Embed Size (px)
Citation preview

1/6/2015 Prof.Dr.R.R.Deshpande 1
Introduction to IHD
• Presented By –
• Prof.Dr.R.R.Deshpande (M.D in Ayurvdic
Medicine & M.D. in Ayurvedic Physiology)
• www.ayurvedicfriend.com
• Mobile – 922 68 10 630

1/6/2015 Prof.Dr.R.R.Deshpande 2
WE ALL WILL TALK
• For the Heart
• With our hearts
• From our hearts
• This is real Democracy !!

1/6/2015 Prof.Dr.R.R.Deshpande 3
Preventive Cardiology
• To boost up Immunity or Vyadhikshamatva
• What is Immunity ? ( Ayurved )
1) Vyadhi bala virodhitvam ( To arrest the
progress of disease )
2) Vyadhi utpadaktava pratibandhakatva
( To prevent occurrence of disease )

1/6/2015 Prof.Dr.R.R.Deshpande 4
Primary Prevention
• Heart is like synonym of Rhythm .For
Healthy Heart ---- keep the Rhythm in our
life style !
• Balanced Diet ,Regular Exercise,
Adequate sleep & Rest ,Yoga will
maintain the Rhythm of our life .

1/6/2015 Prof.Dr.R.R.Deshpande 5
Primary Prevention 2
• Avoid risk factors & keep away from vices

1/6/2015 Prof.Dr.R.R.Deshpande 6
To arrest disease progress

1/6/2015 Prof.Dr.R.R.Deshpande 7
What to Prevent ? -- IHD
• IHD – Ischemic Heart Diseases
• Angina Pectoris & Myocardial Infarction
(M.I.)
• Ischemia – Inadequate blood supply
• Infarct ------ Complete stoppage of blood
supply

1/6/2015 Prof.Dr.R.R.Deshpande 8
Angina Pectoris
• Angina means
• Heart muscles are crying due to
inadequate coronary blood supply to
myocardium.

1/6/2015 Prof.Dr.R.R.Deshpande 9
Angina Pectoris 2
• Cardiac pain of short duration & relieved by rest or sublingual vasodilator (sorbitrate)
• Pain in mid or upper sternal region or may be felt over left side of chest.
• Pain is constricting, squeezing,pressing or crushing in character. Neck is frequently described as chocking in character. There may be tingling sensation in left arm.

1/6/2015 Prof.Dr.R.R.Deshpande 10
Angina Pectoris 3
• Pain may radiate -- along both the
shoulder & upper arm ,more commonly on
left side.
• Pain usually starts after---- exercise –
walking uphill or upstairs ,after heavy
meals ,emotional upsets, exposure to cold
weather or even during sexual intercourse.

1/6/2015 Prof.Dr.R.R.Deshpande 11
Angina -- Investigations
• Resting ECG most of the time is not
useful.
But REMEMBER –
• Chest Pain = Cardiac Pain ,unless
proved otherwise .

1/6/2015 Prof.Dr.R.R.Deshpande 12
Angina – Investigations 2
• Resting ECG may be helpful to diagnose LVH in chronic HT & RVH in COPD.
• Rule out or confirm Angina by Treadmill or step Test ( ECG monitoring when patient do walking exercise on moving belt under supervision )

1/6/2015 Prof.Dr.R.R.Deshpande 13
Who has Angina ? Guess

1/6/2015 Prof.Dr.R.R.Deshpande 14
Stable Angina
Exercise Testing
N.A.N
2009

1/6/2015 Prof.Dr.R.R.Deshpande 15
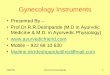
Types of ST seg Depression. 1) Horizontal or plain ST seg Depression.
This signifies myocardial ischemia.
2) Upward slopping ST seg Depression.
This is variant of Normal & significant only if,
point Depression > 2mm

1/6/2015 Prof.Dr.R.R.Deshpande 16
1)Horizontality of ST seg -
-ST seg – Horizontal & Isoelectric
-This is early manifestation of ischemia.
2)Downward slopping of ST seg -
This indicates severe Ischaemia
– Also seen in Digitalis toxicity.

1/6/2015 Prof.Dr.R.R.Deshpande 17
Exercise (stress) Test 1) ST Depression
2) Sometimes T Inversion

1/6/2015 Prof.Dr.R.R.Deshpande 18
1) ST Depression
2) Sometimes T Inversion

1/6/2015 Prof.Dr.R.R.Deshpande 19
Stress Test Positive- What Next?
• Stress test positive – ST depression –
indicates weakness of Heart !!
• How much is the Weakness ? ---
Advice 2 D echo of Heart ,which costs
only Rs.700 TO 1000 /-

1/6/2015 Prof.Dr.R.R.Deshpande 20
Stable Angina
2 D Echo
N.A.N
2009

1/6/2015 Prof.Dr.R.R.Deshpande 21
2 D Echo Test
• This test gives measurements of walls of
cardiac chambers & also functional
Capacity.
• In Chronic Hypertension mostly there is
Left Ventricular Hypertrophy ( LVH)
• Carefully note Ejection Fraction ( EF )
EF is < 50 --- It indicates Heart is weak !

