N on - i nvasive endoscopic technique Br. J. Surg. 1987, Vol. 74, November, 1053-1 055
P. I. M. Allen, D. Gourevitch and M. Goldman
East Birmingham Hospital, Bordesle y Green East, Birmingham B9 5ST, UK Correspondence to: Miss P. I. M. Allen
to assess gastrointestinal perfusion
Changes in mucosal blood flow may occur in many gastrointestinal disorders, but assessment is impossible without a non-invasive in vivo technique. We have compared endoscopic laser Doppler (LD) with oxygen electrode ( O E ) measurements in a dog isolated colon preparation, using variable perfusion measured with an electromagnetic flow probe. At maximum flow, LD measurements were made at three sites to compare mucosal with serosal readings. Flow rate was varied (1-38 mllmin) and measurements of microcirculatory flux obtained using LD, and of oxygen tension using a serosal OE. A progressive trend towards increasing flux was demonstrated from caecum to rectum-serosa: 46.8 f 18.7 V (caecum), 52-6 k 17.9 V (mid-colon) and 61.3 f 17.6 V (rectum). A parallel trend was observed in mucosal values: 41.1 f 18.2 V (caecum), 45 .7 f 15.2 V (mid-colon) and 54-1 f 15.1 V (rectum). At all sites, serosal and mucosal values were not signijicantly different (Student’s t test). LD serosal values correlated signijicantly with EM flow (r =0.544, 0-01 > P> 0.001). A similar linear correlation was found between O E and EM flow (r =0*65, P < 0.001). Oxygen tension measurements varied as expected with microcirculatory f lux (r = 0.441, 0.02> P > 0.01). Endoscopic LD assessment of colonic microcirculation accurately reflects changes in blood flow. Keywords: Colonic blood flow, oximetry, laser Doppler
Most of our knowledge about microcirculation has been gained indirectly from experimental results extrapolated to the human, or from in uitro studies on micro-anatomy. A new instrument, laser Doppler, uses a fibreoptic probe small enough to pass along the biopsy channel of a flexible endoscope, perhaps permitting in uiuo studies of gastrointestinal mucosal perfusion in Datients.
(Perimed, Sweden) instrument was used, with the probe unheated and a gain of 1.
With a frequency limit (bandwidth) of 4 2 0 kHz, mean flux after 44 readings was 37.6k0.49 v (+s.d.); coefficient of variation for this bandwidth was 1.25 per cent. When the experiment was repeated using a bandwidth of 12-20 kHz, mean flux rose to 66.6 k 0.72 V; the coefficient of variation at this level was 1,1 per cent,
The laser Doppler technique of measuring blood flow was developed by two groups, Watkins and Holloway’ in America and Nilsson, Tenland and Oberg’ in Sweden. Briefly, according to the Doppler principle, any radiation which is reflected from a moving object undergoes a shift in frequency, and therefore also in wavelength. In the case of light, this is shifted towards the red end of the spectrum. In the laser Doppler instrument, coherent light is generated by a helium-neon source at 632.8 nm. This is directed at the tissue under study via a flexible optical fibre. All moving cells (principally red blood cells) within this volume of tissue will be struck by the light and will reflect some of it; the reflected light will be Doppler shifted and form an interference pattern with unshifted light reflected from stationary cells. The reflected light is collected in two more optical fibres, and returned to the instrument where it is then analysed mathematically to give a measure of the amount of cellular movement under the probe which is termed the flux. Flux is thus defined as the number of cells moving in the measured volume multiplied by the mean velocity of those cells. Since the erythrocytes in the capillaries are moving in many different directions, the instrument does not give a direct measure of tissue blood flow, and the flux is registered arbitrarily as the voltage output of the instrument (V).
We have evaluated this technique in the dog colon and compared it with an existing experimental method, oximetry.
