Embed Size (px)
Citation preview

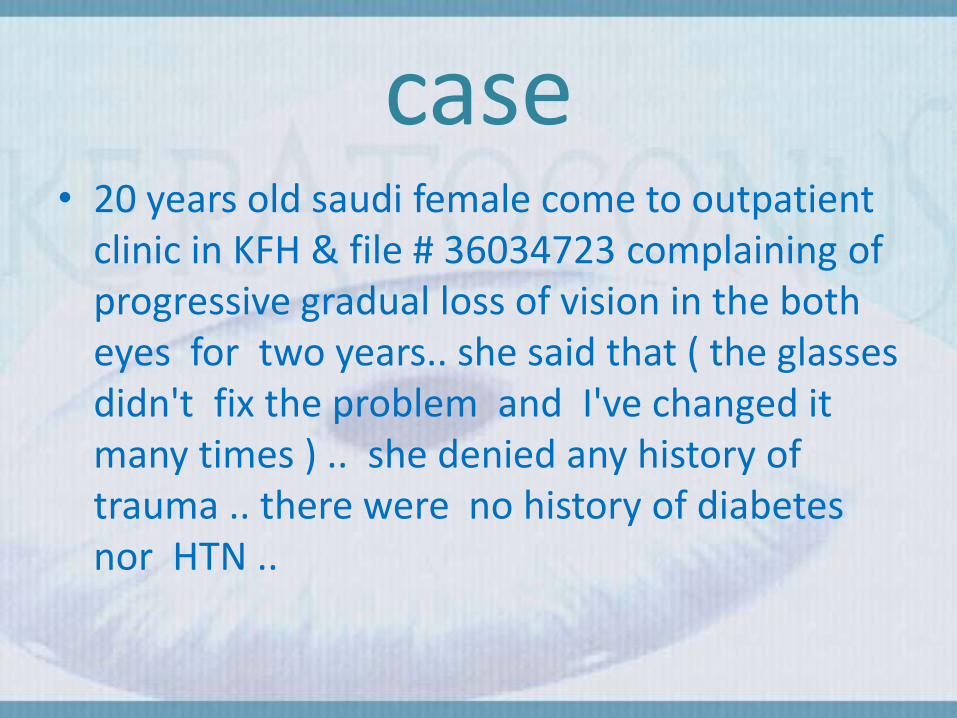
case• 20 years old saudi female come to outpatient
clinic in KFH & file # 36034723 complaining of progressive gradual loss of vision in the both eyes for two years.. she said that ( the glasses didn't fix the problem and I've changed it many times ) .. she denied any history of trauma .. there were no history of diabetes nor HTN ..

Examination :
on examination :-VA 6/9 OD ( right ) .
6/18 OS ( left ).IOP was 17 mmHg in both eyes .External sign ( Munson's sign ) .
SLE : 1- stromal thinning 2- Vogt's striae
Ophthalmoscope shows oil droplet sign .Funduscopy appeared normal.

differential diagnosis
• Astigmatism
• Myopia
•

management
• Contact lens because he still on stage 2


Anatomy of cornea:• The cornea is the transparent, dome-shaped
or Prolate which is flatter in the periphery and steeper centrally & its window covering the front of the eye. It is a powerful refracting surface, providing 2/3 of the eye's focusing power.
• Average size:
11mm vertically
12mm horizontally

