Embed Size (px)
Citation preview
Journal of The Association of Physicians of India ■ Vol. 64 ■ February 201674
Ebstein’s Anomaly with Various Unexplained Arrhythmias in a 57-Year Old ManM Chaturvedi1, Sushil Singh2, A Pandey3, S Kumar2
1Associate Professor, 2Junior Resident, 3Assistant Professor, P.G. Dept. of Medicine, S.N. Medical College, Agra, Uttar PradeshReceived: 03.01.2014; Accepted: 06.03.2014
AbstractThere are very few congenital cardiac disease which may remain asymptomatic up to adulthood, Ebstein’s anomaly is one of them. With rapid advancement in the field of echocardiography many new cases identified in day-to-day practice. Timely surgical intervention in these cases may distinct survival advantage. We present a case of Ebstein’s anomaly of adult age group which is seen with typical manifestation and seen in less than 5% cases.
Introduction
Presentation of arrhythmias in adult patients is generally suggestive
of ischemic heart disease, valvular heart disease or cardiomyopathy but presentat ion of mult iple types of arrhythmias in elderly patients may sometimes give clue of congenital heart disease. Ebstein’s anomaly is otherwise a rare disease after 50 years of age, only 5% of patients live beyond fifth decade. With advancing age, the enlarged right atrium predisposes to atrial fibrillation or atrial flutter, which with reentrant supraventricular tachycardia occurs in approximately one-third patients.
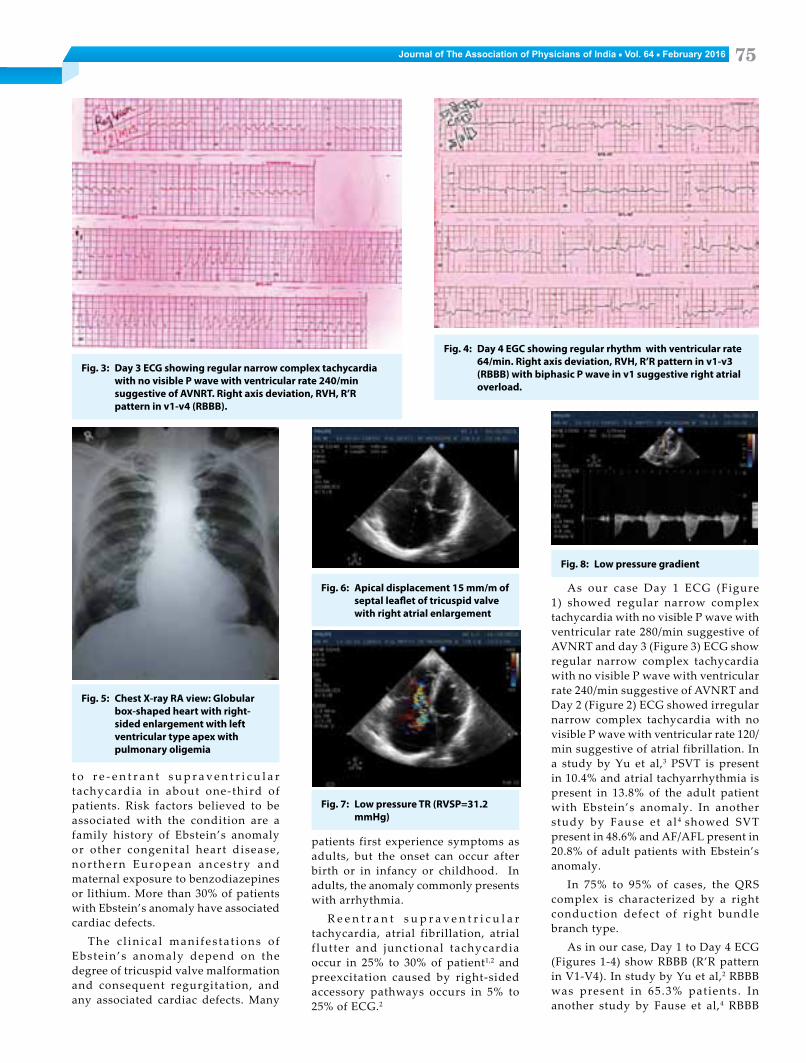
Echocardiography finding showed, apical displacement 15 mm/m of septal leaflet of tricuspid valve with right atrial enlargement with presence of low pressure tricuspid regurgitation. These finding were suggestive of Ebstein’s anomaly (Figures 6 - 8).
