-
7/28/2019 Boala Pakinson
1/120
Boala Parkinson
Conf. Dr. Bogdan O. PopescuDisciplina de Neurologie Spitalul
Clinic ColentinaU.M.F. Carol Davila Bucuresti
-
7/28/2019 Boala Pakinson
2/120
1817
-
7/28/2019 Boala Pakinson
3/120
-
7/28/2019 Boala Pakinson
4/120
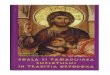
Substantia nigra and Parkinsons disease
The pathological changes in certain neurological diseases
provide insights about the function of thebasal ganglia. (A) Left:
The midbrain from a patient with Parkinson's disease. The
substantia nigra(pigmented area) is largely absent in the region
above the cerebral peduncles (arrows). Right: Themesencephalon from
a normal subject, showing intact substantia nigra (arrows). (B) The
size of the
caudate and putamen (the striatum) (arrows) is dramatically
reduced in patients with Huntington'sdisease. (From Bradley et al.,
1991.)
PD CTR
http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=neurosci.biblist.1266http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=neurosci.biblist.1266
-
7/28/2019 Boala Pakinson
5/120
SN in Parkinsons disease
-
7/28/2019 Boala Pakinson
6/120
Patogeneza bolii Parkinson
-
7/28/2019 Boala Pakinson
7/120
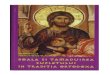
Corpii Lewy
www.saigata-nh.go.jp/saigata/rinken/neuropat/
http://www.saigata-nh.go.jp/saigata/rinken/neuropat/http://www.saigata-nh.go.jp/saigata/rinken/neuropat/http://www.saigata-nh.go.jp/saigata/rinken/neuropat/http://www.saigata-nh.go.jp/saigata/rinken/neuropat/
-
7/28/2019 Boala Pakinson
8/120
Scenariul Heiko Braak desprestadializarea BP si posibila
etiologie a
BP
-
7/28/2019 Boala Pakinson
9/120
-
7/28/2019 Boala Pakinson
10/120
Definitia Bolii Parkinson
Boala Parkinson (BP) este o afectiuneneurodegenerativa
progresiva, marcata, din
punct de vedere motor, de semne precumtremorul de repaus,
rigiditatea, bradikinezia siinstabilitatea posturala.
Apare din cauza mortii celulare progresive aunor celule din
regiuni bine determinate aleSNC, inclusiv substanta neagra din
mezencefal.
-
7/28/2019 Boala Pakinson
11/120
PD description
Usually beginning in a person's late fifties or early
sixties
Parkinson disease causes a progressive decline inmovement
control, affecting the ability to controlinitiation, speed, and
smoothness of motion
Symptoms of PD are seen in up to 15% of those ages65-74, and
almost 30% of those ages 75-84
PD affects approximately 1,000,000 people in theUnited States,
both men and women, with as many asfifty thousand new cases each
year
Most cases of PD are sporadic 1-5% PD genetic mutations
inherited
-
7/28/2019 Boala Pakinson
12/120
PD etiology (I)
The immediate cause of PD: degeneration of brain cells in the
area known as the substantianigra , one of the movement control
centers of the brain
Damage to this area leads to the cluster of symptoms known as
"parkinsonism"
In PD, degenerating brain cells contain Lewy bodies, which help
identify the disease
-
7/28/2019 Boala Pakinson
13/120
PD etiology (II)
The cell death leading to parkinsonism may be causedby a number
of conditions: Infection Trauma Poisoning Drugs given for
psychosis, such as haloperidol (Haldol) or
chlorpromazine (thorazine) When no cause for nigral cell
degeneration can be
found, the disorder is called idiopathic parkinsonism,
orParkinson disease Parkinsonism may be seen in other
degenerative
conditions, known as the "parkinsonism plus"syndromes, such as
progressive supranuclear palsy
-
7/28/2019 Boala Pakinson
14/120
PD etiology (III)
The substantia nigra , or "black substance," is one of the
principal movement control centers in the brain
By releasing dopamine , it helps to refine movementpatterns
throughout the body
The dopamine released by nerve cells of substantianigra
stimulates another brain region, the corpusstriatum
Without enough dopamine, the corpus striatum cannotcontrol its
targets, and so on down the line
Ultimately, the movement patterns of walking, writing,reaching
for objects, and other basic programs cannotoperate properly, and
the symptoms of parkinsonismare the result.
-
7/28/2019 Boala Pakinson
15/120
PD etiology (IV) There are some known toxins that can cause
parkinsonism, most
notoriously a chemical called MPTP
(1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine) , found as an
impurity in someillegal drugs.
Parkinsonian symptoms appear within hours of ingestion, andare
permanent
MPTP may exert its effects through generation of toxicmolecular
fragments called free radicals, and reducing freeradicals has been
a target of several experimental treatments forPD using
antioxidants
It is possible that early exposure to some
as-yet-unidentifiedenvironmental toxin or virus leads to undetected
nigral celldeath, and PD then manifests as normal age-related
declinebrings the number of functioning nigral cells below the
thresholdneeded for normal movement
It is also possible that, for genetic reasons, some people
aresimply born with fewer cells in their substantia nigra than
others, and they develop PD as a consequence of normal
decline.
