Embed Size (px)
Citation preview

CHAPTER 25
ACID-BASE HOMEOSTASIS AND IMBALANCES

INTRODUCTION
• Understanding normal mechanisms of acid-base homeostasis contributes to understanding of acid-base imbalances
• pH of a fluid reflects its degree of acidity or alkalinity
• Cellular function is impaired when the pH of body fluids becomes abnormal

PH
• Normal pH of adult blood ranges from 7.25 to 7.45
• Range is somewhat wider in infants and children
• If blood or other body fluids become too acidic or too alkalytic, dysfunction and even death can occur
• Maintenance of acid-base balance reflects homeostatic functions of normal cellular metabolism

TABLE 25-1
Normal Laboratory Values for Acid-Base Parameters
CharacteristicCharacteristic Normal RangeNormal Range
PaCOPaCO22 (arterial blood) (arterial blood) 36-44 mm Hg (adults)36-44 mm Hg (adults)30-34 mm Hg (infants)30-34 mm Hg (infants)
HCOHCO33-- (serum) (serum) 22-26 mEq/L (adults)22-26 mEq/L (adults)
19-23 mEq/L (infants)19-23 mEq/L (infants)
PH (arterial blood)PH (arterial blood) 7.35-7.45 (adults)7.35-7.45 (adults)7.11-7.36 (neonates)7.11-7.36 (neonates)7.36-7.41 (infants)7.36-7.41 (infants)

ACID-BASE HOMEOSTASIS
• Three major mechanisms regulate acid-base status of body• Buffers• Respiratory system• Renal system

ACID-BASE HOMEOSTASIS (CONT.)
• Arterial blood gas (ABG) measures are useful indicators of acid-base status of extracellular fluids• PaCO2: respiratory function• HCO3: renal (metabolic) function• pH indicates:
• Net result of expected acid-base regulation• Any dysfunction of pH regulation• Body’s compensatory responses

BUFFERS
• First line of defense against pH changes in body fluids
• Chemicals that help control pH of body fluids• Contained in all body fluids• Consist of weak acids that take up hydrogen
ions when a fluid is too acidic• Types
• Bicarbonate buffers• Phosphate buffers• Hemoglobin buffers• Protein buffers

BICARBONATE BUFFER SYSTEM
• Primary defense against acid-base disorders• Most important buffer in extracellular fluid
(ECF)• Components
• Bicarbonate ions (HCO3-)
• Carbonic acid (H2CO3)• Maintained in chemical equilibrium in ECF

FUNCTION OF BICARBONATE BUFFERS
• If too much acid (e.g., lactic acid) is present, bicarbonate ions take up hydrogen ions (H+) releasedby the acid and become carbonic acid
• If too little acid present in ECF, bicarbonate buffer releases hydrogen ions to increase pH

RESPIRATORY CONTRIBUTION
• Second defense against acid-base disorders• Lungs excrete CO2 and water from body• Changes in rate and depth of respiration
• Result from stimulation of chemoreceptors that sense PaCO2 and pH of blood
• Exert an influence on and serve to alter amount of PaCO2 in blood

RESPIRATORY RESPONSE
• Excessive carbonic acid accumulation• Increases rate and depth of respiration• Excess carbonic acid removed
• Insufficient carbonic acid• Respiratory rate and depth decrease• Allows for temporary accumulation of carbonic
acid• Hyperventilation results in:
• Decrease in carbonic acid accumulation in blood

RESPIRATORY RESPONSES TO CHANGES IN CARBONIC AND
METABOLIC ACIDSStimulusStimulus Respiratory ResponseRespiratory Response ResultResult
Increased PaCOIncreased PaCO22, , decreased pHdecreased pH
HyperventilationHyperventilation Correction of imbalanceCorrection of imbalance
Decreased PaCODecreased PaCO22, , increased pHincreased pH
HypoventilationHypoventilation Correction of imbalanceCorrection of imbalance
Decreased pH from Decreased pH from excess metabolic acidsexcess metabolic acids
HyperventilationHyperventilation Compensation for Compensation for imbalanceimbalance
Increased pH from Increased pH from deficit of metabolic acidsdeficit of metabolic acids
HypoventilationHypoventilation Compensation for Compensation for imbalanceimbalance

RENAL CONTRIBUTION
• Kidneys• Third defense against acid-base disorders• Can excrete any acid from the body except
carbonicacid (solely excreted by the lungs)
• Excrete metabolic acids produced continuously during normal metabolism
• Body’s ability to correct an excess or deficit of a metabolic acid depends on normal function of renal system
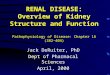
• See Figure 25-1 for review of renal physiology

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
RENAL PHYSIOLOGY

RENAL ACID EXCRETION
• Increased if a metabolic acid begins to accumulate in blood
• Slowed if a metabolic acid is deficient in blood

