Embed Size (px)
Citation preview

CL IN ICAL STUDIES
XRCC1genetic polymorphismArg399Gln and hepatocellular carcinomarisk: ameta-analysisFei Liu, Bo Li, Yonggang Wei, Lvnan Yan, Tianfu Wen, Jichun Zhao and Mingqing Xu
Department of Liver and Vascular Surgery, West China Hospital, Sichuan University, Chengdu, Sichuan Province, China
Keywords
hepatocellular carcinoma – meta-analysis –
polymorphism – XRCC1
Abbreviations
CI, confidence interval; HBV, hepatitis B virus;
HCC, hepatocellular carcinoma; HCV,
hepatitis C virus; HWE, Hardy–Weinberg
equilibrium; OR, odds ratio; SNP, single
nucleotide polymorphisms; XRCC1, X-ray
repair cross-complementing group 1.
Correspondence
Yonggang Wei, Department of Liver and
Vascular Surgery, West China Hospital, Sichuan
University, 37 Guo Xue Road, Chengdu,
610041, Sichuan Province, China.
Tel: 186 28 85422476
Fax: 186 28 85423724
e-mail: [email protected]
Received 17 October 2010
Accepted 21 February 2011
DOI:10.1111/j.1478-3231.2011.02508.x
AbstractBackground: Studies investigating the association between X-ray repair cross-complementing group 1 (XRCC1) genetic polymorphism Arg399Gln andhepatocellular carcinoma (HCC) risk report conflicting results. The aim ofthis study was to quantitatively summarize the evidence for such a relation-ship. Methods: Two investigators independently searched the Medline, Em-base, CNKI and Chinese Biomedicine Database. Summary odds ratios (ORs)and 95% confidence intervals (95% CIs) for XRCC1 polymorphism and HCCwere calculated in a fixed-effects model (the Mantel–Haenszel method) and arandom-effects model (the DerSimonian and Laird method) when appro-priate. The pooled ORs were performed for a codominant model (Gln/Gln vs.Arg/Arg, Arg/Gln vs. Arg/Arg), a dominant model (Gln/Gln1Arg/Gln vs.Arg/Arg) and a recessive model (Gln/Gln vs. Arg/Gln1Arg/Arg). Results: Thismeta-analysis included 11 case–control studies, which included 2208 HCCcases and 3265 controls. Overall, the variant genotypes (Gln/Gln and Arg/Gln)of Arg399Gln were not associated with HCC risk when compared withthe wild-type Arg/Arg homozygote (Gln/Gln vs. Arg/Arg, OR = 1.01, 95%CI = 0.79–1.28; Arg/Gln vs. Arg/Arg, OR = 1.09, 95% CI = 0.81–1.45). Simi-larly, no associations were found in the dominant and recessive models(dominant model, OR = 1.12, 95% CI = 0.85–1.47; recessive model,OR = 0.99, 95% CI = 0.79–1.25). Limiting the analysis to the studies withinHardy–Weinberg equilibrium, the results were persistent and robust. Whenstratifying for ethnicity, country/region and source of controls, no evidence ofa significant association was observed in any subgroup. No publication biaswas found in the present study. Conclusion: No association is found betweenthe XRCC1 polymorphism Arg399Gln and the risk of HCC.
Hepatocellular carcinoma (HCC), which is the fifth mostcommon cancer and the third leading cause of cancer-related death worldwide, is a global health problem (1).The estimated annual number of cases exceeds 500 000,with a mean annual incidence of around 3–4% (2).Patients with HCC have a poor prognosis, with a 5-yearsurvival rate of 5% in developing countries in 2002 (1)because of the lack of effective therapy in most patients(3). Aetiologically, carcinogenesis of HCC is a complex,multistep and multifactor process, in which many factorsare implicated. As we know, chronic infection withhepatitis B virus (HBV) or hepatitis C virus (HCV) isthe most well-established environmental risk factor forHCC worldwide. However, only a fraction of HBsAgcarriers eventually develop HCC and only 2.5% of HCV-infected individuals develop HCC later in life (4). Theexact mechanism of hepatocarcinogenesis is still incom-pletely understood, and the risk factors for HCC stillneed to be further elucidated.
Human cancer can be initiated by DNA damagecaused by UV, ionizing radiation and environmentalchemical agents. Importantly, to counteract the deleter-ious consequences of the DNA-damaging agents,evolution has moulded a number of DNA repair systemsthat as a whole take care of most of the insults infli-cted on a cell’s vital genetic information. The repairingof different types of DNA damages is importantfor safeguarding genomic integrity (5). Among these,the base excision repair (BER) pathway constitutes theprimary defence against lesions generated by ionizingradiation and strong alkylating agents as well as lesionsformed by endogenous DNA-damaging agents likeviruses (6).
The XRCC1 protein, which is encoded by the X-rayrepair cross-complementing group 1 (XRCC1) gene, isan important component of the BER pathway. XRCC1fixes base damage and DNA single-strand breaks causedby ionizing radiation and alkylating agents by directly
Liver International (2011)802 c� 2011 John Wiley & Sons A/S
Liver International ISSN 1478-3223

interacting with polymerase-b, DNA ligase III and poly(ADP ribose) polymerase (PARP) (7).
