Embed Size (px)
Citation preview

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
CHAPTER 13ALTERATIONS IN OXYGEN
TRANSPORT

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
COMPOSITION OF BLOOD
• Total blood volume• 75.5 ml/kg in men• 66.5 ml/kg in women
• 8% of body weight or 5-6 L• Blood cells make up 45% of blood volume• Plasma 55% of blood volume
• Composed of 92% water, 7% plasma proteins

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
COMPOSITION OF BLOOD (CONT.)
Organic and Inorganic Components• Plasma proteins formed in the liver• Contribute to colloid osmotic pressure• Three general types of plasma proteins
• Serum albumin• Serum globulin• Fibrinogen
• Regulatory proteins (hormones and enzymes); also in plasma

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
COMPOSITION OF BLOOD (CONT.)
Organic and Inorganic Components• Organic constituents
• Products of tissue metabolism• Nutritive organic materials
• Inorganic constituents• Electrolytes• Iron

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
COMPOSITION OF BLOOD (CONT.)
Cellular Components• Erythrocytes• Leukocytes
• Neutrophils• Eosinophils
• Basophils • Lymphocytes• Monocytes
• Platelets

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
COMPOSITION OF BLOOD (CONT.)
Erythrocytes—Red Blood Cells• Most numerous• Transport oxygen to tissues• Remove carbon dioxide from the tissues• Buffer blood pH

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
COMPOSITION OF BLOOD (CONT.)
Leukocytes—White Blood Cells• Act primarily in tissues but circulate in blood and
lymphatic system• Protect the body by phagocytosis of
microorganisms• Form immune antibodies

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
COMPOSITION OF BLOOD (CONT.)
Platelets• Circulating cytoplasmic fragment of
megakaryocytes• Incapable of mitotic division• Form blood clots and control bleeding• Release biochemical mediator involved in the
hemostatic process

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
COMPOSITION OF BLOOD (CONT.)

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
COMPOSITION OF BLOOD (CONT.)

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
STRUCTURE AND FUNCTION OF RED BLOOD CELLS
• Originate in the yolk sac mesenchyme• Move to liver and spleen during fetal life• Limited to marrow of the body skeleton after birth
• Held in a fine reticular meshwork• Free access to plasma nutrients• Retained until maturity allows penetration of the
endothelial barrier

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
STRUCTURE AND FUNCTION OF RED BLOOD CELLS (CONT.)
Hematopoiesis• Developmental process of RBCs leading from
pluripotential stem cells to mature, differentiated red cells
• Lymphopoiesis is the process for lymphocytes

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
STRUCTURE AND FUNCTION OF RED BLOOD CELLS (CONT.)
Hematopoiesis• Two-stage process involving:
• Mitotic division (proliferation)• Maturation (differentiation)
• Continues throughout life and can be accelerated by: • Increase in differentiation of daughter cells• Increase in number of stem cells• Conversion of yellow bone marrow to red marrow

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
STRUCTURE AND FUNCTION OF RED BLOOD CELLS (CONT.)
Hemoglobin Synthesis• Hemoglobin is the oxygen-carrying protein in the
mature red cell• Comprises 90% of a cell’s dry weight• Two pairs of polypeptide chains, the globins, each
with an attached heme molecule composed of iron and protoporphyrin molecule

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
HEMOGLOBIN SYNTHESIS

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
STRUCTURE AND FUNCTION OF RED BLOOD CELLS
Nutritional Requirements for Erythropoiesis• Requires adequate amounts of iron, protein,
vitamins, and minerals• Folate and B12 deficiencies lead to impaired DNA
synthesis in erythroid cells because the vitamins are coenzymes of key reactions in cellular metabolism

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
STRUCTURE AND FUNCTION OF RED BLOOD CELLS (CONT.)
Energy and Maintenance of Erythrocytes• Circulate for 120 days; removed by spleen’s
filtering action and mononuclear phagocyte system
• Anaerobic Embden-Meyerhof pathway provides ATP for regulation of electrolytes via cation pumps
• Aerobic hexose monophosphate shunt protects cell from permanent oxidant injury
• Rapoport-Leubering pathway facilitates oxygen release to tissues

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
STRUCTURE AND FUNCTION OF RED BLOOD CELLS (CONT.)
Red Cell Production• Erythron describes blood as a single body system
composed of blood cells and bone marrow precursors
• Erythropoiesis is regulated by the concentration of hemoglobin in blood
• In response to decreased hemoglobin the kidney secretes erythropoietin

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
STRUCTURE AND FUNCTION OF RED BLOOD CELLS (CONT.)
Red Cell Destruction• Methemoglobin is removed by mononuclear
phagocytic system• Globin is broken down into amino acids and the
iron is recycled• Porphyrin is reduced to bilirubin• Conjugated bilirubin is excreted in the bile as
glucuronide

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
RED CELL DESTRUCTION

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
GAS TRANSPORT AND ACID-BASE BALANCE
• Oxygen combines with heme portion to form oxyhemoglobin
• Carbonic anhydrase in the RBC help to form carbonic acid
• 90% of CO2 in arterial blood and 60% in venous blood transported as bicarbonate
• Hemoglobin binds with CO2 to form carbaminohemoglobin

