Embed Size (px)
Citation preview
Lecture F. Arrigo, Messina
Saturday, October, 11-2014 10.00 - 10.30
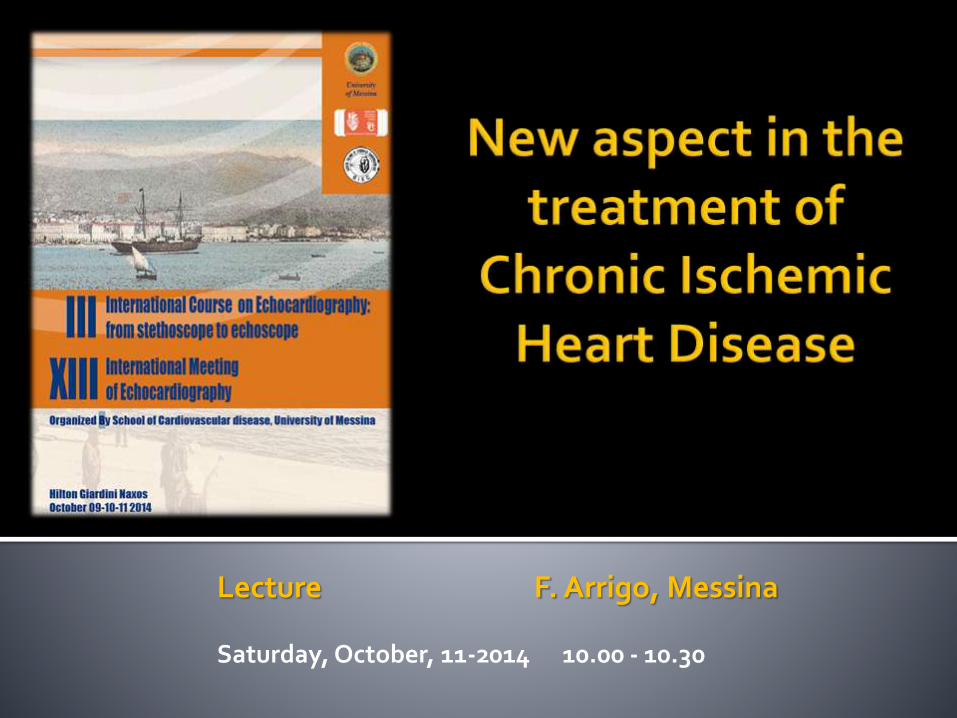
I25.0 Atherosclerotic cardiovascular disease, so described
I25.1 Atherosclerotic heart diseaseCoronary (artery):• atheroma• atherosclerosis• disease• sclerosis
I25.2 Old myocardial infarction• Healed myocardial infarction• Past myocardial infarction diagnosed by ECG
or other special investigation, but currently presenting no symptoms
I25.3 Aneurysm of heart
Aneurysm: a) mural b) ventricular
I25.4 Coronary artery aneurysmCoronary arteriovenous fistula, acquiredExcludes congenital coronary (artery) aneurysm
I25.5 Ischaemic cardiomyopathy
I25.6
Silent myocardial ischaemia
I25.8
Other forms of chronic ischaemicheart diseaseAny condition in I21-I22 and I24.- specified as chronic or with a stated duration of more than 4 weeks (more than 28 days) from onset
I25.9
Chronic ischaemic heart disease, unspecifiedIschaemic heart disease (chronic) NOS
Stable coronary artery disease (ESC) Stable Ischemic Heart Disease (ACC/AHA) Stable angina pectoris (NICE) Stable coronary Heart disease (Braunwald)
Some authors include
Microvascular Angina
Vasospastic Angina
Inducible myocardial Ischemia
Previous revascularization (CABG o PCI)

