8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 1/47
Case 11
Qi Wang, Liz Croisant, KristinHarris, Nancy Mercier, Stefanie
Brown
1

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 2/47
• Mrs. Jones, 54 yo, F
• Fell and injured right hip
• 6-month history of backache, lethargy, and weakness
• Postmenopausal, taking hormone replacement therapy
• 3 episodes of pneumococcal pneumonia in last 2 yrs.
2

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 3/47
• Swollen, tender, and bruised right hip
• One inch of true shortening of the right leg
• Clinically anemic with pallor of her mucous
membranes and nailbeds
• Mild tachycardia
3

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 4/47
TESTS RESULTS X-ray of pelvis
and upper femurs Fracture of the neck of
femur througharea of decreased bonedensity
Red cell count 3.0 x 1012 /L
Hemoglobin 8.0 g/dL White cell count 3.6 x 109 /L Differential See photograph below
Platelet count 130 x 103 /mm3 ESR 32 mm/h BUN 30 mg/dL Creatinine 3 mg/dL Total protein 132 g/dL Serum albumin 2.6 g/dL Bilirubin (total) 0.8 mg/dL Alkalinephosphatase 150 U/L AP-1, 2 50 /L AP-2, 1 160 /L AP-3, 2 15 /L
Serum calcium 20 mg/dL 4

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 5/47
• Fracture in the neck of the femur (hip)
• Area of decreased bone density
• Decreased RBCs and hemoglobin (anemia)
• Decreased WBC - Diff shows plasma cell (may indicate
MM)
• Thrombocytopenia
5

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 6/47
• Elevated BUN and creatinine, decreased serum albumin
(possible renal problems)
• Elevated ESR (inflammation - most likely due to broken bone)
• Extremely elevated total protein (indicates an increase of
immunoglobulins)
• Elevated alkaline phosphatase and serum calcium (due to hip
fracture)
6

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 7/47
• Back pain
• Broken bones
• Weakness/lethargy
• Repeated
pneumococcal
pneumonia infections
• Elevated total protein
• Elevated calcium level
• Decreased WBC
• Plasma cell
7

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 8/47
• Waldenstrom's Macroglobulinemia
• MGUS
• Smoldering MM
8

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 9/47
9

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 10/47
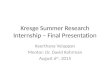
• Serum Protein Electrophoresis• Basic principle: electrophoresis
• Charged molecules exposed to electric field, migrate towardanode (+) or cathode (-)
• Migratory direction and rate of migration dependent on size, shape,charge, voltage, buffer pH
• Method to separate and isolate different molecular species within asample
• Serum protein electrophoresis (SPE)
• Used to separate and isolate major protein fractions withinpatient serum sample (5)
• Albumin, alpha, alpha 2, beta, gamma
• Gamma region
• Immunoglobulins
10

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 11/47
• SPE
• Procedure
• Agarose gel electrophoresis or cellulose acetateelectrophoresis may be performed
• Sample placed at cathode (-) end, voltage applied to system
• Alkaline buffer used (pH 8.6)
• Proteins net negative charge under alkaline conditions
• Serum proteins move toward anode
• 5 major serum protein fractions separated• Fractions fixed and stained
• Fractions quantitated using densitometer
11

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 12/47
Normal Serum ProteinElectrophoresis
12

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 13/47
• SPE
• Applications
• Detection of monoclonal immunoglobulin (M protein, paraprotein)
• Abnormal SPE pattern
• Monoclonal immunoglobulin appears as spike in gamma region
• Identical immunoglobulins from monoclonal plasma cells migrate to the
same position causing spike
• Monoclonal immunoglobulins the hallmark of Multiple Myeloma
13

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 14/47
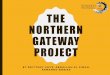
Mrs. Jones’ Abnormal
SPE pattern
Spike in gammaregion – M protein
14