MECHANISMS OF RENAL ACID EXCRETION
• Increase production of ammonia (NH3) • Compensate for carbonic acid imbalances
by increasing or decreasing the excretion of metabolic acids• Renal compensatory response to an imbalance of
carbonic acid requires several days to be fully operative

RENAL RESPONSES TO CHANGES IN METABOLIC AND CARBONIC
ACIDSStimulusStimulus Renal ResponseRenal Response ResultResult
Decreased pH from Decreased pH from excess of metabolic excess of metabolic acidsacids
Secrete more HSecrete more H++
Make more ammoniaMake more ammoniaCorrection of Correction of imbalanceimbalance
Increased pH from Increased pH from deficit of metabolic deficit of metabolic acidsacids
Secrete fewer HSecrete fewer H++
Make less ammoniaMake less ammoniaExcrete HCOExcrete HCO33
--
Correction of Correction of imbalanceimbalance
Decreased pH from Decreased pH from excess of carbonic excess of carbonic acidsacids
Secrete more HSecrete more H++
Make more ammoniaMake more ammonia
Compensation for Compensation for imbalanceimbalance
Increased pH from Increased pH from deficit of carbonic acidsdeficit of carbonic acids
Secrete fewer HSecrete fewer H++
Make less ammoniaMake less ammoniaExcrete HCOExcrete HCO33
--
Compensation for Compensation for imbalanceimbalance

ACID-BASE IMBALANCES
Four primary disordersFour primary disorders Metabolic acidosisMetabolic acidosis Respiratory acidosisRespiratory acidosis Metabolic alkalosisMetabolic alkalosis Respiratory alkalosisRespiratory alkalosis Mixed acid-base imbalancesMixed acid-base imbalances
Acidosis is presence of condition that tends to Acidosis is presence of condition that tends to decrease pH of blood making it more acidicdecrease pH of blood making it more acidic
Alkalosis is presence of factor that increases pH Alkalosis is presence of factor that increases pH of blood above normal, making it more alkalineof blood above normal, making it more alkaline

METABOLIC ACIDOSIS
• Relative excess of any acid except carbonic acid
• May be caused by:• Increase in acid• Excess removal or decrease in base• Combination of increase in acid and decrease in
base• Results in decrease of normal 20:1 ratio of
HCO3- to H2CO3

INCREASE IN ACID
• Decreases normal ratio of bicarbonate to carbonic acid because bicarbonate ions are used up in buffering the excess acid
• Example: starvation ketoacidosis• Caloric intake is insufficient• Body begins to use fat stores for energy• Too little glucose ingested• Fat metabolized incompletely• Ketoacids accumulate in blood, causing metabolic
acidosis

EXCESS REMOVAL OF BASE
• Excessive removal of bicarbonate ions from the body
• Example: diarrhea• Loss of intestinal fluid that is rich in bicarbonate ions
that originate from pancreatic secretions

ETIOLOGY OF METABOLIC ACIDOSIS
• Increase in acid• Ketoacidosis (diabetes mellitus, starvation,
alcoholism)• Severe hyperthyroidism• Severe infection• Burns• Circulatory shock• Tissue anoxia• Oliguric renal failure• Intake of acids or acid precursors (e.g., salicylates,
methanol, ethylene glycol)

ETIOLOGY OF METABOLIC ACIDOSIS
• Decrease in base• Diarrhea• Gastrointestinal fistula that drains intestinal or
pancreatic secretions• Intestinal decompression• Renal tubular acidosis

CLINICAL MANIFESTATIONS
• ABGs show below-normal bicarbonate concentration
• pH may be below normal if uncompensated• Headache• Abdominal pain• Central nervous system depression
• Confusion• Lethargy• Stupor• Coma

CLINICAL MANIFESTATIONS (CONT.)
• Ventricular dysrhythmias (from myocardial intracellular acidity)
• Decreased cardiac contractility • Death from brainstem dysfunction usually
occurs if pH falls below 6.9

COMPENSATORY RESPONSE
• Hyperventilation is typical respiratory compensatory response• Low blood pH stimulates peripheral chemoreceptors• Ventilatory neurons respond to increase rate and
depth of respiration• Increased rate and depth of respiration result in
increased excretion by lungs of carbonic acid (CO2 + water)
• Does not remove metabolic acids from body

COMPENSATORY RESPONSE (CONT.)
• Does change ratio of bicarbonate ions to carbonic acid
• Results in compensatory increase in pH

ARTERIAL BLOOD GASES
• In compensated metabolic acidosis, show:• Decreased bicarbonate concentration• Slightly decreased or even normal pH, depending
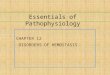
on the degree of compensation• See Figure 25-2 for interpreting laboratory
measures specific to acid-base imbalances

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
LABORATORY MEASURES

ETIOLOGY OF RESPIRATORY ACIDOSIS
• Impaired gas exchange• Chronic obstructive pulmonary disease (COPD)• Pneumonia• Severe asthma• Pulmonary edema• Acute (adult) respiratory distress syndrome• Obstructive sleep apnea