REACH registryAnnual event rates in stable CAD outpatients (n=38602), 1-year follow-up
Steg PG, et al. JAMA. 2007;297:1197-1206
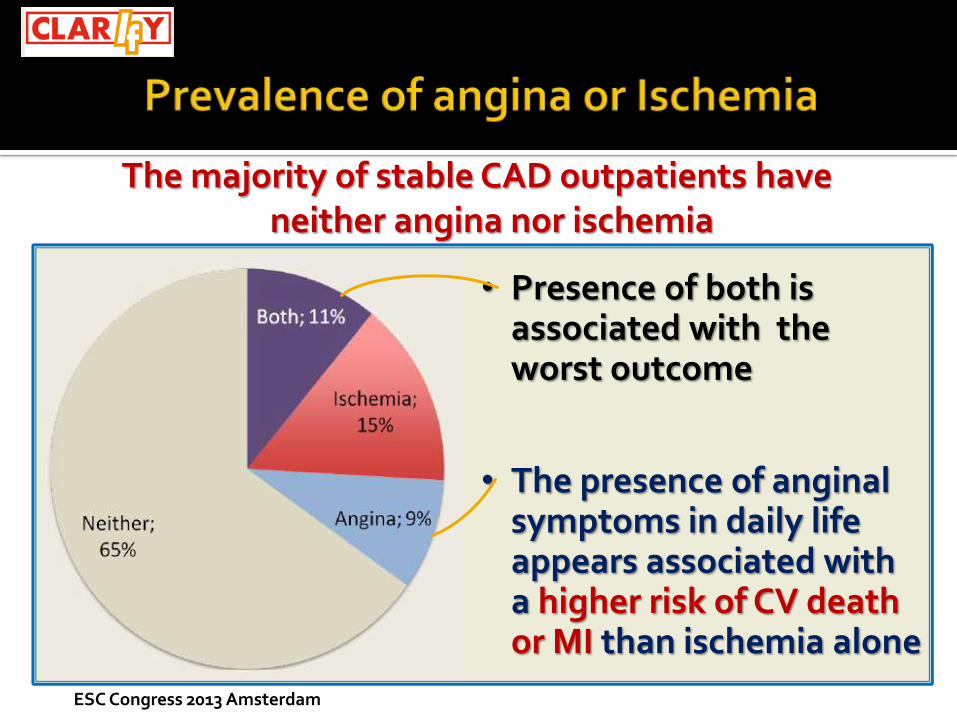
The majority of stable CAD outpatients haveneither angina nor ischemia
ESC Congress 2013 Amsterdam
• Presence of both isassociated with the worst outcome
• The presence of anginalsymptoms in daily life appears associated witha higher risk of CV deathor MI than ischemia alone
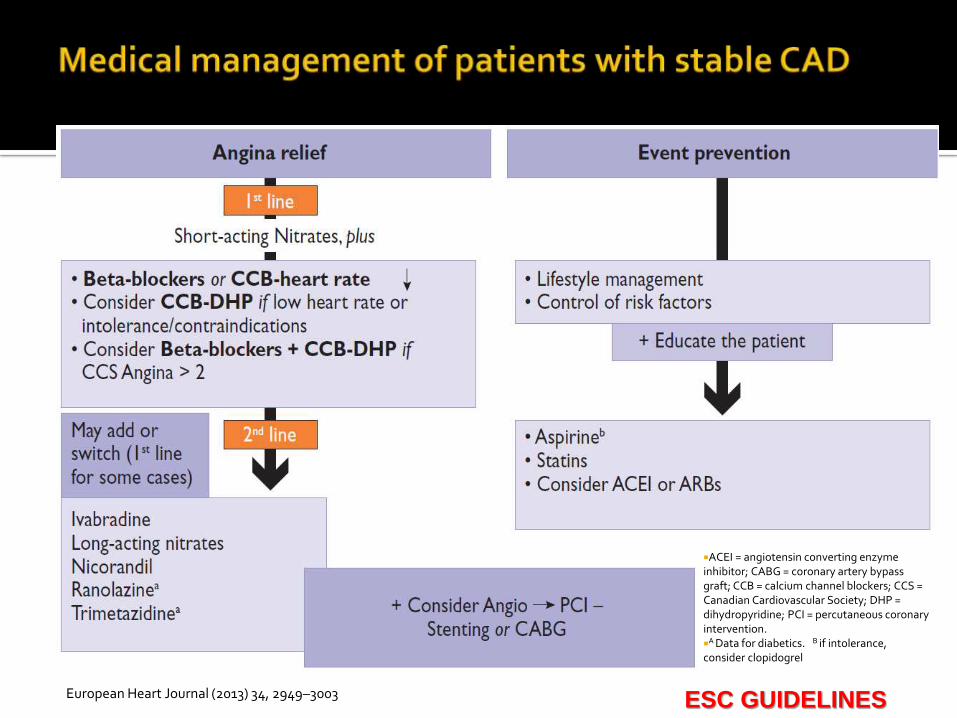
Event preventionAngina/ischemia relief
European Heart Journal (2013) 34, 2949–3003
European Heart Journal (2013) 34, 2949–3003
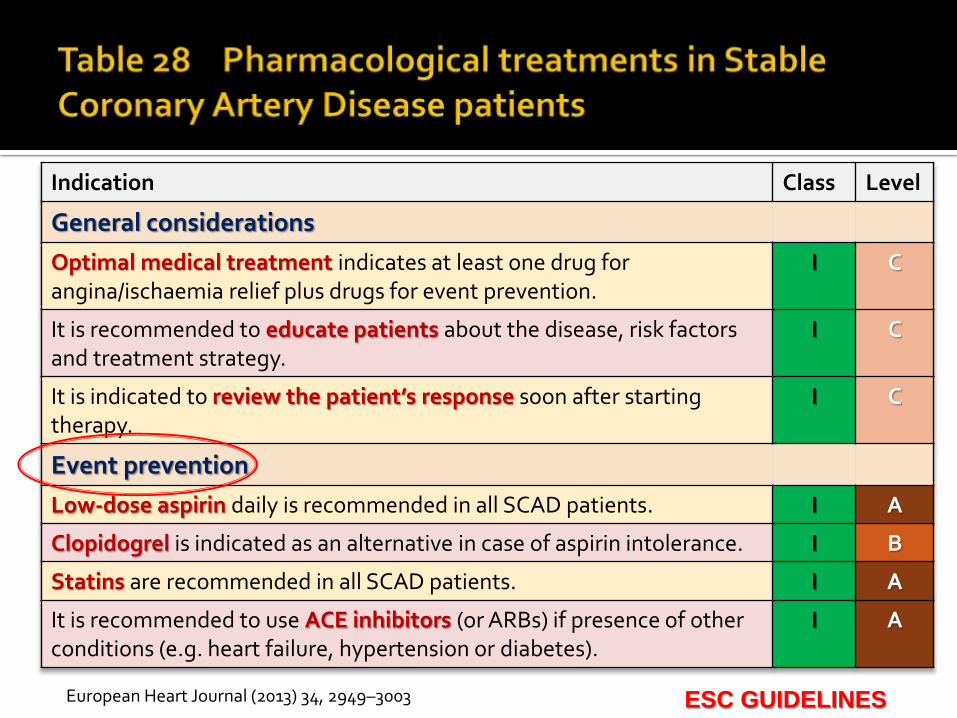
Indication Class Level
General considerations
Optimal medical treatment indicates at least one drug for angina/ischaemia relief plus drugs for event prevention.
I C
It is recommended to educate patients about the disease, risk factors and treatment strategy.
I C
It is indicated to review the patient’s response soon after starting therapy.
I C
Event prevention
Low-dose aspirin daily is recommended in all SCAD patients. I A
Clopidogrel is indicated as an alternative in case of aspirin intolerance. I B
Statins are recommended in all SCAD patients. I A
It is recommended to use ACE inhibitors (or ARBs) if presence of other conditions (e.g. heart failure, hypertension or diabetes).
I A
ESC GUIDELINES
European Heart Journal (2013) 34, 2949–3003
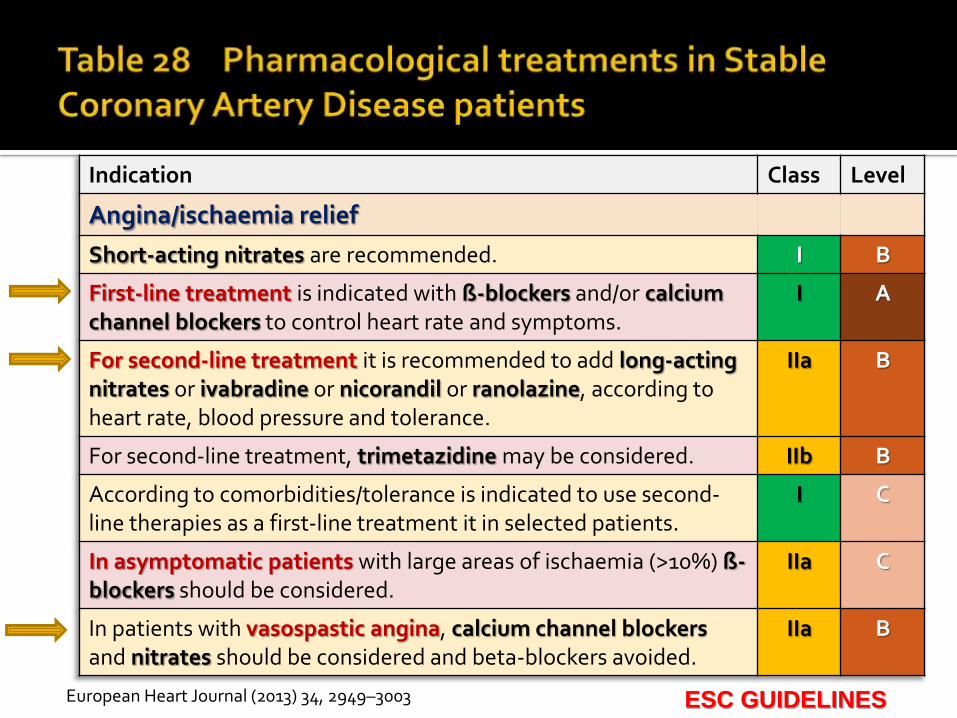
Indication Class Level
Angina/ischaemia relief
Short-acting nitrates are recommended. I B
First-line treatment is indicated with ß-blockers and/or calcium channel blockers to control heart rate and symptoms.
I A
For second-line treatment it is recommended to add long-acting nitrates or ivabradine or nicorandil or ranolazine, according to heart rate, blood pressure and tolerance.
IIa B
For second-line treatment, trimetazidine may be considered. IIb B
According to comorbidities/tolerance is indicated to use second-line therapies as a first-line treatment it in selected patients.
I C
In asymptomatic patients with large areas of ischaemia (>10%) ß-blockers should be considered.
IIa C
In patients with vasospastic angina, calcium channel blockers and nitrates should be considered and beta-blockers avoided.
IIa B
ESC GUIDELINES
European Heart Journal (2013) 34, 2949–3003
ACEI = angiotensin converting enzyme inhibitor; CABG = coronary artery bypass graft; CCB = calcium channel blockers; CCS = Canadian Cardiovascular Society; DHP = dihydropyridine; PCI = percutaneous coronaryintervention.
A Data for diabetics. B if intolerance, consider clopidogrel
ESC GUIDELINES

