-
7/27/2019 Santa Clara County Emergency Medical Services Agency
Semi-Annual Report (2012 May)
1/26
Santa Clara County Emergency Medical
Services Agency
Semi-AnnualReport
M a y 2 0 1 2
-
7/27/2019 Santa Clara County Emergency Medical Services Agency
Semi-Annual Report (2012 May)
2/26
2
Santa Clara County EMS Agency May 2012 Report to the Hospitals
and Health Committee
-
7/27/2019 Santa Clara County Emergency Medical Services Agency
Semi-Annual Report (2012 May)
3/26
3
Santa Clara County EMS Agency May 2012 Report to the Hospitals
and Health Committee
Table of Contents
Table of Contents
...................................................................................................................................
3
EMS Agency Activities
..........................................................................................................................
4
Start of Rural Metro as New County Ambulance Provider
.......................................................................
4
Evaluation of the Impact on Inebriates on the EMS System
....................................................................
5
Strategic Assessment and Strategic Planning Process
..............................................................................
6
Receiving Hospital Contracts
....................................................................................................................
6
EMS Trust Fund
.........................................................................................................................................
6
EMS Agency Fee Schedule
........................................................................................................................
8
EMS System Descriptive Statistics
.................................................................................................
10
Prehospital Clinical Care and Quality Improvement
..............................................................
11
911 Ambulance Response Times
............................................................................................................
11
Santa Clara County EOA Response Subzones and City Boundaries
........................................................ 14
Mutual Aid Provided by County 911 Ambulance
....................................................................................
15
Fire Department First Responder Response Times
................................................................................
16
Air Ambulance Transports
......................................................................................................................
18
Hospital and Specialty Care Facilities
..........................................................................................
19
Hospital Volume and
Destinations..........................................................................................................
19
Hospital Diversion
...................................................................................................................................
20
Trauma Care System
...............................................................................................................................
21
Stroke Care System
.................................................................................................................................
23
Cardiac Care (STEMI) System
..................................................................................................................
24
-
7/27/2019 Santa Clara County Emergency Medical Services Agency
Semi-Annual Report (2012 May)
4/26
4
Santa Clara County EMS Agency May 2012 Report to the Hospitals
and Health Committee
EMS Agency ActivitiesStart of Rural Metro as New County
Ambulance Provider
The period of July 1, 2011 through December 31, 2011 was marked
by dynamic change for the Santa
Clara County EMS Agency and the EMS System. On July 1, 2011, the
most significant change in 30 years
of EMS in Santa Clara County occurred, as Rural Metro became the
Countys exclusive 911 ambulanceprovider, taking over from American
Medical Response.
The exclusive 911 ambulance contract between Santa Clara County
and Rural Metro is widely regarded
as the most comprehensive and progressive EMS contract in the
State, and the personnel of the Chief
Executives Office, County Counsels Office, the Department of
Public Health, and the EMS Agency
should be commended for outstanding performance in the
development and execution of this contract.
Under the new contract,
ambulances are arriving on
scene of emergency and
non-emergency calls quickerthan before July 1. Except for
minor challenges during the
first two weeks of the contract implementation, Rural Metro has
met response time standards for
emergency and non-emergency calls in all zones and in aggregate.
The EMS Agency is working closely
with County Communications and Rural Metro to fine tune
ambulance deployment and dispatch
performance to further improve system efficiency.
In addition to faster response times, the EMS System presents
other significant improvements:
Improved medical support to law enforcement and fire services
across the county. Rural Metrowill provide at no cost, standby
ambulances and supervisors for critical public safety events,
such as large fires, and police SWAT operations.
Increased disaster response capability, including the ability to
dispatch a strike team of fiveambulances and a field supervisor in
less than 8 minutes of receiving a request.
Improved field supervision, coordination, and training through
24/7 staffing of EMS Duty Chiefs.
Improved public information and community education
programs.
Implementing a comprehensive electronic data system. This system
will provide criticalinformation about system clinical care,
operational efficiency, and cost effectiveness. When
completed, all EMS System providers, including communications
centers, fire and ambulance
providers, and hospitals will contribute data. This will allow
the EMS System to make evidence-
based decisions and better evaluate the medical care we provide.
Santa Clara County will be the
largest EMS System in the nation to have this level and
sophistication of data integration.
More detailed information, including Rural Metros response time
performance statistics, is provided on
pages 11 through 14.
-
7/27/2019 Santa Clara County Emergency Medical Services Agency
Semi-Annual Report (2012 May)
5/26
5
Santa Clara County EMS Agency May 2012 Report to the Hospitals
and Health Committee
Valley Medical Center 472
Regional Medical Center of San Jose 368
Kaiser San Jose 94
El Camino Hospital of Mt View 88
Kaiser Santa Clara 81
O'Connor Hospital 67
Good Samaritan Hospital 60
St. Louise Hospital 46
O'Connor Hospital 37
Palo Alto Veterans Admin Hospital 19
Stanford University Hospital 18
El Camino Hospital of Los Gatos 8
In the following pages, three of the EMS Agencys strategic
projects are highlighted. These projects
include the evaluation of the Impact of Inebriates on the EMS
System, the EMS System Strategic
Assessment and Planning Process, entering into contracts with
hospitals to receive ambulance patients.
Additional information is provided regarding expenditures from
the EMS Trust Fund and the EMS
Agencys fee schedule.
Evaluation of the Impact on Inebriates on the EMS System
At the direction of Public Health Administration, the EMS Agency
began evaluating the need and
feasibility of establishing an inebriate care system. The
impetus for this evaluation was numerous
comments from stakeholders identifying a large volume of
inebriate patients intensively using EMS and
hospital services. The core group of stakeholders involved in
the analysis included the Public Health
Department, Valley Medical Center, Valley Homeless Health
Program, the Mental Health Department,
Department of Alcohol and Drug Services, Jail Health Services,
Destination Home, and the EMS Agency.