-
7/28/2019 Boala Pakinson
16/120
Pure Parkinsonism Parkinsonism with otherfeatures
Pseudoparkinsonism
Parkinson's disease Progressive supranuclear palsy Essential
Tremor
Drug-inducedparkinsonism Multiple system atrophy Vascular
(aterosclerotic) parkinsonism
Postencephaliticparkinsonism Basal ganglia calcification
MPTP parkinsonism Repetitive head trauma
Other toxins, e.g.manganese Cerebral anoxia
Parkinsons disease and parkinsonism
-
7/28/2019 Boala Pakinson
17/120
PD symptoms Tremors , usually beginning in the hands, often
occurring on one
side before the other. The classic tremor of PD is called a
"pill-rolling tremor," because the movement resembles rolling a
pillbetween the thumb and forefinger. This tremor occurs at
afrequency of about three per second.
Slow movements (bradykinesia) occur, which may involveslowing
down or stopping in the middle of familiar tasks such as
walking, eating, or shaving. This may include freezing in
placeduring movements (akinesia).
Muscle rigidity or stiffness, occuring with jerky
movementsreplacing smooth motion.
Postural instability or balance difficulty occurs. This may
leadto a rapid, shuffling gait (festination) to prevent
falling.
In most cases, there is a "masked face," with little
facialexpression and decreased eye-blinking = hypomimia
-
7/28/2019 Boala Pakinson
18/120
PD symptoms non-motor (II)
Depression Anxiety Speech changes , including rapid speech
without
inflection changes Sleep problems , including restlessness and
nightmares Emotional changes , including fear, irritability,
and
insecurity Bladder disorders incontinence, polyuria, urinary
urgency Constipation Sexual dysfunction
-
7/28/2019 Boala Pakinson
19/120
-
7/28/2019 Boala Pakinson
20/120
Stages of Parkinsons disease (Hoehn and Yahr)
Stage 1 : unilateral involvement; blank faces; affected arm
insemiflexed position with tremor; patient lean to unaffected
side.
Stage 2: bilateral involvement with early postural changes;
slow,shuffling gait with decreased excursion of legs.
Stage 3: pronounced gait disturbances; moderate
generalizeddisability; postural instability with tendency to fall
.
Stage 4: significant disability; limited ambulation with
assistance.
Stage 5: complete invalidism; patient confined to bed or
chair;cannot stand or walk even with assistance.
-
7/28/2019 Boala Pakinson
21/120
Diagnosis of Parkinsons disease
Parkinsons disease to be differentiated from: Parkinsonisms of
different etiologies Atypical parkinsonism
Mainly based on typical neurological findingsand to response to
levodopa (l-dopa)
PD is characterized by: Disturbances of motor function
(cardinal
manifestations) Accompanying manifestations (non-motor
signs)
-
7/28/2019 Boala Pakinson
22/120
Cardinal manifestations of PD (I)
Bradykinesia, hypokinesia, akinesia Difficult initiation of
movement ( akinesia ) Sluggishness of movement ( bradykinesia )
Diminished spontaneous movement ( hypokinesia ) Tend to occur
together Spontaneous fluctuations of mobility Motor disturbances
more pronounced on one side (especially
early stages) Mask like facies (hypomimia), defective mouth
closure, reduced
blinking, dysphagia, salivation (drooling) Speech: hypophonia
(diminished in volume), hoarse voice, poorly enunciated, monotonous
in pitch (disarthrophonia), hard toinitiate speech, may repeat
syllables involuntary acceleration of speech toward the end of a
sentence (festination)
-
7/28/2019 Boala Pakinson
23/120
Cardinal manifestations of PD (II)
Postural changes
Stooped posture Flexed andadducted postureof the arms
Postural instability
-
7/28/2019 Boala Pakinson
24/120
Cardinal manifestations of PD (III)
Gait disturbances Appear in the early stages of the disease
Small-stepped gait, shuffling, limping
Reduced arm swinging Difficulty in initiating gait Freezing of
gait = complete arrest of gait when the
patient is confronted by doorway or a narrow pathbetween
furniture
Difficult to stand up from a seated position or toturn over in
bed
-
7/28/2019 Boala Pakinson
25/120
-
7/28/2019 Boala Pakinson
26/120
PD famous people Adolf Hitler had post encephalitic PD, PD that
developed after a
viral infection during the Great Encephalitis, Sleeping
Sickness,Epidemic of 1918 - 1926. Hitler, in 1938, was Time Man of
the
Year.
1945, 56 yo1938, 49 yo
-
7/28/2019 Boala Pakinson
27/120
-
7/28/2019 Boala Pakinson
28/120
Why tremor?
The exact anatomical basis of parkinsonian tremor isnot
known
In animals, experimental lesions to the SN do not result
in tremor neither do lesions in the striatopallidal partsof the
basal ganglia From 8 MPTP intoxicated patients, only 4
developed
tremor
Ward et al. produced parkinsonian tremor in monkeysby lesions in
the ventromedial tegmentum of themidbrain concluded that probably
lesions toreticulospinal pathway induce parkinsonian tremor
alternatively the tegmento-thalamic projection
-
7/28/2019 Boala Pakinson
29/120
Cardinal manifestations of PD (VI)
Rigidity Elevated muscle tone is felt by the patient as
muscle
tension of spasm and by examiner as resistance topassive
movements across the joints
Examination reveal cogwheel rigidity (repeated,ratchet-like
oscillations of resistance to passivemovements across the wrist,
elbow, etc., which arebrought out by alternating passive flexion
andextension)
Pathophisiology: lesions to nigrostriatal system (lessdopamine
normal thalamo-cortical drive isinhibited)
-
7/28/2019 Boala Pakinson
30/120
-
7/28/2019 Boala Pakinson
31/120
The Pope in 1979, age
59, with President Jimmy Carter. ThePope's shouldersstoop, PD
begins.
