Embed Size (px)
Citation preview

Chap
ter
517
73Keith A. Ferguson, MD, andSusan Hilton, MD
AbdominAl UltrAsoUnd
1. What anatomic landmarks can be used to determine in which hepatic segment an abnormality is located?The hepatic veins can be useful in placing an abnormality within a segment (Fig. 73-1).
• The right hepatic vein separates the anterior and posterior segments of the right hepatic lobe.• The middle hepatic vein separates the anterior segment of the right hepatic lobe from the medial segment of the left
hepatic lobe.• The left hepatic vein separates the medial and lateral segments of the left hepatic lobe.• Similar to the middle hepatic vein, the gallbladder separates the anterior segment of the right lobe and the medial
segment of the left lobe.• The ligamentum teres separates the medial and lateral segments of the left hepatic lobe.
2. What is the normal echogenicity of the liver?The liver should normally be equal to or slightly more echogenic than the right kidney and less echogenic than the pancreas.
3. Can one differentiate between hepatic and portal veins on ultrasound (US)?Yes. Because the portal veins travel with hepatic arteries and biliary radicles and are surrounded by periportal fibrofatty tissue, there is a rim of increased echogenicity surrounding the portal veins. The hepatic veins have no such echogenic rim.
4. Name the common benign and malignant focal hepatic lesions.See Table 73-1.
5. What is the significance of a target lesion?Features that characterize a target lesion are an echogenic center with a hypoechoic peripheral rim. This appearance is important because it is relatively specific for malignancy, more commonly metastatic disease and less commonly hepatocellular carcinoma. Hepatic adenomas can also have this appearance, but are relatively rare.
6. What are the possible growth patterns of hepatocellular carcinoma; when should one highly consider the diagnosis?Hepatocellular carcinoma may be solitary, multifocal, or infiltrative. Although US features are generally nonspecific, invasion of the hepatic or portal veins is a feature commonly associated with hepatocellular carcinoma. True invasion can be differentiated from bland (non-neoplastic) thrombus by detecting arterial flow within the thrombus using Doppler imaging or by showing enhancement of the thrombus on computed tomography (CT) or magnetic resonance imaging (MRI). Additionally, hepatocellular carcinoma occurs almost exclusively in patients with cirrhosis, so the presence of a mass in a cirrhotic liver should be considered hepatocellular carcinoma until proven otherwise.
RRP
RA M LLL
LM
Figure 73-1. Transverse US image of the liver shows hepatic venous and segmental anatomy. The right hepatic vein (R ) separates the right hepatic lobe into anterior (RA) and posterior (RP ) segments. The middle hepatic vein (M ) separates the anterior segment of the right hepatic lobe from the medial segment of the left hepatic lobe (LM ), and the left hepatic vein (L) separates the left lobe into medial (LM ) and lateral (LL) segments.
