Embed Size (px)
Citation preview
Reference Committee F
BOT Report(s)
01 Annual Report 04 AMA 2018 Dues 10 Creation of an AMA Fund for Physician Candidates 16 Oppose Physician Gun Gag Rule Policy by Taking our AMA Business Elsewhere 17 Equality for Future Meetings Organized or Sponsored by the AMA
Resolution(s)
601 Reinstate the AMA Commission to End Health Care Disparities 602 Studying Healthcare Institutions that Provide Child Care Services 603 Sexual Orientation and Gender Identity Demographic Collection by the AMA 604 High Cost to Authors for Open Source Peer Reviewed Publications 605 Pronunciation of Pharmaceutical Names
REPORT OF THE BOARD OF TRUSTEES
B of T Report 1-A-17
Subject: Annual Report Presented by:
Patrice A. Harris, MD, MA, Chair
Referred to:
Reference Committee F
(Gary R. Katz, MD, MBA, Chair) The Consolidated Financial Statements for the years ended December 31, 2016 and 2015 and the 1 Independent Auditor’s report have been included in a separate booklet, titled “2016 Annual 2 Report.” This booklet is included in the Handbook mailing to members of the House of Delegates 3 and will be discussed at the Reference Committee F hearing. 4
© 2017 American Medical Association. All rights reserved.
2016 Annual Report
American Medical Association 2016 Annual Report | 1
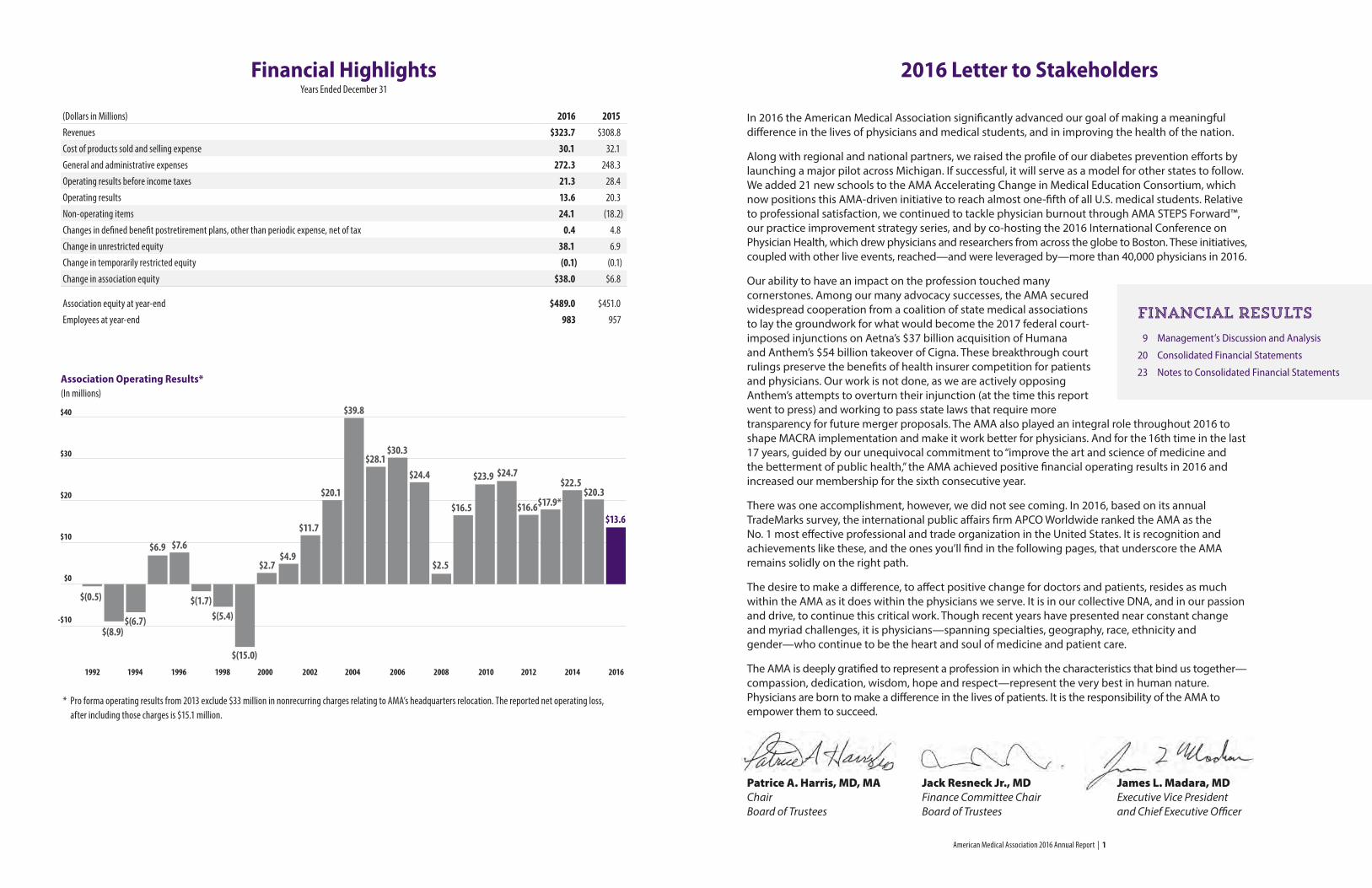
2016 Letter to StakeholdersFinancial HighlightsYears Ended December 31
(Dollars in Millions) 2016 2015Revenues $323.7 $308.8
Cost of products sold and selling expense 30.1 32.1
General and administrative expenses 272.3 248.3
Operating results before income taxes 21.3 28.4
Operating results 13.6 20.3
Non-operating items 24.1 (18.2)
Changes in defined benefit postretirement plans, other than periodic expense, net of tax 0.4 4.8
Change in unrestricted equity 38.1 6.9
Change in temporarily restricted equity (0.1) (0.1)
Change in association equity $38.0 $6.8
Association equity at year-end $489.0 $451.0
Employees at year-end 983 957
$40
$30
$20
$10
$0
-$10
$(0.5)
$(8.9)$(6.7)
$(1.7)$(5.4)
$(15.0)
$6.9 $7.6
$2.7$4.9
$11.7
$20.1
$39.8
$28.1$30.3
$24.4
$2.5
$16.5
$23.9 $24.7
$16.6$17.9*
$22.5$20.3
$13.6
Association Operating Results* (In millions)
* Pro forma operating results from 2013 exclude $33 million in nonrecurring charges relating to AMA’s headquarters relocation. The reported net operating loss, after including those charges is $15.1 million.
1992 1994 1996 1998 2000 2002 2004 2006 2008 2010 2012 2014 2016
9 Management’s Discussion and Analysis
20 Consolidated Financial Statements
23 Notes to Consolidated Financial Statements
Financial results
In 2016 the American Medical Association significantly advanced our goal of making a meaningful difference in the lives of physicians and medical students, and in improving the health of the nation.
Along with regional and national partners, we raised the profile of our diabetes prevention efforts by launching a major pilot across Michigan. If successful, it will serve as a model for other states to follow. We added 21 new schools to the AMA Accelerating Change in Medical Education Consortium, which now positions this AMA-driven initiative to reach almost one-fifth of all U.S. medical students. Relative to professional satisfaction, we continued to tackle physician burnout through AMA STEPS Forward™, our practice improvement strategy series, and by co-hosting the 2016 International Conference on Physician Health, which drew physicians and researchers from across the globe to Boston. These initiatives, coupled with other live events, reached—and were leveraged by—more than 40,000 physicians in 2016.
Our ability to have an impact on the profession touched many cornerstones. Among our many advocacy successes, the AMA secured widespread cooperation from a coalition of state medical associations to lay the groundwork for what would become the 2017 federal court-imposed injunctions on Aetna’s $37 billion acquisition of Humana and Anthem’s $54 billion takeover of Cigna. These breakthrough court rulings preserve the benefits of health insurer competition for patients and physicians. Our work is not done, as we are actively opposing Anthem’s attempts to overturn their injunction (at the time this report went to press) and working to pass state laws that require more transparency for future merger proposals. The AMA also played an integral role throughout 2016 to shape MACRA implementation and make it work better for physicians. And for the 16th time in the last 17 years, guided by our unequivocal commitment to “improve the art and science of medicine and the betterment of public health,” the AMA achieved positive financial operating results in 2016 and increased our membership for the sixth consecutive year.
There was one accomplishment, however, we did not see coming. In 2016, based on its annual TradeMarks survey, the international public affairs firm APCO Worldwide ranked the AMA as the No. 1 most effective professional and trade organization in the United States. It is recognition and achievements like these, and the ones you’ll find in the following pages, that underscore the AMA remains solidly on the right path.
The desire to make a difference, to affect positive change for doctors and patients, resides as much within the AMA as it does within the physicians we serve. It is in our collective DNA, and in our passion and drive, to continue this critical work. Though recent years have presented near constant change and myriad challenges, it is physicians—spanning specialties, geography, race, ethnicity and gender—who continue to be the heart and soul of medicine and patient care.
The AMA is deeply gratified to represent a profession in which the characteristics that bind us together—compassion, dedication, wisdom, hope and respect—represent the very best in human nature. Physicians are born to make a difference in the lives of patients. It is the responsibility of the AMA to empower them to succeed.
Patrice A. Harris, MD, MA Jack Resneck Jr., MD James L. Madara, MD Chair Finance Committee Chair Executive Vice President Board of Trustees Board of Trustees and Chief Executive Officer
American Medical Association 2016 Annual Report | 2 American Medical Association 2016 Annual Report | 3
Protecting patient careDeemed a threat to affordability, accessibility and quality of health care, two insurance mergers—Anthem’s acquisition of Cigna and Aetna’s acquisition of Humana—were blocked in court thanks, in large part, to the AMA’s powerful advocacy efforts and unique capacity to rally and coordinate state-level legislative support.
In another meaningful win for patients, our ongoing Truthinrx.org national campaign generated tremendous engagement and momentum when an AMA petition calling on Congress to act on drug pricing garnered more than 100,000 signatures from activists nationwide.
Confronting the opioid epidemicOur efforts to reverse the nation’s opioid epidemic in 2016 helped drive a strong, united effort from physicians across the country, one that delivered such tangible results as increasing the number of physicians who are registered for and access state prescription drug monitoring programs, naloxone access expanding in nearly every state, and more than 9,000
should be held in their roles as healers, educators, scientists and leaders. The first comprehensive review and update of the Code in 50 years, this resource now offers even more timely and relevant guidance to physicians.
Advancing digital healthTo help ensure the physician voice is represented in the design and implementation of such digital health technology sectors as the mobile health application market, the AMA in 2016 formally announced its founding participation in Xcertia—the new industry collaborative initiated by the AMA, the American Hospital Association, the DHX Group and the Healthcare Information and Management Systems Society (HIMSS). By representing the wisdom and interests of diverse stakeholders, Xcertia aims to develop guidance and to help improve the quality, safety and effectiveness of the fast-expanding mobile health app sector.
... because that’s what leaders do.
physicians becoming certified to provide office-based treatment for opioid use disorders.
Transforming physician education In 2016 the AMA published Health Systems Science, the first-ever textbook to support this fast-emerging third pillar of medical education. Joining basic and clinical sciences, this newest curriculum pillar provides information on health care delivery, quality improvement, patient safety, social determinants of health and other topics relevant to the effective practice of medicine in the 21st century.
Improving health outcomesThe AMA’s efforts to create awareness for both prediabetes and the National Diabetes Prevention Program (National DPP) earned an impressive vote of confidence in 2016 when the secretary of U.S. Department of Health and Human Services extended coverage for the National DPP to all Medicare beneficiaries. This marks the first time ever that a preventive service model from the Centers for Medicare & Medicaid Services (CMS) Innovation Center became eligible for the Medicare program.
Also, the AMA’s national prediabetes awareness campaign, DoIHavePrediabetes.org, developed in partnership with the Centers for Disease Control and Prevention, the American Diabetes Association and the Ad Council, resulted in a million people visiting the site and more than 340,000 taking a simple prediabetes assessment to understand their risk, far surpassing the original goal.
Additionally, in our most significant blood pressure control effort to date, the AMA, in collaboration with the American Heart Association (AHA), launched Target:BP, an initiative to improve blood pressure control across the nation. Many physician practices and health systems have joined the effort and, together, the AHA and AMA are providing physicians and care teams with a platform for data sharing, and for accessing resources and evidence-based tools.
Modernizing ethics guidelinesEight years in the making, we launched the updated AMA Code of Medical Ethics. The Code has long articulated the values that ground the profession and the expectations to which physicians
American Medical Association 2016 Annual Report | 4 American Medical Association 2016 Annual Report | 5
... so physicians can focus on patient care.
Navigating payment reformFollowing the landmark passage of the Medicare Access and CHIP Reauthorization Act (MACRA), the AMA provided the valuable physician point of view to CMS as it shaped its new payment models. Fully articulated in CMS’s final regulations were all six AMA objectives, including the ability for physicians to pick their pace of participation during the transition year. In addition, by providing doctors with tools such as the AMA Payment Model Evaluator (apps.ama-assn.org/pme), we also assisted physician decision-making and participation in Medicare’s Quality Payment Program and in their making the larger move to value-based reimbursement.
Engaging physicians across the country From conducting one-on-one conversations to working with leading research firms using neuroscience techniques, the AMA connected with more than 7,000 physicians around the nation in 2016 to better understand their needs. The AMA is incorporating the learnings from these studies to develop new insights, products and services.
By rebuilding our AMA website (ama-assn.org) and redesigning
AMA Wire® (wire.ama-assn.org), our flagship e-newsletter, we provided physicians far easier access to relevant information and resources designed to help them succeed throughout every stage of their career.
Inspiring thought leadershipJAMA®, the Journal of the American Medical Association, continued to expand the intellectual richness of The JAMA Network® with the addition of two new specialty journals—JAMA Cardiology and JAMA Oncology—and the release of a new, cutting-edge website that is responsive to all browsers and devices.
Improving practice efficiencyIn 2016 we continued to expand and enhance our AMA STEPS Forward™ practice improvement strategy series (stepsforward.org), which now offers more than 40 education and implementation modules that empower physicians and care teams to thrive in the new health care environment.
Furthering our practice efficiency efforts, the Annals of Internal Medicine published the AMA’s landmark study “Allocation of Physician Time in Ambulatory Practice: A Time and Motion Study in 4 Specialties.” This study highlights
data showing that for every hour physicians provide direct clinical face time to patients, nearly two additional hours are spent on EHR and desk work. The article was listed in Altmetrics’ “Top 100 Articles of 2016.”
Pioneering precision medicine To advance medicine and patient care through precision medicine, the AMA partnered with other entities to develop a series of online educational modules on genomics and precision medicine topics that offer free CME.
Connecting physicians and entrepreneurs In 2016 the AMA entered the final stages of beta testing a digital innovation matchmaking website. The AMA Physician Innovation Network (innovationmatch.ama-assn.org) is a new platform where physicians and entrepreneurs can connect online and collaborate on new digital health care solutions.
Keeping pace with molecular diagnostic testing We augmented our CPT® code set to comply with recent Protecting Access to Medicare Act regulations to support the consistent coding of an ever-expanding and complex area of molecular diagnostic testing.
American Medical Association 2016 Annual Report | 6 American Medical Association 2016 Annual Report | 7
By becoming fully immersed in the conversations taking place at MATTER, including two 13-week programs focused on analyzing significant problems facing health care, the AMA gained an amazing first-person view of the opportunities and challenges taking place at the intersection of technology and patient care.
At a grassroots level, we introduced a national innovation challenge that received nearly 400 submissions from physicians, residents and medical students about how to improve our nation’s health. We also marked our support of Sling Health, the student-run biotechnology incubator that supports cutting-edge medical technology development from the next generation of entrepreneurs at schools such as Washington University, Harvard University, Massachusetts Institute of Technology and University of Michigan.
Ensuring accurate physician dataIn 2016 the AMA and AMA Business Solutions (a wholly owned subsidiary of the American Medical
Growing the AMA innovation ecosystem Through partnerships, policy research and new product initiatives, we continued working with passionate health care professionals across various sectors in 2016 to expand our innovation ecosystem—an effort that is bridging the digital divide for physicians and helping them better understand, adapt and participate in the evolution underway.
We began the year with the launch of Health2047, our innovation company whose mission is to develop and achieve adoption of disruptive ideas that enhance, at the system level, the practice of health care. By combining the insights and skills of top innovators in medicine, technology and science with the deep knowledge of the AMA, Health2047 is poised to make health care delivery more effective and efficient.
At MATTER, the Chicago-based health care technology incubator that is now home to more than 130 digital start-ups, the AMA continued expanding our learning curve and our ability to connect physicians with entrepreneurs.
... because there’s strength in numbers.
the International Conference on Physician Health, which convened more than 400 physicians and researchers to explore the many facets of this complicated issue.
Extending transformation efforts The AMA’s CMS Transforming Clinical Practices Initiative grant was renewed for 2017. The grant expands our outreach to practices of all sizes by supporting their transformation efforts including their participation in Qualified Clinical Data Registries.
Expanding our reach in med ed In 2016, through its “Accelerating Change in Medical Education” initiative, the AMA continued to empower innovation by expanding its consortium to 32 schools and their combined coverage of 19,000 MD and DO medical students.
An example of the exciting innovations coming out of the consortium is the Indiana University SOM/Regenstrief Institute’s advanced teaching tool that covers the complexity of the electronic medical record environment.
Deployed at three medical schools in 2016, this teaching resource will expand to four additional schools in 2017.
Partnering with TEDMED The AMA returned to TEDMED in 2016 as a Global Association Partner. We enjoyed more than 400,000 impressions and engagements around this event on social media and an opportunity to showcase our work empowering physician-influenced innovation live at the TEDMED “Hive.”
Association), partnered with LexisNexis® to address the issue of inaccurate provider directories by developing a solution that combines data, technology and analytics to help ensure patients have accurate data to make decisions on health care coverage.
Championing physician wellnessThrough multiple, coordinated efforts the AMA advanced the critical issue of physician wellness. To ensure wellness is being discussed at the highest levels of the profession, we hosted a summit with leading health system CEOs with Cleveland Clinic, Johns Hopkins Medicine, Partners HealthCare, and others in attendance. In an effort to accelerate needed research on physician and staff well-being, we sponsored a practice transformation conference that attracted thought leaders and investigators to debate the issues and share insights. In partnership with the Canadian Medical Association and the British Medical Association, the AMA helped bring this important topic to the world stage by co-hosting
American Medical Association 2016 Annual Report | 9
Management’s Discussion and Analysis
IntroductionThe objective of this section is to help American Medical Association (AMA) members and other readers of our financial statements understand management’s views on the AMA’s financial condition and results of operations. This discussion should be read in conjunction with the audited consolidated financial statements and notes to the consolidated financial statements.
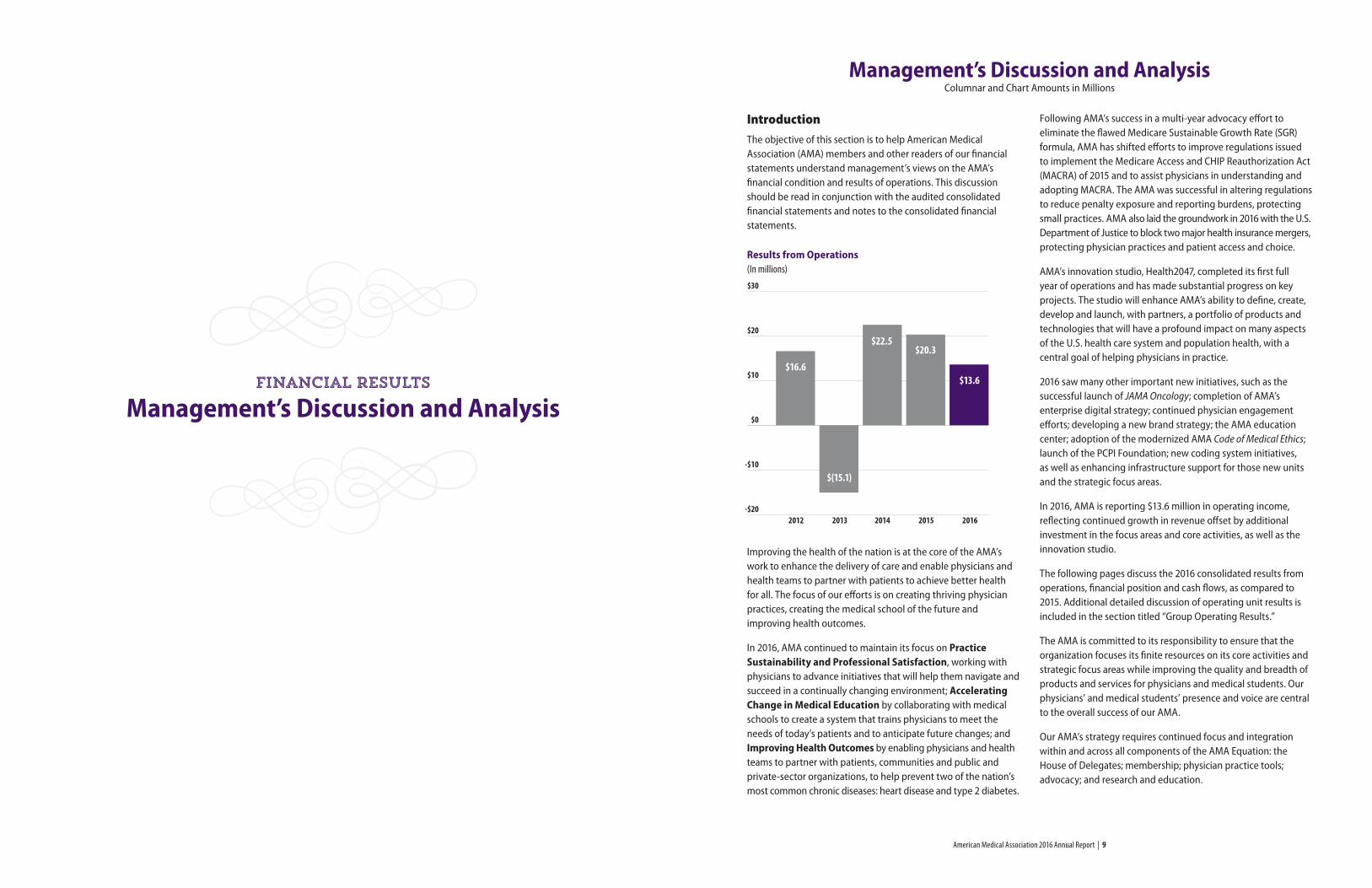
Results from Operations (In millions)
Improving the health of the nation is at the core of the AMA’s work to enhance the delivery of care and enable physicians and health teams to partner with patients to achieve better health for all. The focus of our efforts is on creating thriving physician practices, creating the medical school of the future and improving health outcomes.