-
7/28/2019 Boala Pakinson
32/120
Neurodegeneration: AD and PD
The Pope andPresident RonaldReagan defeatedCommunism
-
7/28/2019 Boala Pakinson
33/120
The Pope in 1988, age68, 2 years after PDdiagnosed. The Pope
is
with President RonaldReagan. The Pope diedof complications of
PD. President Reagan
died of complications of Alzheimer disease.
-
7/28/2019 Boala Pakinson
34/120
The Pope in 1992,age 72, 13 yearsafter PD began, 6years after
PDdiagnosed. ThePope is withPresidentGeorge Herbert
Walker Bush andBarbara Bush
-
7/28/2019 Boala Pakinson
35/120
The Pope in 1999, age79, 20 years after PDbegan, 13 years he
was
diagnosed. The Pope is with President Clintonand Hillary
Clinton
-
7/28/2019 Boala Pakinson
36/120
The Pope in 2004, age84, 25 years after PDbegan, 18 years after
PD
diagnosed. The Pope is with President George W Bush
-
7/28/2019 Boala Pakinson
37/120
PD treatment
There is no cure for Parkinson disease. Most
drugs treat the symptoms of the disease only,although drugs like
rasagiline and dopamineagonists may slow degeneration of the
substantianigra.
-
7/28/2019 Boala Pakinson
38/120
PD treatment physical exercise
Regular, moderate exercise has been shown toimprove motor
function without an increase inmedication for a person with PD
Exercise helps maintain range of motion in stiff muscles,
improve circulation, and stimulate appetite
An exercise program designed by a physical therapisthas the best
chance of meeting the specific needs of the
person with PD A physical therapist may also suggest strategies
for
balance compensation and techniques to stimulatemovement during
slowdowns or freezes.
-
7/28/2019 Boala Pakinson
39/120
PD treatment - nutrition PD patients may lose interest in food ,
especially if depressed, and may have
nausea from the disease or from medications, especially those
known asdopamine agonists Slow movements may make it difficult to
eat quickly, and delayed gastric
emptying may lead to a feeling of fullness without having eaten
much Increasing fiber in the diet can improve constipation, soft
foods can reduce
the amount of needed chewing, and a prokinetic drug such as
cisapride ordomperidone can increase the movement of food through
the digestivesystem.
PD patients may need to limit the amount of protein in their
diets themain drug used to treat PD, L-dopa, is an amino acid, and
is absorbed by thedigestive system by the same transporters that
pick up other amino acidsbroken down from proteins in the diet.
Limiting protein, under the direction
of the physician or a nutritionist, can improve the absorption
of L-dopa. No evidence indicates that vitamin or mineral
supplements can have any effect on the disease other than in the
improvement of the patient's generalhealth
No antioxidants used to date have shown promise as a treatment a
large,carefully controlled study of vitamin E demonstrated that it
could not halt
disease progression
-
7/28/2019 Boala Pakinson
40/120
PD treatment - drugs
The pharmacological treatment of Parkinson disease iscomplex
While there are a large number of drugs that can beeffective,
their effectiveness varies with the patient,disease progression,
and the length of time the drug hasbeen used
Dose-related side effects may preclude using the mosteffective
dose, or require the introduction of a new drug to counteract
them
There are six classes of drugs currently used to treatPD.
-
7/28/2019 Boala Pakinson
41/120
Drug classes to treat PD
1. MAO inhibitors (rasagiline, selegiline) 2. Dopaminergic
agonists, non-ergot (ropinirol,
pramipexol, rotigotine) + apomorphine 3. Levo-dopa 4. Levo-dopa
enzymatic degradation inhibitors:
a. dopa-decarboxylase inhibitor (benserazide or carbidopa) and
b. COMT inhibitors (entacapone)
5. Anticholinergics 6. Amantadine (NMDA inhibitor)
-
7/28/2019 Boala Pakinson
42/120
Levo-dopa
Is never used nowadays without a dopa-decarboxylase inhibitors,
always in
combination (Sinemet, Madopar, Nakom,etc.) Triple combination in
one tablet: levo-dopa
+ carbidopa + entacapone) - Stalevo
Alg ith d P ti P t f
-
7/28/2019 Boala Pakinson
43/120
43
Algorithms and Practice Parameters for Initial Treatment of
PD*
Based on: Olanow, CW et al. Neurology 2001; 56 S5, S1-88 and on
AAN practice parameters. Levodopa provides superior motor benefit
but greater risk of dyskinesia; no evidence of a benefit of
initiating treatment withextended release levodopa versus immediate
release (1)1. Miyasaki et al. 2002 Neurology 58, 11-17; 2.
Suchowersky et al. 2006 Neurology 66, 976-982.
Parkinson s Disease Pharmacologic therapy/functional impairment
Nonpharmacologic therapy
Education
SupportServices
Exercise 2
NutritionDopamineAgonists 1Levodopa
(+/- COMT inhibitor)
Comined treatment
No treatment hasbeen shown to beneuroprotective 2
MAOB Inhibitors(RAS) have only mildsymptomatic benefit 1
-
7/28/2019 Boala Pakinson
44/120
Drugs that replace dopamine Levodopa (L-dopa), is the most
effective treatment for the
symptoms of PD L-dopa is a derivative of dopamine, and is
converted into dopamineby the brain
It may be started when symptoms begin, or when they
becomeserious enough to interfere with work or daily living
L-dopa therapy usually remains effective for all duration of
thedisease Following this, many patients develop motor fluctuations
, including
peak-dose "dyskinesias" (abnormal movements such as twisting,
orrestlessness), rapid loss of response after dosing (known as the
"on-
off" phenomenon), and unpredictable drug response Higher doses
are usually tried, but may lead to an increase indyskinesias
Side effects of L-dopa include: nausea and vomiting
low blood pressure upon standing (orthostatic hypotension) -
causes dizziness these effects usually lessen after several weeks
of therapy.