Long–acting nitrates
what's new

anti-ischaemic efficacy of PETN 80 mg b.i.d. (morning and mid-day) over placebo in 655 patients with chronic stable angina pectoris.
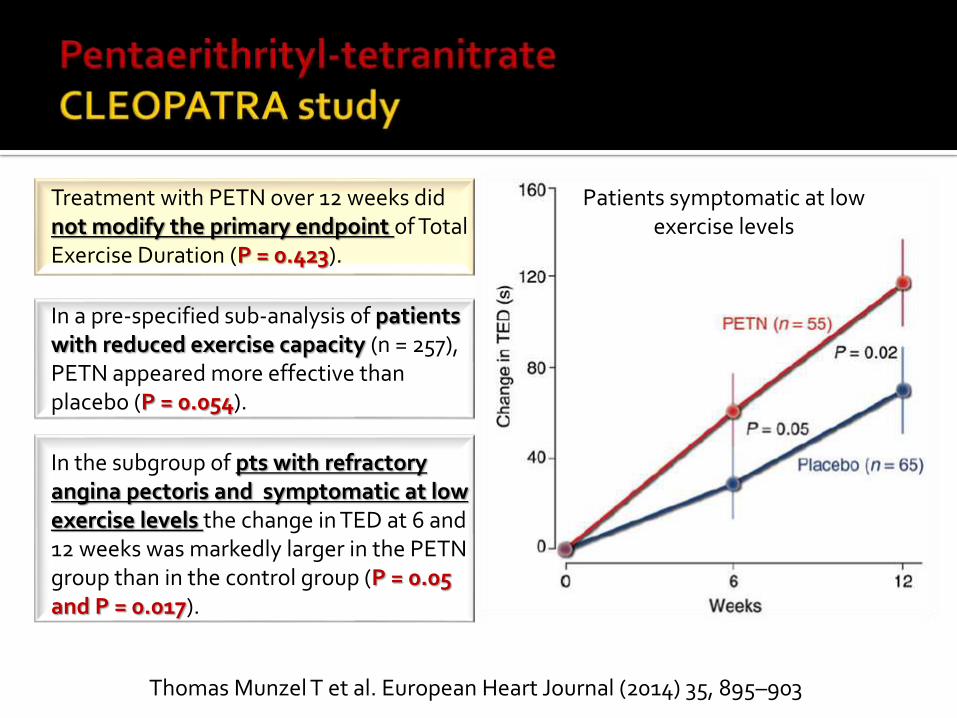
Thomas Munzel T et al. European Heart Journal (2014) 35, 895–903
Treatment with PETN over 12 weeks did not modify the primary endpoint of Total Exercise Duration (P = 0.423).
In a pre-specified sub-analysis of patients with reduced exercise capacity (n = 257), PETN appeared more effective than placebo (P = 0.054).
In the subgroup of pts with refractory angina pectoris and symptomatic at low exercise levels the change in TED at 6 and 12 weeks was markedly larger in the PETN group than in the control group (P = 0.05 and P = 0.017).
Patients symptomatic at low exercise levels

