Anti-CD38, SLAMF-7 and BiTE immunotherapy: Are immune therapeutics ready for the frontline?
AlexanderM.Lesokhin,M.D.AssistantMember,MyelomaServiceMemorialSloanKetteringCancerCenter,NewYork

Disclosures
• ConsultingforBristolMyersSquibb,Janssen,Aduro,andJuno
• ResearchFunding:BristolMyersSquibb,Genentech,CelgeneandJanssen
• Royalties:Serametrix,inc.

Overview
• MonoclonalAntibodiesHaveTransformedRelapsedMMTherapy
– Anti-CD38singleagentandcombinationdata– Anti-SLAMF7combinationdata
• EmergingdataformAbsearlierinMMnaturalhistory
• mAbbasedproductsonthehorizon

Anti-CD38

• Human CD38 IgG1κ monoclonal antibody
• Direct and indirect anti-myeloma activity1-5
• Depletes CD38+ immunosuppressive regulatory cells5
• Promotes T-cell expansion and activation5
Daratumumab Mechanisms
1. Lammerts van Bueren J, et al. Blood. 2014;124:Abstract 3474. 2. Jansen JMH, et al. Blood. 2012;120:Abstract 2974. 3. de Weers M, et al. J Immunol. 2011;186:1840-8. 4. Overdijk MB, et al. MAbs. 2015;7:311-21. 5. Krejcik J, et al. Blood. 2016. Epub ahead of print.

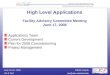
Daratumumab Single Agent: GEN501 Ph I/II and SIRIUS Ph II Pooled
• Daratumumab as a single agent1,2 – Approved by FDA and by EMA in
relapsed/refractory multiple myeloma
• Patients received a median of 5 prior lines of therapy
– 86.5% of patients were double refractory to a proteasome inhibitor (PI) and immunomodulatory drug (IMiD)3
• Combined overall response rate (ORR):31%3
• Median overall survival (OS) of 20.1 months3
– 2-year OS was ~75% in responders – Median OS was 18.5 months in MR/SD
patients
1. Lokhorst HM, et al. N Engl J Med. 2015;373:1207-19. 2. Lonial S, et al. Lancet. 2016;387:1551-60. 3. Usmani SZ, et al. Blood. 2016. 128 (1);:37-44
MR, minimal response; SD, stable disease; PD, progressive disease; OS, overall survival; CI, confidence interval; NE, not evaluable.
6
RespondersMR/SDPD/NE
RespondersMR/SDPD/NE
MedianOS=NE(95%CI,NE-NE)
MedianOS=18.5months(95%CI,15.1-22.4)
MedianOS=3.7months(95%CI,1.7-7.6)
PaAe
ntsA
live(%
)
100
75
50
25
0
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28Months
No.atrisk
467725
467416
466712
456311
44577
43537
43485
41454
40384
39344
28203
1282
1241
210
000*FDAapproved11/2015forrefractorymyelomaaRer3therapies

POLLUX study: design and endpoints
DimopoulosetalNEJM2016

CASTOR study: design and endpoints
PalumboetalNEJM2016

Daratumumab Combination with Lenalidomide or Bortezomib Improves Outcome in Early Relapse
DimopoulosMA,etal.NEnglJMed.2016(updatedASH2017);PalumboA,etal.NEnglJMed.2016(updatedASH2017)
POLLUX(ITT)MedianFollowup:32.9months
CASTOR(ITT)MedianFollowup:19.4months

Addition of Dara in Early Relapse Resulted in Deeper Responses
Dimopoulosetal,ASH2017;Avet-LoiseauH,etal.ASH2016
PolluxTrial

