DOI: 10.1161/CIRCEP.113.000636
1
Fragmented QRS Complex in Adult Patients with Ebstein’s Anomaly and Its Association with Arrhythmic Risk and the Severity of the Anomaly
Running title: Park et al.; Fragmented QRS in Ebstein’s Anomaly
Seung-Jung Park, MD, PhD1; Seungmin Chung, MD1; Young Geun On, MD, PhD1;
June Soo Kim, MD, PhD1; Ji-Hyuk Yang, MD, PhD2; Tae-Gook Jun, MD, PhD2;
Shin Yi Jang, RN, PhD1; Ok Jung Lee, MD3; Jinyoung Song, MD, PhD3;
I-Seok Kang, MD3; June Huh, MD, PhD3
Department of 1Medicine, 2Thoracic and Cardiovascular Surgery, and 3Pediatrics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
Correspondence:
June Huh, MD, PhD
Associate Professor
Grown-Up Congenital Heart Disease Clinic,
Department of Pediatrics, Cardiac and Vascular Center,
Samsung Medical Center, Sungkyunkwan University School of Medicine,
50 Irwon-dong, Gangnam-gu
Seoul 135-710
Korea
Tel: +82-2-3410-3526
Fax: +82-2-3410-0043
E-mail: [email protected]
Journal Subject Code: [171] Electrocardiology
ononnng,g,g,g, MMMMD,D,,, PPPPhDhDhh 3;;;
m uM
n
memememennntn of 1Mediccinne, 2Thorororraca ic anddd Carrdddiovvascuuulalaalar rrr SuSSuS rgggeeery, anand 333PPPeP diaaata rrir ccs,, SaaammmsuMeeedididid cacacal CeCeCeCentnnn errr, Suuuungngngngkyununununkwkwkwanaaa UUUUnininivvvev rsrsrsitttyy Scccchohohoolololl ooof ff MeMeMeM dididiciiine, SeSeSeS ouououull,l KKKooro eaaaa
ndence: by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.113.000636
2
Abstract:
Background - Fragmented QRS complex (fQRS) on 12-lead ECG, a marker of myocardial scar,
is a predictor of arrhythmic events in patients with ischemic and non-ischemic cardiomyopathy.
We investigated whether the presence of fQRS is associated with the severity of the anomaly and
with increased arrhythmic events in adult patients with Ebstein’s anomaly (EA).
Methods and Results - In 51 consecutive adult EA patients (median age, 37 years; 18 males), the
severity index of EA calculated from echocardiographic data and clinical arrhythmic events were
analyzed. The extent of fQRS in each patient was measured by counting the number of ECG
leads showing fQRS. There were 35 (68.6%) patients with fQRS (fQRS group) and 16 (31.4%)
patients without fQRS (non-fQRS group). fQRS was observed more frequently in the inferior
(n=26) and precordial (n=25) leads versus the lateral leads (n=5). The patients in the fQRS group
had a worse functional class, greater cardiothoracic ratios, more severe tricuspid regurgitation,
larger atrialized right ventricular (aRV) areas, higher EA severity scores, and more frequent
arrhythmic events compared to those in the non-fQRS group. The aRV area showed a positive
correlation with the fQRS extent (r=0.51, P<0.001). In multivariable Cox regression models, the
presence of fQRS was independently associated with arrhythmic events (P=0.036).
Conclusions - Fragmented QRS on 12-lead ECG was associated with larger aRV area and an
increased risk of arrhythmic events in adult patients with EA.
Key words: ECG, Ebstein's anomaly, adult congenital heart disease, arrhythmia, fragmented QRS complex
g p) ((
rererereququququenenenentltltltly y y y inininin tttthehehehe ininnnfefefeferririri
patienennntstststs iiiin n nn ththththe e ee fQfQfQfQRSRSRR
i
a n
c t
l
f
n g Q g a
e fufufuncncncnctititit onononnalalala clclclaasaa s, greater cardiothoraciccc rarar tios, more sevee errrreee e tricuspid regurgitati
liiiizeeeed right veeenntn rricucucuulaaaarr r (((aaaaRVRVRVR )))) aaraa eaeeas, hhhhigggher EAEAAA sssevvvveere ititityy scorororees, ananana dd dd momomoorerere fffrererereququququeneee
eeeveveventnn s compmmm arared ttoo thosososeee in ttttheheee nnnonnn-fffQRRSS ggrgrgrooouppp.p Thhheee aRVV arrreaeaeaea showowowo edd a posososit
withhhh the ffQRQRQRQ S exexextett nt ((rrrr=0==0= .51,, P<0.0.0.0001111).).).) IIIIn multltltivariable eee Cox reeeregrgg esesssion model
f fQfQfQQRSRSRS was iiindndndndepppendddentlylyly associiai tteddd d wiii hhth arrhyhyhythhthh imiic eveee entststss (((PPPP((( =000 0.0003636366).).).)
nnss - FrFragagmemmenttnteddedd QQQQRSRSRSRS oon n 1212121 -lelelel adaddd EEEECGCGCGCG wwasas asassosociciciiatatttededdd wwitititith h hh lallal rgrgerer aaRVRVRVRV arareaea aandnd aa by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.113.000636
3
Ebstein’s anomaly (EA) is a congenital malformation of the tricuspid valve (TV) and the right
ventricle (RV). The most prominent morphological feature of EA is the varying degree of apical
displacement of the TV into the RV, dividing the RV into a proximal chamber of “atrialized RV
(aRV)” and distal portion of “functional RV”. This abnormality often causes tricuspid
regurgitation (TR), progressive dilatation and dysfunction of the right atrium (RA) and RV.1
Therefore, the most common clinical presentations in adolescents and adults with this
malformation are arrhythmic events and right-sided heart failure.2-5 Moreover, these
complications are expected to become more frequent with the improvement in long-term survival
of patients5,6 However, there have been very few studies investigating the risk factors for
arrhythmic complications, especially in adults with EA.
Fragmented QRS complexes (fQRS) on 12-lead ECG, which represent conduction delay
caused by myocardial scar, have been identified as a predictor of arrhythmic events in patients
with ischemic or non-ischemic heart disease7,8 Recently, the fQRS found in adults with repaired
tetralogy of Fallot (TOF) was reported to represent more extensive RV scarring and dilatation.9
In this study, we evaluated whether the presence of fQRS reflects a greater risk of
arrhythmic events and more severe abnormalities of the right-sided chambers in adult patients
with EA.
Methods
Patient Population
Fifty-one adult patients (>18 years old) diagnosed consecutively with EA at the Samsung
Medical Center from November 1994 to April 2011 were enrolled for the present study. EA was
diagnosed by echocardiography when the apical displacement of the septal leaflet of the TV
ement in long-g termmmm ssssu
the ririiiskskkk ffffacactotott rsrs fffforororor
c
agmented S complexes on 12-lead ECG, which represent conduction
myocardial scar, have been identified as a predictor of arrhythmic events in patie
m
f Fallot (TOF) as reported to represent more e tensi e RV scarring and dilatati
comomomomplplplpliciciccatatata ioiii nsnsnss,, especially in adults with hhh EAEEA.
aagmgmgmgmented QRSS compmm lexexexes (ffffQRQRQRQ SS) onn 12--leead ddd ECECECCGG, wwwhhhich repeprerresenttt cconono dducttttiooon
myoccccaraardidididial scar, hhhhave beenenenn iiiiddddentififififieieieiedd d as a ppredidididicctc orororor of fff arararar hhrhh ttythhhmh icicicc eeeevventttts iiin p ttatieii
mic or non-iisi chchchhemicii hhheart ddddiisi ease7,77 888 ReRR centlylyly, thhthhe fQfQfQRSRSRSRS fffoundndndnd iiiin daddd lullts wwwwitititith hhh reppp
ff FF lalllott (T(TOFOF)) trt ded tt tt tt isi RRVV iri dd didillattatiti
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCEP.113.000636
4
relative to the insertion of the anterior leaflet of the mitral valve was measured at least 20 mm or
8 mm/m2 body surface area (BSA). Patients with failed ablation of accessory pathways (AP),
paced ventricular rhythms, and a previous cardiac surgery were excluded because these
conditions could affect the QRS morphology. Demographic, electrocardiographic, and
echocardiographic data were analyzed retrospectively. The study protocol was approved by our
institutional review board, and the requirement for written informed consent was waived.
Definition of fQRS and Measurement of ECG Parameters
Standard 12-lead ECGs were obtained with an optimal low-pass filter setting (filter range 0.15 to
100 Hz, alternating current filter 60 Hz, 25 mm/s, 10mm/mV; GE Marquette, Milwaukee, WI,
USA). To assess the correlation between fQRS and the severity of the structural abnormality in
EA, we analyzed the index electrocardiogram recorded closest in time to the echocardiographic
examination performed during the first visit to our institute. The time interval between
electrocardiographic and echocardiographic study ranged from 0 to 105 days (median 1 day).
QRS complexes were defined t ') or notch on the
R/S waves were present in narrow QRS complexes (<120ms), or when >2 notches on the R/S
waves were noted in wide QRS complexes ( .7-9 This fragmentation should be observed
in at least two contiguous leads representing anterior (V1–V5), inferior (II, III, aVF), or lateral (I,
aVL, V6) myocardial segments (Figure 1). The extent of the fQRS in each patient was estimated
by counting the number of ECG leads showing fQRS.9 In the presence of delta-waves in the
QRS complex, electrocardiograms obtained after accessory pathway (AP) ablation were used
because pre-excitation of the ventricle through the AP could alter the QRS morphology,
mimicking fQRS. All ECG tracings were analyzed by two independent cardiologists who were
blinded to clinical outcome data. There was a 97% and 95% intra- and interobserver agreement
setting g (f( ilter rangngggeeee 00
rquetttttetett , MiMiMiMilwlwll auaukekekekeeee,e, WW
a t
a a
o
d y
ple es ere defined t ') or notch on
assssesesesesss ss thththt ee ee coccorrrrelelelation between fQRS and ddd ththththe severity of f the eee sssts ructural abnormalit
alllyl zzzez d the indeexx ellecctrocococaaardiiiiogo rramm reecccorddeed clclclc osososo eseese t innn timee tto thththt e eccchohohoh carrdiooogggra
on peerfrrfrforrorormmmmed ddd dudd riiingng ttthehh fififfirsrsrsr tttt visiit tt totototo ooour iiinstititit tuuutetetete. ThThThThe tititiimememem iii tttntervavavaal lll bebbb tween
diogggraphphphic andndnd echhhoh ca ddrdioii grgg appphihihih c st duddy yy ranggg dded ffffrom 000 0 totototo 1110505055 daddd ysyy (m(m(m( eddddiaaaan nnn 1111 dayyy
lle dd fefiin ded tt ')') ttchh
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCEP.113.000636
5
for the presence of fQRS, respectively. Electrocardiographic parameters such as
PR/QRS/corrected QT/corrected JT intervals and QRS/QT/JT dispersion were also measured
manually.
Echocardiographic Parameters and Severity Grading of Ebstein’s Anomaly
Comprehensive transthoracic echocardiography was performed using 2.5 to 4 MHz transducers
(Vivid 7, GE Medical System, Milwaukee, WI or Acuson 512, Siemens Medical Solution,
Mountain View, CA, USA). Maximal apical displacement of the TV was measured from the
hinge point of TV septal leaflet to the insertion point of the MV anterior leaflet. The severity
index of EA was estimated using the Great Ormond Street Score (GOSE), an echocardiographic
method described previously.10 The GOSE was calculated as the ratio of the combined area of
the RA and aRV divided by the combined area of the RV proper, left atrium (LA), and left
ventricle (LV) in a four-chamber view at the end of diastole (Figure 2). Four grades of increasing
severity were defined: grade 1, ratio<0.5; grade 2, ratio 0.5 to 0.99; grade 3, 1 to 1.49; and grade
-quantitative measurement depending on
vena contracta width, proximal isovelocity surface area, hepatic vein flow reversal, RV or RA
enlargement, and the plethora of the inferior vena cava.11 The LV ejection fraction was
calculated using Simpson's biplane method.