Betablockers
what's new

Meta analysis of 26 trials, including 6,108 patients, showed no significant survival benefits of beta-blockers (OR 0.92, 95% CI 0.62 to 1.38) when compared to placebo in patients with stableangina.
Shu DF, Dong BR, Lin XF, Wu TX, Liu GJ . Eur J Cardiovasc Prev Rehabil Apr 27 2011
REACH registry, which included 44 708 participants, also showed that beta-blocker therapy in stable CAD patients did not provide any benefit.
Bangalore S, et al, on behalf of the REACH Registry Investigators. JAMA. 2012 Oct 3;308(13):1340-9.

The purpose of this study was to assess the association of beta-blockers with outcomes among patients with new-onset CHD.
26,793 consecutive patients discharged after the first CHD event (ACS or coronary revascularization) who did not use beta-blockers in the year before entry.
Average follow-up of 3.7 years
Hazard Ratio (HR) for death or MI associated with beta-blocker
Interaction tests to determine whether the association differed for patients with or without a recent MI.
Andersson C, Shilane D, Go AS, Chang TI, Kazi D, Solomon MD, Boothroyd DB, Hlatky MA. J Am Coll Cardiol. 2014 Jul 22;64(3):247-52.
Andersson C, Shilane D, Go AS, Chang TI, Kazi D, Solomon MD, Boothroyd DB, Hlatky MA. 2014 Jul 22;64(3):247-52.
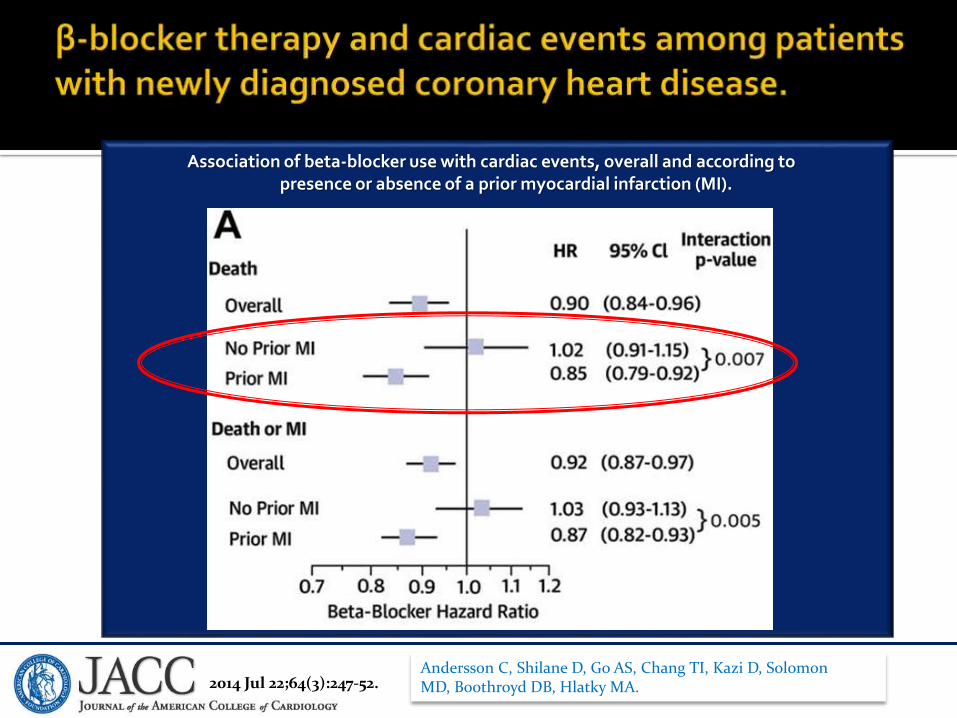
Association of beta-blocker use with cardiac events, overall and according to presence or absence of a prior myocardial infarction (MI).
Andersson C, et al J Am Coll Cardiol. 2014 Jul 22;64(3):247-52. Andersson C, Shilane D, Go AS, Chang TI, Kazi D, Solomon MD, Boothroyd DB, Hlatky MA. 2014 Jul 22;64(3):247-52.

Post hoc analysis from the CHARISMAa trial. The cohorts were divided into 2 groups based on baseline β-blocker use. 28 months of follow-up.
4772 patients with prior MI 7804 patients with known atherothrombosis 2101 patients with risk factors alone but without heart failure.
Primary outcome was a composite of nonfatal MI, stroke, or CV mortality.

