Embed Size (px)
Citation preview
Chap
ter
46Conor P. Shortt, MBBCh, MSc, andHanna M. Zafar, MD, MHS
MRI of the Knee
1. What sequences should be included in a standard magnetic resonance imaging (MRI) knee protocol?Sequences should include sagittal proton density–weighted (non–fat-saturated), and fat-saturated T2-weighted sequences in sagittal, coronal, and axial planes. A non–fat-saturated T1-weighted sequence (preferably in the coronal plane) is also recommended.
2. What structures in the knee are best evaluated in each plane?• Sagittal: Anterior cruciate ligament (ACL)and posterior cruciate ligament (PCL), medial and lateral menisci, medial and
lateral compartment cartilage, patellofemoral cartilage, and extensor mechanism• Coronal : Medial and lateral collateral ligaments, medial and lateral menisci, and medial and lateral compartment
cartilage• Axial : Patella, patellar retinacula, patellofemoral cartilage, and Baker cysts
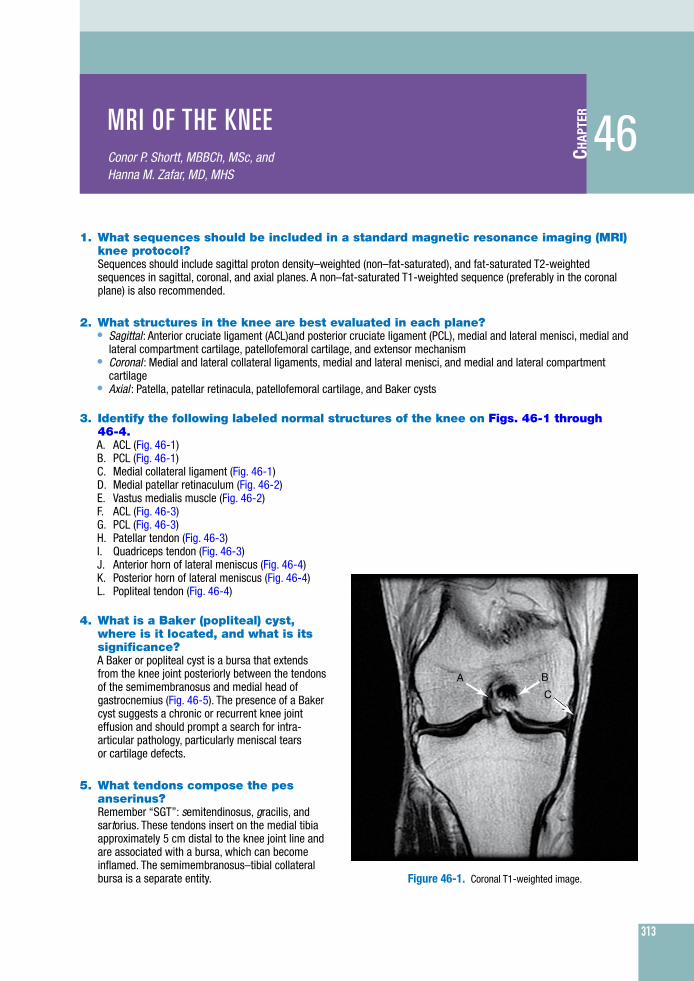
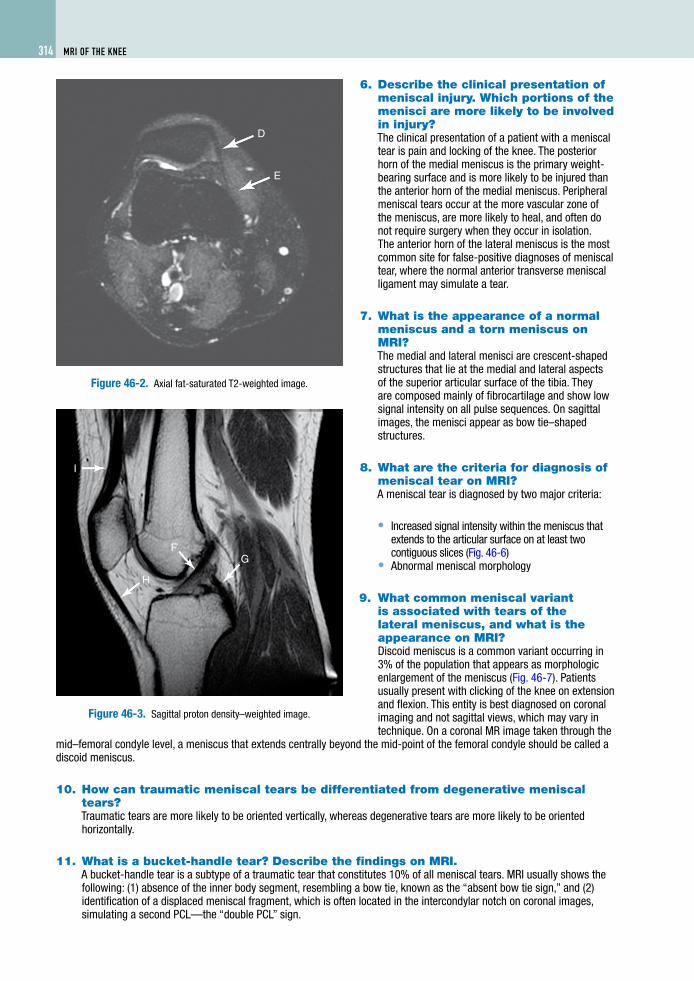
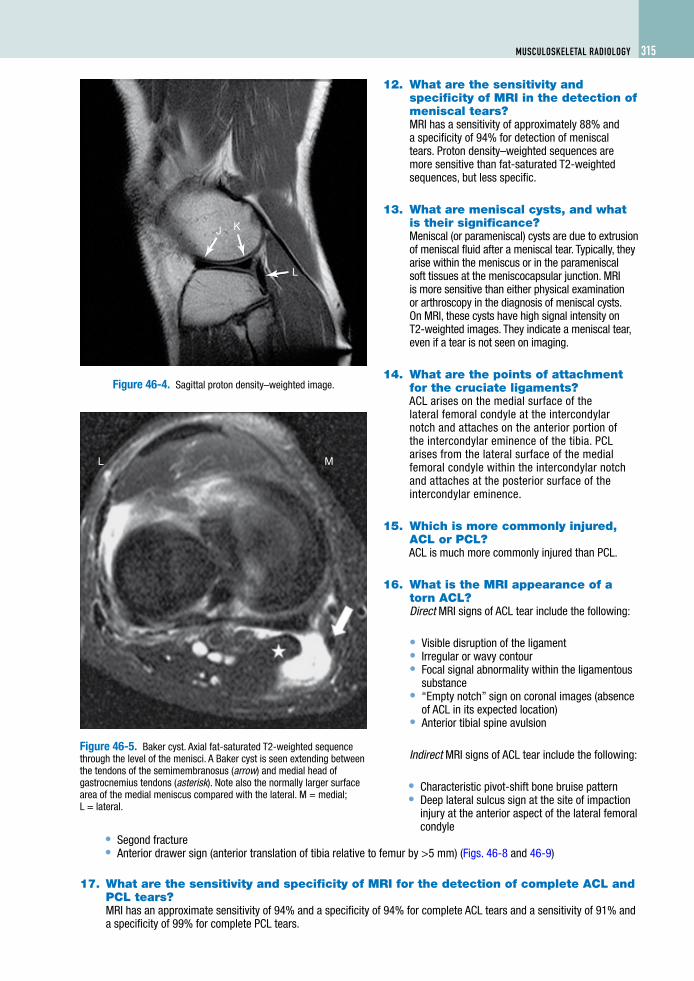
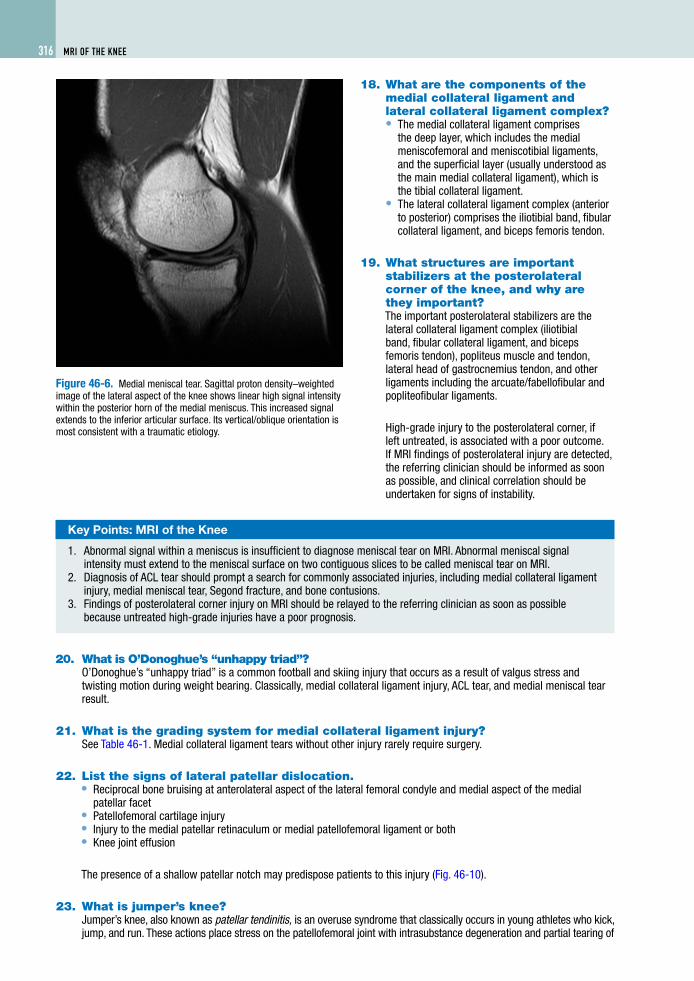