In 2016, AMA continued to maintain its focus on Practice Sustainability and Professional Satisfaction, working with physicians to advance initiatives that will help them navigate and succeed in a continually changing environment; Accelerating Change in Medical Education by collaborating with medical schools to create a system that trains physicians to meet the needs of today’s patients and to anticipate future changes; and Improving Health Outcomes by enabling physicians and health teams to partner with patients, communities and public and private-sector organizations, to help prevent two of the nation’s most common chronic diseases: heart disease and type 2 diabetes.
Following AMA’s success in a multi-year advocacy effort to eliminate the flawed Medicare Sustainable Growth Rate (SGR) formula, AMA has shifted efforts to improve regulations issued to implement the Medicare Access and CHIP Reauthorization Act (MACRA) of 2015 and to assist physicians in understanding and adopting MACRA. The AMA was successful in altering regulations to reduce penalty exposure and reporting burdens, protecting small practices. AMA also laid the groundwork in 2016 with the U.S. Department of Justice to block two major health insurance mergers, protecting physician practices and patient access and choice.
AMA’s innovation studio, Health2047, completed its first full year of operations and has made substantial progress on key projects. The studio will enhance AMA’s ability to define, create, develop and launch, with partners, a portfolio of products and technologies that will have a profound impact on many aspects of the U.S. health care system and population health, with a central goal of helping physicians in practice.
2016 saw many other important new initiatives, such as the successful launch of JAMA Oncology; completion of AMA’s enterprise digital strategy; continued physician engagement efforts; developing a new brand strategy; the AMA education center; adoption of the modernized AMA Code of Medical Ethics; launch of the PCPI Foundation; new coding system initiatives, as well as enhancing infrastructure support for those new units and the strategic focus areas.
In 2016, AMA is reporting $13.6 million in operating income, reflecting continued growth in revenue offset by additional investment in the focus areas and core activities, as well as the innovation studio.
The following pages discuss the 2016 consolidated results from operations, financial position and cash flows, as compared to 2015. Additional detailed discussion of operating unit results is included in the section titled “Group Operating Results.”
The AMA is committed to its responsibility to ensure that the organization focuses its finite resources on its core activities and strategic focus areas while improving the quality and breadth of products and services for physicians and medical students. Our physicians’ and medical students’ presence and voice are central to the overall success of our AMA.
Our AMA’s strategy requires continued focus and integration within and across all components of the AMA Equation: the House of Delegates; membership; physician practice tools; advocacy; and research and education.
Management’s Discussion and AnalysisColumnar and Chart Amounts in Millions
$30
$20
$10
$0
-$10
-$20 2012 2013 2014 2015 2016
$16.6
$22.5$20.3
$13.6
$(15.1)
Financial results
American Medical Association 2016 Annual Report | 10 American Medical Association 2016 Annual Report | 11
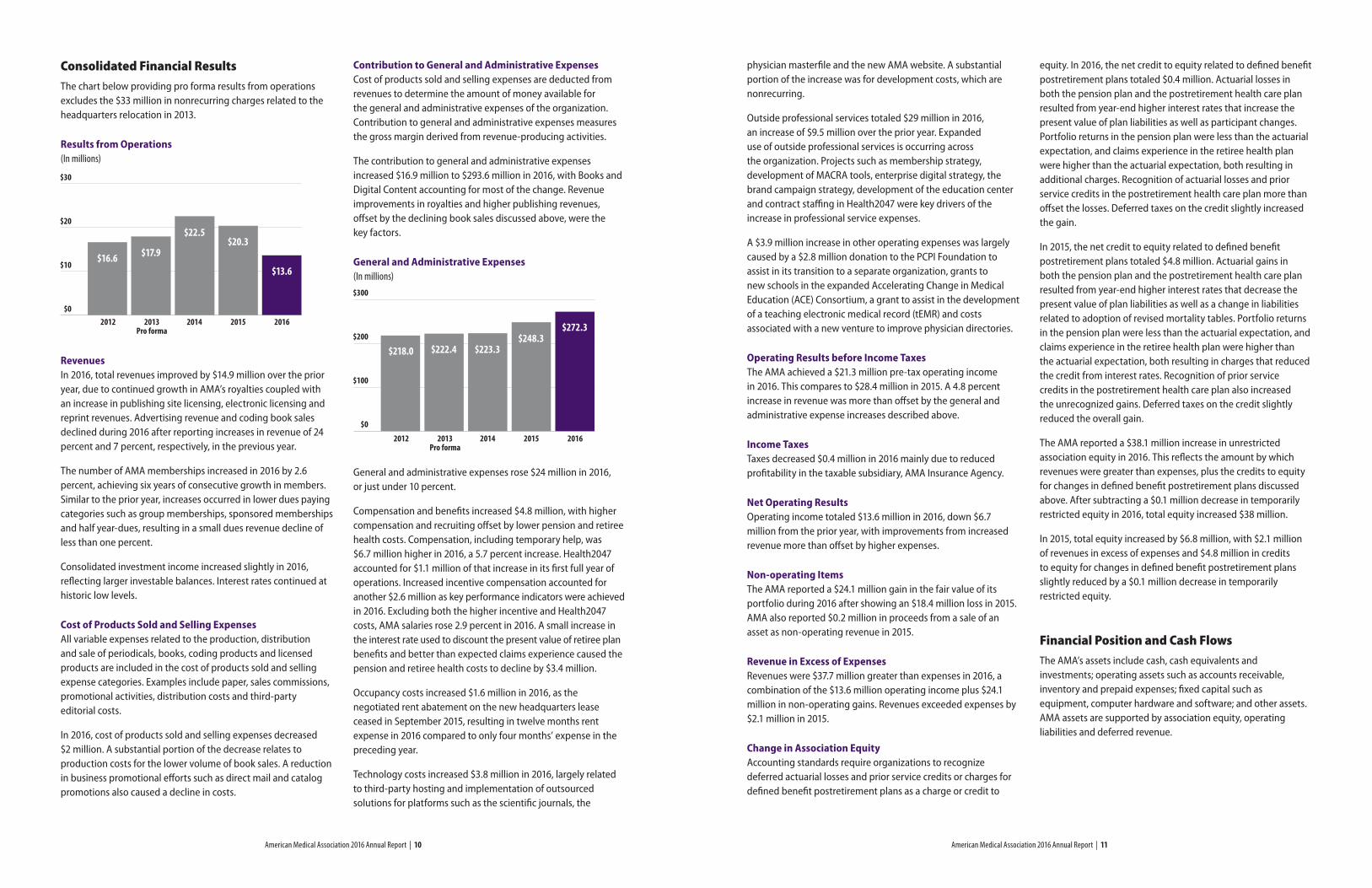
Consolidated Financial ResultsThe chart below providing pro forma results from operations excludes the $33 million in nonrecurring charges related to the headquarters relocation in 2013.
Results from Operations (In millions)
RevenuesIn 2016, total revenues improved by $14.9 million over the prior year, due to continued growth in AMA’s royalties coupled with an increase in publishing site licensing, electronic licensing and reprint revenues. Advertising revenue and coding book sales declined during 2016 after reporting increases in revenue of 24 percent and 7 percent, respectively, in the previous year.
The number of AMA memberships increased in 2016 by 2.6 percent, achieving six years of consecutive growth in members. Similar to the prior year, increases occurred in lower dues paying categories such as group memberships, sponsored memberships and half year-dues, resulting in a small dues revenue decline of less than one percent.
Consolidated investment income increased slightly in 2016, reflecting larger investable balances. Interest rates continued at historic low levels.
Cost of Products Sold and Selling ExpensesAll variable expenses related to the production, distribution and sale of periodicals, books, coding products and licensed products are included in the cost of products sold and selling expense categories. Examples include paper, sales commissions, promotional activities, distribution costs and third-party editorial costs.
In 2016, cost of products sold and selling expenses decreased $2 million. A substantial portion of the decrease relates to production costs for the lower volume of book sales. A reduction in business promotional efforts such as direct mail and catalog promotions also caused a decline in costs.
Contribution to General and Administrative ExpensesCost of products sold and selling expenses are deducted from revenues to determine the amount of money available for the general and administrative expenses of the organization. Contribution to general and administrative expenses measures the gross margin derived from revenue-producing activities.
The contribution to general and administrative expenses increased $16.9 million to $293.6 million in 2016, with Books and Digital Content accounting for most of the change. Revenue improvements in royalties and higher publishing revenues, offset by the declining book sales discussed above, were the key factors.
General and Administrative Expenses(In millions)
General and administrative expenses rose $24 million in 2016, or just under 10 percent.
Compensation and benefits increased $4.8 million, with higher compensation and recruiting offset by lower pension and retiree health costs. Compensation, including temporary help, was $6.7 million higher in 2016, a 5.7 percent increase. Health2047 accounted for $1.1 million of that increase in its first full year of operations. Increased incentive compensation accounted for another $2.6 million as key performance indicators were achieved in 2016. Excluding both the higher incentive and Health2047 costs, AMA salaries rose 2.9 percent in 2016. A small increase in the interest rate used to discount the present value of retiree plan benefits and better than expected claims experience caused the pension and retiree health costs to decline by $3.4 million.
Occupancy costs increased $1.6 million in 2016, as the negotiated rent abatement on the new headquarters lease ceased in September 2015, resulting in twelve months rent expense in 2016 compared to only four months’ expense in the preceding year.
Technology costs increased $3.8 million in 2016, largely related to third-party hosting and implementation of outsourced solutions for platforms such as the scientific journals, the
$30
$20
$10
$0 2012 2013 2014 2015 2016 Pro forma
$16.6 $17.9
$22.5$20.3
$13.6
$300
$200
$100
$0
2012 2013 2014 2015 2016 Pro forma
$218.0 $222.4 $223.3$248.3
$272.3
physician masterfile and the new AMA website. A substantial portion of the increase was for development costs, which are nonrecurring.
Outside professional services totaled $29 million in 2016, an increase of $9.5 million over the prior year. Expanded use of outside professional services is occurring across the organization. Projects such as membership strategy, development of MACRA tools, enterprise digital strategy, the brand campaign strategy, development of the education center and contract staffing in Health2047 were key drivers of the increase in professional service expenses.
A $3.9 million increase in other operating expenses was largely caused by a $2.8 million donation to the PCPI Foundation to assist in its transition to a separate organization, grants to new schools in the expanded Accelerating Change in Medical Education (ACE) Consortium, a grant to assist in the development of a teaching electronic medical record (tEMR) and costs associated with a new venture to improve physician directories.
Operating Results before Income TaxesThe AMA achieved a $21.3 million pre-tax operating income in 2016. This compares to $28.4 million in 2015. A 4.8 percent increase in revenue was more than offset by the general and administrative expense increases described above.
Income TaxesTaxes decreased $0.4 million in 2016 mainly due to reduced profitability in the taxable subsidiary, AMA Insurance Agency.
Net Operating ResultsOperating income totaled $13.6 million in 2016, down $6.7 million from the prior year, with improvements from increased revenue more than offset by higher expenses.
Non-operating ItemsThe AMA reported a $24.1 million gain in the fair value of its portfolio during 2016 after showing an $18.4 million loss in 2015. AMA also reported $0.2 million in proceeds from a sale of an asset as non-operating revenue in 2015.
Revenue in Excess of ExpensesRevenues were $37.7 million greater than expenses in 2016, a combination of the $13.6 million operating income plus $24.1 million in non-operating gains. Revenues exceeded expenses by $2.1 million in 2015.
Change in Association EquityAccounting standards require organizations to recognize deferred actuarial losses and prior service credits or charges for defined benefit postretirement plans as a charge or credit to
equity. In 2016, the net credit to equity related to defined benefit postretirement plans totaled $0.4 million. Actuarial losses in both the pension plan and the postretirement health care plan resulted from year-end higher interest rates that increase the present value of plan liabilities as well as participant changes. Portfolio returns in the pension plan were less than the actuarial expectation, and claims experience in the retiree health plan were higher than the actuarial expectation, both resulting in additional charges. Recognition of actuarial losses and prior service credits in the postretirement health care plan more than offset the losses. Deferred taxes on the credit slightly increased the gain.
In 2015, the net credit to equity related to defined benefit postretirement plans totaled $4.8 million. Actuarial gains in both the pension plan and the postretirement health care plan resulted from year-end higher interest rates that decrease the present value of plan liabilities as well as a change in liabilities related to adoption of revised mortality tables. Portfolio returns in the pension plan were less than the actuarial expectation, and claims experience in the retiree health plan were higher than the actuarial expectation, both resulting in charges that reduced the credit from interest rates. Recognition of prior service credits in the postretirement health care plan also increased the unrecognized gains. Deferred taxes on the credit slightly reduced the overall gain.
The AMA reported a $38.1 million increase in unrestricted association equity in 2016. This reflects the amount by which revenues were greater than expenses, plus the credits to equity for changes in defined benefit postretirement plans discussed above. After subtracting a $0.1 million decrease in temporarily restricted equity in 2016, total equity increased $38 million.
In 2015, total equity increased by $6.8 million, with $2.1 million of revenues in excess of expenses and $4.8 million in credits to equity for changes in defined benefit postretirement plans slightly reduced by a $0.1 million decrease in temporarily restricted equity.
Financial Position and Cash FlowsThe AMA’s assets include cash, cash equivalents and investments; operating assets such as accounts receivable, inventory and prepaid expenses; fixed capital such as equipment, computer hardware and software; and other assets. AMA assets are supported by association equity, operating liabilities and deferred revenue.
American Medical Association 2016 Annual Report | 12 American Medical Association 2016 Annual Report | 13
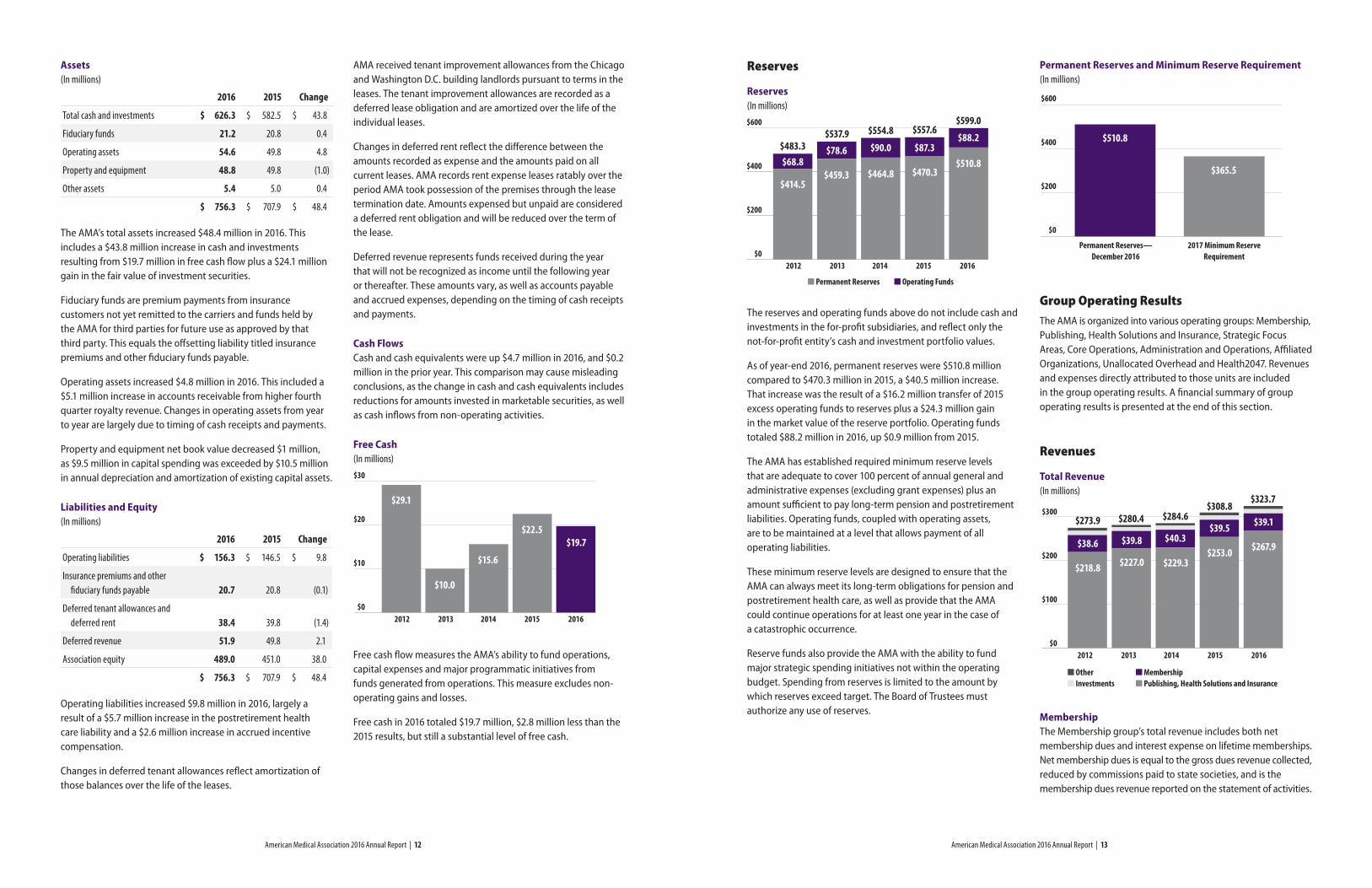
Reserves
Reserves(In millions)
The reserves and operating funds above do not include cash and investments in the for-profit subsidiaries, and reflect only the not-for-profit entity’s cash and investment portfolio values.
As of year-end 2016, permanent reserves were $510.8 million compared to $470.3 million in 2015, a $40.5 million increase. That increase was the result of a $16.2 million transfer of 2015 excess operating funds to reserves plus a $24.3 million gain in the market value of the reserve portfolio. Operating funds totaled $88.2 million in 2016, up $0.9 million from 2015.
The AMA has established required minimum reserve levels that are adequate to cover 100 percent of annual general and administrative expenses (excluding grant expenses) plus an amount sufficient to pay long-term pension and postretirement liabilities. Operating funds, coupled with operating assets, are to be maintained at a level that allows payment of all operating liabilities.
These minimum reserve levels are designed to ensure that the AMA can always meet its long-term obligations for pension and postretirement health care, as well as provide that the AMA could continue operations for at least one year in the case of a catastrophic occurrence.
Reserve funds also provide the AMA with the ability to fund major strategic spending initiatives not within the operating budget. Spending from reserves is limited to the amount by which reserves exceed target. The Board of Trustees must authorize any use of reserves.
Assets(In millions)
2016 2015 Change
Total cash and investments $ 626.3 $ 582.5 $ 43.8
Fiduciary funds 21.2 20.8 0.4
Operating assets 54.6 49.8 4.8
Property and equipment 48.8 49.8 (1.0)
Other assets 5.4 5.0 0.4
$ 756.3 $ 707.9 $ 48.4
The AMA’s total assets increased $48.4 million in 2016. This includes a $43.8 million increase in cash and investments resulting from $19.7 million in free cash flow plus a $24.1 million gain in the fair value of investment securities.
Fiduciary funds are premium payments from insurance customers not yet remitted to the carriers and funds held by the AMA for third parties for future use as approved by that third party. This equals the offsetting liability titled insurance premiums and other fiduciary funds payable.
Operating assets increased $4.8 million in 2016. This included a $5.1 million increase in accounts receivable from higher fourth quarter royalty revenue. Changes in operating assets from year to year are largely due to timing of cash receipts and payments.
Property and equipment net book value decreased $1 million, as $9.5 million in capital spending was exceeded by $10.5 million in annual depreciation and amortization of existing capital assets.
Liabilities and Equity(In millions)
2016 2015 Change
Operating liabilities $ 156.3 $ 146.5 $ 9.8
Insurance premiums and other fiduciary funds payable 20.7 20.8 (0.1)
Deferred tenant allowances and deferred rent 38.4 39.8 (1.4)
Deferred revenue 51.9 49.8 2.1
Association equity 489.0 451.0 38.0
$ 756.3 $ 707.9 $ 48.4
Operating liabilities increased $9.8 million in 2016, largely a result of a $5.7 million increase in the postretirement health care liability and a $2.6 million increase in accrued incentive compensation.
