Benefit Trends: Evaluating Consumer-Based Models
Presented By:
Christopher J. DeLoreyPresident
Telamon Insurance & Financial [email protected]
617-614-1215

Key Points
Factors driving trends
Employer options
Employee perspective
Consumer Driven Health Plans (CDHP)
What’s next?

Factors Driving Trends
Rising Health Insurance Costs
The national average for medical plan rate increases is 15% to 20%
These increases are driving employers to look for solutions
Fueling interest in consumer models

Factors Driving Trends
Health Care Cost Drivers:◦ Skyrocketing Rx costs
◦ Rising hospital and physician costs
◦ Advances in technology
◦ Increase in chronic conditions
◦ Increased utilization
◦ Aging population
◦ Lack of consumer involvement in purchase

Factors Driving Trends
In 1960, consumers paid for 50% of health care costs
In 2003, they pay for only 15%
Consumers don’t know the true costs of health care

Factors Driving Trends
Entitlement Perspective in America◦ Corporations are bottomless pits
◦ Unrestrained desires
◦ Employees are unaware of the actual costs
◦ “Want it All” for a $10 co-pay

Employer Options
Medical Cost Outlook ◦ Impossible for employer to pay for all the future drug/medical
technology and services desired by employees
◦ Employers have a few options:• Drop coverage• Absorb the cost• Pass on the premium increase to employees• Reduce coverage• Offer a consumer-based model

Employer OptionsMoving Toward Consumer Models ◦ Determine level of medical benefits needed to recruit/retain
employees
◦ Provide a menu of group medical options
◦ Set employer subsidies based on efficient plans or base year subsidy level
◦ Encourage employees to select efficient medical plans
◦ Motivate employees to “own” their personal health status
◦ Facilitate employee use of pre-tax flexible spending accounts

Employee Perspective
Educate them on health care costs
Educate them on products
Provide them tools

Employee Perspective
Are Your Employees Ready for Consumerism?◦ 87% of employees confident in choosing a health plan
◦ 70% of employees understand how to navigate the health care delivery system
◦ 87% willing to take on more responsibility for researching, choosing, and maintaining their health coverage
◦ 49% want full responsibility for purchasing their own health care coverage

Consumer Driven Health Plans (CDHPs)
A concept, not a product
Often referred to as “consumerism”
Engages the consumer in making health care decisions and purchases
Encourages better health
Many variations

History of CDHPs
MERPS (Medical Expense Reimbursement Account)◦ Allowed tax-free reimbursement to employees
◦ 100% employer-funded
◦ Sometimes called 105(h) plan or direct reimbursement plan
◦ Uncertainty as to ability to rollover unused funds or spend downs
◦ Typically did not include any health tools or health assessments

History of CDHPs
Health Flexible Spending Accounts◦ Allowed for tax-free reimbursement to employees
◦ Typically funded via employee salary deduction or flex credits
◦ No rollover allowed
◦ Individual insurance premium ineligible

Web-Based Resources & CDHPs
Carrier Resources◦ Current balances
◦ Claims activity
Medical Libraries◦ Johns Hopkins
◦ First Data Bank
◦ Reuters News
◦ The Natural Pharmacist
Personal Health Tools◦ Health risk assessments
◦ Health calculators
◦ Personal health records
◦ Drug interaction information
Provider Search
Healthcare Prices◦ Diseases/conditions
◦ Procedures and providers
◦ Visits
◦ Prescription drugs
Marketplace◦ Online shopping

Types of Consumer Driven Health Plans
Popular emerging options:◦ Defined Contribution Plans
◦ Health Reimbursement Accounts (HRAs)
◦ Health Flexible Spending Accounts (FSAs)

Defined Contribution Plans
Defining the contribution employers will spend and passing the rest of the cost onto the participant
An employer gives employees a fixed sum of money to purchase one of several healthcare plans; if an employee chooses a plan that costs more than the amount provided by the employer, the employee pays the difference

Defined Contribution Plans
Establish a high deductible plan which is partially funded by the employer; any employer monies not spent by the end of the year may be rolled over to the next year
Employer defines the amounts of reimbursement to providers, thus encouraging the participant to negotiate directly with provider to accept the plan’s reimbursement as payment in full

Defined Contribution Plans
Add additional co-pays for care at more expensive
facilities
Providers are grouped into mini-networks based on
cost/quality; employee pays a higher contribution in
order to access higher cost providers (Patient Choice
Model)

Defined Contribution Plans
ProEmployees◦ May have choice of plans
◦ Become better consumers
Employers◦ Predictable cost
ConsEmployees◦ Member responsibility
◦ May be more involved in negotiating with providers
Employers◦ Potentially complex
enrollment
◦ Employee education

Health Reimbursement Arrangements (HRAs)
IRS Sec. 105 Plans
Allows employer to reimburse employees tax free for medical expenses

