Embed Size (px)
Citation preview
DIABETIC RETINOPATHY MANAGEMENT
BY Dr. Nitish
DIAGNOSIS
• Visual acuity test
• Pupil dilation
• Fundus examination
• Slit Lamp Biomicroscopy
• Ophthalmoscopy
• Flouresceine angiography
• Optical coherence tomography (OCT)

FUNDUS EXAMINATION WHEN ??

• FIRST EXAMINATIONIDDM-5yr after onset/puberty
NIDDM-immediately after diagnosisDIABETIC PREGNANT-early first
trimester• FOLLOW UP
NPDR without maculopathy-min 6mthsNPDR with maculopathy-min 3-4mthsPDR-2-3mthsDIABETIC PREGNANT-each trimester
FLUORESCEIN ANGIOGRAPHY
• Sodium fluorescein dye injected to Ant-cubitalvein
• 80% bound to plasma protein ,20% unbound
• Pictures taken for 12 secs at interval of 1.5 to 2 secs
• Blue light used to excite
• Green light emitted

Hyperfluorescent dots which leak in later stage bordering areas of capillary non perfusion
MICRO-ANEURYSMS

HYPOFLUORESCENC DUE TO NON FILLING
CAPILLARY CLOSURE

HYPOFLUORESCENCE DUE TO BLOCKAGE OF BACKGROUND CHOROIDAL FLUORESCENCE
HARD EXUDATE
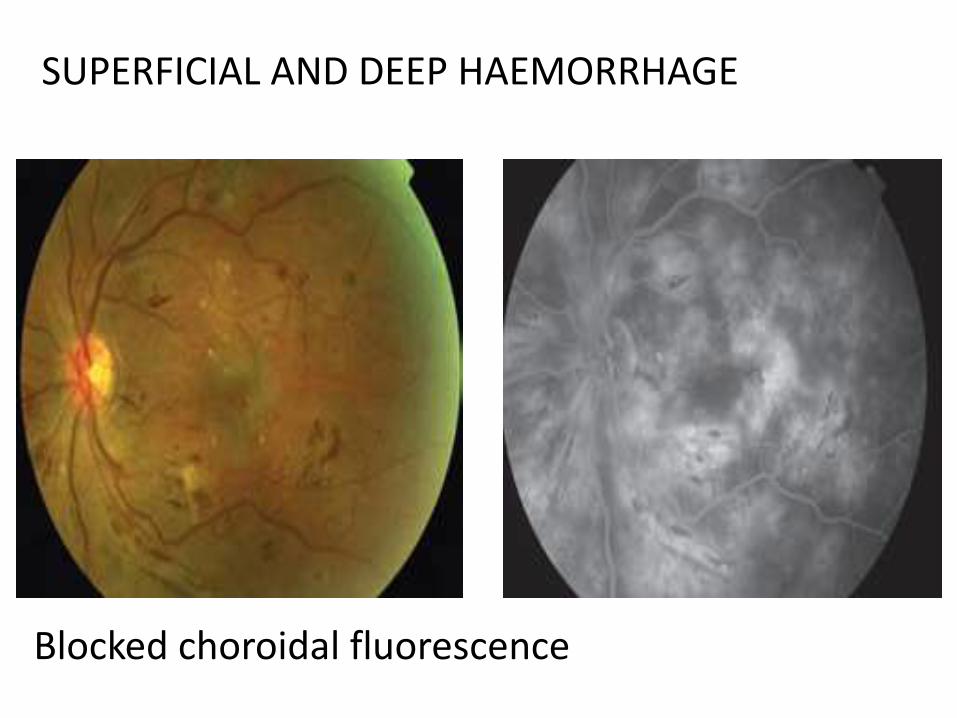
SUPERFICIAL AND DEEP HAEMORRHAGE
Blocked choroidal fluorescence

Do not leak fluorescence except at their growing tips
IRMA

Venous dilatation , venous beading
VENOUS ABNORMALITIES

FREELY LEAKS THE DYE(hyperfluorescence )
NEO VASCULARISATION

CYSTOID MACULAR EDEMA
Capillary dilatation in perifoveal regionPetaloid pattern (fusiform cystoid spaces arranged in radial pattern)

