8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 1/34
Hernias
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 2/34
Hernia
a protrusion of any viscus from its proper
cavity. The protruded parts are generally
contained in a sac-like structure, formed by
the membrane with which the cavity is
naturally lined
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 3/34
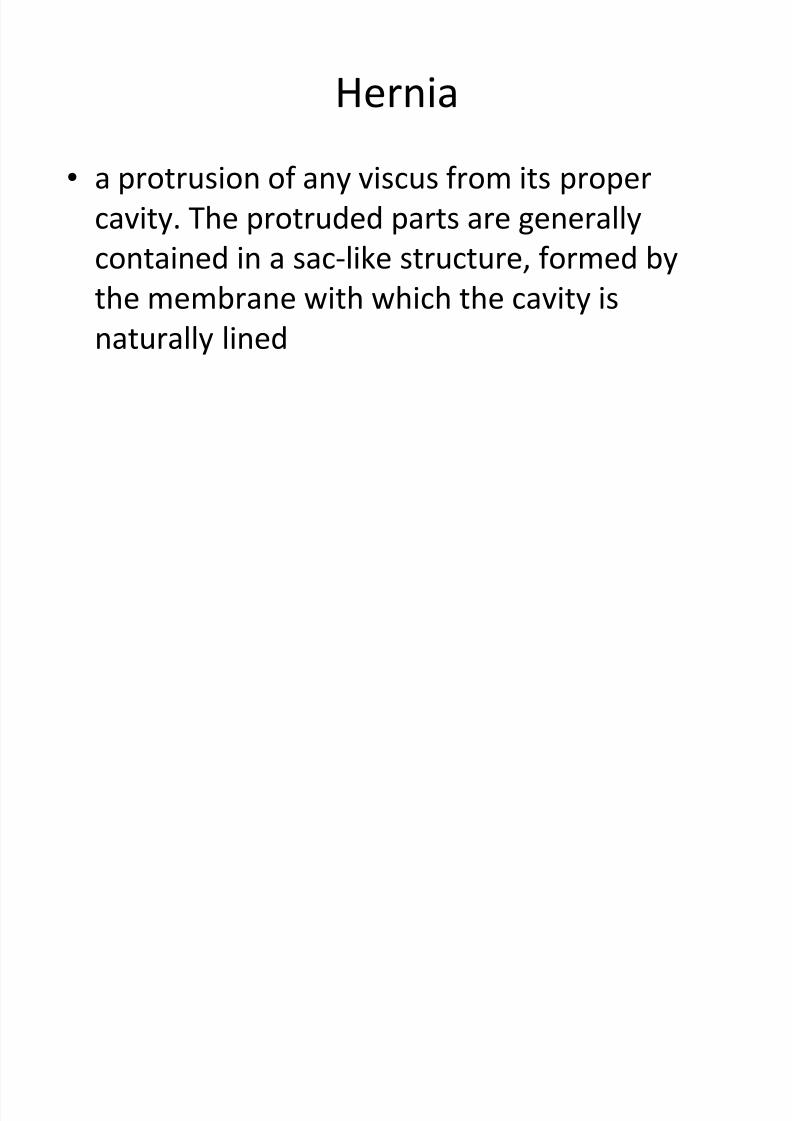
Abdominal Hernias
Indirect Inguinal Hernia
Direct Inguinal Hernia
Umbilical
Femoral
Richter
Incisional
Spigelian
Obturator
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 4/34
Hernia - Conditions
Reducible hernia: This term refers to the ability toreturn the contents of the hernia into the abdominalcavity, either spontaneously or manually.
Incarcerated hernia: An incarcerated hernia is nolonger reducible. The vascular supply of the bowel isnot compromised. Bowel obstruction is common.
Strangulated hernia: A strangulated hernia occurswhen the vascular supply of the bowel is compromisedsecondary to incarceration of hernia contents.
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 5/34
What are the symptoms of inguinal
hernia?
Symptoms of inguinal hernia include:
a small bulge in one or both sides of the grointhat may increase in size and disappear when
lying down; in males, it can present as a swollenor enlarged scrotum
discomfort or sharp painespecially whenstraining, lifting, or exercisingthat improveswhen resting
a feeling of weakness or pressure in the groin
a burning, gurgling, or aching feeling at the bulge
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 6/34
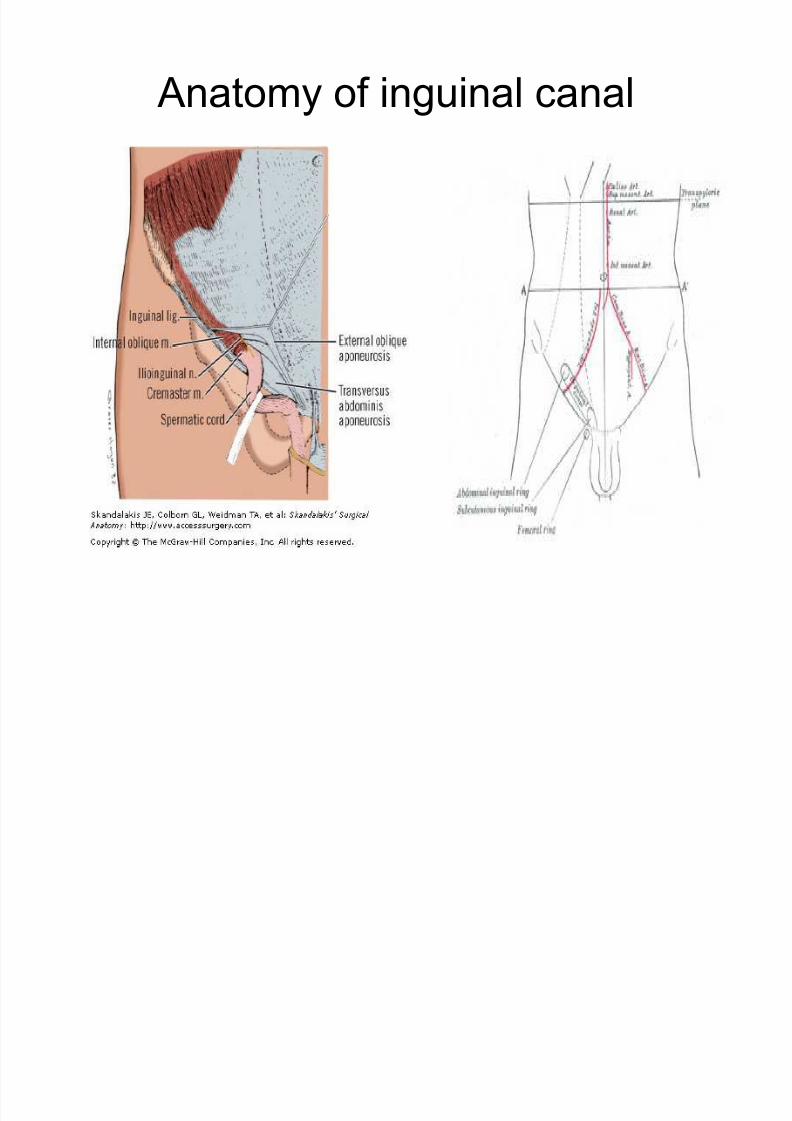
Anatomy of inguinal canal
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 7/34
Boundaries of inguinal canal
Ant : External oblique aponeurosisand few fibers of internal oblique
laterally Post : Fascia transversalis andconjoined tendon
Superior : Arched fibres of conjoinedtendon
Inferior : Inguinal ligament
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 8/34
Contents of inguinal canal
Spermatic cord, ilioinguinal nerve, genital
br. of genitofemoral nerve.
