Looking ForwardA AMA P tiAn AMA Perspective
Alliance of Independent AcademicAlliance of Independent Academic Medical Centers Annual Meeting
March 26 2010March 26, 2010Paul Rockey, MD, MPH
Director Graduate Medical EducationDirector, Graduate Medical Education

Today’s Themes . . .
• AMA Strategic Issues• AMA Strategic Issues • AMA Advocacy Agenda • Physician Workforce and GME• International IssuesInternational Issues• 100 Year Shadow of Flexner

The DoctorThe DoctorThe DoctorThe DoctorBy Samuel Luke Fildes, 1891
AMA Strategic Issues
• Access• Access • Quality• Cost• Prevention and WellnessPrevention and Wellness• Payment Models
AMA Advocacy Agenda
• Voice for the uninsured• Funding research and medical
education, especially GME, p y• Expand Title VII and NHSC programs• Patient-centered medical homes and• Patient-centered medical homes and
accountable care organizations
www.ama-assn.org/ama/pub/advocacy/current-topics-advocacy.shtml

AMA HSR Advocacy Agenda
• Medical liability reform• Medicare physician payment reform and
regulatory relief• Quality, affordable health care for all• Combat third-party interference with
physician-patient relationship• Medicare balance billing• Improving the health of the public• Patient safety and quality improvementPatient safety and quality improvement
FL3

Slide 6
FL3 Fred Lenhoff, 2/11/2010
Upcoming AMA Reports
Securing Funding for GME• Securing Funding for GME• Primary Care & Medical Home Model• Maintenance of Certification/
Maintenance of Licensure• Visa and Licensure Process for IMG
Residents• Employment Benefits for Residents
and Fellows
Physician Workforce and GME
• U S physicians per capita• U.S. physicians per capita• Physician workforce shortages• Demand vs. supply• GME funding issuesGME funding issues• COGME’s recommendations• MedPAC issues related to GME

U.S. Physicians per Capita
276 283300
MDs to 100,000
202
276 283
250
300
175
125140
202
150
200
50
100
0
50
1900 1930 1960 1980 2000 20101900 1930 1960 1980 2000 2010Year

States Reporting Physician Shortages
• Montana (2009)• New Jersey (2009)
• North Carolina (2007)• Virginia (2007)
• California (2008)• Georgia (2008)• Maryland (2008)
• Alaska (2006)• Michigan (2006)• New Mexico (2006)y ( )
• Massachusetts (2008)• Minnesota (2008)• Nebraska (2008)
• New Mexico (2006)• Nevada (2006)• Utah (2006)
• Nebraska (2008)• Pennsylvania (2008)• Colorado (2007)
( )
• Arizona (2005)• Florida (2005)• Oregon (2004)• Kentucky (2007)
• Idaho (2007)• Iowa (2007)
• Oregon (2004)• Wisconsin (2004)• Mississippi (2003)
• New York (regional) (2007) • Texas (2002)