-
7/28/2019 Boala Pakinson
45/120
Dopamine
-
7/28/2019 Boala Pakinson
46/120
-
7/28/2019 Boala Pakinson
47/120
Enzyme inhibitors (I)
Dopamine is broken down by several enzyme systems in thebrain
and elsewhere in the body, and blocking these enzymesis a key
strategy to prolonging the effect of dopamine
The two most commonly prescribed forms of L-dopa containa drug
to inhibit the amino acid decarboxylase (an AADCinhibitor), one
type of enzyme that breaks down dopamine
These combination drugs are Sinemet, Nakom, Isicom (L-dopa plus
carbidopa ) and Madopar (L-dopa plusbenzaseride ).
Controlled-release formulations also aid inprolonging the effective
interval of an L-dopa dose
-
7/28/2019 Boala Pakinson
48/120
Enzyme inhibitors (II)
The enzyme monoamine oxidase B (MAO-B)inhibitors selegiline and
rasagiline may be given asadd-on therapy for L-dopa. Research
indicatesrasagiline may have a neuroprotective effect, sparing
nigral cells from damage by free radicals. Because of this, and
the fact that it has few side effects, it is alsofrequently
prescribed early in the disease before L-dopais begun
Entacapone and tolcapone, two inhibitors of anotherenzyme system
called catechol-O-methyltransferase( COMT ), may soon reach the
market as early studiessuggest that they effectively treat PD
symptoms withfewer motor fluctuations and decreased daily
L-dopa
requirements.
-
7/28/2019 Boala Pakinson
49/120
-
7/28/2019 Boala Pakinson
50/120
-
7/28/2019 Boala Pakinson
51/120
-
7/28/2019 Boala Pakinson
52/120
-
7/28/2019 Boala Pakinson
53/120
-
7/28/2019 Boala Pakinson
54/120
-
7/28/2019 Boala Pakinson
55/120
-
7/28/2019 Boala Pakinson
56/120
-
7/28/2019 Boala Pakinson
57/120
Typical pattern of wearing-off
Daily fluctuations in wearing-off
-
7/28/2019 Boala Pakinson
58/120
-
7/28/2019 Boala Pakinson
59/120
PRELUDE survey : Importance of wearing-off for patients and
healthcare professionals
Managingdyskinesia #1 for
MovementDisorder
Specialists
Managingwearing-off #1for PD patients
and PCPs
Dyskines ia
What is the biggest challenge with levodopa therapy?
-
7/28/2019 Boala Pakinson
60/120
Within two years 12% of neurologists recognizewearing-off but
54% modify the levodopa regimen
Comtan Diagnostic survey, 2002
The large discrepancy in the numbers (54% Vs 12%) highlightsthe
difficulty in identifying the first signs of wearing-off
-
7/28/2019 Boala Pakinson
61/120
Study, year Definition and Incidence
Rajput et al. 2002
A predictable decline in motor function at the end of dose in a
patient with previously stable responsereceiving 3 or more daily
levodopa doses25% of patients had wearing-off after 4.9 years
Parkinson Study Group,2000
A perception of loss of mobility or dexterity, usuallytaking
place gradually over minutes and usuallybearing close resemblance
to the timing of antiparkinsonian medications38% of patients had
wearing-off after only 2 years
No universal definition of wearing-off
The lack of a universal definition of wearing-off may be
reflected
in its reported incidence in patients PSG, 2000Rajput et al.,
2002
-
7/28/2019 Boala Pakinson
62/120
Useful definitions of wearing-off
Wearing -off happens w hen a dose that
p rev ious ly used to he lp your symptom s does no t las t as
long and yo ur next dos e is
needed so oner. Symp toms of wear ing-off
includ e changes in mov ement and m obi l i ty,
thoug hts and feelings , sensat ions and
sense of well being.
PinK working group
Wearing -off refers to th e predictable
emergence of one or more PD s igns or sym ptom s before the next
scheduled
antiparkinsonian medication dosage.
For the ph ysic ian : For the pat ien t :
Stacy et al, 2004
-
7/28/2019 Boala Pakinson
63/120
Consensus definition of wearing-off
A generally predictable recurrence of motor o r n o n m o t o r
s y m p t o m s t h at
precedes a sc hedu led do se and u su a lly imp roves wi th an t
ipark inso n ian
medication.
In September 2004, a wearing-off working group meeting of
leading international Movement Disorder Specialists arrived
at a consensus definition.
-
7/28/2019 Boala Pakinson
64/120
Symptoms of wearing-off
-
7/28/2019 Boala Pakinson
65/120
Challenges in identification of wearing-off
Because patients may not be aware that thech anges th ey are exp
eriencin g are related to th eir PD and are t reatable, they m ay
not s pon taneou sly d iscu ss their symptoms
It is, therefore, important that physicians treating PD be aware
of th e m any different sym ptom s of w earing- o ff and sp ec if
ical ly ask about the occu r rence of s uch changes.