Round ligament in females. Vestigial remnant of processes vaginalis.
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 9/34
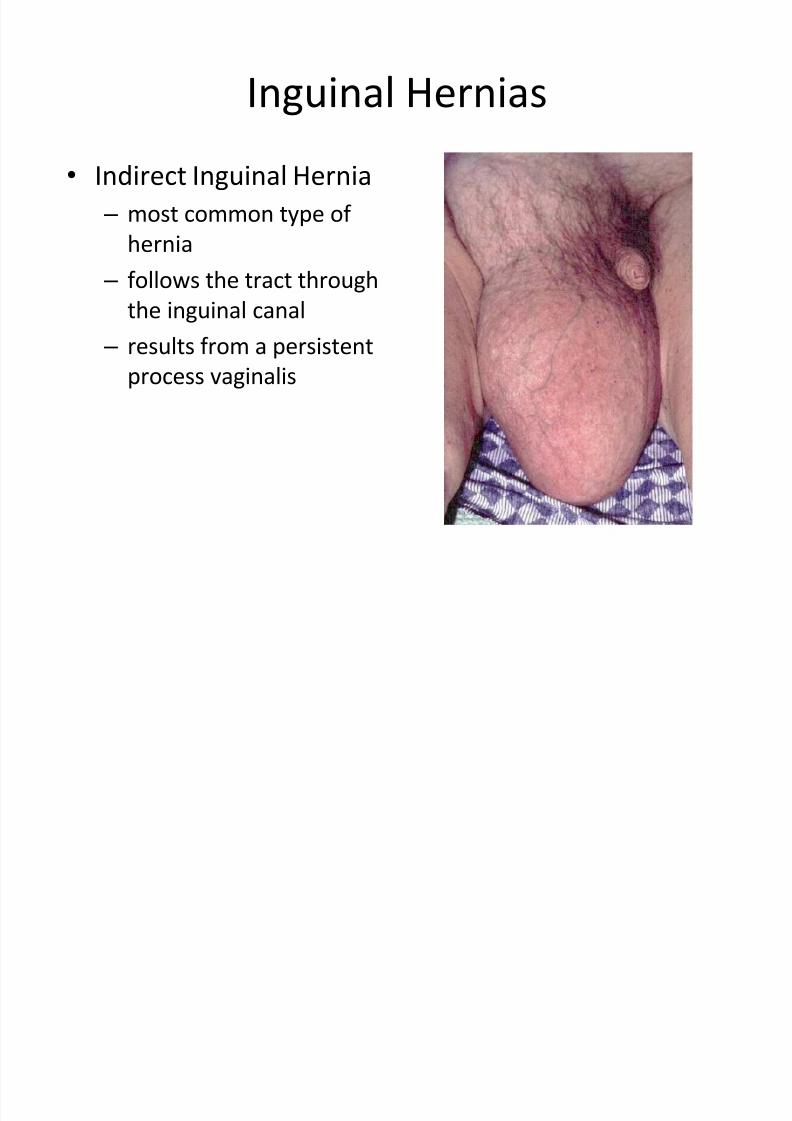
Inguinal Hernias
Indirect Inguinal Hernia
± most common type of
hernia
± follows the tract throughthe inguinal canal
± results from a persistent
process vaginalis
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 10/34
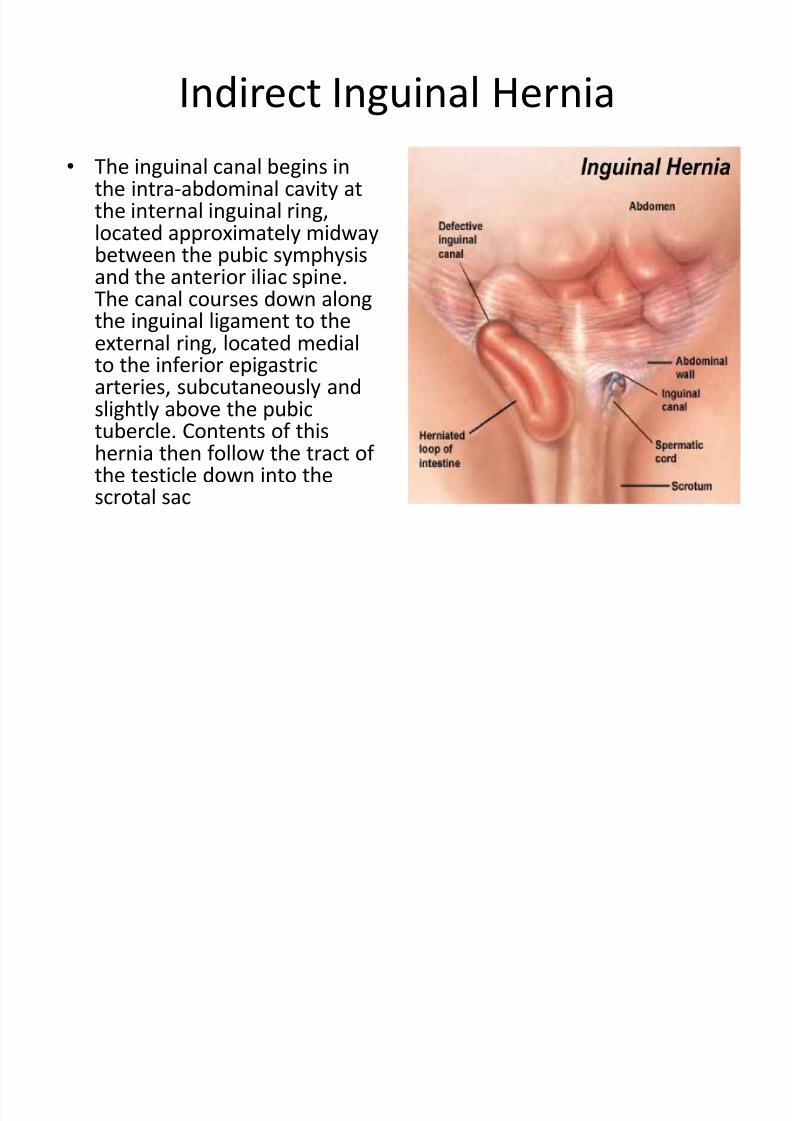
Indirect Inguinal Hernia
The inguinal canal begins inthe intra-abdominal cavity atthe internal inguinal ring,located approximately midwaybetween the pubic symphysis
and the anterior iliac spine.The canal courses down alongthe inguinal ligament to theexternal ring, located medialto the inferior epigastricarteries, subcutaneously and
slightly above the pubictubercle. Contents of thishernia then follow the tract of the testicle down into thescrotal sac
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 11/34