PRE PROLIFERATIVE DIABETIC RETINOPATHY
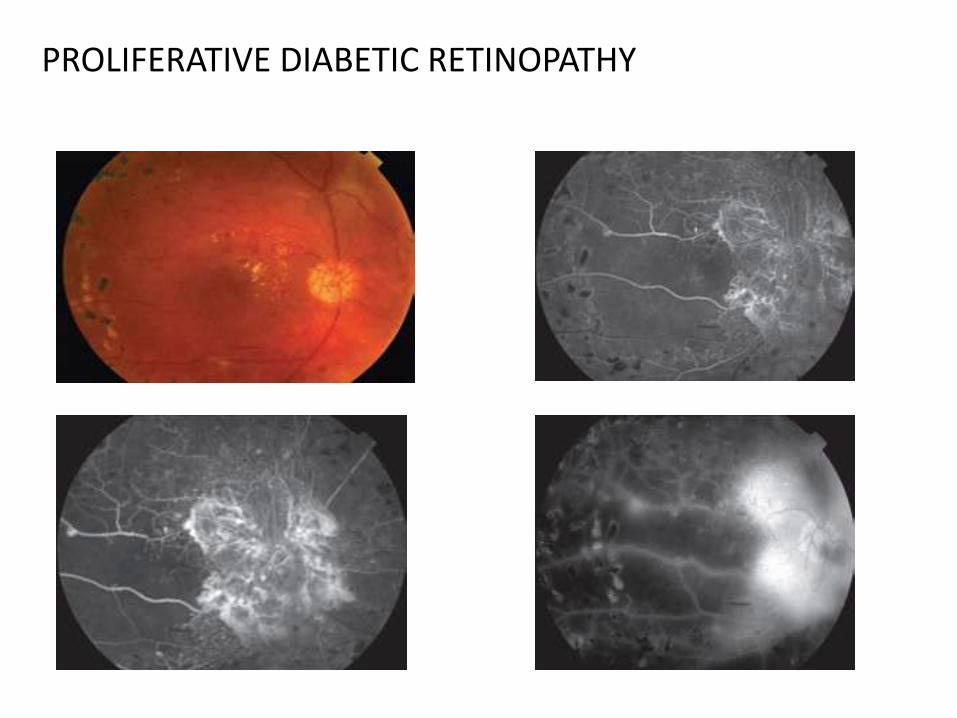
PROLIFERATIVE DIABETIC RETINOPATHY
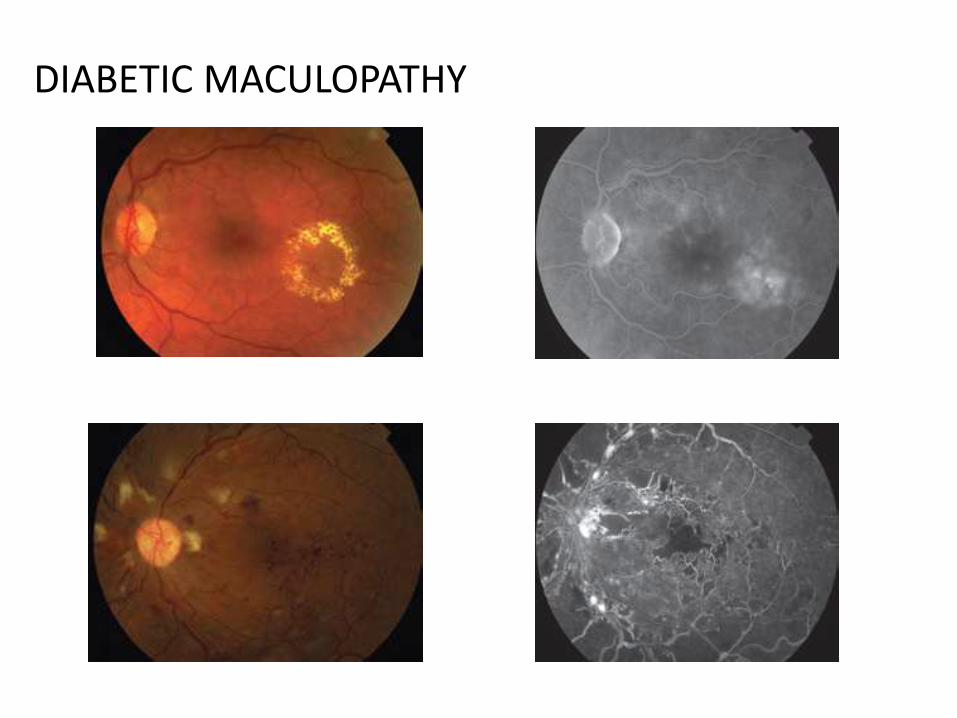
DIABETIC MACULOPATHY