This group identified four short-term objectives: 1) Quantify
the volume of chronic inebriate
EMS transports and emergency department visits; 2) Estimate
costs associated with these events; 3)
Determine the safety and efficacy of various types inebriate
centers; and, 4) Identify other organizationsthat should be
involved in inebriate system planning.
The preliminary analysis identified:
Between July 1, 2011 and December 31, 2011, Rural Metro had
1,453 transports of patients whoappeared to be only or primarily
inebriated. This equates to 2,906 transports annually.
Inebriated patients' ages ranged from 13 to 110. Twenty-four
percent of the patients werefemale, 76 percent of the patients were
male. For both females and males, the most frequently
occurring age ranges were 40 to 49 and 50 to 59.
The top ten patients were transported 154 times during this six
month period.
Many of the highest-frequency users were transported to multiple
hospitals. The mostfrequently transported patient was transported
to 8 different hospitals. Many of the top ten
highest frequency inebriated patients was transported to four or
more hospitals during the six-
month period.
The patient who was transported mostfrequently was transported
38 times during this
6-month period. This equates to one and one-
half ambulance transports for inebriation per
week.
All of the top ten patients in this data analysis
were homeless and uninsured. In fact, themajority of frequent
use patients (3 times or
more per year) were homeless.
The EMS System and hospitals within Santa ClaraCounty were
impacted by the volume of
inebriate transports. The number of destination-
identified transports is shown on the right:
-
7/27/2019 Santa Clara County Emergency Medical Services Agency
Semi-Annual Report (2012 May)
6/26
6
Santa Clara County EMS Agency May 2012 Report to the Hospitals
and Health Committee
Additional stakeholders have joined the planning process. These
stakeholders include the Sheriffs
Office, municipal law enforcement, hospitals, and Rural Metro
Ambulance. The group is committed to
identifying a system that provides safe, respectful, clinically
appropriate treatment of inebriates;
including pathways to comprehensive wrap around mental health,
social, and other supportive services,
while reducing the operational and economic impact on EMS,
hospitals, and criminal justice systems.
Strategic Assessment and Strategic Planning Process
During the summer of 2012, the EMS Agency will conduct a
strategic assessment of the Santa Clara
County EMS System. This assessment will evaluate the
opportunities and threats facing the EMS System,
from national, regional, and local influences. The assessment
will consider those threats and
opportunities in the context of the strengths and weaknesses of
the EMS System, and emphasize a 3 to
7 year horizon, focusing on maintaining or improving clinical
care, improving operational efficiency,
assuring cost effectiveness, and the financial solvency of the
EMS System. Following the strategic
assessment, the EMS Agency will lead the development of an EMS
System Strategic Plan, based upon a 3
to 7 year timeframe. The desired output of this planning process
is a high-level plan that identifies the
EMS Systems Mission, Vision, Values, Goals, and Objectives. The
strategic plan will be an essential inputto future changes to the
EMS System.
To date we have developed and released the Request for Proposal
(RFP) to engage a professional
consulting firm, who will lead the strategic assessment and
planning process. The scope of work portion
of the RFP was provided to EMS System Stakeholders for comments,
and the EMS Committee reviewed
and approved the RFP scope of work at their March 1, 2012
meeting.
The consulting firm will begin their work near the anticipated
release of the US Supreme Courts
decision on the Patient Protection and Affordable Care Act,
because that decision will materially impact
the financing and provision of medical care, including emergency
medical services, throughout the
nation.
Receiving Hospital Contracts
The EMS Agency entered into new contracts with eleven
ambulance-receiving hospitals within Santa
Clara County. Through this agreement, hospitals agreed to comply
with applicable EMS Agency policies
and procedures, to provide patient care data for analysis, and
to participate in the EMS System Quality
Improvement Program. During development of the agreement, the
EMS Agency and the hospitals
agreed to create a master hospital agreement, and have specific
annexes for receiving facility, trauma
center, stroke center, and cardiac center services. This new
contract structure and increasing the
contract renewal period to five years was well received by
hospital executives, and will save the County
and hospitals significant time and resources.
EMS Trust Fund
The EMS Agency provided the detailed financial report to the
Health and Hospitals Committee on the
EMS Trust Fund at its February 15, 2012. This EMS Trust Fund
summary discusses how the expenditures
from the EMS Trust Fund improve EMS within Santa Clara
County.
-
7/27/2019 Santa Clara County Emergency Medical Services Agency
Semi-Annual Report (2012 May)
7/26
7
Santa Clara County EMS Agency May 2012 Report to the Hospitals
and Health Committee
Category A: Reserve
At the Board of Supervisors direction, starting in Fiscal Year
2011-2012, a reserve category was
established in the EMS Trust Fund. This amount, which is at
least 20% of the EMS Trust Fund, will be
placed into reserve and used only for significant strategic
projects that benefit the EMS System with a
long range focus. These funds could also be used should the EMS
System experience an unanticipated
financial burden, such as the failure of an ambulance provider
or an extraordinary increase of cost ofservice or supplies, or a
material decrease in system-wide third-party payor reimbursement.
During the
2012 Fiscal Year, $342,000 of the EMS Trust was placed into
reserve.
Category B: Training, Education, and Recognition
Allocations were approved to produce a public service
announcement video that informs those in Santa
Clara County when to call an ambulance and what to expect when
an ambulance is called. This multi-
lingual video will be made available in numerous formats.