ETIOLOGY OF RESPIRATORY ACIDOSIS (CONT.)
• Impaired neuromuscular function• Guillain-Barré syndrome• Chest injury or surgery (pain limits ventilation)• Hypokalemic respiratory muscle weakness• Severe kyphoscoliosis• Respiratory muscle fatigue
• Impaired respiratory control (brainstem)• Respiratory-depressants (opioids, barbiturates)• Central sleep apnea

CLINICAL MANIFESTATIONS
• Headache• Tachycardia• Cardiac dysrhythmias• Neurologic abnormalities
• Blurred vision• Tremors• Vertigo• Disorientation• Lethargy• Somnolence

COMPENSATORY RESPONSE
• Increased renal excretion of metabolic acid (kidneys cannot excrete carbonic acid; this is solely a respiratory function)
• Requires several days to be effective• Results in increase of bicarbonate ion
movement of pH toward normal

ARTERIAL BLOOD GASES
• Increased PaCO2
• Slightly decreased or even normal pH, depending on degree of compensation

ETIOLOGY OF METABOLIC ALKALOSIS
• Increase in base• Intake of bicarbonate or bicarbonate precursors
(acetate, citrate, lactate)• Massive transfusion with citrated blood• Mild or moderate extracellular fluid volume deficit
• Decrease in acid• Emesis• Gastric suction• Mild or moderate extracellular fluid volume deficit• Hyperaldosteronism• Hypokalemia

CLINICAL MANIFESTATIONS
• Postural hypotension• Hypokalemia may coexist
• Bilateral muscle weakness• Increased neuromuscular excitability
• “Tingly” fingers and toes• Signs of tetany; may progress to seizures

CLINICAL MANIFESTATIONS (CONT.)
• Increased excitability of nerve cell membranes
• Changes in mentation• Belligerence• Confusion• Lethargy
• Death usually occurs if pH rises to 7.8

COMPENSATORY RESPONSE
• Hypoventilation• Usually incomplete
• Need for oxygen drives ventilation and prevents complete compensation

COMPENSATORY RESPONSE ARTERIAL BLOOD GASES
• Increased bicarbonate concentration• Increased PaCO2
• Slightly increased pH

ETIOLOGY OF RESPIRATORY ALKALOSIS
• Hypoxemia• Acute pain• Anxiety, psychological distress• Prolonged sobbing• Alcohol withdrawal• Stimulation of the brainstem (salicylate
overdose, meningitis, head injury, gram-negative sepsis)

CLINICAL MANIFESTATIONS
• Paresthesias (numbness and tingling) of fingers and around mouth• Carpal and/or pedal spasm• Increased central and peripheral membrane
excitability• Increased pH of cerebrospinal and cerebral
interstitial fluid alters brain cell function, can cause confusion• Cerebral vasoconstriction• Increased neuromuscular excitability

COMPENSATORY RESPONSE
• Decreased renal excretion of metabolic acid• Decrease in bicarbonate ion concentration• Renal compensation tends to return the ratio
of bicarbonate ions to carbonic acid, moving pH toward normal• Because this takes several days and because
many causes are short-lived, may not be fully compensated

COMPENSATORY RESPONSE ARTERIAL BLOOD GASES
• Decreased PaCO2
• Decreased bicarbonate concentration• Slightly increased or perhaps normal pH,
depending on degree of compensation

MIXED ACID-BASE IMBALANCES
• If one type of imbalance persists, a compensatory imbalance may arise• Example: a patient with bacterial pneumonia
and related respiratory acidosis also develops severe diarrhea and concurrent metabolic acidosis

PH IN MIXED IMBALANCES
• Two types of primary acidosis or alkalosis may impair effectiveness of usual compensatory mechanisms• pH will reflect primary mechanism (either
acidosis or alkalosis) • Mixed acid-base disorders may also occur
with a nearly normal pH if a primary acidosis and a primary alkalosis are involved

NEONATAL AND INFANT VARIATIONS
• Neonates often have mild metabolic acidosis• Infants younger than 1 month are at risk for
metabolic acidosis when they have a condition that results in acid accumulation• Reduced ability to excrete large acid load• Kidneys less able to reabsorb bicarbonate• Produce less ammonia• Urinary buffers are limited in quantity

ADOLESCENT VARIATIONS
• Teens with eating disorders may develop metabolic alkalosis from repeated emesis or metabolic acidosis from starvation and/or laxative-induced chronic diarrhea

GERIATRIC VARIATIONS
• Delayed ability to correct respiratory acidosis due to age-related decrease in chemoreceptor response to increased PaCO2 (hyperventilation) • Increased risk of respiratory depression (and
thus respiratory acidosis) from barbiturates because of increased drug half-life• Kidneys less able to excrete large acid load,
increasing risk for metabolic acidosis from acid accumulation

GERIATRIC VARIATIONS (CONT.)
• Metabolic acidosis may result from chronic laxative overuse that results in chronic diarrhea