Exercise-induced bronchoconstriction
Suvanee Charoenlap, M.D.
Outline
• Introduction and definition
• Clinical presentation
• Pathogenesis
• Prevalence and risk factors
• Diagnosis and treatment
Introduction
• First described
: 150 A.D. by Aretaeus of Cappodocia
• First observed among asthma persons
: Exercise-induced asthma (EIA)
• Post-exercise asthma like symptoms in persons without asthma
: Exercise-induced bronchoconstriction (EIB)
AHRQ Publication No. 10-E001 ,January 2010 (Web site posting) ,Revised March 2010
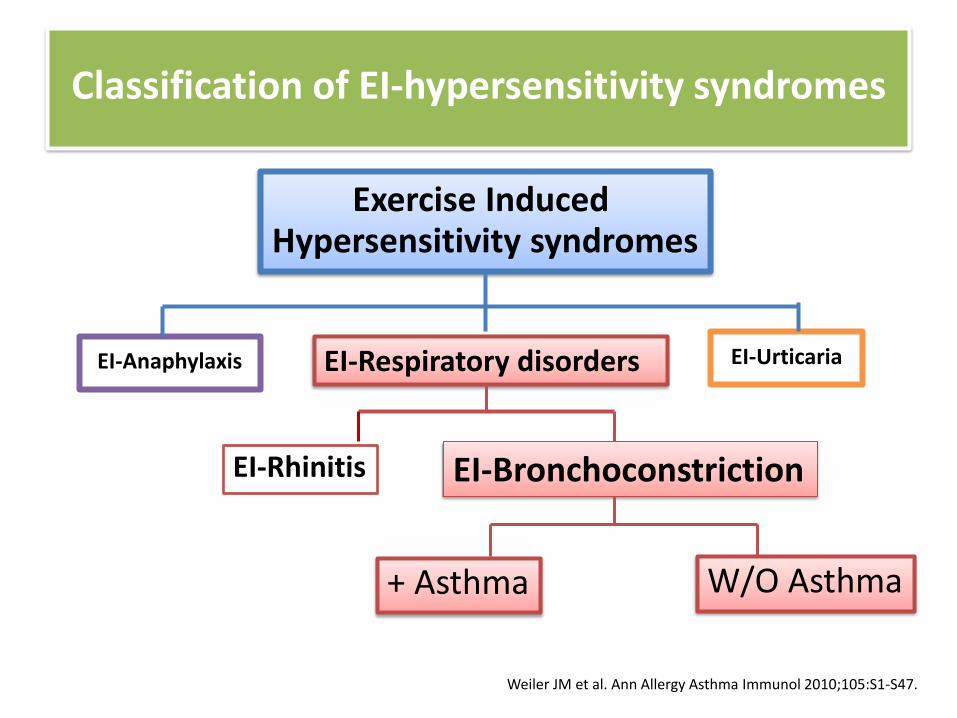
Classification of EI-hypersensitivity syndromes
Exercise Induced Hypersensitivity syndromes
EI-Respiratory disorders
EI-Bronchoconstriction EI-Rhinitis
EI-Anaphylaxis EI-Urticaria
+ Asthma W/O Asthma
Weiler JM et al. Ann Allergy Asthma Immunol 2010;105:S1-S47.
Definition of Exercise-induced bronchoconstriction (EIB)
• “Transient, reversible narrowing of the lower airways that occurs after vigorous exercise.”
– EIB with chronic asthma based on spirometry
– EIB without chronic asthma
• EIA: not used
“Exercise not induce asthma but rather a trigger of bronchoconstriction.”
Weiler JM et al. Ann Allergy Asthma Immunol 2010;105:S1-S47.
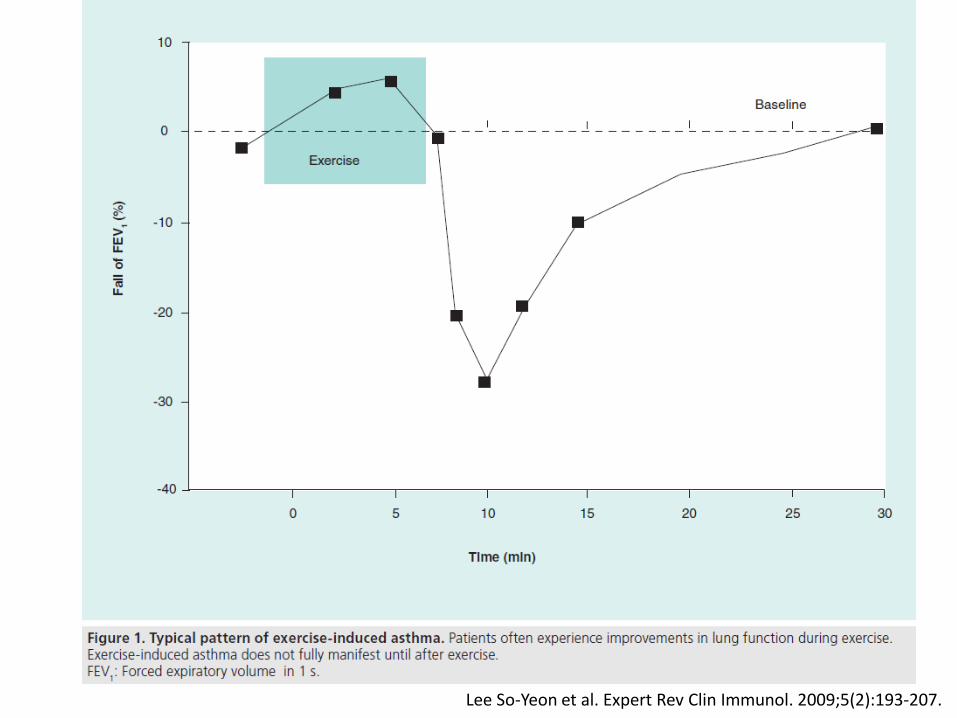
Clinical presentation
Clinical presentation
• The hallmark of EIB
– Acute airflow obstruction (measured FEV1)
– Peak rapidly 3-15 minutes after exercise stop
– Remits spontaneously within 20 – 40 min
(recovery time not prolonged)
AHRQ Publication No. 10-E001 ,January 2010 (Web site posting) ,Revised March 2010
• ATYPICAL presentation
– Appear during prolonged exercise and recovery time often prolonged
– Late-phase constriction:
• 4 -12 hours after exercise
• Generally less severe
• No predictors and not consistent in the same individual
AHRQ Publication No. 10-E001 ,January 2010 (Web site posting) ,Revised March 2010
Clinical presentation
Clinical symptoms in children
Most common
• Cough
• Wheezing
• Chest tightness
• Shortness of breath
• Excess mucus
Non-specific
• Poor performance
• Chest pain
• Prolonged upper respiratory illness
• Avoidance of activity
• Inability to keep up with peers
Lee So-Yeon et al, Expert Rev Clin Immunol.2009;5(2):193-207
Self reported symptoms do not significantly correlate with EIB diagnosis
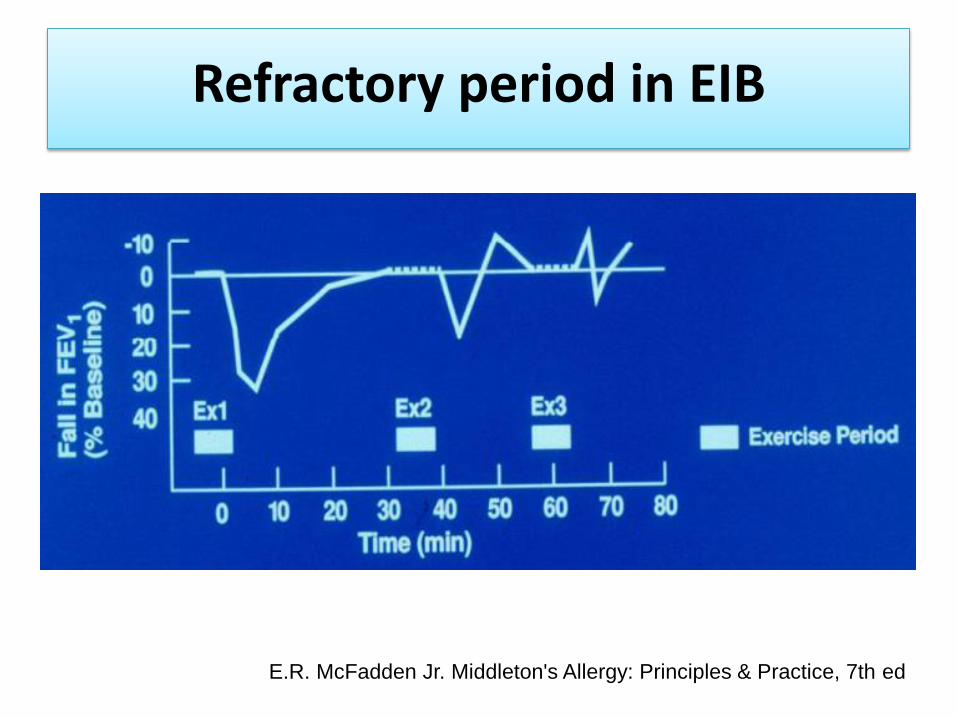
Refractory period in EIB
“A period of diminished responsiveness when
a second period of exercise follows in 1 to 4 hours.”
• 40-50% of EIB have refractory period.