Additionally, the EMS Agency is providing a
series of courses to EMS System stakeholders to improve their
response to mass casualty incidents and
to better understand the use of data and statistical processes
to evaluate quality of care and operational
effectiveness. This training is critical to the strategic goal
of basing EMS System decisions on data and
evidence. In May, the EMS Agency will host its annual conference
and recognize outstanding EMSSystem participants from medical
dispatch centers, hospital emergency departments, field EMTs
and
Paramedics, and members of the public. During the 2012 Fiscal
Year, $150,000 was allocated to training,
education, and recognition.
Category C: Benefit to EMS System Stakeholders
Funds were allocated from this category to assist EMS System
Stakeholders with one-time or short-term
needs. During Fiscal Year 2012, funds were allocated to the fire
departments within Santa Clara County
to establish computer aided dispatch links to the response time
performance software package and to
provide minimal funding for hardware associated with the County
EMS System Data Project. This
allocation was essential to creating a comprehensive EMS System
data collection and analysis capability.
Funds were also allocated to the EMS Section of the Santa Clara
County Fire Chiefs Association to hire a
contractor to develop an Employee Communicable Disease Exposure
Plan and reporting system. This
plan and reporting system will be offered to all fire
departments, law enforcement agencies, and
ambulance agencies within Santa Clara County. A common plan and
reporting format among all
providers reduces the possibility that an exposed employee will
not receive timely exposure
investigation and treatment.
Funding was also allocated to Santa Clara County Communications
to enhance their use of Emergency
Medical Dispatch pre-arrival instructions and to install
additional MARVLIS display terminals in County
Communications. MARVLIS is an ambulance deployment program,
which suggests to the dispatcher
where ambulances should be placed to minimize response times.
During the 2012 Fiscal Year, $108,000was allocated to short term
and one time projects that benefit EMS System Stakeholders.
Category D (Strategic Initiatives)
Projects in this category emphasize the development of
initiatives that strategically advance the Santa
Clara EMS System, often in the longer term. Funds were allocated
to conduct a strategic assessment and
-
7/27/2019 Santa Clara County Emergency Medical Services Agency
Semi-Annual Report (2012 May)
8/26
8
Santa Clara County EMS Agency May 2012 Report to the Hospitals
and Health Committee
to pay for costs in developing the EMS S Data System. Details on
the strategic assessment and strategic
planning process are provided on page 6. During Fiscal Year
2012, $250,000 was allocated to strategic
projects.
EMS Agency Fee Schedule
The EMS Agency relies on its service fees for funding
operations. Effective July 1, 2011, the Board ofSupervisors
authorized fee increases to offset the increased cost of providing
EMS planning, regulation,
oversight, and quality improvement services. Fee increases were
authorized for ambulance and air
ambulance companies, and to permit the individual vehicles
operated by these companies. Additionally,
a new fee was instituted for all hospitals that receive
ambulance patients, and fees for specialty services,
such as Trauma Centers, Stroke Centers, and Cardiac Centers,
were increased to reflect the increasing
costs of system-wide planning, analysis, and quality
improvement. The authorized changes are
indicated in the following charts and the complete EMS Agency
Fee Schedule is on the following page.
Private Ambulance Permit Fees
Description FY11 FY12
Basic Life Support Ambulance Service (8) 5,000.00 5,500.00
Advanced Life Support Ambulance Service (4) 5,000.00
6,000.00
Critical Care Transport Ambulance Service (4) 5,000.00
6,000.00
Air Ambulance Service Permit (3) 5,000.00 8,000.00
Per Unit/Resource Permit (150 est) 800.00 950.00
EMS Receiving Facility Fees
Description FY11 FY12
911 Paramedic Receiving Facility (10) NEW 0 10,000.00
EMS Stroke Receiving Facility (9) 8,000.00 10,000.00
EMS Cardiac Receiving Facility (8) 8,000.00 10,000.00
EMS Trauma Receiving Facility (3) 75,000.00 100,000.00
-
7/27/2019 Santa Clara County Emergency Medical Services Agency
Semi-Annual Report (2012 May)
9/26
9
Santa Clara County EMS Agency May 2012 Report to the Hospitals
and Health Committee
2011 - 2012 EMS Agency Fee Schedule
ITEM/SERVICE FEE
INDIVIDUAL FEES
EMT-Basic Certification $50
EMT Basic Re-Certification (biennial) $50
EMT-P Local Accreditation $150
Identification Card $20
Replacement ID Card (certification, accreditation, system ID)
$20
Photocopying $4.75 (1st page)
$.10/ea. Addl.
CORPORATE FEES
Ambulance Service Permits (annual fee)Basic Life Support
$5,500
Advanced Life Support $6,000
Critical Care Transfer $6,000
Air Service $8,000
Ambulance Vehicle Permits (annual fee)
Basic Life Support $950
Advanced Life Support $950
Critical Care Transfer $950
Air Unit $950
Non-Transport BLS/ALS Unit (Quick Response) $800
Education Program Certification (every 4 years)
EMT Program $1,000
Paramedic Program $5,000
Pre-Hospital Continuing Education $1,000
Specialty Care Designation (annual fee)
Trauma Center Designation $100,000
Stroke Center Designation $10,000
STEMI Receiving Center Designation $10,000
911 Receiving Center Designation $10,000
-
7/27/2019 Santa Clara County Emergency Medical Services Agency
Semi-Annual Report (2012 May)
10/26
10
Santa Clara County EMS Agency May 2012 Report to the Hospitals
and Health Committee
EMS System Descriptive StatisticsListed below are statistics
that describe the characteristics of the Santa Clara County EMS
during
calendar year 2011.
The County of Santa Clara
DaytimePopulation
2.2 mil
ResidentPopulation
1.8 mil
GeographicSize
1,132 sq. mi.
