A. Curnis
GARDONE RIVIERA 15 Aprile 2016
University of Brescia Medical School
Electrophisiology and Cardiostimulation Laboratory
Division of Cardiology
Italy
Patients with Device infection
BL Wilkoff; Texas Heart Inst J 2011

S. K
urt
z e
t A
l, V
ol. 3
3 P
AC
E 2
01
0
The rate of implant Pts health profile
Procedere Mean age
Primary PM 75 + 12.1
Replacent PM 73 + 16.0
Primary ICD 66.2 +12.8
Replacent ICD 67.9 + 13.2
Age of PM Pts at Time of Implantation
J A
m C
oll
Card
iol 2
01
2;6
0:1
54
0–5)

Device-related infections
Not related to Device type
Device –Tissue interaction
Recurrent infections during antibiotic therapy
Infections related to the implant procedure:
0.13 %-19.9 % PMs implants
0.8%- 13% ICDs implants (High variability from different Authors)
Pocket infections: 0.5-5%
Sepsi and endocarditis: 0.5-0.005%
Time to PM infection after implant: 2.5 weeks
Time to leads infection after implant: 33 weeks

Immunosoppression
(Diabetes, renal faliure, steroid therapy, cancer)
Vit K antagonist’s therapy
Post procedure Haematoma
Necessity of replacement Device and or for lead for
dislgment
Abandoned leads
Trombosis of the subclavian vein
Physician experience
Infection-related Factors

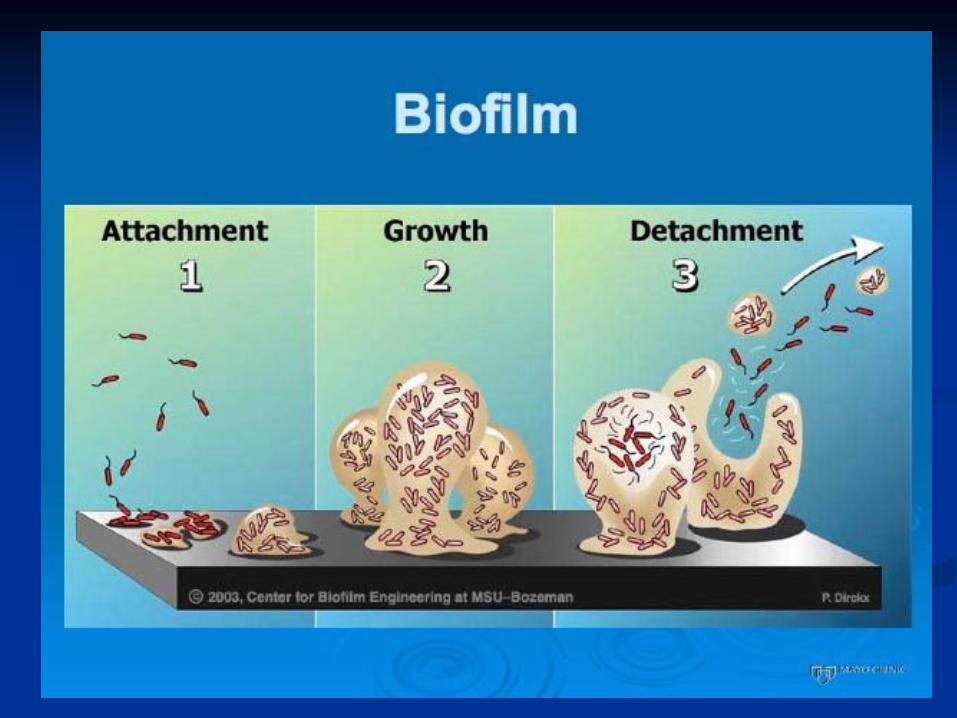
Infection’s mechanisms
Local contamination
(in the poket during implant)
Skin erosion after traumatisms
( with or without leads exposure)
Blood contamination (Methastatic)
Prognosis
Without device explant:
66% mortality
With device explant:
24 to 28% mortality
Parry G et al,PACE 1991;14:1251-7
Klug D,Circulation 1997;95:2098-107

Microbiology
Staphylococci (72-95%):
-St. Aureus (early infection)
-St. Epidermidis (late infection)
Others: Enterococcus
Streptoccocus
Proteus
Klebsielle
E. Coli
Pseudomonas aeruginosa
Fungi (rare)
Others….