Changes in deferred tenant allowances reflect amortization of those balances over the life of the leases.
AMA received tenant improvement allowances from the Chicago and Washington D.C. building landlords pursuant to terms in the leases. The tenant improvement allowances are recorded as a deferred lease obligation and are amortized over the life of the individual leases.
Changes in deferred rent reflect the difference between the amounts recorded as expense and the amounts paid on all current leases. AMA records rent expense leases ratably over the period AMA took possession of the premises through the lease termination date. Amounts expensed but unpaid are considered a deferred rent obligation and will be reduced over the term of the lease.
Deferred revenue represents funds received during the year that will not be recognized as income until the following year or thereafter. These amounts vary, as well as accounts payable and accrued expenses, depending on the timing of cash receipts and payments.
Cash FlowsCash and cash equivalents were up $4.7 million in 2016, and $0.2 million in the prior year. This comparison may cause misleading conclusions, as the change in cash and cash equivalents includes reductions for amounts invested in marketable securities, as well as cash inflows from non-operating activities.
Free Cash(In millions)
Free cash flow measures the AMA’s ability to fund operations, capital expenses and major programmatic initiatives from funds generated from operations. This measure excludes non-operating gains and losses.
Free cash in 2016 totaled $19.7 million, $2.8 million less than the 2015 results, but still a substantial level of free cash.
$30
$20
$10
$0 2012 2013 2014 2015 2016
$15.6
$22.5$19.7
$10.0
$29.1
Permanent Reserves and Minimum Reserve Requirement(In millions)
Group Operating ResultsThe AMA is organized into various operating groups: Membership, Publishing, Health Solutions and Insurance, Strategic Focus Areas, Core Operations, Administration and Operations, Affiliated Organizations, Unallocated Overhead and Health2047. Revenues and expenses directly attributed to those units are included in the group operating results. A financial summary of group operating results is presented at the end of this section.
Revenues
Total Revenue(In millions)
MembershipThe Membership group’s total revenue includes both net membership dues and interest expense on lifetime memberships. Net membership dues is equal to the gross dues revenue collected, reduced by commissions paid to state societies, and is the membership dues revenue reported on the statement of activities.
$600
$400
$200
$0 2012 2013 2014 2015 2016
$414.5$459.3 $464.8 $470.3
$510.8$68.8$78.6 $90.0 $87.3
$88.2$483.3
$537.9 $554.8 $557.6$599.0
n Permanent Reserves n Operating Funds
$600
$400
$200
$0
Permanent Reserves—December 2016
2017 Minimum Reserve Requirement
$510.8
$365.5
$300
$200
$100
$0 2012 2013 2014 2015 2016
n Othern Investments
$218.8 $227.0 $229.3$253.0 $267.9
$39.1$39.5$40.3$39.8$38.6
$273.9 $280.4 $284.6$308.8
$323.7
n Membership n Publishing, Health Solutions and Insurance
American Medical Association 2016 Annual Report | 14 American Medical Association 2016 Annual Report | 15
The AMA achieved its sixth consecutive year of increases in the number of dues-paying members, although total dues revenue declined slightly in 2016. The number of members increased 2.6 percent and 1 percent in 2016 and 2015, respectively.
Gross dues revenue was $39.3 million, a $0.3 million decrease from 2015, as membership increased in categories with lower average dues rates, such as group practices, residents and sponsored memberships. Commissions and incentives paid to state societies totaled $0.1 million in both 2016 and 2015. Interest expense on lifetime memberships was $0.1 million in 2016 and $0 in 2015.
Investments (AMA-only)AMA-only investment income includes dividend and interest earnings on the AMA’s portfolio. Investment income in AMA’s active subsidiaries is included in the Publishing, Health Solutions and Insurance results.
Investments’ income was unchanged in 2016 when compared to 2015. Continued low interest rates have resulted in reduced levels of income in the portfolio during the last several years.
The net gain or loss on investments is not included in operating results, but reported as a non-operating item. This amount is in addition to the investment income discussed above, and totaled a $24.1 million gain in 2016 compared to an $18.4 million loss in 2015. The total investment return on the portfolio was 4.6 percent. The 2016 return compares to a composite benchmark index of slightly over 8 percent. AMA’s portfolio is balanced almost equally between equity and fixed income. AMA does not invest in passive index funds due to the prohibition on tobacco-related investing. Passive index funds have substantially outperformed active management for the last several years.
Publishing, Health Solutions and InsurancePublications in The JAMA Network include the Journal of the American Medical Association (JAMA) and The JAMA Network specialty journals. The JAMA Network was enhanced in 2015 by the very successful launch of JAMA Oncology, followed by the launch of JAMA Cardiology in 2016.
Publishing revenues are derived from advertising, subscriptions, site licensing, reprints, electronic licensing and royalties. Publishing revenues increased $1.4 million in 2016. Growth in site licensing and electronic licensing, coupled with increased reprint revenue in The JAMA Network publications was partially offset by losses in print subscriptions and print advertising.
Health Solutions includes two major lines: Database Products, and Books and Digital Content.
Database Products includes royalties from licensed data sales and credentialing products revenue. Revenues increased slightly in 2016, with $0.6 million combined growth in credentialing product sales and licensed data royalties.
AMA-published books and coding products, such as CPT books, workshops and licensed data files, make up the Books and Digital Content unit. Revenues in this unit increased by $13 million. Royalties drove this increase, reporting a 33 percent increase in revenues in 2016, as the market for electronic use of CPT codes continues to expand. Coding book sales declined substantially in 2016, with overall book sales down $6.8 million in 2016. The move from print books to electronic data files continues to impact these sales, as well as major changes in coding standards, such as required adoption of ICD-10, which drove a large increase in book sales during 2015.
The AMA has two active for-profit subsidiaries, the AMA Insurance Agency (Insurance Agency) and Health2047. The latter is discussed separately at the end of this discussion and analysis. Effective in 2015, AMA Affinity Products are also included in the results of the Insurance Agency. The Insurance Agency revenues were down slightly in 2016. The Insurance Agency, as broker, receives a commission on insurance policies sold.
Other RevenuesOther revenues are derived from grants and other fee income. These increased $0.4 million in 2016, largely due to improved grant and fee income in the core activities.
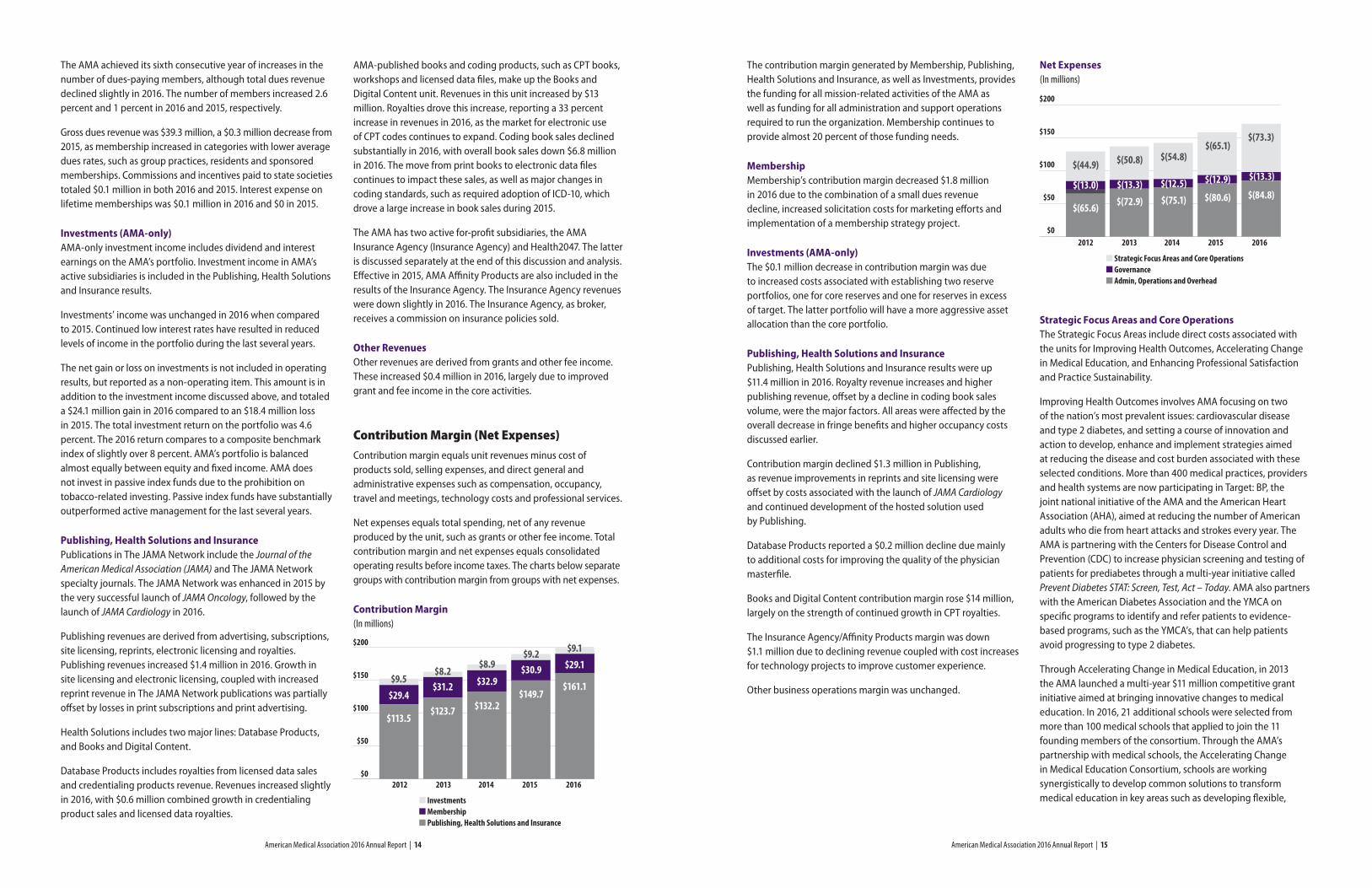
Contribution Margin (Net Expenses)Contribution margin equals unit revenues minus cost of products sold, selling expenses, and direct general and administrative expenses such as compensation, occupancy, travel and meetings, technology costs and professional services.
Net expenses equals total spending, net of any revenue produced by the unit, such as grants or other fee income. Total contribution margin and net expenses equals consolidated operating results before income taxes. The charts below separate groups with contribution margin from groups with net expenses.
Contribution Margin(In millions)
The contribution margin generated by Membership, Publishing, Health Solutions and Insurance, as well as Investments, provides the funding for all mission-related activities of the AMA as well as funding for all administration and support operations required to run the organization. Membership continues to provide almost 20 percent of those funding needs.
MembershipMembership’s contribution margin decreased $1.8 million in 2016 due to the combination of a small dues revenue decline, increased solicitation costs for marketing efforts and implementation of a membership strategy project.
Investments (AMA-only)The $0.1 million decrease in contribution margin was due to increased costs associated with establishing two reserve portfolios, one for core reserves and one for reserves in excess of target. The latter portfolio will have a more aggressive asset allocation than the core portfolio.
Publishing, Health Solutions and InsurancePublishing, Health Solutions and Insurance results were up $11.4 million in 2016. Royalty revenue increases and higher publishing revenue, offset by a decline in coding book sales volume, were the major factors. All areas were affected by the overall decrease in fringe benefits and higher occupancy costs discussed earlier.
Contribution margin declined $1.3 million in Publishing, as revenue improvements in reprints and site licensing were offset by costs associated with the launch of JAMA Cardiology and continued development of the hosted solution used by Publishing.
Database Products reported a $0.2 million decline due mainly to additional costs for improving the quality of the physician masterfile.
Books and Digital Content contribution margin rose $14 million, largely on the strength of continued growth in CPT royalties.
The Insurance Agency/Affinity Products margin was down $1.1 million due to declining revenue coupled with cost increases for technology projects to improve customer experience.
Other business operations margin was unchanged.
Net Expenses(In millions)
Strategic Focus Areas and Core OperationsThe Strategic Focus Areas include direct costs associated with the units for Improving Health Outcomes, Accelerating Change in Medical Education, and Enhancing Professional Satisfaction and Practice Sustainability.
Improving Health Outcomes involves AMA focusing on two of the nation’s most prevalent issues: cardiovascular disease and type 2 diabetes, and setting a course of innovation and action to develop, enhance and implement strategies aimed at reducing the disease and cost burden associated with these selected conditions. More than 400 medical practices, providers and health systems are now participating in Target: BP, the joint national initiative of the AMA and the American Heart Association (AHA), aimed at reducing the number of American adults who die from heart attacks and strokes every year. The AMA is partnering with the Centers for Disease Control and Prevention (CDC) to increase physician screening and testing of patients for prediabetes through a multi-year initiative called Prevent Diabetes STAT: Screen, Test, Act – Today. AMA also partners with the American Diabetes Association and the YMCA on specific programs to identify and refer patients to evidence-based programs, such as the YMCA’s, that can help patients avoid progressing to type 2 diabetes.
Through Accelerating Change in Medical Education, in 2013 the AMA launched a multi-year $11 million competitive grant initiative aimed at bringing innovative changes to medical education. In 2016, 21 additional schools were selected from more than 100 medical schools that applied to join the 11 founding members of the consortium. Through the AMA’s partnership with medical schools, the Accelerating Change in Medical Education Consortium, schools are working synergistically to develop common solutions to transform medical education in key areas such as developing flexible,
$200
$150
$100
$50
$0 2012 2013 2014 2015 2016
n Strategic Focus Areas and Core Operationsn Governance n Admin, Operations and Overhead
$(72.9) $(75.1) $(80.6) $(84.8)$(13.3) $(12.5) $(12.9) $(13.3)
$(50.8) $(54.8)$(65.1)
$(73.3)
$(65.6)
$(13.0)
$(44.9)
$200
$150
$100
$50
$0 2012 2013 2014 2015 2016
n Investmentsn Membership n Publishing , Health Solutions and Insurance
$113.5
$29.4$9.5
$123.7
$31.2$8.2
$132.2
$32.9
$8.9$9.2
$30.9 $29.1
$149.7$161.1
$9.1
American Medical Association 2016 Annual Report | 16 American Medical Association 2016 Annual Report | 17
competency-based pathways, teaching new content in health care delivery sciences, making technology work for learning and shaping tomorrow’s leaders.
In Professional Satisfaction and Practice Sustainability (PS2), the AMA is investing significant resources in evaluating a path to long-term sustainability of and satisfaction with medical practice. The goals of this initiative are to promote successful models in both the public and private sectors; create tools focused on helping physicians implement practice improvements, improving the usability of electronic health records, shaping the evolution of payment models for sustainability and satisfaction, and promoting physician representation and leadership in the governance structure of hospitals and health systems. The AMA’s STEPS Forward™ practice transformation series is a collection of interactive, educational modules developed by physicians to help physicians address common practice challenges. These tools are based on key insights of the AMA-RAND study, “Factors affecting physician professional satisfaction and their implications for patient care, health systems and health policy.” A variety of the modules focus on preventing physician burnout.
The AMA also offers many opportunities for physicians to enhance their leadership skills and engage in leadership opportunities. The AMA is critically examining the role health IT plays in providing high-quality care to patients, helping physicians navigate and successfully use these technologies to improve health. Identifying key challenges physicians face with health IT and focusing on improved usability and interoperability is a major initiative. An AMA-RAND study investigated the real-world impact of these payment reforms on physician practices. The study findings are guiding the AMA’s efforts to improve alternative physician payment models and to help physician practices successfully adapt and succeed.
In 2016, Advocacy and PS2 teamed together to launch the new “AMA Payment Model Evaluator,” which holds educational resources on MACRA as well as providing an online tool for physicians to use to help determine how MACRA will impact their practice. The AMA’s Advocacy group will also remain engaged in shaping government policy and legislation that incentivizes and enables proven models.
The Strategic Focus Areas continued to expand staff and operations during 2016, the fourth full year of implementation of AMA’s new strategic plan. The expansion of the ACE Consortium as well as a grant to develop a tEMR, accounts for almost half of the $2.7 million in net expense increase during 2016. Development of MACRA resources, leadership education and digital health accounted for the rest.
Core Operations includes three groups: Advocacy; Health, Science and Core Medical Education; and Communications and Marketing.
The Advocacy Group includes federal and state level advocacy to enact laws and advance regulations on issues important to patients and physicians; economic, statistical and market research to support advocacy efforts; political education for physicians; grassroots advocacy; and maintaining relations with the federation of medicine. Strategic areas in 2016 centered on successful efforts to improve regulations issued to implement MACRA and to assist physicians in understanding and adopting MACRA, laying groundwork to block large insurance mergers, meaningful use; opioid abuse prevention; and administrative simplification, to name a few. In 2016, Advocacy net spending was down $2 million, reflecting the absence of costs in early 2015 related to eliminating SGR.
Health, Science and Core Medical Education includes Science; Core Medical Education; Ethics; and Grants. The group is involved in developing AMA policies on scientific issues for the House of Delegates (HOD); public health advocacy; defining or influencing standards for undergraduate, graduate and continuing medical education; establishing and disseminating ethical standards for the profession; enhancing quality of care and patient safety; and providing support for the Councils on Ethical and Judicial Affairs, Science and Public Health and Medical Education. In 2016, this group successfully spearheaded the adoption of the modernized AMA Code of Medical Ethics. The Physician Consortium for Performance Improvement (PCPI) was successfully transitioned in 2016 to a separate organization, the PCPI Foundation, to which AMA continues to provide substantial support. A new initiative for this group is education delivery services for the education center, providing a platform for lifelong learning, which caused a $1 million net expense increase in Health, Science and Core Medical Education. That was offset by a slight reduction in overall funding related to the PCPI Foundation.
Communications and Marketing focuses its efforts on enhancing the AMA’s brand image; informing the public about the AMA’s positions and policies; supporting the AMA’s advocacy efforts and maintaining effective member communications. Net expenses were up $6.8 million in 2016, mainly due to costs associated with two major initiatives, development of a new brand strategy and implementation of the enterprise digital strategy project. AMA continues to sponsor major health care events such as TEDMED and Health 2.0 challenges.
GovernanceGovernance includes the Board of Trustees and Officer Services, the HOD, Sections and Special Constituencies and International units. The Board of Trustees unit includes costs related to governance activities as well as expenses associated with support of the Strategic Focus Areas and Core Operations. The HOD, Sections and Special Constituencies and International
unit includes costs associated with annual and interim meetings, groups and sections and other HOD activities, as well as costs associated with AMA’s involvement in the World Medical Association.
In 2016, Governance net spending increased $0.4 million, with a $0.1 million increase in the Board of Trustees unit and a $0.3 million increase in the HOD and Sections and Special Constituencies and International unit.
Administration and OperationsThese units provide administrative and operational support for Publishing and Health Solutions, Membership and all other operating groups. Net expenses increased by $2.7 million in 2016, or 4 percent. Higher occupancy expense and lower overall AMA fringe benefits, mainly due to the decreases in pension and retiree health previously discussed, netted to a $0.4 million increase. Information Technology costs rose $1.9 million, of which $0.8 million was due to the enterprise digital strategy project.
Affiliated OrganizationsAffiliated Organizations represent either grant or in-kind service support provided by the AMA to other foundations and societies. In some cases, the AMA is reimbursed for services provided. Net expenses were unchanged in 2016.
Unallocated OverheadThe net expenses in this area include costs not allocated back to operating units such as corporate insurance and actuarial services, employee incentive compensation, valuation allowances or other reserves. In 2016, these expenses totaled $15.2 million, up from $13.7 million in 2015. Higher incentive compensation accounted for the entire increase.
Health2047 In 2015, the AMA Board approved the use of reserves to establish this subsidiary with plans to use third-party resources to partially assist in funding in future years.
Health2047 will provide strategic insights through privileged access to the AMA and its physician network, help execute in product development and bring massive channel strength, all within a culture that can rapidly innovate and have the capacity to pursue multiple products and create a portfolio.
The innovation studio began operations in mid-2015 with costs in the initial year totaling $2.8 million. The formal launch of the studio occurred in early 2016 and costs rose to $6.6 million in the first full year of operations. Development of initial projects are underway with strong market interest expressed by major corporations.
The summary of group operating results is included on the following page.
