Embed Size (px)
DESCRIPTION
Cofactores virales en el síndrome de inmunodeficiencia adquirida
Citation preview

Reviews in
MEDICALVIROLOGY VOL. 2: 29-34 (1992) 29
INTRODUCTION
Viral Cofactors in Acquired Immune Deficiency Syndrome Alison Webster Department of Virology. Royal Free Hampstead NHS Trust, London NW3, UK
Symptomatic immunodeficiency does not usually occur until several years after infection with human immuno- deficiency virus (HIV), although the length of this time interval is subject to considerable individual variation. This can be explained to some extent by the life cycle of HIV within an infected cell: reverse transcription of viral RNA is followed by integration of the proviral DNA into the host cell genome, in which form the virus may remain latent for prolonged periods. Subsequent activation of the virus results in lysis of the infected CD4 lymphocyte and release of infectious virions. Symptoms of AIDS might also be caused by the dissemination of HIV to cell populations other than CD4 lymphocytes.
In an infected individual markers of HIV disease pro- gression, such as loss of CD4 lymphocytes and the pres- ence of HIV viraemia suggest that the disease processes commence at the time of HIV seroconversion. The rate at which these processes occur may determine the interval at which AIDS develops, and potentially could be modulated by the effects of a cofactor virus defined as one which hastens the onset of acquired immune deficiency syndrome (AIDS). A viral cofactor may not be essential for the devel- opment of AIDS, since AIDS is probably the inevitable consequence of HIV infection, although for some individ- uals, the time taken to develop AIDS may exceed their natural life span.
The acquisition of HIV itself may be enhanced by other viral infections, such as genital ulceration due to herpes simplex virus. Once AIDS has supervened, other viruses may play an opportunist role in the development of life- threatening infections or neoplasms. The scope of this review is limited to consideration of the progression from asymptomatic HIV infection to AIDS, and the role that other viruses, acting as cofactors in conjunction with HIV, may play in this process. In practical terms, identification of viral cofactors is extremely important, since abrogation of their effects, even if it extends the disease-free interval by I to 2 years, may offer a worthwhile benefit to the patient, equivalent to any currently available anti- retroviral therapy. Laboratory studies have suggested many potential mechanisms by which heterologous viruses may accelerate HIV disease, which are discussed below.
INTERACTIONS AT THE MOLECULAR LEVEL
Transcription of the HIV proviral DNA is under the control of regulatory elements located in the long terminal repeat (LTR). Both viral and cellular proteins interact with sequences in this region to modulate expression of the genome. These include the HIV trans-acting protein (tat), and several cellular transcriptional factors such as NFKB, SP-I and LBP-I.
The ability of various heterologous viral proteins to transactivate the HIV LTR has been studied by many groups using cells cotransfected with plasmids containing the HIV- I LTR linked to the reporter gene chloramphenicol acetyl transferase (CAT), and plasmids containing the viral gene of interest. Alternatively, cell lines chronically infected with the heterologous virus have been transfected with the HIV LTR-CAT construct. Herpes simplex virus (HSV), cyto- megalovirus (CMV), human herpesvirus-6 (HHVd), Epstein-Barr virus (EBV), papovaviruses, hepatitis B virus (HBV), human T cell leukaemia virus (HTLV) type I and adenoviruses’-’ have all been reported to transactivate the HIV LTR under these conditions. Interest has focused on identifying the particular viral proteins involved, and the HIV sequences with which they interact. Transactivation by heterologous viruses appears to be independent of the interaction between HIV tat and its response element, tar. The HBV x gene and HTLV-1 tax gene products have been identified as transactivators of the HIV LTR, and the immediate early (IE) gene products of the herpesviruses have been shown to mediate this effect, but there is some disagreement as to precisely which herpesvirus genes are responsible. The fact that nonproductive herpesvirus infec- tion may be sufficient to stimulate HIV gene expression is worth noting.