Inguinal Hernias
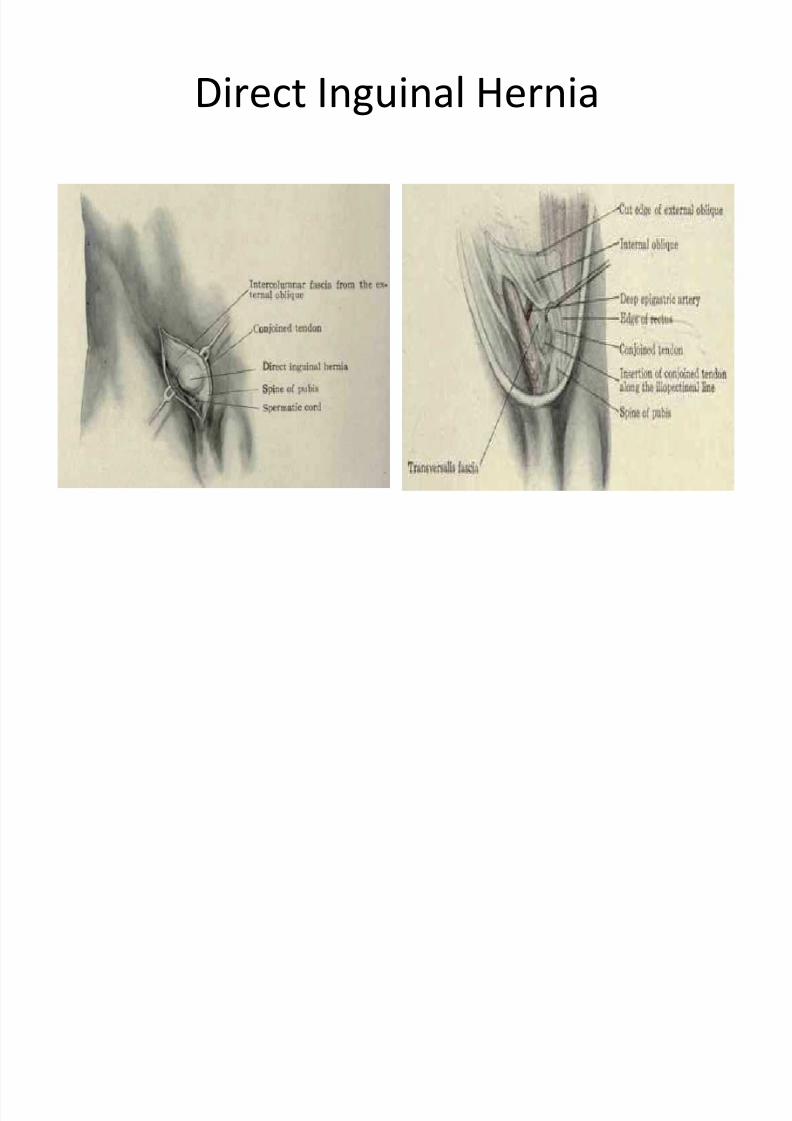
Direct Inguinal Hernia ± caused by connective tissue degeneration of the abdominal
muscles, which causes weakening of the muscles during theadult years.
± occurs due to a defect or weakness in the transversalis fasciaarea of the Hesselbach triangle The triangle is defined inferiorly by the inguinal ligament, laterally by
the inferior epigastric arteries, and medially by the conjoined tendon
± One or more of the following factors can cause pressure on theabdominal muscles and may worsen the hernia:
sudden twists, pulls, or muscle strains lifting heavy objects
straining on the toilet because of constipation
weight gain
chronic coughing
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 12/34
Direct Inguinal Hernia
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 13/34
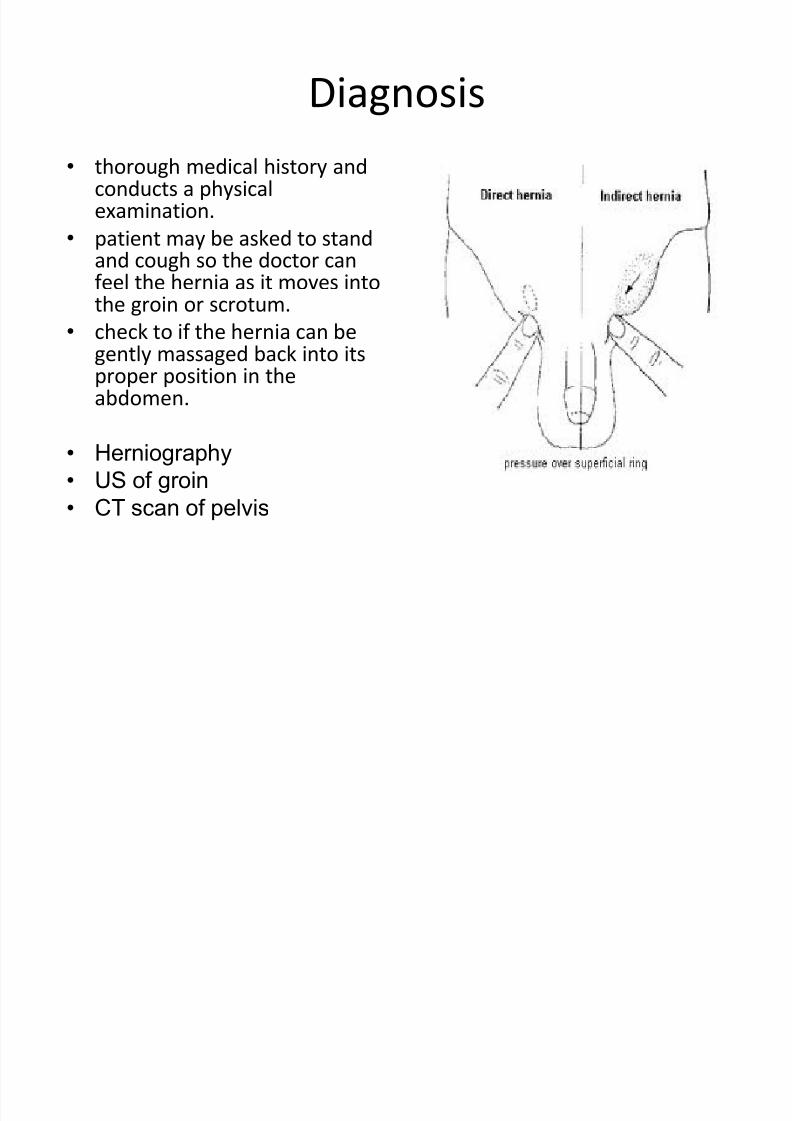
Diagnosis
thorough medical history andconducts a physicalexamination.
