Aortic Dissection
Riya Chacko, MD
November 4, 2009

BackgroundPathophysiologyImaging ModalitiesManagement

Incidence 3/100,000 per yearMen more likely to have aortic dissections
compared to women78% have chronic hypertensionPeak for proximal dissection 50-55, distal
60-70At least 20% die before arriving at the
hospital

Michael Ellis Debakey 1908-2008
http://www.nytimes.com/2008/07/13/health/13debakey.html?pagewanted=1&_r=1

High mortality rate: 25% during 1st 24 hours, 70% in 1st week, 80% at 2 weeks for proximal dissections, 10% in distal in 24 hours
Acute versus chronic – present of symptoms within 2 weeks
30% are chronic 50% start in ascending aorta
Khan et al. Chest 2002.

Death from: aortic rupture, aortic regurgitation, branch vessel rupture
75% of proximal untreated aortic dissections will rupture into pericardium, left pleural cavity, and mediastinum

Pathophysiology
Medial degeneration Intimal tear

Disorders Associated with Increased Risk
Hypertension Marfan’s – most common cause of dissection in patients
<40 years of age Ehlers-Danlos syndrome Turner’s syndrome Biscupid aortic valve Cocaine Trauma Pregnancy Noonan syndrome Aortitis Aortic coarctation

Trauma

Double Barrel Sign – Aortic Disruption

Presentation
Von Kodolitsch et al studied 3 variables: mediastinal widening, acute onset chest pain, and BP differential.
Dissection probability high with any combo of 3 or isolated pulses/BP differential (>83%)
Aortic pain 31%Mediastinal widening 39%Absence of all 37%

IRAD registry: Severe sharp pain
84.8% 31% nonspecific
EKG changes 12.7% presented
with syncope

Golledge et al. Lancet 2008.

Variants of Acute Aortic Syndromes
Aortic intramural hematomaAortic ulceration

Aortic intramural hematoma
No intimal flap Rupture of vasa vasorum Occurs in 10-15% acute aortic
syndromes Descending thoracic aorta Atherosclerosis Crescentic shape Can result in pseudoaneurysm High incidence of aortic
rupture, prognosis SAME as dissection
Ascending hematoma same risk as ascending dissection

Intramural Hematoma
On TEE, see localized thickening of aortic wall >7 mm, echo-free spaces within the aortic wall, centrally displaced calcium, or absence of dissection flap/communication
MRI can detect age of the hematoma (methemoglobin)
30-47% will lead to dissection, tamponade, or aortic rupture
Pseudoaneurysm 20-45%
Hematoma <1.0 cm better prognosis

Aortic Ulceration
2.3-7.6% of acute aortic syndromes
Also seen in elderly patients with hypertension, severe atherosclerosis
Descending thoracic aorta (AAA) Ulcer crater with thickened aortic
wall extending from elastic lamina to media
May lead to aneurysms and/or dilation
Less commonly dissections Rare to have thromboembolism MRI most accurate 40% lead to aortic rupture

Khan et al. CHEST / 122 / 1 / JULY, 2002

Classification of Aortic Dissections
Golledge et al. Lancet. 2008.

Copyright ©2007 BMJ Publishing Group Ltd.
Ince, H. et al. Heart 2007;93:266-270
Figure 1 Classification of distal or proximal aortic dissection. De Bakey: type I, originates in the ascending aorta, propagates at least to the aortic arch and often beyond it distally; type II,
originates in and is confined to the ascending aorta; type III, originates in the descending aorta and extends distally down to the aorta or, rarely, retrograde into the aortic arch and ascending aorta. Stanford: type A, all dissections involving the ascending aorta, regardless of the site of origin; type B, all dissections not involving the ascending aorta. Adapted from Nienaber et al.3

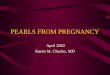
Aortogram in a Patient with a Type A Aortic Dissection. The anterior view is shown. The well-opacified true lumen (T) and the poorly opacified false lumen (F) are separated by an intimal flap (I), which is visible in some parts of this image as a thin radiolucent line within the aorta. In addition, the proximal portions of both coronary arteries are well visualized. Cigarroa JE, Isselbacher EM et al. NEJM. Volume 328:35-43 January 7, 1993 Number 1

Ascending aortic dissections posterior and to the right, above the right coronary artery ostium
Descending aortic dissections posterior and to the left, more commonly affecting left renal and left iliofemoral arteries

Organ Involvement
Cardiovascular Neurologic

The left oblique view is shown. The aortic root is dilated. The true lumen (T) and the false lumen (F) are separated by a faintly visible radiolucent line, which is the intimal flap (I). Note the abundance of contrast agent in the left ventricle (LV), which is indicative of substantial aortic insufficiency.