3. Identify the following labeled normal structures of the knee on Figs. 46-1 through 46-4.A. ACL (Fig. 46-1)B. PCL (Fig. 46-1)C. Medial collateral ligament (Fig. 46-1)D. Medial patellar retinaculum (Fig. 46-2)E. Vastus medialis muscle (Fig. 46-2)F. ACL (Fig. 46-3)G. PCL (Fig. 46-3)H. Patellar tendon (Fig. 46-3)I. Quadriceps tendon (Fig. 46-3)J. Anterior horn of lateral meniscus (Fig. 46-4)
A B
C
Figure 46-1. Coronal T1-weighted image.
K. Posterior horn of lateral meniscus (Fig. 46-4)L. Popliteal tendon (Fig. 46-4)
4. What is a Baker (popliteal) cyst, where is it located, and what is its significance?A Baker or popliteal cyst is a bursa that extends from the knee joint posteriorly between the tendons of the semimembranosus and medial head of gastrocnemius (Fig. 46-5). The presence of a Baker cyst suggests a chronic or recurrent knee joint effusion and should prompt a search for intra-articular pathology, particularly meniscal tears or cartilage defects.
5. What tendons compose the pes anserinus?Remember “SGT”: semitendinosus, gracilis, and sartorius. These tendons insert on the medial tibia approximately 5 cm distal to the knee joint line and are associated with a bursa, which can become inflamed. The semimembranosus–tibial collateral bursa is a separate entity.
313
314 MRI of the Knee
D
E
Figure 46-2. Axial fat-saturated T2-weighted image.
F
I
H
G
Figure 46-3. Sagittal proton density–weighted image.
6. Describe the clinical presentation of meniscal injury. Which portions of the menisci are more likely to be involved in injury?The clinical presentation of a patient with a meniscal tear is pain and locking of the knee. The posterior horn of the medial meniscus is the primary weight-bearing surface and is more likely to be injured than the anterior horn of the medial meniscus. Peripheral meniscal tears occur at the more vascular zone of the meniscus, are more likely to heal, and often do not require surgery when they occur in isolation. The anterior horn of the lateral meniscus is the most common site for false-positive diagnoses of meniscal tear, where the normal anterior transverse meniscal ligament may simulate a tear.