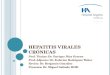
The precise mechanism of transactivation is unclear; it may result directly from binding of the viral protein to the HIV LTR, or indirectly from the interaction of the viral protein with cellular transcription factors (see Figure I). Binding sites for several cellular transcription factors have been identified on the HIV LTR. Recent studies have suggested that the relative abilities of HIV tat, and two CMV IE genes to transactivate the HIV LTR are highly dependent upon the cell system underlining the importance of cellular transcription factors. Interaction
ISSN I05 2-92 76/92/010029-06 $05 .OO 0 1992 by John Wiley & Sons, Ltd. Accepted 29 June 1991

A. WEBSTER
r
Monocyte
Cytokine Cofactor eg TNF-a viral antigen
1 \ 4 Transcription
HIVLTR * Figure 1. Transactivation of the HIV long terminal repeat (LTR). Possible mechanisms of interaction between extracellular or intracellular cofactor virus, and the HIV LTR, resulting in stimulation of HIV gene expression.
with the binding site for the cellular transcription factor, NFKB may be a common pathway in transactivation of the HIV LTR by HHV-6, HSV and HBV.’&’’
Molecular interaction between HIV and cofactor viruses may be a two way process. Upregulation of a cofactor virus by HIV may be a mechanism by which opportunistic viral infections develop, independently of a decline in immune surveillance. This reciprocal enhancement of viral expression has been demonstrated in vitro for CMV’3*’4 and the papovavirus JC,I5 but not for HSV.I6 For such direct molecular interactions to occur in vivo, it is necessary that both viruses are present within the same cell. This may occur coincidentally for some viruses, especially the lymphotropic viruses such as HHV-6 and HTLVs, but specific mechanisms may facilitate dual infection (see below). However, the extent to which coinfection occurs in vivo is unclear.
The results of cotransfection experiments should be interpreted with caution, however, since this artificial sys- tem may not predict the result of coinfection in vih-o or in viva. Both CMV and HSV increase the expression of HIV in dually infected cells,” and CMV enhances lysis” of T lymphoblasts infected with HIV. Conflicting results have been reported for HHV-6 since different groups have found an increase3 or decrease” in HIV replication in dually infected cells.
INTERACTIONS AT THE CELLULAR LEVEL Upregulation of HIV gene expression by cellular transcrip- tion factors may also be brought about by external stimuli such as mitogens or cytokines. Stimulation of HIV infected peripheral blood mononuclear cells (PBMC) by inactivated HTLV-1 has been shown to increase HIV expression,” and HIV expression in a chronically infected T-cell line” can be increased by the cytokine tumour necrosis factor alpha (TNF-a). Production of cytokines can be stimulated by viral infections, so providing an alternative mechanism by which viruses upregulate HIV (see Figure I), and this has been investigated in u i h . Soluble mediators, identified as
TNF-a, produced by PBMC following challenge with inactivated viral antigens, are capable of upregulating HIV expression in chronically infected T-cell lines.” Cells stimulated with CMV, EBV or HIV produced cytokines which upregulated HIV; in contrast, challenge with HSV-I, HSV-2, varicella-zoster virus, HHV-6, vaccinia or HBV was ineffective in this
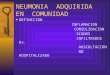
In addition to these interactions, mediated via the stimu- lation of HIV gene expression, the presence of cofactor viruses may facilitate the progression of HIV disease by other specific and nonspecific mechanisms. One specific mechanism might be the enhancement of cellular tropism, so allowing HIV to penetrate cells which do not express CD4, for example within the central nervous system, where it may cause local pathology. Cofactor-enhanced uptake of HIV may also increase the opportunity for direct molecular interaction between the two viruses by increas- ing the frequency of dually infected cells. Infection and transformation of cord-blood B lymphocytes by EBV has been shown to render these cells susceptible to HIV infec- t i ~ n . ’ ~ It is known that antibody-coated HIV is able to gain entry into cells via the receptor for the Fc component of IgG on the cell ~urface.’~ The herpesviruses CMV and HSV induce the expression of these receptors on the surface of infected cells, which could then be exploited by HIV (see Figure 2a). This possibility has been demonstrated in vitro: it has been shown that antibody-coated HIV can be taken up into CMV-infected fibroblasts, cells which lack CD4 expression, and which are not normally permissive for
HIV uptake may also be facilitated by infection with a cofactor virus through the induction of transcription of the cellular gene encoding the HIV receptor, the CD4 molecule (see Figure 2b). Expression of the CD4 molecule has been shown to occur in mature CD8+CD4- lymphocytes following HHV-6 infection, so rendering the cells suscept- ible to infection with HIV.” In contrast, cells infected with CMV or HSV in this system did not behave in the same way.