histology
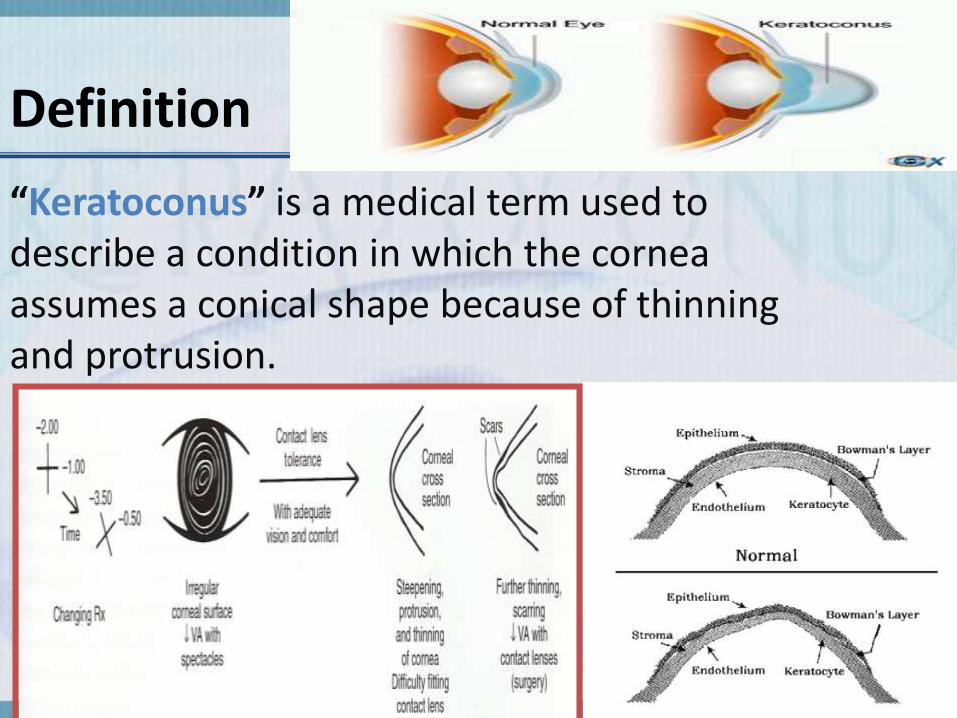
Definition
“Keratoconus” is a medical term used to describe a condition in which the cornea assumes a conical shape because of thinning and protrusion.

Keratoconus
• Keratoconus (KC) is a progressive,noninflammatory, bilateral (but usually asymmetrical) ectatic corneal disease, characterized by paraxial stromal thinning and weakening that leads to corneal surface distortion(forming conical shape) induces irregular astigmatism, myopia and protrusion leading to mild to moderate impairment in the quality of vision.

Histopathology
• Inherited ectatic disorder leading to reduction of corneal thickness
Characterized by:
- Extreme corneal thinning.
- Focal defects in epithelial basement membrane and Bowmans’ layer.
( Pathognomonic)
Clinical Presentation• The earliest Symptoms
blurring of vision ( 10Y – 30Y)
Changing eye glass prescription
Uncorrectable vision to 20/20
with glasses

Evaluation and diagnosis of keratoconus
History and family history
Follow up evaluation
Slit -lamp exams
Keratoscopy- Keratometry
Corneal thickness - pachymetry
Topography - Orbscan –Pentacam

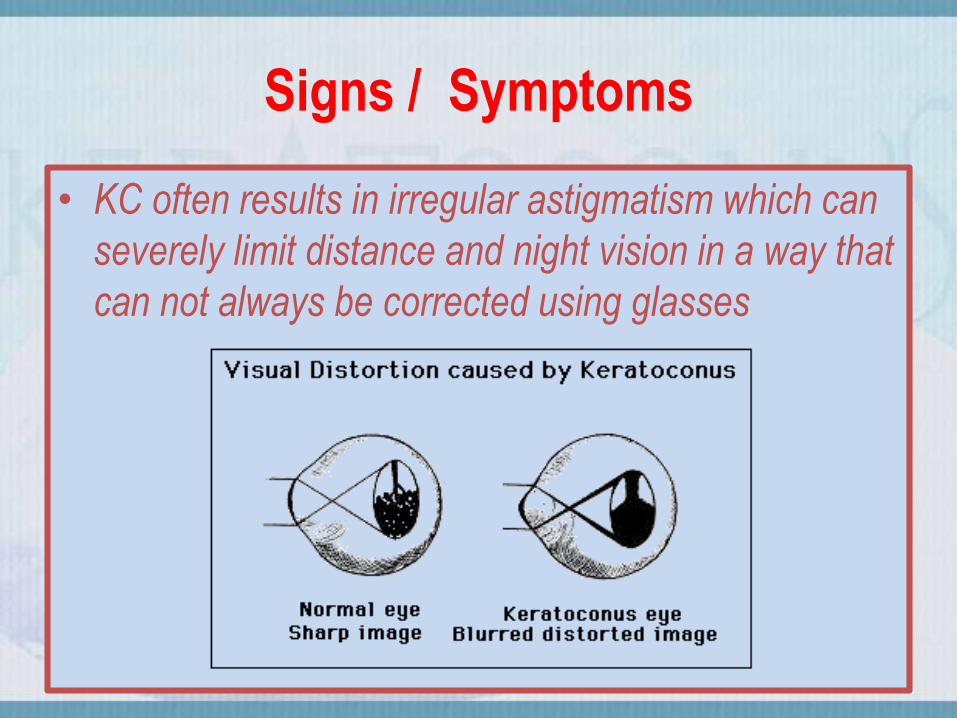
Signs / Symptoms
• KC often results in irregular astigmatism which can
severely limit distance and night vision in a way that
can not always be corrected using glasses
• Ghosting/ monocular diplopia
• Glare at night
• Haloes around lights
• Blurred/ distorted vision
Signs / Symptoms
• KC often results in irregular astigmatism which can
severely limit distance and night vision in a way that
can not always be corrected using glasses