Cardiac Involvement
Aortic regurgitation in 18-50%Pericardial effusion most commonly from
transudation of fluid through intact false lumen, NOT rupture or leak
Regional wall motion abnormalities 10-15% due to low coronary perfusion
38% of patients have pulse differential (right and left arm)
31-60% have EKG changes

Mechanism of Aortic Regurgitation


Neurologic Involvement
Stroke 5-10% of all aortic dissectionsSpinal cord ischemia in 10% with distal
involvementIntercostal arteries, artery of Adamkiewicz
and thoracic radicular arteries

The Aortic Dissection
Distinguishing true and false lumen False lumen has spontaneous echo contrast
with delayed/reverse flow Thrombus only in false lumen – usually distal to
entry site True lumen expands during systole,
compressed during diastole False lumen usually larger (not always true) Color flow: true lumen forward systolic flow,
false lumen variable



Thrombus in False Lumen

Imaging Modalities To Assess Dissections
CTMRI TEETTE

Goals of Imaging

Barbant et al reported in 1992 results from CT, MRI and TEE
PPV for all three in high-risk patients >85%
In low-risk patients, PPV <50% for CT and TEE but 100% for MRI
NPV high for all three >85%

Cigarroa JE, Isselbacher EM et al. NEJM. Volume 328:35-43 January 7, 1993 Number 1


CT
Sensitivity for ascending aorta <80% but up to 94% in descending and 87-100% specific overall
Limitations: use of IV contrast, identifying intimal tear, branch vessel involvement, aortic regurgitation
Helical CT superior

MRI
Sensitivity and specificity 95-100%Limitations: lack of immediate availability,
scan timing, restricted vitals monitoring

MRI of the Ascending Aorta in a Patient with a Type A Aortic Dissection. The coronal plane is shown. The aortic root (AR) and the pulmonary artery (P) are visualized. In the ascending aorta an intimal flap (I) separates the true (T) and false (F) lumens.

TTE
Sensitivity 35-80%Specificity 39-96%

Xray
30-60% have mediastinal wideningBulges to the right with ascending and left
with descendingLeft pleural effusion

TEE
Sensitivity 98% Specificity 63-96% Identifies: entry site with intimal flap, thrombus,
abnormal flow, involvement of coronary and arch vessels, pericardial effusion, aortic valve regurgitation, left ventricular function
Limitations: operater experience, limited to thoracic and proximal abdominal aorta (cannot see below the celiac trunk), also “blind spot” proximal aortic arch where trachea and left mainstem bronchus along between esophagus and aorta






Methods by TEE of Assessing Aorta
Understand relationship of aorta to esophagus – distal arch, aorta is anterior to the esophagus, at diaphragm aorta is posterior to the esophagus
Communicating location – try to identify relative to known surgical structures (ie aortic valve, subclavian artery) versus incisors (less helpful to surgeons, helpful for serial exams)
Focus on area just above aortic valve (Type A) and area just beyond left subclavian (Type B)
Difficult to assess distal aortic arch because of trachea (between aorta and esophagus)

Ascending Aorta
30-35 cm from incisors Start at 0 ME 5 chamber view Spin to 40-60 for AV short axis Spin to 90-120 AV long axis – measure sinus of
Valsalva and ST junction Slowly withdraw to see additional 2-3 cm of
ascending aorta Beware of swan catheters (artifact) Decrease to 60 then 0 and withdraw

Descending Aorta
Adjust depth to 6-8 cm so descending aorta enlarged
Advance to stomach, rotate and spin to 90 degrees, slowly withdraw gradually rotating

Intimal tear in 70% of dissections occurs 1-3 cm above sinus of Valsalva
20-30% at ligamentum arteriosumEntry site can be identified 88% of the time
(Adachi et al.)

Differentiating Intimal Tear vs. Reverberation
Intimal TearReverberation
Undulates with cardiac cycle
Distinct borders
Crosses anatomic borders
Blurred borders
Does NOT undulate


Preferred Imaging Modalities
Moore, A. et al. Am J Cardiology, 89:1235-1238, 2002


Medical Treatment
B-blocker + nitroprusside (Beta-blocker 1st) or
Labetalol (alpha and beta-blocker)

Surgical Treatment
Operative mortality 5-10%, higher if complications present
Goal is to replace the ORIGIN of dissection, not entire involved segment
Mortality of surgery higher than medical therapy in Type B dissections
15% treated surgically require a 2nd operation

Copyright ©2007 BMJ Publishing Group Ltd.
Ince, H. et al. Heart 2007;93:266-270
Figure 2 Fourteen-day mortality in 645 patients from the International Registry of Aortic Dissection (IRAD) registry stratified by medical and surgical treatment in both type A and B
aortic dissection. Adapted from Hagan et al.1

Endovascular Stents
Success rate of 76-100% with 25% 30-day mortality
Palliative or those unsuitable for surgery
13% of aortic dissections receive stents

Proximal Dissection Followup
65-80% survival if treated at 5 years40-50% at 10 years

Distal Dissection Follow up
75% survival regardless of medical/surgical management if treated

Recommended