patient may be asked to standand cough so the doctor can
feel the hernia as it moves intothe groin or scrotum.
check to if the hernia can begently massaged back into itsproper position in theabdomen.
Herniography
US of groin
CT scan of pelvis
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 14/34
Examination
Inguino scrotal swelling
Expansile cough
Reducibility Finger Invagination Test
Deep Ring occlusion Test
(Three finger Test)
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 15/34
Treatment
Surgical
Watchful waiting for elderly pt. with smallasymptomatic hernia
Truss
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 16/34
Surgery
Herniorrhaphy:
± Bassini¶s Repair
± Shouldice Repair
± Mc Vay Hernioplasty : Mesh graft application
Laparoscopic Repair
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 17/34
Types of repair
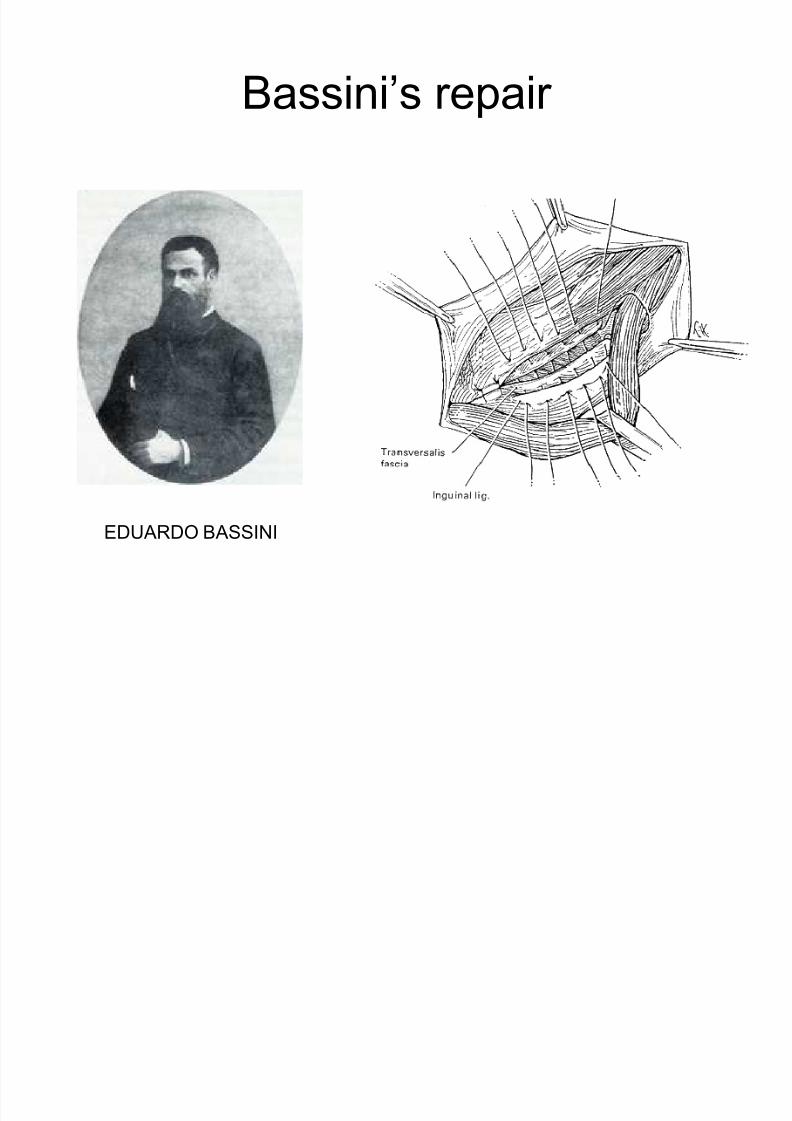
Bassini (early 20th Century) ± The conjoined tendon of the transversus abdominis and
the internal oblique muscles is sutured to the inguinal
ligament
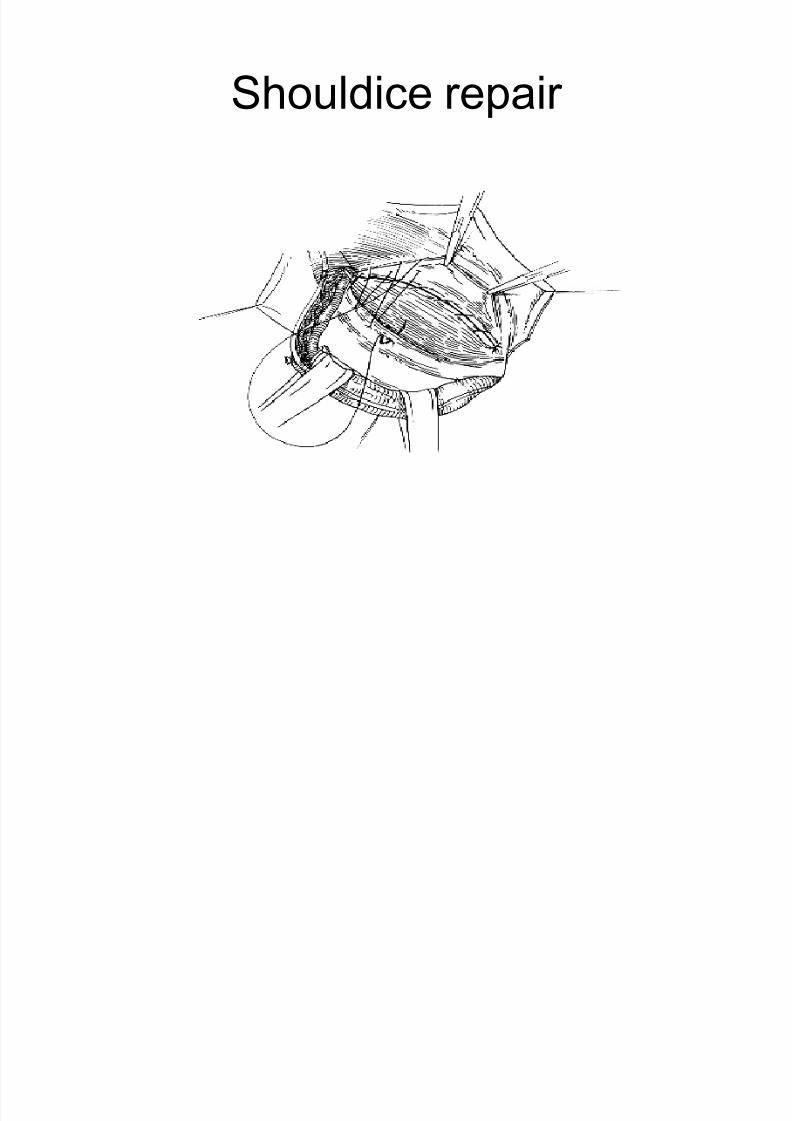
Shouldice (1930s) ± Multilayer imbricated repair of the posterior wall of the
