How to Assess the Risk of VTE in Ambulatory Cancer Patients Receiving ChemotherapyMarc Carrier MD FRCPC
SAES.ENO.20.02.0157b FEBRERO 2020
VTE SAFE
TY ZONE
Spain
202
0
VTE SAFE
TY ZONE
Spain
202
0
Objectives
• 1) To review the epidemiology and clinical relevance of venous thromboembolic (VTE) complications in cancer patients
• 2) To discuss the role of different Risk Assessment Models to stratify ambulatory cancer patients according to their underlying risk of VTE
• 3) To review if these Risk Assessment Models can help clinicians in providing VTE awareness to patients and help decision about thromboprophylaxis.
VTE SAFE
TY ZONE
Spain
202
0
VTE SAFE
TY ZONE
Spain
202
0
Incidence
Annual incidence of VTE in the general population is 117 per 100,000• Cancer alone was associated with a 4.1-fold risk of thrombosis• Chemotherapy increased the risk 6.5-fold
Combining these estimates yields an approximate annual incidence of venous thromboembolism (VTE) of 1 per 200 in a population of cancer patients
Heit JA et al. Arch Intern Med. 2000; 160: 809–815.
VTE SAFE
TY ZONE
Spain
202
0
VTE SAFE
TY ZONE
Spain
202
0
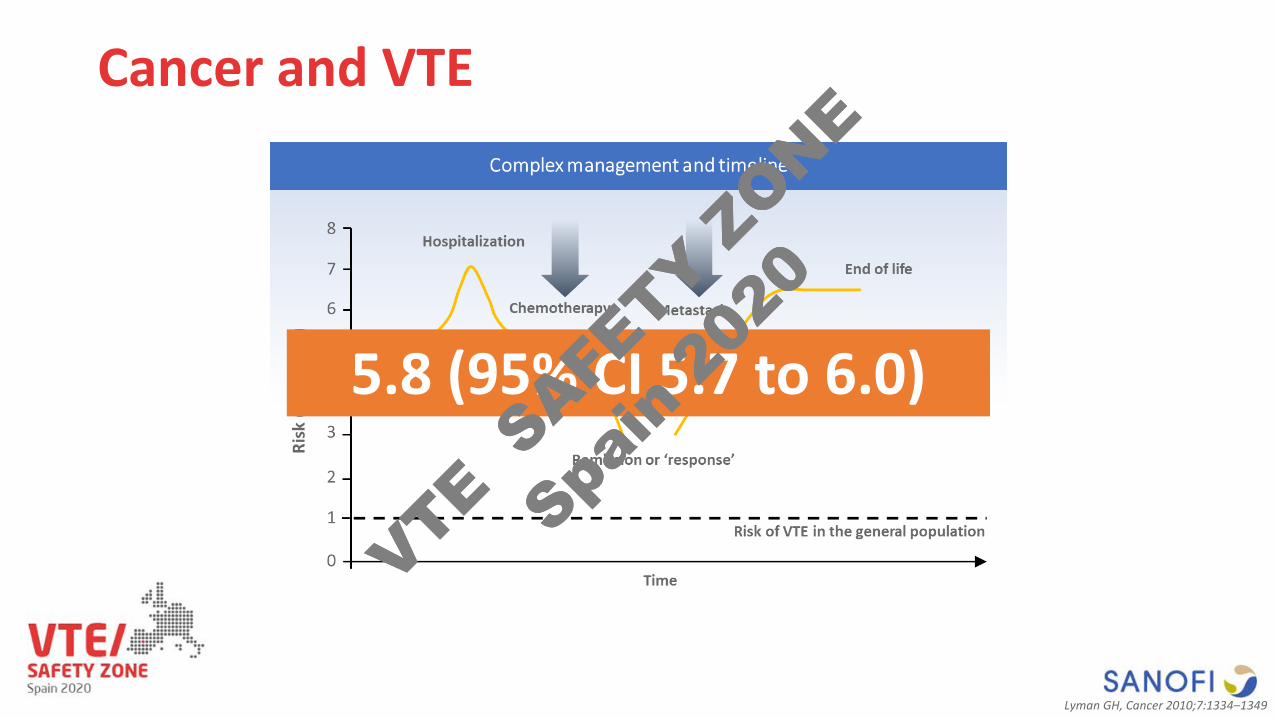
Cancer and VTE
5.8 (95% CI 5.7 to 6.0)
Lyman GH, Cancer 2010;7:1334–1349
VTE SAFE
TY ZONE
Spain
202
0
VTE SAFE
TY ZONE
Spain
202
0
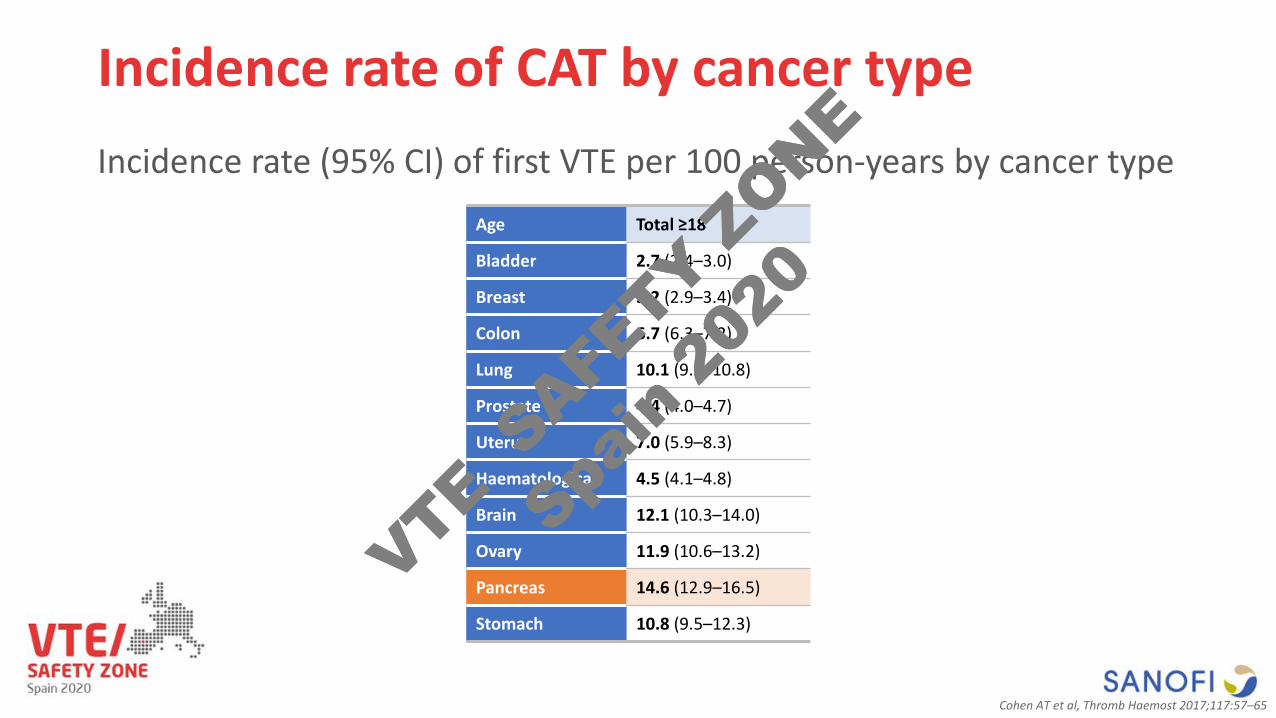
Incidence rate of CAT by cancer typeIncidence rate (95% CI) of first VTE per 100 person-years by cancer type