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
GAS TRANSPORT AND ACID-BASE BALANCE (CONT.)
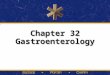
Oxygen Transport• Each hemoglobin molecule can bind 4 atoms of
oxygen• Average person has about 15 g of hemoglobin per
100 ml of blood• Partial pressure of oxygen reflects the pressure or
tension that oxygen exerts when it is dissolved in blood

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
OXYGEN TRANSPORT

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
OXYGEN-HEMOGLOBIN DISSOCIATION CURVE

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
GAS TRANSPORT AND ACID-BASE BALANCE
Carbon Dioxide Transport• Transported in the blood by:
• Dissolved gas• Bicarbonate ion• Bound to hemoglobin
• Partial pressure of carbon dioxide reflects the pressure or tension it exerts when dissolved in blood

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
CARBON DIOXIDE TRANSPORT

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
GAS TRANSPORT AND ACID-BASE BALANCE
Alterations in Oxygen Transport• Decreased oxygen reaching the tissues results in
secretion of erythropoietin and increase in the production of RBCs
• Factors that decrease hemoglobin mass (anemia) or decrease arterial saturation (hypoxia) lead to increased release of erythropoietin

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
ALTERATIONS IN OXYGEN TRANSPORT

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
ANEMIA
• Anemia is a deficit of red cells• Low oxygen-carrying capacity leads to hypoxia
• Polycythemia is an excess of red cells• Increased blood viscosity and volume
• Relative anemia—normal total red cell mass with disturbances in regulation of plasma volume
• Absolute anemia—actual decrease in numbers of red cells

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
GENERAL EFFECTS OF ANEMIA
• Reduction in oxygen-carrying capacity• Tissue hypoxia
• Compensatory mechanism to restore tissue oxygenation• Increased heart rate, cardiac output, circulatory rate, and
flow to vital organs• Increase in 2,3-DPG in erythrocytes and decreased
oxygen affinity of hemoglobin in tissues

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
MANIFESTATIONS OF ANEMIA
• Mild anemia (hemoglobin above 8g/dl• Minimal symptoms• Elderly with CV, pulmonary disease may have symptoms

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
MANIFESTATIONS OF ANEMIA (CONT.)
• Moderate/severe anemia (hemoglobin below 8g/dl• Orthostatic hypotension/nonorthostatic• Pallor• Tachypnea• HA/lightheaded, fainting• Angina, heart failure• Nighttime leg cramps• Tinnitus or roaring in ears• Fatigue, weakness

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
ANEMIA RELATED TO DECREASED RED CELL PRODUCTION
Aplastic Anemia• Stem cell disorder characterized by reduction of
hematopoietic tissue in the bone marrow, fatty marrow replacement and pancytopenia
• Caused by toxic, radiant, or immunologic injury to the bone marrow stem cells

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
ANEMIA RELATED TO DECREASED RED CELL PRODUCTION (CONT.)
Aplastic Anemia• Insidious onset of symptoms• Late symptoms include weakness, fatigue,
lethargy, pallor, dyspnea, palpitations, transient murmurs and tachycardia
• Pancytopenia and granulocytopenia

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
ANEMIA RELATED TO DECREASED RED CELL PRODUCTION (CONT.)
Aplastic Anemia• Treatment
• Identify and avoid of further toxic exposure• Type human leukocyte antigen (HLA) and ABO to
identify serologically defined loci and potential donors• Maintain minimally essential levels of hemoglobin and
platelets• Prevent and manage infection• Determine efficacy of bone marrow transplantation• Administer immunosuppressive therapy or stimulate
hematopoiesis and bone marrow regeneration

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
ANEMIA RELATED TO DECREASED RED CELL PRODUCTION (CONT.)
Anemia of Chronic Renal Failure• Failure of the renal endocrine function impairs
erythropoietin production and bone marrow compensation
• Decreased RBC count with low HCT and HGB level• Treatment consists of dialysis and administration
of erythropoietin

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
ANEMIA RELATED TO DECREASED RED CELL PRODUCTION (CONT.)
Anemia Related to Vitamin B12 (Cobalamin) or Folate Deficiency• Disruption in DNA synthesis of blast cells in bone
marrow produces megaloblasts• Pernicious anemia due to lack of intrinsic factor
leading to vitamin B12 deficiency• Low RBC, WBC, and platelet counts with
increased MCV; megaloblastic dysplasia• Treatment: replacing nutritional deficiencies

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
ANEMIA RELATED TO DECREASED RED CELL PRODUCTION (CONT.)
Iron Deficiency Anemia• Most common nutritional deficiency in the world• Insufficient iron for hemoglobin synthesis• Hypochromic, microcytic RBCs; low MCV, MCH,
and MCHC• Treatment: oral administration of ferrous sulfate
or intravenous ferric gluconate

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
ANEMIA RELATED TO INHERITED DISORDERS OF THE RED CELL
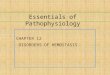
Thalassemia• Increased RBC destruction (hemolysis) resulting
in decreased RBC survival rates• Group of disorders associated with the presence
of mutant genes that suppress the rate of synthesis of globin chains
• Classified by the polypeptide chain(s) with deficient synthesis