Methods and results In vitro reproducibility Laser Doppler readings, at 5-s intervals, were made with the standard probe suspended in 20ml of milk (a uniform emulsion) at 10°C. The Pf2
In vivo reproducibility Six beagle dogs (average weight 14kg) were given 2.5g sodium picosulphate, then a fluid diet for 24 h. They were premedicated with barbiturate, then anaesthesia was induced with sodium pentobarbitone (25 mg/kg), an endotracheal tube passed, and the animals maintained on nitrous oxide and oxygen. The colon was exposed by a midline laparotomy and, starting at the pelvic brim, three silk sutures placed 5 cm apart were used to mark sites along the colon. Six readings were then made from each site using the standard LD probe held against the serosa by hand.
The results are shown in Table I. The mean coefficient of variation is 16.9 per cent.
Serosal compared with mucosal readings A caecostomy was created to pass a large Foley catheter (24 french) through which orthograde lavage of the colon was performed using warmed normal saline, until the effluent ran clear. The endoscopic probe was passed via the biopsy channel of a flexible endoscope (KeyMed), itselfpassed per rectum. At the same three sites, six further readings were recorded using the endoscopic probe held against the mucosa.
Mean serosal flux in the lower colon was 60.8k5.1 V which was not significantly different from the mean mucosalflux of 54.0k9.1 V (Student’s t test). In midcolon, mean serosal flux of 48.0& 15.3 V was similar to mean mucosal flux, 47.0&8.4V. This was also found in the upper colon-serosal flux 47.0& 15.1 V, mucosal flux 41.0k 13.9V.
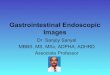
Variation of laser Doppler readings with arterial inflow That part of the descending colon supplied by the caudal mesenteric artery was identified and isolated by dividing the marginal artery at the limits ofits territory, and the bowel flush at the same level. The aorta was then cleared below the renal vessels and a ligature was placed distal to the origin of the caudal mesenteric artery. All direct aortic branches- mostly lumbar arteries-to this level were ligated (Figure 1) .
0007-1323/87/111053-03$3.00 0 1987 Butterworth & Co (Publishers) Ltd 1053
Endoscopic technique in gastrointestinal perfusion: P. I. M. Allen et al.
60-
40-
20-
Table 1 In vivo reprodircibility: LD readings at an equiualent colonic site in six indioiduals
Experiment Band-width no. ( k W Gain
Coefficient of variation LDV (mean+_s.d.) (V) ( %)
12 12 12 12 4
12
35.3 12.7 48.0+ 5.7 29.3+ 5.5 72.8 16.5 8 5 3 k 4.1 48.3+ 8.7
36.0 11.8 18.7 22.7 4.8
17.9
oxygen e lec t rode
Electrm f l O W D
Loser o m l e r Probe
Figure 1 Experimental preparation for flux and oximetry measurements with variable arterial inflow
Flow in the caudal mesenteric artery was measured using a 2.5 mm electromagnetic flow probe (Gould Electronics SP2204), and shown to be the same as flow in the aorta, using a 4.5 mm flow probe. Thereafter, flow was monitored in the aorta. A snare was placed distal to the probe, and inflow to the colon varied (1-38 ml/min).
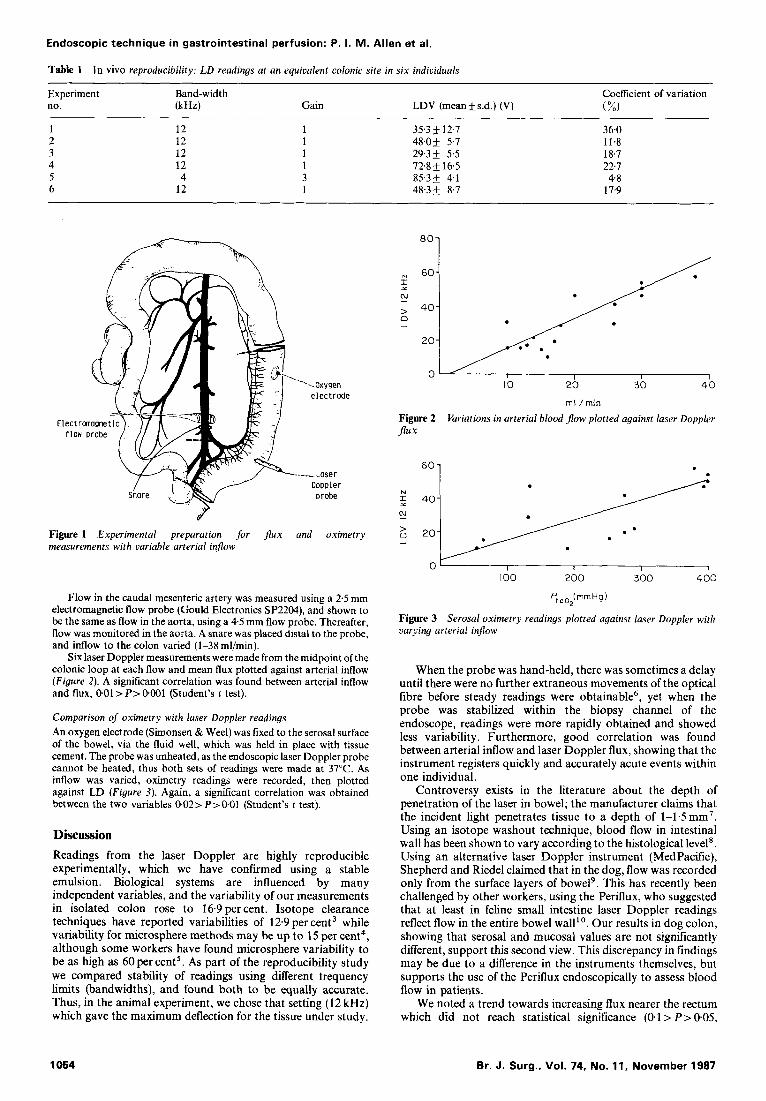
