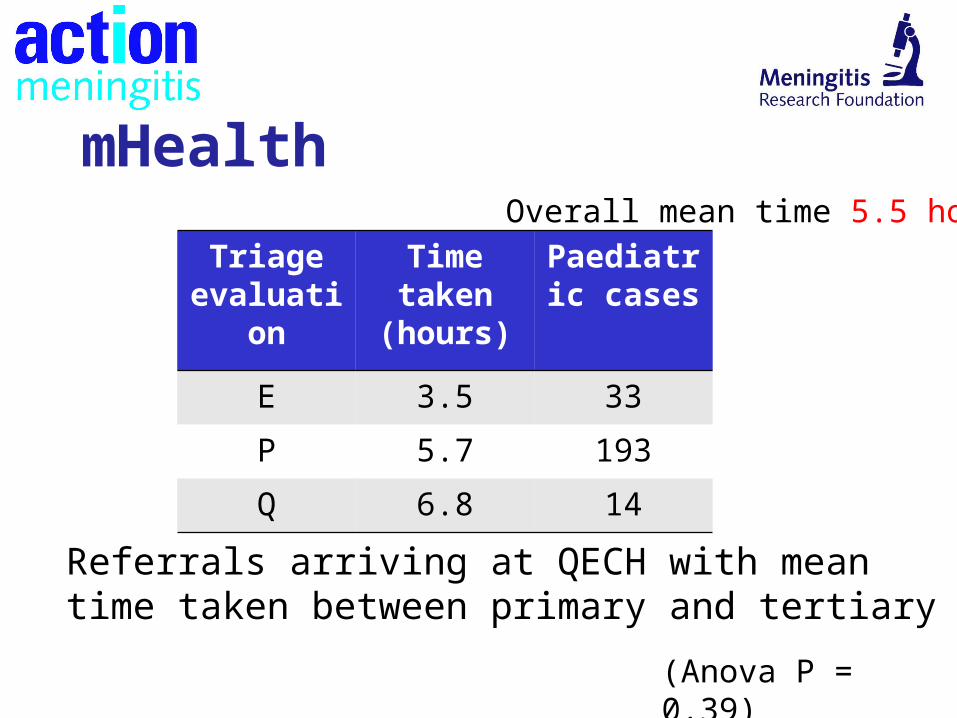
Referrals arriving at QECH with mean time taken between primary and tertiary
(Anova P = 0.39)
mHealth
Triage evaluation
Time taken
(hours)
Paediatric cases
E 3.5 33
P 5.7 193
Q 6.8 14
Overall mean time 5.5 hours
Background Research
• £700K MRF research in Malawi
• Late presentation at tertiary level contributes to
mortality from acute bacterial meningitis (ABM)
• Study into barriers of recognition and action in
treating ABM in Malawi…