American Medical Association 2016 Annual Report | 18
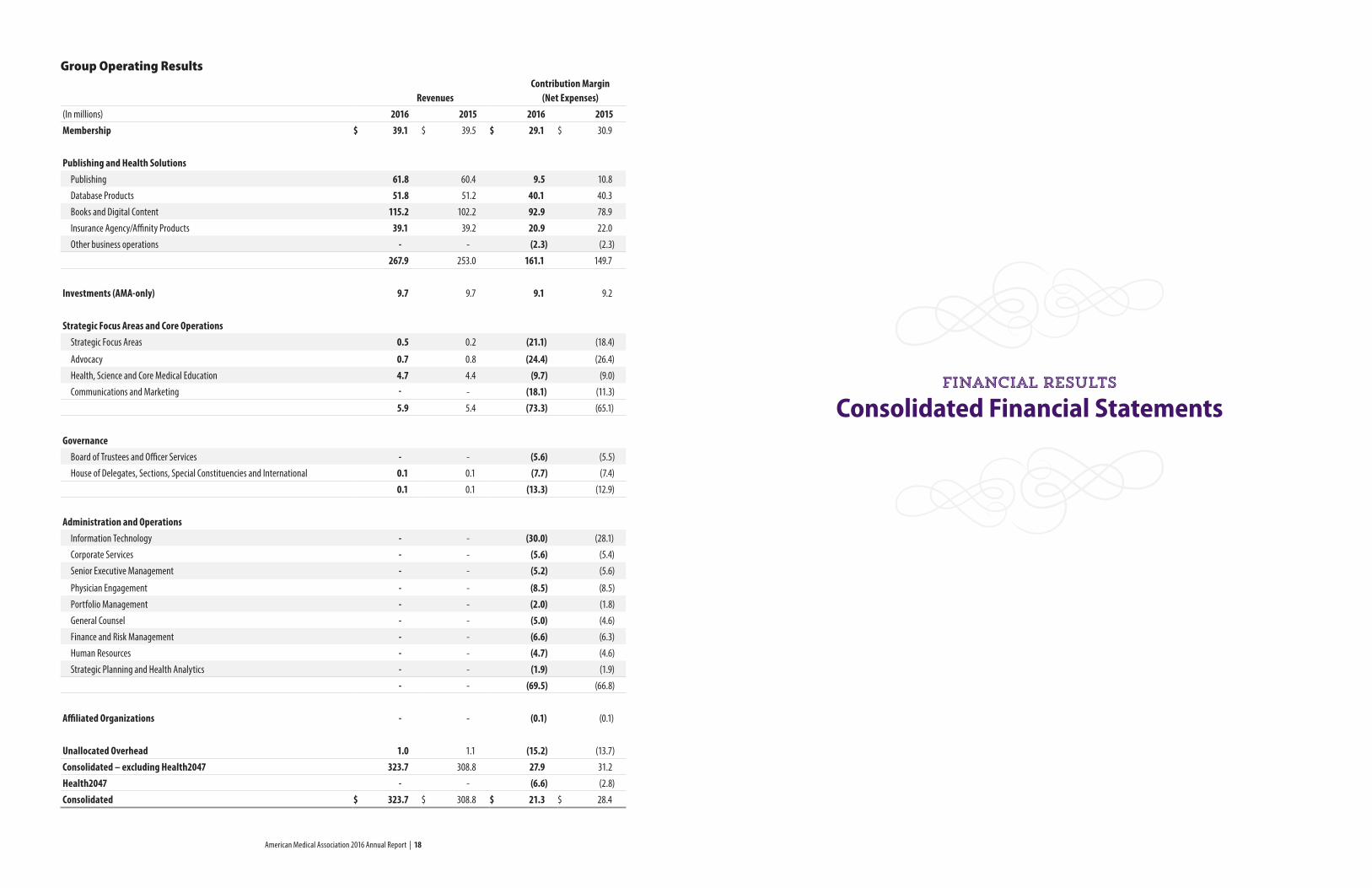
Group Operating Results
Revenues Contribution Margin (Net Expenses)
(In millions) 2016 2015 2016 2015Membership $ 39.1 $ 39.5 $ 29.1 $ 30.9
Publishing and Health Solutions Publishing 61.8 60.4 9.5 10.8
Database Products 51.8 51.2 40.1 40.3
Books and Digital Content 115.2 102.2 92.9 78.9
Insurance Agency/Affinity Products 39.1 39.2 20.9 22.0
Other business operations - - (2.3) (2.3)
267.9 253.0 161.1 149.7
Investments (AMA-only) 9.7 9.7 9.1 9.2
Strategic Focus Areas and Core Operations Strategic Focus Areas 0.5 0.2 (21.1) (18.4)
Advocacy 0.7 0.8 (24.4) (26.4)
Health, Science and Core Medical Education 4.7 4.4 (9.7) (9.0)
Communications and Marketing - - (18.1) (11.3)
5.9 5.4 (73.3) (65.1)
Governance Board of Trustees and Officer Services - - (5.6) (5.5)
House of Delegates, Sections, Special Constituencies and International 0.1 0.1 (7.7) (7.4)
0.1 0.1 (13.3) (12.9)
Administration and Operations Information Technology - - (30.0) (28.1)
Corporate Services - - (5.6) (5.4)
Senior Executive Management - - (5.2) (5.6)
Physician Engagement - - (8.5) (8.5)
Portfolio Management - - (2.0) (1.8)
General Counsel - - (5.0) (4.6)
Finance and Risk Management - - (6.6) (6.3)
Human Resources - - (4.7) (4.6)
Strategic Planning and Health Analytics - - (1.9) (1.9)
- - (69.5) (66.8)
Affiliated Organizations - - (0.1) (0.1)
Unallocated Overhead 1.0 1.1 (15.2) (13.7)
Consolidated – excluding Health2047 323.7 308.8 27.9 31.2
Health2047 - - (6.6) (2.8)
Consolidated $ 323.7 $ 308.8 $ 21.3 $ 28.4
Consolidated Financial StatementsFinancial results
American Medical Association 2016 Annual Report | 21
American Medical Association and Subsidiaries
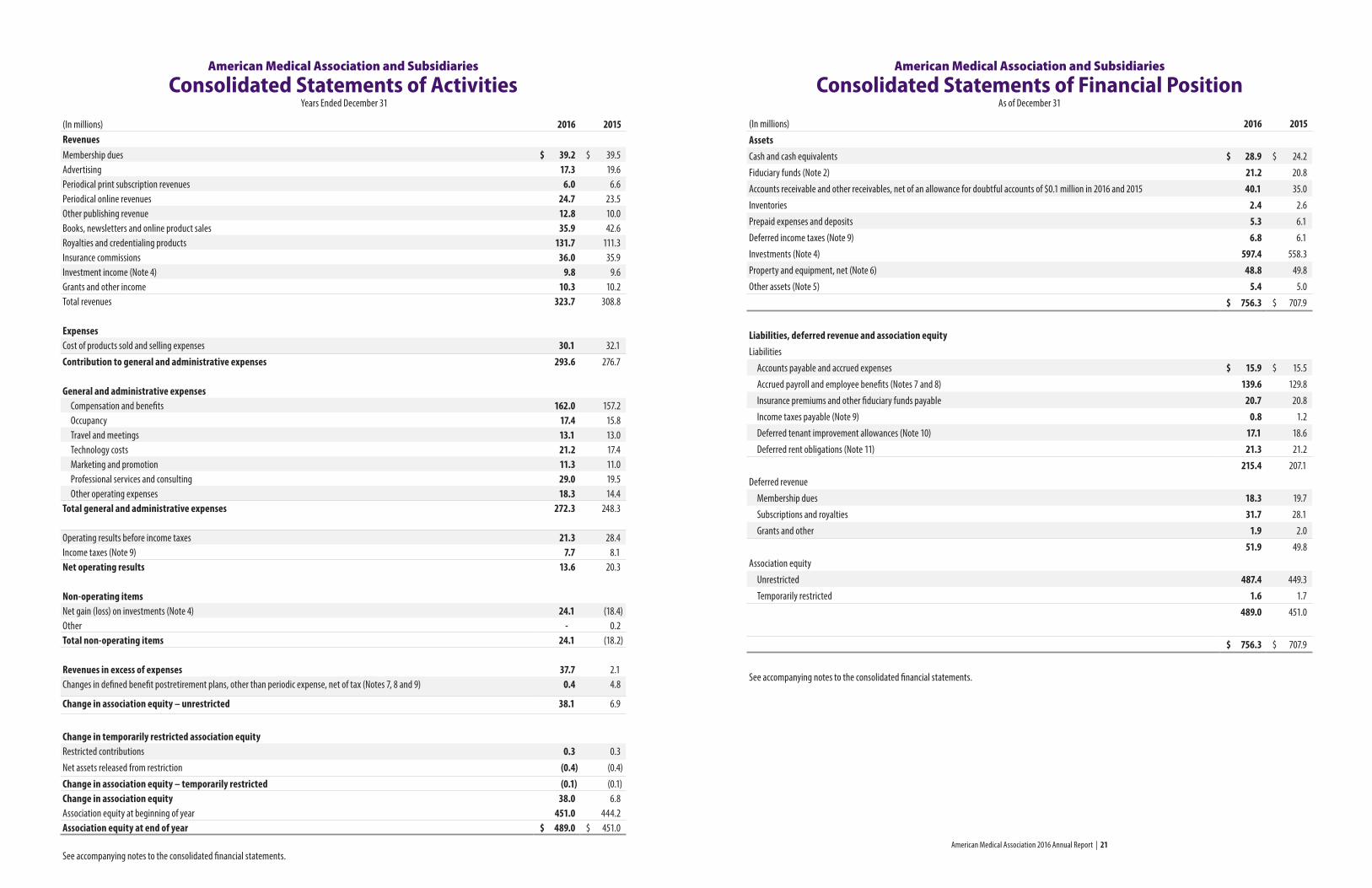
Consolidated Statements of ActivitiesYears Ended December 31
(In millions) 2016 2015RevenuesMembership dues $ 39.2 $ 39.5Advertising 17.3 19.6Periodical print subscription revenues 6.0 6.6Periodical online revenues 24.7 23.5Other publishing revenue 12.8 10.0Books, newsletters and online product sales 35.9 42.6Royalties and credentialing products 131.7 111.3Insurance commissions 36.0 35.9Investment income (Note 4) 9.8 9.6Grants and other income 10.3 10.2Total revenues 323.7 308.8
ExpensesCost of products sold and selling expenses 30.1 32.1
Contribution to general and administrative expenses 293.6 276.7
General and administrative expenses Compensation and benefits 162.0 157.2 Occupancy 17.4 15.8 Travel and meetings 13.1 13.0 Technology costs 21.2 17.4 Marketing and promotion 11.3 11.0 Professional services and consulting 29.0 19.5 Other operating expenses 18.3 14.4Total general and administrative expenses 272.3 248.3
Operating results before income taxes 21.3 28.4Income taxes (Note 9) 7.7 8.1Net operating results 13.6 20.3
Non-operating itemsNet gain (loss) on investments (Note 4) 24.1 (18.4)Other - 0.2Total non-operating items 24.1 (18.2)
Revenues in excess of expenses 37.7 2.1Changes in defined benefit postretirement plans, other than periodic expense, net of tax (Notes 7, 8 and 9) 0.4 4.8
Change in association equity – unrestricted 38.1 6.9
Change in temporarily restricted association equityRestricted contributions 0.3 0.3
Net assets released from restriction (0.4) (0.4)
Change in association equity – temporarily restricted (0.1) (0.1)Change in association equity 38.0 6.8Association equity at beginning of year 451.0 444.2Association equity at end of year $ 489.0 $ 451.0
See accompanying notes to the consolidated financial statements.
American Medical Association and Subsidiaries
Consolidated Statements of Financial Position As of December 31
(In millions) 2016 2015AssetsCash and cash equivalents $ 28.9 $ 24.2
Fiduciary funds (Note 2) 21.2 20.8
Accounts receivable and other receivables, net of an allowance for doubtful accounts of $0.1 million in 2016 and 2015 40.1 35.0
Inventories 2.4 2.6
Prepaid expenses and deposits 5.3 6.1
Deferred income taxes (Note 9) 6.8 6.1
Investments (Note 4) 597.4 558.3
Property and equipment, net (Note 6) 48.8 49.8
Other assets (Note 5) 5.4 5.0
$ 756.3 $ 707.9
Liabilities, deferred revenue and association equityLiabilities
Accounts payable and accrued expenses $ 15.9 $ 15.5
Accrued payroll and employee benefits (Notes 7 and 8) 139.6 129.8
Insurance premiums and other fiduciary funds payable 20.7 20.8
Income taxes payable (Note 9) 0.8 1.2
Deferred tenant improvement allowances (Note 10) 17.1 18.6
Deferred rent obligations (Note 11) 21.3 21.2
215.4 207.1
Deferred revenue
Membership dues 18.3 19.7
Subscriptions and royalties 31.7 28.1
Grants and other 1.9 2.0
51.9 49.8
Association equity
Unrestricted 487.4 449.3
Temporarily restricted 1.6 1.7
489.0 451.0
$ 756.3 $ 707.9
See accompanying notes to the consolidated financial statements.
American Medical Association 2016 Annual Report | 22 American Medical Association 2016 Annual Report | 23
American Medical Association and Subsidiaries
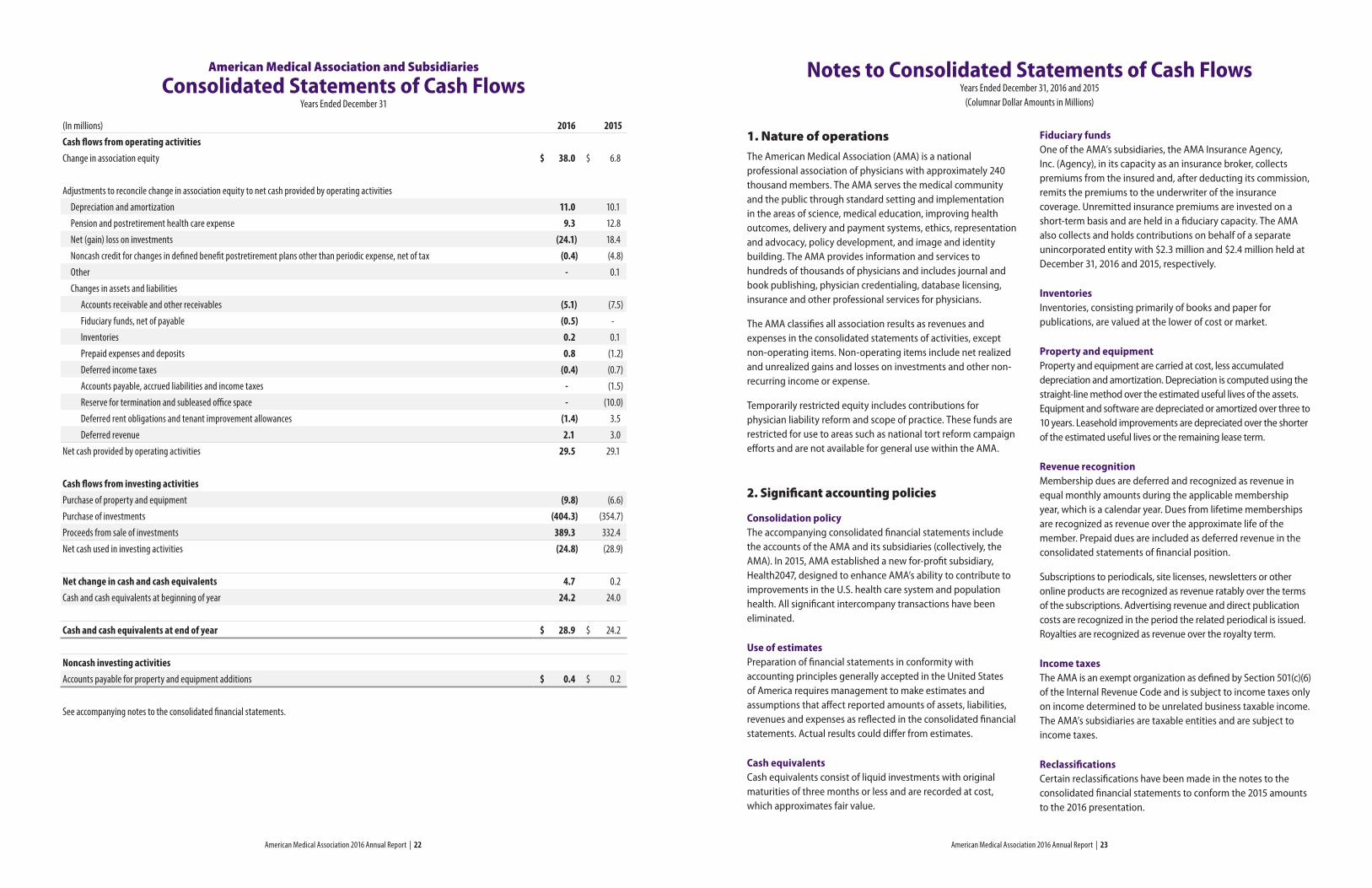
Consolidated Statements of Cash FlowsYears Ended December 31
(In millions) 2016 2015Cash flows from operating activitiesChange in association equity $ 38.0 $ 6.8
Adjustments to reconcile change in association equity to net cash provided by operating activities
Depreciation and amortization 11.0 10.1
Pension and postretirement health care expense 9.3 12.8
Net (gain) loss on investments (24.1) 18.4
Noncash credit for changes in defined benefit postretirement plans other than periodic expense, net of tax (0.4) (4.8)
Other - 0.1
Changes in assets and liabilities
Accounts receivable and other receivables (5.1) (7.5)
Fiduciary funds, net of payable (0.5) -
Inventories 0.2 0.1
Prepaid expenses and deposits 0.8 (1.2)
Deferred income taxes (0.4) (0.7)
Accounts payable, accrued liabilities and income taxes - (1.5)
Reserve for termination and subleased office space - (10.0)
Deferred rent obligations and tenant improvement allowances (1.4) 3.5
Deferred revenue 2.1 3.0
Net cash provided by operating activities 29.5 29.1
Cash flows from investing activitiesPurchase of property and equipment (9.8) (6.6)
Purchase of investments (404.3) (354.7)
Proceeds from sale of investments 389.3 332.4
Net cash used in investing activities (24.8) (28.9)
Net change in cash and cash equivalents 4.7 0.2
Cash and cash equivalents at beginning of year 24.2 24.0
Cash and cash equivalents at end of year $ 28.9 $ 24.2
Noncash investing activitiesAccounts payable for property and equipment additions $ 0.4 $ 0.2
See accompanying notes to the consolidated financial statements.
1. Nature of operationsThe American Medical Association (AMA) is a national professional association of physicians with approximately 240 thousand members. The AMA serves the medical community and the public through standard setting and implementation in the areas of science, medical education, improving health outcomes, delivery and payment systems, ethics, representation and advocacy, policy development, and image and identity building. The AMA provides information and services to hundreds of thousands of physicians and includes journal and book publishing, physician credentialing, database licensing, insurance and other professional services for physicians.
The AMA classifies all association results as revenues and expenses in the consolidated statements of activities, except non-operating items. Non-operating items include net realized and unrealized gains and losses on investments and other non-recurring income or expense.
Temporarily restricted equity includes contributions for physician liability reform and scope of practice. These funds are restricted for use to areas such as national tort reform campaign efforts and are not available for general use within the AMA.
2. Significant accounting policies
Consolidation policyThe accompanying consolidated financial statements include the accounts of the AMA and its subsidiaries (collectively, the AMA). In 2015, AMA established a new for-profit subsidiary, Health2047, designed to enhance AMA’s ability to contribute to improvements in the U.S. health care system and population health. All significant intercompany transactions have been eliminated.
Use of estimatesPreparation of financial statements in conformity with accounting principles generally accepted in the United States of America requires management to make estimates and assumptions that affect reported amounts of assets, liabilities, revenues and expenses as reflected in the consolidated financial statements. Actual results could differ from estimates.
Cash equivalentsCash equivalents consist of liquid investments with original maturities of three months or less and are recorded at cost, which approximates fair value.
Fiduciary fundsOne of the AMA’s subsidiaries, the AMA Insurance Agency, Inc. (Agency), in its capacity as an insurance broker, collects premiums from the insured and, after deducting its commission, remits the premiums to the underwriter of the insurance coverage. Unremitted insurance premiums are invested on a short-term basis and are held in a fiduciary capacity. The AMA also collects and holds contributions on behalf of a separate unincorporated entity with $2.3 million and $2.4 million held at December 31, 2016 and 2015, respectively.
InventoriesInventories, consisting primarily of books and paper for publications, are valued at the lower of cost or market.
Property and equipmentProperty and equipment are carried at cost, less accumulated depreciation and amortization. Depreciation is computed using the straight-line method over the estimated useful lives of the assets. Equipment and software are depreciated or amortized over three to 10 years. Leasehold improvements are depreciated over the shorter of the estimated useful lives or the remaining lease term.
Revenue recognitionMembership dues are deferred and recognized as revenue in equal monthly amounts during the applicable membership year, which is a calendar year. Dues from lifetime memberships are recognized as revenue over the approximate life of the member. Prepaid dues are included as deferred revenue in the consolidated statements of financial position.
Subscriptions to periodicals, site licenses, newsletters or other online products are recognized as revenue ratably over the terms of the subscriptions. Advertising revenue and direct publication costs are recognized in the period the related periodical is issued. Royalties are recognized as revenue over the royalty term.
Income taxesThe AMA is an exempt organization as defined by Section 501(c)(6) of the Internal Revenue Code and is subject to income taxes only on income determined to be unrelated business taxable income. The AMA’s subsidiaries are taxable entities and are subject to income taxes.
Reclassifications Certain reclassifications have been made in the notes to the consolidated financial statements to conform the 2015 amounts to the 2016 presentation.