Specialties Reporting Shortages
• Gastroenterology (2009)• Thoracic Surgery (2009)
• Child Psychiatry (2006) • Critical Care Workforce
• General Surgery (2008)• Generalist Physicians
(2008)
(2006)• Emergency Medicine
(2006)(2008)• Geriatric Medicine (2008)• Oncology (2007)
• Family Medicine (2006)• Neurosurgery (2005)
C di l (2004)• Pediatric Subspecialties (2007)
• Public Health (2007)
• Cardiology (2004)• Dermatology (2004)• Medical Genetics (2004)( )
• Rheumatology (2007)• Allergy and Immunology
(2006)
( )• Anesthesiology (2003)• Endocrinology (2003)
P hi t (2003)(2006) • Psychiatry (2003)
Drivers of Future Demand for U.S. Physicians
• Population growth: 25 million/decade• Population growth: 25 million/decade • Aging population: Over 65s will double
2000 2030 major illness/chronic illness2000-2030, major illness/chronic illness • Public expectations: Boomers have
more resources and higher expectationsmore resources and higher expectations • Lifestyle factors: e.g., obesity, diabetes • Economic growth of nation• Medical advances: cut both ways
Future Physician Supply
• Medical school (MD) enrollment doubled from• Medical school (MD) enrollment doubled from 1960 to 1980, then flat for 20+ years
• ~ 19 000 MDs & DOs graduate each year 19,000 MDs & DOs graduate each year• Aging of physician workforce and retirement
• Gender and generational differences• Gender and generational differences
• Residency positions key to future supply
• International migration and IMG policies
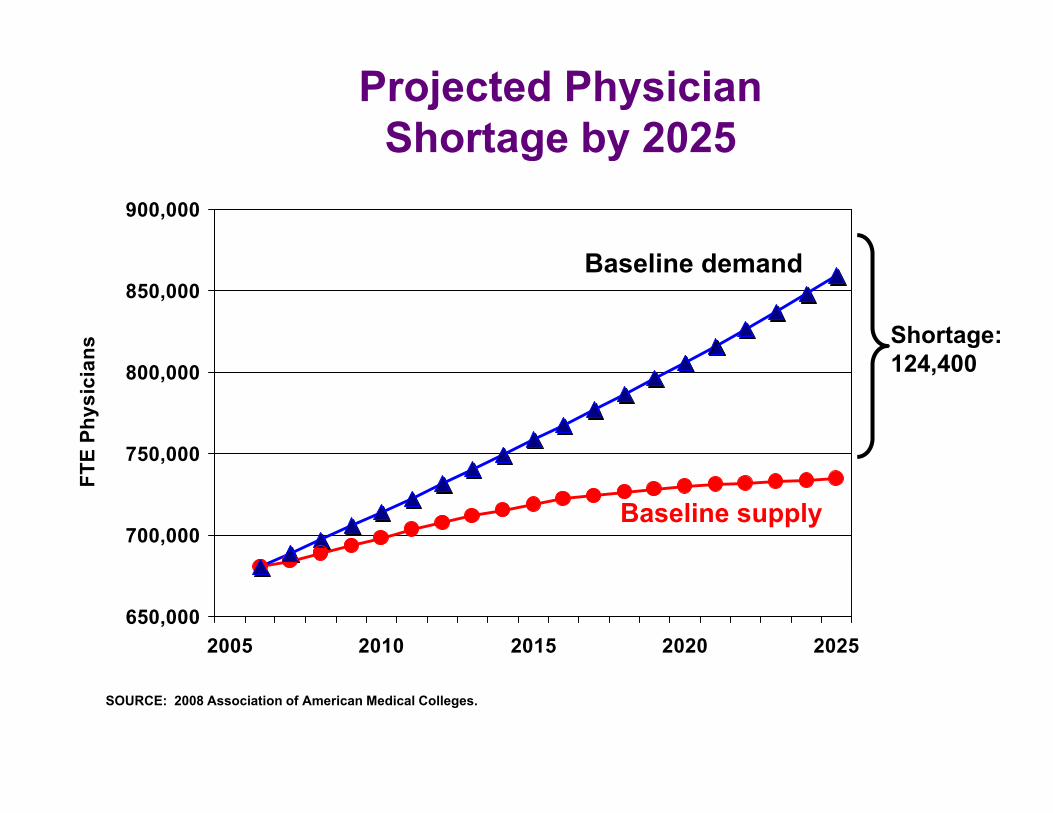
Projected Physician Shortage by 2025
900,000
Shortage by 2025
850,000
ns
Baseline demand
Shortage:124 400
750 000
800,000
E Ph
ysic
ian 124,400
700,000
750,000
FTE
Baseline supply
650,0002005 2010 2015 2020 2025
SOURCE: 2008 Association of American Medical Colleges.
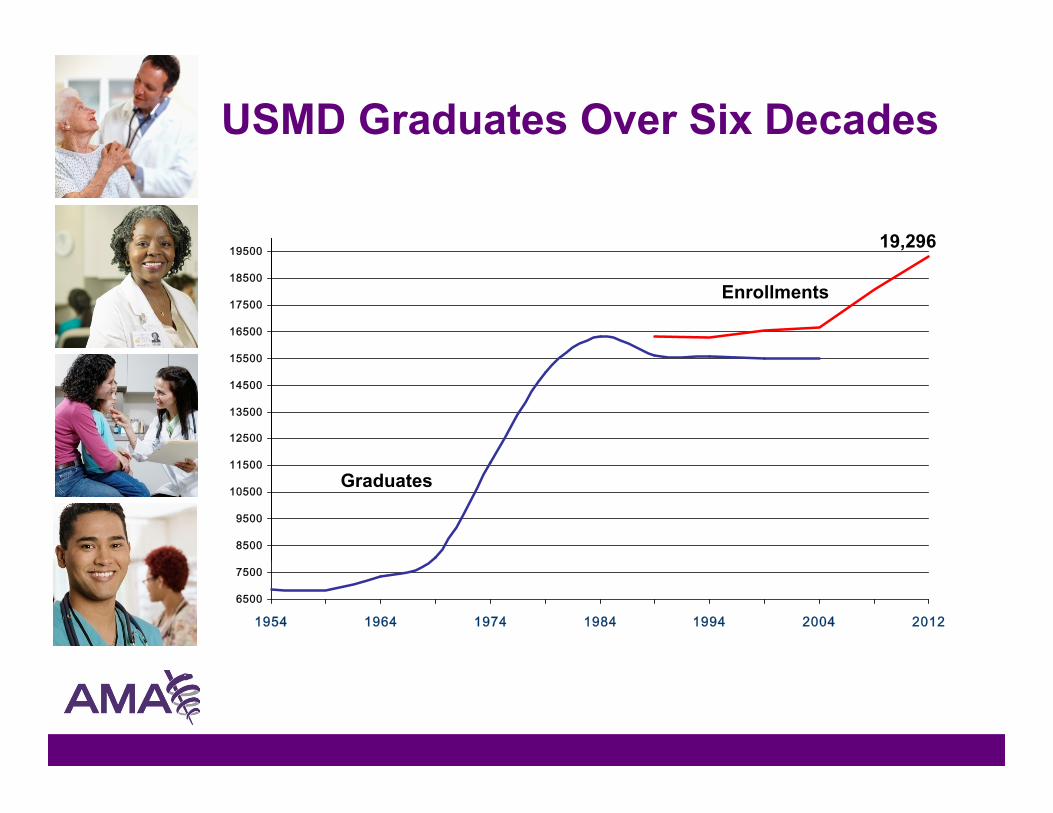
USMD Graduates Over Six Decades
19500 19,296
15500
16500
17500
18500
19500
Enrollments
12500
13500
14500
15500
8500
9500
10500
11500Graduates
6500
7500
1954 1964 1974 1984 1994 2004 2012