GeographicDes.
2/3 rural
Municipalities 15
911 System Call Volume
Calendar Year 2011
TotalResponses
76,163
GroundAmbulanceTransports
69,508
EMS AircraftResponse
192
EMS AircraftTransports
110
CalendarYear 2010Total
Responses95,092
Ground
Ambulance
Transports
64,507
EMS Aircraft
Response176
EMS Aircraft
Transports103
Interfacility Transports
Ground Ambulance
(2011)22,627
Ground Ambulance
(2010)44,839
Ground Ambulance
(2009)39,603
Patients at Specialty Centers
Stroke Patients 2,642
Trauma Patients 7,619
STEMI Patients 423
Pre-hospital Care Provider
Agencies
Fire Departments 11
Ground AmbulanceServices
10
Air AmbulanceServices
3
Pre-hospital Care Personnel
Emergency MedicalTechnicians
3019
Paramedics 744
Mobile IntensiveCare Nurses
35
Accredited EMS FieldSupervisors
21
Permitted EMS Assets
Fire Apparatus 159
Private GroundAmbulances
*162
Private AirAmbulances
4
Private EMS Non-Transport Units
11
*26 additional ambulance arebeing added to the system
Communications Centers
Public Safety AnsweringPoints (PSAPs)
13
Secondary PSAPs 3
Private AmbulanceDispatch Centers
9
Air Ambulance DispatchCenters
3
Acute Care Facilities
Acute Care
Hospitals12
Emergency
Departments11
Level 1 Trauma
Centers2
Level 2 Trauma
Centers1
Base Hospitals 1
Burn Centers 1
Stroke Centers 9
STEMI Centers 8
County Managed Medical-
Health Resources
Field Treatment
Site Trailers9
Specialty Service
Trailers4
Electronic Patient
Tracking Systems0
Chem-Packs 8Medical-Health
Operations Center1
EMS Radio Caches 6
Disaster Medical
Support Unit1
Training Programs
Emergency Medical
Technician6
Paramedic 2
EMS Fellowship 1
-
7/27/2019 Santa Clara County Emergency Medical Services Agency
Semi-Annual Report (2012 May)
11/26
11
Santa Clara County EMS Agency May 2012 Report to the Hospitals
and Health Committee
Prehospital Clinical Care and Quality ImprovementThere were
several advances in Clinical Care and Quality Improvement in 2011.
In this report, we
highlight the implementation of therapeutic hypothermia,
mechanical trauma tourniquets, and
improvements in our clinical performance indicators.
Therapeutic hypothermia is the process of intentionally cooling
the bodys core temperature to improve
brain function following cardiac arrest. One European study
showed a favorable outcome rate of 55
percent with therapeutic hypothermia, versus a favorable outcome
rate of 39 without therapeutic
hypothermia1. A favorable outcome is defined as a discharge from
the hospital and the patient is able to
live independently, work, and live a productive enjoyable life.
Having the capability to induce
therapeutic hypothermia in the field provides the citizens of
Santa Clara County a better chance of
surviving with intact brain function following a sudden cardiac
arrest.
Mechanical tourniquets provide paramedics greater ability to
control life-threatening bleeding from
extremities. These tourniquets are the type used by soldiers in
battle, and can be applied quickly.
Mechanical tourniquets provide improved control of bleed and
reduce tissue damage, improving thepatients chance of recovery and
quality of life.
Clinical performance indicators (CPIs) are measures of elements
of clinical care that provide a method of
assessing the quality and safety of care at a system level. The
use of CPIs provides the EMS Agency the
ability to assess the efficacy of our treatment protocols and
policies. In 2011, the EMS Agency used
clinical performance indicators to evaluate the appropriate use
and frequency of intraosseous infusion
(placing a needle into a hollow portion of a bone to administer
fluids), the efficacy of dispatch protocols
and medications used to treat patients experiencing chest pain
from suspected cardiac ischemia, and
the time required to complete the first 12-lead EKG in patients
having a heart attack. Based on the use
of clinical performance indicators, we are confirming that our
processes work well, and are continuing toexamine potential
improvements to clinical care in the Santa Clara EMS System.
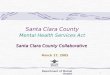
911 Ambulance Response Times
Ambulance Response Times to Emergency Calls
The chart below identifies the ambulance response times to Code
3 (emergency red light and siren) calls
by month from July 2011 thought December 2011 in each of the
five ambulance subzones within Santa
Clara County. The response time standard is 90% or greater, and
is represented by the blue horizontal
line on this graphic. Note the response time for Sub-Zone One
for July was 83.46%, and is not shown on
this graphic. The boundaries of each zone are displayed on page
14.
1Nolan, J.P and Morley, P.T. "Theraputic Hypotheria After
Cardiac Arrest." Circulation 108 (2003): 118-121.
-
7/27/2019 Santa Clara County Emergency Medical Services Agency
Semi-Annual Report (2012 May)
12/26
12
Santa Clara County EMS Agency May 2012 Report to the Hospitals
and Health Committee
July August September October November December
Sub-Zone 1 83.46 92.25 93.17 93.50 93.49 91.68
Sub-Zone 2 90.36 95.64 94.58 93.45 93.77 94.91
Sub-Zone 3 93.40 96.69 95.03 95.28 94.63 96.10Sub-Zone 4 90.30
91.80 92.03 91.48 92.60 93.56
Sub-Zone 5 93.73 97.01 95.73 95.51 96.85 96.03
*The response time in sub-zone 1 was 83.46 percent. This number
does not show on the chart, due to Excels scaling
characteristics.