percutaneous removal of CIEDs in patients with IE withlarge vegetations.
Aim:
•in-hospital morbidity and mortality related to percutaneous removal
of vegetations ≥20 mm.
•8 cases with a follow-up period of 20 months.
• We removed 100% of leads in the study population.
Conclusions:
• Transvenous extraction of pacing leads with larger vegetations is a feasible
technique.
•There was a tendency toward symptomatic pulmonary embolism in patients with
vegetations larger than 20 mm;
•morbidity and mortality were not influenced
Clin. Cardiol. 35, 4, 244–249 (2012)
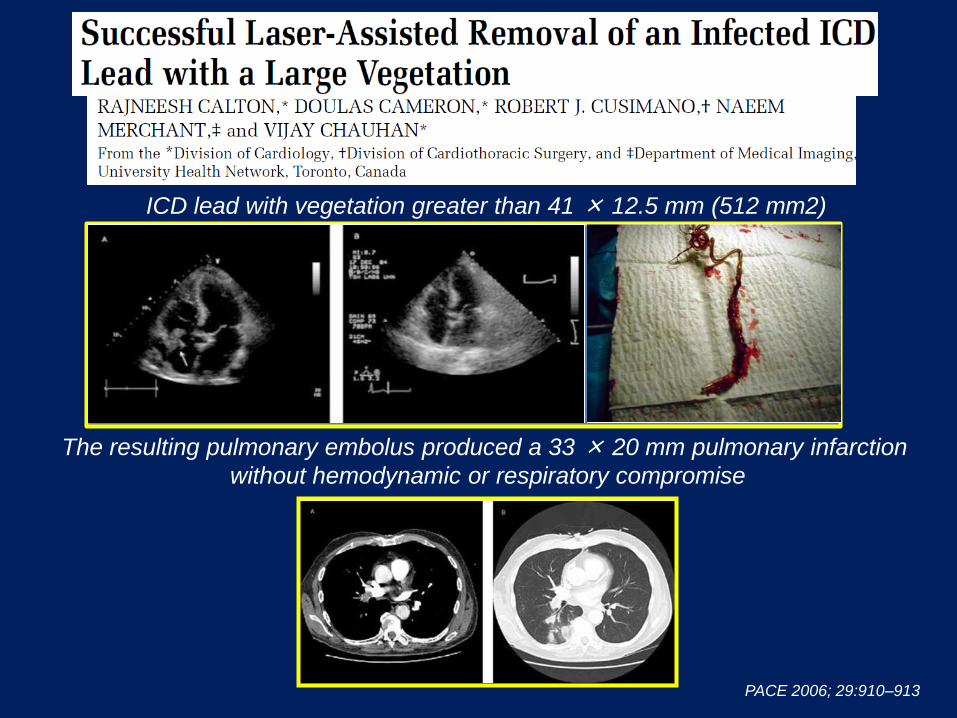
ICD lead with vegetation greater than 41 × 12.5 mm (512 mm2)
The resulting pulmonary embolus produced a 33 × 20 mm pulmonary infarction
without hemodynamic or respiratory compromise
PACE 2006; 29:910–913
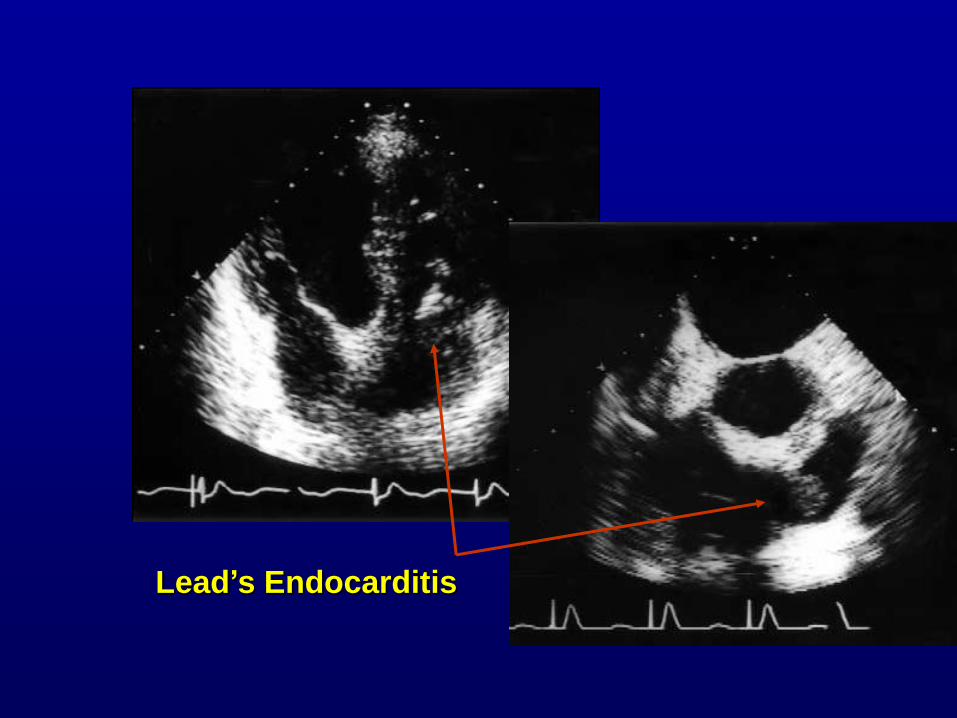
Lead’s Endocarditis
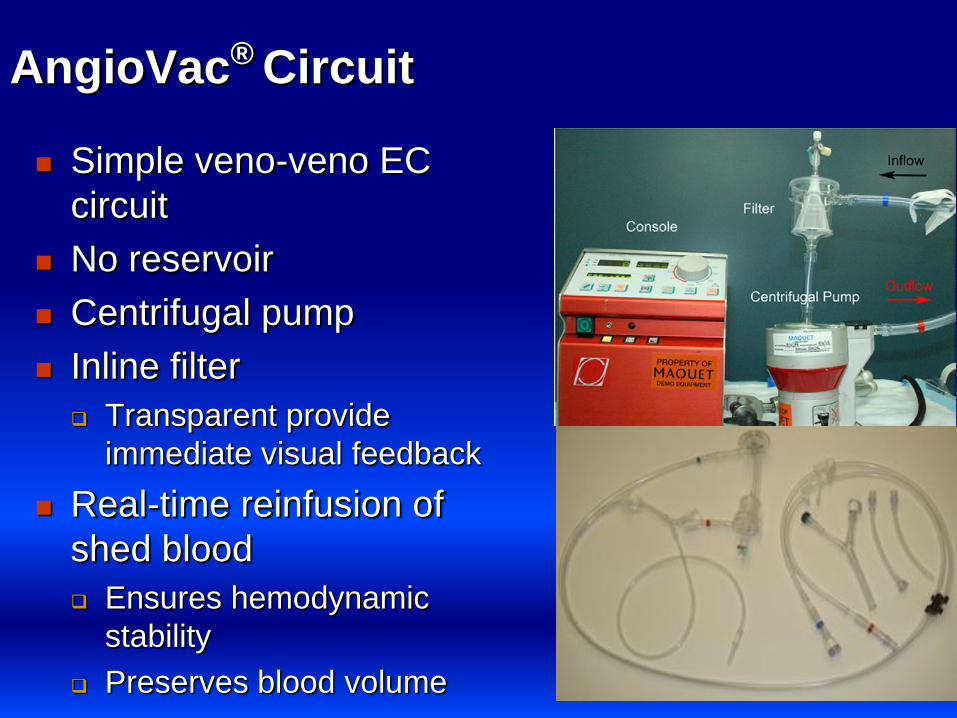
AngioVac® Circuit
Simple veno-veno EC
circuit
No reservoir
Centrifugal pump
Inline filter
Transparent provide
immediate visual feedback
Real-time reinfusion of
shed blood
Ensures hemodynamic
stability
Preserves blood volume