Notes to Consolidated Statements of Cash FlowsYears Ended December 31, 2016 and 2015
(Columnar Dollar Amounts in Millions)
American Medical Association 2016 Annual Report | 24 American Medical Association 2016 Annual Report | 25
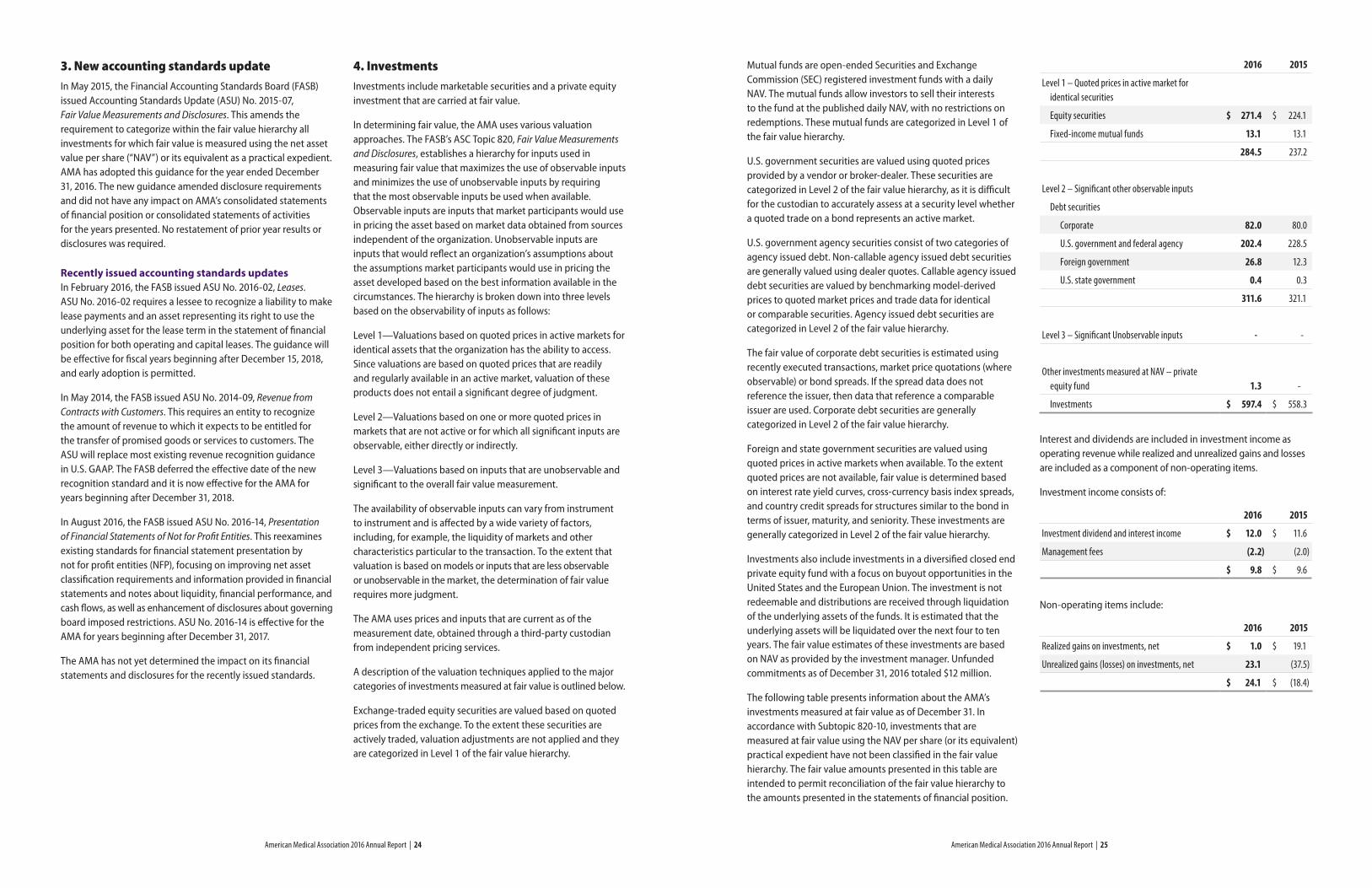
3. New accounting standards updateIn May 2015, the Financial Accounting Standards Board (FASB) issued Accounting Standards Update (ASU) No. 2015-07, Fair Value Measurements and Disclosures. This amends the requirement to categorize within the fair value hierarchy all investments for which fair value is measured using the net asset value per share (“NAV”) or its equivalent as a practical expedient. AMA has adopted this guidance for the year ended December 31, 2016. The new guidance amended disclosure requirements and did not have any impact on AMA’s consolidated statements of financial position or consolidated statements of activities for the years presented. No restatement of prior year results or disclosures was required.
Recently issued accounting standards updatesIn February 2016, the FASB issued ASU No. 2016-02, Leases. ASU No. 2016-02 requires a lessee to recognize a liability to make lease payments and an asset representing its right to use the underlying asset for the lease term in the statement of financial position for both operating and capital leases. The guidance will be effective for fiscal years beginning after December 15, 2018, and early adoption is permitted.
In May 2014, the FASB issued ASU No. 2014-09, Revenue from Contracts with Customers. This requires an entity to recognize the amount of revenue to which it expects to be entitled for the transfer of promised goods or services to customers. The ASU will replace most existing revenue recognition guidance in U.S. GAAP. The FASB deferred the effective date of the new recognition standard and it is now effective for the AMA for years beginning after December 31, 2018.
In August 2016, the FASB issued ASU No. 2016-14, Presentation of Financial Statements of Not for Profit Entities. This reexamines existing standards for financial statement presentation by not for profit entities (NFP), focusing on improving net asset classification requirements and information provided in financial statements and notes about liquidity, financial performance, and cash flows, as well as enhancement of disclosures about governing board imposed restrictions. ASU No. 2016-14 is effective for the AMA for years beginning after December 31, 2017.
The AMA has not yet determined the impact on its financial statements and disclosures for the recently issued standards.
4. Investments Investments include marketable securities and a private equity investment that are carried at fair value.
In determining fair value, the AMA uses various valuation approaches. The FASB’s ASC Topic 820, Fair Value Measurements and Disclosures, establishes a hierarchy for inputs used in measuring fair value that maximizes the use of observable inputs and minimizes the use of unobservable inputs by requiring that the most observable inputs be used when available. Observable inputs are inputs that market participants would use in pricing the asset based on market data obtained from sources independent of the organization. Unobservable inputs are inputs that would reflect an organization’s assumptions about the assumptions market participants would use in pricing the asset developed based on the best information available in the circumstances. The hierarchy is broken down into three levels based on the observability of inputs as follows:
Level 1—Valuations based on quoted prices in active markets for identical assets that the organization has the ability to access. Since valuations are based on quoted prices that are readily and regularly available in an active market, valuation of these products does not entail a significant degree of judgment.
Level 2—Valuations based on one or more quoted prices in markets that are not active or for which all significant inputs are observable, either directly or indirectly.
Level 3—Valuations based on inputs that are unobservable and significant to the overall fair value measurement.
The availability of observable inputs can vary from instrument to instrument and is affected by a wide variety of factors, including, for example, the liquidity of markets and other characteristics particular to the transaction. To the extent that valuation is based on models or inputs that are less observable or unobservable in the market, the determination of fair value requires more judgment.
The AMA uses prices and inputs that are current as of the measurement date, obtained through a third-party custodian from independent pricing services.
A description of the valuation techniques applied to the major categories of investments measured at fair value is outlined below.
Exchange-traded equity securities are valued based on quoted prices from the exchange. To the extent these securities are actively traded, valuation adjustments are not applied and they are categorized in Level 1 of the fair value hierarchy.
Mutual funds are open-ended Securities and Exchange Commission (SEC) registered investment funds with a daily NAV. The mutual funds allow investors to sell their interests to the fund at the published daily NAV, with no restrictions on redemptions. These mutual funds are categorized in Level 1 of the fair value hierarchy.
U.S. government securities are valued using quoted prices provided by a vendor or broker-dealer. These securities are categorized in Level 2 of the fair value hierarchy, as it is difficult for the custodian to accurately assess at a security level whether a quoted trade on a bond represents an active market.
U.S. government agency securities consist of two categories of agency issued debt. Non-callable agency issued debt securities are generally valued using dealer quotes. Callable agency issued debt securities are valued by benchmarking model-derived prices to quoted market prices and trade data for identical or comparable securities. Agency issued debt securities are categorized in Level 2 of the fair value hierarchy.
The fair value of corporate debt securities is estimated using recently executed transactions, market price quotations (where observable) or bond spreads. If the spread data does not reference the issuer, then data that reference a comparable issuer are used. Corporate debt securities are generally categorized in Level 2 of the fair value hierarchy.
Foreign and state government securities are valued using quoted prices in active markets when available. To the extent quoted prices are not available, fair value is determined based on interest rate yield curves, cross-currency basis index spreads, and country credit spreads for structures similar to the bond in terms of issuer, maturity, and seniority. These investments are generally categorized in Level 2 of the fair value hierarchy.
Investments also include investments in a diversified closed end private equity fund with a focus on buyout opportunities in the United States and the European Union. The investment is not redeemable and distributions are received through liquidation of the underlying assets of the funds. It is estimated that the underlying assets will be liquidated over the next four to ten years. The fair value estimates of these investments are based on NAV as provided by the investment manager. Unfunded commitments as of December 31, 2016 totaled $12 million.
The following table presents information about the AMA’s investments measured at fair value as of December 31. In accordance with Subtopic 820-10, investments that are measured at fair value using the NAV per share (or its equivalent) practical expedient have not been classified in the fair value hierarchy. The fair value amounts presented in this table are intended to permit reconciliation of the fair value hierarchy to the amounts presented in the statements of financial position.
2016 2015
Level 1 – Quoted prices in active market for identical securities
Equity securities $ 271.4 $ 224.1
Fixed-income mutual funds 13.1 13.1
284.5 237.2
Level 2 – Significant other observable inputs
Debt securities
Corporate 82.0 80.0
U.S. government and federal agency 202.4 228.5
Foreign government 26.8 12.3
U.S. state government 0.4 0.3
311.6 321.1
Level 3 – Significant Unobservable inputs - -
Other investments measured at NAV – private equity fund 1.3 -
Investments $ 597.4 $ 558.3
Interest and dividends are included in investment income as operating revenue while realized and unrealized gains and losses are included as a component of non-operating items.
Investment income consists of:
2016 2015
Investment dividend and interest income $ 12.0 $ 11.6
Management fees (2.2) (2.0)
$ 9.8 $ 9.6
Non-operating items include:
2016 2015
Realized gains on investments, net $ 1.0 $ 19.1
Unrealized gains (losses) on investments, net 23.1 (37.5)
$ 24.1 $ (18.4)
American Medical Association 2016 Annual Report | 26 American Medical Association 2016 Annual Report | 27
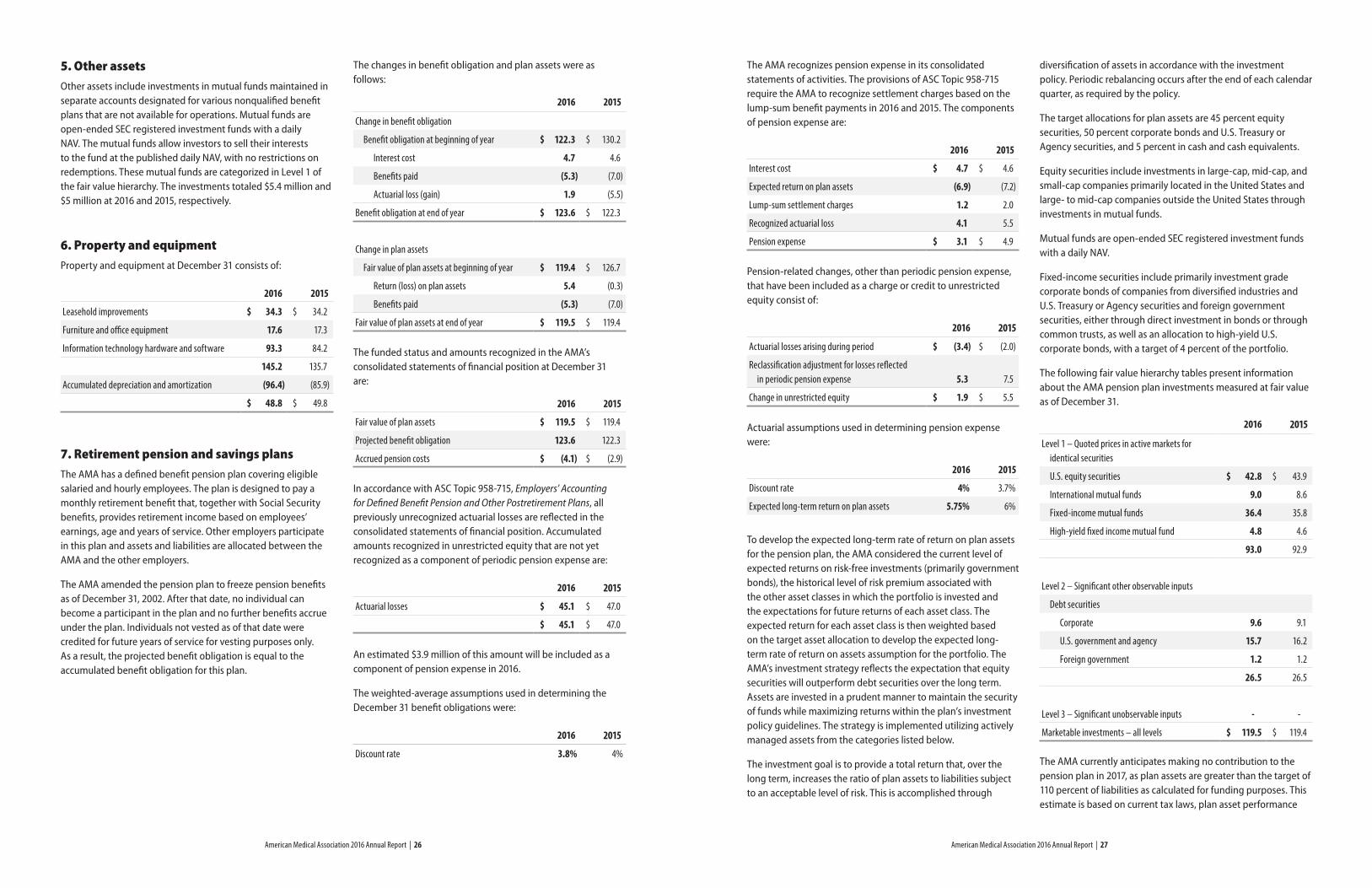
5. Other assetsOther assets include investments in mutual funds maintained in separate accounts designated for various nonqualified benefit plans that are not available for operations. Mutual funds are open-ended SEC registered investment funds with a daily NAV. The mutual funds allow investors to sell their interests to the fund at the published daily NAV, with no restrictions on redemptions. These mutual funds are categorized in Level 1 of the fair value hierarchy. The investments totaled $5.4 million and $5 million at 2016 and 2015, respectively.
6. Property and equipmentProperty and equipment at December 31 consists of:
2016 2015
Leasehold improvements $ 34.3 $ 34.2
Furniture and office equipment 17.6 17.3
Information technology hardware and software 93.3 84.2
145.2 135.7
Accumulated depreciation and amortization (96.4) (85.9)
$ 48.8 $ 49.8
7. Retirement pension and savings plansThe AMA has a defined benefit pension plan covering eligible salaried and hourly employees. The plan is designed to pay a monthly retirement benefit that, together with Social Security benefits, provides retirement income based on employees’ earnings, age and years of service. Other employers participate in this plan and assets and liabilities are allocated between the AMA and the other employers.
The AMA amended the pension plan to freeze pension benefits as of December 31, 2002. After that date, no individual can become a participant in the plan and no further benefits accrue under the plan. Individuals not vested as of that date were credited for future years of service for vesting purposes only. As a result, the projected benefit obligation is equal to the accumulated benefit obligation for this plan.
The changes in benefit obligation and plan assets were as follows:
2016 2015
Change in benefit obligation
Benefit obligation at beginning of year $ 122.3 $ 130.2
Interest cost 4.7 4.6
Benefits paid (5.3) (7.0)
Actuarial loss (gain) 1.9 (5.5)
Benefit obligation at end of year $ 123.6 $ 122.3
Change in plan assets
Fair value of plan assets at beginning of year $ 119.4 $ 126.7
Return (loss) on plan assets 5.4 (0.3)
Benefits paid (5.3) (7.0)
Fair value of plan assets at end of year $ 119.5 $ 119.4
The funded status and amounts recognized in the AMA’s consolidated statements of financial position at December 31 are:
2016 2015
Fair value of plan assets $ 119.5 $ 119.4
Projected benefit obligation 123.6 122.3
Accrued pension costs $ (4.1) $ (2.9)
In accordance with ASC Topic 958-715, Employers’ Accounting for Defined Benefit Pension and Other Postretirement Plans, all previously unrecognized actuarial losses are reflected in the consolidated statements of financial position. Accumulated amounts recognized in unrestricted equity that are not yet recognized as a component of periodic pension expense are:
2016 2015
Actuarial losses $ 45.1 $ 47.0
$ 45.1 $ 47.0
An estimated $3.9 million of this amount will be included as a component of pension expense in 2016.
The weighted-average assumptions used in determining the December 31 benefit obligations were:
2016 2015
Discount rate 3.8% 4%
The AMA recognizes pension expense in its consolidated statements of activities. The provisions of ASC Topic 958-715 require the AMA to recognize settlement charges based on the lump-sum benefit payments in 2016 and 2015. The components of pension expense are:
2016 2015
Interest cost $ 4.7 $ 4.6
Expected return on plan assets (6.9) (7.2)
Lump-sum settlement charges 1.2 2.0
Recognized actuarial loss 4.1 5.5
Pension expense $ 3.1 $ 4.9
Pension-related changes, other than periodic pension expense, that have been included as a charge or credit to unrestricted equity consist of:
2016 2015
Actuarial losses arising during period $ (3.4) $ (2.0)
Reclassification adjustment for losses reflected in periodic pension expense 5.3 7.5
Change in unrestricted equity $ 1.9 $ 5.5
Actuarial assumptions used in determining pension expense were:
2016 2015
Discount rate 4% 3.7%
Expected long-term return on plan assets 5.75% 6%
To develop the expected long-term rate of return on plan assets for the pension plan, the AMA considered the current level of expected returns on risk-free investments (primarily government bonds), the historical level of risk premium associated with the other asset classes in which the portfolio is invested and the expectations for future returns of each asset class. The expected return for each asset class is then weighted based on the target asset allocation to develop the expected long-term rate of return on assets assumption for the portfolio. The AMA’s investment strategy reflects the expectation that equity securities will outperform debt securities over the long term. Assets are invested in a prudent manner to maintain the security of funds while maximizing returns within the plan’s investment policy guidelines. The strategy is implemented utilizing actively managed assets from the categories listed below.
The investment goal is to provide a total return that, over the long term, increases the ratio of plan assets to liabilities subject to an acceptable level of risk. This is accomplished through
diversification of assets in accordance with the investment policy. Periodic rebalancing occurs after the end of each calendar quarter, as required by the policy.
The target allocations for plan assets are 45 percent equity securities, 50 percent corporate bonds and U.S. Treasury or Agency securities, and 5 percent in cash and cash equivalents.
Equity securities include investments in large-cap, mid-cap, and small-cap companies primarily located in the United States and large- to mid-cap companies outside the United States through investments in mutual funds.
Mutual funds are open-ended SEC registered investment funds with a daily NAV.
Fixed-income securities include primarily investment grade corporate bonds of companies from diversified industries and U.S. Treasury or Agency securities and foreign government securities, either through direct investment in bonds or through common trusts, as well as an allocation to high-yield U.S. corporate bonds, with a target of 4 percent of the portfolio.
The following fair value hierarchy tables present information about the AMA pension plan investments measured at fair value as of December 31.