Age Total ≥18
Bladder 2.7 (2.4–3.0)
Breast 3.2 (2.9–3.4)
Colon 6.7 (6.3–7.2)
Lung 10.1 (9.5–10.8)
Prostate 4.4 (4.0–4.7)
Uterus 7.0 (5.9–8.3)
Haematological 4.5 (4.1–4.8)
Brain 12.1 (10.3–14.0)
Ovary 11.9 (10.6–13.2)
Pancreas 14.6 (12.9–16.5)
Stomach 10.8 (9.5–12.3)
Cohen AT et al, Thromb Haemost 2017;117:57–65
VTE SAFE
TY ZONE
Spain
202
0
VTE SAFE
TY ZONE
Spain
202
0
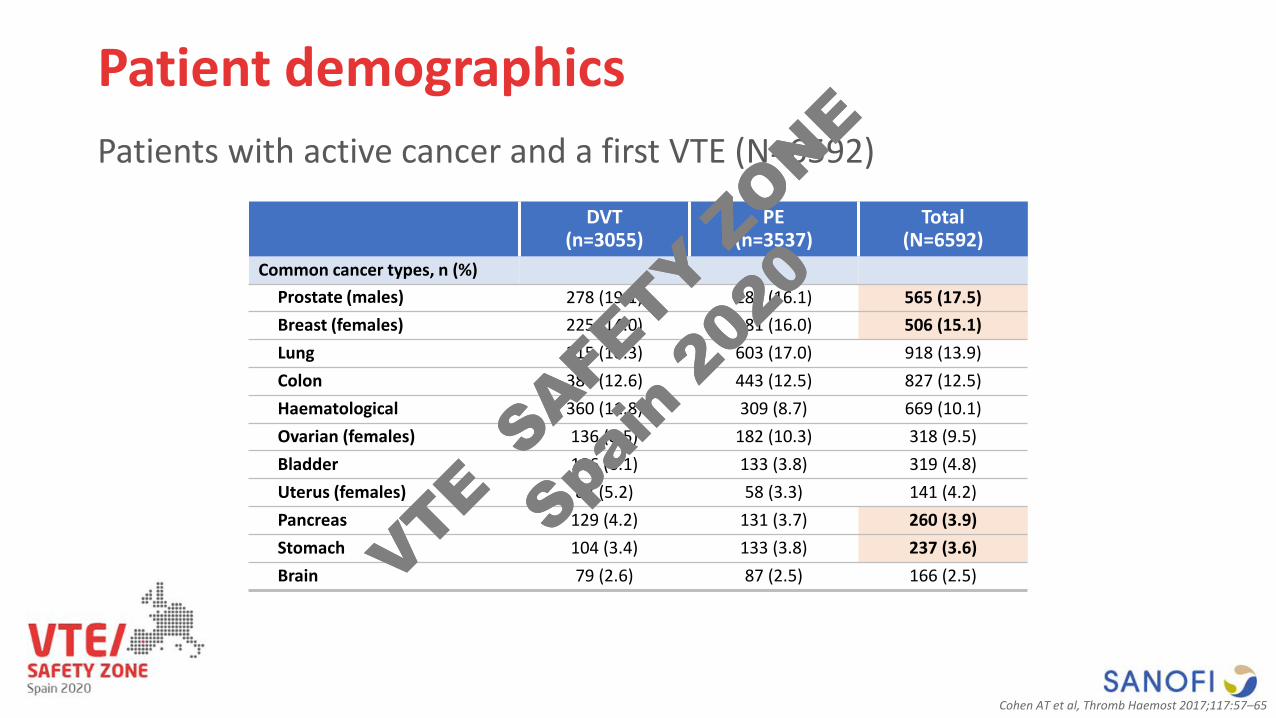
Patient demographicsPatients with active cancer and a first VTE (N=6592)
DVT (n=3055)
PE (n=3537)
Total (N=6592)
Common cancer types, n (%)Prostate (males) 278 (19.1) 287 (16.1) 565 (17.5)Breast (females) 225 (14.0) 281 (16.0) 506 (15.1)Lung 315 (10.3) 603 (17.0) 918 (13.9)Colon 384 (12.6) 443 (12.5) 827 (12.5)Haematological 360 (11.8) 309 (8.7) 669 (10.1)Ovarian (females) 136 (8.5) 182 (10.3) 318 (9.5)Bladder 186 (6.1) 133 (3.8) 319 (4.8)Uterus (females) 83 (5.2) 58 (3.3) 141 (4.2)Pancreas 129 (4.2) 131 (3.7) 260 (3.9)Stomach 104 (3.4) 133 (3.8) 237 (3.6)Brain 79 (2.6) 87 (2.5) 166 (2.5)
Cohen AT et al, Thromb Haemost 2017;117:57–65
VTE SAFE
TY ZONE
Spain
202
0
VTE SAFE
TY ZONE
Spain
202
0
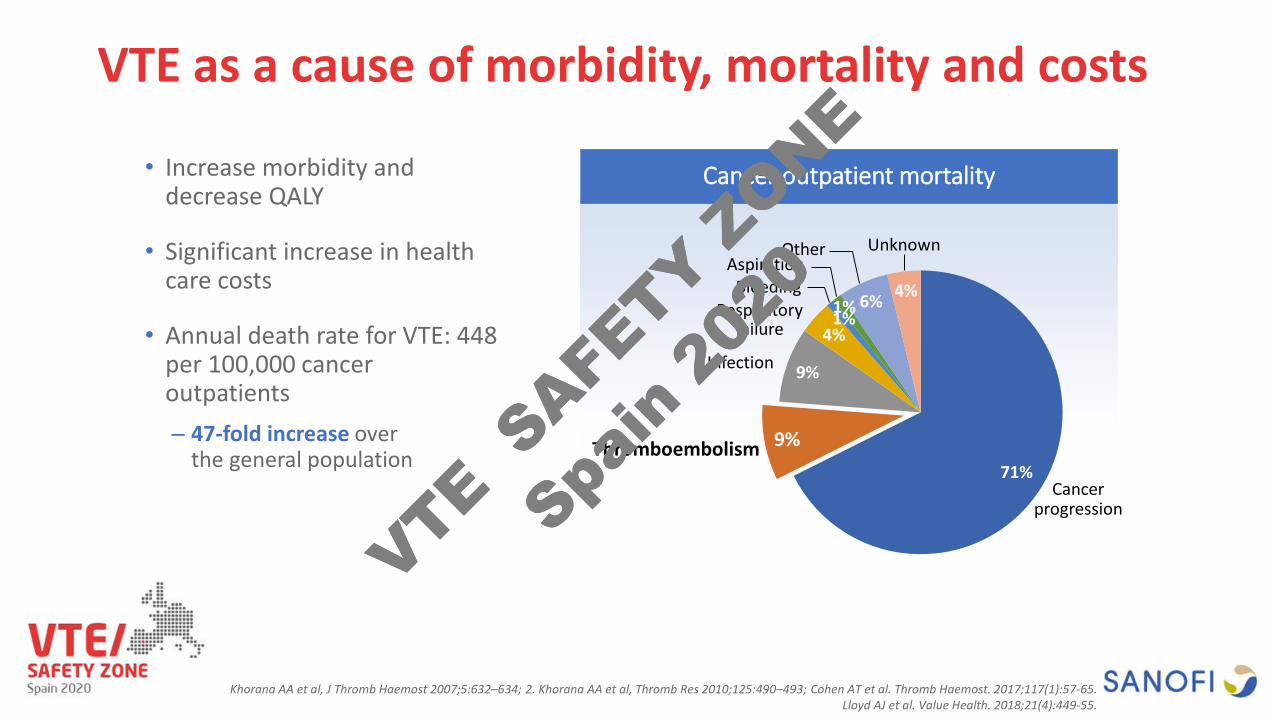
VTE as a cause of morbidity, mortality and costs
Cancer outpatient mortality
71%
9%
9%
4%1%1% 6% 4%
Cancer progression
Thromboembolism
Respiratory failure
BleedingAspiration
Other Unknown
Infection
• Increase morbidity and decrease QALY
• Significant increase in health care costs