Daratumumab Associated Toxicities
• InfusionReactions– 48%(5%G3/4)inPOLLUXtrial– 45%(8.6%G3/4)inCASTORtrialHemeToxicities*(%) DRd Rd DVd VdNeutropenia 51.9 37.0 12.8 4.2Thrombocytopenia 12.4 13.5 45.3 32.9Lymphopenia 5.3 3.6 9.5 2.5
*Grade3and4
Non-HemeToxicities*(%) DRd Rd DVd VdNeuropathy NR NR 47.3 37.6Diarrhea 42.8 24.6 31.7 22.4Fatigue 35.3 27.8 21.4 24.5Infection(G3orG4) 28.3 22.8 21.4 19.0Upperrespiratoryinfxn 31.8 20.6 24.7 18.1Pneumonia 14.1 13.2 11.9 11.8
*Allgrade,unlessotherwisestated
DimopoulosMA,etal.NEnglJMed.2016;PalumboA,etal.NEnglJMed.2016

HemeToxicities*(%) DRd Rd DVd VdNeutropenia 51.9 37.0 12.8 4.2Thrombocytopenia 12.4 13.5 45.3 32.9Lymphopenia 5.3 3.6 9.5 2.5
*Grade3and4
Non-HemeToxicities*(%) DRd Rd DVd VdNeuropathy NR NR 47.3 37.6Diarrhea 42.8 24.6 31.7 22.4Fatigue 35.3 27.8 21.4 24.5Infection(G3orG4) 28.3 22.8 21.4 19.0Upperrespiratoryinfxn 31.8 20.6 24.7 18.1Pneumonia 14.1 13.2 11.9 11.8
*Allgrade,unlessotherwisestated
Daratumumab Associated Toxicities
• InfusionReactions– 48%(5%G3/4)inPOLLUXtrial– 45%(8.6%G3/4)inCASTORtrial
DimopoulosMA,etal.NEnglJMed.2016;PalumboA,etal.NEnglJMed.2016

HemeToxicities*(%) DRd Rd DVd VdNeutropenia 51.9 37.0 12.8 4.2Thrombocytopenia 12.4 13.5 45.3 32.9Lymphopenia 5.3 3.6 9.5 2.5
*Grade3and4
Non-HemeToxicities*(%) DRd Rd DVd VdNeuropathy NR NR 47.3 37.6Diarrhea 42.8 24.6 31.7 22.4Fatigue 35.3 27.8 21.4 24.5Infection(G3orG4) 28.3 22.8 21.4 19.0Upperrespiratoryinfxn 31.8 20.6 24.7 18.1Pneumonia 14.1 13.2 11.9 11.8
*Allgrade,unlessotherwisestated
Daratumumab Associated Toxicities
• InfusionReactions– 48%(5%G3/4)inPOLLUXtrial– 45%(8.6%G3/4)inCASTORtrial
DimopoulosMA,etal.NEnglJMed.2016;PalumboA,etal.NEnglJMed.2016

HemeToxicities*(%) DRd Rd DVd VdNeutropenia 51.9 37.0 12.8 4.2Thrombocytopenia 12.4 13.5 45.3 32.9Lymphopenia 5.3 3.6 9.5 2.5
*Grade3and4
Non-HemeToxicities*(%) DRd Rd DVd VdNeuropathy NR NR 47.3 37.6Diarrhea 42.8 24.6 31.7 22.4Fatigue 35.3 27.8 21.4 24.5Infection(G3orG4) 28.3 22.8 21.4 19.0Upperrespiratoryinfxn 31.8 20.6 24.7 18.1Pneumonia 14.1 13.2 11.9 11.8
*Allgrade,unlessotherwisestated
Daratumumab Associated Toxicities
• InfusionReactions– 48%(5%G3/4)inPOLLUXtrial– 45%(8.6%G3/4)inCASTORtrial
DimopoulosMA,etal.NEnglJMed.2016;PalumboA,etal.NEnglJMed.2016

Daratumumab plus Pomalidomide and Dexamethasone in Relapsed and/or Refractory Multiple Myeloma
ChariA,etal.Blood.2017.
MedianPFS8.8months
PaAe
nt
Timefromfirstdosingdate(months)

Side Effect Profile
• IRRin50%ofpatients;most1stdose• Neutropenia77%G3/4
– Febrileneutropenia8%– G-CSFrequiredin57%
• Infection32%G3/4– Pneumonia9%;Sepsis5%
• Upperrespiratorytractinfections29%
ChariA,etal.Blood.2017.