• Mechanism not fully understood
– Bronchial smooth muscle tolerant to mediators
– Depletion of catecholamines
– Increased circulation of prostaglandin
– Degranulation of mast cell mediators
– PGE2 may be the important mediator in refractory period AHRQ Publication No. 10-E001 ,January 2010 (Web site posting) ,Revised March 2010
Refractory period in EIB
E.R. McFadden Jr. Middleton's Allergy: Principles & Practice, 7th ed
Pathogenesis
• Thermal theory
• Osmotic theory
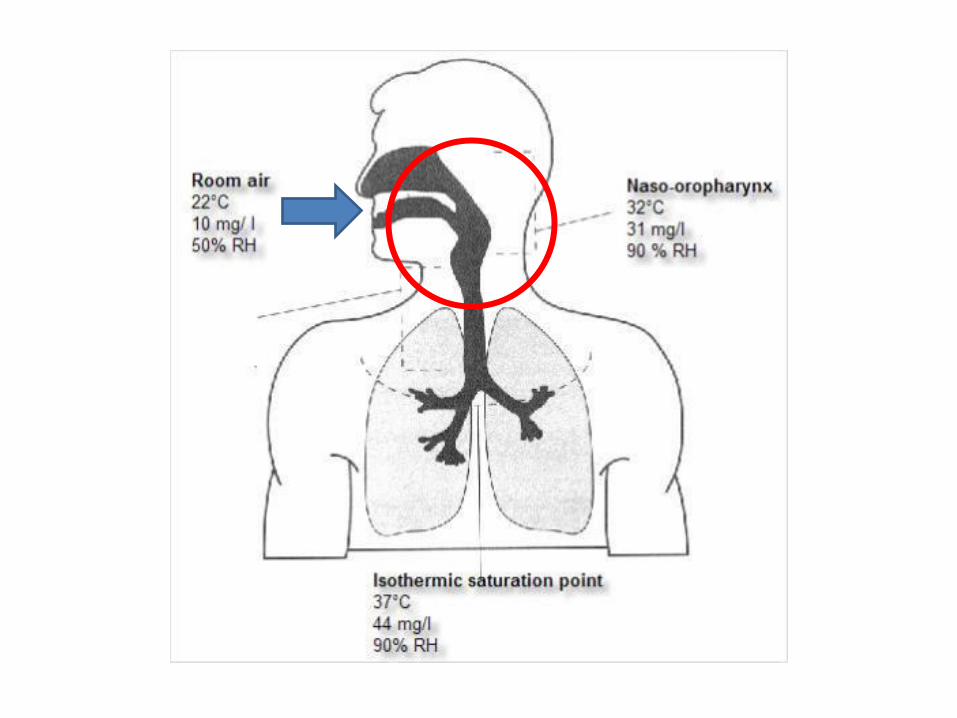
Pathophysiologic mechanism of EIB
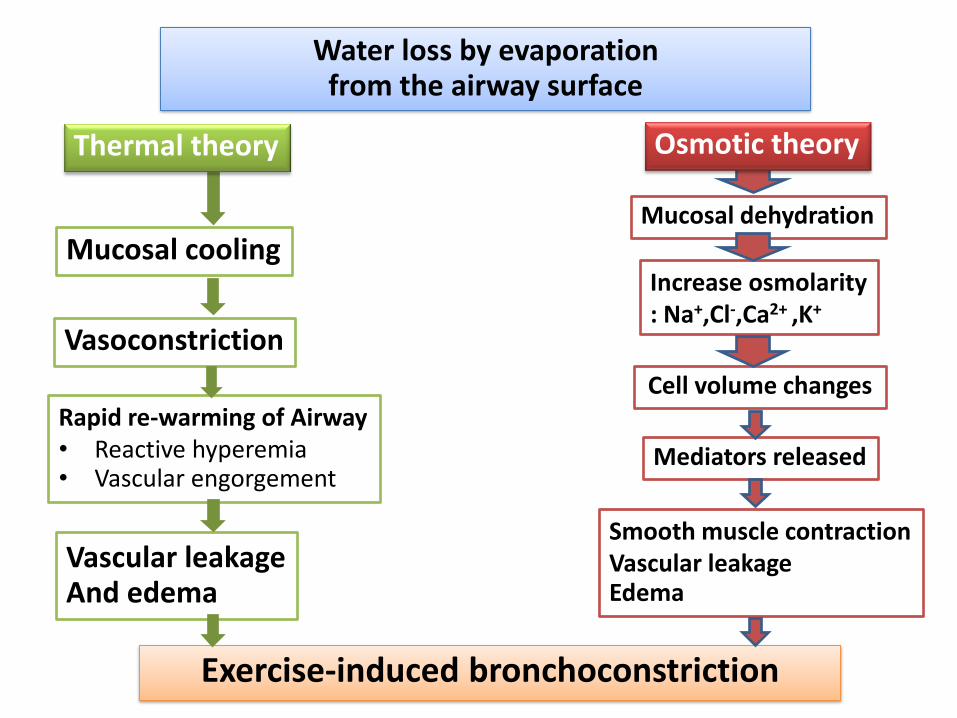
Water loss by evaporation from the airway surface
Mucosal dehydration
Increase osmolarity : Na+,Cl-,Ca2+ ,K+
Cell volume changes
Mediators released
Smooth muscle contraction Vascular leakage Edema
Mucosal cooling
Vasoconstriction
Rapid re-warming of Airway • Reactive hyperemia • Vascular engorgement
Vascular leakage And edema
Exercise-induced bronchoconstriction
Thermal theory Osmotic theory
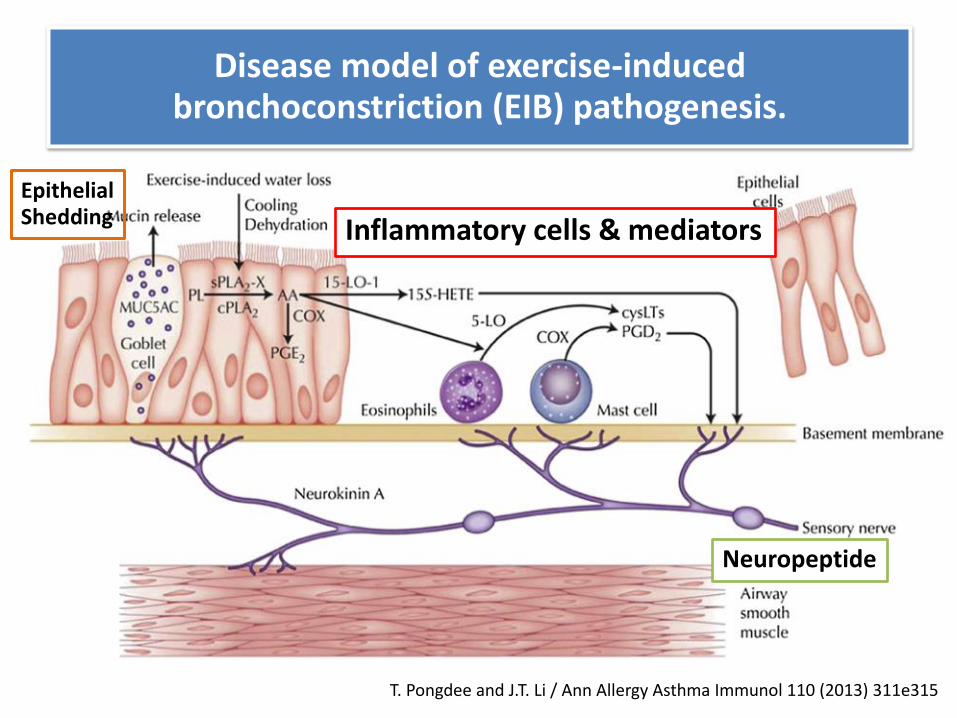
Disease model of exercise-induced bronchoconstriction (EIB) pathogenesis.
T. Pongdee and J.T. Li / Ann Allergy Asthma Immunol 110 (2013) 311e315
Inflammatory cells & mediators
Neuropeptide
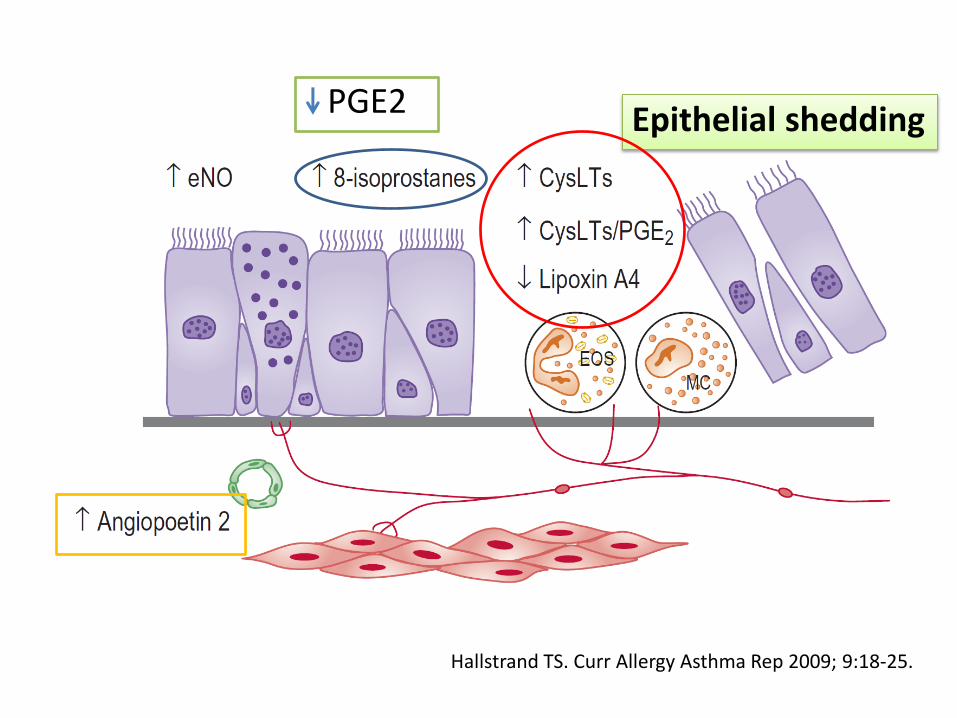
Epithelial Shedding
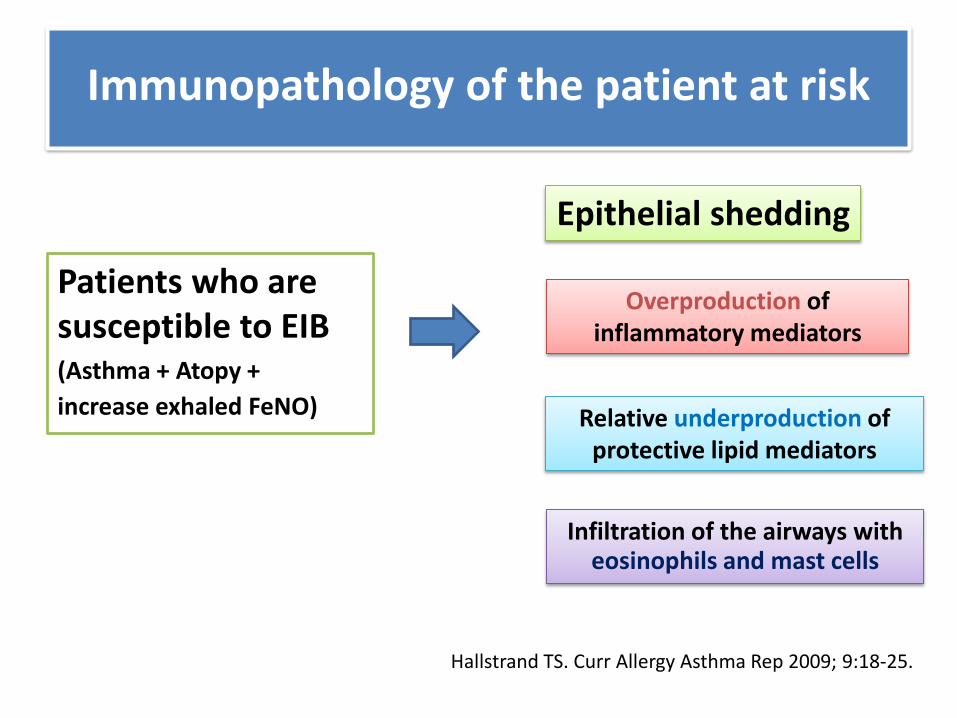
Patients who are susceptible to EIB (Asthma + Atopy +
increase exhaled FeNO)
Immunopathology of the patient at risk
Epithelial shedding
Overproduction of inflammatory mediators
Relative underproduction of protective lipid mediators
Infiltration of the airways with eosinophils and mast cells
Hallstrand TS. Curr Allergy Asthma Rep 2009; 9:18-25.
Hallstrand TS. Curr Allergy Asthma Rep 2009; 9:18-25.
Epithelial shedding PGE2
Hallstrand TS. Curr Allergy Asthma Rep 2009; 9:18-25.