MASTER E&E

Tricuspid Vegetation Goldman, et al – Lankenau Hosp, PA

Tricuspid vegetation Goldman, et al – Lankenau Hosp, PA

Devices infections are more frequent
Key point is to identify the pathogen responsible for infection
Mandatory is a target antibiotic therapy
The complete removal of the system is required to eradicate
infection
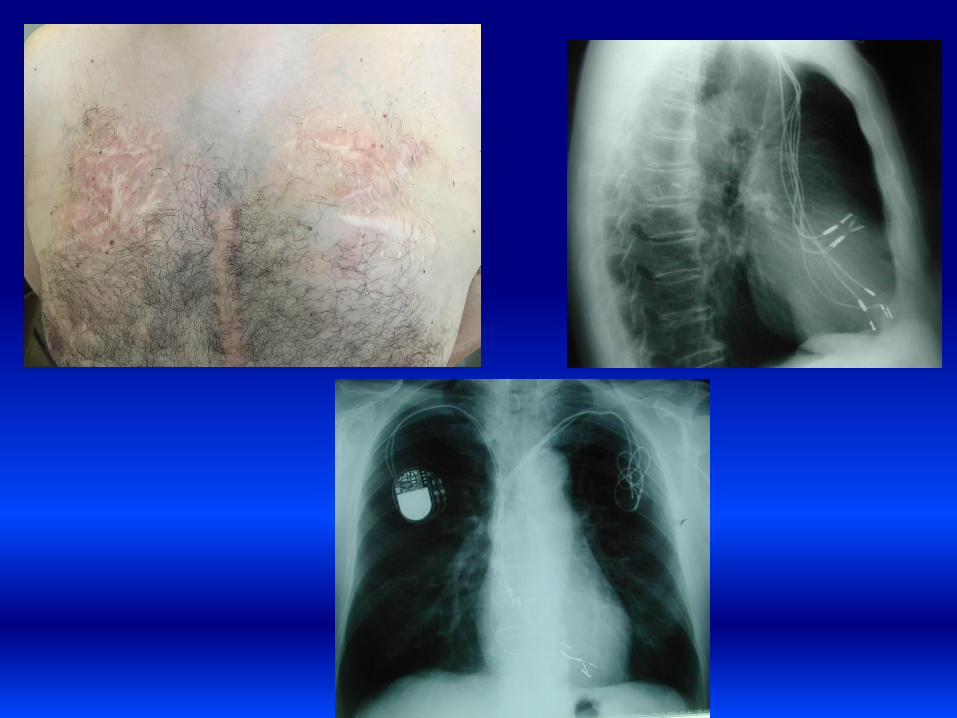
Key points:

Different situations of device infection
Three different aspects of the same
problem :
A) edema of the pocket
B) skin retraction and initial necrosis
without device exposure
C) skin erosion with system exposure


Implant’s complications
1990-1999
PM 28% at 10 years
ICD 40% at 8 years
15 - 40% Venous trombosis

Problems of assistance
Infected CIEDs Non infected
CIEDs
p
National
incidence (USA)
31256 631422 NS
Age (mean) 67 ± 16 66 ± 16 NS
Females 34% 26% 0.008
In hospital stay
(days)
11 ± 10
4 ± 3
< 0.001
Hospital
mortality
5.2%
1.0%
< 0.001
Data related of 2004-2006
Voigt A; PACE 2010

Patients more at risk
Pz with infection (n = 75)
Controls (n = 75)
Adjusted OR (multivariate)
Device revision (leads and device)
60%
33%
3.67 (1.51 – 8.96)
eGFR < 60 ml/min 32% 11% 4.64 (1.48 – 14.62)
Anticoagulants Use*** 48% 21% 2.83 (1.20 – 6.68)
Lekkerkerker JC; Heart 2009

Early diagnosis and prognosis -1- Variable Group A Group B
Fever > 38 ° C 81% 14%
PAS < 90 mmHg 68% 19%
Leukocytes >
10000/mm3
97%
33%
Positive blood
cultures
100%
0%
Positive pocket
cultures
19%
57%
Leads vegetations
68%
0%
Valvular vegetations
19%
5%
Local involvement
of the pocket
0 – 13%
43% - 90%
Group A: signs of systemic infection
Group B: signs of local infection
Viganego F; Am J Cardiol 2012
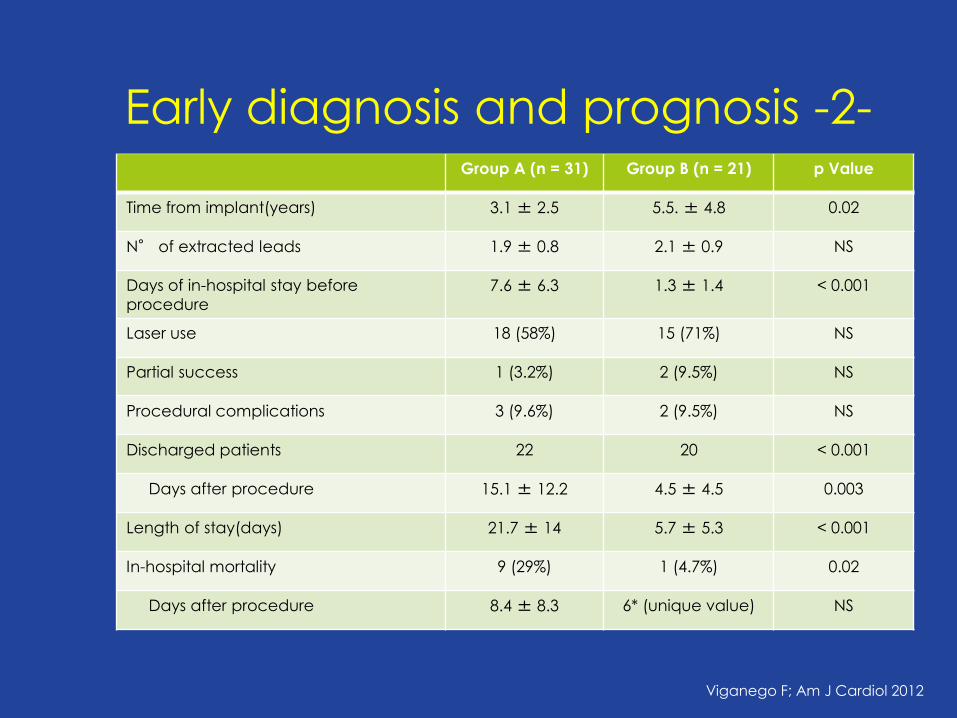
Group A (n = 31) Group B (n = 21) p Value
Time from implant(years) 3.1 ± 2.5 5.5. ± 4.8 0.02
N° of extracted leads 1.9 ± 0.8 2.1 ± 0.9 NS
Days of in-hospital stay before
procedure 7.6 ± 6.3 1.3 ± 1.4 < 0.001
Laser use 18 (58%) 15 (71%) NS
Partial success 1 (3.2%) 2 (9.5%) NS
Procedural complications 3 (9.6%) 2 (9.5%) NS
Discharged patients 22 20 < 0.001
Days after procedure 15.1 ± 12.2 4.5 ± 4.5 0.003
Length of stay(days) 21.7 ± 14 5.7 ± 5.3 < 0.001
In-hospital mortality 9 (29%) 1 (4.7%) 0.02
Days after procedure 8.4 ± 8.3 6* (unique value) NS
Viganego F; Am J Cardiol 2012
Early diagnosis and prognosis -2-