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 15/47
• Immunofixation electrophoresis (IFE)
• Qualitative technique that combines zone electrophoresis with
immunoprecipitation
• Procedure used to identify the paraprotein causing the sharp peak on serum
protein electrophoresis in the gamma region
• Sometimes the alpha2 or beta region
• Characterization of paraproteins is critical to the proper diagnosis of the
plasma cell disorder
15

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 16/47
• IFE
• Separation of patient serum proteins using gel electrophoresis
• Application of IgG, IgA, IgM, kappa, and lambda antisera to the
electrophoresed samples in their respective lanes
• Precipitation of the antibodies complexed to their antigen occurs at
the region where the antigen (the IgA, IgG, IgM, etc proteins in the
patient’s serum) has migrated
16

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 17/47
• Precipitated antigen-antibody complex is then visualized by
staining the precipitated bands
• A sharp band in the lane for a heavy chain class and a sharp
band in one of the light chain lanes indicates the presence
of a monoclonal immunoglobulin
17

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 18/47
Mrs. Jones’ serum protein IFE
results
18

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 19/47
• IFE: Results
• Excess IgA antibodies with lambda light chains are present in the
plasma of this patient
• Blood serum paraprotein levels of more than 30 g/L diagnostic of
multiple myeloma
• The presence of excessive IgA antibody is characteristic of this
disorder
• 20% of patients with multiple myeloma produce excessive IgA antibodies
19

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 20/47
• Free Light Chains (FLC)
• Also known as Bence Jones Proteins (BJP)
• Monoclonal free kappa or lambda light chains of immunoglobulin
molecules
• Components of immunoglobulin molecules
• Single immunoglobulin monomer includes two light chains (either kappa or
lambda) and heavy chains
• FLC and Multiple Myeloma
• 60-70% of Multiple Myeloma patients excrete FLC in urine
• About 10% of Multiple Myeloma patients have only FLC20

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 21/47
• Testing for FLC
• Screening test – Heat Test for FLC in urine
• BJPs soluble at RT (in acidified urine),
• Precipitate at 40-60°C
• Resolubilize at 95-100°C
• *Note
• Other tests for protein in urine not very reliable for detecting FLC proteins, focus
primarily on albumin (urinalysis reagent strip)
21

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 22/47
• Testing for FLC• Screening Test- a serum FLC assay (Freelite)
• A quantitative method to measure Kappa
light chains, Lambda light chains, and theserum free kappa:free lambda ratio
• Uses nephelometry to measure
• Very sensitive for detecting plasma cell
disorders• Significantly increased free light chain
production and abnormal kappa/lambdaratios indicate an increased risk of disease
progression 22

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 23/47
• Serum FLC
• SPE and IFE
• Urine FLC
• Urine Protein Electrophoresis (UPE) and IFE
• Concentrated 24 hour urine without preservative used
23

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 24/47
Mrs. Jones’ urine IFE results
show free lambda lights chains
present in her urine 24

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 25/47
• Additional testing to confirm
diagnosis of Multiple Myeloma
• Bone marrow aspirate and biopsy
• Evaluate marrow for malignant
plasma cells
• Evaluate for increased numbers
of plasma cells in marrow
(>30%)
• X-ray, MRI, and CT
• Evaluate bone damage and
tumors (plasmacytoma)
• Peripheral blood smear
• May reveal plasma cells25

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 26/47
26

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 27/47
• All three must be met
• Monoclonal plasma cells must be present in bone marrow ≥10%
and/or presence of biopsy-proven plasmacytoma
• Presence of monoclonal antibodies in serum and/or urine
• Myeloma-related organ dysfunction (one or more must be met)
• Calcium elevation in the blood (serum calcium >10.5 mg/L or
upper limit of normal)
• Renal insufficiency as evidenced by serum creatinine >2 mg/100
mL
• Anemia as evidenced by Hgb <10 g/100 mL or 2 g < normal
• Presence of lytic bone lesions or osteoperosis 27