518 AbdominAl UltrAsoUnd
Table 73-1. Characteristics of Common Focal Hepatic Lesions
LESION US APPEARANCE ADDITIONAL INFORMATION
Cysts
Anechoic lumen, imperceptible wall, increased through-transmission, well-defined posterior wall; may contain septations
These characteristics apply to cysts in other organs as well (see Fig. 73-11 for an example of a renal cyst)
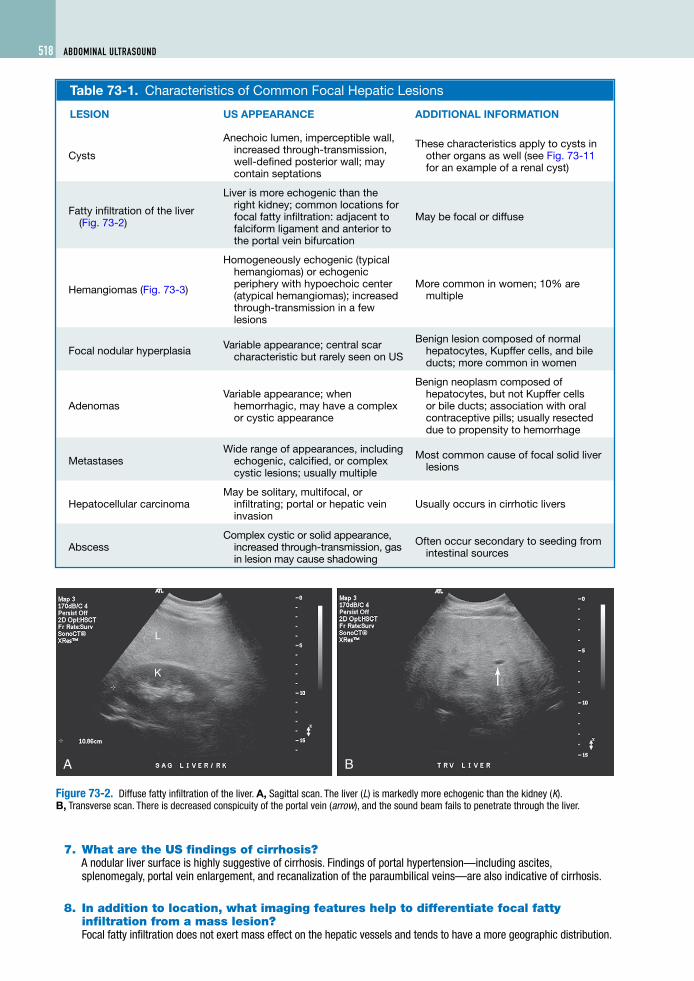
Fatty infiltration of the liver (Fig. 73-2)
Liver is more echogenic than the right kidney; common locations for focal fatty infiltration: adjacent to falciform ligament and anterior to the portal vein bifurcation
May be focal or diffuse
Hemangiomas (Fig. 73-3)
Homogeneously echogenic (typical hemangiomas) or echogenic periphery with hypoechoic center (atypical hemangiomas); increased through-transmission in a few lesions
More common in women; 10% are multiple
Focal nodular hyperplasia Variable appearance; central scar characteristic but rarely seen on US
Benign lesion composed of normal hepatocytes, Kupffer cells, and bile ducts; more common in women
AdenomasVariable appearance; when
hemorrhagic, may have a complex or cystic appearance
Benign neoplasm composed of hepatocytes, but not Kupffer cells or bile ducts; association with oral contraceptive pills; usually resected due to propensity to hemorrhage
MetastasesWide range of appearances, including
echogenic, calcified, or complex cystic lesions; usually multiple
Most common cause of focal solid liver lesions
Hepatocellular carcinomaMay be solitary, multifocal, or
infiltrating; portal or hepatic vein invasion
Usually occurs in cirrhotic livers
AbscessComplex cystic or solid appearance,
increased through-transmission, gas in lesion may cause shadowing
Often occur secondary to seeding from intestinal sources
7. What are the US findings of cirrhosis?A nodular liver surface is highly suggestive of cirrhosis. Findings of portal hypertension—including ascites, splenomegaly, portal vein enlargement, and recanalization of the paraumbilical veins—are also indicative of cirrhosis.
8. In addition to location, what imaging features help to differentiate focal fatty infiltration from a mass lesion?Focal fatty infiltration does not exert mass effect on the hepatic vessels and tends to have a more geographic distribution.
K
L
A B
Figure 73-2. Diffuse fatty infiltration of the liver. A, Sagittal scan. The liver (L) is markedly more echogenic than the kidney (K). B, Transverse scan. There is decreased conspicuity of the portal vein (arrow), and the sound beam fails to penetrate through the liver.