2016 2015
Level 1 – Quoted prices in active markets for identical securities
U.S. equity securities $ 42.8 $ 43.9
International mutual funds 9.0 8.6
Fixed-income mutual funds 36.4 35.8
High-yield fixed income mutual fund 4.8 4.6
93.0 92.9
Level 2 – Significant other observable inputs
Debt securities
Corporate 9.6 9.1
U.S. government and agency 15.7 16.2
Foreign government 1.2 1.2
26.5 26.5
Level 3 – Significant unobservable inputs - -
Marketable investments – all levels $ 119.5 $ 119.4
The AMA currently anticipates making no contribution to the pension plan in 2017, as plan assets are greater than the target of 110 percent of liabilities as calculated for funding purposes. This estimate is based on current tax laws, plan asset performance
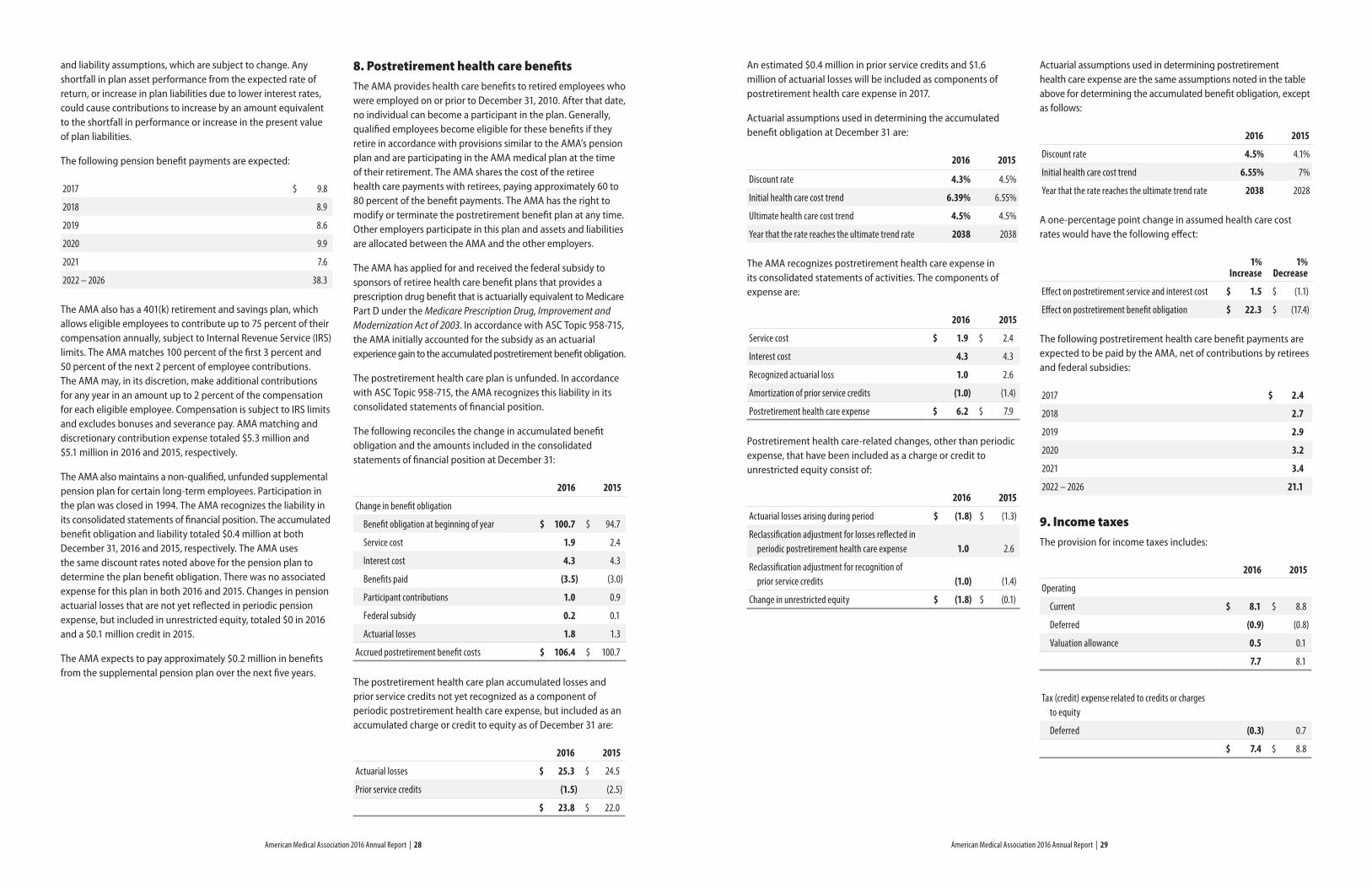
American Medical Association 2016 Annual Report | 28 American Medical Association 2016 Annual Report | 29
and liability assumptions, which are subject to change. Any shortfall in plan asset performance from the expected rate of return, or increase in plan liabilities due to lower interest rates, could cause contributions to increase by an amount equivalent to the shortfall in performance or increase in the present value of plan liabilities.
The following pension benefit payments are expected:
2017 $ 9.8
2018 8.9
2019 8.6
2020 9.9
2021 7.6
2022 – 2026 38.3
The AMA also has a 401(k) retirement and savings plan, which allows eligible employees to contribute up to 75 percent of their compensation annually, subject to Internal Revenue Service (IRS) limits. The AMA matches 100 percent of the first 3 percent and 50 percent of the next 2 percent of employee contributions. The AMA may, in its discretion, make additional contributions for any year in an amount up to 2 percent of the compensation for each eligible employee. Compensation is subject to IRS limits and excludes bonuses and severance pay. AMA matching and discretionary contribution expense totaled $5.3 million and $5.1 million in 2016 and 2015, respectively.
The AMA also maintains a non-qualified, unfunded supplemental pension plan for certain long-term employees. Participation in the plan was closed in 1994. The AMA recognizes the liability in its consolidated statements of financial position. The accumulated benefit obligation and liability totaled $0.4 million at both December 31, 2016 and 2015, respectively. The AMA uses the same discount rates noted above for the pension plan to determine the plan benefit obligation. There was no associated expense for this plan in both 2016 and 2015. Changes in pension actuarial losses that are not yet reflected in periodic pension expense, but included in unrestricted equity, totaled $0 in 2016 and a $0.1 million credit in 2015.
The AMA expects to pay approximately $0.2 million in benefits from the supplemental pension plan over the next five years.
8. Postretirement health care benefitsThe AMA provides health care benefits to retired employees who were employed on or prior to December 31, 2010. After that date, no individual can become a participant in the plan. Generally, qualified employees become eligible for these benefits if they retire in accordance with provisions similar to the AMA’s pension plan and are participating in the AMA medical plan at the time of their retirement. The AMA shares the cost of the retiree health care payments with retirees, paying approximately 60 to 80 percent of the benefit payments. The AMA has the right to modify or terminate the postretirement benefit plan at any time. Other employers participate in this plan and assets and liabilities are allocated between the AMA and the other employers.
The AMA has applied for and received the federal subsidy to sponsors of retiree health care benefit plans that provides a prescription drug benefit that is actuarially equivalent to Medicare Part D under the Medicare Prescription Drug, Improvement and Modernization Act of 2003. In accordance with ASC Topic 958-715, the AMA initially accounted for the subsidy as an actuarial experience gain to the accumulated postretirement benefit obligation.
The postretirement health care plan is unfunded. In accordance with ASC Topic 958-715, the AMA recognizes this liability in its consolidated statements of financial position.
The following reconciles the change in accumulated benefit obligation and the amounts included in the consolidated statements of financial position at December 31:
2016 2015
Change in benefit obligation
Benefit obligation at beginning of year $ 100.7 $ 94.7
Service cost 1.9 2.4
Interest cost 4.3 4.3
Benefits paid (3.5) (3.0)
Participant contributions 1.0 0.9
Federal subsidy 0.2 0.1
Actuarial losses 1.8 1.3
Accrued postretirement benefit costs $ 106.4 $ 100.7
The postretirement health care plan accumulated losses and prior service credits not yet recognized as a component of periodic postretirement health care expense, but included as an accumulated charge or credit to equity as of December 31 are:
2016 2015
Actuarial losses $ 25.3 $ 24.5
Prior service credits (1.5) (2.5)
$ 23.8 $ 22.0
An estimated $0.4 million in prior service credits and $1.6 million of actuarial losses will be included as components of postretirement health care expense in 2017.
Actuarial assumptions used in determining the accumulated benefit obligation at December 31 are:
2016 2015
Discount rate 4.3% 4.5%
Initial health care cost trend 6.39% 6.55%
Ultimate health care cost trend 4.5% 4.5%
Year that the rate reaches the ultimate trend rate 2038 2038
The AMA recognizes postretirement health care expense in its consolidated statements of activities. The components of expense are:
2016 2015
Service cost $ 1.9 $ 2.4
Interest cost 4.3 4.3
Recognized actuarial loss 1.0 2.6
Amortization of prior service credits (1.0) (1.4)
Postretirement health care expense $ 6.2 $ 7.9
Postretirement health care-related changes, other than periodic expense, that have been included as a charge or credit to unrestricted equity consist of:
2016 2015
Actuarial losses arising during period $ (1.8) $ (1.3)
Reclassification adjustment for losses reflected in periodic postretirement health care expense 1.0 2.6
Reclassification adjustment for recognition of prior service credits (1.0) (1.4)
Change in unrestricted equity $ (1.8) $ (0.1)
Actuarial assumptions used in determining postretirement health care expense are the same assumptions noted in the table above for determining the accumulated benefit obligation, except as follows:
2016 2015
Discount rate 4.5% 4.1%
Initial health care cost trend 6.55% 7%
Year that the rate reaches the ultimate trend rate 2038 2028
A one-percentage point change in assumed health care cost rates would have the following effect:
1% Increase
1% Decrease
Effect on postretirement service and interest cost $ 1.5 $ (1.1)
Effect on postretirement benefit obligation $ 22.3 $ (17.4)
The following postretirement health care benefit payments are expected to be paid by the AMA, net of contributions by retirees and federal subsidies:
2017 $ 2.4
2018 2.7
2019 2.9
2020 3.2
2021 3.4
2022 – 2026 21.1
9. Income taxesThe provision for income taxes includes:
2016 2015
Operating
Current $ 8.1 $ 8.8
Deferred (0.9) (0.8)
Valuation allowance 0.5 0.1
7.7 8.1
Tax (credit) expense related to credits or charges to equity
Deferred (0.3) 0.7
$ 7.4 $ 8.8
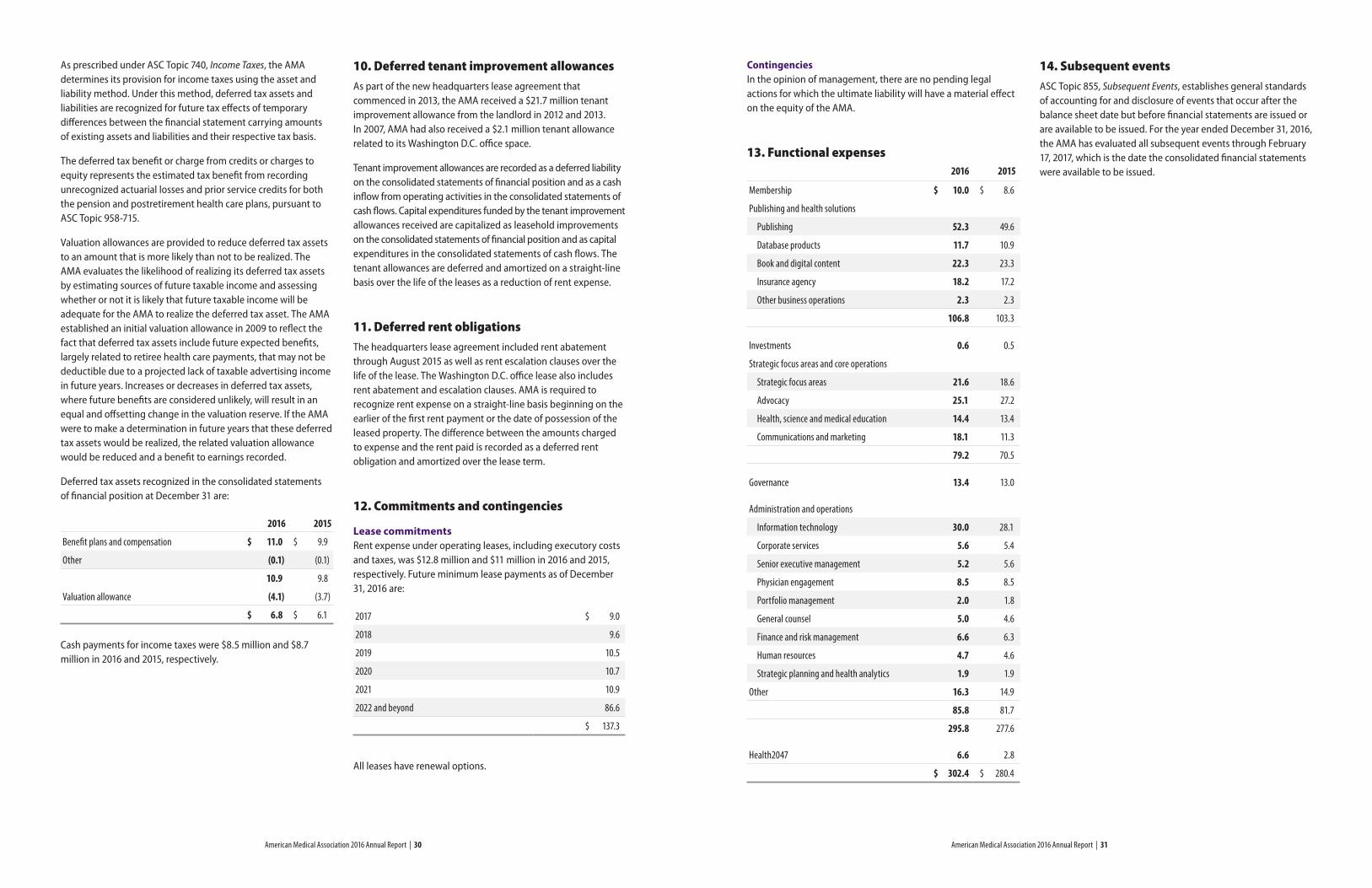
American Medical Association 2016 Annual Report | 30 American Medical Association 2016 Annual Report | 31
As prescribed under ASC Topic 740, Income Taxes, the AMA determines its provision for income taxes using the asset and liability method. Under this method, deferred tax assets and liabilities are recognized for future tax effects of temporary differences between the financial statement carrying amounts of existing assets and liabilities and their respective tax basis.
The deferred tax benefit or charge from credits or charges to equity represents the estimated tax benefit from recording unrecognized actuarial losses and prior service credits for both the pension and postretirement health care plans, pursuant to ASC Topic 958-715.
Valuation allowances are provided to reduce deferred tax assets to an amount that is more likely than not to be realized. The AMA evaluates the likelihood of realizing its deferred tax assets by estimating sources of future taxable income and assessing whether or not it is likely that future taxable income will be adequate for the AMA to realize the deferred tax asset. The AMA established an initial valuation allowance in 2009 to reflect the fact that deferred tax assets include future expected benefits, largely related to retiree health care payments, that may not be deductible due to a projected lack of taxable advertising income in future years. Increases or decreases in deferred tax assets, where future benefits are considered unlikely, will result in an equal and offsetting change in the valuation reserve. If the AMA were to make a determination in future years that these deferred tax assets would be realized, the related valuation allowance would be reduced and a benefit to earnings recorded.
Deferred tax assets recognized in the consolidated statements of financial position at December 31 are:
2016 2015
Benefit plans and compensation $ 11.0 $ 9.9
Other (0.1) (0.1)
10.9 9.8
Valuation allowance (4.1) (3.7)
$ 6.8 $ 6.1
Cash payments for income taxes were $8.5 million and $8.7 million in 2016 and 2015, respectively.
10. Deferred tenant improvement allowancesAs part of the new headquarters lease agreement that commenced in 2013, the AMA received a $21.7 million tenant improvement allowance from the landlord in 2012 and 2013. In 2007, AMA had also received a $2.1 million tenant allowance related to its Washington D.C. office space.
Tenant improvement allowances are recorded as a deferred liability on the consolidated statements of financial position and as a cash inflow from operating activities in the consolidated statements of cash flows. Capital expenditures funded by the tenant improvement allowances received are capitalized as leasehold improvements on the consolidated statements of financial position and as capital expenditures in the consolidated statements of cash flows. The tenant allowances are deferred and amortized on a straight-line basis over the life of the leases as a reduction of rent expense.
11. Deferred rent obligationsThe headquarters lease agreement included rent abatement through August 2015 as well as rent escalation clauses over the life of the lease. The Washington D.C. office lease also includes rent abatement and escalation clauses. AMA is required to recognize rent expense on a straight-line basis beginning on the earlier of the first rent payment or the date of possession of the leased property. The difference between the amounts charged to expense and the rent paid is recorded as a deferred rent obligation and amortized over the lease term.
12. Commitments and contingencies
Lease commitmentsRent expense under operating leases, including executory costs and taxes, was $12.8 million and $11 million in 2016 and 2015, respectively. Future minimum lease payments as of December 31, 2016 are:
2017 $ 9.0
2018 9.6
2019 10.5
2020 10.7
2021 10.9
2022 and beyond 86.6
$ 137.3
All leases have renewal options.
ContingenciesIn the opinion of management, there are no pending legal actions for which the ultimate liability will have a material effect on the equity of the AMA.
13. Functional expenses 2016 2015
Membership $ 10.0 $ 8.6
Publishing and health solutions
Publishing 52.3 49.6
Database products 11.7 10.9
Book and digital content 22.3 23.3
Insurance agency 18.2 17.2
Other business operations 2.3 2.3
106.8 103.3
Investments 0.6 0.5
Strategic focus areas and core operations
Strategic focus areas 21.6 18.6
Advocacy 25.1 27.2
Health, science and medical education 14.4 13.4
Communications and marketing 18.1 11.3
79.2 70.5
Governance 13.4 13.0
Administration and operations
Information technology 30.0 28.1
Corporate services 5.6 5.4
Senior executive management 5.2 5.6
Physician engagement 8.5 8.5
Portfolio management 2.0 1.8
General counsel 5.0 4.6
Finance and risk management 6.6 6.3
Human resources 4.7 4.6
Strategic planning and health analytics 1.9 1.9
Other 16.3 14.9
85.8 81.7
295.8 277.6
Health2047 6.6 2.8
$ 302.4 $ 280.4
14. Subsequent eventsASC Topic 855, Subsequent Events, establishes general standards of accounting for and disclosure of events that occur after the balance sheet date but before financial statements are issued or are available to be issued. For the year ended December 31, 2016, the AMA has evaluated all subsequent events through February 17, 2017, which is the date the consolidated financial statements were available to be issued.
American Medical Association 2016 Annual Report | 33American Medical Association 2016 Annual Report | 32
Independent Auditor’s Report
The Board of Trustees of American Medical Association
We have audited the accompanying consolidated financial statements of the American Medical Association (the “AMA”) and subsidiaries, which comprise the consolidated statements of financial position as of December 31, 2016 and 2015, and the related consolidated statements of activities and of cash flows for the years then ended, and the related notes to the consolidated financial statements.
Management’s Responsibility for the Consolidated Financial StatementsManagement is responsible for the preparation and fair presentation of these consolidated financial statements in accordance with accounting principles generally accepted in the United States of America; this includes the design, implementation, and maintenance of internal control relevant to the preparation and fair presentation of consolidated financial statements that are free from material misstatement, whether due to fraud or error.
Auditors’ ResponsibilityOur responsibility is to express an opinion on these consolidated financial statements based on our audits. We conducted our audits in accordance with auditing standards generally accepted in the United States of America. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the consolidated financial statements are free from material misstatement.
An audit involves performing procedures to obtain audit evidence about the amounts and disclosures in the consolidated
financial statements. The procedures selected depend on the auditor’s judgment, including the assessment of the risks of material misstatement of the consolidated financial statements, whether due to fraud or error. In making those risk assessments, the auditor considers internal control relevant to the AMA’s preparation and fair presentation of the consolidated financial statements in order to design audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of the AMA’s internal control. Accordingly, we express no such opinion. An audit also includes evaluating the appropriateness of accounting policies used and the reasonableness of significant accounting estimates made by management, as well as evaluating the overall presentation of the consolidated financial statements.
We believe that the audit evidence we have obtained is sufficient and appropriate to provide a basis for our audit opinion.
OpinionIn our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the financial position of the American Medical Association and subsidiaries as of December 31, 2016 and 2015, and the results of its activities and changes in its equity and its cash flows for the years then ended in accordance with accounting principles generally accepted in the United States of America.
Deloitte & Touche LLP Chicago, Illinois February 17, 2017
Written Statement of Certification of Chief Executive Officer and Chief Financial OfficerThe undersigned hereby certify that the information contained in the audited financial statements of the American Medical Association for the years ended December 31, 2016 and 2015 fairly presents, in all material respects, the financial condition and the results of operations of the American Medical Association.
James L. Madara, MD Executive Vice President and Chief Executive Officer
Denise M. Hagerty Senior Vice President and Chief Financial Officer
February 17, 2017
Executive CommitteePatrice A. Harris, MD, MA, Chair
Gerald E. Harmon, MD
Andrew W. Gurman, MD
David O. Barbe, MD, MHA
Steven J. Stack, MD
Jack Resneck Jr., MD
Susan R. Bailey, MD
Stephen R. Permut, MD, JD
Audit CommitteeGeorgia A. Tuttle, MD, Chair
Willarda V. Edwards, MD, MBA
Russell W.H. Kridel, MD
William A. McDade, MD, PhD
Albert J. Osbahr III, MD
Jack Resneck Jr., MD
Bruce A. Scott, MD
Awards and Nominations CommitteeAlbert J. Osbahr III, MD, Chair
Jesse M. Ehrenfeld, MD, MBA
Russell W.H. Kridel, MD
Omar Z. Maniya, MBA
Barbara L. McAneny, MD
William A. McDade, MD, PhD
Bruce A. Scott, MD
Compensation CommitteeDavid O. Barbe, MD, MHA, Chair
William E. Kobler, MD
Jack Resneck Jr., MD
Carl A. Sirio, MD
Patrice A. Harris, MD, MA (ex-officio w/vote)
Gerald E. Harmon, MD (ex-officio w/vote)
Stephen R. Permut, MD, JD (ex-officio w/vote)
Andrew W. Gurman, MD President
David O. Barbe, MD, MHA President-elect
Steven J. Stack, MD Immediate Past President
Susan R. Bailey, MD Speaker, House of Delegates
Bruce A. Scott, MD Vice Speaker, House of Delegates
Patrice A. Harris, MD, MA Chair
Gerald E. Harmon, MD Chair-elect
Stephen R. Permut, MD, JD Immediate Past Chair
Jack Resneck Jr., MD Secretary
Maya A. Babu, MD, MBA
Willarda V. Edwards, MD, MBA
Jesse M. Ehrenfeld, MD, MPH
William E. Kobler, MD
Russell W.H. Kridel, MD
Omar Z. Maniya, MBA
Barbara L. McAneny, MD
William A. McDade, MD, PhD
Albert J. Osbahr III, MD
Carl A. Sirio, MD
Georgia A. Tuttle, MD
Kevin W. Williams
Executive ManagementJames L. Madara, MD Executive Vice President and Chief Executive Officer
Standing Committees
Finance CommitteeJack Resneck Jr., MD, Chair
Maya A. Babu, MD, MBA
Susan R. Bailey, MD
David O. Barbe, MD, MHA
Willarda V. Edwards, MD, MBA
Georgia A. Tuttle, MD
Kevin W. Williams
Note: Drs. Harris, Harmon and Permut serve on all committees, except where otherwise noted, as ex-officio members without vote. Dr. Gurman serves on all committees as an ex-officio member with vote.
