Embed Size (px)
Citation preview

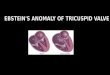
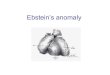
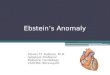
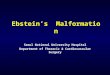
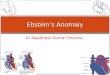
Ebstein’s anomaly
Stephanie MerharJanuary 21, 2011

Anatomy

Pathophysiology

Associated defects
• Commonly associated with:– ASD or PFO (90%)– VSD, AV canal defect– Pulmonary stenosis/atresia (20-25%)– Wolff-Parkinson-White
• Syndromes:– Down, Marfan, Noonan, Cornelia de Lange
• Maternal lithium ingestion?

Epidemiology
• Ebstein’s anomaly occurs in 0.3-0.8% of all congenital heart diseases
• 1 in 20,000-50,000 live births• Equal male:female occurrence• Mortality in children presenting in the
neonatal period is 30-50% • Mortality at all ages is 12.5%

Prenatal presentation• Difficult to diagnose prenatally • Fetal presentation is variable: possible features
include cardiomegaly, RA enlargement, tricuspid regurgitation or dysplasia, arrhythmia, or fetal hydrops
• Prognosis for the fetus diagnosed in utero with significant tricuspid valve disease is very poor (20% survival)– Progressive right heart dilatation– Cardiac failure– Lung hypoplasia– Pulmonary stenosis/atresia

Neonatal presentation
• Congestive heart failure– Due to TR and RV dysfunction
• Cyanosis– Decreased pulmonary blood flow due to R L
shunt through ASD or PFO– Increased pulmonary vascular resistance in the
neonatal period compounds this problem
• Murmur

CXR

EKG

Physical exam
• Heart sounds– First heart sound widely split with loud tricuspid
component– Second heart sound usually is normal but may be
widely split due to RBBB– Third and fourth heart sounds commonly present
• Murmurs– Holosystolic murmur of tricuspid regurgitation

Later presentation
• Cyanosis– Due to R L shunt at atrial level
• Fatigue and dyspnea– Secondary to RV failure and decreased LV ejection
fraction
• Palpitations and sudden cardiac death• Incidental murmur• Paradoxic embolism

Arrhythmias
• Due to right atrial enlargement and high prevalence of accessory pathways
• 30-50% have evidence of WPW secondary to the atrialized RV tissue
• Mapping and ablation are difficult – Atrial dilation disrupts anatomic landmarks– Accessory pathways are often multiple

Initial management• Prostaglandin infusion? (see next slide)
• Placement of umbilical catheters• Initiation of mechanical ventilation
– Minimum possible mean airway pressure– Tidal volumes of 10-15 ml/kg to overcome
atelectasis
• Management of pulmonary hypertension

Management of pulmonary hypertension
• Nitric oxide– Reduces afterload of right ventricle– Helps distinguish functional from actual
pulmonary atresia
• Sedation• Other pulmonary vasodilators?

PGEs – good or bad?

PGEs – good or bad?
• Definitely need to start PGEs if functional pulmonary atresia– Need some way to get blood to
lungs if going through PA is not an option
• If patient gets worse on PGEs, discuss with cardiologist!

Usual postnatal evaluation
• Define anatomy with echocardiography– Nature of the RV outflow tract
• If pulmonary atresia/severe stenosis, likelihood of biventricular repair is very low
– Great Ormond Street Ebstein (GOSE) score for severity
• Ratio of combined areas of true RA plus atrialized RV to the combined areas of the functional RV, LA, and LV

Echo

GOSE score
Grade Ratio Mortality
1 <0.5 8%
2 0.5-0.99
3(acyanotic)
1-1.49 10% (neonatal)45% (later)
3 (cyanotic)
1-1.49 100%
4 >1.5 100%

Surgical repair

Single ventricle repair

Transport issues
• Things to tell receiving cardiologist:– location of pulse ox (ideally pre and post), arterial
blood gas, 4 point blood pressures, appearance of the CXR
• Main problem to anticipate on transport– Desaturation!– Manage these babies like other babies with
pulmonary hypertension

References• Aggarwal S, Chintala K, and R Humes. Sildenafil use in a symptomatic neonate with severe
Ebstein’s anomaly. Am J Perinatol 2008; 25(2): 125-128.• Brown ML and JA Dearani. Ebstein malformation of the tricuspid valve: current concepts in
management and outcomes. Curr Treat Options in CV Med 2009; 11:396-402.• Cherry C, Debord S, and N Moustapha-Nadler. Ebstein’s anomaly: a complex congenital
heart defect. AORN Journal 2009; 89:1098-1111.• Dearani JA, O’Leary PW, and GK Danielson. Surgical treatment of Ebstein’s malformation:
state of the art in 2006. Cardiol Youn 2006; 16(12-20).• Jaquiss RDB and M Imamura. Management of Ebstein’s anomaly and pure tricuspid
insufficiency in the neonate. Semin Thorac Cardiovas Surg 2007;19:258-263.• Knott-Craig CJ and SP Goldbert. Management of neonatal Ebstein’s anomaly . Semin Thorac
CV Surg 2007; 10:112-116.• Paranon S and P Acar. Ebstein’s anomaly of the tricuspid valve: from fetus to adult. Heart
2008; 94:237-243.• Pashia SE. Ebstein’s anomaly. Neonatal Network 2007; 26:197-207.