Role of FFA
• To asess the level of DR
• To guide laser photocoagulation of microaneurysms
• To asess capillary drop out at macula-poor prognosis
• To identify lesions such as NVE or NVD

SIDE EFFECTS AND COMPLICATIONS
• Local tissue necrosis
• Nausea and vomiting
• Vasovagal reaction(circulatory shock,myocardial infarction)
• Allergic reaction,anaphylaxis
• Thrombophlebitis
• Pyrexia
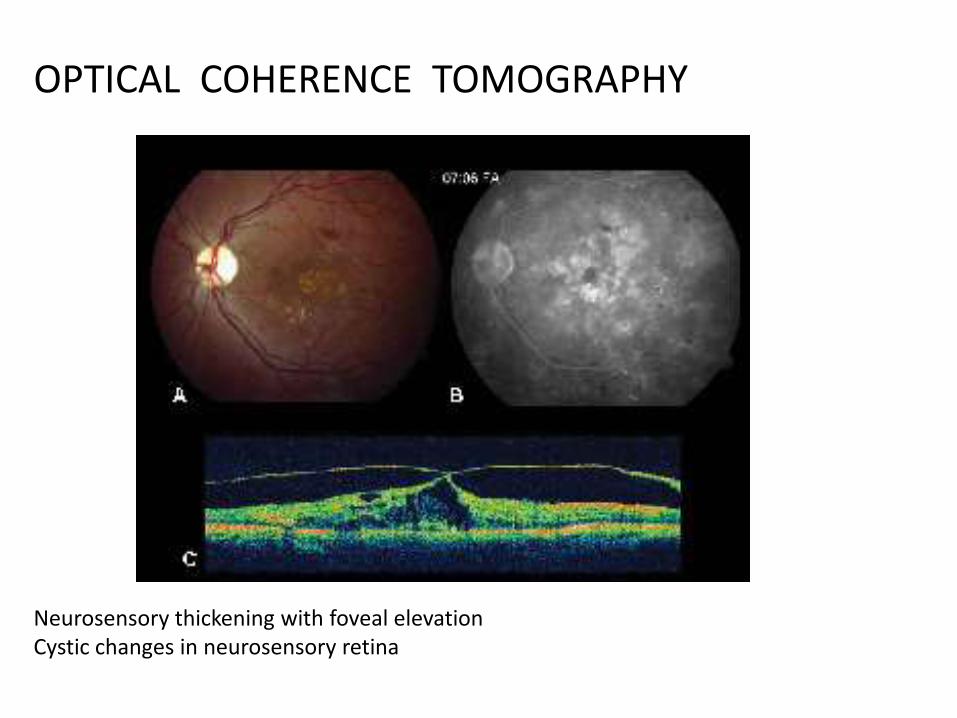
Neurosensory thickening with foveal elevationCystic changes in neurosensory retina
OPTICAL COHERENCE TOMOGRAPHY

MANAGEMENT
• APPROACH• Primary level-prevention
-target high risk group(duration ,blood sugar level,asso with hypertention ,renal disease,pregnancy)
-educating• Secondary level-early diagnosis and treatment
-regular follow up-laser treatment-controlling risk factor