88.00
90.00
92.00
94.00
96.00
98.00
100.00
July August September October November December
Rural Metro Ambulance Code 3 Response Time
Sub-Zone 1
Sub-Zone 2
Sub-Zone 3
Sub-Zone 4
Sub-Zone 5
-
7/27/2019 Santa Clara County Emergency Medical Services Agency
Semi-Annual Report (2012 May)
13/26
13
Santa Clara County EMS Agency May 2012 Report to the Hospitals
and Health Committee
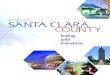
Ambulance Response Times to Non-Emergency Calls
The chart below identifies the ambulance response times to Code
2 (non emergency) calls by month
from July 2011 thought December 2011 in each of the five
ambulance subzones within Santa Clara
County. The response time standard is 90% or greater, and is
represented by the blue horizontal line on
this graphic.
July August September October November December
Sub-Zone 1 94.27 97.33 97.16 95.95 97.52 96.88
Sub-Zone 2 92.89 95.85 96.61 94.71 92.78 94.88
Sub-Zone 3 93.01 96.75 97.30 96.39 95.30 95.99
Sub-Zone 4 93.17 94.38 95.54 91.74 93.86 91.57
Sub-Zone 5 100.00 98.91 98.82 94.51 100.00 94.59
The following graphic identifies the Response Subzones and the
City Boundaries within Santa Clara
County.
88.00
89.00
90.00
91.00
92.00
93.00
94.00
95.00
96.00
97.00
98.00
99.00
100.00
Rural Metro Ambulance Code 2 Response Time
Zone 1-5
Sub-Zone 1Sub-Zone 2
Sub-Zone 3
Sub-Zone 4
Sub-Zone 5
-
7/27/2019 Santa Clara County Emergency Medical Services Agency
Semi-Annual Report (2012 May)
14/26
14
Santa Clara County EMS Agency May 2012 Report to the Hospitals
and Health Committee
Santa Clara County EOA Response Subzones and City Boundaries
Subzone 1: Los Altos Hills, Los Altos, Mountain View, Sunnyvale
and unincorporated areas Loyola, Moffet FieldSubzone 2: Campbell,
Cupertino, Los Gatos, Monte Sereno, San J ose (West), Saratoga and
the unincorporated areas of Burbank,Redwood EstatesSubzone 3:
Milpitas, San J ose (North), Santa ClaraSubzone 4: San J ose (East,
South)Subzone 5: Gilroy, Morgan Hill and unincorporated areas San
MartinSource: Santa Clara County Exclusive Operating Agreement,
Exhibit BDeveloped by: Santa Clara County Emergency Medical
Services AgencyCreated: 20090903
-
7/27/2019 Santa Clara County Emergency Medical Services Agency
Semi-Annual Report (2012 May)
15/26
15
Santa Clara County EMS Agency May 2012 Report to the Hospitals
and Health Committee
Mutual Aid Provided by County 911 AmbulanceThe chart below
identifies the number of times neighboring EMS Systems requested
assistance from the
Santa Clara County 911 ambulance provider by month from July
2011 through December 2011. In these
instances, a County Ambulance is immediately dispatched, unless
the loss of that ambulance would
degrade response times in the Santa Clara County EMS System.
July August September October November December
City of Palo Alto Requests 55 43 64 59 43 56
County of Santa Cruz Requests 4 3 1 0 0 2
County of San Mateo Requests 1 0 0 1 2 0
County of San Benito Requests 0 1 1 1 1 0
County of San Benito Requests 0 0 0 1 0 0
County of Alameda Requests 0 0 0 0 2 0
Total Requests 60 47 66 61 48 58
0
10
20
30
40
50
60
70
Requests for Mutual Aid Assistance from County Ambulance by
Month
City of Palo Alto Requests
County of Santa Cruz Requests
County of San Mateo Requests
County of San Benito Requests
County of Alameda Requests
-
7/27/2019 Santa Clara County Emergency Medical Services Agency
Semi-Annual Report (2012 May)
16/26
16
Santa Clara County EMS Agency May 2012 Report to the Hospitals
and Health Committee
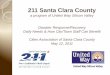
Fire Department First Responder Response Times
Fire Department Response Times to Emergency Calls
The chart below identifies the fire department response times to
Code 3 (emergency red light and siren)
calls by month from July 2011 thought December 2011 for each of
the first-response fire departments
within Santa Clara County. Fire departments should achieve a
response time of 90% or greater, andthose who achieve a response
time of 95% or greater are exempted from any response time
liquidated
damages incurred during that month.
Code 3 Response
(RLS)July August September October November December
Gilroy 98.24% 95.71% 97.92% 97.21% 98.27% 96.41%
Milpitas 97.79% 98.01% 97.66% 99.33% 99.31% 95.93%
Mt View 96.87% 97.40% 97.95% 97.14% 98.93% 96.70%
San Jose 92.67% 94.05% 92.80% 92.18% 92.62% 92.22%
Santa Clara City 96.22% 95.31% 95.29% 94.56% 96.20% 96.95%
Santa Clara Co. 96.07% 96.56% 96.97% 95.40% 95.59% 96.43%
So. Santa Clara Co. 96.36% 96.74% 97.52% 98.95% 100.00%
99.02%
Sunnyvale 97.49% 98.08% 98.88% 99.13% 98.47% 98.57%
90.00%
91.00%
92.00%
93.00%
94.00%
95.00%
96.00%97.00%
98.00%
99.00%
100.00%
Fire Department Code 3 Response Time Compliance by Month
J uly
August
September
October
November
December
-
7/27/2019 Santa Clara County Emergency Medical Services Agency
Semi-Annual Report (2012 May)
17/26
17
Santa Clara County EMS Agency May 2012 Report to the Hospitals
and Health Committee
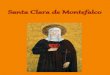
Fire Department Response Times to Non-Emergency Calls
The chart below identifies the fire department response times to
Code 2 (non-emergency) calls by
month from July 2011 thought December 2011 for each of the
first-response fire departments within
Santa Clara County. Fire departments should achieve a response
time of 90% or greater, and those who
achieve a response time of 95% or greater are exempted from any
response time liquidated damages
incurred during that month. The jurisdictions that are do not
have response time data in this graphic
below, did not submit the specified data to the EMS Agency.