• Annual death rate for VTE: 448 per 100,000 cancer outpatients– 47-fold increase over
the general population
Khorana AA et al, J Thromb Haemost 2007;5:632–634; 2. Khorana AA et al, Thromb Res 2010;125:490–493; Cohen AT et al. Thromb Haemost. 2017;117(1):57-65.Lloyd AJ et al. Value Health. 2018;21(4):449-55.
VTE SAFE
TY ZONE
Spain
202
0
VTE SAFE
TY ZONE
Spain
202
0
Assessment for risk of VTE in ambulatory cancer patients
VTE SAFE
TY ZONE
Spain
202
0
VTE SAFE
TY ZONE
Spain
202
0
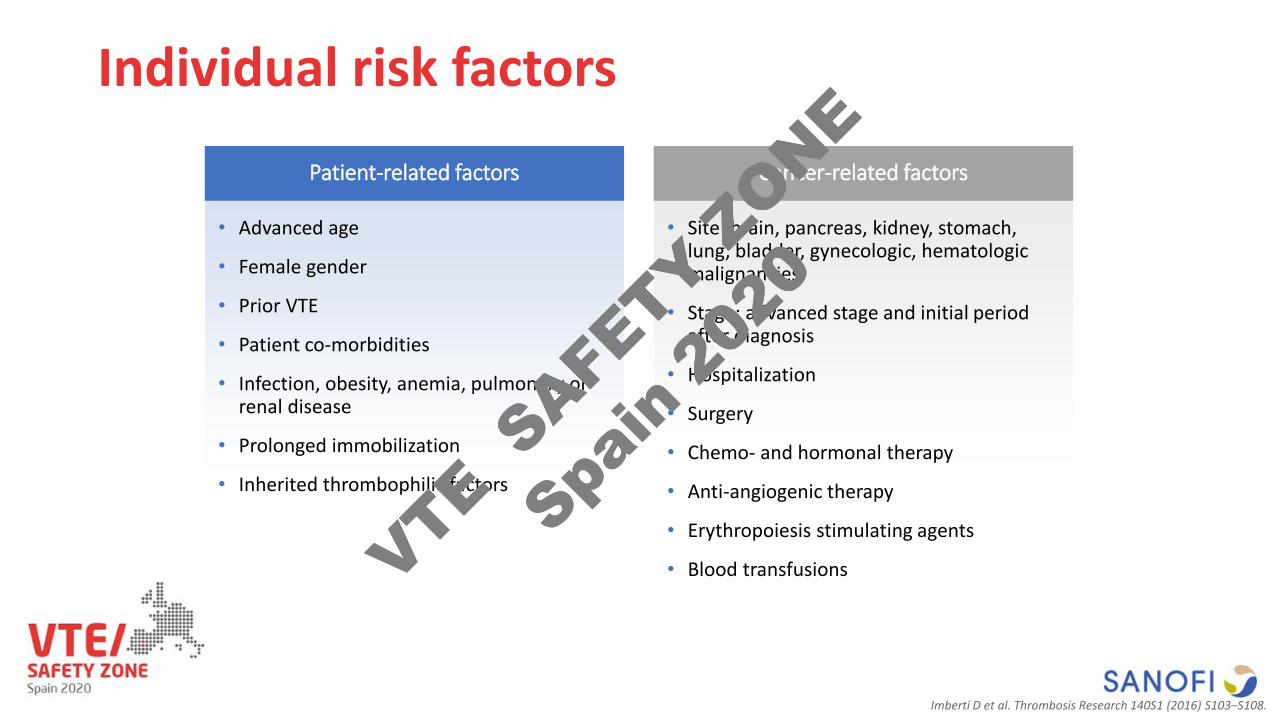
Individual risk factors
• Advanced age
• Female gender
• Prior VTE
• Patient co-morbidities
• Infection, obesity, anemia, pulmonary or renal disease
• Prolonged immobilization
• Inherited thrombophilic factors
• Site: brain, pancreas, kidney, stomach, lung, bladder, gynecologic, hematologic malignancies
• Stage: advanced stage and initial period after diagnosis
• Hospitalization
• Surgery
• Chemo- and hormonal therapy
• Anti-angiogenic therapy
• Erythropoiesis stimulating agents
• Blood transfusions
Patient-related factors Cancer-related factors
Imberti D et al. Thrombosis Research 140S1 (2016) S103–S108.
VTE SAFE
TY ZONE
Spain
202
0
VTE SAFE
TY ZONE
Spain
202
0
ASCO Guidelines
Individual risk factors, including biomarkers and
cancer site, do not reliably identify patients with
cancer at high risk of VTE. In the outpatient
setting, risk assessment can be conducted based
on a validated risk assessment tool.