HRAs - Financing
HRAs must be paid by employers
HRAs may be unfunded or funded
◦Typically, employers use unfunded “credits”
HRAs may accept some after-tax employee contributions
(e.g., COBRA premiums)
HRAs may not accept pre-tax employee contributions,
either directly or indirectly
Use of debit cards when employer pays first

HRAs - Reimbursement
HRAs can reimburse deductible “medical expenses”
◦ Health expenses not reimbursed by other plans
◦ Health insurance premiums (including LTC, unless HRA is a
health FSA)
HRAs can’t reimburse non-health expenses
◦ Can’t pay bonus, severance, or death benefits
◦ Can’t reimburse premiums paid with pre-tax dollars

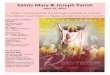
How Does a High Deductible Plan Work?
Either member or HRA
pays first
100% for preventive
Rollover of account is an
option
Member Responsibility
HRA
Preven
tive 100%
Deductible
Health Coverage

HRAs and COBRA
HRAs are subject to COBRA rules
Issues to consider:◦ Notices
◦ Elections
◦ Reimbursement amounts
◦ Duration of coverage
◦ Premiums
Non-Discrimination rules apply

Coordinating HRAs with High-Deductible Plans
An HRA may be offered as a stand-alone option◦ Employees can be required to elect high-deductible coverage to
receive an HRA
◦ Employees can pay for the high-deductible coverage with pre-tax contributions (but can’t subsidize HRA coverage with pre-tax dollars)
HRAs may be coordinated with high-deductible health plansNo fixed coordination rules; typically, HRA pays first and covers same expenses as high-deductible plan

HRAs and the Rollover Feature
Provides incentive to save for future needsIf an employee knows they are leaving they may spend quickerPrevious rollovers may encourage higher dollar claim submissionBe aware of “look back loophole” (HRAs can cover expenses from previous years)How do you have a COBRA premium “actuarially determined?”How do employees get health care cost information?Can create a future liability for plan (plan can cap the rollover)

EducationEducation
EducationEducation
CommunicationCommunication
Personal Health Management ToolkitOnline provider information
Online prescription drug cost informationHealth Risk Appraisals24-hour nurselineeWellness program
Preventive Care Covered 100%
Prescription & OTC Alternative Drugs
Covered 70%
Personal Care Account$1,000 Employee only
$1,500 Employee + 1 dependent$2,000 Employee + 2 or more dependents
Bridge – Employee Deductible$2,000 Employee only
$3,000 Employee + 1 dependent$4,000 Employee + 2 or more dependents
Catastrophic Health Coverage90/70 PPO Plan
Designed to encourage network utilization
Preventive care is carved out of the program and is
provided at 100%
The employer funds this portion
The employee funds this portion
Employer and employee share the premium cost of this traditional
PPO plan
Prescription drugs carved
out and provided on a coinsurance
basis
Employee uses this first to cover healthcare expenses. Unused
portions are carried over to next plan year.
Once the PCA is exhausted, employee is responsible for 100% of
healthcare expenses until the maximum is
reached.
PPO plan covers employee after
bridge deductible is met.

HRA Pros and Cons
ProEmployees◦ Rollover of unspent funds
◦ Employee directs own care
◦ Preventive coverage
◦ Decision support tools
Employers◦ Less involved in coverage
◦ Cost control
◦ Shares risk of cost/utilization w/employee
ConsEmployees◦ Member responsibility
◦ Cost, if chronic disease
Employers◦ Adverse selection
◦ Actual cost savings
◦ Accuracy of actuarial assumptions
◦ High HRA administrative cost

Health Flexible Spending Accounts (FSAs)
Allowed for tax-free reimbursement to employees
Typically funded via employee salary reduction
No rollover allowed
Individual insurance premiums ineligible for reimbursement

HRA Coordination with Health FSAs
HRAs may be offered in lieu of FSAs
HRAs may be offered in addition to FSAs
Coordination rules◦ Health FSA may reimburse expenses before the HRA is
exhausted if written into both plan documents
◦ FSA can also pay first if expenses are different expenses than HRA

HRA – FSA Rules Ignored
HRAs are not subject to “use-it-or-lose-it” rule◦ Permits carry forward of unused amounts
◦ Accumulations may be capped
◦ Terminated employees may spend down accumulations
HRAs are not subject to “uniform coverage” rule◦ Permits HRA credits/contributions to accrue by payroll period, or
less frequently (e.g., monthly, quarterly, semi-annually)

Health Savings Accounts (HSAs)
Tax deduction for amounts contributed
Employer and employee contributions
Must offer with high deductible health plan
May not be covered by any other health plan
Self employed individuals are eligible
May include in cafeteria plan

HSA Pros and Cons
ProsEmployees◦ Rollover of unspent funds◦ Own account◦ Can reimburse some
insurance premiums◦ Can save tax free for later
use
Employers◦ Limits liability◦ Employees may put cost
pressure on health care providers
◦ Employer contribution may be used as employee incentive
◦ Employer contributions not subject to FICA
ConsEmployees◦ More cost sharing
◦ New information to learn
◦ Must take more responsibility
Employers◦ Requires a high deductible
plan
◦ Trustee requirement can add cost and complexity
◦ HDHPs may cause employee resentment
◦ Can’t control employer contributions