Six laser Doppler measurements were made from the midpoint of the colonic loop at each flow and mean flux plotted against arterial inflow (Figure 2). A significant correlation was found between arterial inflow and flux, 001 > P > 0401 (Student’s t test).
Comparison of oximetry with laser Doppler readings An oxygen electrode (Simonsen & Weel) was fixed to the serosal surface of the bowel, via the fluid well, which was held in place with tissue cement. The probe was unheated, as the endoscopic laser Doppler probe cannot be heated, thus both sets of readings were made at 37°C. As inflow was varied, oximetry readings were recorded, then plotted against LD (Figure 3) . Again, a significant correlation was obtained between the two variables 002> P>O.O1 (Student’s t test).
Discussion Readings from the laser Doppler are highly reproducible experimentally, which we have confirmed using a stable emulsion. Biological systems are influenced by many independent variables, and the variability of our measurements in isolated colon rose to 16.9 per cent. Isotope clearance techniques have reported variabilities of 12.9 per cent3 while variability for microsphere methods may be up to 15 per cent4, although some workers have found microsphere variability to be as high as 60percent5. As part of the reproducibility study we compared stability of readings using different frequency limits (bandwidths), and found both to be equally accurate. Thus, in the animal experiment, we chose that setting (12 kHz) which gave the maximum deflection for the tissue under study.
N
1 I
N
n > 1
*O1
rnl /min
Variations in arterial blood flow plotted against laser Doppler Figure 2 flux
6o 1
0‘ I I I 1
I00 200 300 400
pt c,2(rnrn Hg )
Figure 3 Serosal oximetry readings plotted against laser Doppler with uarying arterial inflow
When the probe was hand-held, there was sometimes a delay until there were no further extraneous movements of the optical fibre before steady readings were obtainable6, yet when the probe was stabilized within the biopsy channel of the endoscope, readings were more rapidly obtained and showed less variability. Furthermore, good correlation was found between arterial inflow and laser Doppler flux, showing that the instrument registers quickly and accurately acute events within one individual.
Controversy exists in the literature about the depth of penetration of the laser in bowel; the manufacturer claims that the incident light penetrates tissue to a depth of 1-1.5mm’. Using an isotope washout technique, blood flow in intestinal wall has been shown to vary according to the histological level’. Using an alternative laser Doppler instrument (MedPacific), Shepherd and Riedel claimed that in the dog, flow was recorded only from the surface layers of bowel’. This has recently been challenged by other workers, using the Periflux, who suggested that at least in feline small intestine laser Doppler readings reflect flow in the entire bowel wall’’. Our results in dog colon, showing that serosal and mucosal values are not significantly different, support this second view. This discrepancy in findings may be due to a difference in the instruments themselves, but supports the use of the Periflux endoscopically to assess blood flow in patients.