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 28/47
• Lab findings supporting diagnosis of Multiple Myeloma• Decreased RBC and hemoglobin (anemia)• Decrease in WBCs• Plasma cells observed on peripheral blood film• Thrombocytopenia• Elevated BUN, creatinine, decreased serum albumin – renal dysfunction• Elevated total serum protein – elevated immunoglobulin levels• Hypercalcemia• Punched out lesions in skull• M spike in gamma region seen in SPE• Excess IgA antibodies with lambda light chains seen on IFE
• > 2.0 g/L serum IgA• Decrease in other immunoglobulins• < 600 mg/dL for IgG
• FLC in urine seen on IFE• >30% plasma cells seen in bone marrow
28

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 29/47
• Plasma cell myeloma, Kahler's disease
• Cancer of the plasma cells in bone marrow
• Most common monoclonal gammopathy
• 2nd most common hematological malignancy
(10%)
• 1% of all cancers
29

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 30/47
• Plasma cells: Type of WBC that helps the body fight
infection by producing proteins called antibodies
• MM: plasma cells grow out of control in bone marrow,
form tumors (plasmacytoma) in areas of solid bone
• These bone tumors make it harder for the bone marrow
to make healthy RBCs and platelets
30

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 31/47
• Immune system keeps proliferation of B cells and
secretion of antibodies under tight control
• Control is lost when chromosomes and genes aredamaged, often through rearrangement
• Chromosomal translocation between the immunoglobulin
heavy chain gene and an oncogene is frequently
observed in patients with MM
31

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 32/47
• Mutation results in dysregulation of the oncogene
(thought to be an important initiating event in the
pathogenesis of myeloma)
• Results in proliferation of a plasma cell clone and
genomic instability that leads to further mutations and
translocations
• Chromosome 13 and 14 abnormality - 50% cases
• Production of cytokines (IL-6) by the plasma cells causes
localized damage – osteoporosis 32

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 33/47
• Creates a microenvironment in which the malignant cells
thrive
• Angiogenesis (the attraction of new blood vessels) isincreased
• Produced antibodies are deposited in various organs -
leads to renal failure, polyneuropathy and various other
myeloma-associated symptoms
33

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 34/47
• Precise etiology not yet been established
• Genetic
• Environmental/Occupational
• Significant exposures in agriculture, food, and petrochemicalindustries
• Increased risk in farmers, especially those who use herbicides andinsecticides
• Exposure to benzene and other organic solvents
• Long-term (>20 y) exposure to hair dyes
34

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 35/47
• MGUS (~19% of patients develop MM within 2-19 yrs)
• Radiation (risk in atomic-bomb survivors exposed to > 50
Gy)
• Chronic inflammation (preexisting chronic inflammatory
diseases)
• Infection (HPV8 infection of bone marrow dendritic cells)
35

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 36/47
• 4.3 cases per 100,000 white men
• 3 cases per 100,000 white women
• 9.6 cases per 100,000 black men
• 6.7 cases per 100,000 black women.• Median age is 68 years for men, 70 years for women
• 18% of patients <50 years, 3% of patients <40 years
• Male-to-female ratio ~ 3:2
• In U.S., African Americans are twice as likely asCaucasian
• Rare among people of Asian descent (1-2cases/100,000)
36

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 37/47
• Many organs affected, symptoms and signs vary greatly
• CRAB: C = Calcium (↑), R = Renal failure, A = Anemia,
B = Bone lesions (common tetrad of MM)
• Symptoms• Severe bone pain - Pathologic fracture
• Easy fatigability - Anemia, possible amyloid
• Nausea, confusion - Hypercalcemia
• Nausea, fatigue - Renal failure
• Recurrent infections - Decrease in normal Ig
• Paraplegia - Spinal cord compression
• Confusion, blurred vision - Hyperviscosity (rare)
• Bleeding - Thrombocytopenia
• Skin Nodules - Plasma cell tumors
37