Level Raccomandation
Class 1 In all the patients shoud be done almost two blood cultures before the beginning of
the antibiotic therapy or before the procedure of extraction
Class 1 Once the extraction, should be sent to culture the tissue that surrounds the
generator and the tips of leads
Class 1 Patients with suspected CIED infection who have positive blood cultures or who
have negative blood cultures but already in the course of antibiotic therapy prior to
sampling, should undergo transesophageal echocardiogram
Class 1 Patients with endocarditis on leads, should undergo transesophageal echo to
highlight endocarditis on the left valves. Exception can be done in pediatric
patients, in which the echo TT may be sufficient
Class 2a Patients with CIED who develop fever or positive blood cultures unexplained should
be seen by a cardiologist or an infectivologist
Class 3 The fine-needle aspiration of the pocket of the device should not be performed as a
diagnostic step for suspected CIED
Baddour LM; Circulation 2010
RACCOMANDATION

Diagnostic Flow-chart - 1 Initial evaluation and empiric antibiotic therapy
Chemistry exams:
Blood count Electrolytes Sieric creatinine ESV PCR 2 set blood cultures
To decide timing of antibiotic therapy
Systemic signs Poket inflammation (cellulitis, chronic draining sinus, swelling)
System exposition
Begin an antibiotic therapy for Gram negative and St. Aureus methicillin-resistant
Is possible the extraction of the system within 24 h)
No
Do not administer antibiotics
since the pre-operatory time
Yes
Dababneh AS, Sohail MR; Clev Clin J Med 2011

Diagnostic Flow-chart – 2 To determinate the duration of therapy
Blood culture and pockets’ swab
Culture positive, clinical signs of endocardities
or previus antibiotic therapy Negative blood cultures
Pocket infection System exposition
Antibiotics for 10-14 days*
Antibiotics for
7-10 days*
Echo TE
Valvular vegetations
Leads vegetations Negative
Guidelines for treatment of bacterial endocardieties
Osteomyelitis or septic venous thrombisis
Not complicated St. Aureus Others
Antibiotics for 4 – 6 weeks*
Antibiotics for 2 – 4 weeks*
Antibiotics for 2 – 4 weeks*
Antibiotics for 2 weeks*
* Time is calculated from the day of procedure
Dababneh AS, Sohail MR; Clev Clin J Med 2011

Survival
Group 2 (Malf. + Occl.)
Group 1 (Infections)
p = 0.022
Infected WITHOUT vegetations
Infected WITH vegetations
General population Infected patients
p = 0.04
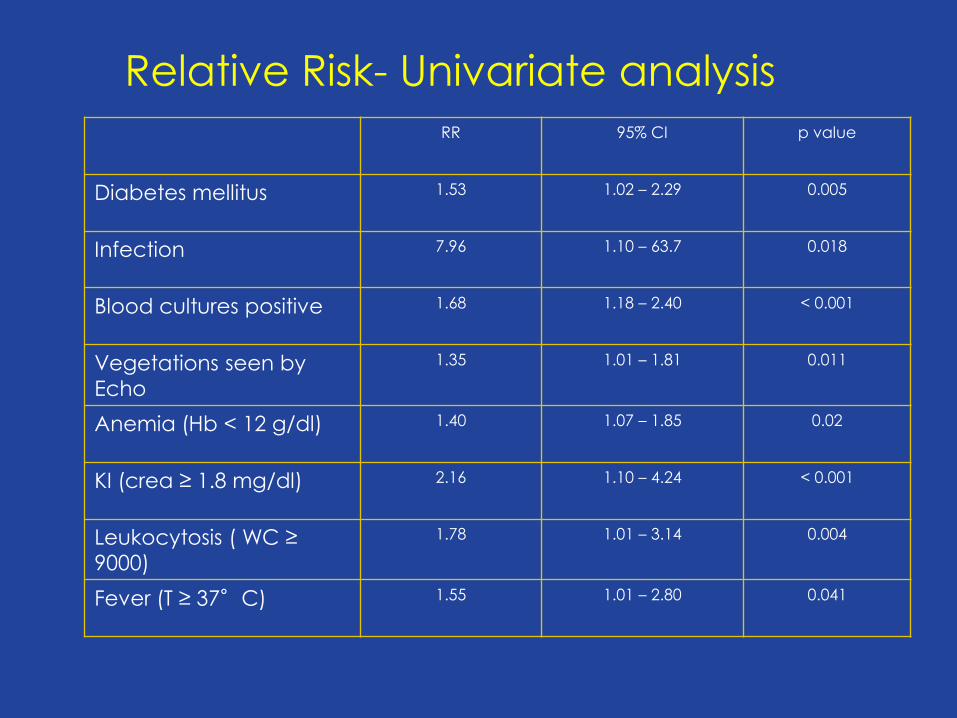
Relative Risk- Univariate analysis
RR 95% CI p value
Diabetes mellitus 1.53 1.02 – 2.29 0.005
Infection 7.96 1.10 – 63.7 0.018
Blood cultures positive 1.68 1.18 – 2.40 < 0.001
Vegetations seen by
Echo
1.35 1.01 – 1.81 0.011
Anemia (Hb < 12 g/dl) 1.40 1.07 – 1.85 0.02
KI (crea ≥ 1.8 mg/dl) 2.16 1.10 – 4.24 < 0.001
Leukocytosis ( WC ≥
9000)
1.78 1.01 – 3.14 0.004
Fever (T ≥ 37°C) 1.55 1.01 – 2.80 0.041