Daratumumab - Infusion time
• Acceleratedinfusionstartingwith3rddose– 90minuteinfusionstartingwith3rddose(Barretal,Leukemia2018)
• Dara-rHuPH20(PAVOtrial)PhI/II(Charietal,ASCO2018)– Recombinanthyaluronidaseformulationpermitssubqinjection– 25patientstreatedat1800mg/15mlsubq
• 12%Infusionrelatedreactions;8%neutropenia
• 44%ORR;28%VGPR– PhaseIIIcomparingIVandscformulationaccruing(NCT03277105)

Anti-SLAMF7

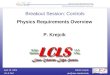
Elotuzumab: Immunostimulatory Mechanisms of Action
TheimmunomodulatorydrugsmaysynergizewithelotuzumabthroughmultiplemechanismstoincreasethekillingofMMcells
ADCC, antibody-dependent cell cytotoxicity; ADCP, antibody-dependent cellular phagocytosis; FcγR, Fc gamma receptor; NK, natural killer; SLAMF7, signaling lymphocytic activation molecule F7 1. Hsi ED et al, Clin Cancer Res 2008 and Tai YT et al, Blood 2008. 2. Balasa B et al, Cancer Immunol Ther 2015. 3. Collins SM et al, Cancer Immunol Ther 2013 and Pazina T et al, Oncoimmunology 2017. 4. Pazina T et al, EHA 2018 [PS1277]. 5. Kurdi AT et al, Mol Cancer Ther 2018. 6. Chen J et al, Nature 2017
NK
MM
Macrophage-mediated ADCP of MM cells NK-cell activation
through SLAMF7
MM cells tagged for recognition; mediation of
cell death via ADCC
NK-cell activation through CD16 (FcγR)
2
3 4
Macrophage
5
6
1
SLAMF7 Elotuzumab FcγR
Immune enhancement MM cell killing

Blood2012,120(3):552-559
• Maximumtesteddoseof20mg/kgwithoutDLT• Stabledisease(26.7%)
LancetHematology2015,2:e516-27
• 73paAentstreatedwithcombinaAonelotuzumab,lenalidomide,dexamethasone• 10mg/kgand20mg/kgcohorts• 84%responserate(92%in10mg/kgcohort)• PFSimprovedrelaAvetohistoricallenalidomide/dexamethasonedata
Elotuzumab

ELOQUENT-2—Len/Dex ± Elotuzumab: Design
• Elotuzumab*10mg• Cycles1-3d1,8,15,22• Cycle4+d1,15
• Lenalidomide25mgd1-21• Dexamethasone40mgweek
w/o• Elotuzumab8mgIV+28mg
POw/Elo
• Lenalidomide25mgd1-21• Dexamethasoned1,8,15,22
PrimaryEnd-Points:PFS,ORR
SecondaryEnd-Points:
Timetotumorresponse,duraAonofresponse,HRQoL,safety
Cyclesrepeatedun?ldiseaseprogression,unacceptabletoxicity,orwithdrawal
LonialetalNEJM2015

3-yearPFS 5-yearPFSElotuzumabgroup:26% 18%Controlgroup: 18% 12%
ELOQUENT-2—Len/Dex ± Elotuzumab: PFS
LonialetalNEJM2015

34% 29%
ORR79%*ORR66%
*P<.001 • Commongrade3or4AEswerelymphocytopenia,neutropenia,faAgue,andpneumonia
• InfusionreacAonsoccurredin33paAents(10%)intheelotuzumabgroup
1 ElotuzumabGroup(n=321)
Controlgroup(n=325)
MedianTimeToResponse(IR)–mo 2.8 2.8
MedianDuraAonofResponse(≥PR)-mo
20.73 16.25
0
20
40
60
80
100
Elo-Rd Rd
Res
pons
e R
ate,
%ELOQUENT-2—Len/Dex ± Elotuzumab: response and safety
LonialetalNEJM2015
PR:45%
VGPR:29%
CR:5%
PR:37%
VGPR:20%
CR:9%