PRIOR MI COHORT β-blocker use was associated with
▪ lower risk of the primary outcome (HR 0.69; 95% CI, 0.50-0.94; P=0.021)
▪ lower risk of recurrent MI (HR 0.62; 95% CI, 0.39-1.00; P=0.049) ▪ no difference in mortality (52 [5.3%] versus 66 [6.7%]; P=0.20).
KNOWN ATHEROTHROMBOSIS AND RISK FACTORS ALONE COHORTS β-blocker use was not associated with lower ischemic
outcomes
RISK FACTORS ALONE COHORTS trend toward a higher risk of stroke (3.5% versus 1.5%;
HR 2.13; 95% CI 0.92-4.92; P=0.079)
Bangalore S, Bhatt DL, Steg PG, et al. Circ Cardiovasc Qual Outcomes 2014; Sep 30. [Epub ahead of print]
a Clopidogrel for High Atherothrombotic Risk and Ischemic Stabilization, Management, and Avoidance
Ivabradine
what's new
Presented at ESC Congress 2014 Hotline 2
19,102 patients who had both stable CAD without clinicalheart failure and a heart rate of 70 beats per minute or more.
After a median follow-up of 27.8 months, there was nosignificant difference between the ivabradine group andthe placebo group in the incidence of the primary endpoint, death from CV causes and nonfatal MyocardialInfarction.
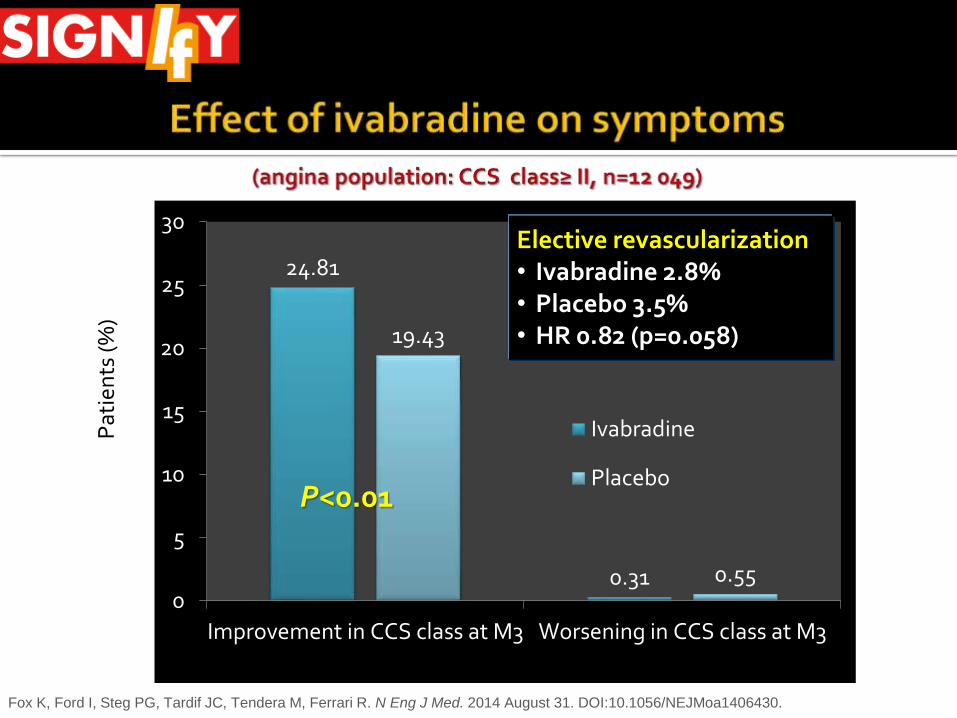
24.81
0.31
19.43
0.550
5
10
15
20
25
30
Improvement in CCS class at M3 Worsening in CCS class at M3
Ivabradine
Placebo
Pat
ien
ts (%
)
P<0.01
Elective revascularization• Ivabradine 2.8% • Placebo 3.5% • HR 0.82 (p=0.058)
Fox K, Ford I, Steg PG, Tardif JC, Tendera M, Ferrari R. N Eng J Med. 2014 August 31. DOI:10.1056/NEJMoa1406430.