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
BETA-THALASSEMIA

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
ANEMIA RELATED TO INHERITED DISORDERS OF THE RED CELL
Thalassemia• Hypochromic, microcytic RBCs, MCV, MCH, and
MCHC are low, erythroblastic hyperplasia• Treatment
• Blood transfusions• Splenectomy• Chelation therapy• Bone marrow transplantation

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
ANEMIA RELATED TO INHERITED DISORDERS OF THE RED CELL
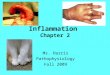
(CONT.)Sickle Cell Anemia• Genetically determined defect of hemoglobin
synthesis resulting in hemoglobin instability and insolubility
• Sickled cells cause vascular occlusion• Severe anemia, RBCs of different shapes and
sizes• Treatment of choice is stem cell transplant

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
SICKLE CELL ANEMIA

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
ANEMIA RELATED TO INHERITED DISORDERS OF THE RED CELL
Hereditary Spherocytosis• Defective red cell membrane skeleton, altered
membrane properties, and altered cell metabolism
• Autosomal dominant trait• RBCs are fragile microspherocytes, with increased
destruction of spherocytes• Treatment consists of splenectomy

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
ANEMIA RELATED TO INHERITED DISORDERS OF THE RED CELL
(CONT.)Glucose-6-Phosphate Dehydrogenase Deficiency• Genetic disorder resulting in RBC membrane
destruction• Do not have hemolytic anemia unless challenged
by drugs• Treatment is preventive by avoidance of drugs
that trigger hemolytic episodes and aggressive infection management

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
ANEMIA RELATED TO EXTRINSIC RED CELL DESTRUCTION OR LOSSHemolytic Disease of the Newborn• Fetal RBCs cross placenta, stimulate production
of maternal antibodies against antigen on fetal RBC not inherited by mother
• Maternal antibodies cross into the fetal circulation causing destruction of fetal cells• ABO incompatibility most common• Rh incompatibility more clinically relevant

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
ANEMIA RELATED TO EXTRINSIC RED CELL DESTRUCTION OR LOSS
(CONT.)Hemolytic Disease of the Newborn• Anemia, reticulocytosis, and nucleated RBCs in
blood of infant• Standard dose of anti-Rh immune globulin
(RhoGAM) is given to the mother before or after delivery
• In severe cases, in utero blood transfusion and early delivery

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
ANEMIA RELATED TO EXTRINSIC RED CELL DESTRUCTION OR LOSS
(CONT.)Antibody-Mediated Drug Reactions• Exposure to a drug causes destruction and lysis
of the sensitized person’s own RBCs• Mechanisms include:
• Hapten mechanisms• Neoantigen formation• Membrane modification• Autoantibody Induction
• Recognize and discontinue offending medications

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
ANEMIA RELATED TO EXTRINSIC RED CELL DESTRUCTION OR LOSS
(CONT.)Acute Blood Loss• May be from trauma or secondary to a disease
process• Symptoms develop with activity at 20% loss of
blood volume (tachycardia and postural drop in BP), and increase in severity with continued blood loss
• Blood volume replacement therapy with crystalloids, colloids, and fresh whole blood

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
ANEMIA RELATED TO EXTRINSIC RED CELL DESTRUCTION OR LOSS
(CONT.)Other Extrinsic Abnormalities• Mechanical heart valves and cardiopulmonary
bypass machines can result in hemolysis• Drugs and chemicals, physical agents, and
infectious diseases can cause anemia• Venom from insects and snakes can cause
hemolytic anemia• Hypersplenism and splenomegaly can result in
anemia, leukopenia, or thrombocytopenia

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
TRANSFUSION THERAPY
• Medical indications include:• Restoration or maintenance of oxygen-carrying capacity,
blood volume, hemostasis and leukocyte function• Donor testing to ensure safety of blood products• Specific pretransfusion testing to ensure blood
component will not harm recipient

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
POLYCYTHEMIA
• Excess RBCs resulting in increased blood viscosity, leading to clinical symptoms such as hypertension
• Types of polycythemia are categorized by cause

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
POLYCYTHEMIA (CONT.)
Polycythemia Vera• Neoplastic transformation of bone marrow stem
cells• Absolute increase in RBC mass and leukocytosis,
and thrombocytopenia; increased uric acid due to excess proliferation
• Treatment directed at reducing increased blood volume, viscosity, RBC mass and platelet count with phlebotomy, radioactive phosphorus, and chemotherapeutic agents

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
POLYCYTHEMIA (CONT.)
Secondary Polycythemia• Due to chronic hypoxemia with resultant increase
in erythropoietin production• Increased RBC production without increase in
WBCs or platelets• Identifying and managing underlying cause of
hypoxemia; phlebotomy may be used to decrease cardiovascular workload

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
POLYCYTHEMIA (CONT.)
Relative Polycythemia• Due to dehydration with spurious increase in RBC
production• Elevated hematocrit, hemoglobin, and RBC count• Recognize and manage underlying cause; fluid
administration is used with management of long-term conditions