inguinal canal
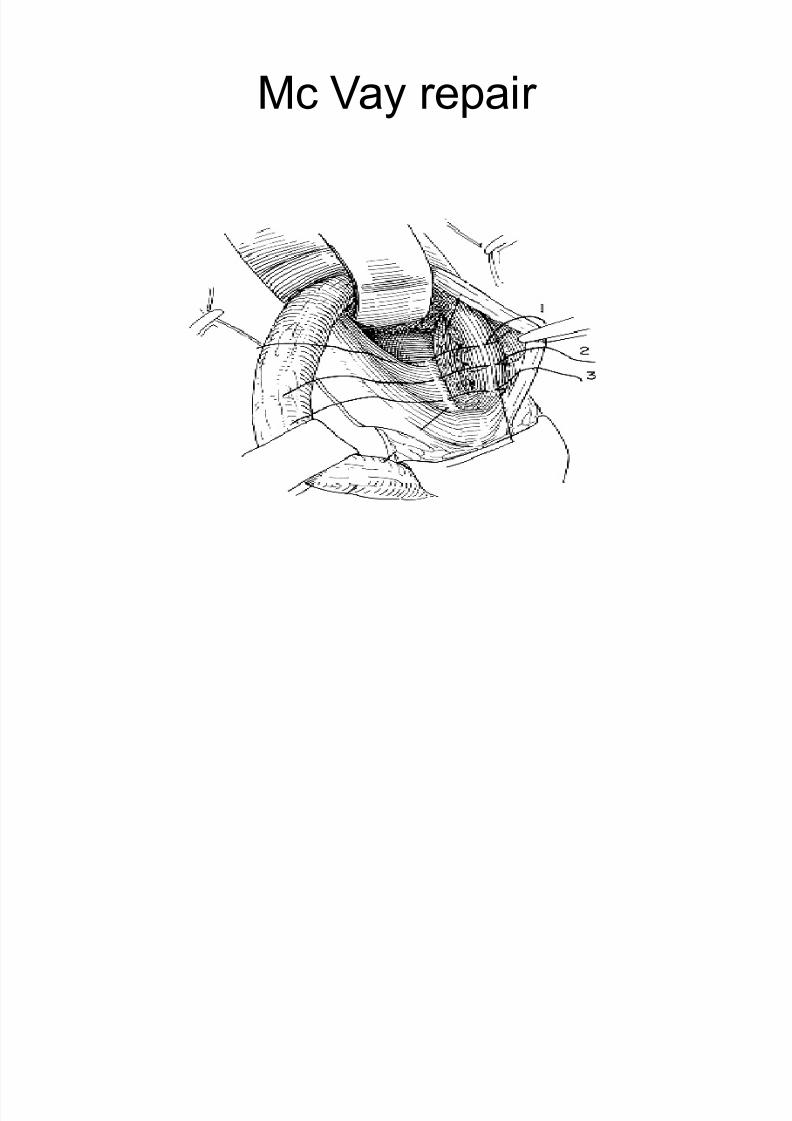
McVay (1948)
± Edge of the transversus abdominis aponeurosis to
Cooper s ligament; incorporate Cooper s ligament andthe iliopubic tract (transition suture)
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 18/34
Bassini¶s repair
EDUARDO B ASSINI
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 19/34
Shouldice repair
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 20/34
Mc Vay repair
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 21/34
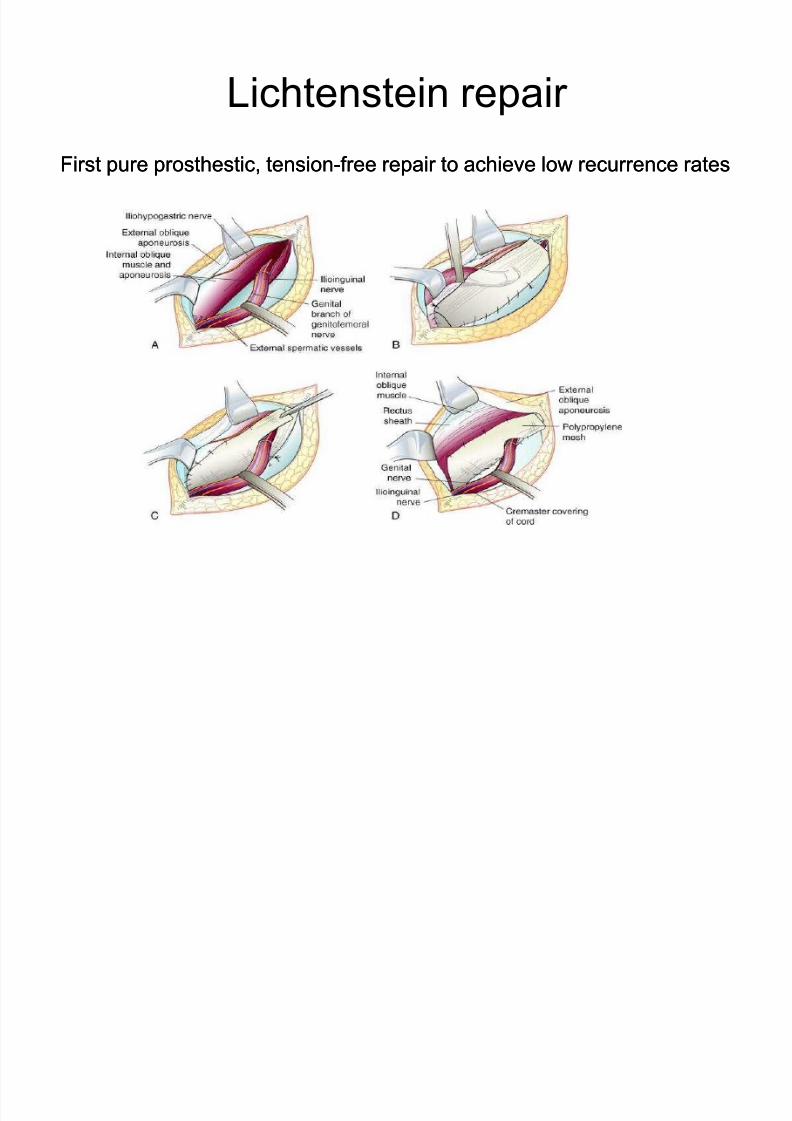
Lichtenstein repair
First pure prosthestic, tensionFirst pure prosthestic, tension--free repair to achieve low recurrence ratesfree repair to achieve low recurrence rates
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 22/34
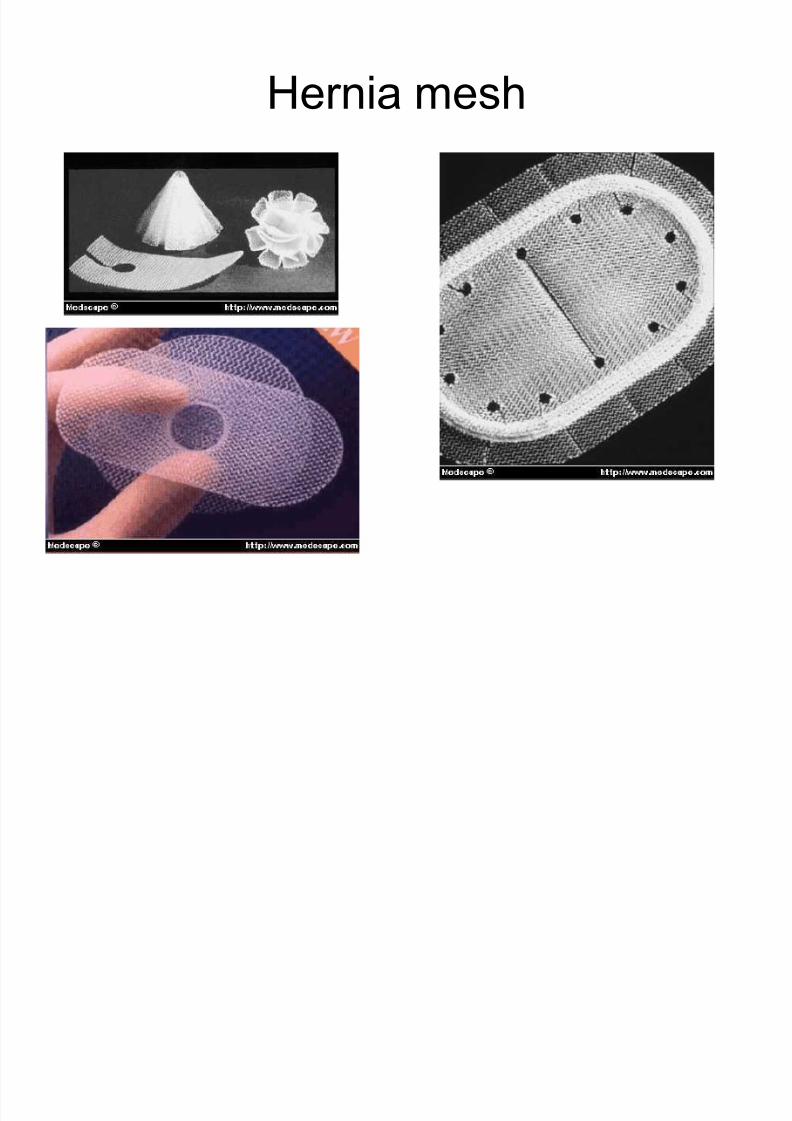
Types of Prosthesis
Polypropylene mesh most common andpreferred
± allows for a fibrotic reaction to occur betweenthe inguinal floor and the posterior surface of
the mesh, thereby forming scar andstrengthening the closure of the hernia defect
Polytetrafluoroethylene (PTFE) mesh