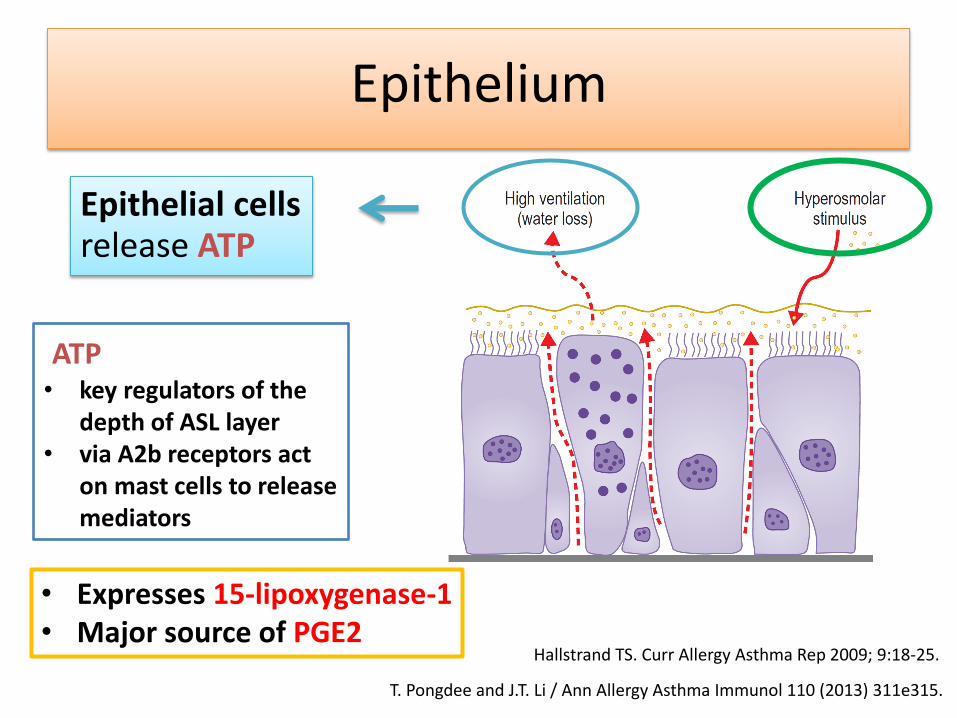
Epithelial cells release ATP
ATP • key regulators of the
depth of ASL layer • via A2b receptors act
on mast cells to release mediators
• Expresses 15-lipoxygenase-1 • Major source of PGE2
T. Pongdee and J.T. Li / Ann Allergy Asthma Immunol 110 (2013) 311e315.
Epithelium
Mast cell & Eosinophil
• Mast cells
: PGD2, LTs, histamine
• Eosinophils
: LTs, Eosinophilic cationic protein (ECP)
T. Pongdee and J.T. Li / Ann Allergy Asthma Immunol 110 (2013) 311e315
Sensory nerve
• Eicosanoids (CysLTs) activated sensory nerves release : Neurokinins
bronchoconstriction , mucous release
• Mucin 5AC (MUC5AC) increase in airway
: predominant gel-forming mucin of goblet cells
T. Pongdee and J.T. Li / Ann Allergy Asthma Immunol 110 (2013) 311e315

Inflammatory mediator release
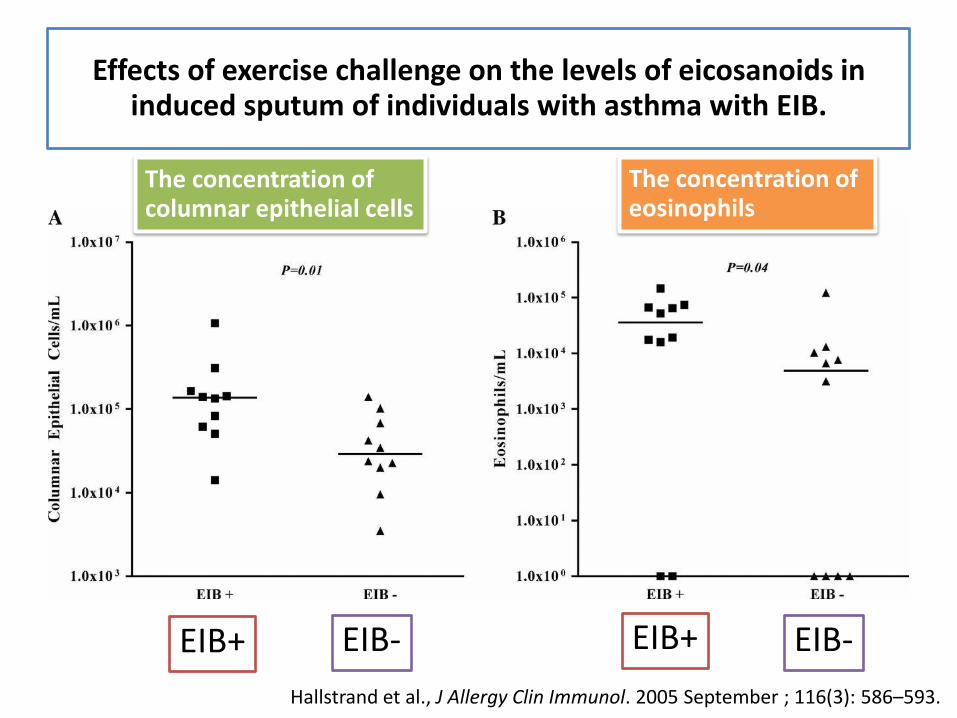
The concentration of columnar epithelial cells
The concentration of eosinophils
EIB+ EIB+ EIB- EIB- Hallstrand et al., J Allergy Clin Immunol. 2005 September ; 116(3): 586–593.
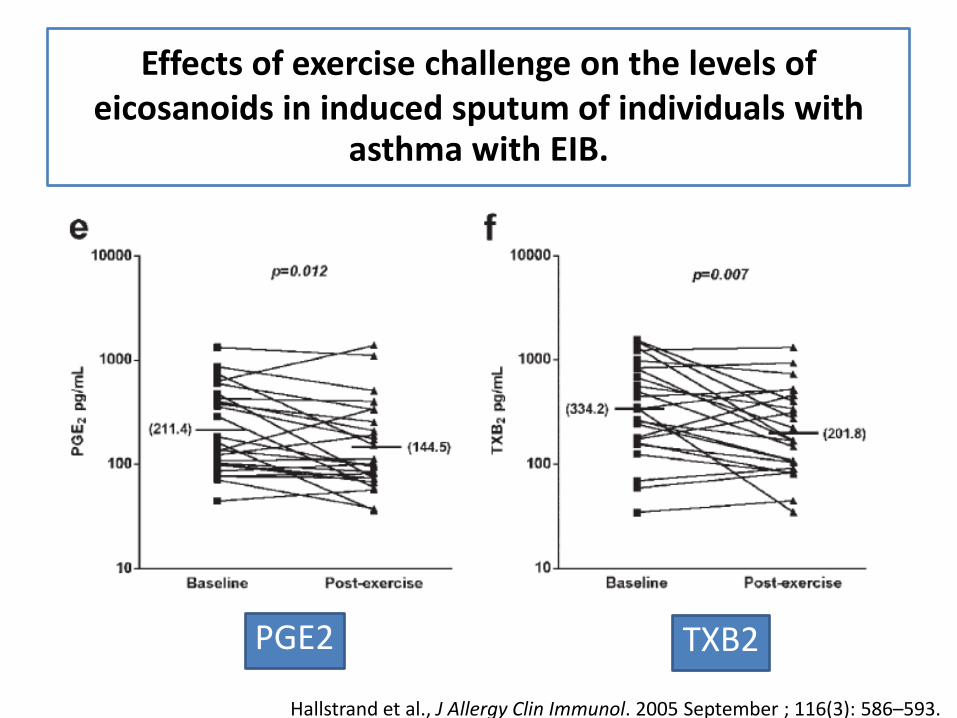
Effects of exercise challenge on the levels of eicosanoids in induced sputum of individuals with asthma with EIB.
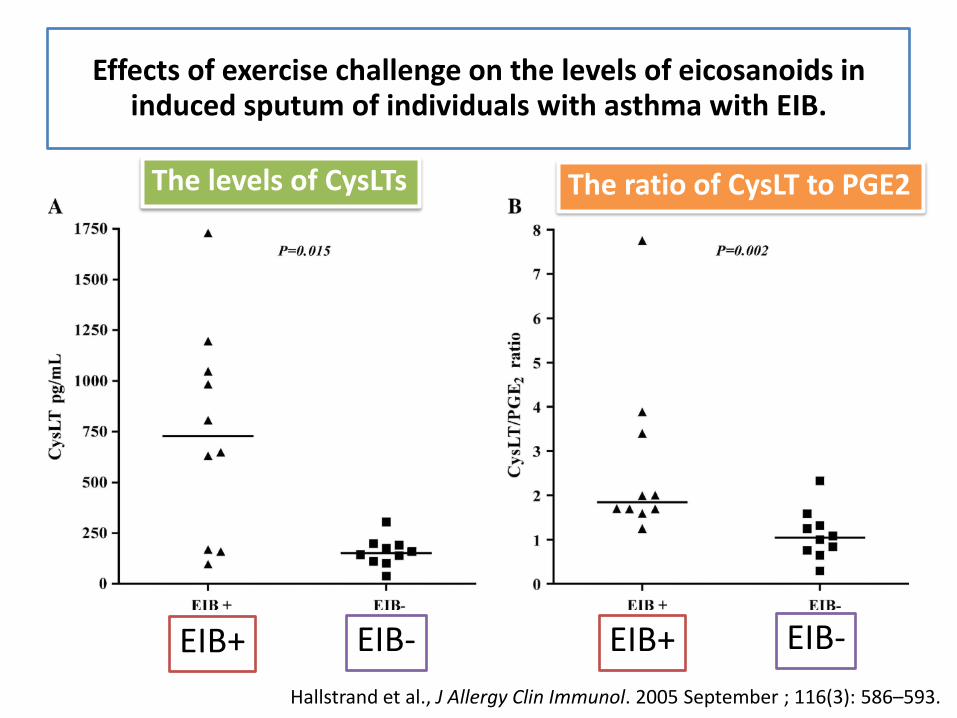
EIB+ EIB+ EIB- EIB-
The levels of CysLTs The ratio of CysLT to PGE2
Hallstrand et al., J Allergy Clin Immunol. 2005 September ; 116(3): 586–593.
Effects of exercise challenge on the levels of eicosanoids in induced sputum of individuals with asthma with EIB.
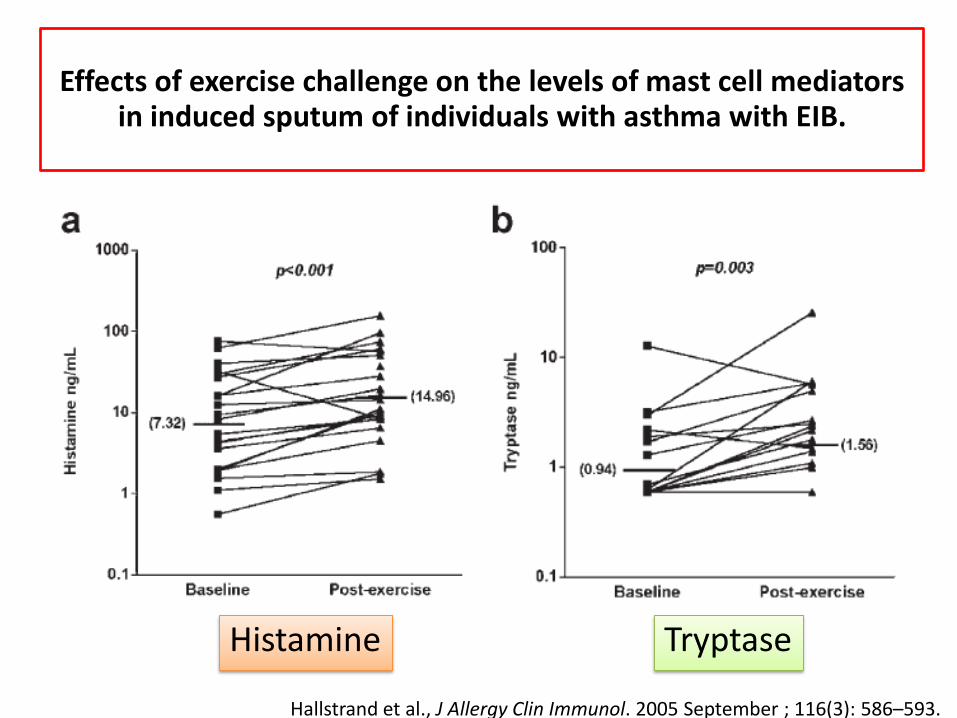
Effects of exercise challenge on the levels of mast cell mediators in induced sputum of individuals with asthma with EIB.
Histamine Tryptase
Hallstrand et al., J Allergy Clin Immunol. 2005 September ; 116(3): 586–593.