Stacy , 2003
Identification of Wearing Off
-
7/28/2019 Boala Pakinson
66/120
Identification of Wearing Off Symptoms
Wearing-Off
Non-Motor Symptoms(often precede/coincide with Motor
Symptoms)
Motor Symptoms
AUTONOMICpallor BP changesshortness of
breathtachycardiasweatingfacial flushinglaryngeal stridor papillary
dilationdroolingdysphagiabelchingabdominal bloatingurinary
frequencymicturition disturbances
Tremor R igidityAkinesia/BradykinesiaP ostural
Instability/Balance
Blanchet (2003) CJNS, 30(1): S19-S26
SENSORYPainParesthesiasSensory lossAkathisiaFatigue
PSYCHIATRICAnxietyParanoiaHallucinationsDepressionPanicCognitive
changes
-
7/28/2019 Boala Pakinson
67/120
Non-motor fluctuations (NMF)
1976: Marsden and Parkes recognized NMF in fluctuating PD
1993: Riley and Lang proposed a classification that is often
usedtoday
1996: Hillen and Sage studied the frequency of NMF in
afluctuating population
Using an open-ended question they identified NMF in 17% of
fluctuatingpatients
2002: Witjas et al studied the frequency and disability caused
byNMF in advanced PD patients
Using a structured questionnaire they identified NMF in 100% of
patientsexperiencing motor fluctuations
Marsden and Parkes, 1976Riley and Lang, 1993Hillen and Sage,
1996Witjas et al, 2002
-
7/28/2019 Boala Pakinson
68/120
Non-motor fluctuations in wearing-off
Non-motor fluctuation Frequency (%) Frequency during off state
(%)
Anxiety 66 88
Drenching sweats 64 59
Slowness of thinking 58 83
Fatigue 56 75
Akathisia 54 63
Irritability 52 88
Hallucinations 49 25
In a study of 50 patients with advanced PD and motor
fluctuations: All patients with motor off periods had at least one
non -motor fluctuation Most non- motor fluctuations were associated
with the off state
Witjas et al. 2002
-
7/28/2019 Boala Pakinson
69/120
Causes of Wearing Off
-
7/28/2019 Boala Pakinson
70/120
Causes of Wearing Off :Impact of striatal dopamine levels
Olanow 2004
Dopaminergic neurons die, growing lack of buffering capacity
Striatal pulsatility increasingly mirrors exogenous delivery
-
7/28/2019 Boala Pakinson
71/120
Obeso et al. 2000
Altered neuronal firing patterns
Pulsatile stimulation of striataldopamine receptors
Downstream dysregulation of genes, proteins and second
messenger systems
Development of dyskinesia
Altered basal ganglia firingpatterns
-
7/28/2019 Boala Pakinson
72/120
Pulsatility
1. Pulsatile stimulation contributes to the development of
complications related to dopaminergic therapy
Pulsatile stimulation of brain dopamine receptors results from
:progressive PD pathology
the use of dopaminergic agents with short half-lives2. Levodopa
has a relatively short half-life (60 90 min)
The therapeutic hypothesis:Strategies that provide levodopa to
the brain in a less
pulsatile and more continuous manner may reduce the riskof motor
complications
Obeso et al. 2000
-
7/28/2019 Boala Pakinson
73/120
Wearing -Off
L-Dopa Dosing
Off
ON
-
7/28/2019 Boala Pakinson
74/120
Management of wearing-off
The Management of Wearing-off :
-
7/28/2019 Boala Pakinson
75/120
g gDopamine Agonists
The dopamine agonists are a viable option, but many patients are
already on adopamine agonist when they are given levodopa
Furthermore the dopamine agonists do not change
thepharmacokinetic/pharmacodynamics of levodopa and therefore do
not address theunderlying issue of pulsatility associated with
traditional levodopa therapy
Providing a dopamine agonist to patients already on levodopa may
reduce levodopaefficacy through competitive inhibition of dopamine
on the post-synaptic striatalreceptor
CALM-PD (PSG), 4 yr Pramipexole vs. Levodopa, 2004
A) Levodopa Modification
-
7/28/2019 Boala Pakinson
76/120
A) Levodopa Modification1. Increase Dose
C l i n i c a
l E f f e c t
Increased likelihood of peak-dose dyskinesia
A) Levodopa Modification
-
7/28/2019 Boala Pakinson
77/120
The challenge of CDS with levodopa:Increasing the frequency of
oral levodopa doses- troughs
With permission from F. Stocchi* Data f rom different f luctuat
ing pat ients
* *
A) Levodopa Modification2. Increase Dose Frequency
-
7/28/2019 Boala Pakinson
78/120
Pharmacokinetic evidence of significant pulsatility with hourly
dosing
With permission from F. Stocchi
ON
OFF
Fluctuating patient
2. Increase Dose Frequency
-
7/28/2019 Boala Pakinson
79/120
-
7/28/2019 Boala Pakinson
80/120
A History of Levodopa Delivery
1961 Levodopa introduced, 1% converted to Dopamine in the
brain.