Signs / Symptoms
• Frequently changing spectacle Rx and axis of astigmatism
• Poor repeatability of subjective refraction
• Ghosting/ monocular diplopia
• Glare at night
• Haloes around lights
• Blurred/ distorted vision
• Scissors reflex: (swirling retinoscopy reflex)
• Distorted/ irregular keratometer mires with steep readings
• Prominent corneal nerves

Detection of Keratoconus
1. Retinoscpy
2. Slit lamp
3. Keratometry
4. KeratoscpyVogt’s striae
fleisher’ ring

SIGNS OF KCN• External signs :
– Munson” sign– Rizzuti phenomenon
• Slit-lamp findings:– Stromal thining– Posterior stress lines(vogt,s striae)– Iron ring ( fleischer ring )– Scarring - epithelial or subepithelial
• Retroillumination signs:– Scissoring on retinoscopy– Oil droplet sign (charleaux”)
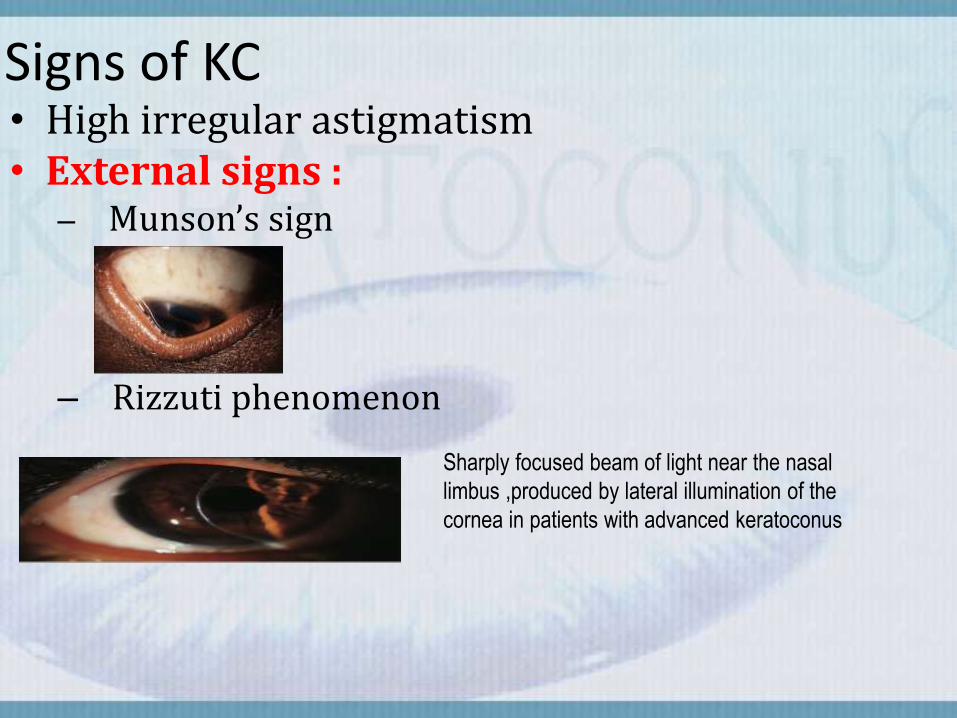
Signs of KC• High irregular astigmatism• External signs :
– Munson’s sign
– Rizzuti phenomenon
Sharply focused beam of light near the nasal
limbus ,produced by lateral illumination of the
cornea in patients with advanced keratoconus