When reimplantation is safe ?
• Studies indicate that up to 30% of patients may no longer
require a cardiac device. 1,2
1-J Am Coll Cardiol 2007; 49:1851–1859
2-J Am Coll Cardiol 2007; 49:1851–1859..
• Presence positive pre / post operative blood cultures
• Presence of valvular- or lead-associated vegetations
• Positive lead-tip cultures or preoperative sepsis
• PCR –ESV Procalcitonine resolution of fever, normal white
blood cell count
• PM dependent ?
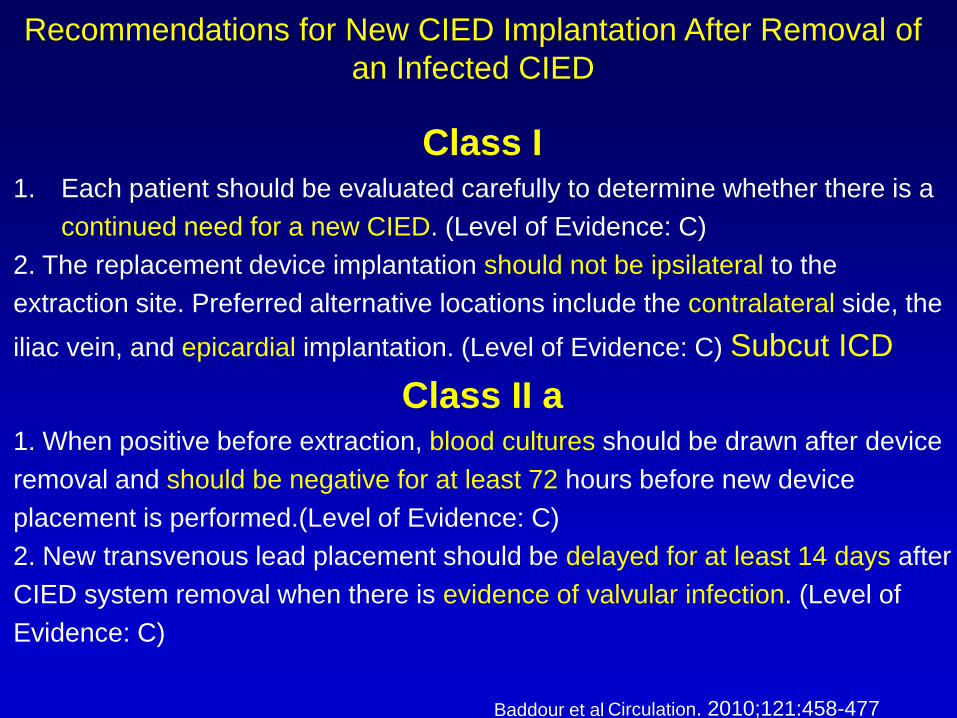
Class I 1. Each patient should be evaluated carefully to determine whether there is a
continued need for a new CIED. (Level of Evidence: C)
2. The replacement device implantation should not be ipsilateral to the
extraction site. Preferred alternative locations include the contralateral side, the
iliac vein, and epicardial implantation. (Level of Evidence: C) Subcut ICD
Class II a 1. When positive before extraction, blood cultures should be drawn after device
removal and should be negative for at least 72 hours before new device