7. What is the appearance of a normal meniscus and a torn meniscus on MRI?The medial and lateral menisci are crescent-shaped structures that lie at the medial and lateral aspects of the superior articular surface of the tibia. They are composed mainly of fibrocartilage and show low signal intensity on all pulse sequences. On sagittal images, the menisci appear as bow tie–shaped structures.
8. What are the criteria for diagnosis of meniscal tear on MRI?A meniscal tear is diagnosed by two major criteria:
• Increased signal intensity within the meniscus that extends to the articular surface on at least two contiguous slices (Fig. 46-6)
• Abnormal meniscal morphology
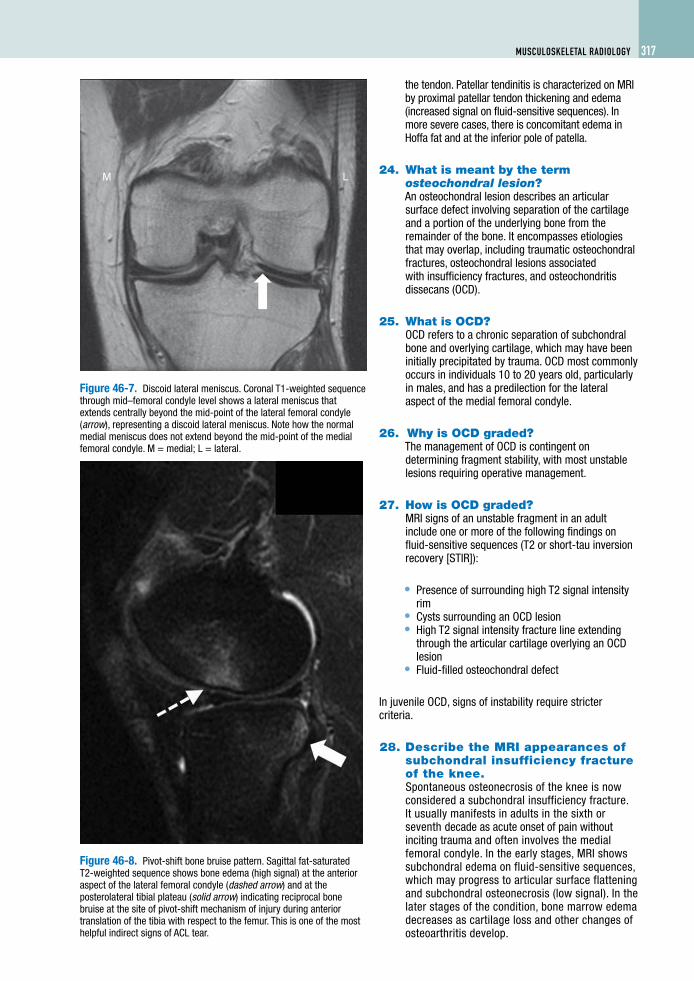
9. What common meniscal variant is associated with tears of the lateral meniscus, and what is the appearance on MRI?Discoid meniscus is a common variant occurring in 3% of the population that appears as morphologic enlargement of the meniscus (Fig. 46-7). Patients usually present with clicking of the knee on extension and flexion. This entity is best diagnosed on coronal imaging and not sagittal views, which may vary in technique. On a coronal MR image taken through the
mid–femoral condyle level, a meniscus that extends centrally beyond the mid-point of the femoral condyle should be called a discoid meniscus.
10. How can traumatic meniscal tears be differentiated from degenerative meniscal tears?Traumatic tears are more likely to be oriented vertically, whereas degenerative tears are more likely to be oriented horizontally.
11. What is a bucket-handle tear? Describe the findings on MRI.A bucket-handle tear is a subtype of a traumatic tear that constitutes 10% of all meniscal tears. MRI usually shows the following: (1) absence of the inner body segment, resembling a bow tie, known as the “absent bow tie sign,” and (2) identification of a displaced meniscal fragment, which is often located in the intercondylar notch on coronal images, simulating a second PCL—the “double PCL” sign.