HSAs – Open Issues
Claims adjudication & substantiation
ERISA
DOL claims rules
COBRA
HIPAA

Comparison of HSA, HRA, FSA:HSA
(Health Saving Account)
HRA
(Health Reimbursement Arrangement)
FSA
(Health Flexible Spending Account)
Account Overview Tax Exempt trust or custodial account created to pay for the qualified medical expenses of the account holder and his/her spouse or dependents.
An employer funded account used to reimburse employees for qualified medical care expenses.
A cafeteria plan authorized under Section 125 of the IRC. FSAs can be created to reimburse for qualified medical expenses, health insurance premiums for Premium-only account, or dependent care expenses.
High Deductible Health Plan? (HDHP)
Required Customary Not Required
Who can fund the account? High Deductible Health Plan?
Employee and/or Employer Employer Only Typically only the Employee. However, Employer can also contribute
Are there any contribution limits?
$2,900 | $5,800 F **
Catch-up contributions: $900/yr – age 55 by end of tax year. Reduced by MSA contributions in same year
There are no limits to the amount an employer can contribute.
There are no limits to contributions for a health care FSA. However, employers typically set a limit.
Who owns account? Participant Employer Employer

Comparison of Tax-Advantaged Accounts:HSA HRA FSA
Can unused funds be rolled over from year to
year?
Yes Yes, subject to COBRA No, but in some cases employee may elect COBRA through end of plan year.
What expenses are eligible for
reimbursement?
Section 213 (d) medical expenses
-COBRA premiums
-QLTC premiums
-Health premiums while receiving unemployment benefits
-If Medicare eligible due to age, health insurance premiums except medical supplement policies.
Section 213 (d) medical expenses
Health Insurance premiums for current employees, retirees, and qualified beneficiaries, and QLTC premiums. Employer can define “eligible medical expenses”
Section 213 (d) medical expenses
Expenses for Insurance premiums are not reimbursable
Employer can define “eligible medical expenses”
Must claims submitted for reimbursement be
substantiated?
No Yes Yes
May account reimburse non-medical expenses?
Yes, but taxed as income and 10% penalty (no
penalty if distributed after death, disability, or eligible
for Medicare)
No No
Is interest earned on tax-advantaged account?
Yes, accrues tax-free Yes, paid to the employer No

Comparison of HSA, HRA, FSA Continued…
HSA
(Health Savings Account)
HRA
(Health Reimbursement Arrangement)
FSA
(Flexible Spending Account)
Is plan Year Carry Over Allowed?
Yes Employer Choice Employer
Is fund portable? Yes Employer Choice No
Substantiate claims to withdraw money?
No No No
How are Allowable Medical Expenses
Determined?
Medical IRC 213 (d), Some premiums, non
medical
Medical IRC 213 (d), Some Premiums, non
medical
Medical IRC 213 )d)
Uniform Coverage No Employer Choice Required
Applicable IRC Section 223 Section 105 Section 125

Comparison of FSA, HRA and HSA
FSA HRA HSA
Eligibility All Employees All Employees Anyone not eligible for Medicare
Contributions Employer and/or employee Employer Employer and/or employee
Contribution Limits None None Generally the less of annual deductible or $2,650 single/$5,250 family for 2005
Tax Status of Contribution
Excluded for employee Excluded for employee Deductible for employee and employer
Roll-over No Yes, but not required Yes
Portability None Depends on Plan Full
Withdrawals allowed Qualified medical Qualified medical and premium Qualified medical, limited premiums; penalty for other

Where Are We?93% of US companies offer some type of health promotion program (Hewitt Associates 7/02)
First view of 2002 CDHP customers cut cost increases by 60% with greater consumer incentives and choice (Humana SmartSuite)
PricewaterhouseCoopers' touts:◦ Reductions in number of Rx & office visits by 5% - 25%
◦ Overall utilization dropped 10%
◦ First year health care trend was in the range of 5% to 10%
58% of HMOs either have or plan to have a CDHP within 1 year (Milliman 2003 Intercompany Rate Survey)

What’s Next?
We need to start somewhere…
Develop a strategy
Educate employees on healthcare costs◦ Will help eliminate the “entitlement” perception
◦ It’s “our” money being spent
Explore CDHP plans in our market
Create/evaluate contribution strategy

What’s Next?
Employer creates consumerism incentives◦ Encourage employee self-care
◦ Utilize community wellness resources
◦ Tie financial incentives to participation in programs
◦ Maximize disease management programs
◦ Promote Web tools by carriers/TPAs

Review
Factors driving trends
Employer options, status quo won’t work
Employee perspective, ready
Consumer Driven Health Plans (CDHP)
What’s next?

Recommended