AbdominAl UltrAsoUnd 519UltrAsonogrAphy
9. Describe the US appearance of gallstones.A gallstone has a curvilinear, hyperechoic (bright) leading edge with posterior acoustic shadowing (Fig. 73-4). The posterior shadowing is caused by absorption of the sound beam by the gallstones and should be seen with stones bigger than 3 mm. Gallstones are also typically mobile, although they may occasionally adhere to the gallbladder wall.
10. What is meant by the “WES” sign?The “wall-echo-shadow (WES)” sign may be seen when the gallbladder is completely filled with stones (Fig. 73-5). This sign consists of two curvilinear structures followed by a shadow. The first line is hypoechoic and represents the gallbladder wall. The second is echogenic, representing multiple gallstones, with their associated shadowing making up the third portion of the sign. The “WES” sign may be difficult to differentiate from a gas-filled bowel loop.
11. How does the US appearance of gallstones differ from that of other intraluminal abnormalities?Similar to gallstones, tumefactive sludge (sludge balls) is typically mobile, but does not shadow. Gallbladder polyps are nonmobile and do not shadow.
12. What is the normal gallbladder wall thickness, and what diseases can produce gallbladder wall thickening?The normal thickness of the gallbladder wall is 3 mm or less. Gallbladder wall thickening may be seen in numerous disease processes of biliary and nonbiliary origin. Biliary causes of gallbladder wall thickening include acute or chronic cholecystitis, adenomyomatosis, acquired immunodeficiency syndrome (AIDS) cholangiopathy, sclerosing cholangitis, and gallbladder carcinoma. Nonbiliary causes include hepatitis, cirrhosis, portal hypertension, hypoproteinemia, and heart failure.
13. Describe the US signs of early or uncomplicated acute cholecystitis.Findings on US in early or uncomplicated acute cholecystitis may include gallstones (which may be impacted in the gallbladder neck or cystic duct), gallbladder wall thickening, and gallbladder distention. A sonographic Murphy sign (focal tenderness over the gallbladder when compressed by the US transducer) may also be elicited. The combination of gallstones and Murphy sign has a positive predictive value of 92% and a negative predictive value of 95% for acute cholecystitis.
14. What are additional findings in advanced or complicated cholecystitis?Signs of advanced acute cholecystitis include pericholecystic fluid, a striated appearance of the thickened gallbladder wall, and intraluminal
Figure 73-4. Gallstones on sagittal scan. Characteristics of gallstones include a curvilinear, echogenic leading edge and posterior acoustic shadowing.
Figure 73-3. Hepatic hemangioma. Sagittal scan shows well-circumscribed echogenic lesion (arrow) seen in the left lobe of the liver, typical for hemangioma.
Figure 73-5. WES complex consists of a hypoechoic line (arrow), which represents the gallbladder wall, followed by an echogenic line (asterisk), which represents the leading edge of the gallstones, and posterior shadowing (arrowheads).

520 AbdominAl UltrAsoUnd
membranes caused by sloughed gallbladder mucosa (Fig. 73-6). Emphysematous cholecystitis is most commonly seen in elderly patients with diabetes, in whom the gallbladder becomes infected by gas-producing organisms. The presence of gas in the gallbladder wall or lumen results in bright reflections along the nondependent portion of the gallbladder wall, with “dirty” posterior shadowing.
15. Describe the US appearances of gallbladder carcinoma, and tell which is the most common.Most commonly, gallbladder carcinoma appears as a soft tissue mass centered in the gallbladder fossa, completely or partially replacing the gallbladder lumen. In a few cases, gallbladder carcinoma may also appear as asymmetric gallbladder wall thickening or as a polypoid intraluminal mass. In the latter case, the mass is usually larger than 1 cm, which helps to distinguish it from benign cholesterol polyps.
16. What malignancy has the highest propensity to metastasize to the gallbladder?Melanoma has the highest propensity to metastasize to the gallbladder.