MRI of the Knee 315MusculosKeletal RadIology
L M
Figure 46-5. Baker cyst. Axial fat-saturated T2-weighted sequence through the level of the menisci. A Baker cyst is seen extending between the tendons of the semimembranosus (arrow) and medial head of gastrocnemius tendons (asterisk). Note also the normally larger surface area of the medial meniscus compared with the lateral. M = medial; L = lateral.
J
L
K
Figure 46-4. Sagittal proton density–weighted image.
12. What are the sensitivity and specificity of MRI in the detection of meniscal tears?MRI has a sensitivity of approximately 88% and a specificity of 94% for detection of meniscal tears. Proton density–weighted sequences are more sensitive than fat-saturated T2-weighted sequences, but less specific.
13. What are meniscal cysts, and what is their significance?Meniscal (or parameniscal) cysts are due to extrusion of meniscal fluid after a meniscal tear. Typically, they arise within the meniscus or in the parameniscal soft tissues at the meniscocapsular junction. MRI is more sensitive than either physical examination or arthroscopy in the diagnosis of meniscal cysts. On MRI, these cysts have high signal intensity on T2-weighted images. They indicate a meniscal tear, even if a tear is not seen on imaging.
14. What are the points of attachment for the cruciate ligaments?ACL arises on the medial surface of the lateral femoral condyle at the intercondylar notch and attaches on the anterior portion of the intercondylar eminence of the tibia. PCL arises from the lateral surface of the medial femoral condyle within the intercondylar notch and attaches at the posterior surface of the intercondylar eminence.
15. Which is more commonly injured, ACL or PCL?ACL is much more commonly injured than PCL.
16. What is the MRI appearance of a torn ACL?Direct MRI signs of ACL tear include the following:
• Visible disruption of the ligament• Irregular or wavy contour• Focal signal abnormality within the ligamentous
substance• “Empty notch” sign on coronal images (absence
of ACL in its expected location)• Anterior tibial spine avulsion
Indirect MRI signs of ACL tear include the following:
• Characteristic pivot-shift bone bruise pattern• Deep lateral sulcus sign at the site of impaction
injury at the anterior aspect of the lateral femoral condyle
• Segond fracture• Anterior drawer sign (anterior translation of tibia relative to femur by >5 mm) (Figs. 46-8 and 46-9)
17. What are the sensitivity and specificity of MRI for the detection of complete ACL and PCL tears?MRI has an approximate sensitivity of 94% and a specificity of 94% for complete ACL tears and a sensitivity of 91% and a specificity of 99% for complete PCL tears.
316 MRI of the Knee
Figure 46-6. Medial meniscal tear. Sagittal proton density–weighted image of the lateral aspect of the knee shows linear high signal intensity within the posterior horn of the medial meniscus. This increased signal extends to the inferior articular surface. Its vertical/oblique orientation is most consistent with a traumatic etiology.
Key Points: MRI of the Knee
1. Abnormal signal within a meniscus is insufficient to diagnosintensity must extend to the meniscal surface on two contig
2. Diagnosis of ACL tear should prompt a search for commonlyinjury, medial meniscal tear, Segond fracture, and bone cont
3. Findings of posterolateral corner injury on MRI should be relbecause untreated high-grade injuries have a poor prognosi
18. What are the components of the medial collateral ligament and lateral collateral ligament complex?• The medial collateral ligament comprises
the deep layer, which includes the medial meniscofemoral and meniscotibial ligaments, and the superficial layer (usually understood as the main medial collateral ligament), which is the tibial collateral ligament.
• The lateral collateral ligament complex (anterior to posterior) comprises the iliotibial band, fibular collateral ligament, and biceps femoris tendon.
19. What structures are important stabilizers at the posterolateral corner of the knee, and why are they important?The important posterolateral stabilizers are the lateral collateral ligament complex (iliotibial band, fibular collateral ligament, and biceps femoris tendon), popliteus muscle and tendon, lateral head of gastrocnemius tendon, and other ligaments including the arcuate/fabellofibular and popliteofibular ligaments.