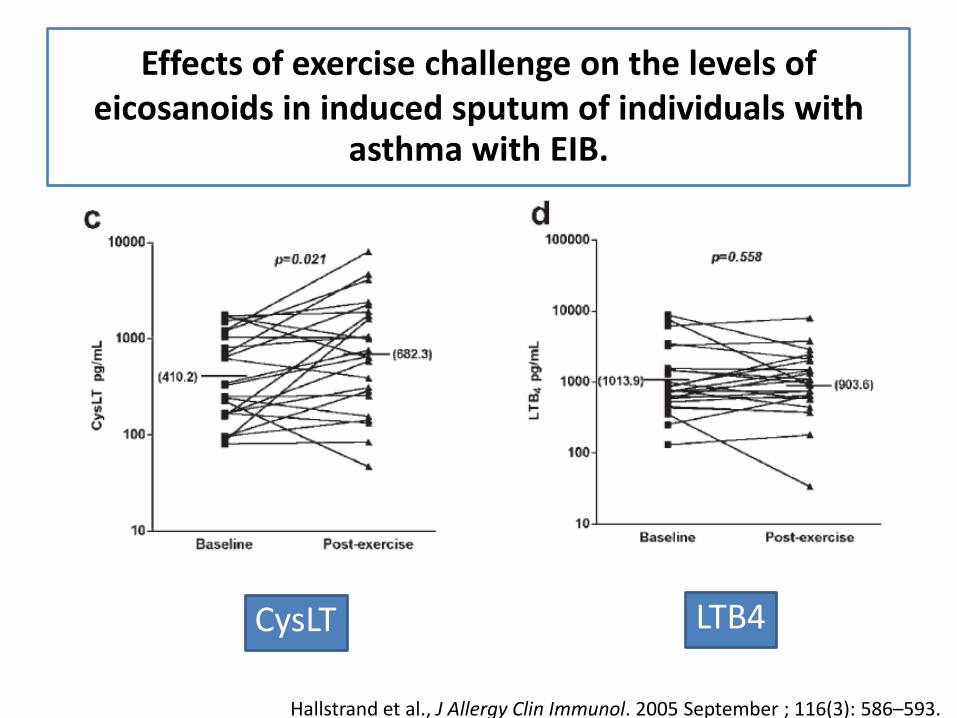
Effects of exercise challenge on the levels of eicosanoids in induced sputum of individuals with
asthma with EIB.
CysLT LTB4
Hallstrand et al., J Allergy Clin Immunol. 2005 September ; 116(3): 586–593.
Effects of exercise challenge on the levels of eicosanoids in induced sputum of individuals with
asthma with EIB.
PGE2 TXB2
Hallstrand et al., J Allergy Clin Immunol. 2005 September ; 116(3): 586–593.
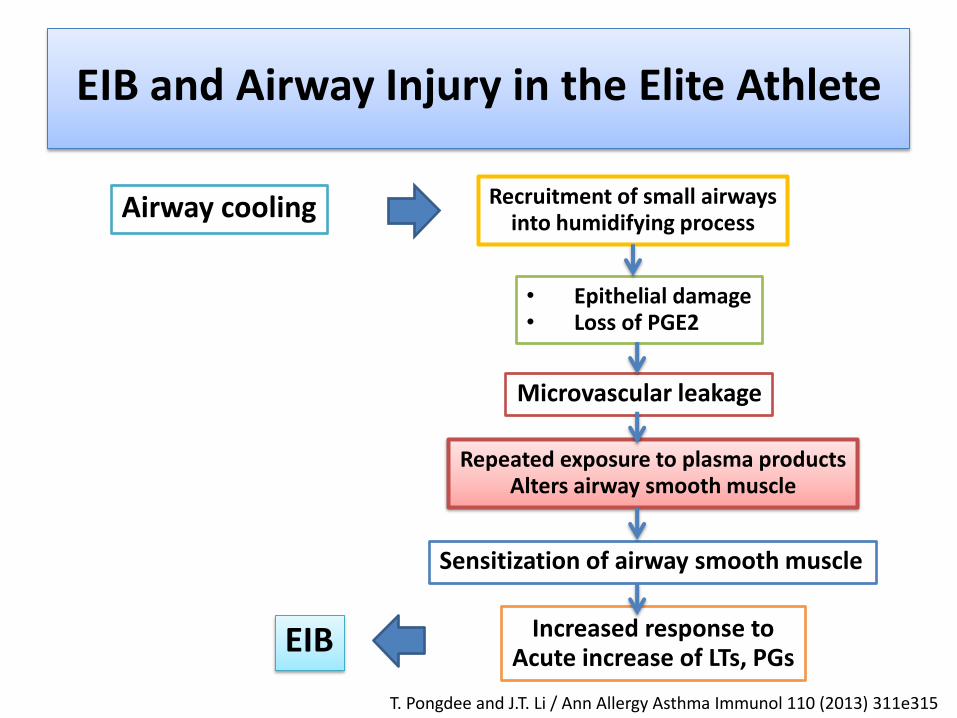
EIB and Airway Injury in the Elite Athlete
Airway cooling Recruitment of small airways into humidifying process
• Epithelial damage • Loss of PGE2
Microvascular leakage
Repeated exposure to plasma products Alters airway smooth muscle
Sensitization of airway smooth muscle
Increased response to Acute increase of LTs, PGs EIB
T. Pongdee and J.T. Li / Ann Allergy Asthma Immunol 110 (2013) 311e315
Prevalence of EIB
• 7 – 20% in general population
• Up to 50% in competitive athletes
• EIB is reported to occur in
– up to 90% of individuals with asthma
– 40% of those with allergic rhinitis
Prevalence of EIB
T. Pongdee and J.T. Li. Ann Allergy Asthma Immunol 2013;110: 311-315
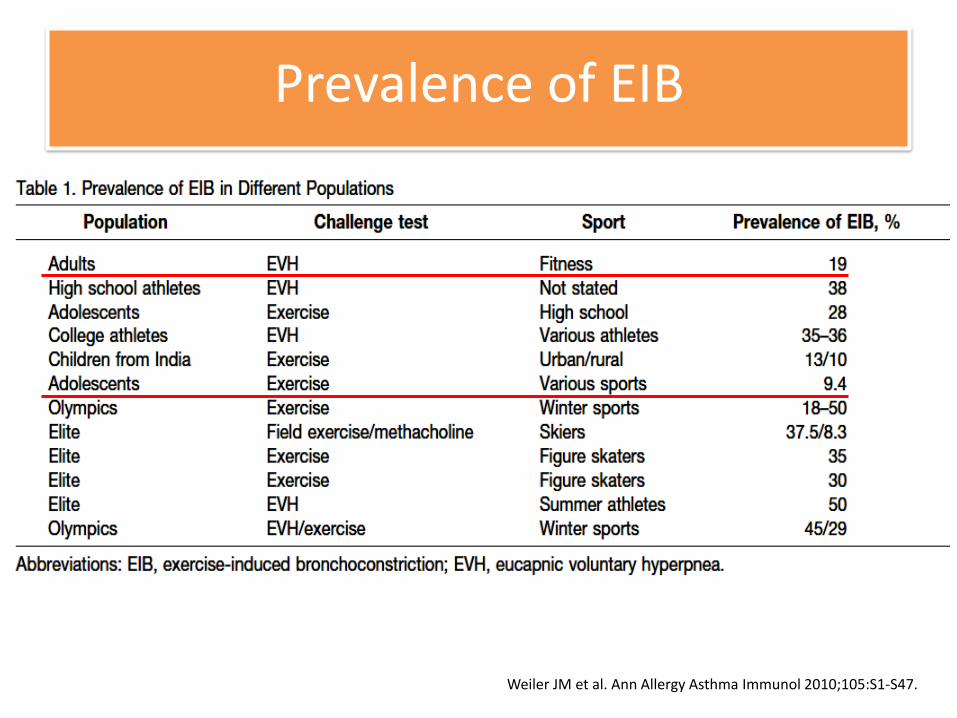
Prevalence of EIB
Weiler JM et al. Ann Allergy Asthma Immunol 2010;105:S1-S47.
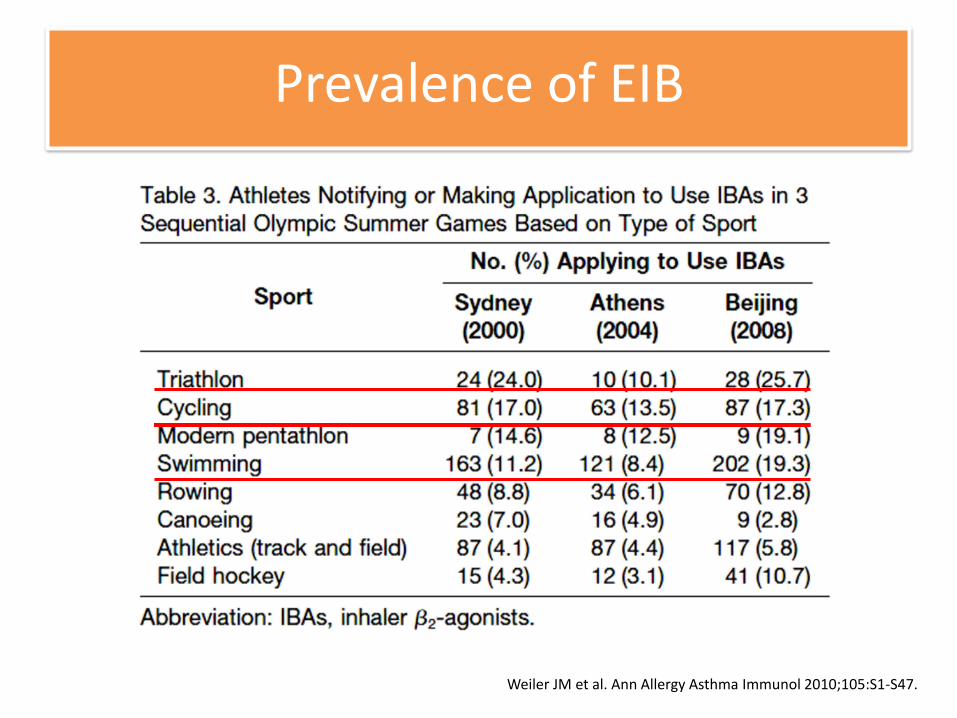
Prevalence of EIB
Weiler JM et al. Ann Allergy Asthma Immunol 2010;105:S1-S47.
• 56 asthmatic children, 6-15 years old
• Criteria : 15% reduction in PEFR or having wheezing during exercise-challenge test was considered as having EIB.
• Prevalence of EIB was 41% (n=23)
– 16/23 (69.5 %) had EIB history
– 7/23 (30.4%) had no EIB history
• EIB history (p=0.021) and family history of asthma (p=0.04) correlated with EIB.