• Tertiary level-vitreous surgery
-visual rehabilitation
-social and vocational rehabilitation

LEVELS OF RETINOPATHY
• Non-proliferative diabetic retinopathy (NPDR)• Mild non-proliferative diabetic retinopathy• Microaneurysms• Dot and blot haemorrhages • Hard ( intra-retinal ) exudates
• Moderate-to-severe non-proliferative diabetic retinopathy• The above lesions, usually with exacerbation, plus: • Cotton-wool spots • Venous beading and loops • Intraretinal microvascular abnormalities ( IRMA )
• Proliferative diabetic retinopathy
• Neovascularization of the retina, optic disc or iris
• Fibrous tissue adherent to vitreous face of retina
• Retinal detachment
• Vitreous haemorrhage
• Pre retinal haemorrhage
• Maculopathy
• Clinically significant macular oedema (CSME )
• Ischaemic Maculopathy

LASER TREATMENT
FOCAL PHOTOCOAGULATION
• INDICATIONS
Eyes with CSME with center involved
Eyes with CSME without center also
Eyes with macular edema-watched
• TECHNIQUE
FA prior-identify treatable lesions
Microaneurysms,IRMA,leaking

• FOCAL
Micro aneurysms ,Hard Exudate
Spot size-100 to 200 m
duration-0.1 sec
End point-whitening or darkening of lesion
• GRID
Thickened retina showing leakage
Spot size-100 m
Duration-0.1 sec
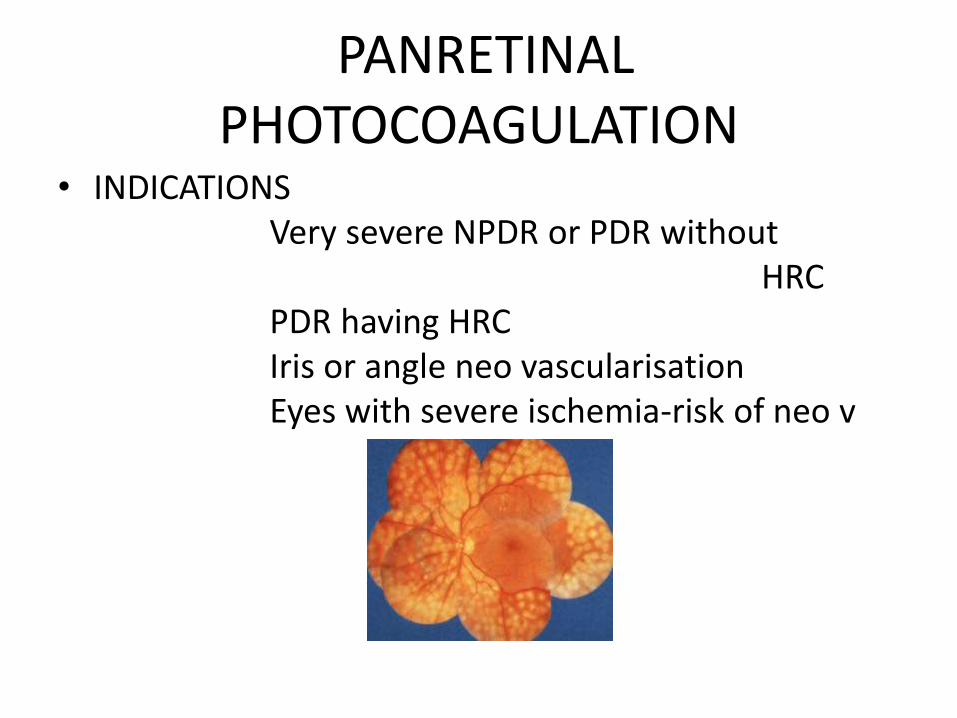
PANRETINAL PHOTOCOAGULATION
• INDICATIONSVery severe NPDR or PDR without
HRC PDR having HRC Iris or angle neo vascularisationEyes with severe ischemia-risk of neo v

• Proliferative diabetic retinopathy (PDR)
create 1,000 – 2,000 burns
Reduce retina's oxygen demand-ischemia
• Advanced diabetic retinopathy
Destroy the abnormal blood vessels that form in the retina.