± often used for repair of ventral or incision
hernias in which the fibrotic reaction with theunderlying serosal surface of the bowel isbest avoided
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 23/34
Hernia mesh
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 24/34
Complications
Hernia recurrence
Bleeding
Wound infection Painful scar
Injury to internal organs
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 25/34
Conservative treatment
Trusses can provide symptomatic relief
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 26/34
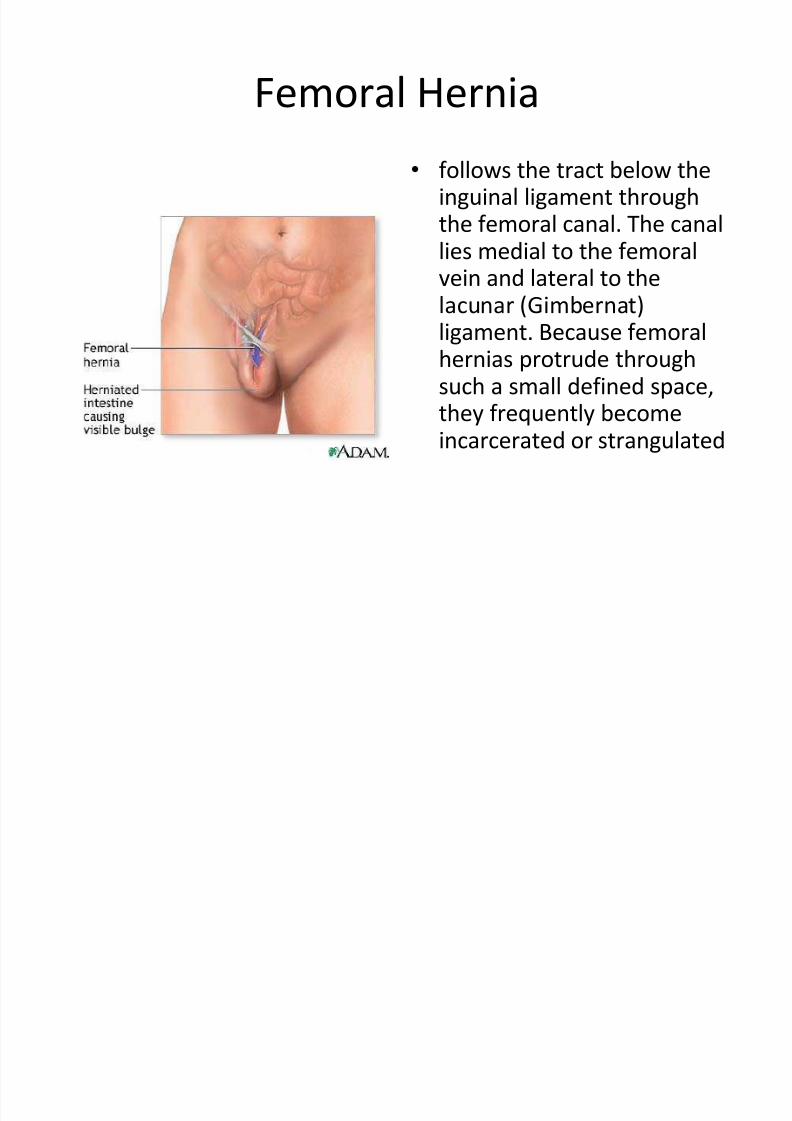
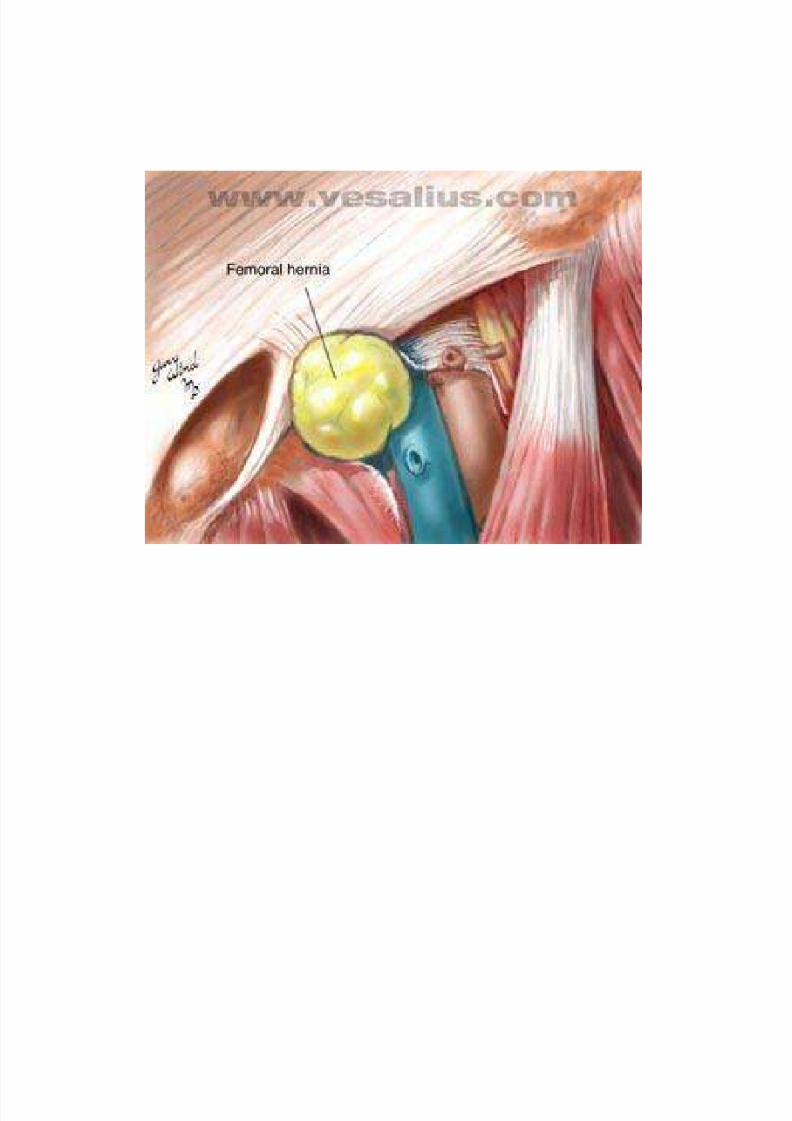
Femoral Hernia
follows the tract below theinguinal ligament throughthe femoral canal. The canallies medial to the femoral
vein and lateral to thelacunar (Gimbernat)ligament. Because femoralhernias protrude throughsuch a small defined space,
they frequently becomeincarcerated or strangulated
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 27/34
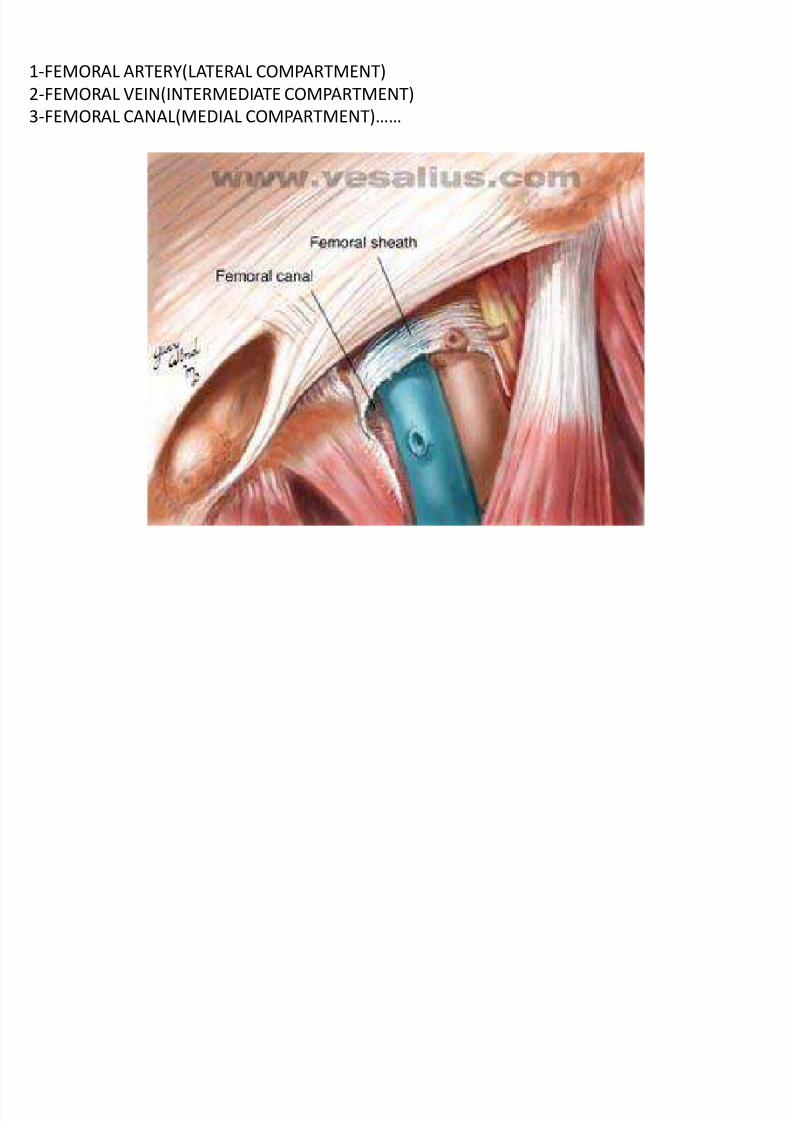
1-FEMORAL ARTERY(LATERAL COMPARTMENT)
2-FEMORAL VEIN(INTERMEDIATE COMPARTMENT)