Signs of KC Slit-lamp findings– Stromal thinningA hallmark, occurs at the apex of the cone
(the point of maximal protrusion)
:
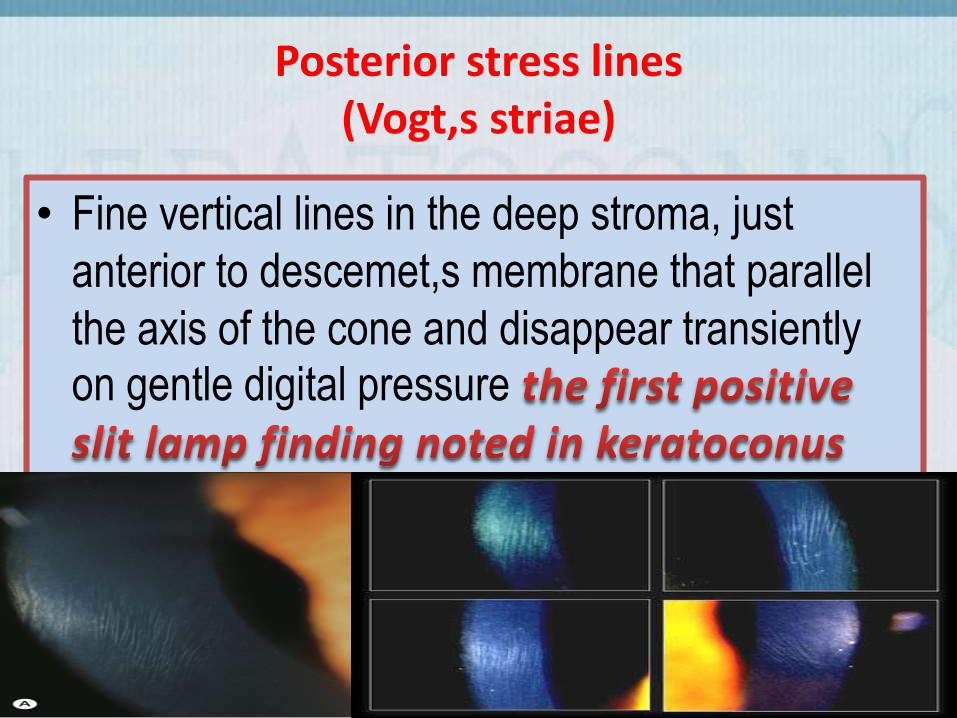
Posterior stress lines(Vogt,s striae)
• Fine vertical lines in the deep stroma, just
anterior to descemet,s membrane that parallel
the axis of the cone and disappear transiently on gentle digital pressure
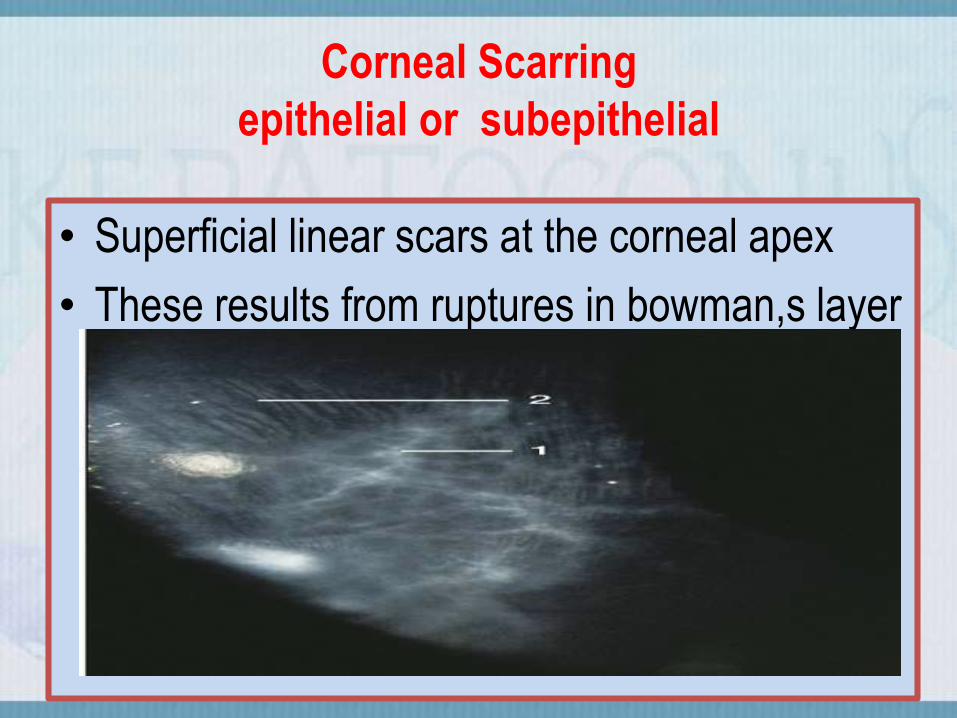
Corneal Scarring
epithelial or subepithelial
• Superficial linear scars at the corneal apex
• These results from ruptures in bowman,s layer