Ranolazine
what's new

The late inward Na current is increased in ischemic myocardium
direct antiischemiceffect
not dependent on changes in cardiac
work
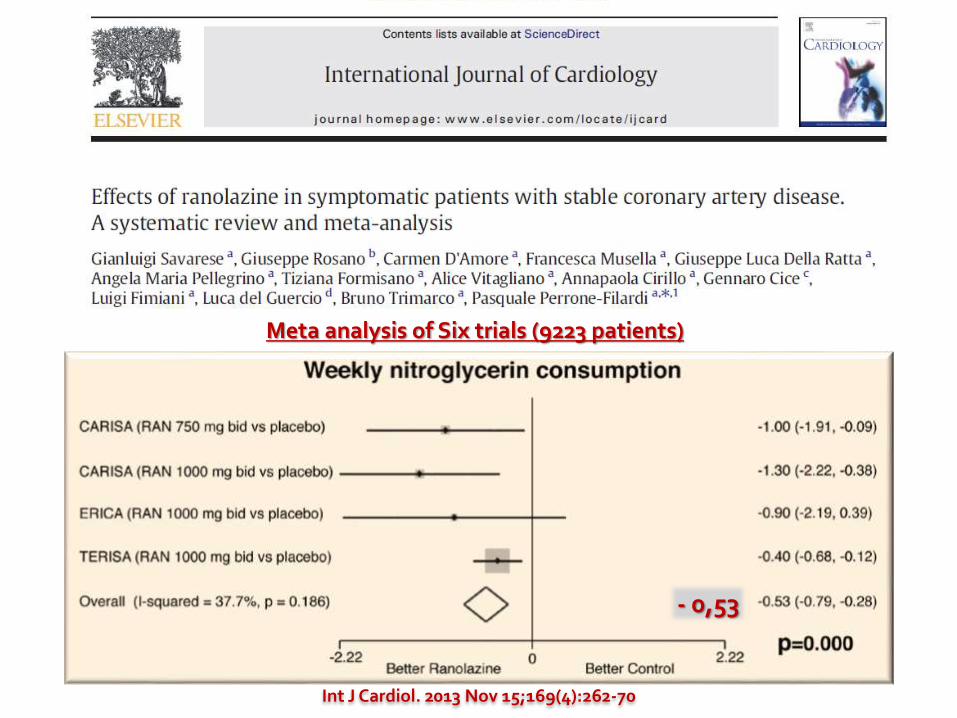
Meta analysis of Six trials (9223 patients)
- 0,53
Int J Cardiol. 2013 Nov 15;169(4):262-70
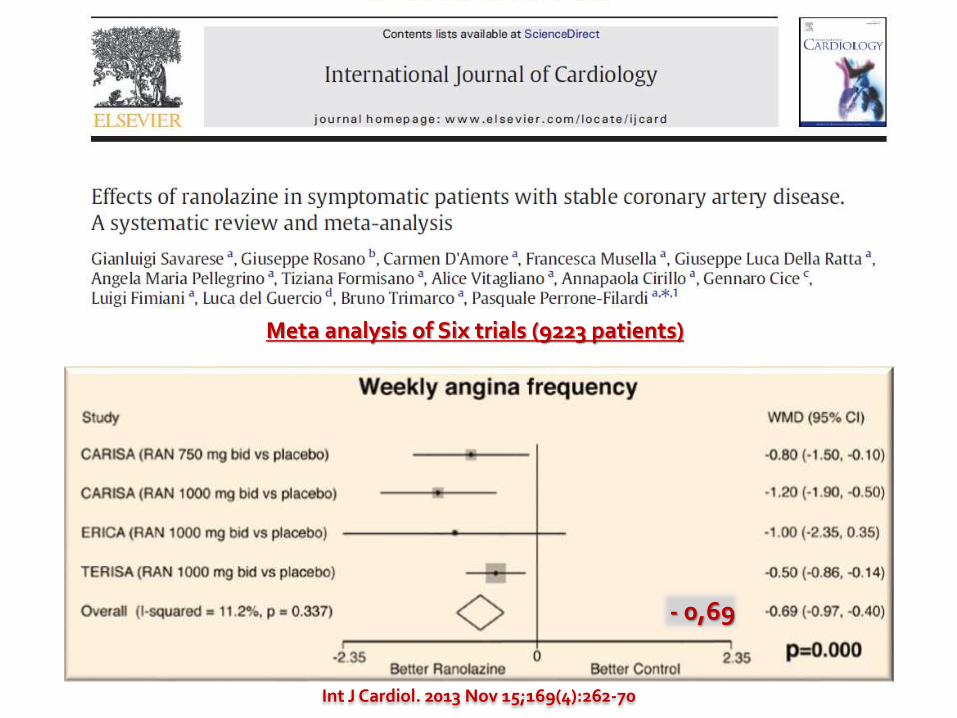
Meta analysis of Six trials (9223 patients)
- 0,53
Int J Cardiol. 2013 Nov 15;169(4):262-70
- 0,69
Patients (N = 92) answered a survey evaluating their perceptions of angina prior to ranolazineinitiation (based on recall of previous experience) and during ranolazine treatment.
Change in QoL was assessed using the PatientGlobal Impression of Change scale.
J. B. Muhlestein, S. Grehan. Drugs, 2013; 13:2007-213

N = 92 respondents
Patient-reportedchanges in quality of life on the Patient Global Impression ofChange scale sinceinitiating ranolazinetreatment.
79,4 %
J. B. Muhlestein, S. Grehan. Drugs, 2013; 13:2007-213
46 patients with stable microvascular angina pectoris (effort angina, positive exercise stress test [EST], normal coronary angiography, coronary flow reserve <2.5), whith symptoms inadequately controlled by standard anti-ischemic therapy
Ivabradine (5 mg twice daily), Ranolazine (375 mg twice daily), or placebo for 4 weeks.
The Seattle Angina Questionnaire (SAQ), EuroQoL scale, and EST were assessed at baseline and after treatment.
Coronary microvascular dilation in response to adenosine and to cold pressor test and peripheral endothelial function (by flow-mediated dilation) were also assessed.
Villano A, Di Franco A, Nerla R, Sestito A, Tarzia P, Lamendola P, Di Monaco A, Sarullo FM, Lanza GA, Crea F. Am J Cardiol. 2013 Jul 1;112(1):8-13
Both drugs improved SAQ items and EuroQoL scale (p <0.01)
Time to 1-mm ST-segment depression and EST duration improved by ranolazine.
No effects on coronary microvascular function and on flow-mediated dilation with drugs or placebo.
In conclusion, ranolazine and ivabradine may have a therapeutic role in MVA patients with inadequate control of symptoms with usual anti-ischemic therapy.
Villano A, Di Franco A, Nerla R, Sestito A, Tarzia P, Lamendola P, Di Monaco A, Sarullo FM, Lanza GA, Crea F. Am J Cardiol. 2013 Jul 1;112(1):8-13
Ranolazine Refractory Angina Registry was designed to evaluate the safety, tolerability, and effectiveness in RA patients.
100 patients were enrolled. Angina class, medications, major adverse cardiac events including
death, myocardial infarction, and revascularization were obtained at 1, 6, and 12 months.
Overall 43% of patients had a ≥2 class improvement in angina.
At 1 year, 57% patients remained on ranolazine Reasons for discontinuation included: side effects (n = 16), major
adverse cardiac events (n = 10), cost (n = 5), ineffective (n = 6), cost and ineffective (n = 3), and unknown (n = 3).
Bennett NM et al. Crit Pathw Cardiol. 2014 Sep;13(3):96-8.
The combination of ranolazine and dronedaroneappeared to lower the burden of atrial fibrillation (AF) by>70% over three months in 45% to 60% of patients withthe paroxysmal form of the arrhythmia.
A placebo-controlled limited size and phase 2 study