Will Vision Improve After Laser Treatment?

• Laser therapy can ONLY STOP the PROGRESSION of the retinopathy. It CANNOT REVERSE the damage already done.

COMPLICATIONS OF LASER TREATMENT
Optic disk damage
• Foveal burn• Macular edema• Choroidal –Hemorrhage
Neo vascularisationDetachment
• Retinal detachment• Pain • Loss of visual field• Increase in traction detachment• IOP

Intravitreal Triamcinoloneacetonide
• Injected in the vitreous cavity
Decreases the macular edema (thickening of the retina at the macula)
• The effect –transient
lasting up to three months
Repeated injections for maintaining the beneficial effect.
• Complications - cataract, steroid-induced glaucoma and Endophthalmitis
Whats New in Non-Laser Treatment?
• Anti- vascular endothelial growth factor(VEGF)
Block the signal causing growth of
abnormal retinal blood vessels
• common anti-VEGFs
pegaptanib , ranibizumab , bevacizumab
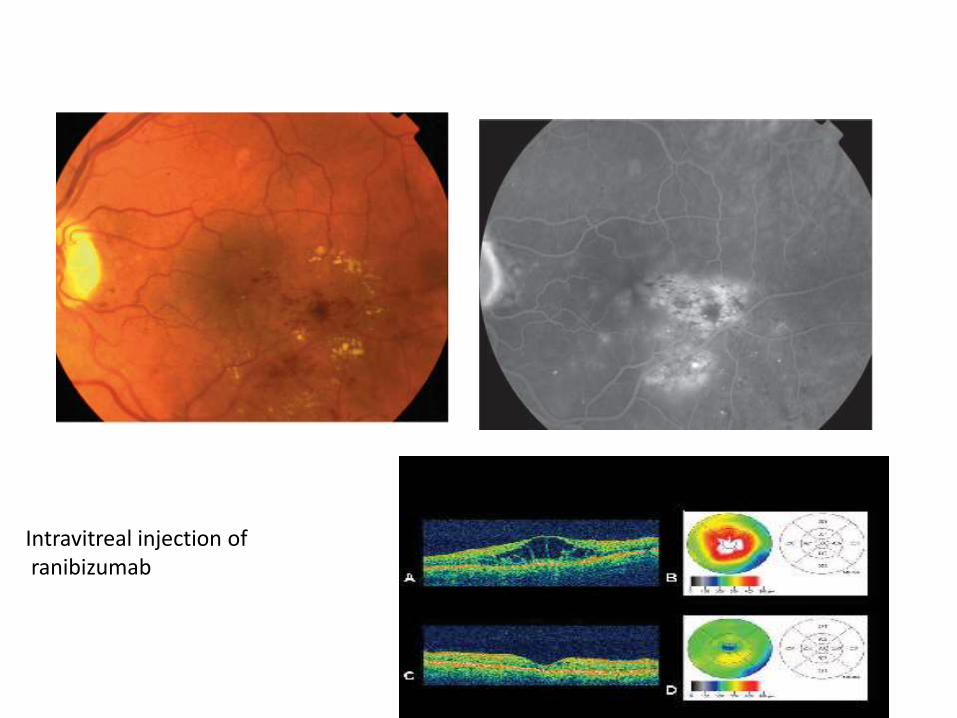
Intravitreal injection ofranibizumab

VITRECTOMY
• INDICATIONS
Vitreous hemorrhage
Tractional retinal detachment
Severe progressive fibro vascular
proliferation
Ant seg neo vascularisation with post seg
opacity
Macular edema with premaculartraction

PDR After Vitrectomy surgeryPDR before vitrectomy

CONCLUSION
• “PROMPT factors
Patient education
Research application
Ophthalmological evaluation
Mass media utilization
Physician and primary health care personel
orientation
TIMELY laser treatment

THANK
YOU

How does diabetic retinopathy cause vision loss?
Blood vessels damaged from diabetic retinopathy can cause vision loss in
two ways:
• Fragile, abnormal blood vessels
• and leak blood
• blurring vision
• Fluid can leak into the center of the macula
• fluid makes the macula swell, blurring vision

Who is at risk for diabetic retinopathy?