Board of Trustees
© 2017 American Medical Association. All rights reserved.17:68848:4/17
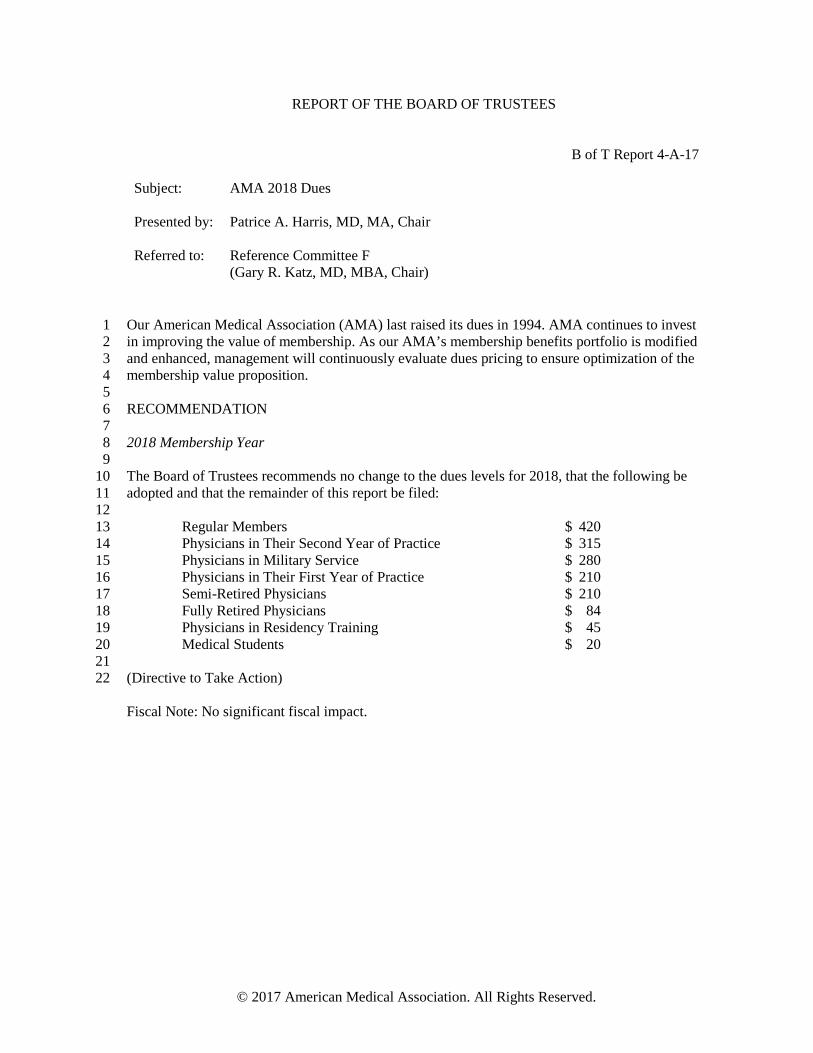
REPORT OF THE BOARD OF TRUSTEES
B of T Report 4-A-17 Subject: AMA 2018 Dues Presented by:
Patrice A. Harris, MD, MA, Chair
Referred to:
Reference Committee F
(Gary R. Katz, MD, MBA, Chair)
Our American Medical Association (AMA) last raised its dues in 1994. AMA continues to invest 1 in improving the value of membership. As our AMA’s membership benefits portfolio is modified 2 and enhanced, management will continuously evaluate dues pricing to ensure optimization of the 3 membership value proposition. 4 5 RECOMMENDATION 6 7 2018 Membership Year 8 9 The Board of Trustees recommends no change to the dues levels for 2018, that the following be 10 adopted and that the remainder of this report be filed: 11 12 Regular Members $ 420 13 Physicians in Their Second Year of Practice $ 315 14 Physicians in Military Service $ 280 15 Physicians in Their First Year of Practice $ 210 16 Semi-Retired Physicians $ 210 17 Fully Retired Physicians $ 84 18 Physicians in Residency Training $ 45 19 Medical Students $ 20 20 21 (Directive to Take Action) 22 Fiscal Note: No significant fiscal impact.
© 2017 American Medical Association. All Rights Reserved.
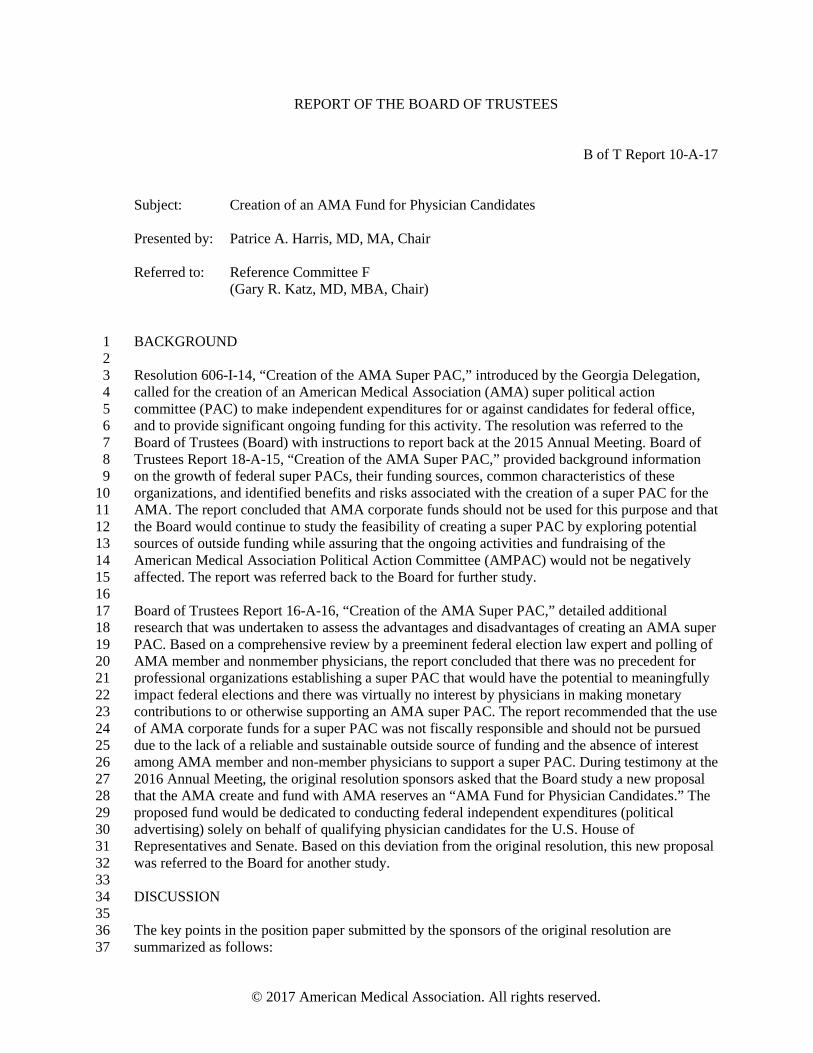
REPORT OF THE BOARD OF TRUSTEES
B of T Report 10-A-17
Subject: Creation of an AMA Fund for Physician Candidates Presented by:
Patrice A. Harris, MD, MA, Chair
Referred to:
Reference Committee F
(Gary R. Katz, MD, MBA, Chair) BACKGROUND 1 2 Resolution 606-I-14, “Creation of the AMA Super PAC,” introduced by the Georgia Delegation, 3 called for the creation of an American Medical Association (AMA) super political action 4 committee (PAC) to make independent expenditures for or against candidates for federal office, 5 and to provide significant ongoing funding for this activity. The resolution was referred to the 6 Board of Trustees (Board) with instructions to report back at the 2015 Annual Meeting. Board of 7 Trustees Report 18-A-15, “Creation of the AMA Super PAC,” provided background information 8 on the growth of federal super PACs, their funding sources, common characteristics of these 9 organizations, and identified benefits and risks associated with the creation of a super PAC for the 10 AMA. The report concluded that AMA corporate funds should not be used for this purpose and that 11 the Board would continue to study the feasibility of creating a super PAC by exploring potential 12 sources of outside funding while assuring that the ongoing activities and fundraising of the 13 American Medical Association Political Action Committee (AMPAC) would not be negatively 14 affected. The report was referred back to the Board for further study. 15 16 Board of Trustees Report 16-A-16, “Creation of the AMA Super PAC,” detailed additional 17 research that was undertaken to assess the advantages and disadvantages of creating an AMA super 18 PAC. Based on a comprehensive review by a preeminent federal election law expert and polling of 19 AMA member and nonmember physicians, the report concluded that there was no precedent for 20 professional organizations establishing a super PAC that would have the potential to meaningfully 21 impact federal elections and there was virtually no interest by physicians in making monetary 22 contributions to or otherwise supporting an AMA super PAC. The report recommended that the use 23 of AMA corporate funds for a super PAC was not fiscally responsible and should not be pursued 24 due to the lack of a reliable and sustainable outside source of funding and the absence of interest 25 among AMA member and non-member physicians to support a super PAC. During testimony at the 26 2016 Annual Meeting, the original resolution sponsors asked that the Board study a new proposal 27 that the AMA create and fund with AMA reserves an “AMA Fund for Physician Candidates.” The 28 proposed fund would be dedicated to conducting federal independent expenditures (political 29 advertising) solely on behalf of qualifying physician candidates for the U.S. House of 30 Representatives and Senate. Based on this deviation from the original resolution, this new proposal 31 was referred to the Board for another study. 32 33 DISCUSSION 34 35 The key points in the position paper submitted by the sponsors of the original resolution are 36 summarized as follows: 37
© 2017 American Medical Association. All rights reserved.
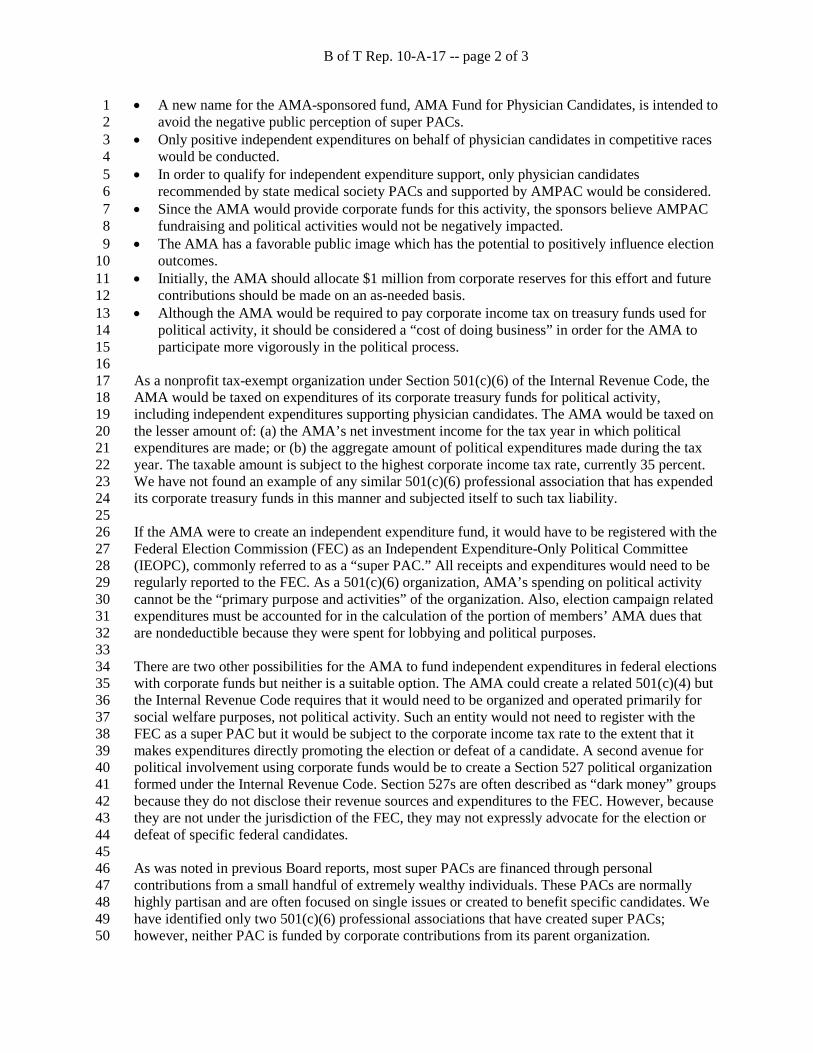
B of T Rep. 10-A-17 -- page 2 of 3
• A new name for the AMA-sponsored fund, AMA Fund for Physician Candidates, is intended to 1 avoid the negative public perception of super PACs. 2
• Only positive independent expenditures on behalf of physician candidates in competitive races 3 would be conducted. 4
• In order to qualify for independent expenditure support, only physician candidates 5 recommended by state medical society PACs and supported by AMPAC would be considered. 6
• Since the AMA would provide corporate funds for this activity, the sponsors believe AMPAC 7 fundraising and political activities would not be negatively impacted. 8
• The AMA has a favorable public image which has the potential to positively influence election 9 outcomes. 10
• Initially, the AMA should allocate $1 million from corporate reserves for this effort and future 11 contributions should be made on an as-needed basis. 12
• Although the AMA would be required to pay corporate income tax on treasury funds used for 13 political activity, it should be considered a “cost of doing business” in order for the AMA to 14 participate more vigorously in the political process. 15
16 As a nonprofit tax-exempt organization under Section 501(c)(6) of the Internal Revenue Code, the 17 AMA would be taxed on expenditures of its corporate treasury funds for political activity, 18 including independent expenditures supporting physician candidates. The AMA would be taxed on 19 the lesser amount of: (a) the AMA’s net investment income for the tax year in which political 20 expenditures are made; or (b) the aggregate amount of political expenditures made during the tax 21 year. The taxable amount is subject to the highest corporate income tax rate, currently 35 percent. 22 We have not found an example of any similar 501(c)(6) professional association that has expended 23 its corporate treasury funds in this manner and subjected itself to such tax liability. 24 25 If the AMA were to create an independent expenditure fund, it would have to be registered with the 26 Federal Election Commission (FEC) as an Independent Expenditure-Only Political Committee 27 (IEOPC), commonly referred to as a “super PAC.” All receipts and expenditures would need to be 28 regularly reported to the FEC. As a 501(c)(6) organization, AMA’s spending on political activity 29 cannot be the “primary purpose and activities” of the organization. Also, election campaign related 30 expenditures must be accounted for in the calculation of the portion of members’ AMA dues that 31 are nondeductible because they were spent for lobbying and political purposes. 32 33 There are two other possibilities for the AMA to fund independent expenditures in federal elections 34 with corporate funds but neither is a suitable option. The AMA could create a related 501(c)(4) but 35 the Internal Revenue Code requires that it would need to be organized and operated primarily for 36 social welfare purposes, not political activity. Such an entity would not need to register with the 37 FEC as a super PAC but it would be subject to the corporate income tax rate to the extent that it 38 makes expenditures directly promoting the election or defeat of a candidate. A second avenue for 39 political involvement using corporate funds would be to create a Section 527 political organization 40 formed under the Internal Revenue Code. Section 527s are often described as “dark money” groups 41 because they do not disclose their revenue sources and expenditures to the FEC. However, because 42 they are not under the jurisdiction of the FEC, they may not expressly advocate for the election or 43 defeat of specific federal candidates. 44 45 As was noted in previous Board reports, most super PACs are financed through personal 46 contributions from a small handful of extremely wealthy individuals. These PACs are normally 47 highly partisan and are often focused on single issues or created to benefit specific candidates. We 48 have identified only two 501(c)(6) professional associations that have created super PACs; 49 however, neither PAC is funded by corporate contributions from its parent organization. 50
B of T Rep. 10-A-17 -- page 3 of 3
While super PACs continue to play an outsized role in elections—spending on federal campaigns 1 reported to the FEC for the 2016 election cycle was $1.1 billion—their effectiveness is not 2 universally accepted. Super PAC contributions to opposing candidates in most competitive races 3 tend to cancel out each other. For example, super PAC spending in U.S. Senate races this cycle 4 totaled $500 million, including $52 million in their efforts to influence the outcome of the Nevada 5 Senate race involving Dr. Joe Heck. Even though super PAC expenditures favoring Dr. Heck 6 exceeded those on behalf of his opponent, he lost that election. 7 8 The AMA commissioned a poll of AMA member and non-member physicians last year to assess 9 physician support for the creation of an AMA super PAC and their willingness to contribute to it. 10 As noted in Board of Trustees Report 16-A-16, 87 percent of the respondents said they would not 11 be likely to donate to an AMA super PAC. The reasons they cited for their lack of interest were 12 that the super PAC might contribute to candidates they do not personally support; they do not agree 13 with the concept of super PACs; they are not politically inclined or in general do not make political 14 contributions; or their political views do not align with those of the AMA. The general finding 15 from that poll was that there was little to no interest by either AMA or non-member physicians in 16 making monetary contributions to or otherwise supporting an AMA-established super PAC. 17 18 In late February of this year, the AMA sponsored a poll of AMA member physicians to gauge 19 reaction to the AMA creating and using corporate funds for partisan political activity. The top 20 messages we tested in support of establishing this fund for this purpose were that organized 21 medicine needs more champions in Congress and that the fund would help make sure physician 22 candidates have the financial support they need, especially in highly competitive races. The top 23 arguments in opposition to the fund were that the use of AMA corporate funds for election 24 activities could alienate some AMA members who might object from a partisan or ethical 25 perspective and that there would be significant tax implications to the AMA. 26 27 There was initial support for a “Fund for Physician Candidates” when it was not identified as a 28 super PAC. A majority of respondents (65 percent) expressed support; however, the intensity of 29 support was extremely low. Only 11 percent “strongly” supported the creation of a fund, while a 30 majority (54 percent) said they “only somewhat” supported it. When AMA members learned that 31 the fund would be a super PAC funded by AMA corporate funds, opposition to the establishment 32 of this fund increased and its support decreased. Support for the fund fell to less than a majority (47 33 percent) and opposition to it rose to 32 percent. 34 35 RECOMMENDATION 36 37 While the Board fully understands the goal of enhancing the AMA’s advocacy efforts in Congress, 38 we continue to have significant concerns about expending corporate treasury funds for the purpose 39 of influencing federal elections and the reaction this activity might have among portions of our 40 AMA membership due to their own personal partisan and ethical viewpoints. As noted earlier, the 41 results of our two physician polls conducted in 2016 and earlier this year indicate little support for 42 the creation of an AMA super PAC. 43 44 Therefore, the Board of Trustees recommends that the following be adopted in lieu of Resolution 45 606-I-14 and that the remainder of this report be filed: 46 47
That our American Medical Association not use AMA corporate treasury funds to engage in 48 partisan political activity. (New HOD Policy) 49 Fiscal Note: Less than $500.
REPORT OF THE BOARD OF TRUSTEES
B of T Report 16-A-17
Subject: Oppose Physician Gun Gag Rule Policy by Taking our AMA Business Elsewhere Presented by:
Patrice A. Harris, MD, MA, Chair
Referred to:
Reference Committee F
(Gary R. Katz, MD, MBA, Chair) Resolution 604-I-16, introduced by American Thoracic Society, asked that our American Medical 1 Association (AMA) adopt policy that bars our AMA from holding House of Delegates (HOD) 2 meetings in states that enact physician gun gag laws, and that our AMA contact governors and 3 convention bureaus of states that have enacted physician gun gag rules to inform them that our 4 AMA will no longer hold House of Delegates meetings in their state, until the restrictive physician 5 gun gag rule is repealed or struck down by the courts. 6 7 A few states have enacted some form of “gun gag” laws. Currently Montana prohibits physicians 8 from requiring patients to answer questions about guns as a condition of receiving care, Missouri 9 prohibits requiring physicians to ask or record information about patient gun ownership, and 10 Minnesota prohibits the state health programs from collecting data about gun ownership. In 11 addition, “gun gag” bills have been introduced in Iowa and Texas recently. Similar bills have been 12 introduced in Indiana (prohibits requiring physicians to ask and record) and Oklahoma. 13 14 Major AMA meetings are not typically held in Montana, Missouri, Minnesota, Iowa, Indiana or 15 Oklahoma and none are currently planned in these states. 16 17 While the State of Florida had enacted such a provision (The Firearms Owner’s Privacy Law 18 (FOPL)), that law was overturned by the 11th Circuit Court of Appeals on February 16, 2017. The 19 State of Florida may appeal that decision to the Supreme Court, which may or may not take up that 20 appeal if made. In the meantime, the 2021 Interim Meeting of the House of Delegates is contracted 21 for Orlando, Florida. The cancellation fee for that meeting within two years of the planned date and 22 moving to a new location would be $424,000. Orlando is being considered for future meetings as 23 well. 24 25 Texas is the only other state currently contemplating a gun gag law where the AMA has held major 26 meetings in the past and has viable venues for the future. 27 28 DISCUSSION: 29 30 Often, AMA meeting venues are selected several years in advance to secure locations and begin 31 meeting planning. Among the other considerations, management is directed by current AMA 32 policy to choose hotels for its meetings, conferences, and conventions based on size, service, 33 location, cost, and similar factors. For our Interim and Annual meetings, efforts are made to locate 34 the Section Assembly Meetings in the House of Delegates Meeting hotel or in a hotel in close 35 proximity. In addition, policy directs management to not hold meetings in locations that have 36 exclusionary policies, only in venues that require smoke-free worksites and public places, and to 37
© 2017 American Medical Association. All rights reserved.