1/6/2015 Prof.Dr.R.R.Deshpande 22
Heart is Weak --- Why ?
• Heart is weak due to less blood supply
through Coronary Arteries .
• Advice Coronary Angiography ,which
costs only around Rs. 10,000/-/
• This gives idea about which Coronary has
block ? Where ? & How much ?

1/6/2015 Prof.Dr.R.R.Deshpande 23
Angiography
N.A.N
2009

1/6/2015 Prof.Dr.R.R.Deshpande 24
Angiography
• Coronary Arteries are affected as follows
• Anterior Descending branch of Left
Coronary Artery ----- 75 %
• Right Coronary Artery -------- 20 %
• Left Circumflex branch ------- 05 %
• This gives idea whether there is one
vessel disease or 2 vessel disease or 3
vessel disease ?

1/6/2015 Prof.Dr.R.R.Deshpande 25
Angiography ---- What Next ?
• If one or two vessel disease or blocks are
below 50 % ---- Advice Angioplasty .
• If 3 vessel Disease or block is more than
70 % -------- Advice CABG ( Coronary
Artery Bypass Grafting = Bypass Surgery )

1/6/2015 Prof.Dr.R.R.Deshpande 26
Angioplasty
• During angioplasty, your doctor inserts a
special balloon-tipped catheter into your artery
and guides it to the blockage.
• Depending on the specifics of the blockage, your
doctor may place a stent in your artery. The
stent is an expandable device that is mounted
on a balloon catheter. The stent and balloon
are advanced to the blockage area, and the
stent is expanded into place.

1/6/2015 Prof.Dr.R.R.Deshpande 27
Angioplasty
• A stent supports the artery and helps it
remain open for a longer time. After the
stent has been placed, the body will grow
tissue over the stent to help maintain its
position. The stent will not move around
inside your body.
• An angioplasty procedure usually takes
from one to three hours

1/6/2015 Prof.Dr.R.R.Deshpande 28
Coronary Artery Bypass Grafting
( CABG )
• CHD is a condition in which a substance
called plaque ( plak) builds up inside the
coronary arteries.
• During CABG ,a healthy artery or vein
from the body is connected or grafted to
the blocked artery.
• The grafted artery or vein bypass the
blocked portion of the coronary artery.

1/6/2015 Prof.Dr.R.R.Deshpande 29
Progress of Angina
1 ) Stable Angina
2 )Unstable Angina – Pain more severe,
lasts longer ,occurs at rest ,not completely
relieved by Nitroglycerines.
3 ) Myocardial Infarction

1/6/2015 Prof.Dr.R.R.Deshpande 30
Prevent --- Progress of Angina
• R/o Diabetes Mellitus
• Not Known Diabetic --- Fasting & Post
Glucose Sugar
• Borderline Sugar Levels ---- Glucose
Tolerance Test or Modified Glucose
Tolerance Test.
• Known Diabetic ---- Fasting & Post
prandial Blood sugar, Glcosylated Hb

1/6/2015 Prof.Dr.R.R.Deshpande 31
Diabetes & Heart
• Blood Vessels become fragile
• Silent Myocardial Infarction --- May be
no pain .Can occur in long standing
Diabetes ,Hypertension ,elderly or middle
post operative patients

1/6/2015 Prof.Dr.R.R.Deshpande 32
Prevent progress of Angina
• Ageing ----- Arteriosclerosis ------- High
Cholesterol --------- Atherosclerosis ------
Hypertension -------- LVH ( Left Ventricular
Hypertrophy ) ------- Angina ------ M.I.

1/6/2015 Prof.Dr.R.R.Deshpande 33
Prevent Progress of Angina
1 Cholesterol Less than
200 mg %
2 HDL ( Good Cholesterol ) Greater than
45 mg %
3 LDL ( Bad Cholesterol ) Less than
130 mg %
4 Triglycerides Less than
150 mg %

1/6/2015 Prof.Dr.R.R.Deshpande 34
Prevent -- Progress of Angina
• Rule out causes of Secondary Hypertension
• 1 ) Serum Urea & Creatinine
• 2 ) Abdominal Sonography
• 3 ) T 3 ,T 4 ,TSH
• 4 ) Renal Angiography ( To r/o Renal Artery Stenosis )
• 5 ) 24 hour Urine – 17 Keto steroids ( Pheochromocytoma )

1/6/2015 Prof.Dr.R.R.Deshpande 35
Diagnose M.I --- At the Earliest !!
• Typical retrosternal Pain of Angina ,but
unlike Angina it starts at rest ,persists
longer & is not relieved by coronary
dilators (Angised ).

1/6/2015 Prof.Dr.R.R.Deshpande 36
Diagnose M.I --- At the Earliest !!
• Patient is anxious & restless .
• Profuse sweating but limbs are cold.
• Sometimes nausea, vomiting,sensation for
urination or defecation

1/6/2015 Prof.Dr.R.R.Deshpande 37
Diagnose M.I --- At the Earliest !!
• Yes !! ECG will definitely help !!
• But ECG changes may not be that much clear within first few hours & then you must repeat ECG & also can take help of other Investigations -----
• Let us have a look on various ECG patterns related with Heart Attack ----

1/6/2015 Prof.Dr.R.R.Deshpande 38
Myocardial Infarction
3 cardinal signs on ECG in AMI -
1)Elevation of ST segment.
2)Inverted T wave.
3)Deep & wide Q wave.