Optimal Medical Therapy
what's new
Many trials do not include “second line treatments”.
Adherence to prolonged and multiple treatments is very poor.
Observational studies (Reach, Euro Heart Survey, Clarify) showed underutilization of preventive and antianginal drugs.
Garg P et al. J Am Heart Assoc. 2014;3:e000882
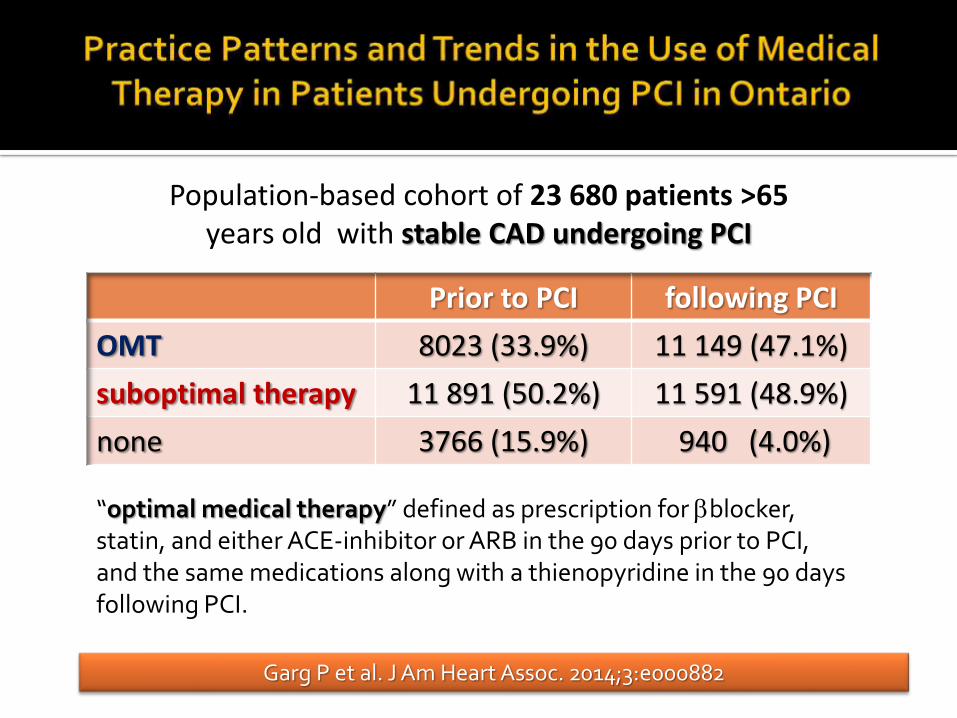
Prior to PCI following PCI
OMT 8023 (33.9%) 11 149 (47.1%)
suboptimal therapy 11 891 (50.2%) 11 591 (48.9%)
none 3766 (15.9%) 940 (4.0%)
Population-based cohort of 23 680 patients >65 years old with stable CAD undergoing PCI
“optimal medical therapy” defined as prescription for bblocker, statin, and either ACE-inhibitor or ARB in the 90 days prior to PCI, and the same medications along with a thienopyridine in the 90 days following PCI.
PCI / CABG