Code 2 Response July August September October November
December
Gilroy N/A N/A N/A N/A N/A N/A
Milpitas N/A N/A N/A N/A N/A N/A
Mt. View 100.00 100.00 100.00 100.00 100.00 100.00
San Jose 97.86 98.76 97.79 98.70 98.32 98.21
Santa Clara City 98.36 96.21 97.26 95.63 97.14 97.30Santa Clara
Co. 100.00 100.00 100.00 99.48 99.00 99.52
So. Santa Clara Co. N/A N/A N/A N/A 100.00 100.00
Sunnyvale Dept
Public SafetyN/A N/A N/A N/A N/A N/A
90.00
91.00
92.00
93.00
94.00
95.00
96.00
97.00
98.00
99.00
100.00
Fire Department Code 2 Response Time Compliance by Month
July
August
September
October
November
December
-
7/27/2019 Santa Clara County Emergency Medical Services Agency
Semi-Annual Report (2012 May)
18/26
18
Santa Clara County EMS Agency May 2012 Report to the Hospitals
and Health Committee
Air Ambulance Transports
Air ambulance utilization continued at relatively low levels in
2011. This volume of responses and
transports has remained static since approximately 2009. The EMS
Agency considers appropriate, this
volume of air ambulance responses and transports.
YearNumber ofDispatches
Number ofTransports
Dispatch totransport percent
2001 557 254 46%
2002 540 254 47%
2003 524 236 45%
2004 545 251 46%
2005 463 205 44%2006 443 221 50%
2007 442 207 47%
2008 248 137 55%
2009 184 111 60%
2010 176 103 59%
2011 179 107 60%
254 254
236
251
205
221207
137111 103 107
557540
524
545
463443
442
248
184176
179
100
200
300
400
500
600
ResponsevTrans
port
Air Ambulance Utilzation by YearTransports
Responses
Source: Santa Clara County EMS Agency, County Communications
-
7/27/2019 Santa Clara County Emergency Medical Services Agency
Semi-Annual Report (2012 May)
19/26
19
Santa Clara County EMS Agency May 2012 Report to the Hospitals
and Health Committee
Hospital and Specialty Care Facilities
Hospital Volume and DestinationsDuring 2011, there were 69,508
ambulance transports from the 911 System to hospitals within
Santa
Clara County. This is an approximate increase of 8% over the
transport volume of 64,507 patients in
calendar year 2010. The distribution of the patients to
hospitals has not materially changed in the past
year.
Hospital
(2011)Jan Feb Mar Apr May Jun July Aug Sep Oct Nov Dec
Totals
Los Gatos-El Camino
92 70 86 89 86 80 89 76 69 81 82 85 985
Mt. View-
El Camino666 628 698 603 598 593 645 575 565 583 572 681
7,407
Good
Samaritan578 502 620 529 558 559 561 566 578 568 518 619
6,756
Kaiser-
San Jose606 566 614 640 639 577 574 577 591 578 550 580
7,092
Kaiser-
Santa
Clara
617 607 658 599 602 618 612 631 560 606 559 663 7,332
O'Connor 585 519 533 523 501 492 500 492 492 538 510 506
6,191
Regional-
San Jose1,133 958 1,099 1,039 1,031 973 1,005 971 1,060 1,054
1,002 952 12,277
Saint
Louise216 202 214 220 226 209 223 214 222 224 208 214 2,592
Stanford 421 437 398 413 416 365 256 165 161 157 148 410
3,747
VA - Palo
Alto49 53 47 47 63 47 57 46 42 54 45 63 613
VMC 1,123 1,049 1,154 1,134 1,136 1,227 1,327 1,248 1,239 1,363
1,236 1,280 14,516
Total 6,086 5,591 6,121 5,836 5,856 5,740 5,849 5,561 5,579
5,806 5,430 6,053 69,508
Source: Santa Clara County Communications; Palo Alto Fire
Dept.*
0
1,000
2,0003,000
4,000
5,000
6,000
7,000
Patients Transported to Hospital Emergency
Departments from 911 System 2011
VMC
VA - Palo Alto
Stanford
Saint Louise
Regional - San JoseO'Connor
Kaiser - Santa Clara
Kaiser - San Jose
Good Samaritan
Mt. View - El Camino
Los Gatos - El Camino
-
7/27/2019 Santa Clara County Emergency Medical Services Agency
Semi-Annual Report (2012 May)
20/26
20
Santa Clara County EMS Agency May 2012 Report to the Hospitals
and Health Committee
Hospital DiversionHospital diversion is the practice by which a
hospital closes to ambulances transporting non-critical or
non-specialty care patients. In the Santa Clara EMS System,
hospitals should not use diversion more
than 36 hours per month. This standard is graphically identified
in the blue horizontal line.
Hospital diversion levels appeared to trend toward
stabilization, with hospitals in general achievinglower diversion
levels in Calendar Year 2011. However, the EMS Agency is monitoring
a concerning
trend of increased ambulance wall times. This is the practice of
busy hospital emergency departments
not timely accepting the ambulance patient, causing the
ambulance crew to wait for extended periods
at the hospital. The EMS Agency is developing measurement
methods and metrics to quantify and
resolve this problem.