The Number of Active Physicians Approaching R ti t A i I i Sh l
30,000
s
Retirement Age is Increasing Sharply
22 52623,902
20 000
25,000
Phys
icia
ns 25,000 Physicians Enter Training Each Year
Number of Physicians Reaching Age 63
22,526(2025)
(2017)
15,000
20,000
of A
ctiv
e P
13,708(2008)10,000
Num
ber
5,0002008 2010 2012 2014 2016 2018 2020 2022 2024
Source: AMA Physician Masterfile (January 2008)Source: AMA Physician Masterfile (January 2008)

One Out of Three Would Retire Today if They Could Afford to
Percent of active physicians over 50 who would retire today, by age
42% 41%
33%40%
50%
33%
21%16%
32%
20%
30%
16%12%
10%
20%
0%50-54 55-59 60-64 65-69 70-74 75+ Total
Age CategoryAge Category
Source: 2006 AAMC/AMA Survey of Physicians 50 and Over

Percentage of Women in Medicine i Ri i St dilis Rising Steadily
42% 44% 45% 46% 47%40%45%50%
e
Medical School Graduates
29%34%
39%
27% 28% 29%25%30%35%
t F
em
ale
23%
13%15%
20%23% 24%
27% 28%
10%15%20%
Pe
rce
nt
Practicing MDs
10%13%
0%5%
10%
1980 1985 1990 1995 2000 2002 2003 2004 20051980 1985 1990 1995 2000 2002 2003 2004 2005