Key N et al. J Clin Oncol. 2019 Aug 5:JCO1901461. [Epub ahead of print]
VTE SAFE
TY ZONE
Spain
202
0
VTE SAFE
TY ZONE
Spain
202
0
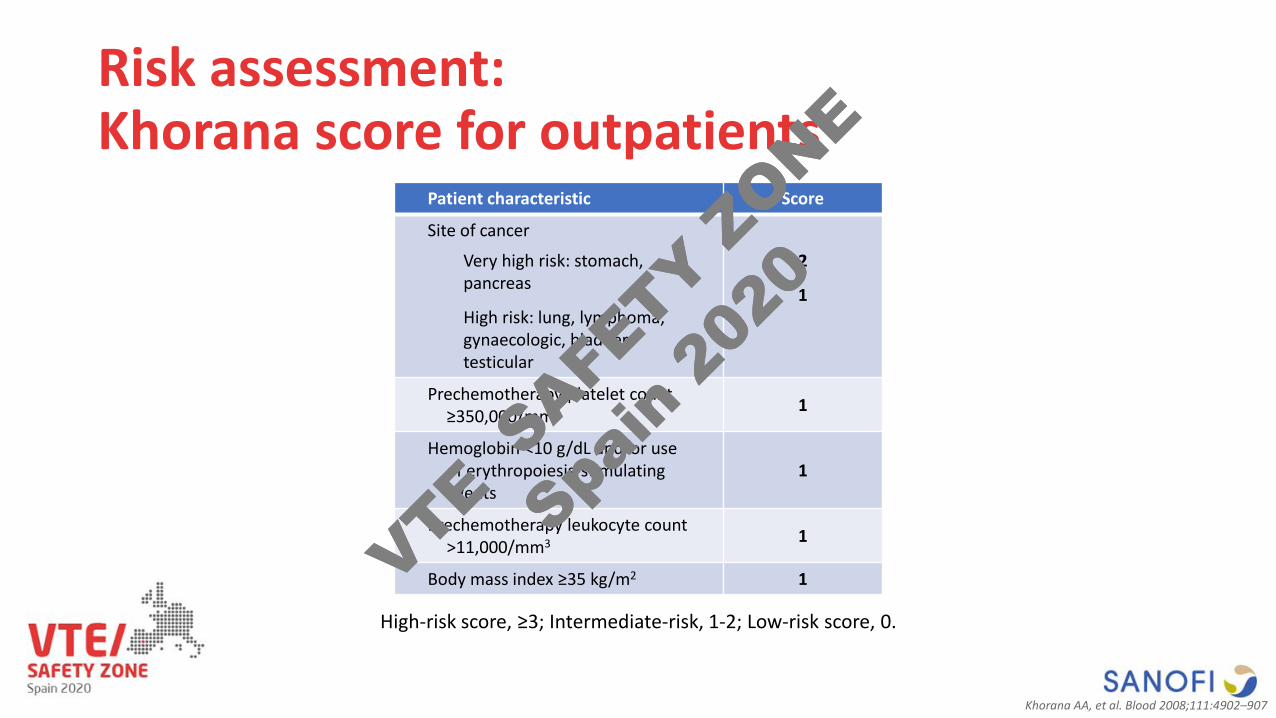
Risk assessment: Khorana score for outpatients
Patient characteristic Score
Site of cancer
Very high risk: stomach, pancreas
High risk: lung, lymphoma, gynaecologic, bladder, testicular
2
1
Prechemotherapy platelet count ≥350,000/mm3 1
Hemoglobin <10 g/dL and/or use of erythropoiesis-stimulating agents
1
Prechemotherapy leukocyte count >11,000/mm3 1
Body mass index ≥35 kg/m2 1
High-risk score, ≥3; Intermediate-risk, 1-2; Low-risk score, 0.
Khorana AA, et al. Blood 2008;111:4902–907
VTE SAFE
TY ZONE
Spain
202
0
VTE SAFE
TY ZONE
Spain
202
0
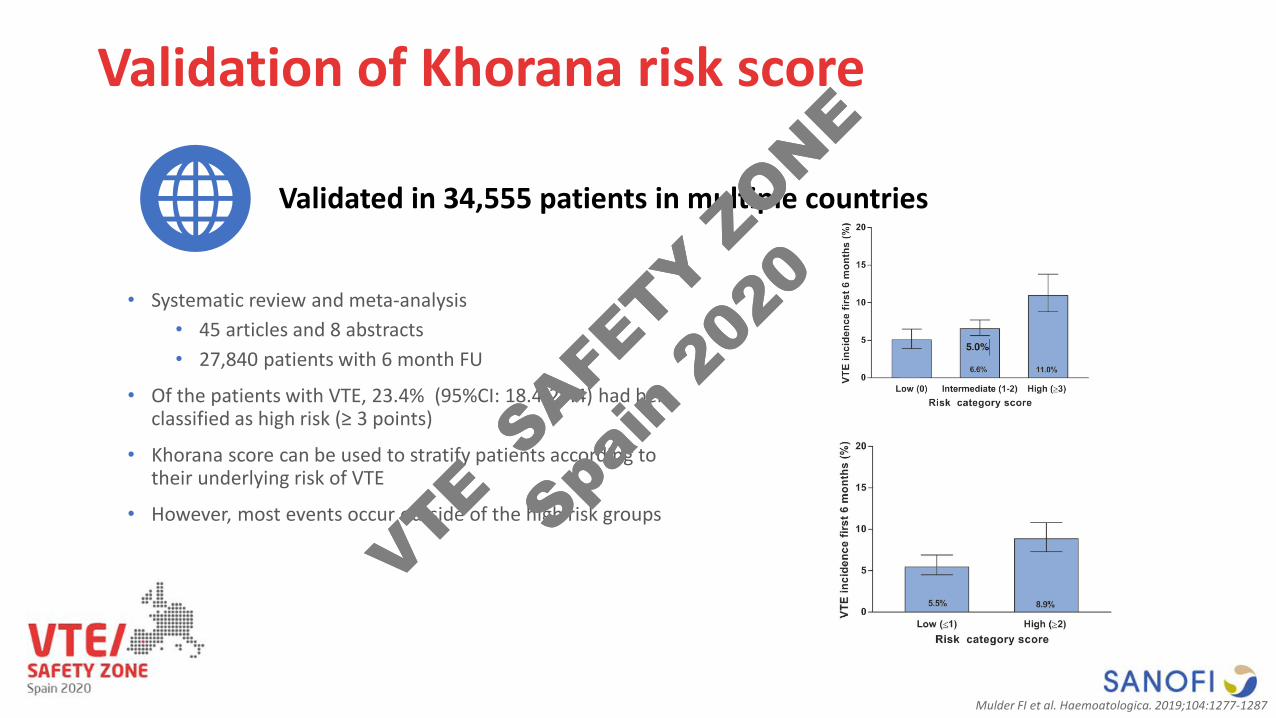
Validation of Khorana risk score
• Systematic review and meta-analysis• 45 articles and 8 abstracts• 27,840 patients with 6 month FU
• Of the patients with VTE, 23.4% (95%CI: 18.4-29.4) had ben classified as high risk (≥ 3 points)
• Khorana score can be used to stratify patients according to their underlying risk of VTE
• However, most events occur outside of the high risk groups
Validated in 34,555 patients in multiple countries