Iron ring ( fleischer ring )
• The ring is a partial or complete annular line
commonly seen at the base of the cone
• The ring is formed from hemosiderin pigment
deposited in the basal epithelium
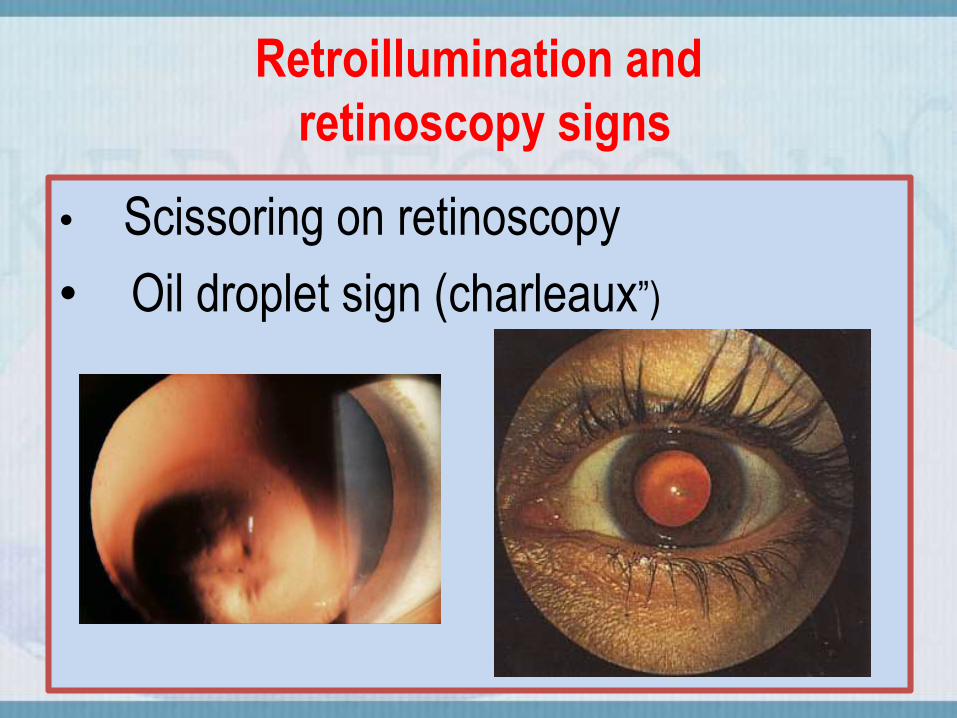
Retroillumination and
retinoscopy signs
• Scissoring on retinoscopy
• Oil droplet sign (charleaux”)

Corneal hydrops•Acute descemet membrane rupture and corneal
hydrops it will led to the deranges of Aq. Humor
inside the cornea

Risk Factors
• Uncontrolled ocular surface allergic disease• Chronic rubbing of the eyes• ocular associations
– vernal keratoconjunctivitis– retinitis pigmentosa
• systemic associations– connective tissue disorders
(eg, Ehlers-Danlos and Marfan syndromes)– mitral valve prolapse– Atopic dermatitis– Down syndrome.
Computerized Corneal Topography
• Corneal topography is the method by which the corneal shape, curvature, power, and irregularities are measured