17. What is the normal measurement of the common duct?The normal common duct (a term generally used to refer to the common hepatic duct and the common bile duct because these are difficult to distinguish on US) may vary in size based on the patient’s age and cholecystectomy status, and where the measurement is taken. Generally, the normal common duct should measure less than 7 mm in patients younger than 60. In older patients and patients who have had previous cholecystectomy, the common duct should measure less than 10 mm.
18. Name three causes of extrahepatic biliary dilation.• Choledocholithiasis• Biliary stricture• Tumor within or adjacent to the biliary tree
19. Does a normal-appearing pancreas exclude the diagnosis of pancreatitis?No. Although the pancreas may be diffusely or focally enlarged and hypoechoic in patients with pancreatitis, it may also have a normal appearance.
20. Because the pancreas may appear normal in pancreatitis, what is the role of US in patients suspected to have pancreatitis?One major role of US is to evaluate for the presence of stones in the biliary tree as the cause of pancreatitis, which may alter clinical management of a patient with pancreatitis. Additionally, US can evaluate for complications of pancreatitis, such as peripancreatic fluid collections and pseudocysts, thrombosis of the splenic or superior mesenteric vein, and pseudoaneurysm formation.
21. What is the differential diagnosis of a hypoechoic pancreatic mass lesion?The top two considerations of a hypoechoic pancreatic mass lesion are pancreatic adenocarcinoma and focal pancreatitis (Fig. 73-7). A helpful finding in differentiating these entities is the presence of vascular encasement or metastases, which would support the diagnosis of adenocarcinoma. Pancreatic ductal dilation may be seen in either
A
g
K
L
B
Figure 73-6. Cholecystitis. A and B, Sagittal (A) and transverse (B) scans. Gallbladder wall is thickened and striated (arrows). Two gallstones (g) are present, one of which (asterisk) is impacted in the gallbladder neck. The liver (L) and right kidney (K ) are also seen.

AbdominAl UltrAsoUnd 521UltrAsonogrAphy
process, although the obstructed pancreatic duct in adenocarcinoma is typically smoothly dilated, whereas the duct in chronic pancreatitis most often has an irregular appearance. Other differential diagnostic considerations include islet cell tumors, pancreatic lymphoma, metastases, and peripancreatic lymph nodes.
22. What are the two major types of cystic pancreatic neoplasm?• Serous pancreatic cystadenoma, also known
as microcystic adenoma, usually manifests as a large pancreatic mass composed of multiple small cysts. A calcified central scar may be present. This lesion is benign, most commonly located within the pancreatic tail and most commonly seen in elderly women.
• Mucinous pancreatic tumors (macrocystic adenomas) either have malignant potential or are frankly malignant. They are typically composed of fewer larger cysts, which may contain internal septations or mural nodules. These are most common in middle-aged women and most often occur in the pancreatic body or tail.
23. What genetic diseases are associated with pancreatic cysts?von Hippel-Lindau disease is an autosomal dominant disease associated with pancreatic cysts and neoplasms; cerebellar, retinal, and spinal cord hemangioblastomas; renal cysts; renal cell carcinoma; and pheochromocytoma. Autosomal dominant polycystic kidney disease may be associated with pancreatic cysts in less than 5% of cases.
24. Describe the normal US appearance of a kidney.Kidneys have a more complex US appearance than the other abdominal organs (Fig. 73-8). The central renal sinus is predominantly composed of fat and appears hyperechoic on US. Occasionally, renal blood vessels or the collecting system may be seen as anechoic tubular structures within the sinus. The renal pyramids are hypoechoic triangular or slightly rounded structures that abut the renal sinus. The renal cortex is slightly more echogenic than the renal pyramids. The renal cortex should be equally or less echogenic than the liver and much less echogenic than the spleen. In normal adults, the kidneys should measure 9 to 13 cm in length.
25. What is the main function of US in the setting of acute renal failure?US is very beneficial in determining whether urinary obstruction is present. Although urinary obstruction is an uncommon cause of acute renal failure (accounting for approximately 5% of cases), early detection and treatment are crucial to prevent permanent damage to the kidneys.