Phenotypic mixing of HIV with other viruses may result in the formation of pseudotypes with altered target cell tropism. Incorporation of additional viral proteins into the HIV envelope could allow HIV to exploit a wider range of host cell receptors (see Figure 2c). Pseudotypes have been reported to occur in T-cell lines coinfected with HTLV-1 and HIV,” with progeny virus able to penetrate into vari- ous cells lacking CD4, and also in T-cell lines coinfected with HIV and HSV.29
Nonspecific mechanisms of interaction might include the recruitment and activation of HIV-infected cells of the monocyte-macrophage lineage in response to an active infection with a cofactor virus, so increasing dissemination of HIV. Differentiation from monocyte to macrophage, as part of the immune response, may be a prerequisite for activation of latent HIV within these cells.
HIV?
EPIDEMIOLOGICAL STUDIES
Epidemiological studies have not satisfactorily confirmed or refuted the clinical relevance of the experimental results

VIRAL COFACTORS IN AIDS 31
Cofactor k + virus Cofactor k 4
antibody
Uptake
Cofactor Ifr virus
HIV
Cof act0 r virus infected cell
PseudotvDe +- containing HIV genome
Cofactor virus infected cell
SU Uptake
Figure 2. Possible mechanisms by which HIV host cell range may be expanded. (a) Cofactor virus infection may induce expression of receptors for Fc com onent of IgG (FcR) on cell surface, so enabling uptake of antibody-coated HIV. (b) Cofactor virus infection may induce expression orthe CD4 molecule, the receptor for HIV gp120 on the cell surface, which may then mediate uptake of HIV. (c) Phenotypic mixing of cofactor virus and HIV may result in an HIV pseudotype expressing cofactor viral proteins. HIV may then exploit cofactor virus-receptor interactions.
described above, and it is useful to spend a few moments considering why this might be so. The prolonged period to development of AIDS demands that patients must be followed for many years from the time of HIV serocon- version; merely documenting an association between a particular measure of viral infection and the severity of HIV disease in a cross-sectional study cannot be taken as proof of a causative role. Even when groups are followed prospectively, results may be inconclusive. Other host factors, including a e?' genetic background?' and con- tinuing drug abuse!' have been identified as important variables in determining the time to onset of AIDS, and failure to account for these may confound the analysis of a cofactor effect. Other factors, relating to patient lifestyle, underlying diseases, and route and quantity of HIV inocu- lum may also affect the progression of AIDS. This latter factor is especially important where HIV and a putative cofactor share routes of transmission, since the presence of a cofactor may simply reflect an increased exposure to HIV itself. This may to some extent preclude extrapolation from studies undertaken in particular risk groups or geographical areas to the HIV-infected population in gen- eral. Few studies have been undertaken in heterosexuals, yet it is this group that is likely to occupy our attention in future.
Herpesviruses The herpesvimses are ubiquitous amongst the general population, and HIV infection therefore frequently occurs against a background of herpesvirus infection. Their role as cofactors in AIDS, particularly the lymphotropic herpes- viruses CMV and HHV-6, has been investigated in various HIV risk groups. Infection with these viruses has generally been diagnosed on the basis of serological studies.
Human herpesvirus-6 HHV-6 has been isolated from T and B lymphocytes, and infection is common amongst the general population, being acquired during the first few years of life. Antibodies to HHV-6 are generally detected by immunofluorescence, which is a subjective technique, and prevalence rates are to some extent arbitrarily determined by the cut-off titre chosen. The possible influence of HHV-6 on progression to AIDS has been analysed in a group of homosexual men with lymphadenopathy, whose dates of HIV serocon- version were not known, 66% of whom were reported to be seropositive for HHV-6.33 Over a period of 5 years, 30% of patients developed AIDS; no association was found between HHV-6 and disease progression. However, it is not clear whether the serological criterion chosen is a true reflection of HHV-6 infection, since prevalence rates higher

~~ ~
3 2 A. WEBSTER
than this have been reported to occur in the general popu- lation. Epidemiological studies to elucidate the role of HHV-6 are likely to be difficult because of its very high prevalence.
Cytomegalovirus CMV is found in 50-60% of adults from developed countries, but is even more prevalent amongst certain groups because of their high-risk sexual behaviour. For this reason, the cofactor effect of CMV cannot be studied in HIV-infected homosexuals since CMV infection is vir- tually universal in this group. Furthermore, because both viruses are transmitted via the same route, an absence of CMV may merely reflect a lower HIV inoculum.