Computerized Corneal Topography
• Corneal topography provides:
The Axial Curvature Map.
Describe the Shape and Power including the central 1-2 mm
The Elevation Maps.
The Pachymetric Map.
Quantitative Indices
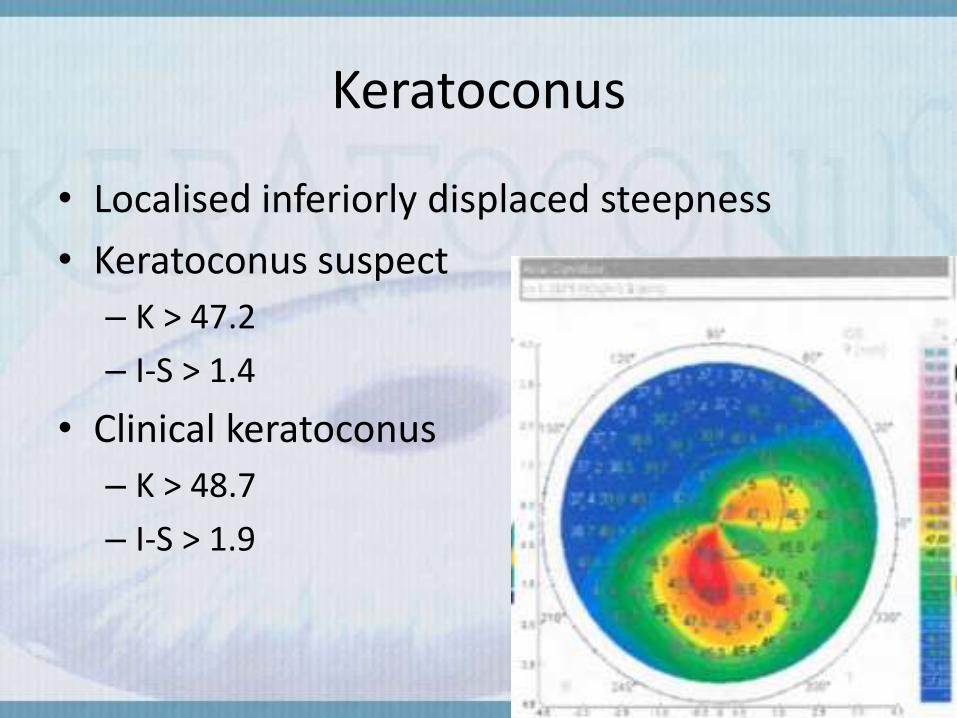
Keratoconus
• Localised inferiorly displaced steepness
• Keratoconus suspect
– K > 47.2
– I-S > 1.4
• Clinical keratoconus
– K > 48.7
– I-S > 1.9

How to reade am mape
• be sure you are reading for same Pt & be sure
File # & age & sex & this map for whice eye
• green colure is near to normal Yellow is boredr line and red in like patches its is hot spote
• Focus on avery map alone
• Put one point & strata reading

Anterior Map

Posterior Map

Keratometric Map

Pachemetry Map
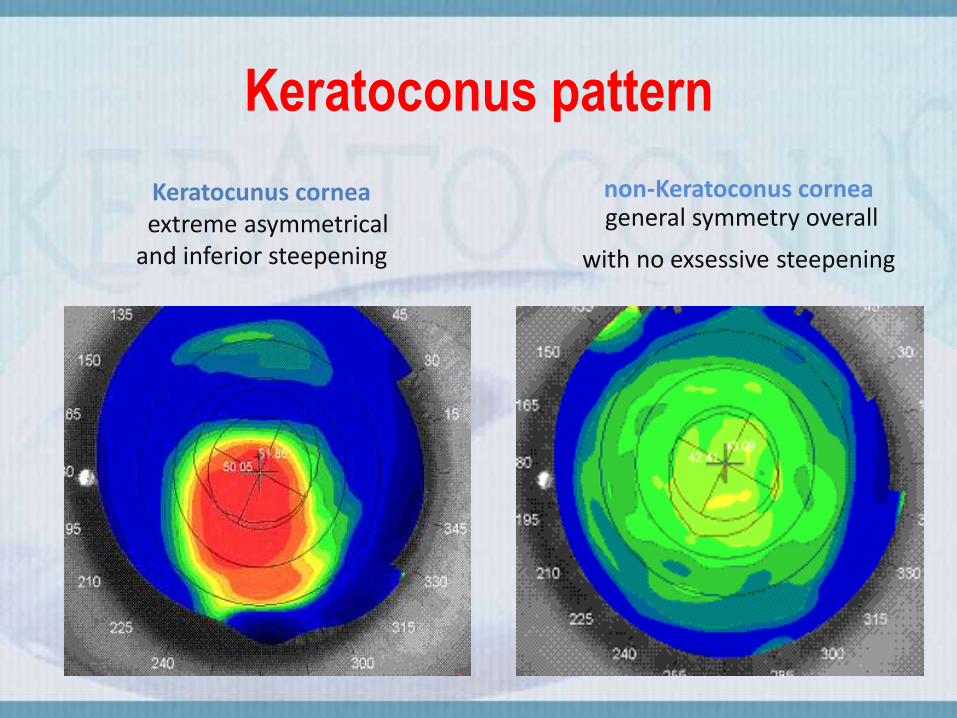
Keratoconus pattern
non-Keratoconus corneageneral symmetry overall
with no exsessive steepening
Keratocunus corneaextreme asymmetrical
and inferior steepening