placement is performed.(Level of Evidence: C)
2. New transvenous lead placement should be delayed for at least 14 days after
CIED system removal when there is evidence of valvular infection. (Level of
Evidence: C)
Recommendations for New CIED Implantation After Removal of
an Infected CIED
Circulation. 2010;121:458-477 Baddour et al
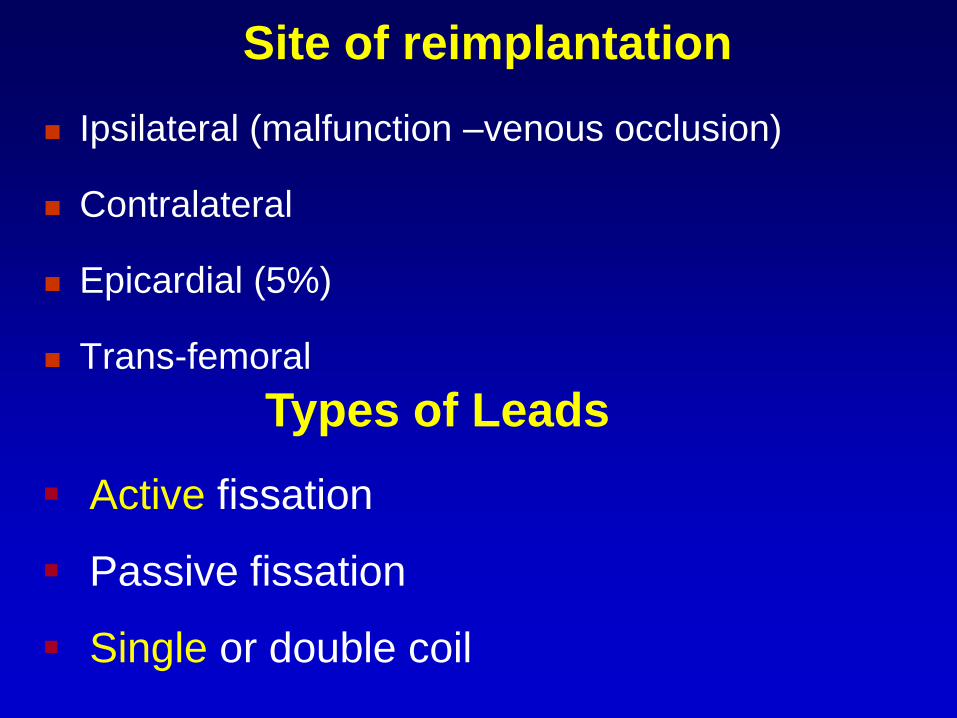
Site of reimplantation
Ipsilateral (malfunction –venous occlusion)
Contralateral
Epicardial (5%)
Trans-femoral
Types of Leads
Active fissation
Passive fissation
Single or double coil
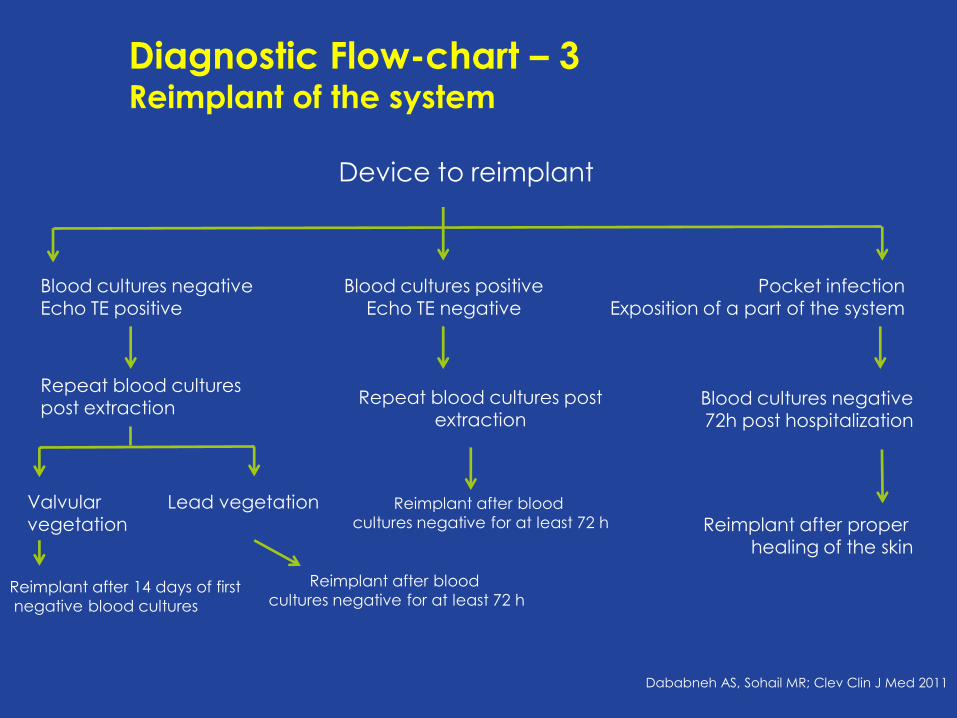
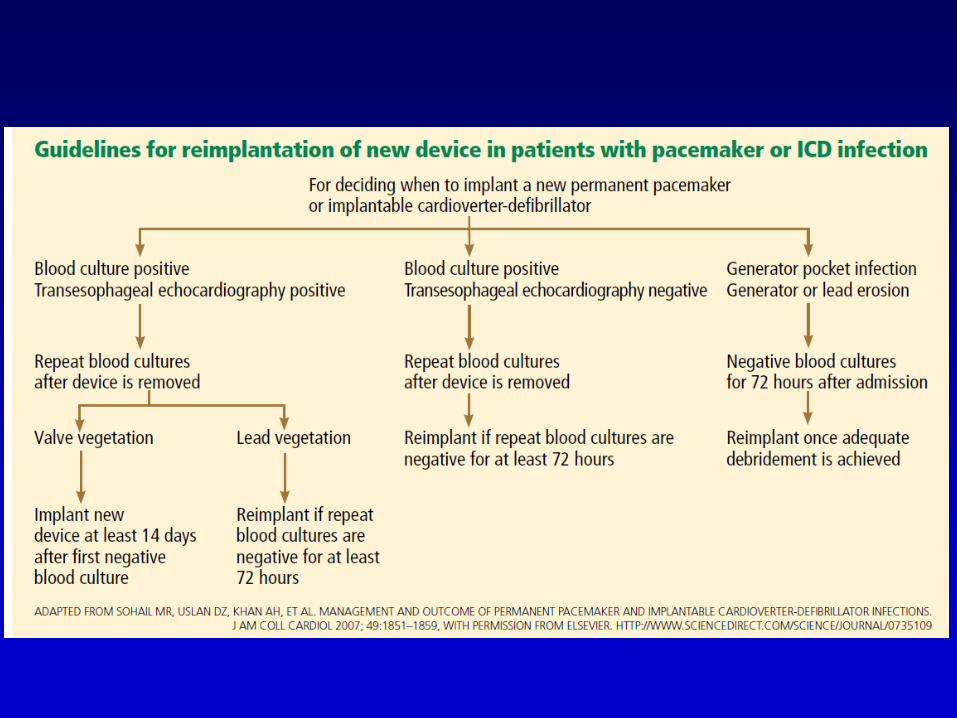
Diagnostic Flow-chart – 3 Reimplant of the system
Device to reimplant
Blood cultures negative
Echo TE positive
Blood cultures positive
Echo TE negative
Pocket infection
Exposition of a part of the system
Repeat blood cultures post extraction
Repeat blood cultures post extraction
Blood cultures negative 72h post hospitalization
Valvular vegetation
Lead vegetation