Mulder FI et al. Haemoatologica. 2019;104:1277-1287
VTE SAFE
TY ZONE
Spain
202
0
VTE SAFE
TY ZONE
Spain
202
0
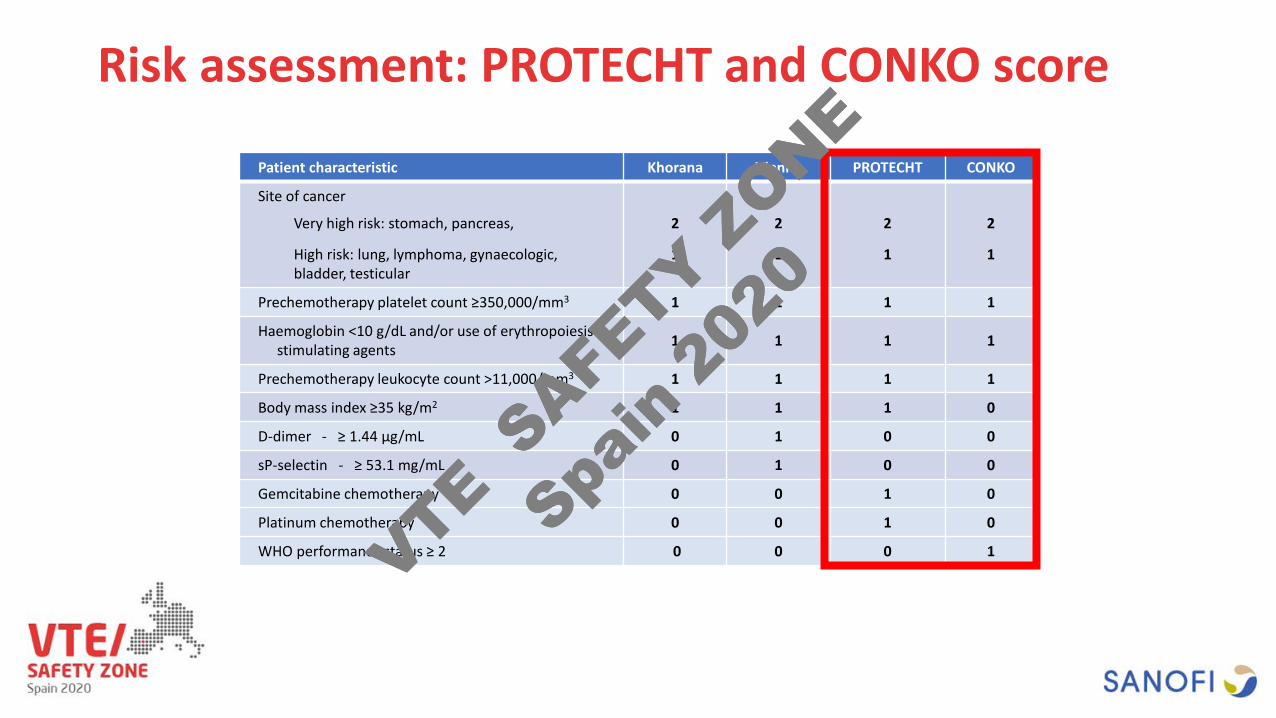
Risk assessment: PROTECHT and CONKO score
Patient characteristic Khorana Vienna PROTECHT CONKO
Site of cancer
Very high risk: stomach, pancreas,
High risk: lung, lymphoma, gynaecologic, bladder, testicular
2
1
2
1
2
1
2
1
Prechemotherapy platelet count ≥350,000/mm3 1 1 1 1
Haemoglobin <10 g/dL and/or use of erythropoiesis-stimulating agents 1 1 1 1
Prechemotherapy leukocyte count >11,000/mm3 1 1 1 1
Body mass index ≥35 kg/m2 1 1 1 0
D-dimer - ≥ 1.44 µg/mL 0 1 0 0
sP-selectin - ≥ 53.1 mg/mL 0 1 0 0
Gemcitabine chemotherapy 0 0 1 0
Platinum chemotherapy 0 0 1 0
WHO performance status ≥ 2 0 0 0 1VTE SAFE
TY ZONE
Spain
202
0
VTE SAFE
TY ZONE
Spain
202
0
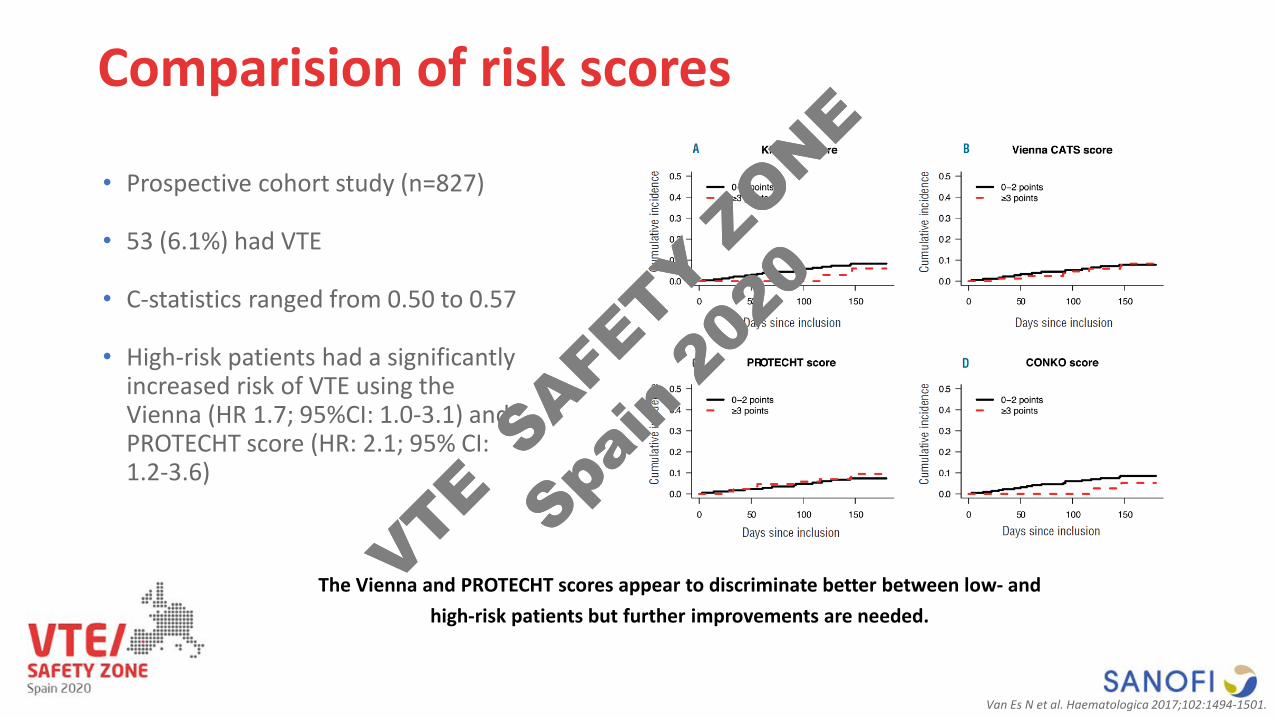
Comparision of risk scores
• Prospective cohort study (n=827)
• 53 (6.1%) had VTE
• C-statistics ranged from 0.50 to 0.57
• High-risk patients had a significantly increased risk of VTE using the Vienna (HR 1.7; 95%CI: 1.0-3.1) and PROTECHT score (HR: 2.1; 95% CI: 1.2-3.6)
Van Es N et al. Haematologica 2017;102:1494-1501.