High-grade injury to the posterolateral corner, if left untreated, is associated with a poor outcome. If MRI findings of posterolateral injury are detected, the referring clinician should be informed as soon as possible, and clinical correlation should be undertaken for signs of instability.
e meniscal tear on MRI. Abnormal meniscal signal uous slices to be called meniscal tear on MRI. associated injuries, including medial collateral ligament usions.ayed to the referring clinician as soon as possible s.
20. What is O’Donoghue’s “unhappy triad”?O’Donoghue’s “unhappy triad” is a common football and skiing injury that occurs as a result of valgus stress and twisting motion during weight bearing. Classically, medial collateral ligament injury, ACL tear, and medial meniscal tear result.
21. What is the grading system for medial collateral ligament injury?See Table 46-1. Medial collateral ligament tears without other injury rarely require surgery.
22. List the signs of lateral patellar dislocation.• Reciprocal bone bruising at anterolateral aspect of the lateral femoral condyle and medial aspect of the medial
patellar facet• Patellofemoral cartilage injury• Injury to the medial patellar retinaculum or medial patellofemoral ligament or both• Knee joint effusion
The presence of a shallow patellar notch may predispose patients to this injury (Fig. 46-10).
23. What is jumper’s knee?Jumper’s knee, also known as patellar tendinitis, is an overuse syndrome that classically occurs in young athletes who kick, jump, and run. These actions place stress on the patellofemoral joint with intrasubstance degeneration and partial tearing of
MRI of the Knee 317MusculosKeletal RadIology
LM
Figure 46-7. Discoid lateral meniscus. Coronal T1-weighted sequence through mid–femoral condyle level shows a lateral meniscus that extends centrally beyond the mid-point of the lateral femoral condyle (arrow), representing a discoid lateral meniscus. Note how the normal medial meniscus does not extend beyond the mid-point of the medial femoral condyle. M = medial; L = lateral.
Figure 46-8. Pivot-shift bone bruise pattern. Sagittal fat-saturated T2-weighted sequence shows bone edema (high signal) at the anterior aspect of the lateral femoral condyle (dashed arrow) and at the posterolateral tibial plateau (solid arrow) indicating reciprocal bone bruise at the site of pivot-shift mechanism of injury during anterior translation of the tibia with respect to the femur. This is one of the most helpful indirect signs of ACL tear.
the tendon. Patellar tendinitis is characterized on MRI by proximal patellar tendon thickening and edema (increased signal on fluid-sensitive sequences). In more severe cases, there is concomitant edema in Hoffa fat and at the inferior pole of patella.
24. What is meant by the term osteochondral lesion?An osteochondral lesion describes an articular surface defect involving separation of the cartilage and a portion of the underlying bone from the remainder of the bone. It encompasses etiologies that may overlap, including traumatic osteochondral fractures, osteochondral lesions associated with insufficiency fractures, and osteochondritis dissecans (OCD).
25. What is OCD?OCD refers to a chronic separation of subchondral bone and overlying cartilage, which may have been initially precipitated by trauma. OCD most commonly occurs in individuals 10 to 20 years old, particularly in males, and has a predilection for the lateral aspect of the medial femoral condyle.
26. Why is OCD graded?The management of OCD is contingent on determining fragment stability, with most unstable lesions requiring operative management.
27. How is OCD graded?MRI signs of an unstable fragment in an adult include one or more of the following findings on fluid-sensitive sequences (T2 or short-tau inversion recovery [STIR]):
• Presence of surrounding high T2 signal intensity rim
• Cysts surrounding an OCD lesion• High T2 signal intensity fracture line extending
through the articular cartilage overlying an OCD lesion
• Fluid-filled osteochondral defect
In juvenile OCD, signs of instability require stricter criteria.
28. Describe the MRI appearances of subchondral insufficiency fracture of the knee.Spontaneous osteonecrosis of the knee is now considered a subchondral insufficiency fracture. It usually manifests in adults in the sixth or seventh decade as acute onset of pain without inciting trauma and often involves the medial femoral condyle. In the early stages, MRI shows subchondral edema on fluid-sensitive sequences, which may progress to articular surface flattening and subchondral osteonecrosis (low signal). In the later stages of the condition, bone marrow edema decreases as cartilage loss and other changes of osteoarthritis develop.