Clinical Outcomes
Clinical arrhythmias were defined as spontaneous episodes associated with palpitation, dizziness,
or syncope with ECG documentation. Occurrence of clinical arrhythmias has been investigated
since the index electrocardiograms were taken. The index electrocardiograms were obtained
during the first visit as mentioned above. Regular clinical and electrocardiographic follow-up (3
to 6 month interval) was performed in all patients. If a patient reported symptoms suggesting
or leaflet. The seveveveveririrr t
SE), aan n ecechohhoh cacardrdioioioiogggrgra
s 10 a
d
L r
ere defined: grade 1, ratio<0.5; grade 2, ratio 0.5 to 0.99; grade 3, 1 to 1.49; and
q antitati e meas rement depending
scrrrribibbibedededed ppprererer vivv ouououuslss y.10 The GOSE was callllccuc llated as the rrratiooo ooof the combined area
d aRRRVR dividedd bby ttthee cooombmmm innneeed arrea offf thhe RV VVV prprprpropoopo errr, left attriuuuumm (LLLLAA)AA , annd leleleft
LV) iiiinnnn aaa ffofof ur- hhhchambbber viiieweweww at thhhhe ee enenendddd fofff dddiiiai sttttolololole (F(F(F(Fiigurururre 2)2)2). FoFFF urururr ggggrades ffof iiiincr
ere deddd fififined:dd gggrarararadeddd 111, ratiiio<00.0 5; gggraddded 2, ratiiio 000.555 5 tto 000 99.99;9;9;9 gggraaadededede 333, 1111 to 1111 4.4449;9;9;9 aaaand
tntitit tatii tt dde dndiin
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.113.000636
6
arrhythmia at any time, ECG and 24-hour Holter monitoring were repeated. Ventricular
tachyarrhythmia included ventricular fibrillation (VF), ventricular tachycardia (VT), appropriate
implantable cardioverter-defibrillator (ICD) shock, and nonsustained VT ( 3 consecutive
ventricular beats at a rate of 100 beats/min with a duration of <30 seconds). Atrial
tachyarrhythmia included atrial tachycardia (AT), atrial fibrillation (AF), atrial flutter (AFL), and
atrioventricular reentrant tachycardia (AVRT) using AP. For the present study, tachycardia
episodes caused by AVRT using AP were not included when analyzing the relationship between
fQRS and arrhythmic events. Since fQRS is a marker of myocardial fibrosis, we focused on
specific relationships between fQRS and arrhythmias more directly related to myocardial
dysplasia/degeneration. Therefore, the AVRT with a bypass tract was analyzed separately. Open
heart surgery and cardiac death were also investigated.
Statistical Analysis
Continuous variables were expressed as medians (25th and 75th percentiles) and were compared
using the Mann-Whitney test. The results for categorical variables were described as percentages
and the Fisher’s exact test was performed to compare these results. Correlations between QRS
duration or fragmentation and the severity of disease were assessed by the Spearman rank
correlation coefficient. Crude survival in each group was assessed using the Kaplan–Meier
method and the log-rank test was applied. Hazard ratios (HR) with 95% confidence intervals (CI)
were computed using Cox regression models after the proportional hazards assumption was
tested based on correlations between survival rankings and Schoenfeld residuals. The overall C-
index was calculated using Cox survival methods to evaluate the discriminatory accuracy of
several electrocardiographic variables (see supplemental Table) for the occurrence of arrhythmic
events (12). All analyses were performed using SAS software version 9.2 (SAS Institute, Cary,
brosis, we focuseed d d d onooo
lated ddd totott mymyococarardidiiialalalal
d
e
s m
Mann Whitne test The res lts for categorical ariables ere described as percen
degegegegenenenenerarrattttioioioionn. ThThThTherefore, the AVRT withhhh aaa bbypass tract was sss aanaa alyzed separately.
errrry and cardiacc ddeaaathhh weeerrre alslslsoo iinvvesttigggateded.
Analalalalysysysisisisis
s variablbb es werererre exprpp essedddd as medididians (2(2(2555thh h anddd d 7575757 thhhh pppeeere centntntt lillles))) and dd weeeerererere ccccom
MMa WhWhitit tte tst ThTh ltlt ffo tte iri ll iri bablle dd ibib ded
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCEP.113.000636
7
North Carolina, USA). All p values were two-sided and results with a p value less than 0.05 were
considered statistically significant.
Results
Patient Demographics
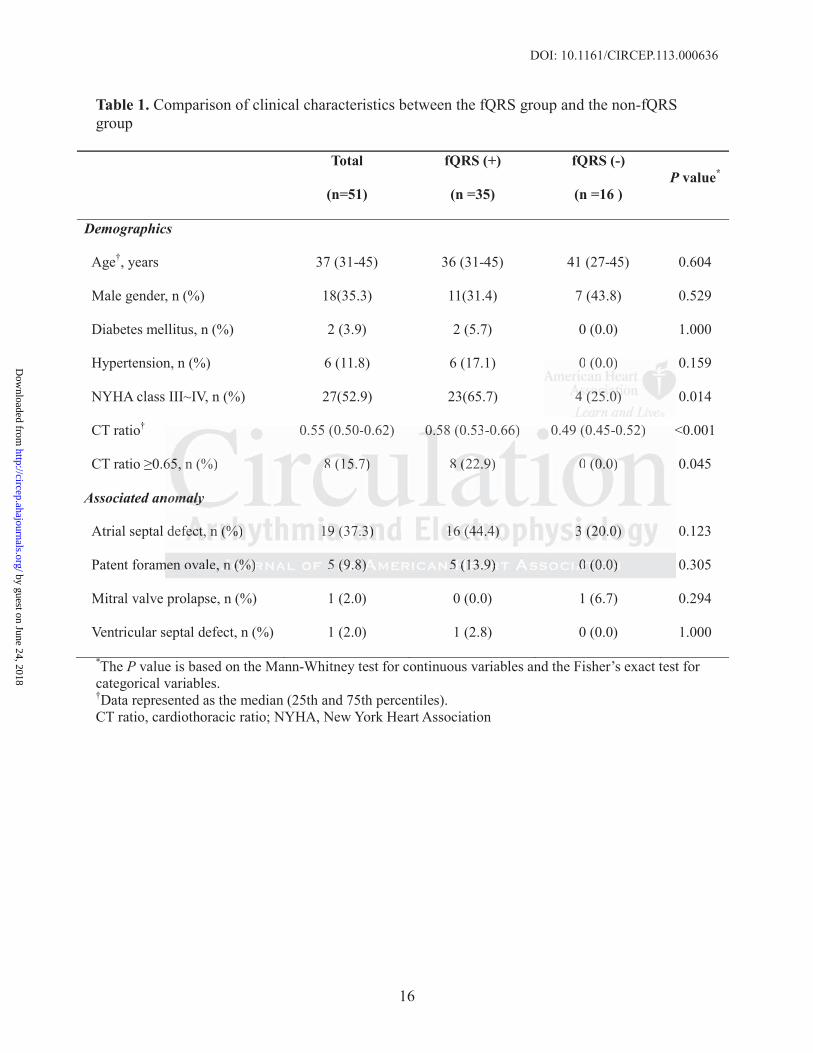
Baseline characteristics of the 51 patients are summarized in Table 1. Median (25th and 75th
percentiles) age was 37 (31-45) years, and the median (25th and 75th percentiles) cardiothoracic
(CT) ratio was 0.55 (0.50-0.62). About half of the patients (27/51, 52.9%) were in New York
Heart Association functional class III-IV. Atrial septal defects were the most common associated
cardiac defect (n=19, 37.3%). In most of the patients (48/51, 94.1%), the right-sided chamber
was much larger than the left, with a combined RA and RV area of 53 (43-75) cm2 compared to a
combined LA and LV area of 37 (32-44) cm2 (P<0.001). The median (25th and 75th percentiles)
value of the EA severity index was 0.79 (0.63-0.94).
Comparison Between the fQRS and Non-fQRS Groups
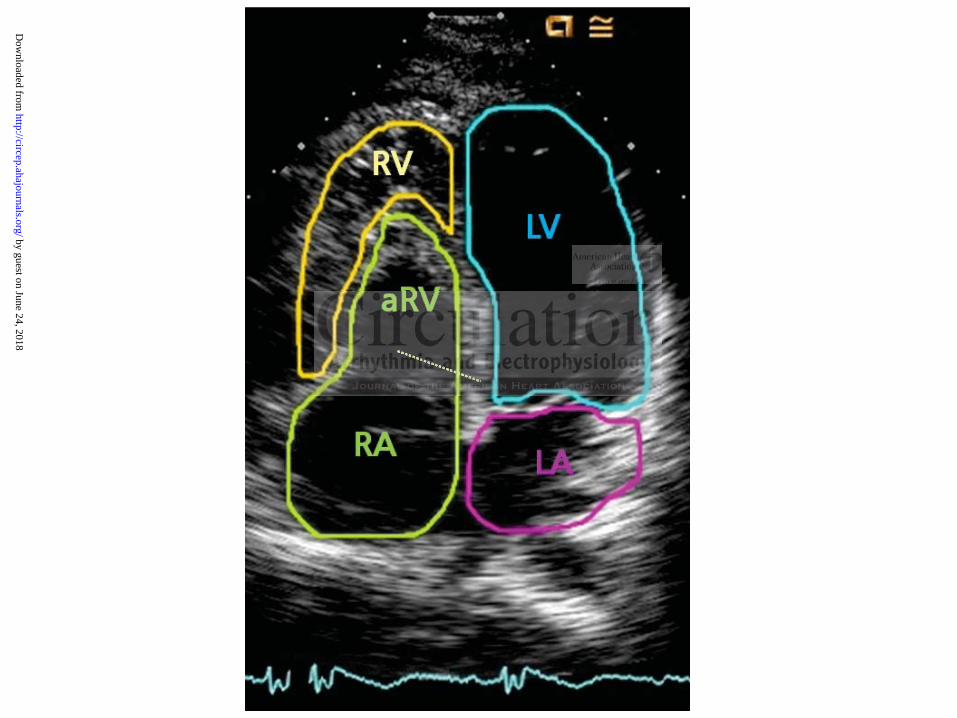
Approximately two-thirds of the patients (35/51, 68.6%) showed
(fQRS group). fQRS occurred primarily in the inferior (26 patients) and precordial (25 patients)
leads. fQRS in the lateral leads was observed in only 5 patients. The detailed distribution of
fQRS complexes is presented in Figure 3.