EXERCISE‐INDUCED BRONCHOCONSTRICTION IN THAI PEDIATRIC ASTHMA
Yimsuwan U, et al. JACI, Vol 219, Page AB3, Feb 2012
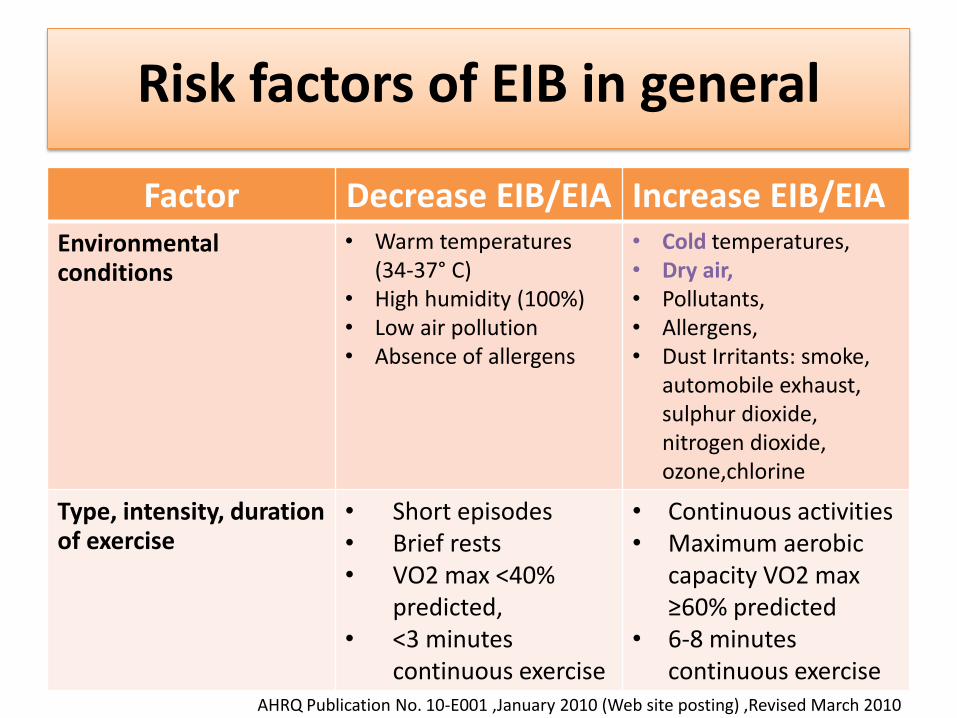
Risk factors of EIB in general
Factor Decrease EIB/EIA Increase EIB/EIA Environmental conditions
• Warm temperatures (34-37° C)
• High humidity (100%) • Low air pollution • Absence of allergens
• Cold temperatures, • Dry air, • Pollutants, • Allergens, • Dust Irritants: smoke,
automobile exhaust, sulphur dioxide, nitrogen dioxide, ozone,chlorine
Type, intensity, duration of exercise
• Short episodes • Brief rests • VO2 max <40%
predicted, • <3 minutes
continuous exercise
• Continuous activities • Maximum aerobic
capacity VO2 max ≥60% predicted
• 6-8 minutes continuous exercise
AHRQ Publication No. 10-E001 ,January 2010 (Web site posting) ,Revised March 2010
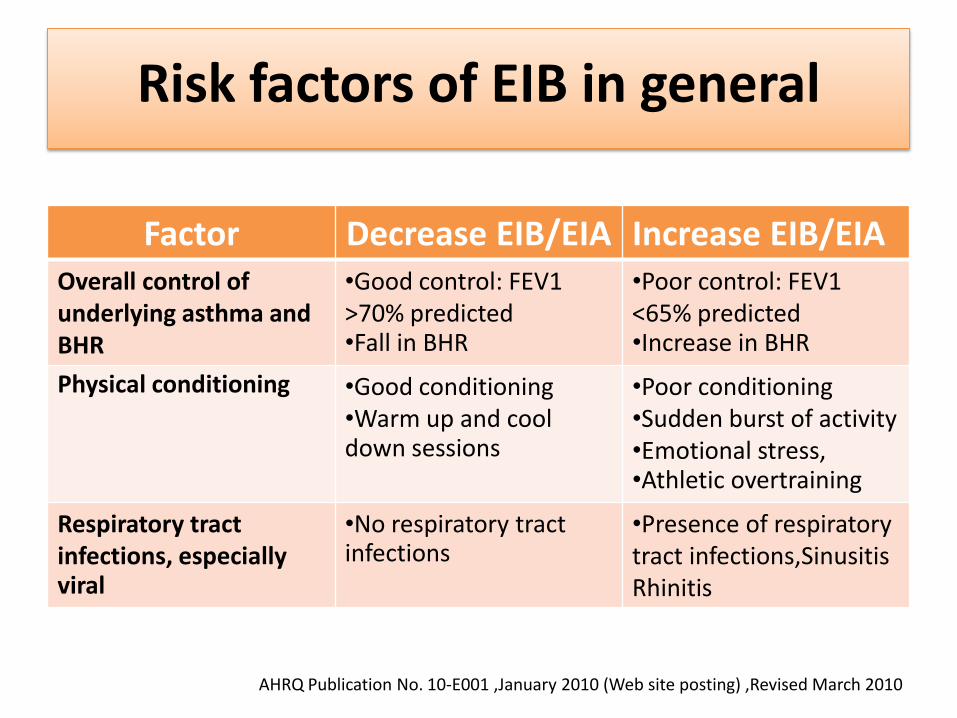
Risk factors of EIB in general
Factor Decrease EIB/EIA Increase EIB/EIA Overall control of underlying asthma and BHR
•Good control: FEV1 >70% predicted •Fall in BHR
•Poor control: FEV1 <65% predicted •Increase in BHR
Physical conditioning •Good conditioning •Warm up and cool down sessions
•Poor conditioning •Sudden burst of activity •Emotional stress, •Athletic overtraining
Respiratory tract infections, especially viral
•No respiratory tract infections
•Presence of respiratory tract infections,Sinusitis Rhinitis
AHRQ Publication No. 10-E001 ,January 2010 (Web site posting) ,Revised March 2010
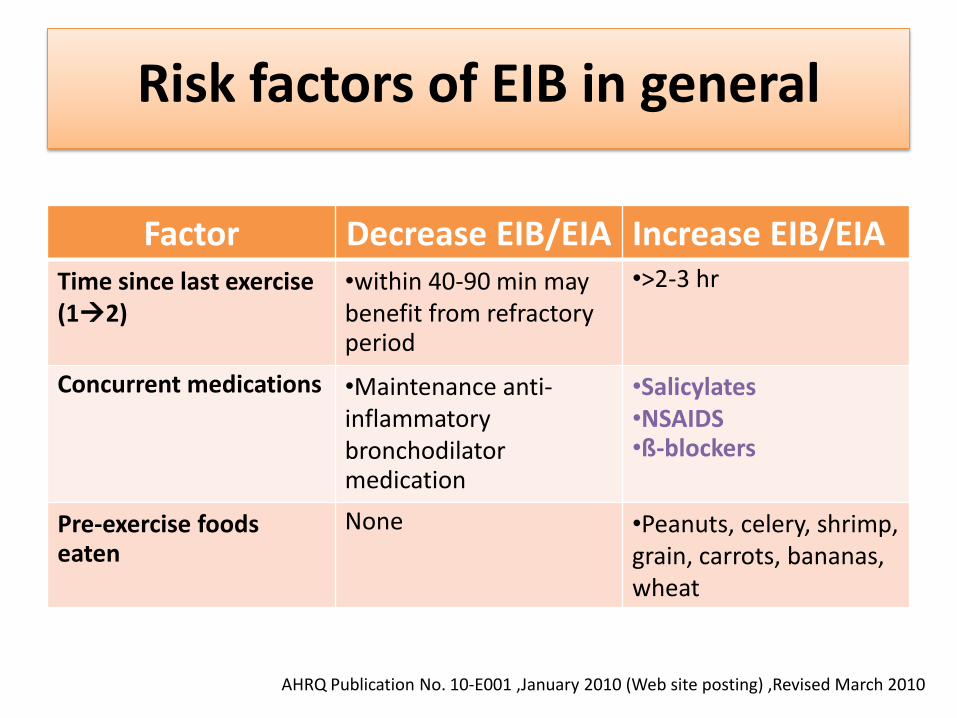
Risk factors of EIB in general
Factor Decrease EIB/EIA Increase EIB/EIA Time since last exercise (12)
•within 40-90 min may benefit from refractory period
•>2-3 hr
Concurrent medications •Maintenance anti-inflammatory bronchodilator medication
•Salicylates •NSAIDS •ß-blockers
Pre-exercise foods eaten
None
•Peanuts, celery, shrimp, grain, carrots, bananas, wheat
AHRQ Publication No. 10-E001 ,January 2010 (Web site posting) ,Revised March 2010

Diagnosis and treatment
Step for evaluation suspected EIB +/- asthma
• History
• Physical examination
• Pulmonary function test (pre/post bronchodilator)
• Diagnostic challenges
• Try treatment of EIB +/- asthma
• Further investigations
History suggest EIB
• Common clinical symptoms :
– coughing, wheezing, shortness of breath, excessive mucus production, chest tightness, chest pain prolonged recovery time following exercise
• Less common clinical symptoms:
– stomach pain, nausea and near-death experiences
• Symptoms relieved or prevented by SABA/LABA
AHRQ Publication No. 10-E001 ,January 2010 (Web site posting) ,Revised March 2010
Physical examination
• Asthma
– Co-morbid allergic disease: AR,AD
• Non-asthma
– Chronic lung disease
– Cardiovascular disease
– Obesity
– Etc.
Weiler JM et al. Ann Allergy Asthma Immunol 2010;105:S1-S47.
Pulmonary function test
FEV1 <70%
• Suspected asthma
• Try treat with ICS/ LTRA
• SABA as needed
• Avoid triggers
• Repeat FEV1 after treatment – Improve: possible EIB with
asthma need objective testings
– NOT improve: other diseases
FEV1 >70%
• Suspected EIB without asthma
• Perform objective testings : one or more – Standardized ECT
– Eucapnic Voluntary Hyperventilation (EVH)
– Mannitol test
– Sport specific field challenge test
Weiler JM et al. Ann Allergy Asthma Immunol 2010;105:S1-S47.
Differential diagnosis and further investigations
Differential diagnosis
• Physiologic limitation
• VCD,EILD, EIH
• Anxiety hyperventilation syndrome
• Obesity related dyspnea
• Cardiac abnormality: IHSS, tachyarrythmia
• Pulmonary AVM.
• Other diagnosis
Further investigations
• EKG
• Echocardiogram
• Holter monitoring
• Chest x-ray
• CT, MRI
• Pulmonary exercise stress test
• Exercise rhinoscopy
• Laryngoscopy
Weiler JM et al. Ann Allergy Asthma Immunol 2010;105:S1-S47.
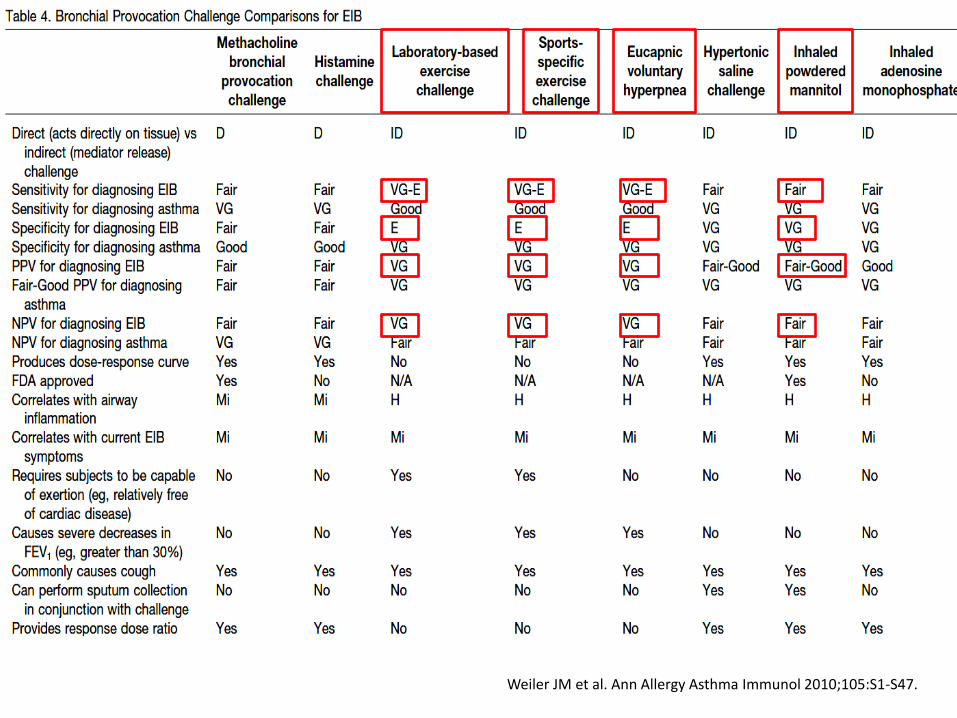
Diagnostic challenges
• Direct Challenges : Methacholine / Histamine
• Indirect Challenges :
– Exercise Challenge test (ECT)
– Surrogate
• Eucapnic Voluntary Hyperventilation (EVH)
• Inhalation of Mannitol, Adenosine monophosphate (AMP) or hypertonic saline (4.5%NaCl)
IOC-MC recommend for elite athlete suspected EIB
Weiler JM et al. Ann Allergy Asthma Immunol 2010;105:S1-S47.