We have reported the adverse effect of CMV serostatus on the progression of HIV disease on a cohort of HIV infected haemophiliacs, a population with a CMV pre- valence of 54%. CMV is not transmitted by clotting factor concentrates, and is therefore not a marker of increased exposure to HIV in this group.34 Further follow-up (for a median of 8.3 years) confirms that CMV-positive patients are significantly more likely to have progressed to AIDS, compared with CMV-negative patients, after controlling for age. This study attempted to address the difficulties outlined in the introduction to this section. Other groups who have not reached the same conclusions, have been less rigorous in their approach.
A small study of HIV-infected haemophiliacs failed to find an association between CMV status and the develop- ment of symptoms of HIV infecti0n.3~ However, this category included patients with generalised lymphaden- opathy, a condition which does not carry prognostic sig- nificance. Two other longitudinal studies have also failed to find a relationship between CMV serostatus and pro- gression to AIDS; one in HIV-infected haemophiliac~,~~ and another in a diverse population of blood donors and recipients of blood or blood pr0ducts.3~ The dates of HIV seroconversion were unknown for most of these indi- viduals, and few of their patients developed a measurable end-point during the study period. Differences in the study design prevent comparisons being made between these reports.
A study of a small number of infants perinatally exposed to HIV suggests that infants infected with CMV and HIV have a worse prognosis, as reflected in AIDS mortality, than those infected with HIV alone.38 Interaction between CMV and HIV may occur in the mother, with transmission of a higher HIV inoculum to her offspring, or within the infant. However, the possibility cannot be excluded that mothers who have more advanced HIV disease for whatever reason are more likely to reactivate and transmit CMV, and so give birth to infants who have a worse prognosis because they have received a larger inoculum of HIV.
Epstein-Barr virus Evidence in support of a role for EBV in HIV disease pro- gression is lacking. Lang and colleagues report no associ- ation between EBV seropositivity (as measured by IgC antibodies against virus capsid antigen) and progression to AIDS over a study period of up to 32 months in a popu-
lation of blood donors and blood or blood product recipi- ents whose dates of HIV seroconversion were unknown.37 The proportion of HIV-infected homosexuals who have elevated IgA antibody titres to EBV virus capsid antigen increases with the stage of HIV di~ease,~’ but this may be a consequence, rather than a cause, of progressive HIV infection.
There is some circumstantial evidence that suppression of herpesviruses might have a beneficial effect in HIV infected patients. In a small placebo-controlled trial, therapy with high dose acyclovir has been shown to im- prove some markers of HIV disease rogression in patients with asymptomatic HIV infection. 49
Human T-cell leukaemia viruses The HTLVs are infrequently found within the general population in the western world, but are endemic in Japan and the Caribbean. These viruses are tropic for T cells, and share certain routes of transmission with HIV, and are thus found in certain risk groups for HIV, such as i.v. drug abusers (IVDA). Their role as potential cofactors for AIDS has been investigated in IVDA and in homosexuals in the Caribbean. Serological methods are generally unable to distinguish between infections with HTLV-I or 2, so epidemiological studies have considered both viruses together.
Two studies in IVDA in the USA report an association between HTLV seropositivity and severity of HIV disease. Lee ef al. report4’ that 15% of HIV infected IVDA are also infected with HTLV. Dually infected subjects were signifi- cantly more likely to have fever or weight loss, compared with those infected with HIV alone. However, the non- specific nature of these symptoms, the possible shared route of transmission, the lack of knowledge of the length of HIV seropositivity and the variation in prevalence of both viruses in different age groups prevent us from draw- ing many conclusions from this study. Page ef al. report4’ a prospective study of HIV-infected IVDA, 21% of whom were also infected with HTLV. After a follow-up of about 2 years, mortality from AIDS was significantly higher in dually infected patients (35% vs 12%) after controlling for age and injecting frequency. These results are certainly suggestive of a cofactor role for HTLV 112 in AIDS, but a more detailed study in patients with known dates of HIV seroconversion is required.
A study of a small number of HIV-infected homosexuals in Trinidad reveals that dually infected individuals are more likely to have HIV disease, but this re ort suffers from the limitations of a cross-sectional study.