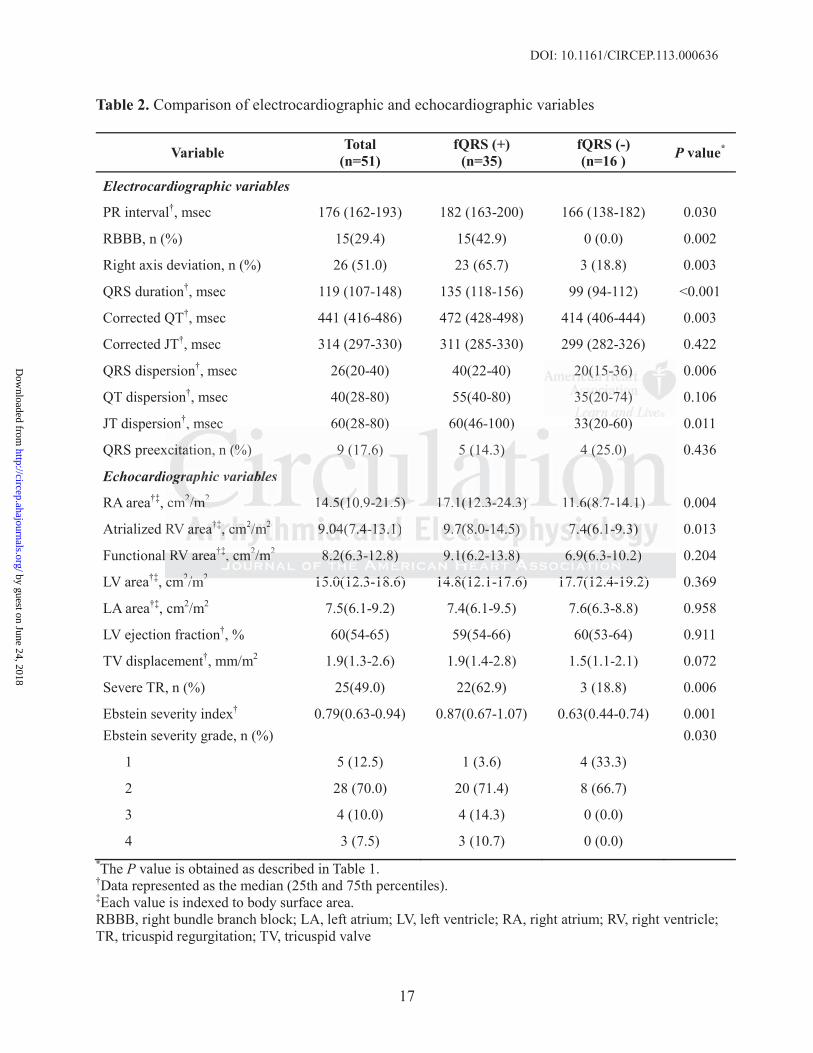
The fQRS group had a worse functional class, a greater CT ratio, a longer PR interval, a
longer QRS duration, more frequent right bundle branch blocks (RBBB), and more frequent right
axis deviations compared to the non-fQRS group (Table 1 and 2). On echocardiographic
examination, apical displacement and regurgitation of the TV were more severe in patients with
fQRS versus those without (Table 2). Functional RV, LV, and LA areas indexed to BSA showed
9%)) were in NNew w YoYoYoY r
e mosost tt cocommmmonon aaaassssssssoo
f b
l
L n
e
B t th fQRS d N fQRS G
fectttt ((((n=n=n=n 191999, ,, 3737.3.3.33%). In most of the patientntnts ss (48/51, 94.1%)% , thththe right-sided chamb
laaara gggeg r than thee lleftt, wwithhh aa combmbmbinned RRRA anand RVRVRVR aaarreaaa ooof 533 ((43-3-3-3 75) cmcmcmc 22 ccommpmpar
LA anananandddd LVLVLVL area offff 3333777 (32-222 44444444) cmmm222222 ((((PPPP( <0<0<0<0.00001010101). TTTThehehe mmmmedededediaiaiaian (2(2(225t555 h hh anananandddd 75555ththth percen
e EA AAA severiiitytyty iiiinddddex was 0000 77.79 (0(0(0( .666333-00.00 94444).).).
BB tt thth fQfQRSRS dd NN fQfQRSRS GG
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCEP.113.000636
8
no significant differences between the two groups. However, aRV and RA enlargements were
more prominent in the fQRS group; therefore, the fQRS group showed a greater severity index
compared to the non-fQRS group (P<0.001). The indexed aRV area (Spearman’s r=0.51,
P<0.001), indexed RA areas (Spearman’s r=0.60, P<0.001), and Ebstein severity index
(Spearman’s r=0.58, P<0.001) were positively correlated with the extent of the fQRS (see
supplemental Figure 1).
Associations Between fQRS Complexes and Arrhythmic Complications
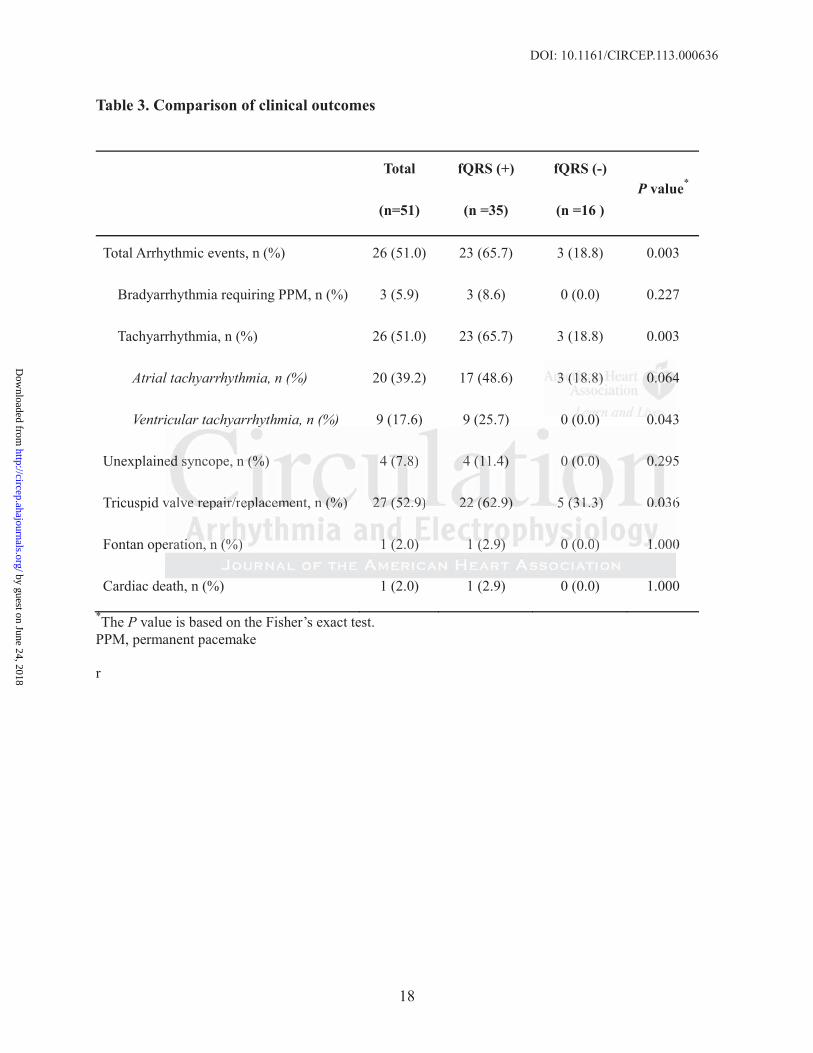
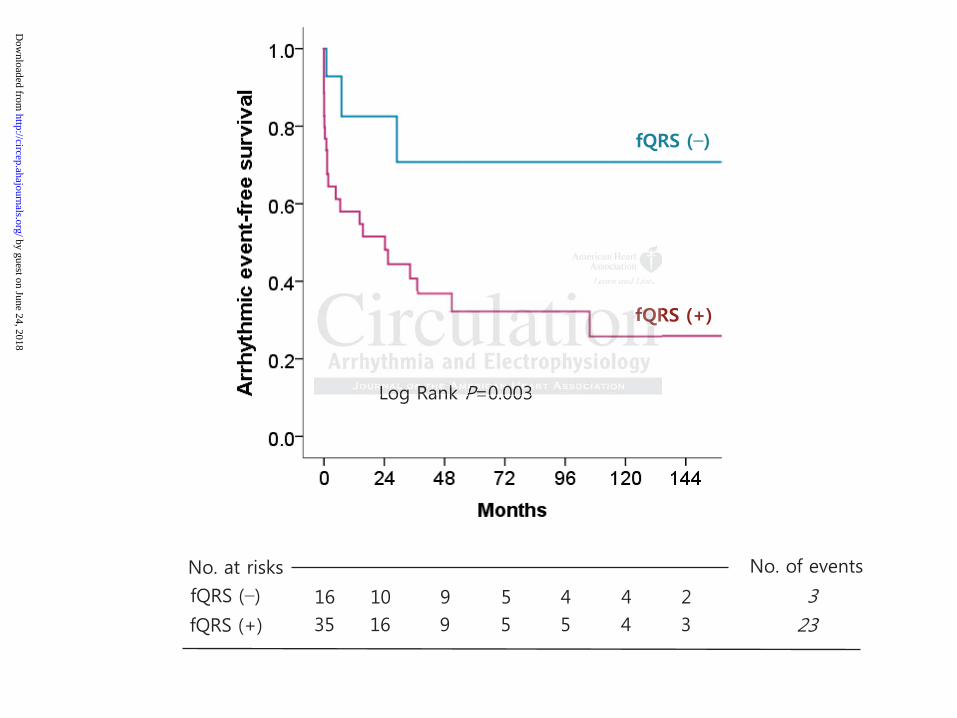
Table 3 summarizes clinical outcomes. Median follow-up duration (25th and 75th percentiles)
was 49 (25-116) months with no significant difference between the fQRS and non-fQRS groups
[49 (29-112) versus 51 (1-126) months, P=0.699]. Compared to the non-fQRS group, a greater
proportion of patients in the fQRS group underwent TV replacement/repair or a Fontan operation
due to severe TR and right heart failure. The incidence of AVRT with AP was not significantly
different between the two groups (fQRS versus non-fQRS group, 5/35 versus 4/16, P=0.436).
However, ventricular tachyarrhythmia (9/35, 25.7%), unexplained syncope (4/35, 11.4%), and
cardiac death due to right heart failure (1/35, 2.9%) were only found in patients with fQRS.
Sustained VT, appropriate shock for VF, and non-sustained VT episodes occurred in five, one,
and three patients with fQRS, respectively. The atrial tachyarrhythmic event (AF, AFL, and AT)
rate was also higher in the fQRS group (48.6% versus 18.8%, P=0.064). In addition, permanent
pacemaker implantation was performed only in patients with fQRS due to complete (n=2) or
advanced (n=1) AV block. Overall, total arrhythmic events occurred more frequently in the
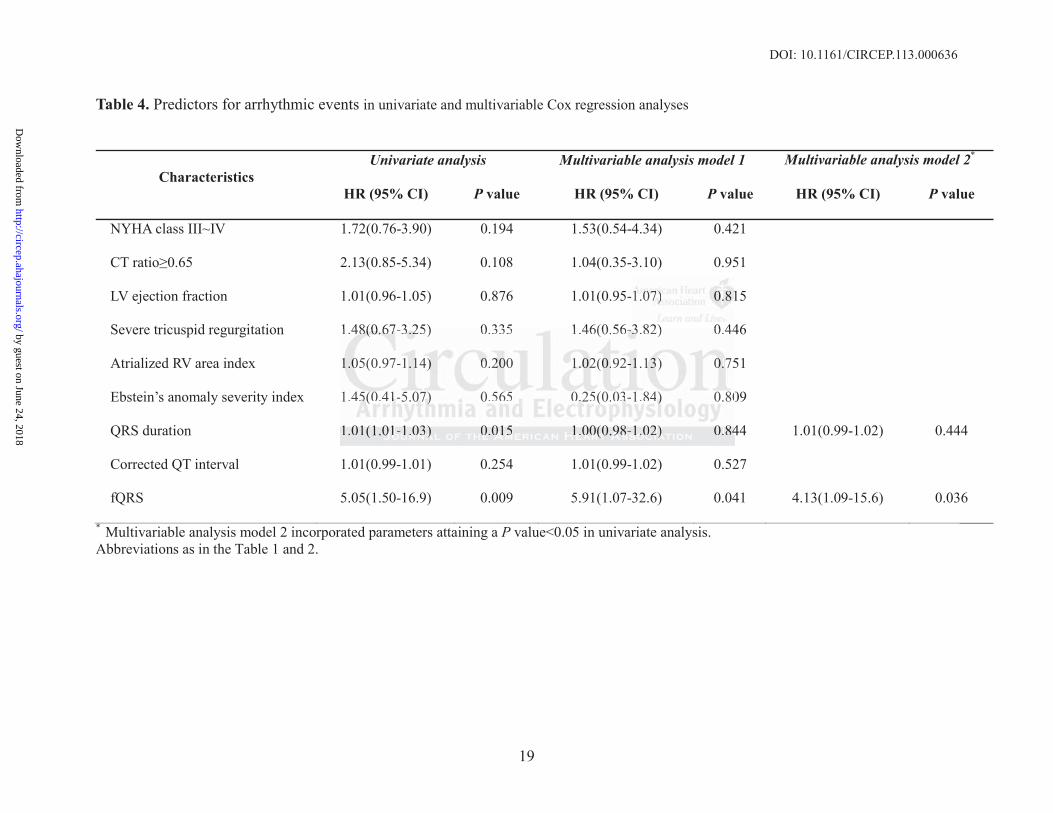
fQRS group compared to the non-fQRS group during the follow-up (Figure 4). The presence of
fQRS in Cox regression analysis was independently associated with total arrhythmic events,
even after adjusting for relevant clinical, radiographic, echocardiographic, and
5th and 75th pep rcenenenntititt l
QRS aandddnd nnonon-fQfQfQfQRSRSRSRS ggr
2 e
of patients in the RS group underwent TV re acement/repair or a Fontan ope
e a
e
entric lar tach arrh thmia (9/35 25 7%) ne plained s ncope (4/35 11 4%) a
2) vvvverererersussuss s 51551 (1-1-1-1 126) months, P=0.699]. CCCoompared to theh nnnononono -fQRS group, a gre
oooof pappp tients in thhe fQfQfQRSS ggggroupp undnnderweww nt TTV rrereplplpllaccemmment/rerepaaairirir or aa aa FoFoF ntntan ooope
ere TRTRTRTR aaandndndn rigiii hththt hhhhea ttrt faiiilulululurerere. Thhhhe ee ininininciciiciddded nce ofoffof AAAAVRVRVRVRTTTT wwwiw thththt AAAAP wwasasasas notttt siiigniiiifififica
etween hthhe twtwtwooo o grgg oupspp (((fQfQfQQRRSRR versus non-fQfQfQQRSRSRS gggrouppp, 55/55 353535 vvvversus 4/4/4/4 166166, PPPP=0=0=0=0.43
ttriic ll tt hh hrh tthhmiia ((9/9/3535 2525 77%)%) lpl iai dd (4(4/3/355 1111 4%4%))
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.113.000636
9
electrocardiographic parameters (Table 4).