The Vienna and PROTECHT scores appear to discriminate better between low- andhigh-risk patients but further improvements are needed.
VTE SAFE
TY ZONE
Spain
202
0
VTE SAFE
TY ZONE
Spain
202
0

Can we do better?
VTE SAFE
TY ZONE
Spain
202
0
VTE SAFE
TY ZONE
Spain
202
0
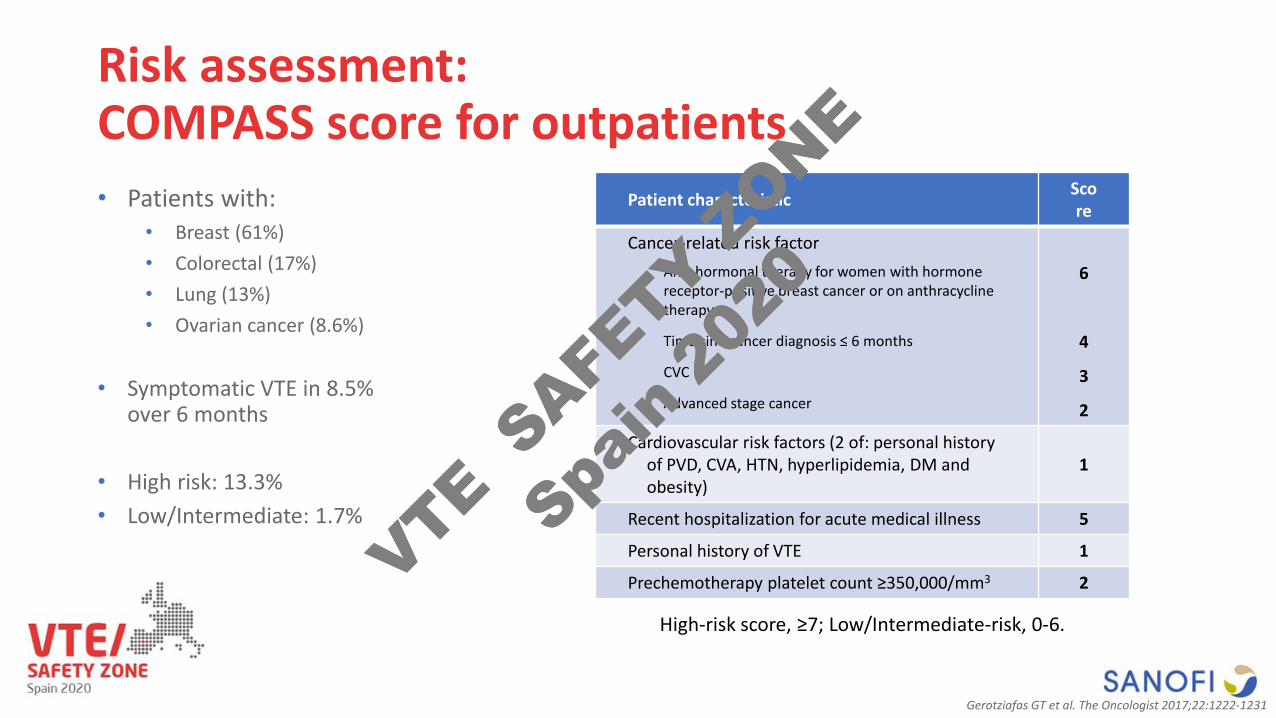
Risk assessment: COMPASS score for outpatients
Patient characteristic Score
Cancer-related risk factorAnti-hormonal therapy for women with hormone receptor-positive breast cancer or on anthracycline therapy
Time sine cancer diagnosis ≤ 6 months
CVC
Advanced stage cancer
6
4
3
2
Cardiovascular risk factors (2 of: personal history of PVD, CVA, HTN, hyperlipidemia, DM and obesity)
1
Recent hospitalization for acute medical illness 5
Personal history of VTE 1
Prechemotherapy platelet count ≥350,000/mm3 2
High-risk score, ≥7; Low/Intermediate-risk, 0-6.