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 38/47
• Major criteria
• Biopsy proven plasmacytoma
• >30% plasma cells in bonemarrow
• Monoclonal protein (M spike)• >3.5 g/dL of serum IgG or
• >2.0 g/dL of serum IgA or
• >1 g/24 h of lambda orkappa urinary L chains
• For diagnosis must have
• 1 major and 1 minor criteria or
• 3 minor criteria (must includefirst 2)
• Minor Criteria
• 10-30% plasma cells in bonemarrow
• M spike present but < levels
under major• Multiple lytic bone lesions
• Low normalimmunoglobulins
• IgM < 50 mg/dL
• IgA < 100
• IgG < 600
38

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 39/47
• Based on 4 factors
• Amount of abnormal monoclonal immunoglobulin in the blood orurine
• Amount of calcium in the blood
• Severity of bone damage based on x-rays• Amount of hemoglobin in the blood
• Factors divide myeloma into 3 stages
• Stage I indicates the smallest amount of tumor, stage III
indicates the largest amount of tumor
39

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 40/47
• Stage I• Hgb >10g/dL• Serum Calcium <12mg/dL• <2 lytic lesions on a skeletal survey• Small M spike (IgG <5g/dL or IgA <3.5g.dL or urine light chains
<4g/24h)• Stage II• Fits neither stage I or III
• Stage III• Hgb <8.5g/dL• Serum Calcium >12mg/dL• >=2 lytic bone lesions• Large M spike (Iga >7g/dL or IgA >5g/dL)
• Subclass• Subclass A: Creatinine level <2mg/dL• Subclass B: Creatinine level >2mg/dL
40

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 41/47
• Stage 2, Subclass B
• Hemoglobin <8.5g/dL (8g/dL)
• Serum Calcium >12mg/dL (20mg/dL)
• >2 Lytic Bone Lesions (multiple)
• Large M spike: IgG > 7g/dL or IgA > 5g/dL (IgG=0.12g/dL,IgA=3.54g/dL)
• Creatinine >2mg/dL (3mg/dL)
• Fits ¾ criteria for stage III (since IgA is <5g/dL), so
defaults to stage II)
41

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 42/47
• Developed ~ 1995
• Easier, more reliable
• Divides myeloma into 3 stages based only on the serum beta-2 microglobulin and serum albumin levels
• Stage I• Serum beta-2 microglobulin <3.5 mg/L and albumin level >3.5 g/L
• Stage II
• Neither stage I or III, meaning that either:
• The beta-2 microglobulin level is 3.5 - 5.5 mg/L (any albuminlevel)
• OR the albumin is <3.5g/L while beta-2 microglobulin is <3.5mg/L
• Stage III
• Serum beta-2 microglobulin >5.5mg/L
• Testing was not done to be able to stage in this system for our42

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 43/47
• Patient’s with a milder or slower progressing case may be carefully
watched without treatment.
• Medications used in treatment:
• Dexamethasone, melphalan, cyclophosphamide, doxil, thalidomide,
lenalidomide and bortezomib (alone or combined)
• Lenalidomide is an immunomodulatory drug, it slows or kills myeloma cells
an impacts blood vessels and surrounding substances that help cancer
cells.
• Bortezomib is known as a proteosome inhibitor and it is given43

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 44/47
• Bisphosphonates
• Reduce bone pain and prevent fractures
• Radiation therapy may be done to treat a bone tumor or give
bone pain relief.
• Bone marrow transplantation
• Autologous or stem cell
• Allogenic
44

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 45/47
• Stay hydrated – preserves kidney function
• Stay active – helps preserve calcium in their bones
• Complications treated quickly
• Avoid X-ray test that use contrast dye
• Consider joining a support group
• Address stress of illness
45

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 46/47
• Prognosis
• Survival is dependent upon age and stage
• Durie & Salmon Stage II ~ 41 months
• Some cases very aggressive• Some cases very slow progressing
• Conclusion:
• The patient was taken off of hormone replacement therapy to avoid
exacerbating bone lesion susceptibility
• Patient put on bisphosphonates to help prevent bone lesions
• The patient was given a bone marrow transplant
46

8/4/2019 Case 11 Presentation_final
http://slidepdf.com/reader/full/case-11-presentationfinal 47/47
Recommended