Discussion
New findings
The present study is the first to reveal a significant relationship between the presence of fQRS
and an increased risk of ventricular or atrial arrhythmic events. We also found fQRS to be
associated with poorer functional class, more severe TR, a larger right-sided chamber, and
greater severity of EA in adult patients with this cardiac defect.
Recently published data suggests that the fQRS detected in patients with EA reflects the
presence of RV dysfunction with greater aRV volume13. However, arrhythmic risk was not
evaluated in that study. Additionally, adult patients (>18 years old) accounted for only 60% of
their study population. Although there have been some studies dealing with arrhythmic
complications in adult patient groups, they only described the prevalence of a few types of
arrhythmias in a limited number of patients.2-5 Most of the previous data focused primarily on the
characteristics or management of AVRT with a bypass tract.14-16
In contrast, we evaluated the association between fQRS and arrhythmic risk as well as
the severity of the structural abnormality. Moreover, we tried to identify predictors for
arrhythmic events more directly associated with dysplasia/degenerative changes in the
atrial/ventricular myocardium; these arrhythmic complications will pose greater challenges to
clinicians than AVRT using bypass tracts especially in adult EA patients because of recent
advances in their long-term survival and in ablation technology. Our data show that
approximately 50% of adult patients with EA experienced arrhythmic complications, which is
consistent with previous studies.2,4,5,16 In addition, we found the presence of fQRS to be
atientttts s wiiiwithththth EEEEAAAA reeflflflfleeecec
f 13 t
n %
o
as in a limited n mber of patients 2 5 Most of the pre io s data foc sed primaril
f RVRVRVRV ddddysysysfufufufunnctititioonoo with greater aRV voluuuumemem 13. However,rr arrrrrrrhhhythmic risk was not
nnnn thhhah t study. AAddditttioonallllylylyy, adddduuulttt ppatienennts (>(>18888 yyyyeaeaeaearss ooolddd) accccounuunttet d fofoff rr r ononly 666000%
popuuuulalalatitiition. AlAlAlA thththhou hhhgh therererer hhhhave bebebebeenenen some ststtstududududieieessss deeealalala iiing withhhh aaaarrrrrrr hhhhythththt iimic
ons iini adddulllt papapaa ittit ent grgg oupspp , theyyy o llnlly yy describebbb d dd hththhe prpp evevvv lallennnceccc of ff a ffef w tytytyypepepep sss s of
a iin lliimitit ded bbe fof tatiie tnt 2 52-22 555 MM tt fof tthhe ii ddatta ff ded iri irill
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCEP.113.000636
10
independently associated with overall arrhythmic events, even after adjusting for relevant clinical
and echocardiographic parameters.
fQRS Complexes and Risk of Ventricular Tachyarrhythmias
Fragmentation of QRS morphology on surface ECG reflects inhomogeneous ventricular
activation caused by myocardial scar in patients with a prior myocardial infarction.7,17 As the
myocardium is replaced by scar tissue following an infarction, myocardial conduction slows or
becomes blocked around the infarcted zone, resulting in a ‘zigzag’ course of activation.18 fQRS
was also associated with an increased risk of arrhythmic events in nonischemic dilated
cardiomyopathy patients.8
Several histopathologic studies on EA demonstrated that the atrialized portion of the RV
becomes disproportionately dilated and has extensive fibrosis with reduced numbers of
myocytes.19,20 Additionally, the abnormal signal observed during endocardial mapping of the
aRV was related to the bizarre configuration of the widened QRS complexes on surface ECG.21,22
They also showed that the aRV was particularly irritable, and therefore, could serve as a
substrate for VF.21,23 Indeed, in our study, patients in the fQRS group had significantly larger
aRV area and more frequent ventricular arrhythmic complications compared to the non-fQRS
group. Moreover, the extent of fQRS complexes was positively correlated with the aRV area
(Spearman’s r=0.51, P<0.001). Therefore, fQRS in adults with EA might signify a higher burden
of arrhythmogenic substrate. We previously reported that in adults with repaired tetralogy of
Fallot (TOF), myocardial fibrosis was predominant in the RV outflow tract, and that fQRS was
found at least twice as frequently in the right to mid precordial leads than in the inferior lead
showing a good spatial concordance between the fQRS and RV scarring.9 In the present study,
however, the most common locations of fQRS were the inferior and precordial leads, and fQRS
ischemic dilated
veral histopathologic studies on EA demonstrated that the atrialized portion of th
i
h
elated to the bizarre configuration of the widened QRS complexes on surface EC
sho ed that the aRV as partic larl irritable and therefore co ld ser e as a
verralalal hhhhisisisi tototoopappathhhololologic studies on EA demmmonononsstrated that tttheh aaaatrtrtrtrialized portion of th
isssps rrror portionattelly dddilllateddd andddd hhhhasss eextenennsiveve fibbbbrorooosisisiis wiiithhh redduucededede nummmmbbeb rsrs of f
99,20002000 AAAAdddddddititititiiionalllllly, ttthhhe abnorororormmmal siiiigngngngnalalal obsbbb ervedddd dududud riririring eeee ddnddocardididiialalala mmapappiiing fffof ttth
elateddd to thhhe bibibiizarre confffigigigurattiiion ffoff the widididden dded QQQRSRSRSRS ccccomplplpllexes on surffffacacaca eee e EC
hsh ded tthhatt thth RaRVV trtiic ll ll ii itit bablle dd thth fef ldld
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCEP.113.000636
11
were negligible in the lateral leads. In EA, the aRV, or the inlet component, is the main site of
congenital dysplasia and subsequent degeneration. With further enlargement, the aRV could
occupy a greater proportion of the inferior wall of the heart, making fQRS complexes in the
inferior leads as frequent as that in precordial leads. Repolarization parameters such as QTc and
QRS/QT dispersions were measured worse in the fQRS group compared to the non-fQRS group.
Repolarization parameters therefore might also be associated with an increased susceptibility to
ventricular arrhythmia.
fQRS Complexes and Risk of Atrial Tachyarrhythmias
The degree of apical displacement, regurgitation of the TV, and RA enlargement were more
severe in the fQRS group than the non-fQRS group. The indexed RA areas were positively
correlated with the extent of the fQRS. These abnormalities could make patients with fQRS more
vulnerable to atrial tachyarrhythmias related to degenerative changes in the atria, such as AF,
AFL, and AT. As mentioned above, atrial tachyarrhythmias including AF, AFL, and AT tended
to occur more frequently in the fQRS group than in the non-fQRS group (48.6% versus 18.8%,
P=0.064).
fQRS Complexes and Risk of Bradyarrhythmias
The AV conduction system in EA, especially the right bundle branch traveling over the
dysplastic aRV portion, is abnormally formed and shows marked fibrosis. The AV node is also
compressed due to enlargement of the right-sided chambers.1,24,25 Additionally, chronic
hemodynamic stress in adult EA patients can aggravate right-sided chamber dilatation,
dysfunction, and fibrosis.1,2 All of these factors could predispose the development of
bradyarrhythmia. The longer PR intervals and more frequent RBBB observed in the fQRS group
might suggest more fibrosis within the right-sided chambers and in the right bundle branch and
nlargegemementnttt wwerere e momomomorr
h y
w S
to atrial tachyarrhythmias related to degenerative changes in the atria, such as A
A n
ore freq entl in the fQRS gro p than in the non fQRS gro p (48 6% ers s 18
he fQfQQfQRSRSRR ggggrorroupppp tthan the non-fQRS grouppp. ThTTT e indexed RAAA aaaareas were positively
wwwwitttth h the extennt of thththe fQQQRRSRR . TThTT eseese abbnnnormmalititittieieiesss cooulllddd maakee pppatattientttts wiwithh fQRQRQRS
to attttririrrialalal ttttachyhhh arrhhhh ttythhhhmias sss rererelated ddd totototo ddddeggeneratattativivivve chchchchannngggeg s iiin tttthe aaaatrtrtrtriiia, su hhchh as AAAA
AT. AAAs mentioioioonneddd d bbabove, atrialll tachhhhyayy rrhyhyhy hthhh iimias iiinclullul dididid nggg AFAFAFAF, AFAFAFFLL,L andndndnd AAAATTTT ten
ff ttll ii thth fQfQRSRS tthha iin tthhe ffQRQRSS (4(488 6%6% 1818
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCEP.113.000636
12
more adverse hemodynamic impact on these structures. Although not statistically significant,
first degree AV block (24% versus 13%, P=0.464) was more prevalent in the fQRS group, and
permanent pacemakers were implanted only in patients showing fQRS due to advanced or
complete AV block.
Clinical Implications
In our study, lower functional class at the time of presentation, a greater CT ratio, more advanced
grade of EA, and a higher rate of corrective surgery were found in the fQRS group, which had a
larger average aRV area. These results are in agreement with previous studies that showed aRV
volume to be independently related to aerobic capacity, and that the volume of the aRV is a
novel CMR measure which may describe the severity of disease in adults with unrepaired
EA.12,26 On the other hand, QRS duration is considered a good surrogate marker for severity of
disease. The wider the QRS complex and the greater the degree of TR and RV enlargement, the
worse the clinical course.12, 27 Our data also showed that QRS duration was as good as QRS
fragmentation in predicting RV structural remodeling (see supplemental Figures 2) and
arrhythmic risks (see supplemental Figures 3).
Therefore, further investigation might be worthwhile in order to ascertain whether fQRS,
independently or in combination with QRS duration, could be a potential marker of worsening
right-sided heart dysplasia/dysfunction (see supplemental Figures 4 and supplemental Table).
Also, it would be useful to further investigate the association between fQRS and increased
vulnerability to atrial and/or ventricular tachyarrhythmia as well as bradyarrhythmia in larger
adult cohorts with this anomaly.