ELOQUENT-3 Study Design
a20 mg in patients aged >75 years bDexamethasone was split between oral (28 or 8 mg in patients aged ≤75 or >75 years) and IV (8 mg) doses on days with elotuzumab cFollow-up continued until disease progression; follow-up for survival occurred at least every 12 weeks HR, hazard ratio
An international, open-label, randomized, phase 2 trial (NCT02654132), with a 2-sidedα=0.2 and 85% power to detect a true HR of 0.57
Database lock: Feb 21, 2018 Minimum follow-up: 9.1
months
Endpoints
Primary • PFS by investigator
Secondary • Overall response rate (ORR)
• Overall survival (OS)
Exploratory • Safety
• Duration of response (DOR)
Elotuzumab 10 mg/kg IV
Weekly
Elotuzumab 20 mg/kg IV
Every 4 weeks
Pomalidomide 4 mg orally; Days 1–21
Cycles 1–2 Cycles 3+
EPd
Pd
Dexamethasone 40 mga equivalentb; weekly
Dexamethasone 40 mga orally; weekly
Cycles are 28 days
Pomalidomide 4 mg orally; Days 1–21
Patients with MM
• ≥2 prior lines of therapy
• Refractory to last therapy
• Refractory or relapsed and refractory to lenalidomide and a proteasome inhibitor
• Prior pomalidomide not permitted
Follow-up every 4 weeksc
Dimopolousetal.EHA2018

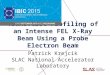
Progression-Free Survival (ITT Definition)
ITT, intent-to-treat; NE, not estimable
60 54 48 46 43 41 37 33 32 27 25 15 7 4 1 1 1 1 1 1 1 1 0
57 51 42 33 31 24 22 20 16 14 10 8 6 3 2 1 1 0 0 0 0 0 0
EPd
Pd
Patients at risk
1.0
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 Time (months)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
Pd
EPd
Prob
abili
ty o
f PFS
EPd n=60
Pd n=57
HR=0.54 (95% CI 0.34, 0.86); p=0.0078
Median PFS
95% CI
10.3 mo 5.6, NE
4.7 mo 2.8, 7.2
• 46% reduction in the risk of progression or death with EPd • Median PFS was more than twice as long with EPd vs Pd
Dimopolousetal.EHA2018

All-Cause Hematologic and Special Interest Adverse Events
EPd (n=60) Pd (n=55) Exposure adjustment No PY=47.7 No PY=34.3 AEs, n (%)a Any grade Grade 3–4 Events/100 PY Any grade Grade 3–4 Events/100 PY
Hematologic AEsb 31 (52) 23 (38) 178 30 (55) 23 (42) 224 Anemia 15 (25) 6 (10) 46 20 (36) 11 (20) 85 Neutropenia 14 (23) 8 (13) 52 17 (31) 15 (27) 73 Thrombocytopenia 9 (15) 5 (8) 23 10 (18) 3 (5) 35 Lymphopenia 6 (10) 5 (8) 21 1 (2) 1 (2) 3
Special interest AEs Infections 39 (65) 8 (13) 182 36 (65) 12 (22) 230 Vascular disorders 8 (13) 2 (3) NR 5 (9) 0 NR Cardiac disorders 7 (12) 4 (7) 17 6 (11) 2 (4) 17 Neoplasmsc 1 (2) 1 (2) 2 12 (22) 6 (11) 38
Second primary malignancy 0 0 NR 1 (2) 1 (2) NR
aIncludes AEs reported between first dose and 60 days after last dose of study therapy; bIncludes hematologic AEs in ≥10% of patients; cIncludes malignant, benign, and unspecified neoplasms NR, not reported
• Neutropenia was less common with EPd vs Pd, despite similar pomalidomide dose intensity • Exposure-adjusted hematologic AEs and infections were lower with EPd vs Pd