The XRCC1 gene is located on chromosome 19q13.2(8), spans a genetic distance of 32 kb, comprises of 17 exonsand encodes a 70-kDa protein consisting of 633 aminoacids (9). Although there are more than 300 validatedsingle nucleotide polymorphisms (SNPs) in the XRCC1gene reported in the dbSNP database (http://www.ncbi.nlm.nih.gov/SNP), three of which are common (10) andlead to amino acid substitutions in XRCC1 at codon 194(exon 6, base C to T, amino acid Arg to Trp, dbSNP no.rs1799782), codon 280 (exon 9, base G to A, amino acidArg to His, dbSNP no. rs25489) and codon 399 (exon 10,base G to A, amino acid Arg to Gln, dbSNP no.rs25487),these non-conservative amino acid changes may alterXRCC1 function. This change in protein biochemistryleads to the supposition that variant alleles may diminishrepair kinetics, thereby influencing susceptibility to adversehealth effects, including cancer.
Over the last two decades, a number of case–controlstudies were conducted to investigate the association be-tween XRCC1 Arg399Gln polymorphism and HCC risk inhumans. But these studies reported conflicting results. Noquantitative summary of the evidence has ever been per-formed. The purpose of this meta-analysis was to quantita-tively summarize the evidence for such a relationship.
Materials and methods
Publication search
We searched the PubMed, Embase, CNKI (China Na-tional Knowledge Infrastructure) and Chinese Biomedi-cine databases for all articles on the association betweenXRCC1 polymorphisms and HCC risk (last search up-date 15 October 2010). The following key words wereused: ‘liver cancer’ or ‘hepatocellular carcinoma’, ‘X-rayrepair cross – complementing group 1’ or ‘XRCC1’ and‘polymorphism’ or ‘variant’. The search was withoutrestriction on language, conducted on human subjects.The reference lists of reviews and retrieved articles werehand searched at the same time. We did not considerabstracts or unpublished reports. If more than one articlewas published by the same author using the same caseseries, we selected the study where the most individualswere investigated.
Inclusion and exclusion criteria
We reviewed abstracts of all citations and retrieved studies.The following criteria were used to include publishedstudies: (i) case–control studies were conducted to evaluatethe association between XRCC1Arg399Gln polymorphismand HCC risk; (ii) sufficient genotypes data were presentedto calculate the odds ratios (ORs) and 95% confidenceintervals (CIs); and (iii) the paper should clearly describeHCC diagnoses and the sources of cases and controls. Themajor reasons for exclusion of studies were (i) no control;(ii) duplicate; and (iii) no sufficient data were reported.
Data extraction
Two investigators (F. L. and Y. W.) extracted informationfrom all eligible publications independently according tothe inclusion criteria listed above. Disagreements wereresolved by discussion between the two investigators. Thefollowing characteristics were collected from each study:first author, year of publication, country/region of thefirst or corresponding author, ethnicity, number of casesand controls, genotyping methods, matching variables,minor allele frequency (MAF) in controls and evidence ofHardy–Weinberg equilibrium (HWE) (Table 1). Differ-ent ethnicities were categorized as Asian and non-Asian.
Statistical analysis
We first assessed HWE in the controls for each studyusing a goodness-of-fit test (chi-square or Fisher’s exacttest), and a Po 0.05 was considered as significantdisequilibrium. The strength of the association betweenHCC and the XRCC1 Arg399Gln polymorphism wasestimated using ORs, with the corresponding 95% CIs.The pooled ORs were performed for a codominantmodel (Gln/Gln vs. Arg/Arg, Arg/Gln vs. Arg/Arg), adominant model (Gln/Gln1Arg/Gln vs. Arg/Arg) and arecessive model (Gln/Gln vs. Arg/Gln1Arg/Arg). We alsocarried out the stratified analyses by ethnicity, country/region, HWE in controls and source of controls.
Both the Cochran’s Q statistic (11) to test for hetero-geneity and the I2 statistic to quantify the proportion of thetotal variation because of heterogeneity (12) were calcu-lated. A P value of more than the nominal level of 0.10 forthe Q statistic indicated a lack of heterogeneity acrossstudies, allowing for the use of a fixed-effects model (theMantel–Haenszel method) (13); otherwise, the random-effects model (the DerSimonian and Laird method) wasused (14). To explore sources of heterogeneity acrossstudies, we performed logistic meta-regression analyses.We examined the following study characteristics: ethnicity,HWE in controls (yes/no), matched controls (yes/no),genotyping methods and study sample size (� 500 and4 500 subjects). Sensitivity analysis was performed toassess the stability of the results.
Several methods were used to assess the potentialpublication bias. A visual inspection of funnel plot asym-metry was conducted. Begg’s rank correlation method (15)and Egger’s weighted regression method (16) were used tostatistically assess publication bias (Po 0.05 was consid-ered statistically significant). All analyses were performedusing STATA software, version 11.0 (STATA Corp., CollegeStation, TX, USA). All the P values were two-sided.