3-FEMORAL CANAL(MEDIAL COMPARTMENT)
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 28/34

8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 29/34
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 30/34
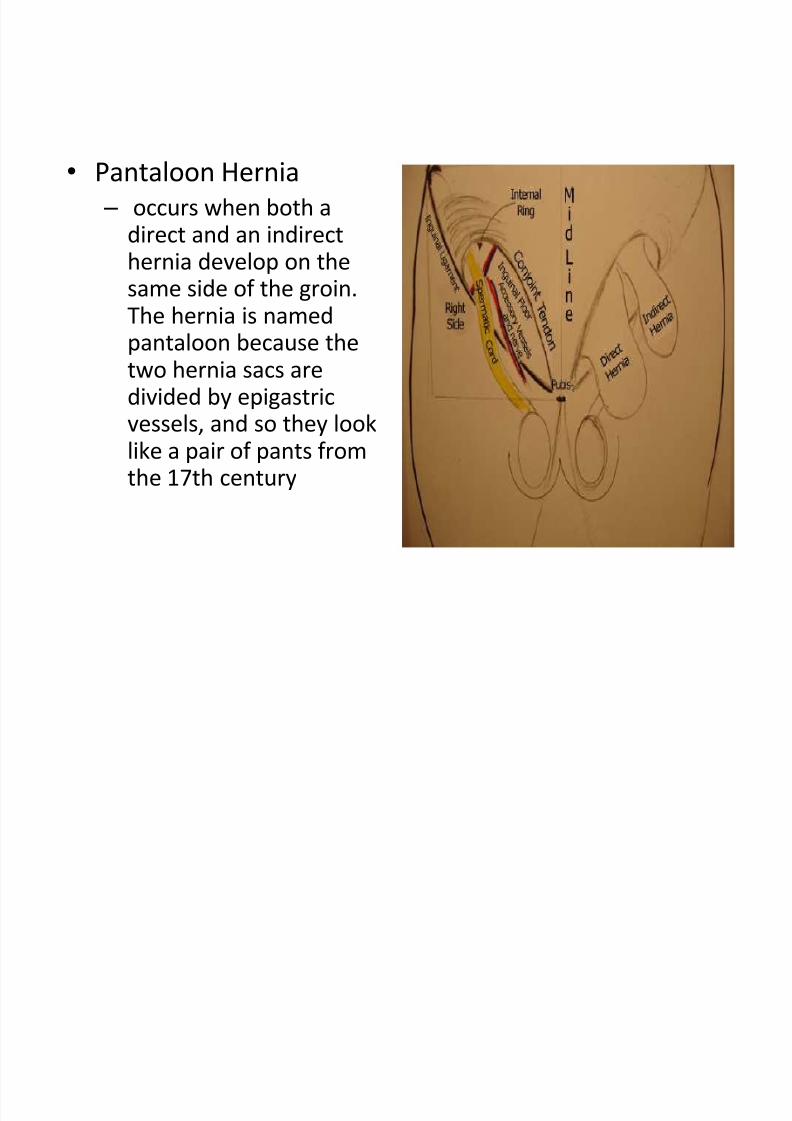
Pantaloon Hernia
± occurs when both adirect and an indirecthernia develop on the
same side of the groin.The hernia is namedpantaloon because thetwo hernia sacs aredivided by epigastric
vessels, and so they looklike a pair of pants fromthe 17th century
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 31/34
Littres Hernia - a hernia involving a Meckel's diverticulum
Sliding Hernia - a variant that is seen in 3% of hernia cases. It occurswhen the wall of the hernia sac is an organ like the bladder or thecolon
Spigelian hernia
± protrusion of preperitoneal fat, a sac of peritoneum, or an organ,through a congenital defect or weakness in the spigelian fascia
± This is typically a soft reducible mass encountered lateral to the rectus
muscle and below the umbilicus ± It advances through different muscle layers of the abdominal wall andspreadsout like a mushroom between external and internal obliquemuscles
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 32/34
Richters hernia
± occurs when only the antimesenteric border of
the bowel herniates through the fascial defect.
± involves only a portion of the circumference of the
bowel
± the bowel may not be obstructed, even if the
hernia is incarcerated or strangulated, and thepatient may not present with vomiting.
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 33/34
Incisional hernia
± This iatrogenic hernia occurs in 2-10% of all abdominaloperations secondary to breakdown of the fascial closure of prior surgery
± patients present with a bulge at the site of a previous incision
Obturator hernia ± passes through the obturator foramen, following the path of the
obturator nerves and muscles
± Obturator hernias occur with a female-to-male ratio of 6:1,because of a gender-specific larger canal diameter
± Because of its anatomic position, this hernia presents morecommonly as a bowel obstruction than as a protrusion of bowelcontents
8/8/2019 Hernias Presentation
http://slidepdf.com/reader/full/hernias-presentation 34/34
Fin
Recommended