HTLVs might prove to be important cofactors in these populations, but are unlikely to have any major impact in patients in the western world because of the rarity of infection with these viruses.
4 P
Hepatitis B virus HBV is transmitted by the same routes as HIV, and this virus is therefore prevalent amongst certain unvaccinated HIV risk groups. Solomon ef al. report a study of HIV- infected homosexuals followed for a period of 2.5 years.44 The presence of serological markers for HBV was not

VIRAL COFACTORS IN AIDS
related to progression to AIDS in this group, although the date of HIV seroconversion was not known for these individuals.
CONCLUSIONS The topic of viral cofactors in AIDS is highly controversial. Other variables, such as age and genetic background, may modulate the size of any cofactor effect in a given study population, as will the prevalence of the virus in that popu- lation. As yet no consensus has emerged on the effects of any virus on progression to AIDS. Evidence in favour of, or against, a particular virus acting as a cofactor can be found in the experiments outlined above. The discrepant labora- tory results may be partly explained by differences in the experimental cell system chosen, since it is becoming increasingly clear that molecular interactions are to some extent dependent upon host cell mediators.
Identification of viral cofactors is undertaken with the aim of prolonging the interval between HIV infection and AIDS by suppressing their effects with antiviral agents. This could conceivably be achieved with active or passive immunoprophylaxis, or with antiviral agents. Vaccines are likely to be useful tools in preventing cofactor infection only as part of a general vaccination policy, since these infections are often acquired in early life. However, vaccines may potentially modulate the effects of prior infection, for example by suppressing active infection. Antiviral agents, such as high dose acyclovir, may be useful in lessening the effect ofacofactor, by inhibiting viral replication.The taskof establishing the precise mechanisms of interaction between cofactor viruses and HIV thus takes on extra importance, so that the molecular targets for antiviral agents can be identified. For example, the development of agents which interfere with transcriptional factors might be effective in suppressing the effects of latent cofactor infections.
1.
2.
3.
4.
5.
REFERENCES Gendelman, H. E., Phelps, W., Feigenbaum, L. et al. (1986). Transactivation of the human immuno- deficiency virus long terminal repeat sequence by DNA viruses. Proc. Natl. Acad. Sci. USA, 83, 9759-9763. Davis, M., Kenney, S. C., Kamine, J., Pagano, J. S. and Huang, E. S. (1987). Immediate-early gene region of human cytomegalovirus trans-activates the promoter of human immunodeficiency virus. Proc. NaB Acad. Sci.
Lusso, P., Ensoli, B., Markham, P. D. et ul. (1989). Pro- ductive dual infection of human CD4+ T lympho- cytes by HIV-1 and HHV-6. Nature, 337,370-373. Kenney, S., Kamine, J., Markovitz, D., Fenrick, R. and Pagano, J. (1988). An Epstein-Barr virus immediate early gene product trans-activates gene expression from the human immunodeficiency virus long terminal repeat. F’roc. Natl. Acad. Sci. USA, 85, 1652-1656. Siddiqui, A., Gaynor, R., Srinivasan, A., Mapoles, J. and Farr, R. W. (1989). Trans-activation of viral enhancers including the long terminal repeat of the human
USA, 84,8642-8646.
33
immunodeficiency virus by the hepatitis B virus X protein. Virology, 169,479-484.
6. Siekevitz, M., Josephs, S. F., Dukovitch, M., Peffer, N., Wong-Staal, F. and Greene, W. C. (1987). Activation of the HIV-1 LTR by T cell mitogens and the transacti- vator protein of HTLV 1. Science, 238, 1575-1578.
7. Rice, A. B. and Matthews, M. B. (1988). Trans- activation of the human immunodeficiency virus long terminal repeat sequences, expressed in an adenovirus vector, by the adenovirus ElA 13s protein. Proc. Natl.
8. Rando, R. F., Srinivasan, A., Feingold, J., Gonczol, E. and Plotkin, S. (1990). Characterization of multiple molecular interactions between human cytomegalo- virus (HCMV) and human immunodeficiency virus type 1 (HIV-1). Virology, 176,87-97.
9. Barry, PA, Pratt-Lowe, E., Unger, R. E. and Luciw, P. A. (1991). Cellular factors regulate transactivation of human immunodeficiency virus type 1. I. Virol., 65,
10. Ensoli, B., Lusso, P., Schachter, F. et al. (1989). Human herpes virus-6 increases HIV-I expression incoinfected T cells via nuclear factors binding to the HIV-1 enhancer. EMBO]., 8,3019-3027.