0.00
20.00
40.00
60.00
80.00
100.00
120.00
Jan Feb Mar Apr May Jun July Aug Sep Oct Nov Dec
Hospital ED Diversion Hours
by Month 2011
El Camino - Los Gatos
El Camino - Mt. View
Good Samaritan
Kaiser - San Jose
Kaiser - Santa Clara
O'Connor
Regional - San Jose
Saint Louise
Stanford
VA - Palo Alto
VMC
-
7/27/2019 Santa Clara County Emergency Medical Services Agency
Semi-Annual Report (2012 May)
21/26
21
Santa Clara County EMS Agency May 2012 Report to the Hospitals
and Health Committee
Hospital Jan Feb Mar Apr May Jun July Aug Sep Oct Nov Dec
Totals
El Camino
Los Gatos0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00
0.00 0.00
El Camino
Mt. View8.61 16.53 9.02 18.11 13.17 21.76 29.08 6.02 16.34 20.25
3.71 15.89 178.49
Good
Samaritan 10.52 30.05 10.52 9.02 7.52 9.04 3.90 0.00 2.46 0.66
7.12 8.12 98.93
Kaiser
San Jose0.00 0.00 0.00 0.00 0.00 0.00 0.21 0.00 0.00 0.00 0.00
0.00 0.21
Kaiser
Santa Clara9.49 3.01 1.22 0.00 4.51 0.00 1.50 1.50 1.50 1.50
1.51 4.50 30.24
O'Connor 22.55 29.64 23.21 35.02 21.04 32.14 16.54 5.83 4.26
4.52 3.42 12.02 210.19
Regional
San Jose33.51 23.92 19.15 25.55 25.30 27.08 16.90 16.53 4.51
4.50 7.91 4.51 209.37
Saint Louise 10.52 16.01 16.56 9.02 10.11 15.67 4.51 16.55 36.76
16.81 4.52 17.01 174.05
Stanford 42.96 19.65 23.90 15.03 7.53 16.71 9.02 0.00 3.00 1.51
0.00 13.29 152.60
VA - Palo
Alto
40.86 41.34 4.07 0.00 17.22 1.50 34.77 25.54 16.52 28.23 72.20
6.00 288.25
VMC 100.68 74.84 69.85 59.52 50.43 15.79 11.15 5.53 8.61 6.91
11.73 6.74 421.78
Total 279.70 254.99 177.50 171.27 156.83 139.69 127.58 77.50
93.96 84.89 112.12 88.08 1,764.11
Trauma Care SystemThe Santa Clara County Trauma Care System has
existed for over 30 years. This evidence- based system
provides patients the opportunity to be transported to the
closest, specially designated hospital, which
can provide immediate trauma care services to patients who are
injured in Santa Clara County, or in
other adjacent counties. There are three trauma centers in Santa
Clara County; Santa Clara Valley
Medical Center (SCVMC), Regional Medical Center of San Jose
(RSJ), and Stanford University Hospital(SUH). SCVMC and SUH are
also designated as Pediatric Trauma Centers. Each Trauma Center
provides
service to an assigned catchment area.
There is much scientific evidence which supports the concept of
the transport of severely injured victims
to a specially designated center that has a concentration of
services able to provide rapid treatment and
continuing care to trauma victims. The low death rates and
decreased limitations from injuries in
Trauma Centers is objective proof of the concept that was
developed many years ago in battle field
medicine.
Since 2008 the trauma centers in Santa Clara County have served
29,640 patients. This includes 26,611
adults and 3029 pediatric patients.
Mode of transport to the Trauma Center: Ambulance transport
occurred in 80% of all trauma cases.
Twelve (12) percent arrived by Air Medical Transport.
County of Injury: The primary county of injury is Santa Clara
County which accounts for 19664 patients
(66%). The top four counties after Santa Clara are: San Mateo
(14%), Santa Cruz (8%), Monterey (4%)
and San Benito (2%).
-
7/27/2019 Santa Clara County Emergency Medical Services Agency
Semi-Annual Report (2012 May)
22/26
22
Santa Clara County EMS Agency May 2012 Report to the Hospitals
and Health Committee
Type of Injury: Blunt injury (motor vehicle/motorcycle injuries,
pedestrian struck, bicycle etc)
represents 91% of total injuries, while penetrating injuries
(gunshot wounds, stabbings etc) are 9% of
total injuries.
Age factors: The age ranges of victims of trauma are as
follows
Age range Total
0-5 years 1112
6-15 years 1752
16-21 Years 4629
22-35 Years 7515
36-45 years 3848
46-65 years 6480
66-75 years 1394
>75 years 2214
>100 years 11
Injury severity: Using a calculation referred to as the Injury
severity score (ISS) we determined that 65%
of the trauma patients are in the minor injury (ISS less than 9)
category, 19% are in the moderately (ISS 9
to less than 15) and 14% are in the severely ( ISS 15 to less
than 75) injured category.
ISS Total Volume Percent volume
1 to less than 9 19266 65%
9 to less than 15 5632 21%
15 to 75 4150 14%
0%
10%
20%
30%
40%
50%
60%
70%
Santa Clara San Mateo Santa Cruz Monterey San Benito
Santa Clara County Trauma System
Percent Volume
County of Injury Percent vol
-
7/27/2019 Santa Clara County Emergency Medical Services Agency
Semi-Annual Report (2012 May)
23/26
23
Santa Clara County EMS Agency May 2012 Report to the Hospitals
and Health Committee
Disposition from Emergency Department: Forty five (45) percent
of all trauma patients are admitted to
the hospitals. Overall 0.06% of patients expire in ED. Total
discharges from the ED represent 47% of
trauma patients.