Fixing U.S. Doctor Shortage Requires More GME Slots
I 1997 M di l d f d d GME• In 1997, Medicare placed caps on funded GME positions (~26,000 GY1s per year)
• GME: only path to U S Physician licensureGME: only path to U.S. Physician licensure • ~ 19,000 MDs and DOs graduate each year• Increasing class sizes, 12 new MD schoolsIncreasing class sizes, 12 new MD schools• 30% increase = 5,700 more U.S. graduates • Unless GME expands, U.S. MDs and DOs will U ess G e pa ds, U S s a d Os
compete with IMGs for the same slots
GME Funding Sources
• Medicare supports 40% of total costMedicare supports 40% of total cost• Medicaid (annual state appropriations
and matching federal payments)and matching federal payments)• Veterans Administration (10% of
residents)residents)• Department of Defense
P i t (b t hifti )• Private payers (by cost shifting)
Council on Graduate Medical Education Recommendations
• Move more physician training to non-Move more physician training to non-hospital settings, including rural and underserved areas
• Make teaching hospitals/academic medical centers more accountable for CMS funding
• Fix the income disparity between p yprimary care and specialist physicians
• Make GME a site for innovations in primary care

Other GME Funding Issues
• Need to expand GME positions to keep up with medical school expansion
• Need for innovative training models to address community needs and contemporary models of health care (medical home/chronic care models)(medical home/chronic care models)
• New and emerging DME costs (technology resident duty hour(technology, resident duty hour restrictions, etc.)

MedPAC Issues Related to GME
• Increasing accountabilityg y• Broadening training settings• Creating career incentives for• Creating career incentives for
residents• Alternative financing models• Alternative financing models• Economic incentives (team-based
care faculty expertise costcare, faculty expertise, cost awareness, cultural competencies, community-based affiliations)y )

International Issues• IMGs – why the concern now?
S it I t ti l A ti iti• Summit on International Activities• International Accreditation of Medical
Ed tiEducation• International Medical Workforce
C ll b ti (IMWC)Collaborative (IMWC)• World Health Professions’ Conference
R l ti (WHPCR)on Regulation (WHPCR)• A local angle

IMGs – Why the concern now?
• IMGs account for 25.9% of total physiciansy• Global shortages of health personnel• Brain drain from less-developed countries • 1 of 4 doctors in GME is non-U.S. IMG • About 2,500 U.S. citizens per year enter
foreign med schools, mostly Caribbean• 1,500 U.S. IMGs enter U.S. GME annually
V i bili i li f f i d h l• Variability in quality of foreign med schools and IMG graduates
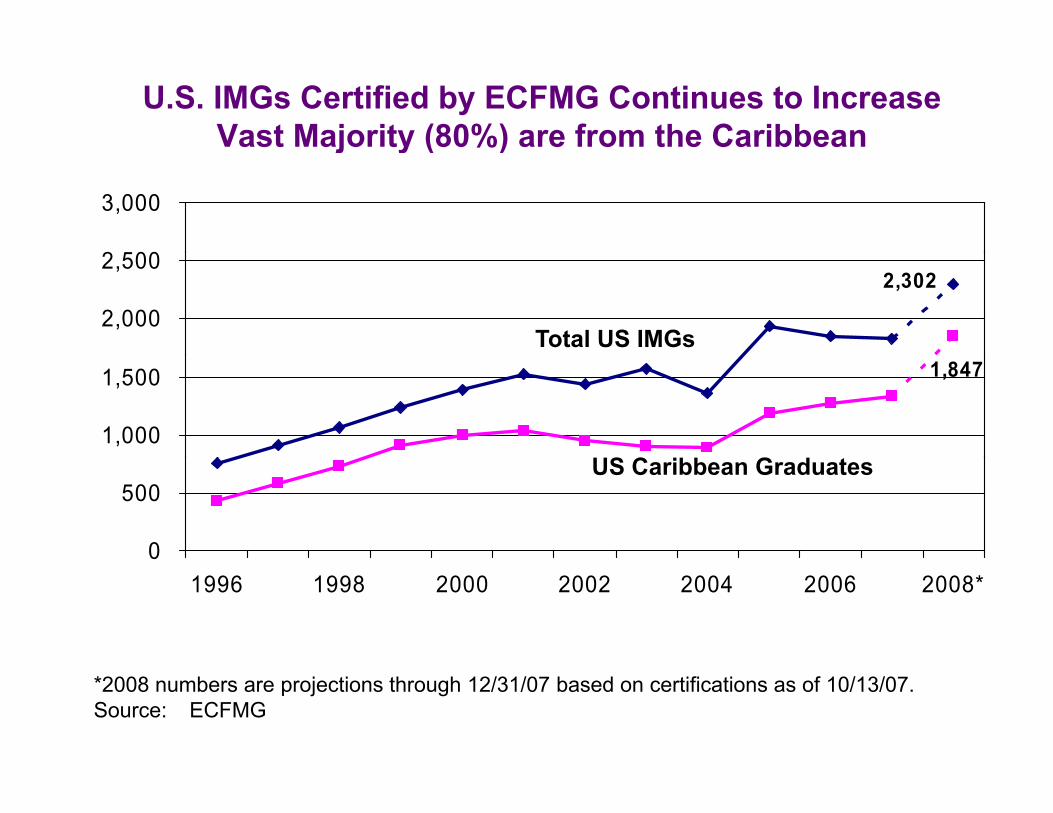
U.S. IMGs Certified by ECFMG Continues to IncreaseVast Majority (80%) are from the Caribbean
2 500
3,000
j y ( )
2,302
2,000
2,500
Total US IMGs1,847
1,000
1,500
US C ibb G d t
0
500US Caribbean Graduates
1996 1998 2000 2002 2004 2006 2008*
*2008 numbers are projections through 12/31/07 based on certifications as of 10/13/07.Source: ECFMG