Weiler JM et al. Ann Allergy Asthma Immunol 2010;105:S1-S47.
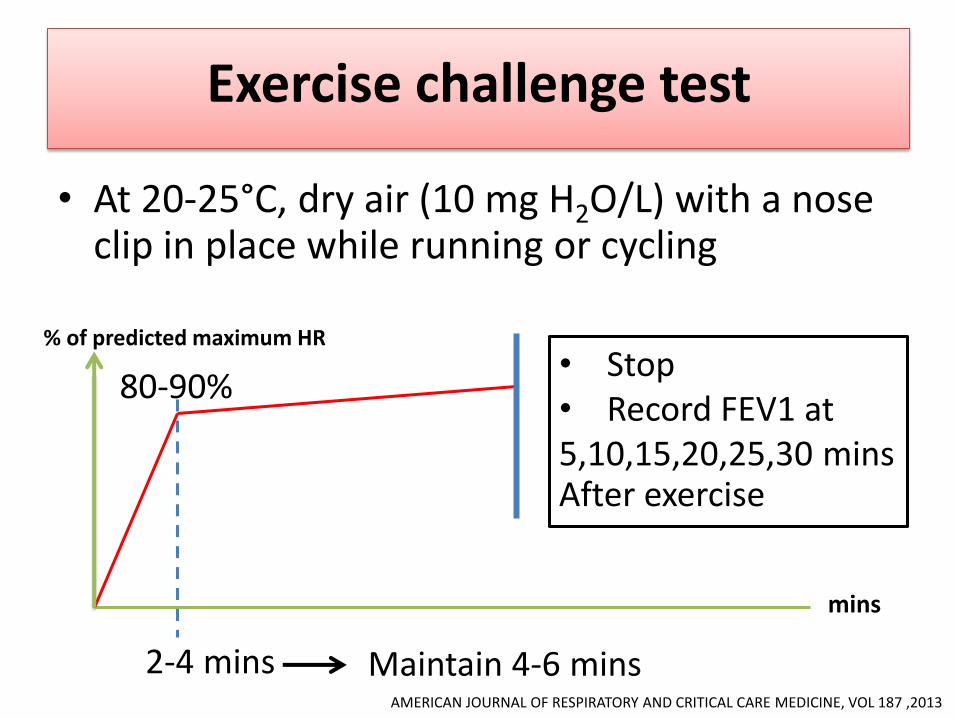
Exercise challenge test
• At 20-25°C, dry air (10 mg H2O/L) with a nose clip in place while running or cycling
% of predicted maximum HR
80-90%
mins
2-4 mins Maintain 4-6 mins
• Stop • Record FEV1 at 5,10,15,20,25,30 mins After exercise
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE, VOL 187 ,2013
Lee So-Yeon et al. Expert Rev Clin Immunol. 2009;5(2):193-207.
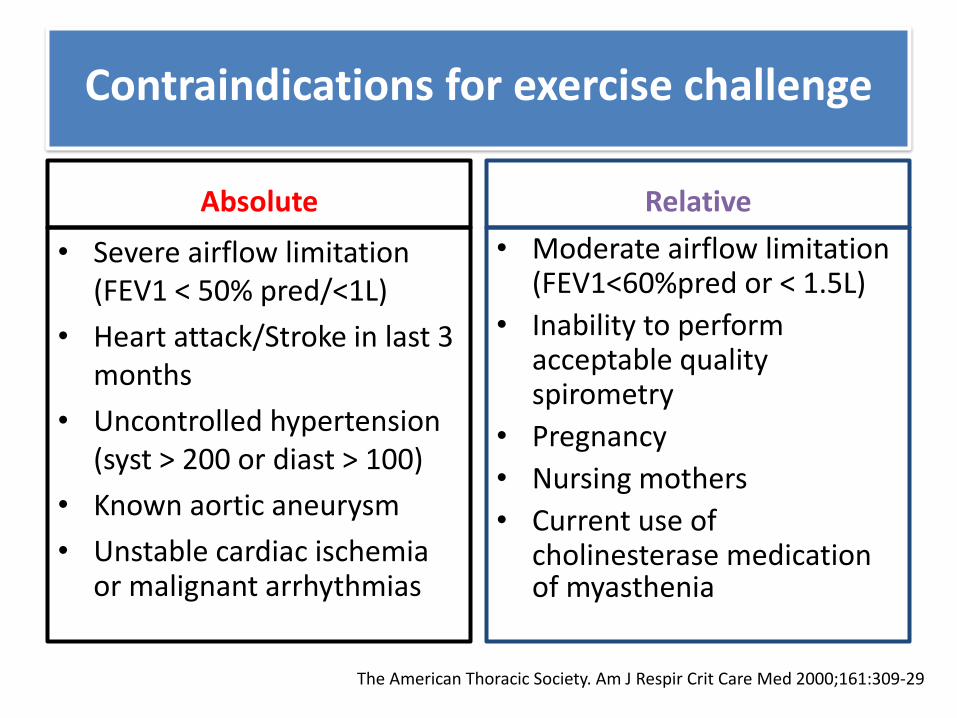
Contraindications for exercise challenge
Absolute
• Severe airflow limitation (FEV1 < 50% pred/<1L)
• Heart attack/Stroke in last 3 months
• Uncontrolled hypertension (syst > 200 or diast > 100)
• Known aortic aneurysm
• Unstable cardiac ischemia or malignant arrhythmias
Relative
• Moderate airflow limitation (FEV1<60%pred or < 1.5L)
• Inability to perform acceptable quality spirometry
• Pregnancy
• Nursing mothers
• Current use of cholinesterase medication of myasthenia
The American Thoracic Society. Am J Respir Crit Care Med 2000;161:309-29
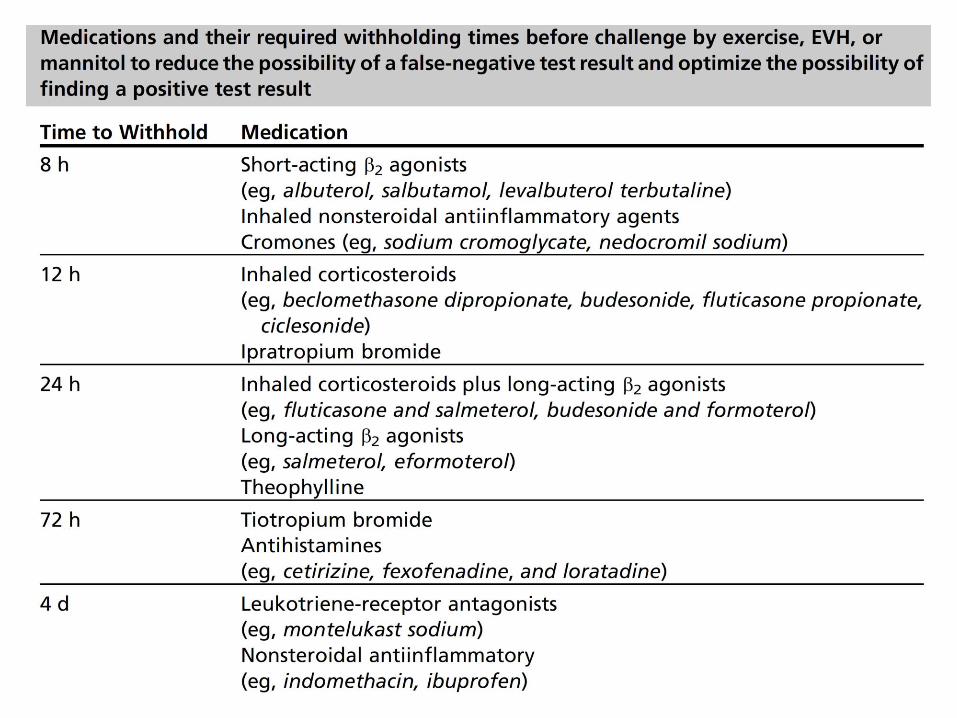
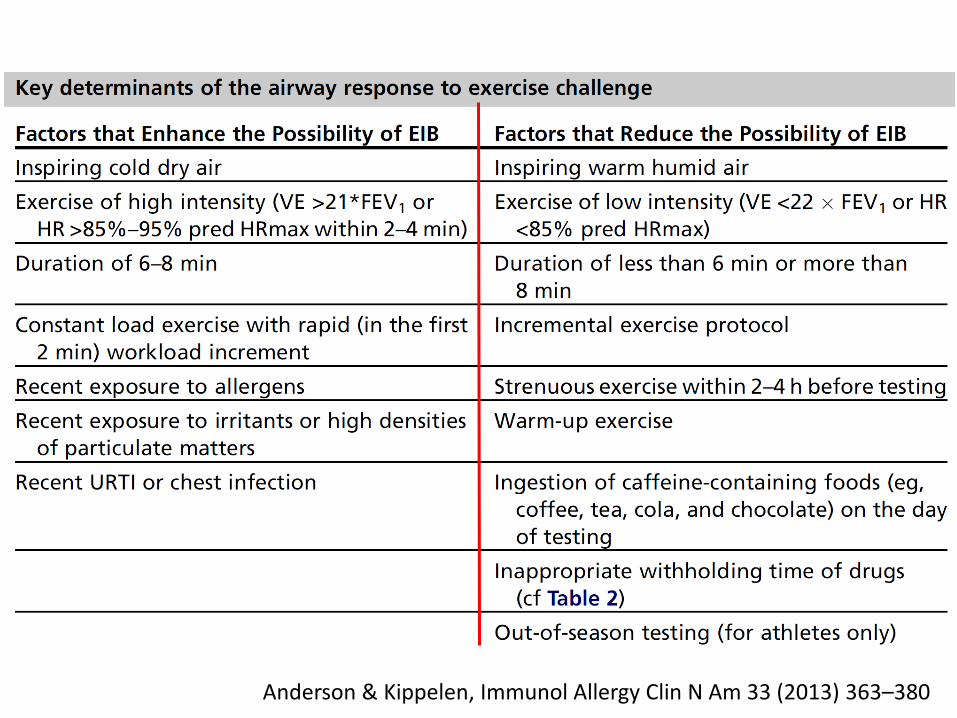
Anderson & Kippelen, Immunol Allergy Clin N Am 33 (2013) 363–380
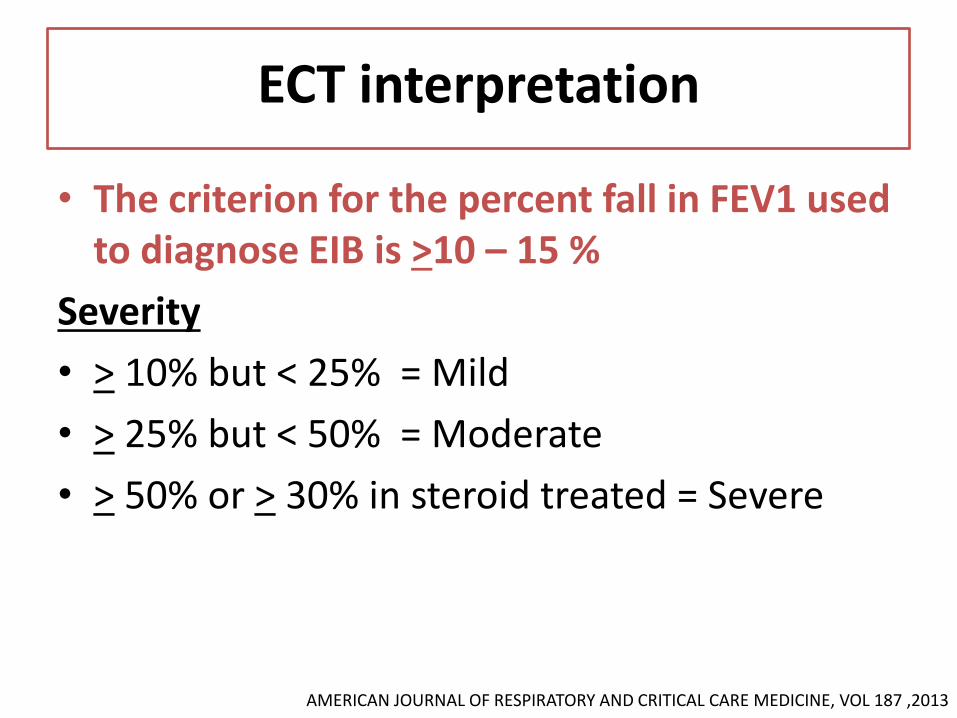
ECT interpretation
• The criterion for the percent fall in FEV1 used to diagnose EIB is >10 – 15 %
Severity
• > 10% but < 25% = Mild
• > 25% but < 50% = Moderate
• > 50% or > 30% in steroid treated = Severe
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE, VOL 187 ,2013
• High sensitivity to identify EIB
• IOC MC
: optimal test to identify EIB for athletes seeking approval to inhaled β2–agonist before an event
Eucapnic Voluntary Hyperventilation (EVH)
Rundell KW, Slee JB. J Allergy Clin Immunol 2008;122:238-46.