11. Gimble, J. M., Duh, E., Ostrove, J. M., Gendelman, H. E., Max, E. E. and Rabson, A. B. (1988). Activation of the human immunodeficiency virus long terminal repeat by herpes simplex virus type 1 is associated with induc- tion of a nuclear factor that binds to the NF-kappa B/ core enhancer sequence. ]. Virol., 62,4104-4112.
12. Twu, J. S., Chu, K. and Robinson, W. S. (1989). Hepa- titis B virus X gene activates kappa B-like enhancer sequences in the long terminal repeat of human immunodeficiency virus 1. Proc. Nutl. Acud. Sci. USA.,
13. Skolnik, P. R., Kosloff, B. R. and Hirsch, M. S. (1988). Bidirectional interactions between human immuno- deficiency virus type 1 and cytomegalovirus. ]. Infect. Dis., 15 7, 508-5 14.
14. Ho, W. Z., Harouse, J. M., Rando, R. F., Gonczol, E., Srinivasan, A. and Plotkin, S. A. (1990). Reciprocal enhancement of gene expression and viral replication between human cytomegalovirus and human immuno- deficiency virus type I. ]. Gen. Virol., 71,97-103.
15. Tada, H., Rappaport, J., Lashgari, M., Amini, S., Wong- Staal, F. and Khalili, K. (1990). Trans-activation fo the JC virus late promotor by the tat protein of type 1 human immunodeficiency virus in glial cells. Proc. Natl. Acad. Sci. USA, 87,3479-3483.
16. Rando, R. E., Pellett, P. E., Luciw, P. A., Bohan, C. A. and Srinivasan, (1987). Transactivation of the human immunodeficiency virus by herpesvirus. Oncogene, 1,
17. Tremblay, M., Gomitsky, M. and Wainberg, M. A. (1989). Active replication of human immunodeficiency virus type 1 by peripheral blood mononuclear cells following coincubation with herpesviruses. 1. Med. Viral., 29, 109-114.
18. Casareale, D., Fiala, M., Chang, C. M., Cone, L. A. and Mocarski, E. S. (1989). Cytomegalovirus enhances
Acud. Sci. USA, 85,4200-4204.
1392-1399.
86,5168-5172.
13-18.

34 A. WEBSTER
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
lysis of HIV-infected T lymphoblasts. Int. ]. Cancer, 44,
Canigan, D. R., Knox, K. K. and Tapper, M. A. (1990). Suppression of human immunodeficiency virus type 1 replication by human herpesvirus-6. ]. Infect. Dis., 162,
Zack, J. A., Cann, A. J., Lugo, J. P. and Chen, I. S. (1988). HIV-I production from infected peripheral blood T cells after HTLV-1 induced mitogenic stimulation. Science, 240,1026-1029. Folks, T. M., Justement, J., Kinter, A., Dinarello, C. A. and Fauci, A. S. (1987). Cytokine-induced expression of HIVl in a chronically infected promonocytic cell line. Science, 238, 800-802. Clouse, K. A., Powell, D., Washington, I. et al. (1989). Monokine regulation of human immunodeficiency virus-I expression in a chronically infected human T cell clone. ]. Immunol., 142,431-438. Clouse, K. A., Robbins, P. B., Femie, B., Ostrove, J. M. and Fauci, A. S. (1989). Viral antigen stimulation of the production of human monokines capable of regulating HIVl expression. ]. Immunol., 143,470-475. Pagano, J. S., Kenney, S., Markovitz, D. and Kamine, J. (1988). Epstein Barr virus and interactions with human retroviruses. ]. Virol. Methods, 21,229-239. Takeda, A., Tuazon, C. U. and Ennis, F. A. (1988). Antibody-enhanced infection by HIV-1 via Fc receptor-mediated entry. Science, 242,580-583. McKeating, J. A. & Griffiths, P. D. and Weiss, R. A. (1990). HIV susceptibility conferred to human fibro- blasts by cytomegalovirus-induced Fc receptor. Nature, 343, 659-661. Lusso, P., DeMaria, A., Malnati, M. et al. (1991). Induc- tion of CD4 and susceptibility to HIV-1 infection in human CD8 + T lymphocytes by human herpesvirus 6. Nature, 349,533-535. Lusso, P., Lori, F. and Gallo, R. C. (1990). CD4- independent infection by human immunodeficiency virus type I after phenotypic mixing with human T cell leukaemia viruses. ]. Virol., 64,6341-6344. Zhu, Z., Chen, S. S. L. and Huang, A. S. (1990). Pheno- typic mixing between human immunodeficiency virus and vesicular stomatitis virus or herpes simplex virus.