MEDICAL- General aspects of the ocular care of diabetics
• All people with diabetes mellitus are at risk –those with Type I diabetes
• Duration and severity of diabetis
• glycaemic control
• Ass with
blood pressure
hyperlipidemia
cardiac problem
Diabetic nephropathy
• Smokers

MEDICAL TREATMENT
• Antiplatelet therapy
• Vit E
• Lipid reduction-Diet-rich in polysaturatedfats(30%)
20% protiens
50% carbohydrates
Hypolipidemic agent
clofibrate
lovastatin
pravastatin

ELECTRORETINOGRAM
• Abnormalities at very early stage -no visible changes in fundus
• Increase in OP time
• Reduction of scotopic b-wave amplitude
• Useful in media opacities-macular function
• Genestein, a soy isoflavone
blocks VEGF receptors
ameliorate retinal vascular permeability in diabetic animals
available as Ocuvite DF.
• vitamin B1
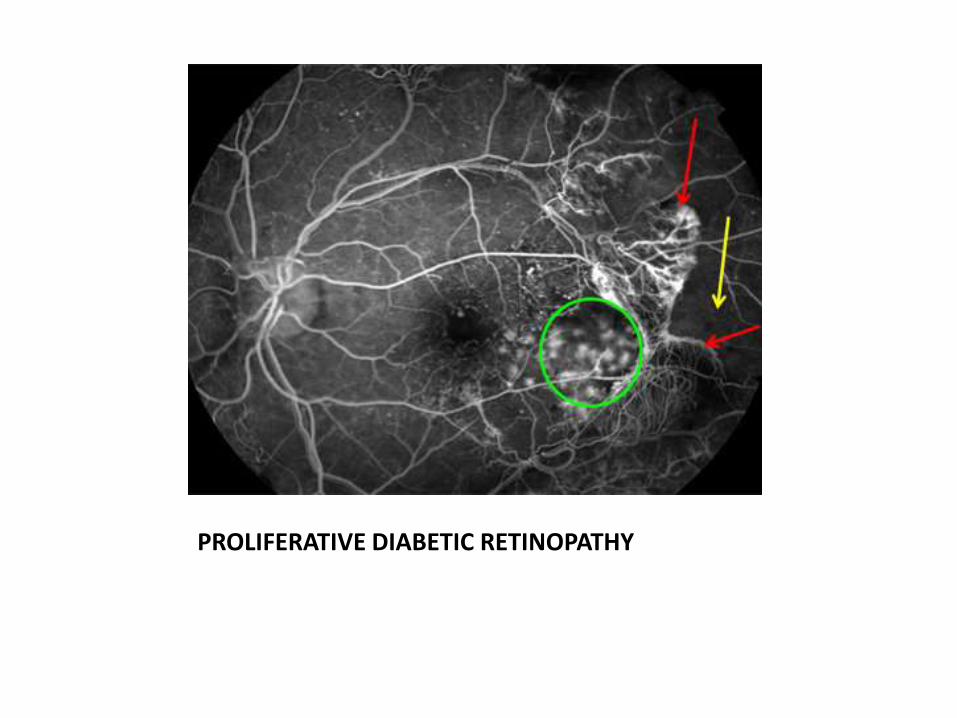
PROLIFERATIVE DIABETIC RETINOPATHY



![The Guide - Diabetic Retinopathy - Vision Lossvisionloss.org.au/wp-content/uploads/2016/05/The... · the guide [diabetic retinopathy] What is Diabetic Retinopathy? Diabetic Retinopathy](https://img.pdfslide.us/doc/110x75/5e3ed00bf9c32e41ea6578a8/the-guide-diabetic-retinopathy-vision-the-guide-diabetic-retinopathy-what.jpg)