Addition of Monoclonal Abs Improves Treatment of Relapsed MM
• DaratumumabadditionimprovesuponLen/DexorBort/DexresponseandPFS
– Activeasasingleagent– Encouragingefficacyinothercombos(PhIIIpending):
• Carfilzomib/dex(84%ORR,CharietalASCO2018)• Pom/DexinRRMM(60%ORR,Charietal,Blood2017)
• ElotuzumabimprovesuponLen/DexorPom/DexresponseandPFS
• BothmAbswelltolerated

Newer myeloma drugs provide better clinical response
Mailankodyetal.NatureReviewsClinOncology2015
DoesmAbbasedtherapyimproveoutcomes?
RVd +/- upfronttransplant2
Transpl armCR:59%CR/VGPR:88%
RVd armCR:48%CR/VGPR:77%
Transpl armMRD10-4:79%
RVd armMRD10-4:65%
KRd withouttransplant3
SinglearmCR:43%CR/VGPR:91%
SinglearmMRD10-5:77%MRD10-6:42%
Modified from Landgren O, et al. Semin Hematolol 2018
CR/VGPRrates
Attaletal,NEJM2017 Korde etal,JAMAOncol 2015,
MRDstatus

Daratumumab in Newly Diagnosed MM
Mateosetal.ASH2017

D-VMP with D Maintenance Improves PFS in Comparison to VMP x 9 cycles
Mateosetal.ASH2017


Charietal.ASH2017
Results • n=22,mediancycles13(range1-13)

Side Effect Profile
• Grade1/2IRRin27%ofpatients–mostly1stdose• 1transientgrade3cardiacfailure
Charietal.ASH2017

Elotuzumab in Newly Diagnosed MM • PhaseIIa:Elo-RVd
– 100%ORR,71%VGPRorbetter(24%CR)Laubachetal.ASCO2017
– Lowrateofgrade3toxicity,however2deathsontrial
• RandomizedStudiesAwaitingReadout:– RVd+/-Elo
• PhIIIinGermany(NCT02495922)• SWOG/NCIPhIIinHRNDMM(NCT01668719)
– Rd+/-Elo• Eloquent1(NCT01335399)

Monoclonal Abs as Drugs ADCC/CDC
– CD38– SLAMF7
FcRegion DrugDelivery
TumorCell
Bi-specifics– BCMA-CD3– CD38-CD3
Abdrugconjugates(ADC)– BCMA
• GSK2857916:60%ORR(n=35)
TargetAn]gen

Engineered Antibodies Targeting BCMA
Taietal.Front.Immunol.,10August2018

Myeloma drug pipeline for clinical practice in the U.S.
Melphalan/prednisone
Highdosemelphalan
Developedin1950sto1980s
Isatuximab
BCMA-ADC
BCMA-CD3
Melflufens.c.Dara
CD38-CD3
Selinexor
CAR-TCells
Ongoingdevelopment
Bortezomib
Thalidomide
Lenalidomide
“Noveldrugs”
2003
2006
Pomalidomide
Carfilzomib
Panobinostat
2012
2013
2015Elotuzumab
Daratumumab
Ixazomib

MyelomaServiceHaniHassoun,MDAlexLesokhin,MDNikolettaLendvai,MDNehaKorde,MDEricSmith,MD,PhDSeanDevlin,PhDShamMailankody,MDOlaLandgren,MD,PhDandteamBMTransplantServiceSergioGiralt,MDHeatherLandau,MDGunjanShah,MDDavidChung,MD,PhDandteam
Myeloma Program at MSKCC MolecularPathologyElliPapaemmanuillab,PhDHematoPathologyAhmetDoganlab,MD,PhDCellularTherapyReneirBrentjenslab,MD,PhDMolecularImagingStevenLarsonlab,MDWolfgangWeberlab,MD,PhDImmunotherapyJeddWolchoklab,MDPhD

Thankyouforyourattention!
AlexanderM.LesokhinAssistantMember
MyelomaServiceandImmunotherapeu]csClinicalCoreMemorialSloanKeaeringCancerCenter
212-639-3069
Recommended