Abnormal Topography

Topographic patterns of keratoconus
Inferior steepening without bowtie pattern specially more prominent temporally
Asymmetrical bow tie (AB)& inferior/superior steepening(IS-SS)
Central steepening +/- superimposed with asymmetrical bowtie pattern
symmetric bow tie (AB) & skewed radial axes (SRAX)


Topographic patterns of keratoconus

Topographic patterns of keratoconus
Topographic patterns of keratoconus
Inferior steepening without bowtie pattern specially more prominent temporally
Asymmetrical bow tie (AB)& inferior/superior steepening (IS-SS)
Central steepening +/- superimposed with asymmetrical bowtie pattern
Asymmetic /symmetric bow tie (AB) & skewed radial axes (SRAX)

Keratoconus pattern:Inferior steepening without bowtie pattern
specially more prominent temporally

Keratoconus pattern:
asymmetrical bow tie (AB)
& inferior steepening(IS)

Keratoconus pattern:asymmetrical bow tie (AB)& superior steepening(SS)

Keratoconus pattern:Central keratoconus
central unusual steepening without bow tie

Keratoconus pattern:Central steepening, superimposed with asymmetrical bowtie-slightly irregular astigmatism asymmetrical central hourglass
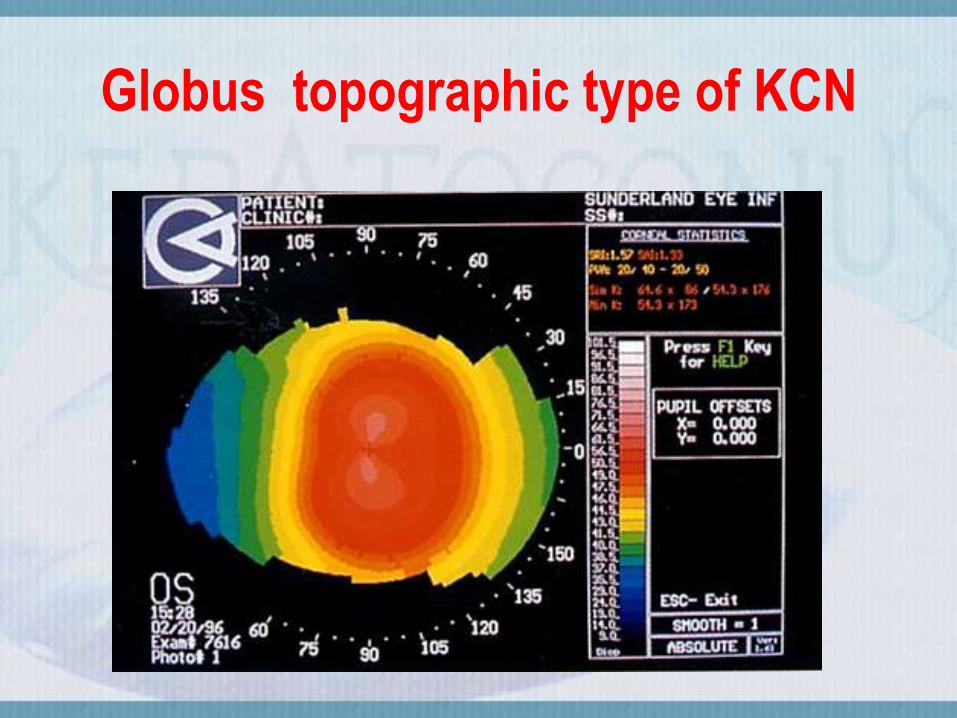
Globus topographic type of KCN