1963 DDCI introduced, 10% of Levodopa converted to Dopamine
2001 Entacapone introduced, increased Levodopa exposure ~35%
Carbidopa or Benserazide
Entacapone
Levodopa/carbidopa/entacapone
-
7/28/2019 Boala Pakinson
81/120
Levodopa/carbidopa/entacaponeFluctuators: Efficacy
In patients with fluctuations:
Mean daily ON -time increased by 1.4 1.6 hours
Efficacy (mean motor UPDRS scores) improved by 1.9 - 3.2
Daily levodopa dosage reduced by 42 - 112 mgrelative to
placebo
1. Rinne et al- Nordic NOMECOMT Study Group (1998) Entacapone
enhances the response to levodopa in parkinsonian patients with
motor fluctuations, Neurol 51: 1309-1314
2. PSG- North American SEESAW Study (1997) Entacapone improves
motor fluctuations in levodopa-treated parkinsons disease patients,
Ann Neurol 42: 747-755
3. Poewe et al- Austrian-German CELOMEN Study Group (2002 )
Efficacy and safety of entacapone in parkinsons disease
patientswith suboptimal levodopa response, Acta Neurol Scand 105:
2345-255
4. Brooks etl al- UK-IRISH (2003). Entacapone is beneficial in
both fluctuating and non- fluctuating patients with Parkinson s
disea se. J Neurol Neurosurg Psych. 74: 1071 1079
Levodopa/carbidopa/entacapone
-
7/28/2019 Boala Pakinson
82/120
Earlier management of wearing-off improves long-term patient
function
Delayed start analysis of 3 long-term studies Over 5 years ,
early initiation of levodopa with a DDCI and entacapone resulted in
a
significant benefit compared with a delayed start in
treatment
-6.0
0.0
6.0
12.0
18.0
Baseline (N=484)
1 (N=410)
2 (N=101)
3(N=90)
4(N=44)
5(N=37)
Years
U P D R S I I I s c o r e s
Levodopa with DDCI and entacapone
Traditional levodopa plus placebo
Sustained Duration of Efficacy or Long Duration Dose
Stability
Nissinen et al (2006 Feb)- Early initiation of entacapone leads
to superior 5 year efficacy comparedto delayed initiation in PD
patients receiving traditional ldopa/DDCI therapyWorld Parkinson
Congress- Poster, Washington
-
7/28/2019 Boala Pakinson
83/120
-
7/28/2019 Boala Pakinson
84/120
STALEVO :
-
7/28/2019 Boala Pakinson
85/120
Mean ADL UPDRS scores improved by 0.9 2.2
Daily levodopa dosage reduced by 22 40 mg relative to
placebo
Stalevo Levodopa/DDCI plus placebo*p
-
7/28/2019 Boala Pakinson
86/120
The use of STALEVO
A) in Fluctuators:
Improves ON time with current levodopa regimen by 1.4- 1.6 hours
(6.8- 16% mean change from baseline) 1-3
Sustains current levodopa efficacy/dose regimen for at least the
next 3years 4 Earlier Stalevo start results in improved long-term
function 5
Improves QOL & ADL6,7
B) In Non-Fluctuators, emerging evidence suggests
Improves QOL & ADL 8,9
Reduces levodopa pulsatility which, over time, is thought to
beresponsible for development of dyskinesias 10.
1. Rinne et al- Nordic NOMECOMT Study Group (1998) Entacapone
enhances the response to levodopa in parkinsonian patients with
motor fluctuations, Neurol 51: 1309-1314
2. PSG- North American SEESAW Study (1997) Entacapone improves
motor fluctuations in levodopa-treated parkinsons disease patients,
Ann Neurol 42: 747-755
3. Poewe et al- Austrian-German CELOMEN Study Group (2002 )
Efficacy and safety of entacapone in parkinsons disease
patientswith suboptimal levodopa response, Acta Neurol Scand 105:
2345-255
4. Larsen et al NOMESAFE Study Group (2003), The tolerability
and efficacy of entacapone over 3 years in patients with parkinsons
disease, Eur J Neur, 10: 137-146
5. Nissinen et al (2006 Feb)- Early initiation of entacapone
leads to superior 5 year efficacy compared to delayed initiation in
PD patients receiving traditional ldopa/DDCI therapy , WPC Poster,
Washington
6. Onofrj et al. (2004) Combining entacapone with levodopa/DDCI
improves clinical status and quality of life regarless of dosing
frequency, J Neurol Transam, 111: 1053-1063
7. Gershanik et al (2003) Efficacy and safety of levodopa with
entacapone in parkinsons disease patients suboptimally controlled
with levodopa alone, Prog Neuro-Psych & Bio-Psych, 27:
963-971
8. Brooks etl al- UK-IRISH (2003). Entacapone is beneficial in
both fluctuating and non- fluctuating patients with Parkinson s
disea se. J Neurol Neurosurg Psych. 74: 1071 1079
9. Olanow et al. (2004) Double-Blind, placebo-controlled study
of entacapone in levodopa-treated patients with stable parkinsons
disease: Arch Neruol 61: 1563-156810. Stocchi and Olanow (2004),
Continuous dopaminergic stimulation in early and advanced PD,
Neurol Sci 62 (Suppl 1): S57-S64
-
7/28/2019 Boala Pakinson
87/120
-
7/28/2019 Boala Pakinson
88/120
-
7/28/2019 Boala Pakinson
89/120
-
7/28/2019 Boala Pakinson
90/120
-
7/28/2019 Boala Pakinson
91/120
-
7/28/2019 Boala Pakinson
92/120
-
7/28/2019 Boala Pakinson
93/120
-
7/28/2019 Boala Pakinson
94/120
Limitations of multiple dosing for Parkinson s disease
Multiple daily doses of a short-acting agent can lead to:
fluctuations in plasma drug concentration throughout
the day decline in plasma drug concentration at night wearing
off of symptom control during the night
May contribute to lack of control of nocturnal symptomsof PD