Study Limitations
This study has several limitations. Firstly, comparisons from this analysis are limited by their
studies that showewewewed ddd
olumme e ooffff ththththee RRaRaRV VVV isisisis a
R
n t
h t
c S
ion in predicting RV str ct ral remodeling (see s pplemental Fig res 2) and
R memememeasasasa ururreeee whwhwhicicich may describe the severrritititityy of disease in nn adddduuults with unrepaired
n thhhhe other handnd, QRQRQRS dududuurationon iiis consnssidereed aaa ggggoooooooodd suurrrroggatte d mamm rkeererr fofof r sevvverrrit
he wididididererer tttthhheh QQQQRSRSRSS complexxxx aaand thehehehe grerere tatter ttthehhh ddddeeegrerereree ofofofof TRTRTRTR and RRRRVVV V enlal rgementRRR
cliniciii alll course.ee 1222 2727712222, 272727 OOOur dddatta allllso shhhoh weddd hthhatt QQQQRSRSRSR dddurratatata ioii n nn wwwaw s as gggoodd d asasasas QQQQRS
iio iin didi tctiin RVRV ttr tt ll ddelili ((s lpl ttall FiFi 2)2) dnd
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.113.000636
13
retrospective design, in which unmeasured confounders may preclude any definite conclusion.
Therefore, prospective studies on a larger scale are needed to and to show
the clinical implications of fQRS complexes more definitely. Secondly, the study population was
relatively small, and the follow-up duration was short. Although, our cohort is one of the largest
adult-only groups. Thirdly, the extent of the cardiac fibrosis and the volumetric measurements
were not confirmed by biopsy or cardiac magnetic resonance (CMR) imaging. However, we
adopted a grading system to quantify the severity of EA, and our data correspond well to those
acquired from CMR examination.13
Conclusions
Fragmented QRS complexes on 12-lead ECG were found in approximately two-thirds of adult
patients with Ebstein’s anomaly. fQRS complexes were associated with larger atrialized right
ventricle, a more severe anomaly, and an increased risk of arrhythmic events in this patient group.
Conflict of Interest Disclosures: None.
References:
1. Attenhofer Jost CH, Connolly HM, Dearani JA, Edwards WD, Danielson GK. Ebstein's anomaly. Circulation. 2007;115:277-285.
2. Celermajer DS, Bull C, Till JA, Cullen S, Vassillikos VP, Sullivan ID, Allan L, Nihoyannopoulos P, Somerville J, Deanfield JE. Ebstein's anomaly: presentation and outcome from fetus to adult. J Am Coll Cardiol. 1994;23:170-176.
3. Hebe J. Ebstein's anomaly in adults. Arrhythmias: diagnosis and therapeutic approach. Thorac Cardiovasc Surg.2000;48:214-219.
4. Chang YM, Wang JK, Chiu SN, Lin MT, Wu ET, Chen CA, Huang SC, Chen YS, Chang CI, Chiu IS, Lin JL, Lai LP, Wu MH. Clinical spectrum and long-term outcome of Ebstein's anomaly based on a 26-year experience in an Asian cohort. Eur J Pediatr. 2009;168:685-690.
n
d d
g
a t
ns
dddd QQQQRS complexexes oon 12-2-2--leadddd ECGCCG weweere ffooundndndnd iiin n n n aapppproooximmaatelelellyy y twoo-oo thtt iirdds ooof ff ad
th EbEbEbbstssteieiiein’s anom llaly. fQRQRQRQRSSSS compmpmpplelelelexexx s were aaassssssssocococociaiaiaiateeedddd iiwithththh larggggerrerer atriiiiallliiizedddd rigii
a more severee aaaanomalylyly, anddd d an iiincreasedddd risii k kkk fofff arrhyhyhyththththmimimim c evevevevents iiiin thhthhisisisis ppppatatattient
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.113.000636
14
5. Lee YS, Baek JS, Kwon BS, Kim GB, Bae EJ, Noh CI, Choi JY, Yun YS. Pediatric emergency room presentation of congenital heart disease. Korean Circ J. 2010;40:36-41.
6. Zomer AC, Vaartjes I, Grobbee DE, Mulder BJ. Adult congenital heart disease: New challenges. Int J Cardiol. 2013;163:105-107.
7. Das MK, Suradi H, Maskoun W, Michael MA, Shen C, Peng J, Dandamudi G, Mahenthiran J.Fragmented wide QRS on a 12-lead ECG: a sign of myocardial scar and poor prognosis. Circ Arrhythm Electrophysiol. 2008;1:258-268.
8. Das MK, Maskoun W, Shen C, Michael MA, Suradi H, Desai M, Subbarao R, Bhakta D.Fragmented QRS on twelve-lead electrocardiogram predicts arrhythmic events in patients with ischemic and nonischemic cardiomyopathy. Heart Rhythm. 2010;7:74-80.
9. Park SJ, On YK, Kim JS, Park SW, Yang JH, Jun TG, Kang IS, Lee HJ, Choe YH, Huh J.Relation of fragmented QRS complex to right ventricular fibrosis detected by late gadolinium enhancement cardiac magnetic resonance in adults with repaired tetralogy of fallot. Am J Cardiol.2012;109:110-115.
10. Celermajer DS, Cullen S, Sullivan ID, Spiegelhalter DJ, Wyse RK, Deanfield JE. Outcome in neonates with Ebstein's anomaly. J Am Coll Cardiol. 1992;19:1041-1046.
11. Zoghbi WA, Enriquez-Sarano M, Foster E, Grayburn PA, Kraft CD, Levine RA,Nihoyannopoulos P, Otto CM, Quinones MA, Rakowski H, Stewart WJ, Waggoner A,Weissman NJ; American Society of Echocardiography. Recommendations for evaluation of the severity of native valvular regurgitation with two-dimensional and Doppler echocardiography. JAm Soc Echocardiogr. 2003;16:777-802.
12. Pencina MJ, D’Agostino RB. Overall c as a measure of discrimination in survival analysis: Model specific population value and confidence interval estimation. Stat Med. 2004;23:2109 -2123.
13. Egidy Assenza G, Valente AM, Geva T, Graham D, Romana Pluchinotta F, Sanders SP,Autore C, Volpe M, Landzberg MJ, Cecchin F. QRS duration and QRS fractionation on surface electrocardiogram are markers of right ventricular dysfunction and atrialization in patients with Ebstein anomaly. Eur Heart J. 2013;34:191-200.
14. Cappato R, Schlüter M, Weiss C, Antz M, Koschyk DH, Hofmann T, Kuck KH. Radiofrequency current catheter ablation of accessory atrioventricular pathways in Ebstein's anomaly. Circulation. 1996;94:376-383.
15. Kanter RJ. Ebstein's anomaly of the tricuspid valve: a Wolf(f) in sheep's clothing. JCardiovasc Electrophysiol. 2006;17:1337-1339.
16. Legius B, Van De Bruaene A, Van Deyk K, Gewillig M, Troost E, Meyns B, Budts W.Behavior of Ebstein's anomaly: single-center experience and midterm follow-up. Cardiology.
e HJ, Choe YH,, HuHuHuHuh hhhccccteteteteddd d bybybyby llllatatatateeee gagagagadodddolilililinniniuuuulogy ooffff fafffallllllllotttot. AmAmAA JJJJ CC
majer DS, Cullen S, Sullivan ID, Spiegelhalter DJ, Wyse RK, Deanfield JE. Outcos
io
op
h di 2003;16:777 802
majajajajerererer DS, CCCCululuullelelen nnn S,,S, SSSulululllilll vavaavan nnn IDIIDI , , SpSpSpieieiegegegelhaaltter DJDJDJDJ, , , WyWyyWysesesee RRRK,KK,K Deaaaeanfnfnfnfieieiei ldll JJJE.E.E.E OOOOutuuu cos wwiwiw th Ebstein's anooommalyyy... J AmAmAmA CCCooll CaCCarddiool. 11119999992;22;2 1999:1110411-10004646464 .
WAAAA, EnEnEnEn iriququez-SaSSS rano MMMM, FFoFoF sterr EEEE, GGGrGrayaybbburnnn PPPPAAAA, KKKKrafafafafttt CDCDCDD, Levivivivinnnen RRRRAAA,opouuulolololosss PPP,,,, OtOtOtttototoo CCCMMMM, QuQuQuQuininininononono essss MMMMAAAA,,, RaRR kokokoowswswsskikikik HHHH, StStStStewewewewararara ttt WJWJWJWJ,,, WaWaWaW ggggggg onononnerererer AAA,,,,NJ; AmAA ericii anannn SSSSociiietytyty off f EEEcE hoca drddioiii grgg appphyhyhy. ReRR commeneee dadd tititiooono s fffor ev laluauauauatititit ooono onative valalalvuvuvuvulalalar rrr rererer gugugugurgrgrgrgititiitataata ioioion nn wiwiwiwithththth ttwowowowo-d-d-d-dimmimimeneee sisisionononnalalalal aaanddndnd DDDDopopopopplplpplerererer eeeechchchchococococara diographh didi 20200303 1;166:777777 808022
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.113.000636
15
2010;117:90-95.
17. Cetin M, Kocaman SA, Kiris T, Erdogan T, Canga A, Durakoglugil ME, Ciçek Y, Dogan S,Satiroglu O. Absence and Resolution of Fragmented QRS Predict Reversible Myocardial Ischemia With Higher Probability of ST Segment Resolution in Patients With ST Segment Elevation Myocardial Infarction. Korean Circ J. 2012;42:674-683.
18. de Bakker JM, van Capelle FJ, Janse MJ, Tasseron S, Vermeulen JT, de Jonge N, Lahpor JR. Slow conduction in the infarcted human heart. 'Zigzag' course of activation. Circulation.1993;88:915-926.
19. Tede NH, Shivkumar K, Perloff JK, Middlekauff HR, Fishbein MC, Child JS, Laks H. Signal-averaged electrocardiogram in Ebstein's anomaly. Am J Cardiol 2004;93:432-436.
20. Celermajer DS, Dodd SM, Greenwald SE, Wyse RK, Deanfield JE. Morbid anatomy in neonates with Ebstein's anomaly of the tricuspid valve: pathophysiologic and clinical implications. J Am Coll Cardiol. 1992;19:1049-1053.
21. Kastor JA, Goldreyer BN, Josephson ME, Perloff JK, Scharf DL, Manchester JH, Shelburne JC, Hirshfeld JW Jr. Electrophysiologic characteristics of Ebstein's anomaly of the tricuspid valve. Circulation. 1975;52:987-995.
22. Shinohara T, Tsuchiya T, Takahashi N, Saikawa T, Yoshimatsu H. The characteristics of an abnormal electrogram on the atrialized right ventricle in a patient with Ebstein's anomaly. Pacing Clin Electrophysiol. 2009;32:269-272.
23. Obioha-Ngwu O, Milliez P, Richardson A, Pittaro M, Josephson ME. Ventricular Tachycardia in Ebstein's Anomaly. Circulation. 2001;104:E92-E94.
24. Munoz-Castellanos L, Barros W, Garcia F, Salinas CH, Kuri M. [A pathological study of valvular dysplasia and attachment in Ebstein's anomaly]. Arch Inst Cardiol Mex. 1993;63:101-109.
25. Ho SY, Goltz D, McCarthy K, Cook AC, Connell MG, Smith A, Anderson RH. The atrioventricular junctions in Ebstein malformation. Heart. 2000;83:444-449.
26. Tobler D, Yalonetsky S, Crean AM, Granton JT, Burchill L, Silversides CK, Wald RM. Right heart characteristics and exercise parameters in adults with Ebstein anomaly: New perspectives from cardiac magnetic resonance imaging studies. Int J Cardiol. 2013;165:146–150.