Discussion
T h e t r i c u s p i d va l v e a n o m a l y described by Ebstein in 1864 consists of apical displacement of the septal a n d p o s t e r i o r t r i c u s p i d l e a f l e t s , which results in an enlarged right atrium functionally integrated with the inlet region of the right ventricle (“atrial ized” r ight ventricle) . The outlet and trabecular portions of the right ventricle constitute an often hypoplastic, “functional” ventricle. Ebstein’s anomaly occurs in 1 per 20,000 live-births, accounting, for 0.3% to 0.7% of all cases of congenital heart disease while only 5% of the patients survive beyond the fifth decade.
With advancing age, the enlarged right atrium predisposes to atrial fibrillation or atrial flutter, predisposing
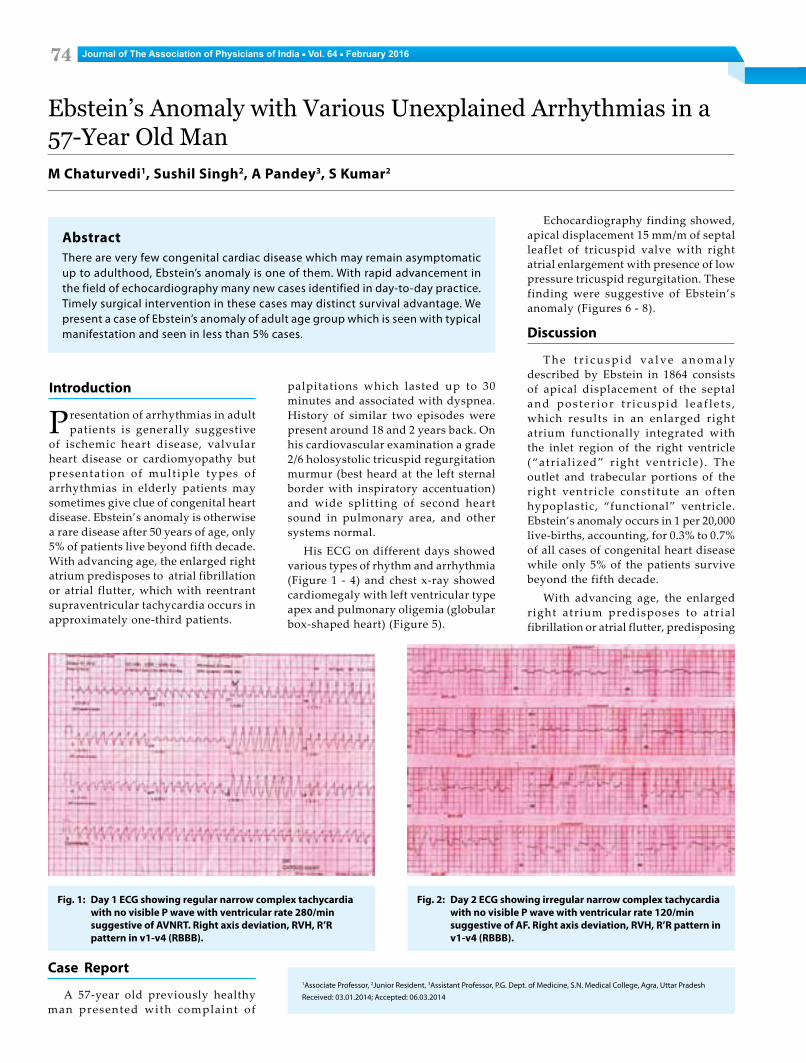
Fig. 1: Day 1 ECG showing regular narrow complex tachycardia with no visible P wave with ventricular rate 280/min suggestive of AVNRT. Right axis deviation, RVH, R’R pattern in v1-v4 (RBBB).
Fig. 2: Day 2 ECG showing irregular narrow complex tachycardia with no visible P wave with ventricular rate 120/min suggestive of AF. Right axis deviation, RVH, R’R pattern in v1-v4 (RBBB).
palpitations which lasted up to 30 minutes and associated with dyspnea. History of similar two episodes were present around 18 and 2 years back. On his cardiovascular examination a grade 2/6 holosystolic tricuspid regurgitation murmur (best heard at the left sternal border with inspiratory accentuation) and wide splitting of second heart sound in pulmonary area, and other systems normal.
His ECG on different days showed various types of rhythm and arrhythmia (Figure 1 - 4) and chest x-ray showed cardiomegaly with left ventricular type apex and pulmonary oligemia (globular box-shaped heart) (Figure 5).
Case Report
A 57-year old previously healthy man presented with complaint of
Journal of The Association of Physicians of India ■ Vol. 64 ■ February 2016 75
t o r e - e n t r a n t s u p r a v e n t r i c u l a r tachycardia in about one-third of patients. Risk factors believed to be associated with the condition are a family history of Ebstein’s anomaly or other congenital heart disease, nor thern European ances t ry and maternal exposure to benzodiazepines or lithium. More than 30% of patients with Ebstein’s anomaly have associated cardiac defects.