Keratoconus pattern:
Symmetic(SB) /asymmetric bow tie (AB) & (SRAX)

Keratoconus pattern:
asymmetrical bow tie & skewed radial axes (AB/SRAX)
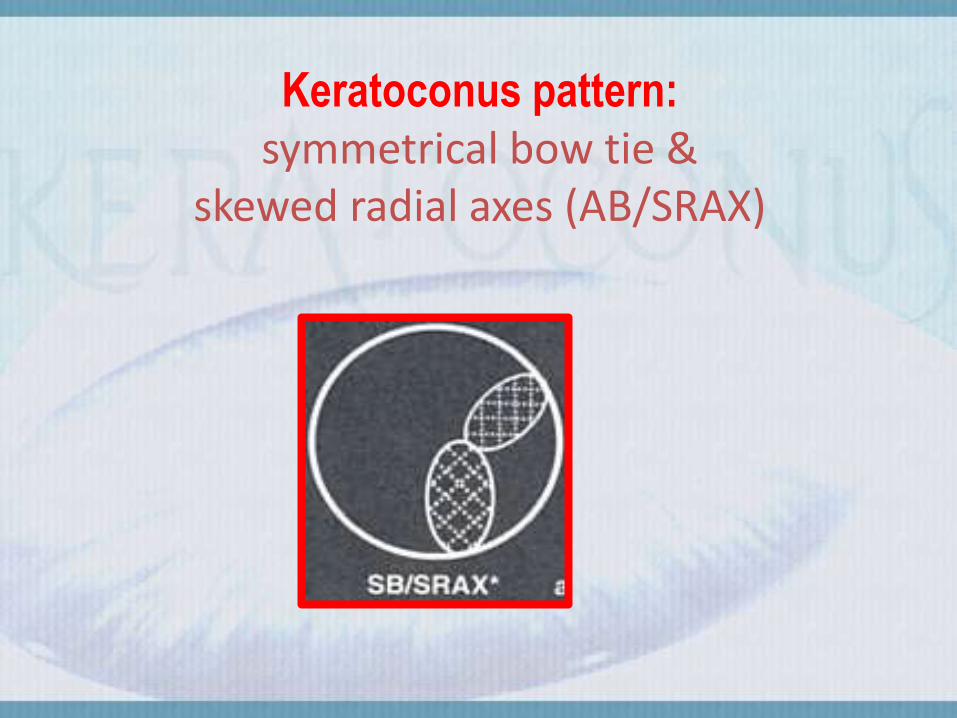
Keratoconus pattern:
symmetrical bow tie & skewed radial axes (AB/SRAX)
Grading of keratoconus according to amsler krumeich classification:
Stage I
• Eccentric steeping
• Myopia and astigmatism < 5.00 D
• Mean central K readings < 48.00 D
Stage II
• Myopia and astigmatism from 5.00 to 8.00 D
• Mean central K readings < 53.00 D
• Absence of scarring
• Minimum corneal thickness >400 μm.

Stage III
• Myopia and astigmatism from 8.00 to 10.00 D
• Mean central K readings >53.00 D
• Absence of scarring
• Minimum corneal thickness 300 to 400 μm.
Stage IV
• Refraction not measurable
• Mean central K readings >55.00 D
• Central corneal scarring
• Minimum corneal thickness 200 μm

treatment
• Spectacles—in stage 1
• Contact lens in stage 1;2 and 3(hard lenses)
• Photothrapeutic keratotomy.(in advanced kc)
• Intrastromal corneal rings.
• Corneal collagene cross linking . (stage 1;2)
• Phakic intraocular lenses.(stage1)
• Keratoplasty. (mainly in stage 4)


END
Prof. M.Barbary