27. Brown ML, Dearani JA, Danielson GK, Cetta F, Connolly HM, Warnes CA, Li Z, Hodge DO, Driscoll DJ; Mayo Clinic Congenital Heart Center. The outcomes of operations for 539 patients with Ebstein anomaly. J Thorac Cardiovasc Surg. 2008;135:1120-1136.
E. Morbid anatomymyyy iiiinnggggicicicic aaaandndndnd cccclilililininininicacacacal lll
JA, Goldreyer BN, Josephson ME, Perloff JK, Scharf DL, Manchester JH, Shelbeld JW Jr. Electrophysiologic characteristics of Ebstein's anomaly of the tricuspic
ara T, Tsuchiya T, Takahashi N, Saikawa T, Yoshimatsu H. The characteristics oe Pr
a Ng O Millie P Richardson A Pittaro M Josephson ME Ventric lar
JA,A,A,A, GGGGolololo drdrdrd eyeeyererrr BBBN, Josephson ME, Perlooooffffffff JK, Scharf DLDD , MMaMM nchester JH, Shelbelllldd dd JJWJJ Jr. EEEEleeectctctctrorophphphp ysysysy ioiiiololologigigigicccc chhharararacccteteterir stticcs ofofof EEEEbsbbsb teeeinininin'sss aanononoomalyyyly oooofff the e e trtrtrt icicicusuusu picuuuulaaaation. 1975;552:9998887-999595959 .
ara T,TT,T TTTsssusuchhhhiyiii a T,T,TT TTTTakahhhhasasasa hhhhi N, SaSaSaSaikikikikawa TT,T,T YYYYooooshihihih mmmamatststssu H.HH TTTThe cccchahahaharacttterisiii tititics oelectrtrtrrogogogo rararam mm onononon tttthehehh aaatrtrtrriaiaiaialililiizezezeed dd riiighghghght t t veveveventnn riiiclclclc eee inininin aaaa ppppataatieieiientntntnt wwwwititith h h h EbEbEbEbstststs eieieie n'n'n'n sss ananananomomomo alalallyy.yy Prophphphhysyy iioi l.ll 222000000999;9 3232323 :222696969-22272727272.
a NN OO MMilillili PP RiRi hch dds AA PiPitttt MM JJ hhs MMEE VV ttriic ll
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCEP.113.000636
16
Table 1. Comparison of clinical characteristics between the fQRS group and the non-fQRS group
Total
(n=51)
fQRS (+)
(n =35)
fQRS (-)
(n =16 ) P value*
Demographics
Age†, years 37 (31-45) 36 (31-45) 41 (27-45) 0.604
Male gender, n (%) 18(35.3) 11(31.4) 7 (43.8) 0.529
Diabetes mellitus, n (%) 2 (3.9) 2 (5.7) 0 (0.0) 1.000
Hypertension, n (%) 6 (11.8) 6 (17.1) 0 (0.0) 0.159
NYHA class III~IV, n (%) 27(52.9) 23(65.7) 4 (25.0) 0.014
CT ratio† 0.55 (0.50-0.62) 0.58 (0.53-0.66) 0.49 (0.45-0.52) <0.001
8 (15.7) 8 (22.9) 0 (0.0) 0.045
Associated anomaly
Atrial septal defect, n (%) 19 (37.3) 16 (44.4) 3 (20.0) 0.123
Patent foramen ovale, n (%) 5 (9.8) 5 (13.9) 0 (0.0) 0.305
Mitral valve prolapse, n (%) 1 (2.0) 0 (0.0) 1 (6.7) 0.294
Ventricular septal defect, n (%) 1 (2.0) 1 (2.8) 0 (0.0) 1.000
*The P value is based on the Mann-Whitney test for continuous variables and the Fisher’s exact test for categorical variables.†Data represented as the median (25th and 75th percentiles).CT ratio, cardiothoracic ratio; NYHA, New York Heart Association
0 (0( .0)))
4444 (2(2(2(25555.0)0)0)0)
0 55 (0 50 0 62) 0 58 (0 53 0 66) 0 49 (0 45 0 52) <
n
m
0.55 (0.50-0.62) 000.5855 (0.53-0.66) 0.49 (0.45-0.52) <
888 (111155.5.7)))) 8888 (((2( 222.2 99)9 0 (0(0(0(0.0.0.00)))
nomamamam lylylyly
deffecececcttt,, nnn (%(%(%))) 191999 (3(( 7.7.7.7 3)3)3)3 16161616 (4(4(4( 444.4444)))) 333 (2(2(2(20.00 0)0)0)0)
men ovale, n nnn (%(%(%(%))) 5555 (9(99(9.88.8.8)))) 5555 (1((1(13.3.3.9)9)99) 0000 (0(0(0(0.0.00.0)))) by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCEP.113.000636
17
Table 2. Comparison of electrocardiographic and echocardiographic variables
Variable Total(n=51)
fQRS (+)(n=35)
fQRS (-)(n=16 ) P value*
Electrocardiographic variables
PR interval†, msec 176 (162-193) 182 (163-200) 166 (138-182) 0.030
RBBB, n (%) 15(29.4) 15(42.9) 0 (0.0) 0.002
Right axis deviation, n (%) 26 (51.0) 23 (65.7) 3 (18.8) 0.003
QRS duration†, msec 119 (107-148) 135 (118-156) 99 (94-112) <0.001
Corrected QT†, msec 441 (416-486) 472 (428-498) 414 (406-444) 0.003
Corrected JT†, msec 314 (297-330) 311 (285-330) 299 (282-326) 0.422
QRS dispersion†, msec 26(20-40) 40(22-40) 20(15-36) 0.006
QT dispersion†, msec 40(28-80) 55(40-80) 35(20-74) 0.106
JT dispersion†, msec 60(28-80) 60(46-100) 33(20-60) 0.011
QRS preexcitation, n (%) 9 (17.6) 5 (14.3) 4 (25.0) 0.436
Echocardiographic variables
RA area†‡, cm2/m2 14.5(10.9-21.5) 17.1(12.3-24.3) 11.6(8.7-14.1) 0.004
Atrialized RV area†‡, cm2/m2 9.04(7.4-13.1) 9.7(8.0-14.5) 7.4(6.1-9.3) 0.013
Functional RV area†‡, cm2/m2 8.2(6.3-12.8) 9.1(6.2-13.8) 6.9(6.3-10.2) 0.204
LV area†‡, cm2/m2 15.0(12.3-18.6) 14.8(12.1-17.6) 17.7(12.4-19.2) 0.369
LA area†‡, cm2/m2 7.5(6.1-9.2) 7.4(6.1-9.5) 7.6(6.3-8.8) 0.958
LV ejection fraction†, % 60(54-65) 59(54-66) 60(53-64) 0.911
TV displacement†, mm/m2 1.9(1.3-2.6) 1.9(1.4-2.8) 1.5(1.1-2.1) 0.072
Severe TR, n (%) 25(49.0) 22(62.9) 3 (18.8) 0.006
Ebstein severity index† 0.79(0.63-0.94) 0.87(0.67-1.07) 0.63(0.44-0.74) 0.001 Ebstein severity grade, n (%) 0.030
1 5 (12.5) 1 (3.6) 4 (33.3)
2 28 (70.0) 20 (71.4) 8 (66.7)
3 4 (10.0) 4 (14.3) 0 (0.0)
4 3 (7.5) 3 (10.7) 0 (0.0)*The P value is obtained as described in Table 1. †Data represented as the median (25th and 75th percentiles).‡Each value is indexed to body surface area. RBBB, right bundle branch block; LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle; TR, tricuspid regurgitation; TV, tricuspid valve
20202020(1(1(1(15-5-5--36363636) ) ) )
35353535(2(2(2(20-0-00 74747474) )))
ion msec 60(28 80) 60(46 100) 33(20 60)
x
i
l2/ 2 15 0(12 3 18 6) 14 8(12 1 17 6) 17 7(12 4 19 2)
ion , msec 60(28 80) 60(46 100) 33(20 60)
xcccciiti aataa ion, n ((((%)%)% 9 9 9 9 (1( 7.7.6)6 555 (1(1(1(14.3)))3) 44 44 (2(2(2( 5.0)))
ioooogrgrgrgraphic variaablles
cmmm2/m/m/m/m2 1414144.5.5.5(1(1(1(10.9-9-9-21212121.5.5.55)))) 17171717.1.1.1.1(1(1(1(12.2.2.2 3-3-3-3-2424244.3.3.33))) 1111.6.6.6.6(8(8(8(8 77.77-11114.44.1)1)1)1
RV arararareaeaea†‡†‡††‡, cmcmcmm2222/m/m/m/ 2222 9.9..0404040 (7777.4.4.4.4-1-1-13.3.3.3 1)1)1)1 9.9.9.9.7(7(7(7(8.888 0-0-0-14141414.5.5.5) ) )) 7.777 4(4(4(4(6.6.6.6 1-1-1-9.9.9.9 3)3)3)3)
lll RRRVVV area†‡†‡,, cm22///m22 888.2(2(2(666.3-3-3-121212 88.8) )) 999.1(1(1(666.222-131313 88.8) ) ) 666.9(9(9(666.333-101010 22.2))) 222// 222 1515 00(1(122 33 1818 66)) 1414 88((1212 11 1177 6)6) 1717 77(1(122 44 1919 22))
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCEP.113.000636
18
Table 3. Comparison of clinical outcomes
Total
(n=51)
fQRS (+)
(n =35)
fQRS (-)
(n =16 ) P value*
Total Arrhythmic events, n (%) 26 (51.0) 23 (65.7) 3 (18.8) 0.003
Bradyarrhythmia requiring PPM, n (%) 3 (5.9) 3 (8.6) 0 (0.0) 0.227
Tachyarrhythmia, n (%) 26 (51.0) 23 (65.7) 3 (18.8) 0.003
Atrial tachyarrhythmia, n (%) 20 (39.2) 17 (48.6) 3 (18.8) 0.064
Ventricular tachyarrhythmia, n (%) 9 (17.6) 9 (25.7) 0 (0.0) 0.043
Unexplained syncope, n (%) 4 (7.8) 4 (11.4) 0 (0.0) 0.295
Tricuspid valve repair/replacement, n (%) 27 (52.9) 22 (62.9) 5 (31.3) 0.036
Fontan operation, n (%) 1 (2.0) 1 (2.9) 0 (0.0) 1.000
Cardiac death, n (%) 1 (2.0) 1 (2.9) 0 (0.0) 1.000
*The P value is based on the Fisher’s exact test.PPM, permanent pacemake
r
3333 (1(1(1(18.8.88 8)8)8)8) 00.0 06006064444
0 (0(0(00 0000)))) 0000 04040 3y y ( ) ( ) ( ) ( )
e 5
v 6
e 0
y y ( ) ( ) ( ) ( )
eeddd d sssys ncope, n (%(%(%(%) 4 (7(7(7(7.8) 4 444 (1(1(1(11.11 4)4)4)) 0 0 0 (0(0(0(0 00.00) ) ) 0.000 2922 5
valvvvveeee rerererepapapaairiririr///repepepeplalalacececec mememementnnn , n nnn (%(%(%(%)))) 2727277 (5(5(5( 2222.99.9))) 22222222 (6(6(6( 2.222 9)9)9)9 5 (3(3(331.1.1.1.3)3)3)3) 0.00.0 030303036
eratioiii n, n (((%)%)%) 111 (2(2(2( .0) ))) 111 (2(2(2( .999)))) 0000 (0(0(0.0000)) 1.111 000
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCEP.113.000636
19
Table 4. Predictors for arrhythmic events in univariate and multivariable Cox regression analyses
CharacteristicsUnivariate analysis Multivariable analysis model 1 Multivariable analysis model 2*
HR (95% CI) P value HR (95% CI) P value HR (95% CI) P value
NYHA class III~IV 1.72(0.76-3.90) 0.194 1.53(0.54-4.34) 0.421
2.13(0.85-5.34) 0.108 1.04(0.35-3.10) 0.951
LV ejection fraction 1.01(0.96-1.05) 0.876 1.01(0.95-1.07) 0.815
Severe tricuspid regurgitation 1.48(0.67-3.25) 0.335 1.46(0.56-3.82) 0.446
Atrialized RV area index 1.05(0.97-1.14) 0.200 1.02(0.92-1.13) 0.751
Ebstein’s anomaly severity index 1.45(0.41-5.07) 0.565 0.25(0.03-1.84) 0.809
QRS duration 1.01(1.01-1.03) 0.015 1.00(0.98-1.02) 0.844 1.01(0.99-1.02) 0.444
Corrected QT interval 1.01(0.99-1.01) 0.254 1.01(0.99-1.02) 0.527
fQRS 5.05(1.50-16.9) 0.009 5.91(1.07-32.6) 0.041 4.13(1.09-15.6) 0.036
* Multivariable analysis model 2 incorporated parameters attaining a P value<0.05 in univariate analysis. Abbreviations as in the Table 1 and 2.