• Patients with:• Breast (61%)• Colorectal (17%)• Lung (13%)• Ovarian cancer (8.6%)
• Symptomatic VTE in 8.5% over 6 months
• High risk: 13.3%• Low/Intermediate: 1.7%
Gerotziafas GT et al. The Oncologist 2017;22:1222-1231
VTE SAFE
TY ZONE
Spain
202
0
VTE SAFE
TY ZONE
Spain
202
0
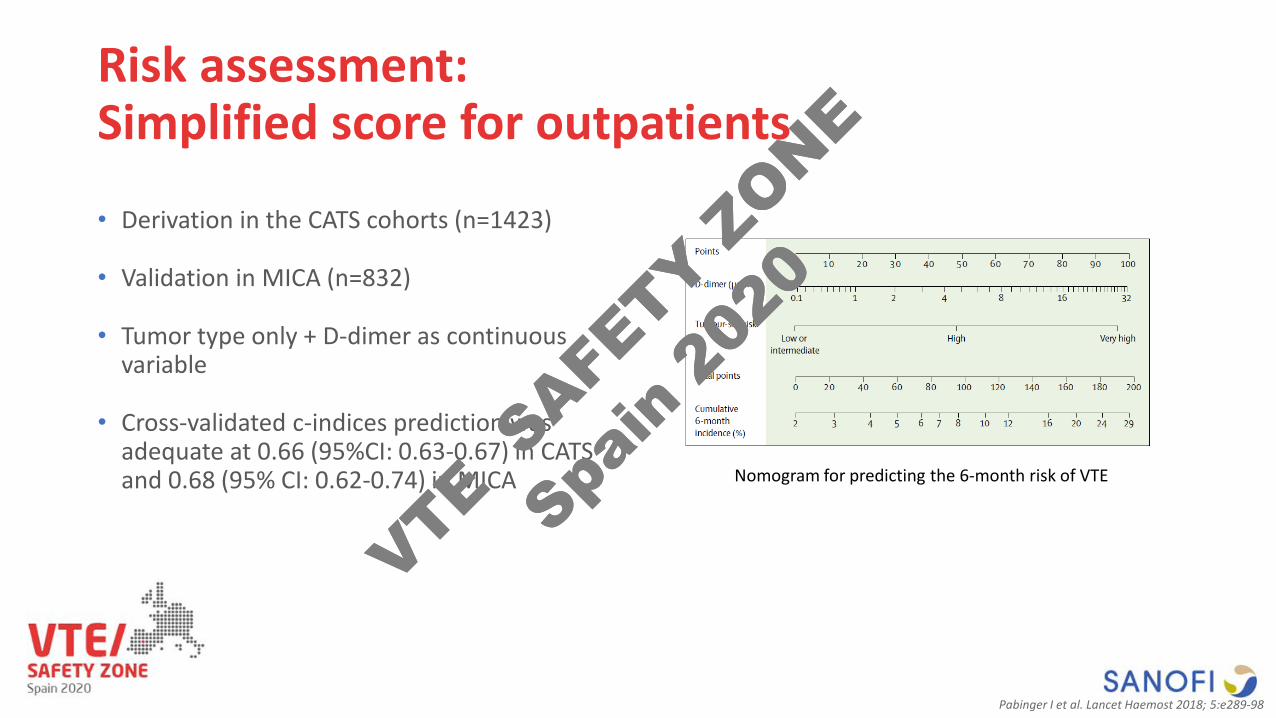
Risk assessment: Simplified score for outpatients
• Derivation in the CATS cohorts (n=1423)
• Validation in MICA (n=832)
• Tumor type only + D-dimer as continuous variable
• Cross-validated c-indices prediction was adequate at 0.66 (95%CI: 0.63-0.67) in CATS and 0.68 (95% CI: 0.62-0.74) in MICA Nomogram for predicting the 6-month risk of VTE
Pabinger I et al. Lancet Haemost 2018; 5:e289-98
VTE SAFE
TY ZONE
Spain
202
0
VTE SAFE
TY ZONE
Spain
202
0
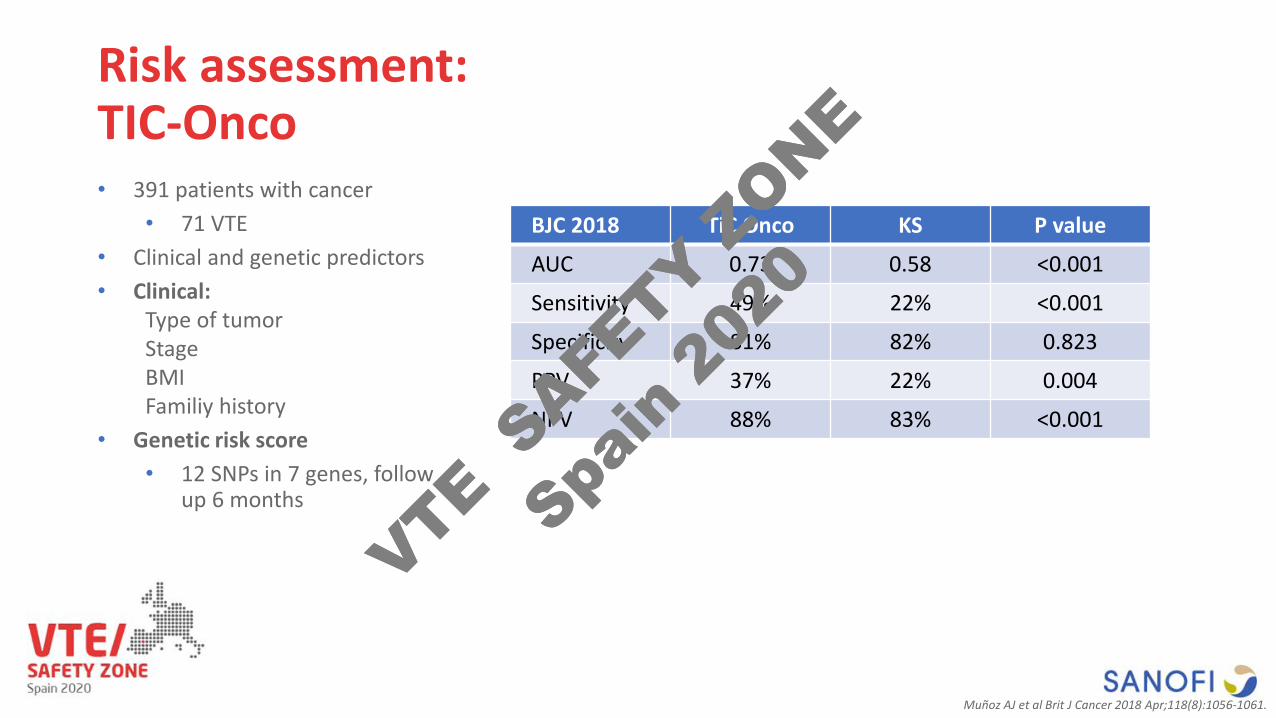
Risk assessment: TIC-Onco
BJC 2018 TiC Onco KS P value
AUC 0.73 0.58 <0.001
Sensitivity 49% 22% <0.001
Specificity 81% 82% 0.823
PPV 37% 22% 0.004
NPV 88% 83% <0.001
• 391 patients with cancer• 71 VTE
• Clinical and genetic predictors• Clinical:
Type of tumorStageBMIFamiliy history
• Genetic risk score• 12 SNPs in 7 genes, follow
up 6 months
Muñoz AJ et al Brit J Cancer 2018 Apr;118(8):1056-1061.
VTE SAFE
TY ZONE
Spain
202
0
VTE SAFE
TY ZONE
Spain
202
0
Can risk stratification help in real life?