318 MRI of the Knee
Table 46-1. Grading System for Medial Collateral Ligament Injury
Grade I (sprain) Edema around intact ligament
Grade II (partial tear) Edema within ligament with or without fiber disruption not involving entire medial collateral ligament at a given level
Grade III (complete tear) Complete disruption of ligament
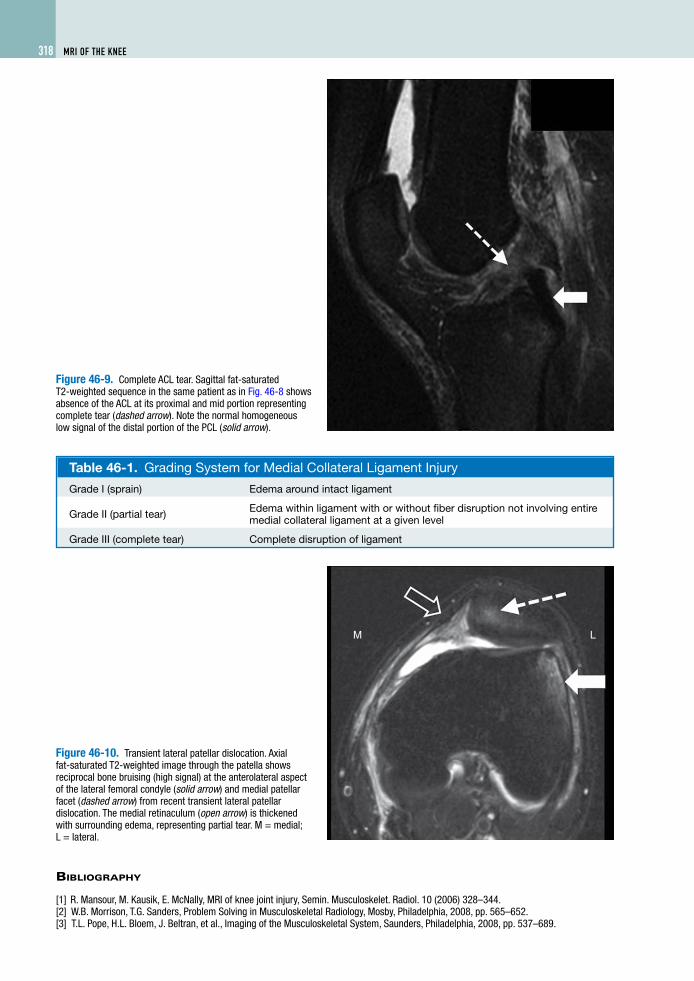
Figure 46-9. Complete ACL tear. Sagittal fat-saturated T2-weighted sequence in the same patient as in Fig. 46-8 shows absence of the ACL at its proximal and mid portion representing complete tear (dashed arrow). Note the normal homogeneous low signal of the distal portion of the PCL (solid arrow).
LM
Figure 46-10. Transient lateral patellar dislocation. Axial fat-saturated T2-weighted image through the patella shows reciprocal bone bruising (high signal) at the anterolateral aspect of the lateral femoral condyle (solid arrow) and medial patellar facet (dashed arrow) from recent transient lateral patellar dislocation. The medial retinaculum (open arrow) is thickened with surrounding edema, representing partial tear. M = medial; L = lateral.
BiBliography
[1] R. Mansour, M. Kausik, E. McNally, MRI of knee joint injury, Semin. Musculoskelet. Radiol. 10 (2006) 328–344. [2] W.B. Morrison, T.G. Sanders, Problem Solving in Musculoskeletal Radiology, Mosby, Philadelphia, 2008, pp. 565–652.[3] T.L. Pope, H.L. Bloem, J. Beltran, et al., Imaging of the Musculoskeletal System, Saunders, Philadelphia, 2008, pp. 537–689.





