1.111 07070707)))) 0.0.0.0.8181811
1 48(0 67 3 25) 0 335 1 46(0 56 3 82) 0.44
5
0
4
1.48888(0(0(0( ..67676767-3.3.3.3 22225) 0.335 1.46(0.56----3.333 82) 0.44
11.1 00050 (0.97-1.114)))) 00.00 202000 1.1.1.1.02020202(00..92--111.1313131 ) 000.75
1.4555((((00.41111-5.07077)))) 0.565 0.0.25(0((( .0333-1.8444)))) 0.80
11.0101(1(1.0.001111-1.1.11.030303)))) 0.0.00 00001515155 1.1.1..00000000(0(0((0.9.999888-1.1.1.1.00002222)))) 00.8484
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCEP.113.000636
20
Figure Legends:
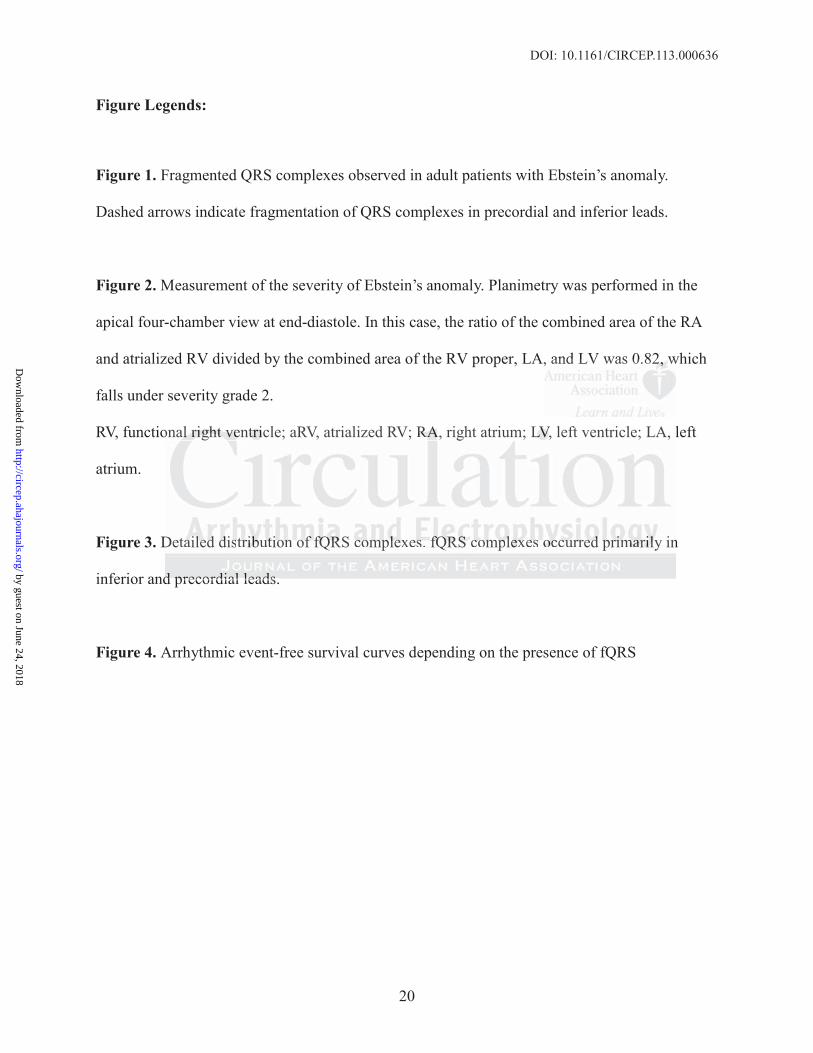
Figure 1. Fragmented QRS complexes observed in adult patients with Ebstein’s anomaly.
Dashed arrows indicate fragmentation of QRS complexes in precordial and inferior leads.
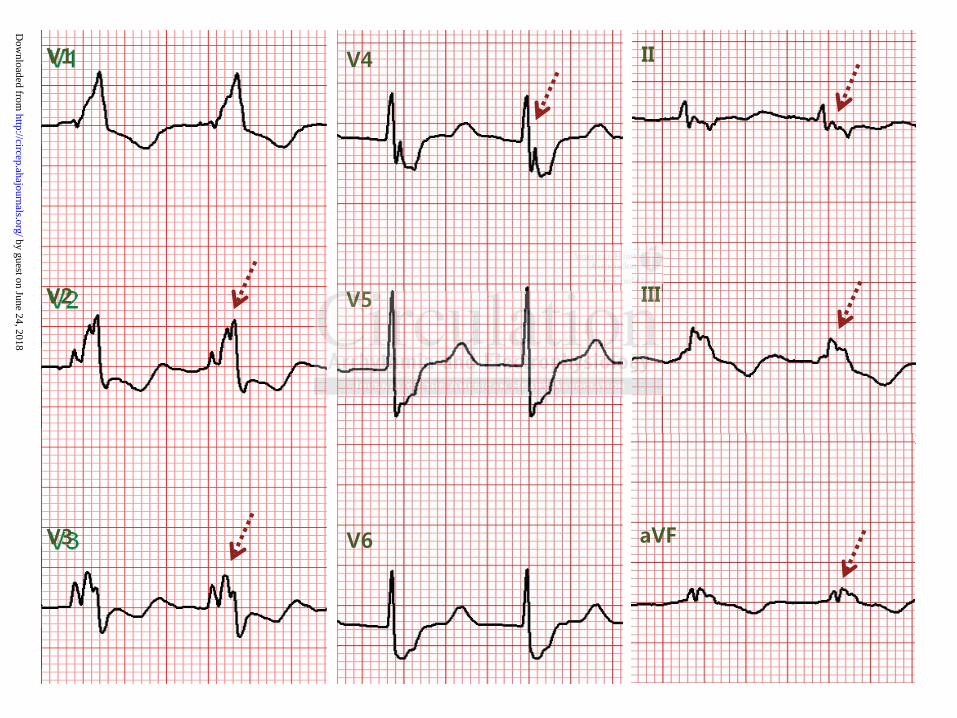
Figure 2. Measurement of the severity of Ebstein’s anomaly. Planimetry was performed in the
apical four-chamber view at end-diastole. In this case, the ratio of the combined area of the RA
and atrialized RV divided by the combined area of the RV proper, LA, and LV was 0.82, which
falls under severity grade 2.
RV, functional right ventricle; aRV, atrialized RV; RA, right atrium; LV, left ventricle; LA, left
atrium.
Figure 3. Detailed distribution of fQRS complexes. fQRS complexes occurred primarily in
inferior and precordial leads.
Figure 4. Arrhythmic event-free survival curves depending on the presence of fQRS
, and LV was 0.82222,, , , ww
onal right ventricle; aRV, atrialized RV; RA, right atrium; LV, left ventricle; LA, l
Detailed distribution of fQRS co lexes. fQRS co lexes occurred rimarily in
d precordial leads
onallalal rrrrigigigi hththtt vvvene trtrtriciii le; aRV, atrialized RV; RARARA, right atrium; LVLVLVLV, left ventricle; LA, l
Detaaaailililledededd ddddissstrtrtribibibbututututioioionn n ofofoff ffffQRQRQRRS cocococ mpmpmplelelel xexexesss. ffffQRQRQRQRS SSS cococoompmpmpplelelel xexexex sss ocococccucucucurrrrrredededd pppriririimamamamariririllylyl in
ddd pprerecocordrdrdiaiaialll leleleadadadss
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from
Shin Yi Jang, Ok Jung Lee, Jinyoung Song, I-Seok Kang and June HuhSeung-Jung Park, Seungmin Chung, Young Geun On, June Soo Kim, Ji-Hyuk Yang, Tae-Gook Jun,
Arrhythmic Risk and the Severity of the AnomalyFragmented QRS Complex in Adult Patients with Ebstein's Anomaly and Its Association with
Print ISSN: 1941-3149. Online ISSN: 1941-3084 Copyright © 2013 American Heart Association, Inc. All rights reserved.
Dallas, TX 75231is published by the American Heart Association, 7272 Greenville Avenue,Circulation: Arrhythmia and Electrophysiology
published online November 14, 2013;Circ Arrhythm Electrophysiol.
http://circep.ahajournals.org/content/early/2013/11/14/CIRCEP.113.000636World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circep.ahajournals.org/content/suppl/2013/11/14/CIRCEP.113.000636.DC1Data Supplement (unedited) at:
http://circep.ahajournals.org//subscriptions/
is online at: Circulation: Arrhythmia and Electrophysiology Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answerinformation about this process is available in the
requested is located, click Request Permissions in the middle column of the Web page under Services. FurtherCenter, not the Editorial Office. Once the online version of the published article for which permission is being
can be obtained via RightsLink, a service of the Copyright ClearanceCirculation: Arrhythmia and Electrophysiology Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on June 24, 2018http://circep.ahajournals.org/
Dow
nloaded from
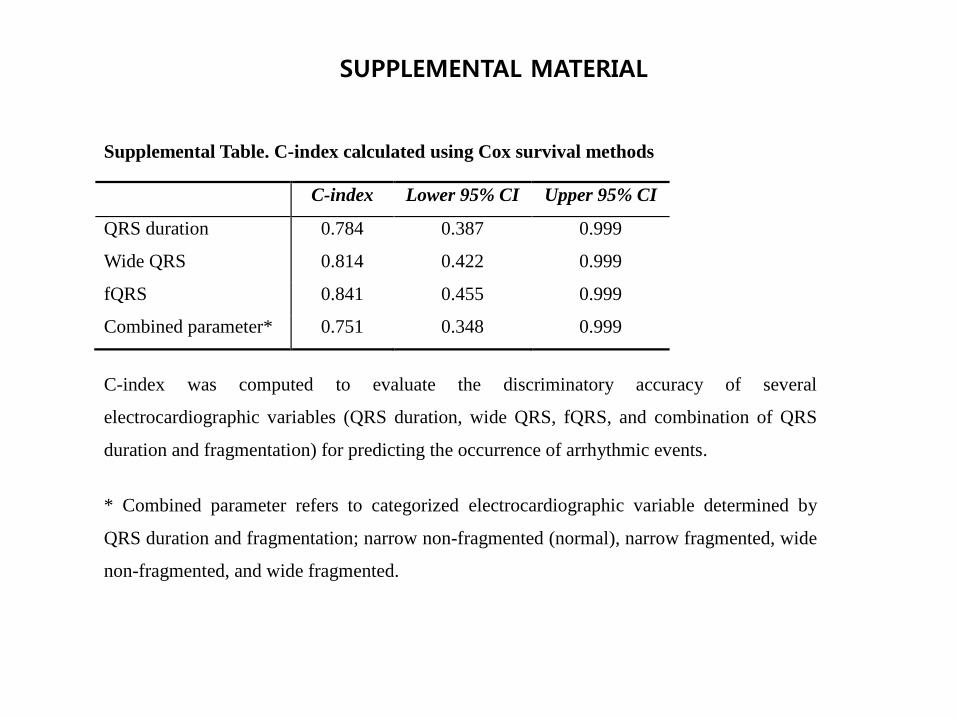
Supplemental Table. C-index calculated using Cox survival methods
C-index Lower 95% CI Upper 95% CI
QRS duration 0.784 0.387 0.999
Wide QRS 0.814 0.422 0.999
fQRS 0.841 0.455 0.999
Combined parameter* 0.751 0.348 0.999
C-index was computed to evaluate the discriminatory accuracy of several
electrocardiographic variables (QRS duration, wide QRS, fQRS, and combination of QRS
duration and fragmentation) for predicting the occurrence of arrhythmic events.