Eucapnic Voluntary Hyperventilation (EVH)
• Induced high ventilation level up to 110 L/min and maintain near normal alveolar CO2
• Protocol – Breathing dry air contained: 5%CO2 +21%O2
– Controlled ventilation rate: 60-85% of MVV* • MVV:max.voluntary ventilation
= 21-30 times of baseline FEV1
– Consistent ventilation for 6 min
– NOT perform in subject with FEV1< 70%
• The criterion for the percent fall in FEV1 used to diagnose EIB is >10 – 15 %
Weiler JM et al. Ann Allergy Asthma Immunol 2010;105:S1-S47.
Inhalation of Mannitol
• Produce hyperosmolar environment
• Protocol (Aridol approved by FDA 2010)
– Mannitol dry powder inhaler progressive doubling doses of 5,10,20,40,80,160,160 and 160mg with maximal total dose 635mg
– 1 min. after each dose, FEV1 measured
– +ve test: % fall in FEV1 >15 compare to baseline
: a between dose % fall in FEV1 >10
Weiler JM et al. Ann Allergy Asthma Immunol 2010;105:S1-S47.
Hypertonic saline challenge
Protocol
• Nebulize 4.5% hypertonic saline inhalation in 15-20 minutes
• Exposure time: 30 & 60 sec, 2 & 4 & 8 min
• FEV1 measurement: 1 min after every exposure
• < 10% fall in FEV1 doubled exposure time
• > 10% fall in FEV1 same exposure
• Termination: ≥ 15% fall in FEV1 or total minimum dose of 23 g (15.5 mins)
Sport specific exercise challenge test
1. Natural setting athlete’s sport in field exercise
2. Simulated condition in laboratory
• Important test in sports under special environment
– Winter sport
– Swimming sport
• Low sensitivity than EVH
Weiler JM et al. Ann Allergy Asthma Immunol 2010;105:S1-S47.

Treatment of EIB
• Pharmacological treatments
1. Therapies given before exercise
2. Long-term therapies
• Non-pharmacological treatments
Treatment of EIB
• Response rate: 30-60% of EIB with asthma
• Degree of efficacy
: variable(complete no effect)
• Practical use
– Combination of ICS with another agents to achieve control such as SABA, LABA, LTRA
– After controlled: step down to regular use of ICS alone
Inhale corticosteroid (ICS)
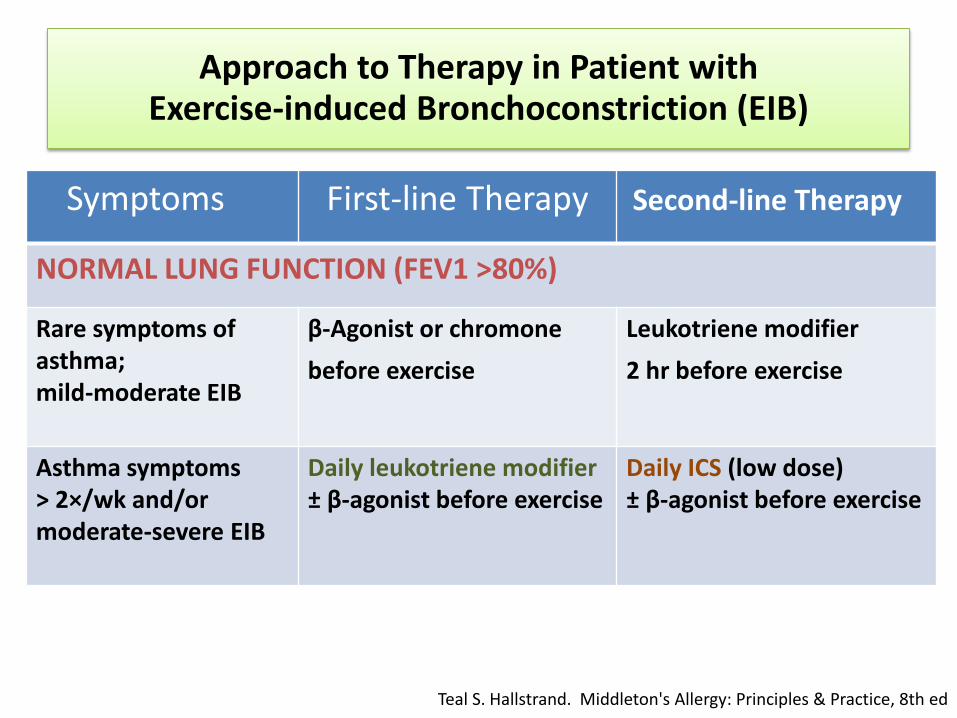
Symptoms First-line Therapy Second-line Therapy
NORMAL LUNG FUNCTION (FEV1 >80%)
Rare symptoms of asthma; mild-moderate EIB
β-Agonist or chromone
before exercise Leukotriene modifier
2 hr before exercise
Asthma symptoms > 2×/wk and/or moderate-severe EIB
Daily leukotriene modifier ± β-agonist before exercise
Daily ICS (low dose) ± β-agonist before exercise
Approach to Therapy in Patient with Exercise-induced Bronchoconstriction (EIB)
Teal S. Hallstrand. Middleton's Allergy: Principles & Practice, 8th ed
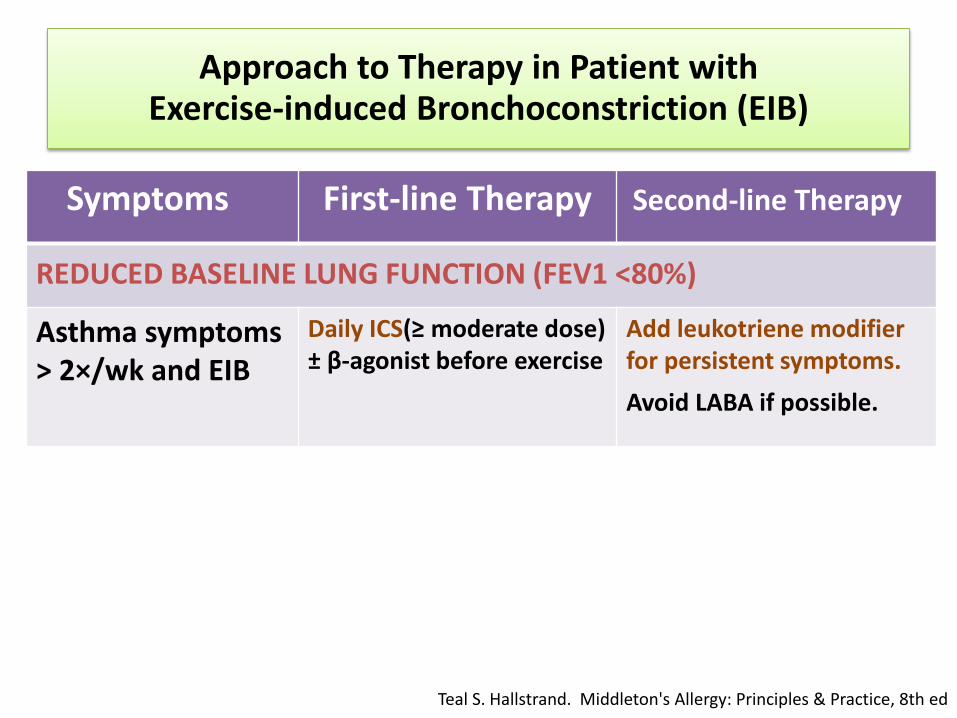
Symptoms First-line Therapy Second-line Therapy
REDUCED BASELINE LUNG FUNCTION (FEV1 <80%)
Asthma symptoms > 2×/wk and EIB
Daily ICS(≥ moderate dose) ± β-agonist before exercise
Add leukotriene modifier for persistent symptoms.
Avoid LABA if possible.
Approach to Therapy in Patient with Exercise-induced Bronchoconstriction (EIB)
Teal S. Hallstrand. Middleton's Allergy: Principles & Practice, 8th ed
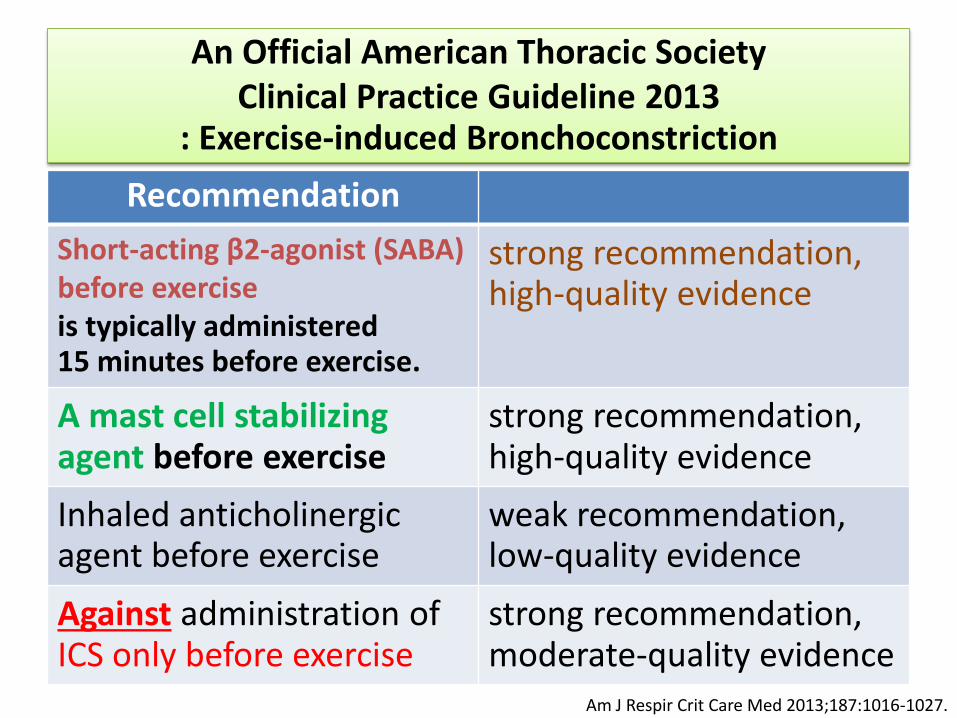
An Official American Thoracic Society Clinical Practice Guideline 2013
: Exercise-induced Bronchoconstriction
Recommendation
Short-acting β2-agonist (SABA) before exercise is typically administered 15 minutes before exercise.
strong recommendation, high-quality evidence
A mast cell stabilizing agent before exercise
strong recommendation, high-quality evidence
Inhaled anticholinergic agent before exercise
weak recommendation, low-quality evidence
Against administration of ICS only before exercise
strong recommendation, moderate-quality evidence
Am J Respir Crit Care Med 2013;187:1016-1027.