Variability of Medical Education by Caribbean Medical Schools
• 55 medical schools in Caribbean55 medical schools in Caribbean• Tuition funded – U.S. DOE student loans• No teaching hospitals – buy U.S. clerkshipsNo teaching hospitals buy U.S. clerkships• Lower pass rates on first-attempt of USMLE• Compete with U.S. graduates and non-U.S. p g
citizen IMGs for U.S. residency positions • U.S. citizen IMG entry to residency enhanced
b E li h fi i U S li i l t i iby English proficiency, U.S. clinical training, no visa requirements

ECFMG Summit on International Activities
I t ti l di l h l t d d• International medical school standards • International GME standards• Accreditation of medical schools and
residency training programs• Licensing and MOL• Certification and MOC• Accreditation of hospitals
International Accreditation of Medical Education
• Undergraduate medical education (Cornell: Qatar; Duke: Singapore)
• UME Accreditation (WFME, FAIMER)• GME (ACGME and Singapore)• Teaching hospitals (Joint Commission)• Specialty medicine (ABMS)Specialty medicine (ABMS)
International Medical Workforce Collaborative
• Team based models of primary medical care and• Team-based models of primary medical care and complex care management (Australia)
• Social mission of medical schools in time of expansion (US)
• Optimizing medical workforce through improved t ffi i & h i i t i i (C d )system efficiency & physician training (Canada)
• Reducing physician requirements by improving practice and organizational efficiency (UK)practice and organizational efficiency (UK)
www.rcpsc.medical.org/publicpolicy/imwc.php/p g p p y p p

World Health Professions’ Conference on Regulation
E l d i d f t f h lth• Explore a desired future for health professional regulation
• Examine regulatory and professional• Examine regulatory and professional issues related to international migration of health professionals
• Evaluate the relationships among health professional education,
l ti d t d d f tiregulation, and standards of practice
www whpa org/whpcr2010/www.whpa.org/whpcr2010/

Ochsner – University of Queensland School of Medicine Collaboration
• New medical school program for U S citizens• New medical school program for U.S. citizens• 2 years of pre-clinical education at University of
Queensland in Australia • 2 years of clinical instruction at Ochsner in
Louisiana
• Emphasis on primary care in the curriculumEmphasis on primary care in the curriculum • 16 U.S. medical students in 2009, 37 students
in 2010, reaching 120 admissions/yr in 2013• Goal is to reduce physician shortages in
Louisiana and the Gulf South
AMA Founded in 1847
Shadow of Flexner
Flexner Report Transformed Medical Education in the United States
Th M di l C TThe Medical Care Team

Recommended