1/6/2015 Prof.Dr.R.R.Deshpande 39
Events in chronological Order
1)on 1st day - ST elevated
- with upright tall T wave
- but No Q wave
2)Over Next 2 day -
T wave will slowly become Inverted, ST seg still raised.
3)Towards the end of 1st wk -
- ST seg returning to base Level, T wave deeply inverted
- Q wave starts appearing.
- T wave - Pointed, Inverted & symmetrical Limbs.

1/6/2015 Prof.Dr.R.R.Deshpande 40
4)In 3rd week -
- Q wave fully developed.
- ST - Base
- T – wave flat & Returning to Normal.
5)By the end of 3 month -
-St seg & T wave – Return to Normal.
-Only Q wave remains permanent.
(of course if size of infarct is TOO small -Q wave may disappear)
-Q wave size is proportional to size of infarct.

1/6/2015 Prof.Dr.R.R.Deshpande 41
Anterior M.I.
= S T Elevation in V1 – V4

1/6/2015 Prof.Dr.R.R.Deshpande 42
Anterior M.I.
= T Inversion in
V1 – V4

1/6/2015 Prof.Dr.R.R.Deshpande 43
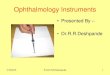
Lateral M. I.
- S T Elevation in I, aVL, V4 – V6
- Hyper acute T waves in V4 & V5

1/6/2015 Prof.Dr.R.R.Deshpande 44
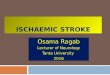
Inferior M.I
i) Q in II, III aVF
ii) T Inversion in II, III, aVF

1/6/2015 Prof.Dr.R.R.Deshpande 45
i) Anterior M. I. - V1 to V4
ii) Lateral M. I. - I, aVL, V5 – V6
iii) Antero Lateral - I, aVL,
V1 – V6.
iv) Antero-septal - V1 – V3
v) Interior M.I. - II, III, aVF
vi) Infero Lateral - I, II, III
aVL, aVF,
V5-V6.

1/6/2015 Prof.Dr.R.R.Deshpande 46
Diagnose M.I --- At the Earliest !!
Sr.
No
Chemical Markers Values Comment
1 Serum Myoglobin (Earliest
Indicator )
(10-46 microgram
per lit)
Rs.1250/-
2 CardiacTroponin T (Rises
earlier)
Positive or
Negative
Rs.900 /-
3 SGOT.
Peak at 18 to 36 hours &
come down in 3 to 4 days.
40 U/L Rise in 8 to 12
hours.

1/6/2015 Prof.Dr.R.R.Deshpande 47
Diagnose M.I --- At the Earliest !!
• CK ( Creatine Kinase ) ----
• Normal Value – 25 to 195 U/L
• Levels start rising within 6 hours of onset
of Infarction. Peak at 24 hours & come to
normal within 48 to 72 hours.
• Cost --- Rs.350/-

1/6/2015 Prof.Dr.R.R.Deshpande 48
Diagnose M.I --- At the Earliest !!
• CKMB
• Normal Value – 0.25 U/L
• Specific Marker of Myocardial Necrosis.
• CKMB – Twice the upper limit indicates AMI

1/6/2015 Prof.Dr.R.R.Deshpande 49
Appeal to all
Ayurvedic Practioner Friends
• Always claim our success with Documentary proof of Objective Parameters .
• Do not only present subjective Expressions of Patients like feeling better ,Pain is less while exertion ,less breathlessness ,feeling energetic etc.etc.

1/6/2015 Prof.Dr.R.R.Deshpande 50
Appeal – Show Results
as follows
Sr.
No
Objective
Parameter
Pre
Treatment
Post
Treatment
1 PP Blood Sugar 400 mg 170 mg
2 Cholesterol 400 mg 180 mg
3 Ejection Fraction
( 2 D Echo )
30 55
4 Coronary
Blockage
(Angiography )
90 % 40 %

1/6/2015 Prof.Dr.R.R.Deshpande 51
Book for your G.P.( Rs. 85 /-)
• Description of 60
common diseases or
218 symptoms
• Causes,Investigations
& readymade
prescriptions

1/6/2015 Prof.Dr.R.R.Deshpande 52
Book for your G.P.( Rs. 60 /-)
• For successful
diagnosis clinical
examination of all 9
Important systems
• Ayurvedic Srotas
Examination
• Clinical Interpretation
of all Lab
Investigations.

1/6/2015 Prof.Dr.R.R.Deshpande 53
Book for your G.P.( Rs. 50 /-)

1/6/2015 Prof.Dr.R.R.Deshpande 54
V C D for your G.P.( Rs 200/-)

1/6/2015 Prof.Dr.R.R.Deshpande 55
THANKS 4 HEARING
MY PRESENTATION
• I hope that it is useful
• My best regards
• Professor
Dr.R.R.Deshpande (M.D)
Mobile –
922 68 10 630