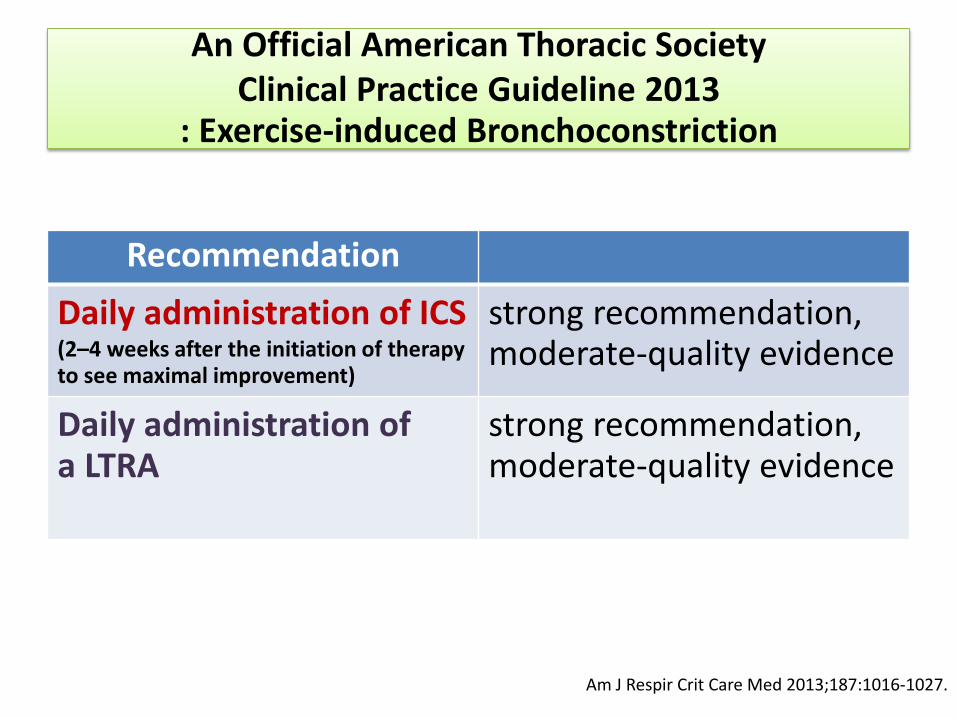
Recommendation
Daily administration of ICS (2–4 weeks after the initiation of therapy to see maximal improvement)
strong recommendation, moderate-quality evidence
Daily administration of a LTRA
strong recommendation, moderate-quality evidence
An Official American Thoracic Society Clinical Practice Guideline 2013
: Exercise-induced Bronchoconstriction
Am J Respir Crit Care Med 2013;187:1016-1027.
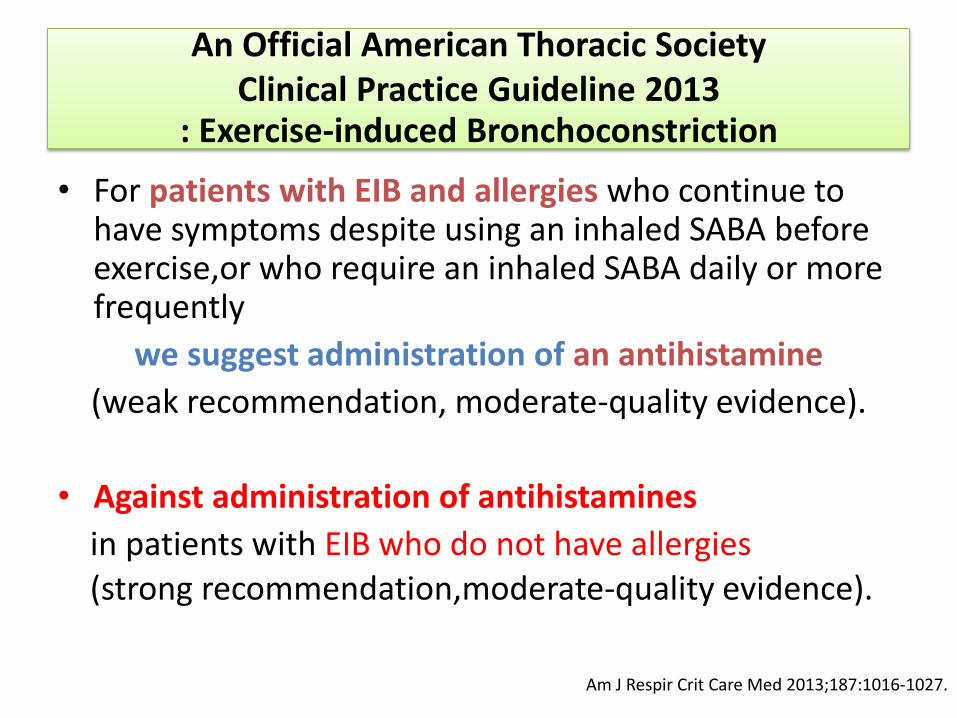
• For patients with EIB and allergies who continue to have symptoms despite using an inhaled SABA before exercise,or who require an inhaled SABA daily or more frequently
we suggest administration of an antihistamine
(weak recommendation, moderate-quality evidence).
• Against administration of antihistamines
in patients with EIB who do not have allergies (strong recommendation,moderate-quality evidence).
An Official American Thoracic Society Clinical Practice Guideline 2013
: Exercise-induced Bronchoconstriction
Am J Respir Crit Care Med 2013;187:1016-1027.
NONPHARMACOLOGIC THERAPIES
• Pre-exercise
: Warm up 60-80% HR max X 10-15 mins
– Given bronchoprotective effect and
extended refractory period from 1 - 4 hr.
– Recommend add on pharmacotherapy better than warm up alone or SABA alone
• Post-exercise
: Warm down X 10-15 mins
Am J Respir Crit Care Med 2013;187:1016-1027.
• Avoidance of triggers
• Nasal breathing
• Wearing a mask in cold environments
• Avoiding exercise in conditions where air is cold and dry
• Low salt diet
• Ѡ-3 fatty acid(fish oil) and Ascorbic acid supplement
NONPHARMACOLOGIC THERAPIES
Am J Respir Crit Care Med 2013;187:1016-1027.
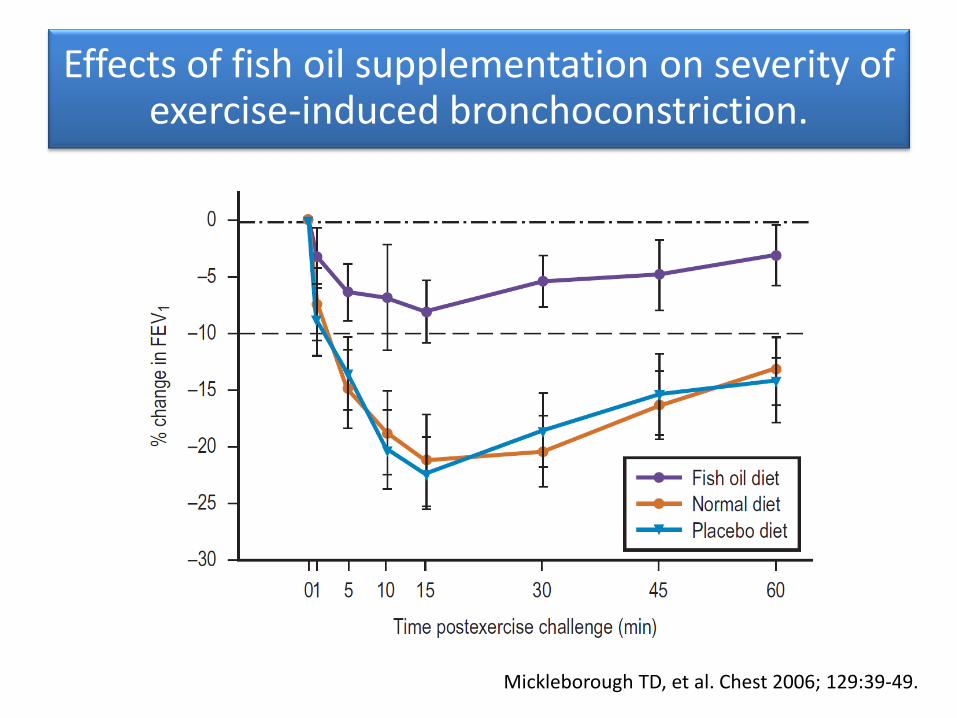
Effects of fish oil supplementation on severity of exercise-induced bronchoconstriction.
Mickleborough TD, et al. Chest 2006; 129:39-49.
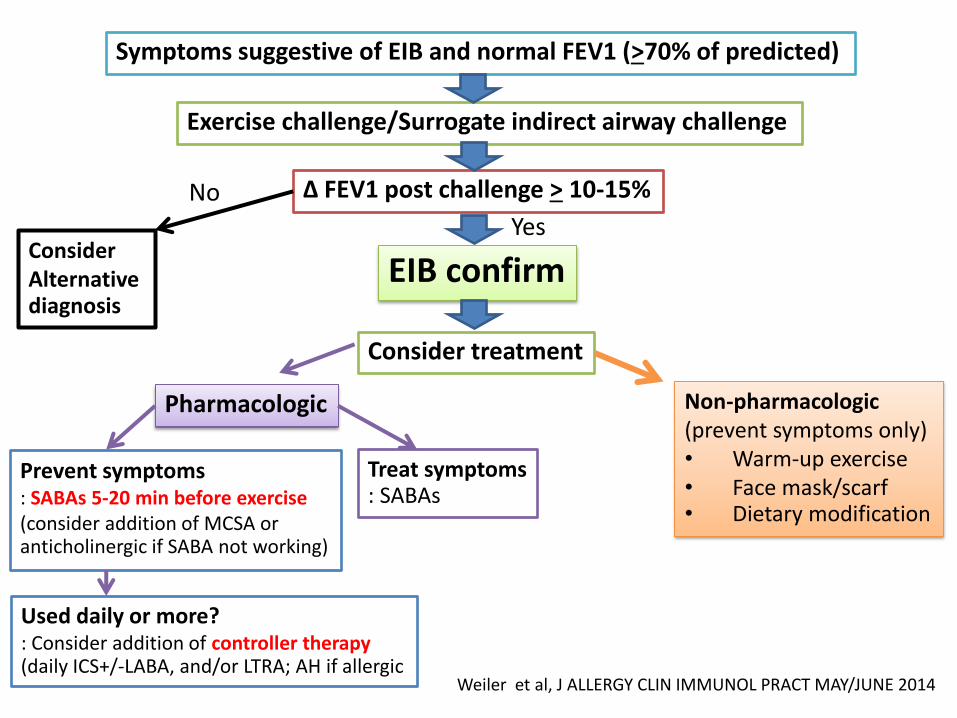
Weiler et al, J ALLERGY CLIN IMMUNOL PRACT MAY/JUNE 2014
Symptoms suggestive of EIB and normal FEV1 (>70% of predicted)
Exercise challenge/Surrogate indirect airway challenge
∆ FEV1 post challenge > 10-15%
Consider Alternative diagnosis
EIB confirm
Consider treatment
Non-pharmacologic (prevent symptoms only) • Warm-up exercise • Face mask/scarf • Dietary modification
Pharmacologic
Treat symptoms : SABAs
Prevent symptoms : SABAs 5-20 min before exercise (consider addition of MCSA or anticholinergic if SABA not working)
Used daily or more? : Consider addition of controller therapy (daily ICS+/-LABA, and/or LTRA; AH if allergic
No Yes

Thank you
Recommended