26. What are the US findings of obstruction?The hallmark for the diagnosis of obstruction on US is the detection of hydronephrosis (Fig. 73-9). A dilated renal collecting system appears as multiple anechoic structures conforming to the expected location of the renal calyces, all connecting with a dilated renal pelvis centrally. Patients with other processes, such as prior obstruction, pregnancy, bladder distention, vesicoureteral reflux, and diuresis, can also present with a dilated collecting system. The lack of ureteral jets in the bladder and elevated resistive indices can be helpful in differentiating acute obstruction from these other processes.
L
PM
Figure 73-7. Hypoechoic mass (M ) in the pancreatic tail on transverse scan. The remainder of the pancreas (P ) is normal in appearance. Note the liver (L) anterior to the pancreas and the splenic vein (arrow) posterior to the pancreas. A small portion of the pancreatic duct is seen (arrowhead ).
L
S
C
Figure 73-8. Normal sagittal image of kidney. Note normal renal architecture, which includes echogenic renal sinus (S ), intermediately echogenic renal cortex (C ), and hypoechoic medullary pyramids (arrows). The renal cortex is slightly less echogenic than the liver (L), which is normal.

522 AbdominAl UltrAsoUnd
27. Describe the US appearance of renal calculi.Renal stones appear as hyperechoic foci within the renal sinus. Stones of sufficient size show posterior acoustic shadowing, whereas smaller stones may not. Technical factors, such as transducer frequency, focal zone depth, and beam width, should be optimized to maximize the chance of detecting a shadow. Because the renal sinus is normally echogenic, renal stones are more difficult to detect on US than gallstones, which are surrounded by fluid. The composition of a renal calculus does not affect its US appearance.
28. What is the most common renal mass lesion?US characteristics of simple cysts in the liver, kidney, or elsewhere are described in Table 73-1. Cysts may be present in 50% of people older than 50. Cysts that contain thin internal septations, small peripheral thin calcification, or hemorrhagic or proteinaceous debris are termed minimally complex cysts, and, similar to simple cysts, are benign. The presence of thick septations or more extensive calcification is more suggestive of a cystic renal neoplasm and should be evaluated further with dedicated renal CT or MRI or followed up closely with US to evaluate for growth.
29. Are any diseases associated with renal cysts?Yes. See Table 73-2 and Fig. 73-10.
30. What is the most common solid renal mass?Renal cell carcinoma is the most common solid renal mass.
Table 73-2. Diseases Associated with Renal Cysts
DISEASE CYST CHARACTERISTICSASSOCIATED RENAL ABNORMALITIES
OTHER ORGAN SYSTEM INVOLVEMENT
Autosomal dominant polycystic disease
Multiple cysts of various sizes; hemorrhage into cysts common
Enlarged kidneys, renal failure, hypertension
Liver and pancreatic cysts, cerebral berry aneurysms
Acquired cystic disease
Multiple small cysts; hemorrhage common
Occurs in dialysis patients; kidneys are small and echogenic; increased risk of renal cell carcinoma
von Hippel-Lindau disease
Multiple bilateral renal cysts; risk of neoplasm arising in cyst walls
Multiple bilateral renal cell carcinomas
Cerebellar and spinal cord hemangioblastomas, retinal angiomas, pancreatic cysts and neoplasms, pheochromocytomas
Tuberous sclerosis
Cysts develop most commonly in infancy and childhood
Multiple bilateral angiomyolipomas
Mental retardation, seizures, central nervous system tumors, cardiac rhabdomyomas, pulmonary lymphangiomyomatosis
L
K
A B
Figure 73-9. Hydronephrosis. A and B, Sagittal images of right kidney (K ) show moderately dilated collecting structures. The liver (L) is also seen.