We noted a trend towards increasing flux nearer the rectum which did not reach statistical significance (0.1 > P > 005,
Br. J. Surg., Vol. 74, No. 11, November 1987 1054

Endoscopic technique in gastrointestinal perfusion: P. I. M. Allen et al.
Student’s t test), possibly because of insufficient numbers. Significant variation in blood flow within one organ has been reported recently”, but there are as yet no studies on the human colon.
Capillary circulation is known to be affected by invasive methods of measuring tissue blood flow” and we therefore chose to compare laser Doppler with oximetry because both are non-invasive. Shandall has shown experimentally that oxygen tension in the colon relates closely to tissue blood flow, and can predict healing of anastomoses’ 3. A significant association between flux and oxygen tension was demonstrated, but was not absolute since oxygen tension depends on metabolic variables as well as tissue perfusion. Comparison with the radio- active xenon washout technique failed to demonstrate reproducible results because of the difficulty of placing the injection of xenon accurately within the bowel wall, the instability of the isotope in saline solution and its affinity for fat in the bowel mesentery.
This new endoscopic method now seems appropriate for use in patients and we are currently mapping gastrointestinal blood flow in normal volunteers with a view to studying the effect of pathological states and therapeutic manoeuvres on capillary circulation.
Acknowledgements This work was supported in part by the West Midlands Regional Health Authority through a Sheldon grant to P. I. M. Allen, and by the Mason Medical Foundation who generously provided an equipment grant. We also thank Dr J. F. Sharp for his surgical assistance.
References 1 . Watkins D, Holloway GA Jnr. An instrument to measure
cutaneous blood flow using the Doppler shift of laser light. IEEE
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
Trans Biomed Eng 1978; 25: 28-33. Nilsson GE, Tenland T, Oberg PA. Evaluation ofa laser Doppler flowmeter for measurement of tissue blood flow. IEEE Trans Biomed Eng 1980; 27: 597-604. Forrester DW, Spence VA, Walker WF. The measurement of colonic mucosalsubmucosal blood flow in man. J Physiol 1980; 299: 1-11. Hales JRS. Radioactive microsphere techniques for studies of the circulation. Clin Exp Pharm Physiol 1974; Suppl 1 : 3146. Neutze JM, Wyler F, Rudolph AM. Use of radioactive microspheres to assess distribution of cardiac output in rabbits. Am J Physiol 1968; 215; 48695. Feld AD, Fondacaro JD, Holloway GA Jnr, Jacobson ED. Laser Doppler velocimetry : a new technique for the measurement of intestinal mucosal blood flow. Gastro Endoscopy 1984; 30: 225- 30. Perimed KB, Stockholm. PeriJlux PF2 User’s Handbook 1985; Ed 1: 11. Kampp M, Lundgren D. Blood flow and flow distribution in the small intestine of the cat as analysed by the KrS5 washout technique. Acta Physiol Scand 1968; 72: 282-97. Shepherd AP, Riedel GL. Continuous measurement of intestinal mucosal blood flow by laser Doppler velocimetry. Am J Physiol
Ahn H, Lindhagen J, Nilsson GE, Salerud EG, Jodal M, Lundgren D. Evaluation of laser Doppler flowmetry in the assessment of intestinal blood flow in cat. Gastroenterology 1985;
Ahn HC. Measurement of gastrointestinal blood flow with laser Doppler flowmetry. Linkoping University Medical Dissertation No. 226 1986; 135. Holloway GA Jnr. Cutaneous blood flow responses to injection trauma measured by laser Doppler flowmetry. J Invest Dermatol 1980; 74: 1 4 . Shandall A, Lowndes R, Young HL. Colonic anastomosis healing and oxygen tension. Br J Surg 1985; 72: 606-9.
1982; 242: 6668-72.
88: 951-7.
Paper accepted 21 June 1987
Br. J. Surg., Vol. 74, No. 11, November 1987 1055
Recommended