Variation of absorption rate with food intake
Li i i f l i l d i f
-
7/28/2019 Boala Pakinson
95/120
P l a s m a
d r u g
c o n c e n
t r a
t i o n s
Dose Dose Dose
Motor complications
Off
On
Patients symptomswell controlled
Patients symptoms notwell controlled
Limitations of multiple dosing for Parkinson s disease
Duration of L dopa treatment and
-
7/28/2019 Boala Pakinson
96/120
P a t i e n
t s w
i t h d y s
k i n e s i a
( % )
Kostic et al. Neurology 1991;41:202 5
Duration of L-dopa treatment (years)
Duration of L-dopa treatment andfrequency of dyskinesia
Treatment with levodopa has dramatically reduced disabilityand
mortality associated with Parkinson s disease
-
7/28/2019 Boala Pakinson
97/120
y
Years since diagnosis
P a
t i e n
t s w i t
h s e v e r e
d i s a
b i l i t y a n d
d e a
t h ( % )
0
20
40
60
80
100
1 5 6 10 11 15
Untreated patients
Levodopa/carbidopa-treated patients
Figure adapted from Poewe et al. Neurol 1996;47:S146;Hoehn et
al. J Neural Trans 1983;19:253
Levodopa consistently provides better symptom controlcompared
with dopamine agonists
-
7/28/2019 Boala Pakinson
98/120
DDCI-=dopa-decarboxylase inhibitor;UPDRS=Unified Parkinson s
Disease Rating Scale
p p g
Pramipexole Levodopa/carbidopa p=0.003
Levodopa /ca rb idopa ver sus p ramipexo le 1
4 2
0 2 4
12 24 42 C h a n g e
i n U P D R S t o
t a l s c o r e 16 14 12 10
8 6
6 18 36 48 Time (months)
I m p r o v e m e n
t
Figure adapted from 1Holloway et al. Arch Neurol
2004;61(7):1044;2
Rascol et al. N Engl J Med 2000;342(20):1484;3Bracco et al. CNS
Drugs 2004;18(11):733
Treatmentregimen
Improvement versuslevodopa/DDCI
Pramipexole 1 5.9 points on total UPDRSscore (p=0.003) at 4
years
Ropinirole 2 4.48 points on UPDRSmotor score (p=0.008)at 5
years
Cabergoline3
2.9 points on UPDRS motor score (p
-
7/28/2019 Boala Pakinson
99/120
Need fo r levodo pa in pat ien ts in i t i ated w i th a dop
amine agon is t
(pramipexole) 1,2
Need for levod op a in pat ien ts in i t i ated w i th a dop
amine agon is t
( rop in iro le) 3,4
Years after randomization Years after randomization
P a
t i e n
t s r e q u
i r i n g
s u p p
l e m e n
t a l l e v o
d o p a
( % )
53%
72%
0
20
40
60
80
2 4
Figure adapted from 1Holloway et al. Arch Neurol
2004;61(7):1044;Figure adapted from 2PSG. JAMA
2000;284(15):1931;
Figure adapted from3
Rascol et al. NEJM 2000;342:1484;Figure adapted from 4Rascol et
al. Mov Disord 1998;13(1):39
P a
t i e n
t s r e q u
i r i n g
s u p p
l e m e n
t a l l e v o
d o p a
( % )
4%
66%
0
20
40
60
80
50.5
Chronic therapy with conventional levodopa is associatedwith the
development of wearing-off and dyskinesia
-
7/28/2019 Boala Pakinson
100/120
Response thresholdDyskinesia threshold
Early diseaseMid-stage disease Advanced disease
Long duration of clinical benefit
Low incidence of dyskinesias
Diminished duration of clinical benefit leads towearing-off
Increased incidence of dyskinesias
Clinical response mirrorslevodopa plasmapharmacokinetic
profile
ON-time is associated withdyskinesias and wearing-off
Levodopa2 4 6
C l i n
i c a
l e f f e c
t
ON
OFF
Levodopa2 4 6
C l i n
i c a
l e f f e c
t
Time (hours)
Levodopa2 4 6
C l i n i c a
l e
f f e c
t
Figure adapted from Obeso et al. Neurology 2000;55(4
Suppl):S13
Time (hours)Time (hours)
Wearing-off
Dyskinesia
In Parkinson s disease, conventional levodopa deliveryleads to
pulsatile stimulation of the brain
-
7/28/2019 Boala Pakinson
101/120
In Parkinson s disease, theability to regulate and
maintain steady levels of dopamine in the brain is
reduced due toprogressingneuronal loss
Deep troughs in plasma levodopa levels lead to
pulsatilestimulation of the brain
The short half-life(60 90 min) of
conventional levodopaleads to peaks and
profound troughs inplasma levodopa levels,which are further
worsened
by intermittent dosing
Olanow et al. Lancet Neurol 2006;5(8):677
In Parkinson s disease, deep troughs in plasma levodopalevels
lead to pulsatile stimulation of dopamine receptors
-
7/28/2019 Boala Pakinson
102/120
Conventionallevodopa
Activated
Unactivated
Normal
Substantia nigra
Striatum
Dopamine receptor state
Nigrostriatal neuronsdegenerate
PD (untreated)Activated
Unactivated
Conventional levodopa
Activated
Unactivated
*Levodopa dose; PD=Parkinson's disease
*
Adapted from Olanow et al. Lancet Neurol 2006;5(8):677
-
7/28/2019 Boala Pakinson
103/120
Normal movement
-
7/28/2019 Boala Pakinson
104/120
-
7/28/2019 Boala Pakinson
105/120
Parkinsonian state
-
7/28/2019 Boala Pakinson
106/120
-
7/28/2019 Boala Pakinson
107/120
Parkinsonian state withintermittent levodopa
-
7/28/2019 Boala Pakinson
108/120
-
7/28/2019 Boala Pakinson
109/120
Parkinsonian state withcontinuous levodopa
-
7/28/2019 Boala Pakinson
110/120
Motor complications associated with chronic levodopa therapymay
be due to pulsatile stimulation of dopamine receptors
-
7/28/2019 Boala Pakinson
111/120
Deep troughs in plasma levodopa levels can lead to
pulsatilestimulation of the dopamine receptors, which, in turn,
may result in
Wearing-off Dyskinesia
How can we avoid deep troughs inplasma levodopa?