The c l in ica l mani fes ta t ions o f Ebstein’s anomaly depend on the degree of tricuspid valve malformation and consequent regurgitation, and any associated cardiac defects. Many
patients first experience symptoms as adults, but the onset can occur after birth or in infancy or childhood. In adults, the anomaly commonly presents with arrhythmia.
R e e n t r a n t s u p r a v e n t r i c u l a r tachycardia, atrial fibrillation, atrial f lutter and junctional tachycardia occur in 25% to 30% of patient1,2 and preexcitation caused by right-sided accessory pathways occurs in 5% to 25% of ECG.2
As our case Day 1 ECG (Figure 1) showed regular narrow complex tachycardia with no visible P wave with ventricular rate 280/min suggestive of AVNRT and day 3 (Figure 3) ECG show regular narrow complex tachycardia with no visible P wave with ventricular rate 240/min suggestive of AVNRT and Day 2 (Figure 2) ECG showed irregular narrow complex tachycardia with no visible P wave with ventricular rate 120/min suggestive of atrial fibrillation. In a study by Yu et al,3 PSVT is present in 10.4% and atrial tachyarrhythmia is present in 13.8% of the adult patient with Ebstein’s anomaly. In another study by Fause et al 4 showed SVT present in 48.6% and AF/AFL present in 20.8% of adult patients with Ebstein’s anomaly.
In 75% to 95% of cases, the QRS complex is characterized by a right conduction defect of right bundle branch type.
As in our case, Day 1 to Day 4 ECG (Figures 1-4) show RBBB (R’R pattern in V1-V4). In study by Yu et al,2 RBBB was present in 65.3% patients . In another study by Fause et al,4 RBBB
Fig. 3: Day 3 ECG showing regular narrow complex tachycardia with no visible P wave with ventricular rate 240/min suggestive of AVNRT. Right axis deviation, RVH, R’R pattern in v1-v4 (RBBB).
Fig. 4: Day 4 EGC showing regular rhythm with ventricular rate 64/min. Right axis deviation, RVH, R’R pattern in v1-v3 (RBBB) with biphasic P wave in v1 suggestive right atrial overload.
Fig. 5: Chest X-ray RA view: Globular box-shaped heart with right-sided enlargement with left ventricular type apex with pulmonary oligemia
Fig. 6: Apical displacement 15 mm/m of septal leaflet of tricuspid valve with right atrial enlargement
Fig. 7: Low pressure TR (RVSP=31.2 mmHg)
Fig. 8: Low pressure gradient

Journal of The Association of Physicians of India ■ Vol. 64 ■ February 201676
was present in 68.1% patients. WPW preexcitation occurs in 5% to 25% of the electrocardiograms in Ebstein’s anomaly.
At r i a l a r r h y t h m i a s w i t h o u t evidence of pre-excitat ion can be treated pharmacologically, whereas percutaneous radiofrequency ablation is indicated in the presence of an accessory pathway. In general, surgical intervention with tricuspid valve repair or replacement is restricted to patients with severe heart failure, cyanosis, intractable arrhythmias or paradoxical embolization (passage of thrombi from the venous circulation into the arterial circulation through a right-to-left shunt at the atrial level). Patients with
Ebstein’s anomaly should be assessed regularly for signs of deterioration in functional capacity, increasing cyanosis or presence of arrhythmia. Prophylaxis aga ins t in fec t ive endocard i t i s i s warranted in all cases.
In conclusion, there is increase in survival of adult congenital heart d i s e a s e d u e t o va s t p r o g r e s s i n congenital cardiac surgery, so this type of cases may be seen more and more in rout ine c l inical pract ice . Presentation with various types of arrhythmias in adult patients with m i n i m a l s y m p t o m a n d p h y s i c a l f indings needs further evaluation by echocardiography because these findings may be manifestation of a
congenital heart disease in adult as in our case.
References1. Kastor JA, Goldreyer BN, Josephson ME, et al.
Electrophysiologic characteristics of Ebstein’s anomaly of the tricuspid valve. Circulation 1975; 52:987–995.
2. Smith WM, G al lagher JJ , Kerr CR, et a l . The electrophysiologic basis and management of symptomatic recurrent tachycardia in patients with Ebstein’s anomaly of the tricuspid valve. Am J Cardiol 1982; 49:1223–1234.
3. Yu H, Pi-hua F, Hao-jie L, et al. Clinical analysis of arrhythmia in 297 Ebstein’s anomaly patients. Chinese Med J 2012; 125:3587-3588
4. Attie, Fause, Rosas, Martin, Rijlaarsdam, Maria, Buendia, Alfonso, Zabal, Carlos, Kuri, Jorge, Granados, Nuria The Adult Patient with Ebstein Anomaly: Outcome in 72 Unoperated Patients 2000; 79:27-36.