Reimplant after 14 days of first
negative blood cultures
Reimplant after blood
cultures negative for at least 72 h Reimplant after proper healing of the skin
Dababneh AS, Sohail MR; Clev Clin J Med 2011
Reimplant after blood
cultures negative for at least 72 h
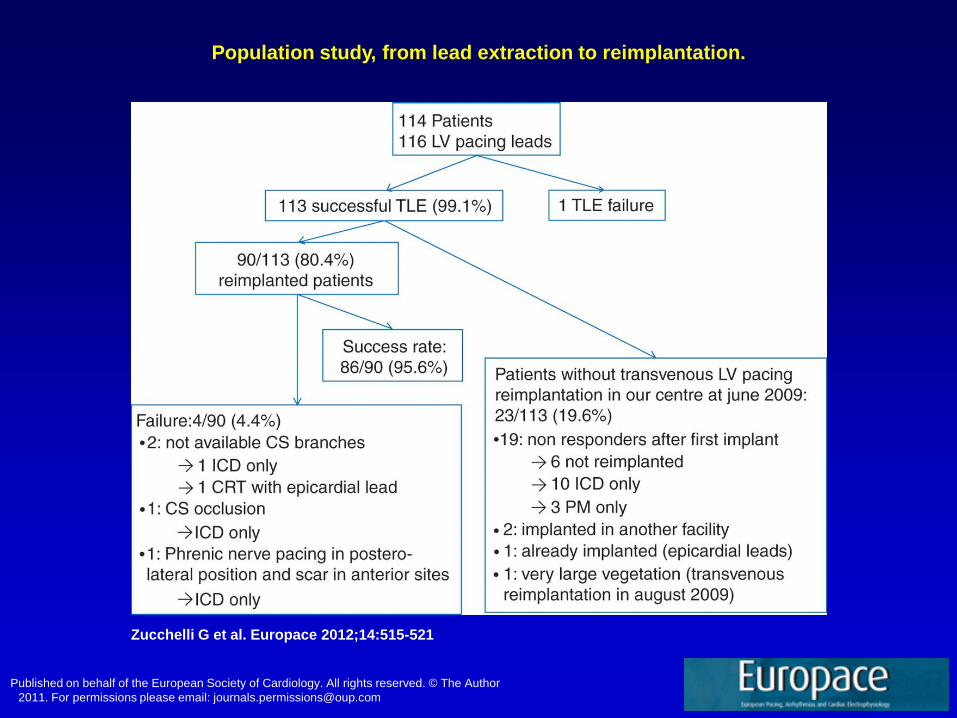
Population study, from lead extraction to reimplantation.
Zucchelli G et al. Europace 2012;14:515-521
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author
2011. For permissions please email: [email protected]

Conclusions The complete removal of the system is the more effective
therapy for the eradication of complications divice-related
(infections, malfunctioning).
Different endovascular approches are available for leads
extraction, and the possibility of combinated use makes
the therapy more effective and safety.
To reduces complications and increase efficiency has a
key role the training and subsequent experience of the
operator
Today there are reliable data on the timing to replant
Recommended