* Combined parameter refers to categorized electrocardiographic variable determined by
QRS duration and fragmentation; narrow non-fragmented (normal), narrow fragmented, wide
non-fragmented, and wide fragmented.
SUPPLEMENTAL MATERIAL
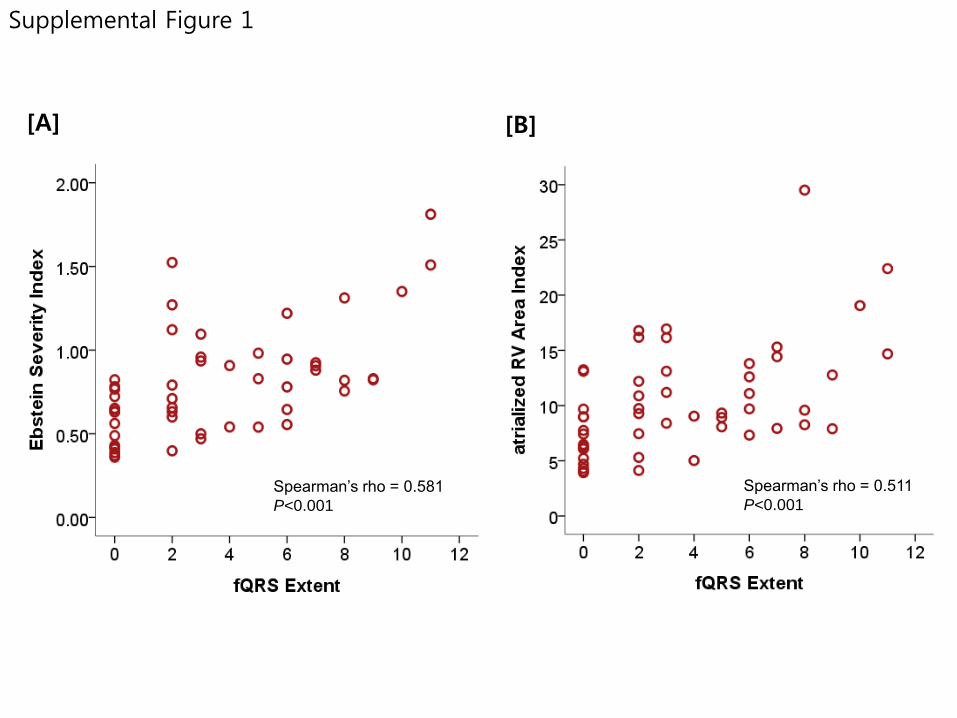
Spearman’s rho = 0.581
P<0.001
[A]
Spearman’s rho = 0.511
P<0.001
[B]
Supplemental Figure 1
Spearman’s rho = 0.396
P=0.018
[B]
Spearman’s rho = 0.453
P=0.001
[A]
Supplemental Figure 2
0
20
40
60
80
Lowest Tertile Mid Tertile Highest Tertile
(%)
QRS duration
* P for trend (total arrhythmic events)=0.004 † P for trend (ventricular arrhythmic events)=0.050
*
†
Total Arrhythmic Events
Ventricular Arrhythmic Events
Supplemental Figure 3
(%)
Total Arrhythmic Events
Ventricular Arrhythmic Events
*
†
* P for trend (total arrhythmic events)=0.002 † P for trend (ventricular arrhythmic events)=0.025
0
20
40
60
80
Normal QRS Narrow fQRS Wide fQRS
Supplemental Figure 4
Supplemental Figure Legends
Supplemental Figure 1. The extent of fQRS and the severity of Ebstein's Anomaly
QRS fragmentation shows a significant positive correlation with the severity of Ebstein's anomaly.
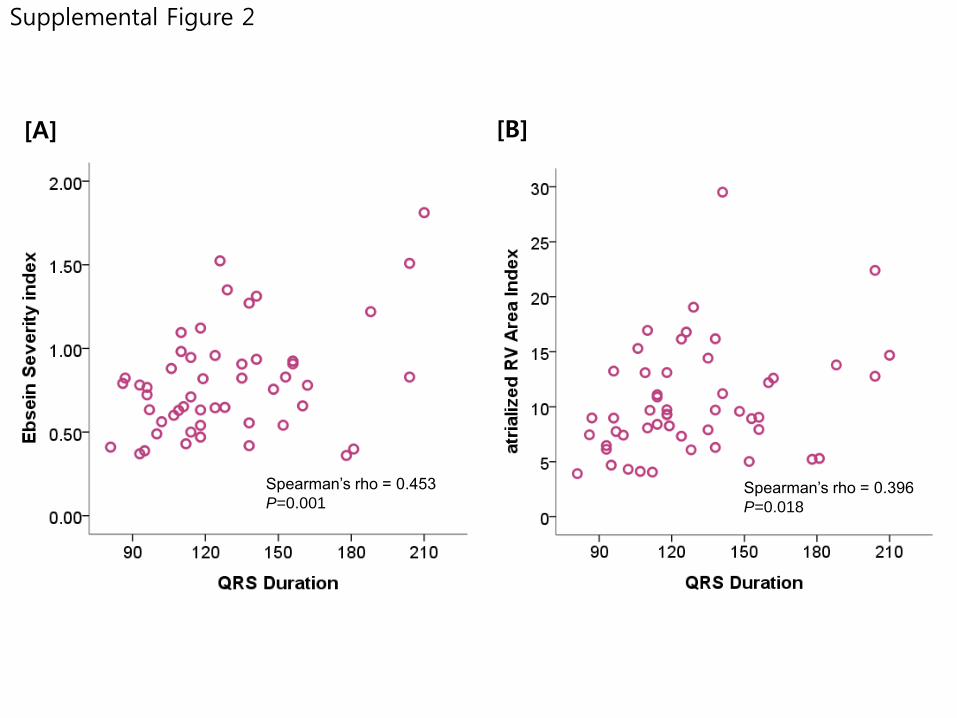
Supplemental Figure 2. QRS duration and the severity of Ebstein's Anomaly
QRS duration seems to represent quite well the severity of Ebstein's anomaly. The degree of QRS widening
showed a significant positive correlation with the aRVAi (A) as well as with the Ebstein severity index (B). The Ebstein
severity index was calculated as described in the method section.
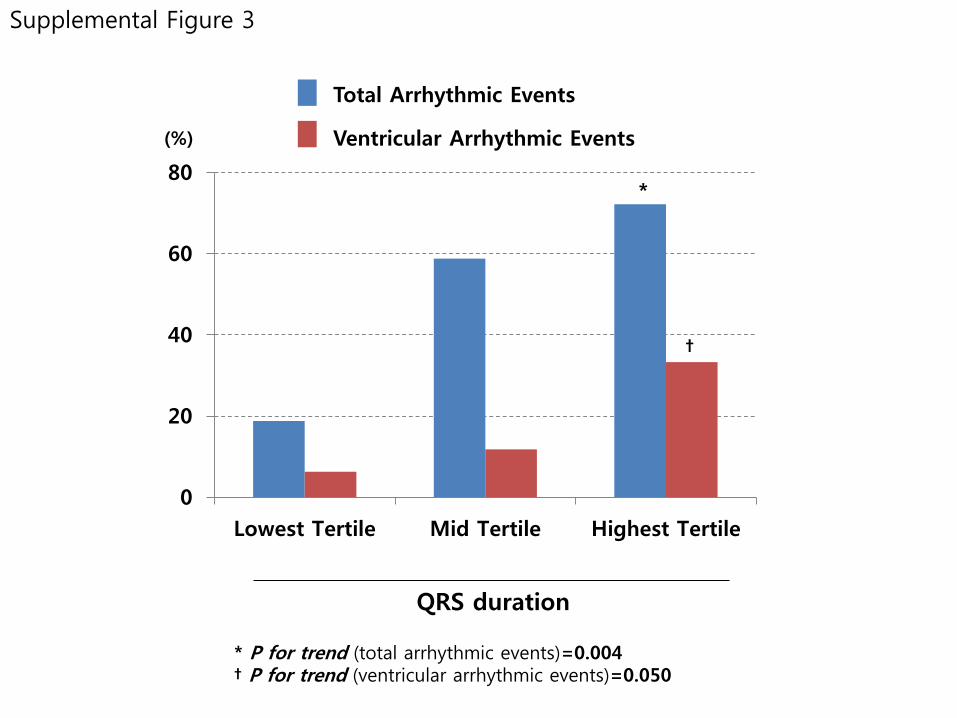
Supplemental Figure 3. QRS duration and arrhythmic burden
When our patients were divided into 3 groups depending on the degree of QRS widening, a clear trend
toward more frequent arrhythmic events (total and ventricular tachyarrhythmias) was noted in patients with longer QRS
duration.
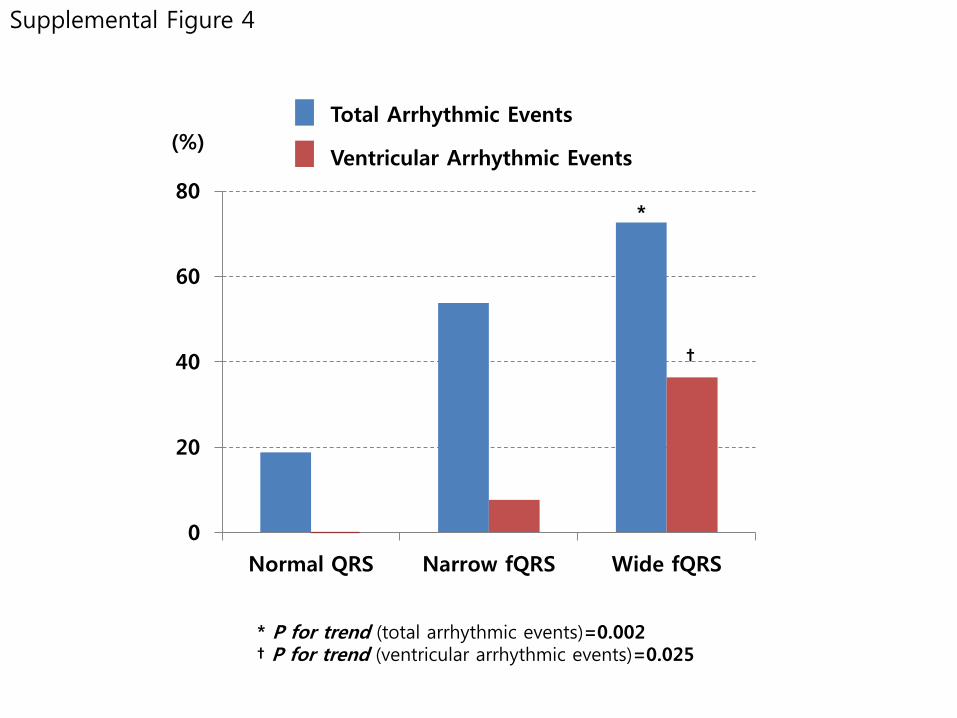
Supplemental Figure 4. Combined QRS morphologic markers (duration & fragmentation) and arrhythmic burden.
The risk of arrhythmic events tended to rise as the abnormal features of QRS morphology (prolongation and
fragmentation) were added (P for trend = 0.002 and 0.025 in total and ventricular arrhythmic events, respectively).
Recommended