Obeso et al. Neurology 2000;55(4 Suppl):S13;Olanow et al. Lancet
Neurol 2006;5(8):677
Dopamine agonists
-
7/28/2019 Boala Pakinson
112/120
Dopamine agonists Dopamine works by stimulating receptors on the
surface of
corpus striatum cells Drugs that also stimulate these cells are
called dopamine
agonists, or DAs DAs may be used before L-dopa therapy, or added
on to avoid
requirements for higher L-dopa doses late in the disease DAs
available in the United States as of early 1998, include
bromocriptine (Permax, Parlodel), pergolide (Permax), and
pramipexole (Mirapex), cabergoline (Dostinex) and ropinirole
(Requip), lisuride (Dopergine) and apomorphine .
Side effects of all the DAs are similar to those of
dopamine,plus confusion and hallucinations at higher doses.
Main advantages: Continuous dopaminergic stimulation DA
treatment complicate with dyskinesias and motor fluctuations
less
thatn levo-dopa
Anticholinergics
-
7/28/2019 Boala Pakinson
113/120
Anticholinergics
Anticholinergics maintain dopamine balance as levelsdecrease
Side effects of anticholinergics (dry mouth,constipation,
confusion, and blurred vision) are usually too severe in older
patients or in patients withdementia.
Anticholinergics rarely work for very long
They are often prescribed for younger patients whohave
predominant shaking. Trihexyphenidyl (Artane) isthe drug most
commonly prescribed.
Acetylcholine in PD
-
7/28/2019 Boala Pakinson
114/120
Acetylcholine in PD
Acetylcholine neurotransmitter involved inmany brain functions
(e.g. memory)
In the striatum : balance between acetylcholine
and dopamine is critical for smooth motorfunction ( striatal
cholinergic interneurons inhibit the medium spiny neurons)
In PD acetylcholine unchanged, dopamine reduced tilts the
balance
Drugs that block acetylcholine transmissionrestore the
balance
The Cochrane Database of Systematic Reviews 2006 Issue
1Copyright 2006 The Cochrane Collaboration. Published by John Wiley
& Sons,
-
7/28/2019 Boala Pakinson
115/120
Ltd.Anticholinergics for symptomatic management of Parkinsons
disease
Katzenschlager R, Sampaio C, Costa J, Lees A
SummaryAnticholinergic drugs can improve movement symptoms of
Parkinson's
disease, but with adverse mental effects, and there is not
enough evidence tocompare the different drugs.
Anticholinergics were the first drugs available for Parkinsons
disease and they arestill widely used. They are believed to work by
counteracting an imbalance whichexists in Parkinsons disease
between two chemicals in the brain which transmitmessages between
nerve cells. However, anticholinergic drugs have beenassociated
with unfavourable side effects. They are used alone, or with other
anti-
Parkinson's drugs. The review of trials found that
anticholinergics can improvemovement problems in people with
Parkinson's disease, but also cause adversemental effects (such as
confusion, memory problems, restlessness andhallucinations). There
is not enough evidence to compare the differentanticholinergic
drugs.
Other drugs
-
7/28/2019 Boala Pakinson
116/120
Other drugs
Amantadine (Symmetrel) is sometimes used as an early therapy
before L-dopa is begun, and as an add-on laterin the disease.
Has an evidence-based antidiskinetic effect Its
anti-parkinsonian effects are mild, and are not seen
in all patients Multiple mechanisms of action, probably the main
one
being the antiglutamatergic effect Clozapine (Clozaril) is
effective especially against
psychiatric symptoms of late PD, including psychosisand
hallucinations; newer quetiapine (Seroquel)
-
7/28/2019 Boala Pakinson
117/120
Duodopa
-
7/28/2019 Boala Pakinson
118/120
Duodopa
Intestinal gel containing levo-dopa Avoids absorbtion problems
Can be titrated precisesly by the pump
Usually substitutes all other PD treatments High efficacy
Disadvantage: pateints have to carry the pump
with them Advantage: can be used when DBS iscontraindicated
(e.g. cognitive disturbance,depression)
PD prognosis
-
7/28/2019 Boala Pakinson
119/120
PD prognosis
Despite medical treatment, the symptoms of Parkinson disease
worsen over time, and
become less responsive to drug therapy Late-stage psychiatric
symptoms are often the
most troubling, including difficulty sleeping,
nightmares, intellectual impairment (dementia),hallucinations,
and loss of contact with reality (psychosis).
-
7/28/2019 Boala Pakinson
120/120