VTE SAFE
TY ZONE
Spain
202
0
VTE SAFE
TY ZONE
Spain
202
0
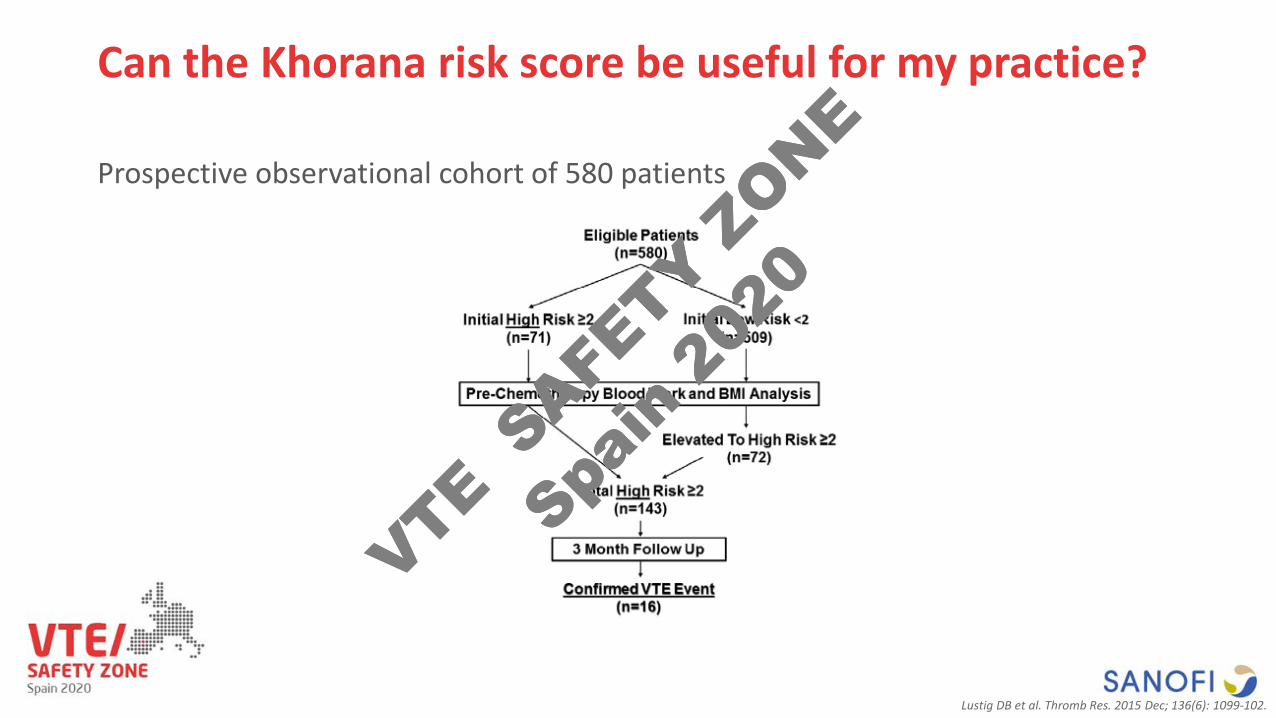
Can the Khorana risk score be useful for my practice?
Prospective observational cohort of 580 patients
Lustig DB et al. Thromb Res. 2015 Dec; 136(6): 1099-102.
VTE SAFE
TY ZONE
Spain
202
0
VTE SAFE
TY ZONE
Spain
202
0
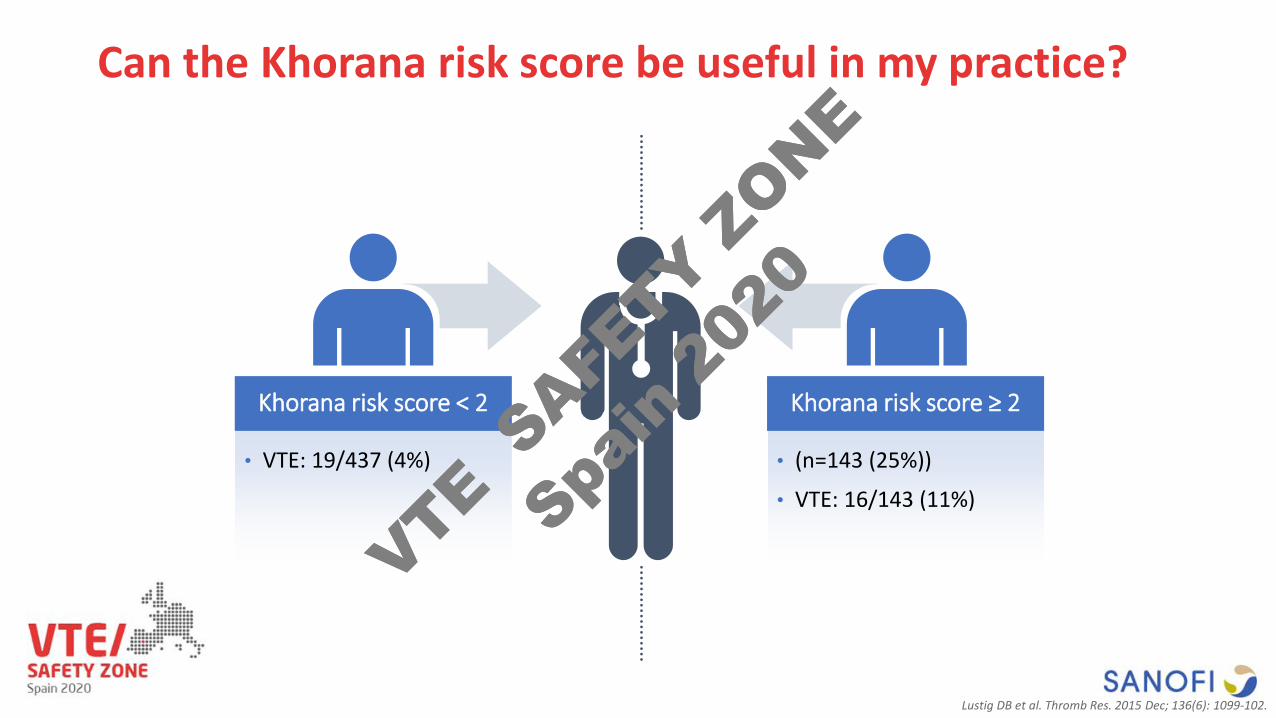
Can the Khorana risk score be useful in my practice?
• VTE: 19/437 (4%)
Khorana risk score < 2
• (n=143 (25%))
• VTE: 16/143 (11%)
Khorana risk score ≥ 2
Lustig DB et al. Thromb Res. 2015 Dec; 136(6): 1099-102.
VTE SAFE
TY ZONE
Spain
202
0
VTE SAFE
TY ZONE
Spain
202
0
Conclusions
VTE is a frequent and important complication of ambulatory cancer patients receiving chemotherapy
Different Risk Assessment Models can identified patients with high thrombotic rates
Findings should inform future studies to derived better or simpler Risk Assessment Models to inform clinicians about the underlying risk of VTE and help recommendations regarding the potential use of thromboprophylaxis for higher-risk ambulatory cancer patients
VTE SAFE
TY ZONE
Spain
202
0
VTE SAFE
TY ZONE
Spain
202
0

Thank you!
VTE SAFE
TY ZONE
Spain
202
0
VTE SAFE
TY ZONE
Spain
202
0
Recommended