Disposition Total Volume Percent Volume
Admitted to hospital 13338 45%
Death in ED 17 0.06%
Discharged from ED 13931 47%
Stroke Care SystemThe Santa Clara County Board of Supervisors
approved a stroke care system developed by the Santa
Clara County Emergency Medical Services Agency in March of 2006.
This evidence- based system
provides patients the opportunity to be transported to the
closest, specially designated hospital, which
can provide immediate stroke care services to patients who are
showing symptoms of an acute stroke.
The need for rapid intervention is based on the a preponderance
of scientific evidence that
demonstrates if the patient is treated with an anti clotting
drug (IV tPa) within three and a half hours of
the onset of their symptoms, the opportunity exists to prevent
and possibly reverse the effects of the
blocked circulation to the brain. In order to respond to the
need for rapid treatment, the system was
designed with a specific goal: to increase the numbers of
patients who arrived in the ED at the stroke
center within the time frame to allow administration of the
drug.
A second goal of the stroke system has been to educate the
public about stroke symptoms, and the
need to call 9-1-1 if symptoms are present. Historically the
percentage of patients who come to a stroke
center by ambulance is approximately 45% of the total stroke
population. Currently (2011) data showsthat 54% of the stoke
patients now arrive by ambulance. This increase is potentially
related to the
outreach activities accomplished by the Stroke Busters: All of
the Santa Clara County Stroke Centers in
conjunction with the County EMS agency, the Prehospital
transport provider, and the two non-profits
who assist with outreach, Stroke Awareness Foundation and the
Peninsula Stroke Association. In
October of 2011 the Stroke Busters attended the Health Concern
Outreach program at the San Jose
Flea Market. A total of 800 people of all ages and ethnicities
were contacted by the group who took
their blood pressures and gave them stroke information. This
annual event will continue indefinitely.
-
7/27/2019 Santa Clara County Emergency Medical Services Agency
Semi-Annual Report (2012 May)
24/26
24
Santa Clara County EMS Agency May 2012 Report to the Hospitals
and Health Committee
2011 Performance Data
Criteria County Performance Data
Total stroke patients 2546
Total number of Ischemic Strokes 2052
Total Stroke patients who arrived by EMS transport 1378
Total Stroke patients who self-transported 1087
Total Stroke patients who arrived by interfacility transfer
153Percentage of Ischemic Stroke Patients who were treated
with IV tPa11% National Avg. (1-8%)
Cardiac Care (STEMI) SystemSanta Clara County Emergency Medical
Services Agency initiated a care system for patients who had
evidence of an acute heart attack (STEMI) on an
electrocardiogram (EKG) performed by the Prehospital
paramedics. This is an evidence- based system which affords
patients the opportunity to be transported
to the closest, specially designated hospital, which can provide
immediate cardiology services including
a cardiac catheterization laboratory, to open their blocked
artery.
The need for rapid intervention is based on the a preponderance
of scientific evidence that
demonstrates if the patient is treated (opening up the blocked
artery) within 90 minutes or less after
arrival, the opportunity exists to prevent and possibly reverse
the effects of the blocked circulation to
the heart. In order to respond to the need for rapid treatment,
the system was designed with a specific
goal: time of entry into the Emergency Department (ED) to the
time of inflation of the balloon to open
the artery (D2B) in less than 90 minutes for 75% of all STEMI
patients (this includes patients who are
0
2
4
6
8
10
12
2009 2010 2011
Santa Clara County Stroke System
Percentage of Ischemic Stroke Patients
Treated with IV tPa
IV tPa
-
7/27/2019 Santa Clara County Emergency Medical Services Agency
Semi-Annual Report (2012 May)
25/26
25
Santa Clara County EMS Agency May 2012 Report to the Hospitals
and Health Committee
transported by ambulance and those who self-transport to the ED)
which is a national standard for
STEMI care.
In the beginning of the system paramedics did not electronically
transmit the EKG prior to arrival at the
ED. Patients who had positive findings on the EKG were
transported with only phone notification. The
paramedic would alert the receiving facility that they had a
positive EKG, at which time the receivingED could elect to
immediately notify the cardiology service that a STEMI patient was
enroute, or the ED
would wait on the notification until the patient arrived with
the EKG. Once the new transport provider
began providing service in July of 2011, the paramedic now
obtains and electronically transmits an EKG
to the hospital with the notification. It was felt that this
transmission would decrease the D2B time by
approximately 10-15 minutes.
2011 Performance Data
Criteria County Performance Data
Total cases with Documented STEMI 444
Median D2B in minutes 62 minutes
Goal Met (D2B in less than 90 minutes in 75% of
cases
98% of all cases were in less than 90
minutes
Total STEMIs who arrived by EMS transport 264
Total STEMIs who self-transported 160
Total STEMIs who arrived by interfacility
transfer20
60
61
62
63
64
65
66
67
68
69
70
2009 2010 2011
Santa Clara County STEMI System Performance
Median D2B time in minutes
D2B
-
7/27/2019 Santa Clara County Emergency Medical Services Agency
Semi-Annual Report (2012 May)
26/26
26
2010 Performance Data
Criteria County Performance Data
Total cases with Documented STEMI 324
Median D2B in minutes 65 minutes
Goal Met (D2B in less than 90 minutes in 75% of
cases
95% of all cases were in less than 90
minutes
Total STEMIs who arrived by EMS transport 209
Total STEMIs who self-transported 109
Total STEMIs who arrived by interfacility
transfer6
2009 Performance Data
Criteria County Performance Data
Total cases with Documented STEMI 97
Median D2B in minutes 69 minutes
Goal Met (D2B in less than 90 minutes in 75% of
cases
90% of all cases were in less than 90
minutes
Total STEMIs who arrived by EMS transport 176
Total STEMIs who self-transported 196
Total STEMIs who arrived by interfacility
transfer16