B of T Rep 16-A-17 -- page 2 of 2
work with facilities where AMA meetings are held to designate an area for breastfeeding and breast 1 pumping (Policy G-630.140). 2 3 By policy the Annual meeting is held each year in Chicago. There are relatively small number of 4 venues that can handle the size and scope of an AMA Interim Meeting without spreading out to 5 multiple hotels and convention center type arrangements which have proven to be less than 6 satisfactory. Management attempts to schedule Interim meetings in variable locations in different 7 regions of our United States and delegates have expressed displeasure with a number of potential 8 venues that have been used in the past. 9 10 As evidenced by Florida, it is possible that legislation contrary to AMA policy may be enacted and 11 later repealed or overturned. Conversely, states that have no such legislation at the time a meeting 12 is scheduled, may subsequently introduce or adopt legislation that would be found objectionable by 13 the time the meeting is convened. 14 15 The AMA has extensive policy on public health issues as well as multiple other policies impacting 16 the health of our patients and physician practice. While the Board recognizes gun violence as a 17 major public health issue they also believe there are a number of other high priority AMA policies. 18 It would be difficult if not impossible to monitor the compliance of states or cities with AMA 19 policy and move meeting venues accordingly. 20 21 In reference committee delegates expressed that if a meeting occurs in a state where laws or 22 statutes are contrary to AMA policy that this provides an opportunity for the AMA to “speak out” 23 on the issue. AMA advocacy activities, working with our local and state medical association 24 partners, does not typically include the selection of venues for our meetings. Convening a meeting 25 at a venue does not endorse the behavior of the hotel, city or state. 26 27 CONCLUSION: 28 29 AMA management considers multiple factors including the directives of the HOD in selecting 30 venues for AMA meetings. Site selection occurs years in advance and typically reservation of 31 select sites requires significant cancellation penalties. Even without consideration of the financial 32 penalty for late cancellation, identifying an available suitable substitute venue becomes 33 increasingly difficult as the meeting date approaches. State and local jurisdictions may at any time 34 adopt legislation or rules that are not aligned with AMA policy including “gun gag” laws. 35 36 The Board of Trustees would prefer AMA meetings always be held in cities and states that 37 embrace AMA policy but recognizes the challenges management faces in selecting venues 38 particularly for the House of Delegates meetings. The Board has requested AMA management to 39 keep a vigilant eye on “gun gag” laws and similar types of laws when selecting future meeting 40 locations. AMA management will be closely monitoring the situation in Florida and Texas; should 41 the gag rule gain new life, we will review our AMA’s options. 42 43 RECOMMENDATION: 44 45 Given that the Board and management will be alert to “gun gag” laws and similar types of laws 46 when selecting future meeting sites even without a specific rigid policy, the Board of Trustees 47 recommends that Resolution 602-I-17 not be adopted and the remainder of the report be filed. 48
REPORT OF THE BOARD OF TRUSTEES
B of T Report 17-A-17
Subject: Equality for Future Meetings Organized or Sponsored by the AMA Presented by:
Patrice Harris, MD, MA, Chair
Referred to:
Reference Committee F
(Gary R. Katz, MD, MBA, Chair) Resolution 602-I-16, “Equality for Future Meetings Organized or Sponsored by the AMA,” 1 introduced by the Young Physicians Section, asked that all future meetings and conferences 2 organized and/or sponsored by our American Medical Association (AMA), not yet contracted, only 3 be held in towns, cities, counties and states that do not have discriminatory policies based on race, 4 color, religion, ethnic origin, national origin, language, creed, sex, sexual orientation, gender, 5 gender identity and gender expression, disability, or age. 6 7 The reference committee recommended referral of the resolution based on a variety of divided 8 testimony involving the complexity of staying abreast of developments across such a wide swath of 9 governmental units and concerns that laws and ordinances may change, and thus communities may 10 be overlooked or inappropriately considered based on outdated information, and also testimony that 11 there may be other categories of non-discrimination not incorporated in the resolution. Testimony 12 also noted that the policy should not restrict AMA business decisions in unproductive or costly 13 ways and suggested establishing a process to vet these types of decisions. 14 15 Our AMA has strong policies against discrimination in all forms and our current policy on lodging 16 and accommodations includes non-discrimination. Nevertheless, the Board is supportive of the 17 spirit and intent of the resolution and believes modifying AMA Policy G-630.140, “Lodging, 18 Meeting Venues, and Social Functions,” accordingly is desirable. 19 20 AMA management already has processes in place in its selection of sites and corresponding 21 contract negotiations to minimize unproductive or overly costly meeting venues. The Board has 22 requested AMA management to negotiate cancellation provisions into contracts for future meetings 23 for this non-discrimination purpose whenever possible and fiscally reasonable. 24 25 In examining this issue the Board notes that current AMA Policy G-630.140, while addressing 26 clubs, restaurants or other institutions, does not specifically address towns, cities, counties and 27 states. The Board’s recommendation addresses that issue. 28 29 RECOMMENDATION 30 31 The Board of Trustees recommends that Policy G-630.140 be amended by addition to read as 32 follows in lieu of Resolution 602-I-16, and that the remainder of this report be filed: 33 34
AMA policy on lodging and accommodations includes the following: (1) Our AMA supports 35 choosing hotels for its meetings, conferences, and conventions based on size, service, location, 36 cost, and similar factors. (2) Our AMA shall attempt, when allocating meeting space, to locate 37
© 2017 American Medical Association. All rights reserved.
B of T Rep. 17-A-17 -- page 2 of 2
the Section Assembly Meetings in the House of Delegates Meeting hotel or in a hotel in close 1 proximity. (3) All meetings and conferences organized and/or primarily sponsored by our 2 AMA will be held in a town, city, county, or state that has enacted comprehensive legislation 3 requiring smoke-free worksites and public places (including restaurants and bars), unless 4 intended or existing contracts or special circumstances justify an exception to this policy, and 5 our AMA encourages state and local medical societies, national medical specialty societies, 6 and other health organizations to adopt a similar policy. (4) It is the policy of our AMA not to 7 hold meetings organized and/or primarily sponsored by our AMA, in cities, counties, or states, 8 or pay member, officer or employee dues in any club, restaurant, or other institution, that has 9 exclusionary policies, including, but not limited to, policies based on, race, color, religion, 10 national origin, ethnic origin, language, creed, sex, sexual orientation, gender, gender 11 identity and gender expression, disability, or age unless intended or existing contracts or 12 special circumstances justify an exception to this policy. (5) Our AMA staff will work with 13 facilities where AMA meetings are held to designate an area for breastfeeding and breast 14 pumping. 15
Fiscal note: Less than $500.
AMERICAN MEDICAL ASSOCIATION HOUSE OF DELEGATES
Resolution: 601 (A-17)
Introduced by: New York Subject: Reinstate the AMA Commission to Eliminate Health Care Disparities Referred to: Reference Committee F (Gary R. Katz, MD, Chair) Whereas, In December 2016, .the American Medical Association Steering Committee dissolved 1 the Commission to Eliminate Health Care Disparities (CHECD); and 2 3 Whereas, The AMA’s Steering Committee made the decision as they are responsible under 4 CEHCD bylaws for establishing and maintaining the direction of the CEHCD, and making 5 recommendations that are consistent with its mission, vision and functions; and 6 7 Whereas, The AMA has indicated that corporate sponsorship has waned in recent years and 8 that the AMA is no longer collectively able to provide the resources necessary to generate 9 income to support the CEHCD; and 10 11 Whereas, There is a looming Congressional battle over the mechanism to provide health care 12 which could significantly increase health disparities; and 13 14 Whereas, There has been a recent increase in violence and discrimination amongst various 15 people due to race, ethnicity, culture, religious beliefs, sexual orientation, gender and gender 16 identify; and 17 18 Whereas, This violence may impact upon health and health outcomes, and 19 20 Whereas, Reconstituting the AMA Commission to Eliminate Health Care Disparities is of utmost 21 importance at this point in the history of the United States and sends a strong message to the 22 country that medicine cares about these issues; therefore be it 23 24 RESOLVED, That our American Medical Association reinstate the Commission to Eliminate 25 Health Care Disparities, including goals and objectives that are Specific, Measurable, Agreed 26 Upon, Realistic and Time Related (SMART) metrics. (Directive to Take Action) 27 Fiscal Note: Estimated annual cost of $50,000 for two yearly meetings. Received: 04/28/17
AMERICAN MEDICAL ASSOCIATION HOUSE OF DELEGATES
Resolution: 602 (A-17)
Introduced by: American Medical Women’s Association Subject: Studying Healthcare Institutions that Provide Child Care Services Referred to: Reference Committee F (Gary R. Katz, MD, Chair) Whereas, Physicians with pre-school age children face significant difficulties finding childcare 1 that is easily accessible to their work place, is affordable, and accommodates the unpredictable 2 work hours faced by physicians; and 3 4 Whereas, This lack of childcare can place additional stress on already stressful careers, likely 5 contributing to burnout, especially for younger physicians; and 6 7 Whereas, Some businesses are starting to provide childcare services, utilizing a variety of 8 funding models; and 9 10 Whereas, Some healthcare institutions are also starting to provide these services; and 11 12 Whereas, Provision of these services could help with retention of physicians, especially those 13 earlier in their careers; and 14 15 Whereas, The number and size of institutions offering this and the models that they use to do so 16 are unknown; therefore be it 17 18 RESOLVED, That our American Medical Association (AMA) study which healthcare institutions 19 currently provide accessible, affordable childcare care services, including the size of the 20 institutions (in terms of the number of physicians) providing these services, the impact of these 21 services on residents and faculty (especially in terms of decreasing stress and increasing 22 retention), and the various funding models used for these (Directive to Take Action); and be it 23 further 24 25 RESOLVED, That our AMA report back to the House of Delegates at the 2018 Annual Meeting 26 the results of its study on which healthcare institutions are providing accessible and affordable 27 childcare care services, how these services are organized, and the various funding models that 28 are utilized. (Directive to Take Action)29 Fiscal Note: Not yet determined Received: 05/02/17 RELEVANT AMA POLICY Child Care in Hospitals H-215.985 Our AMA: (1) strongly encourages hospitals to establish and support child care facilities; (2) encourages that priority be given to children of those in training and that services be structured to take their needs into consideration; (3) supports informing the AHA, hospital medical staffs, and residency program directors of these policies; and (4) supports studying the elements of quality child care and availability of child care on a 24-hour basis. BOT Rep. J, I-90 Reaffirmed: Sunset Report, I-00 Reaffirmed: CME Rep. 2, A-10
AMERICAN MEDICAL ASSOCIATION HOUSE OF DELEGATES
Resolution: 603
(A-17)
Introduced by: Medical Student Section
Subject: Sexual Orientation and Gender Identity Demographic Collection by the AMA Referred to: Reference Committee F (Gary R. Katz, MD, Chair) Whereas, An estimated 5.2 to 9.5 million adults (2.2% to 4.4% of the adult population) in the 1 United States identify as lesbian, gay, bisexual, and/or transgender (LGBT);1 and 2 3 Whereas, Physician diversity that is reflective of patient demographics has been positively 4 associated with improved patient health outcomes, reduced stigmatization of LGBT patients, 5 and enhanced workforce development;2 and 6 7 Whereas, Medical organizations (e.g. Association of American Medical Colleges) collect sexual 8 orientation and gender identity demographics;3 and 9 10 Whereas, Public policy research groups (e.g. The Williams Institute) and research centers 11 focused on LGBT health issues (e.g. The Fenway Institute) have developed best practices and 12 guidelines for collecting this information in population-based surveys and the clinical setting;4,5 13 and 14 15 Whereas, Pursuant to AMA Policy G-635.125, the AMA gathers stratified demographics of its 16 AMA membership, the nature of which includes age, gender, race/ethnicity, education, life 17 stage, present employment, and self-designated specialty; and 18 19 Whereas, The AMA does not have existing policy to collect sexual orientation and gender 20 identity within the AMA Physician Masterfile; and 21 22 Whereas, Expanding the collection of demographic data to include members’ sexual 23 orientations and gender identities will empower the AMA to identify and address professional 24 needs and concerns of an often-marginalized minority population;4,5 therefore be it 25 26 RESOLVED, That our American Medical Association develop a plan with input from the 27 Advisory Committee on LGBTQ Issues to expand the demographics we collect about our 28 members to include both sexual orientation and gender identity information, which may be given 29 voluntarily by members and will be handled in a confidential manner. (New HOD Policy) 30
1 Gates, GA. LGBT Demographics: Population-based surveys. The Williams Institute. Available from: URL: http://williamsinstitute.law.ucla.edu/wp-content/uploads/lgbt-demogs-sep-2014.pdf. Published September 2014. 2 Mansh M. et al. From Patients to Providers: Changing the Culture in Medicine toward Sexual and Gender Minorities. Academic Medicine. 2015;90(5):574-580. doi:10.1097/acm.0000000000000656. 3 Association of American Medical Colleges (AAMC). Matriculating Student Questionnaire 2015 All Schools Summary Report.; 2015. Available at: https://www.aamc.org/download/450608/data/msq2015report.pdf. Accessed March 1, 2016. 4 Gender Identity in U.S. Surveillance (GenIUSS) Group. Best Practices for Asking Questions to Identify Transgender and Other Gender Minority Respondents on Population-Based Surveys. The Williams Institute. 2014. Available from: URL: http://williamsinstitute.law.ucla.edu/wp-content/uploads/geniuss-report-sep-2014.pdf. 5 Do Ask, Do Tell: A Toolkit for Collecting Data on Sexual Orientation and Gender Identity in Clinical Settings. The Fenway Institute and Center for American Progress. 2016. Available from: URL: http://doaskdotell.org. Accessed February 29, 2016.
Resolution: 603 (A-17) Page 2 of 2
Fiscal Note: Moderate - between $5,000 - $10,000 Received: 05/03/17 RELEVANT AMA POLICY: AMA Membership Demographics G-635.125 - 1. Stratified demographics of our AMA membership will be reported annually and include information regarding age, gender, race/ethnicity, education, life stage, present employment, and self-designated specialty. 2. Our AMA will immediately release to each state medical and specialty society, on request, the names, category and demographics of all AMA members of that state and specialty. BOT Rep. 26, A-10 Reaffirmed: CCB/CLRPD Rep. 3, A-12 The Demographics of the House of Delegates G-600.035 - 1. A report on the demographics of our AMA House of Delegates will be issued annually and include information regarding age, gender, race/ethnicity, education, life stage, present employment, and self-designated specialty. 2. As one means of encouraging greater awareness and responsiveness to diversity, our AMA will prepare and distribute a state-by-state demographic analysis of the House of Delegates, with comparisons to the physician population and to our AMA physician membership every other year. 3. Future reports on the demographic characteristics of the House of Delegates will identify and include information on successful initiatives and best practices to promote diversity, particularly by age, of state and specialty society delegations. 4. Our AMA will convene a group of stakeholders at a forum in conjunction with the 2016 Annual Meeting to identify viable solutions with which to promote diversity, particularly by age, of state and specialty society delegations, with a summary of the findings to be included in the next CLRPD report on the demographic characteristics of the House of Delegates. CCB/CLRPD Rep. 3, A-12 Appended: Res. 616, A-14 Appended: CLRPD Rep. 1, I-15 Strategies for Enhancing Diversity in the Physician Workforce H-200.951 - Our AMA supports increased diversity across all specialties in the physician workforce in the categories of race, ethnicity, gender, sexual orientation/gender identity, socioeconomic origin and persons with disabilities.CME Rep. 1, I-06 Reaffirmed: CME Rep. 7, A-08 Reaffirmed: CCB/CLRPD Rep. 4, A-13 Modified: CME Rep. 01, A-16 Reaffirmation A-16 Revisions to AMA Policy on the Physician Workforce H-200.955 - It is AMA policy that: (1) any workforce planning efforts, done by the AMA or others, should utilize data on all aspects of the health care system, including projected demographics of both providers and patients, the number and roles of other health professionals in providing care, and practice environment changes. Planning should have as a goal appropriate physician numbers, specialty mix, and geographic distribution. (2) Our AMA encourages and collaborates in the collection of the data needed for workforce planning and in the conduct of national and regional research on physician supply and distribution. The AMA will independently and in collaboration with state and specialty societies, national medical organizations, and other public and private sector groups, compile and disseminate the results of the research. (3) The medical profession must be integrally involved in any workforce planning efforts sponsored by federal or state governments, or by the private sector. (4) In order to enhance access to care, our AMA collaborates with the public and private sectors to ensure an adequate supply of physicians in all specialties and to develop strategies to mitigate the current geographic maldistribution of physicians. (5) There is a need to enhance underrepresented minority representation in medical schools and in the physician workforce, as a means to ultimately improve access to care for minority and underserved groups. (6) There should be no decrease in the number of funded graduate medical education (GME) positions. Any increase in the number of funded GME positions, overall or in a given specialty, and in the number of US medical students should be based on a demonstrated regional or national need. (7) Our AMA will collect and disseminate information on market demands and workforce needs, so as to assist medical students and resident physicians in selecting a specialty and choosing a career. CME Rep. 2, I-03 Reaffirmation I-06 Reaffirmation I-07 Reaffirmed: CME Rep. 15, A-10 Reaffirmation: I-12 Reaffirmation A-13 Increasing Demographically Diverse Representation in Liaison Committee on Medical Education Accredited Medical Schools D-295.322 - Our AMA will continue to study medical school implementation of the Liaison Committee on Medical Education (LCME) Standard IS-16 and share the results with appropriate accreditation organizations and all state medical associations for action on demographic diversity. Res. 313, A-09 Modified: CME Rep. 6, A-11
AMERICAN MEDICAL ASSOCIATION HOUSE OF DELEGATES
Resolution: 604 (A-17)
Introduced by: Pennsylvania Subject: High Cost to Authors for Open Source Peer Reviewed Publications Referred to: Reference Committee F (Gary R. Katz, MD, Chair) Whereas, Preparing a scholarly document for peer review publication involves research, 1 analysis and synthesis in terms of time, design and energy; and 2 3 Whereas, Once a document is accepted for publication, open source publishers demand a fee 4 averaging between $3,000 and $5,000 per document; and 5 6 Whereas, This fee for open source publication prevents documents deemed worthy for 7 publication by the journal serves as a barrier to publication, due to lack of money; therefore be it 8 9 RESOLVED, That our American Medical Association investigate the high dollar costs open 10 source publication rules currently present to the dissemination of research, especially by less 11 well-funded and/or smaller entities (Directive to Take Action); and be it further 12 13 RESOLVED, That our AMA make recommendations to correct the imbalance of knowledge 14 suppression based solely on financial considerations. (Directive to Take Action).15 Fiscal Note: Minimal - less than $1,000 Received: 04/26/17
AMERICAN MEDICAL ASSOCIATION HOUSE OF DELEGATES
Resolution: 605 (A-17)
Introduced by: Illinois Subject: Pronunciation of Pharmaceutical Names Referred to: Reference Committee F (Gary R. Katz, MD, Chair) Whereas, Pharmaceuticals have a central role in the practice of medicine; and 1 2 Whereas, The spelling of newly released pharmaceuticals has become more and more 3 complex; and 4 5 Whereas, The pronunciation of such pharmaceuticals has become more and more difficult; and 6 7 Whereas, For example, the pharmaceuticals empagliflozin and ixekizumab appeared on the 8 cover of the July 28, 2016 issue of the New England Journal of Medicine; and 9 10 Whereas, The pharmaceuticals inotuzumab ozogamicin, daratumumab, and bortezomib 11 appeared on the cover of the August 25, 2016 issue of the New England Journal of Medicine; 12 and 13 14 Whereas, Similar examples can be found in other journals including JAMA, Gastrointestinal 15 Endoscopy, and the American Journal of Gastroenterology; and 16 17 Whereas, None of these journals offers a notation on how to pronounce these and similar 18 complex pharmaceutical names; and 19 20 Whereas, It is difficult to communicate with other physicians in regard to a new pharmaceutical if 21 one cannot pronounce the name; and 22 23 Whereas, It is extremely difficult to remember a pharmaceutical if one cannot pronounce it or 24 spell the name; and 25 26 Whereas, Brand names are usually easier to spell and pronounce; and 27 28 Whereas, American Medical Association Policy H-115.970, adopted in 2007, encourages the 29 American Hospital Association and the National Nursing Home Association, as well as 30 complementary state and local associations, to consider the use of both generic and common 31 brand names for medications on containers, communications and other applicable areas in 32 health care settings; and 33 34 Whereas, This policy does not clearly include medical journals, nor has the intent been 35 implemented; therefore be it36
Resolution: 605 (A-17) Page 2 of 2
RESOLVED, That our American Medical Association adopt policy that its AMA-sponsored 1 medical journals develop means to convey the proper pronunciation of all new pharmaceutical 2 names. (New HOD Policy) 3 Fiscal Note: Minimal - less than $1,000 Received: 05/01/17 RELEVANT AMA POLICY Usage of Brand and Generic Name for Prescription Medications H-115.970 Our AMA encourages the American Hospital Association, National Nursing Home Association, as well as complementary state and local associations, to consider the use of both generic and common brand names for medications on containers, communications, and other applicable areas in health care settings. Sub. Res. 509, A-07





