AbdominAl UltrAsoUnd 523UltrAsonogrAphy
31. Describe the imaging features of renal cell carcinoma.Most renal cell carcinomas are slightly hyperechoic or isoechoic to the renal parenchyma. Approximately 10% are hypoechoic, and another 10% are much more echogenic than the normal kidney. They may contain areas of calcification, necrosis, or hemorrhage. Predominantly cystic renal cell carcinomas also occur, but are uncommon. Renal cell carcinoma has a propensity to invade the renal veins and inferior vena cava, and these should be evaluated in patients with a solid renal mass. Other benign and malignant neoplasms may involve the kidney and produce a solid mass.
32. Discuss the differential diagnosis for a markedly echogenic renal mass.Angiomyolipomas are usually well-defined, markedly hyperechoic renal masses. These benign lesions consist of varying degrees of fat, vessels, and muscle; the presence of fat accounts for the hyperechoic appearance. As previously noted, a few renal cell carcinomas may also be much more echogenic, however, than the renal parenchyma. Malignancy must also be considered in the differential diagnosis for a hyperechoic renal mass. The presence of posterior acoustic shadowing without calcification is more suggestive of angiomyolipoma, whereas areas of calcification or cystic regions suggest renal cell carcinoma. Nevertheless, CT or MRI is usually indicated to characterize these lesions further.
33. Does pyelonephritis have a characteristic appearance on US?Most patients with pyelonephritis have normal-appearing kidneys on US. In more severe cases, there may be focal areas of masslike enlargement or heterogeneous echotexture of the kidneys. The most important role of US in pyelonephritis is in excluding complications, however, such as renal or perinephric abscess or urinary obstruction.
34. What is meant by renal parenchymal disease?Renal parenchymal disease, or medical renal disease, is a term used to describe kidneys of increased cortical echogenicity (Fig. 73-11). Kidneys that are more echogenic than the liver or equal to or greater in echogenicity than the spleen are too echogenic. Numerous disease processes result in this same US appearance, and biopsy may be necessary to differentiate among them when clinically appropriate. Renal size is helpful to differentiate acute from chronic renal disease.
Figure 73-10. Autosomal dominant polycystic kidney disease. Sagittal scan of right kidney. Normal renal parenchyma is replaced by cysts of varying sizes.
Key Points: Diagnoses to Consider for a Solid Renal Mass
1. Renal carcinoma is the most common cause.2. Angiomyolipoma is usually hyperechoic, but some carcinomas mimic angiomyolipoma on US.3. Other neoplasms include oncocytoma, renal lymphoma, transitional cell carcinoma of the renal collecting system,
and metastasis to the kidney.
A B
Figure 73-11. Renal parenchymal disease. A and B, Sagittal (A) and transverse (B) images show right kidney to be much more echogenic than the liver. Also note the upper pole renal cyst, with its typical features of an anechoic lumen, well-defined posterior wall, and increased through-transmission (arrows).

524 AbdominAl UltrAsoUnd
BiBliography
[1] G.L. Bennett, E.J. Balthazar, Ultrasound and CT evaluation of emergent gallbladder pathology, Radiol. Clin. North. Am. 41 (2003) 1203–1216.
[2] A. Kurtz, W. Middleton, Ultrasound: The Requisites, Mosby, St. Louis, 1996.[3] C.M. Rumack, C.R. Wilson, J.W. Charboneau (Eds.), Diagnostic Ultrasound, second ed., Mosby, St. Louis, 1998.














![S2 EPISODE 06 [0:00:08.4] AS - Ali Shapiro · 2018. 1. 31. · IP S206 Transcript S2 EPISODE 06 [INTRO] [0:00:08.4] AS: When you’re fed up with fighting food and your body, join](https://img.pdfslide.us/doc/110x75/609fac78135d3d1a8c605f2c/s2-episode-06-000084-as-ali-shapiro-2018-1-31-ip-s206-transcript-s2.jpg)