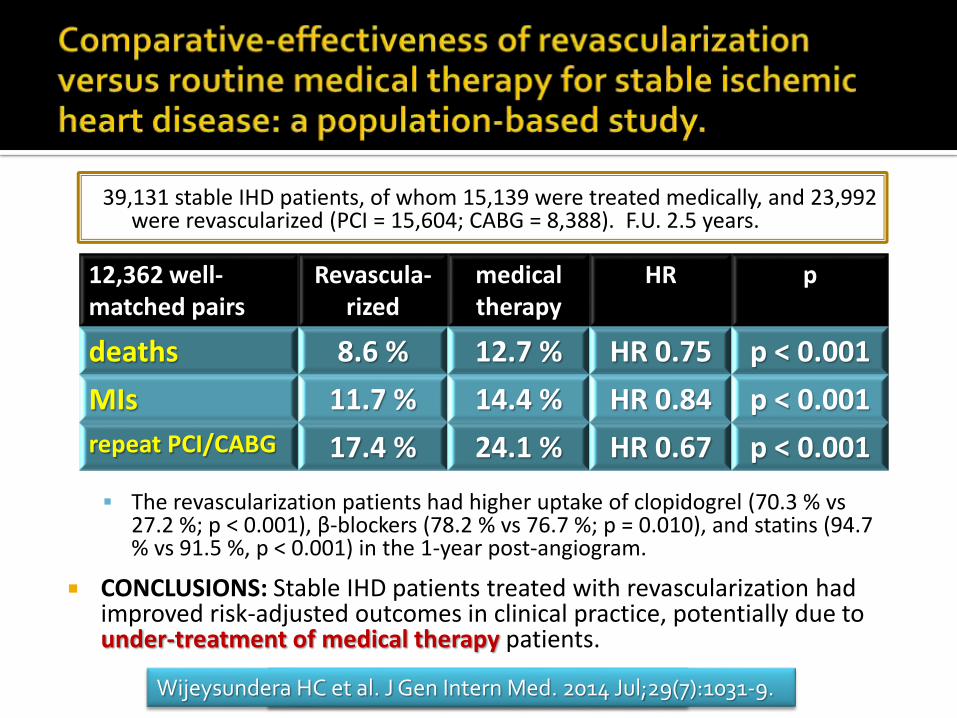
39,131 stable IHD patients, of whom 15,139 were treated medically, and 23,992 were revascularized (PCI = 15,604; CABG = 8,388). F.U. 2.5 years.
The revascularization patients had higher uptake of clopidogrel (70.3 % vs27.2 %; p < 0.001), β-blockers (78.2 % vs 76.7 %; p = 0.010), and statins (94.7 % vs 91.5 %, p < 0.001) in the 1-year post-angiogram.
CONCLUSIONS: Stable IHD patients treated with revascularization had improved risk-adjusted outcomes in clinical practice, potentially due to under-treatment of medical therapy patients.
J Gen Intern Med. 2014 Jul;29(7):1031-9.
12,362 well-matched pairs
Revascula-rized
medical therapy
HR p
deaths 8.6 % 12.7 % HR 0.75 p < 0.001
MIs 11.7 % 14.4 % HR 0.84 p < 0.001
repeat PCI/CABG 17.4 % 24.1 % HR 0.67 p < 0.001
Wijeysundera HC et al. J Gen Intern Med. 2014 Jul;29(7):1031-9.
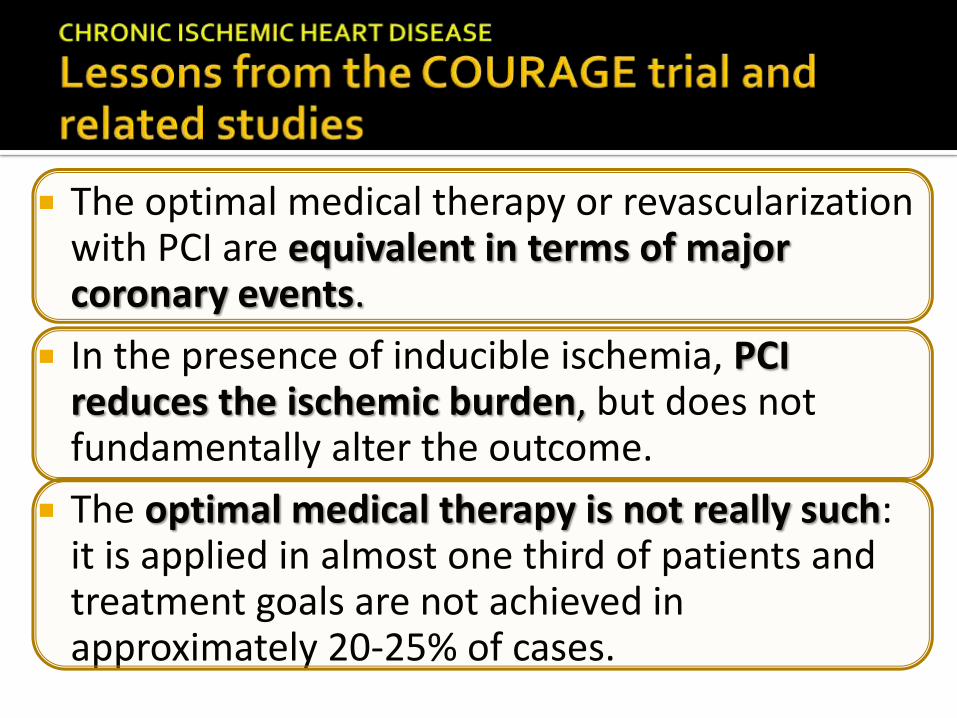
The optimal medical therapy or revascularization with PCI are equivalent in terms of major coronary events.
In the presence of inducible ischemia, PCI reduces the ischemic burden, but does not fundamentally alter the outcome.
The optimal medical therapy is not really such: it is applied in almost one third of patients and treatment goals are not achieved in approximately 20-25% of cases.
2014 ESC/EACTS Guidelines on myocardial revascularization
FFR-guided PCI
what's new

Downloaded from nejm.org by FRANCESCO ARRIGO on September 7, 2014.
N Engl J Med September 1, 2014
This report describes the prespecified 2-year results for the primary end point , a composite of death from any cause, nonfatal myocardialinfarction, or urgent revascularization.

Downloaded from nejm.org by FRANCESCO ARRIGO on September 7, 2014.
N Engl J Med September 1, 2014
1220 patients with stable coronary artery disease. FFR in all stenoses that were visible on angiography. Patients who had at least one stenosis with an FFR ≤ 0.80
were randomly assigned to undergo FFR-guided PCI plus OMT or to receive medical therapy alone.
The rate of the primary end point was significantly lower in the PCI group than inthe medical-therapy group (HR 0.39; P<0.001).
This reduction was driven by a lower rate of urgent revascularization in the PCI group (HR 0.23; P<0.001), with no significant between-group differences in the rates of deathand myocardial infarction.

Downloaded from nejm.org by FRANCESCO ARRIGO on September 7, 2014.
N Engl J Med September 1, 2014
In conclusion, among patients with stable CAD and ischemia, as shown by the presence of at least one stenosis with an FFR ≤ 0.80 in a large epicardial artery, the clinical outcome at 2 years was improved by FFR-guided PCI with second-generation DES plus the best available medical therapy, as compared with medical therapy alone.
In patients without hemodynamically significantstenosis, the best available medical therapy alone was associated with an excellent 2-year clinical outcome, regardless of the angiographic appearance of the stenoses.
Appropriate UseCriteria
what's new
Coronary revascularization is appropriate when the expected benefits, in terms of survival or health outcomes (symptoms, functional status, and/or quality of life) exceed the expected negative consequences of the procedure.

A appropriate; I inappropriate; U uncertain.


Complete Revascularization
what's new
Preventive Angioplasty in Myocardial Infarction(PRAMI)
▪ N Engl J Med. 2013;369:1115-1123
65% reduction in adverse events if complete revascularization was performed at the time of initialPCI
Complete versus Lesion-only Primary PCI Trial (CvLPRIT)
▪ ESC Congress 2014
55% reduction in major adverse CV events in patients presenting for primary PCI when non-infarct related artery is treated on the index admission

Chronic IHD is a very heterogeneous disease
With symptoms
Without symptoms
Treatment is aimed to
prevent acute events
reduce symptoms
To achieve these goals
no choice between OMT and PCI, but ..
…appropriate use of both.