Goedert, J. J., Kessler, C. M., Aledort, L. M. etal. (1989). A prospective study of human immunodeficiency virus type I infection and the development of AIDS in people with haemophilia. N. Engl. ]. Med., 321,
Steel, C. M., Ludlam, C. A., Beatson, D. et al. (1988). HLA haplotype A1 B8 DR3 as a risk factor for HIV- related disease. Lancet, i, 1185-1188. Weber, R., Ledergerber, B., Opravil, M., Siegenthaler, W. and Luthy, R. (1990). Progression of HIV infection in misusers of injected drugs who stop injecting or
124-130.
844-85 1.
]. AIDS, 3,215-219.
1121-1 148.
follow a programme of maintenance treatment with methadone. Br. Med. J., 301,2-5.
33. Spira, T. J., Bozeman, L. H., Sanderlin, K. C. et al. (1990). Lack of correlation between human herpesvirus-6 infection and the course of human immunodeficiency virus infection. ]. Infect. Dis., 161,567-570.
34. Webster, A., Lee, C. A., Cook, D. G. et al. (1989). Cytomegalovirus infection and progression towards AIDS in haemophiliacs with human immunodeficiency virus. Lancet, ii, 63-66.
35. Jackson, J. B., Erice, A., Englund, J. A., Edson, J. R. and Balfour, H. H. (1988). Prevalence of cytomegalovirus antibody in hemophiliacs and homosexuals infected with human immunodeficiency virus type 1. Transfusion, 28, 187-189.
36. Becherer, P. R., Smiley, M. L., Matthews, T. J., Weinhold, K. J., McMillan, C. W. and White, G. C. (1990). Human immunodeficiency virus- I disease progression in hemophiliacs. Am. ]. Hematol., 34(3),
37. Lang, D. J., Kovacs, A. A., Zaia, J. A. e l al. (1989). Seroepidemiologic studies of cytomegalovirus and Epstein-Barr virus infections in relation to human immunodeficiency virus type 1 infection in selected recipient populations. J. AIDS, 2,540-549.
38. Frenkel, L. D., Gaur, S., Tsolia, M., Scudder, R., Howell, R. and Kesarwala, H. (1990). Cytomegalovirus infec- tion in children with AIDS. Rev. Infect. Ds., 1 2 Suppl7, s820-826.
39. Margalith, M., Sarov, B., Sarov, I. et al. (1990). Serum IgC and IgA antibodies specific to Epstein-Barr virus capsid antigen in a longitudinal study of human immunodeficiency virus infection and disease pro- gression in homosexual men. AIDS Res. Hum. Retroviruses, 6, 607-616.
40. Chavanet, P., Malet, J., Waldner, A. et al. (1990). A double blind randomized placebo trial on very high doses of acyclovir in weakly symptomatic HIV- patients. Cancer Detect. Prev., 14, 669-673.
41. Lee, H. A., Weiss, S. H., Brown, L. S. et al. (1990). Patterns of HIV-1 and HTLV-1/11 in intravenous drug abusers from the middle atlantic and central regions of the USA.]. Infect. Dis., 162,347-352.
42. Page, J. B., Lai, S., Chitwood, D. D., Klimas, N. G., Smith, P. C. and Fletcher, M. A. (1990). HTLV-1/11 seropositivity and death from AIDS among HIV-1 seropositive intravenous drug users. Lancet, i,
43. Bartholomew, C., Blattner, W. and Cleghom, F. (1987). Progression to AIDS in homosexual men co-infected with HIV and HTLV-I in Trinidad. Lancet, 2, 1469.
44. Solomon, R. E., Van Raden, M.. Kaslow, R. A. et al. (1990). Association of hepatitis B surface antigen and core antibody with acquisition and manifestations of human immunodeficiency virus type 1 (HIV 1) infection. Am. ]. Public Health, 80, 1475-1478.
204-209.
1439-1441.