Results
Characteristics of studies
A total of 15 published studies (17–31) with full-textarticles examined the association of polymorphismArg399Gln of the XRCC1 gene with HCC were found,four of which were the dissertations of postgraduate
Liver International (2011)c� 2011 John Wiley & Sons A/S 803
Liu et al. XRCC1 polymorphism and HCC risk

students (27–30). Four studies (17, 29–31) were excludedbecause they investigated the same population of re-ported articles. As summarized in Table 1, 11 eligiblearticles (18–28) [six in English (18–23) and five (24–28)in Chinese] were selected for this meta-analysis, includ-ing 2208 HCC cases and 3265 controls.
There were nine studies of Asian patients, one study ofAfrican patients and one study of Caucasian patients.Studies had been carried out in mainland China, Taiwan,India, Gambia and France. The cases definition used in theindividual studies were pathologically or clinically diag-nosed with HCC. Concerning controls’ selection, fourstudies were from healthy volunteer or blood donor, twostudies from HBV carriers, three studies from hospitalpatients without HCC (mixed by chronic hepatitis virus-positive and -negative individuals) and two studies wereseparately used a healthy population and chronic hepatitisvirus (HBV/HCV) carriers as controls. All studies extractedDNA from peripheral blood and a classic polymerase chainreaction–restriction fragment length polymorphism assaywas used in 10 out of 11 studies. Only one study (18)described the use of positive controls and a differentgenotyping assay to confirm the data. The genotypedistributions among the controls of all studies wereconsistent with HWE, except for three studies (18, 25, 27).
Quantitative synthesis
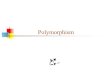
Table 2 lists the main results of this meta-analysis,and Figure 1 shows the association of HCC risk withXRCC1 polymorphism Arg399Gln. Overall, the variantgenotypes (Gln/Gln and Arg/Gln) of Arg399Gln werenot associated with HCC risk when compared with thewild-type Arg/Arg homozygote (Gln/Gln vs. Arg/Arg,OR = 1.01, 95% CI = 0.79–1.28; Arg/Gln vs. Arg/Arg, OR =1.09, 95% CI = 0.81–1.45). Similarly, no associationswere observed in the dominant and recessive models(dominant model, OR = 1.12, 95% CI = 0.85–1.47; reces-sive model, OR = 0.99, 95% CI = 0.79–1.25).
On the basis of the potential overestimation of the trueeffect of the polymorphism on the HCC risk, we strati-fied these studies according to ethnicity, country/region,source of controls and HWE in controls. Because of theinadequate sample populations available for Caucasianand African groups, different ethnicities were categorizedas Asian and non-Asian. Similarly, different countries/regions were categorized as mainland China and others.Different sources of controls were defined as chronichepatitis virus (HBV/HCV) positive and negative. Instratified analyses, the variant genotypes (Gln/Gln andArg/Gln) had no significant relationship with HCC in allof the subgroups, compared with the wild type. Similarresults were observed in the recessive model and thedominant model (Table 2).
Heterogeneity analysis
There was heterogeneity among studies in the overallcomparisons and also subgroup analyses in the heterozygoteTa
ble
1.C
har
acte
rist
ics
of
the
studie
sin
cluded
inth
ism
eta-
anal
ysis
Firs
tau
thor
Ref
eren
ceYea
rC
ountr
y/re
gio
nEt
hnic
ity
Cas
e
Contr
ol(
tota
l)
Gen
oty
pin
gm
ethods
Mat
chin
gcr
iter
iaM
AF
inco
ntr
ol
HW
EC
ontr
ol�
Contr
olw
Kiran
etal
.(1
8)
2009
India
Asi
an63
170
174
PCR–R
FLP
_0.4
2N
oRen
etal
.(2
4)
2008
Mai
nla
nd
Chin
aA
sian
50
92
61
PCR–R
FLP
_0.2
9Yes
Su(2
7)
2008
Mai
nla
nd
Chin
aA
sian
100
111
_PC
R–R
FLP
Age
and
sex
0.2
4N
oW
u(2
8)
2009
Mai
nla
nd
Chin
aA
sian
100
60
_PC
R–R
FLP
_0.3
1Yes
Bore
nta
inet
al.
(19)
2007
Fran
ceC
auca
sian
56
89
_D
irec
tse
quen
cing
_0.4
6Yes
Long
etal
.(2
0)
2006
Mai
nla
nd
Chin
aA
sian
257
649
mix
edco
ntr
olz
PCR–R
FLP
Age,
sex,
race
,H
BV
infe
ctio
nN
AN
AK
irk
etal
.(2
2)
2005
Gam
bia
Afr
ican
216
408
mix
edco
ntr
olz
PCR–R
FLP
Age
and
sex
0.0
8Yes
Chen
etal
.(2
1)
2005
Taiw
anA
sian
577
_389
PCR–R
FLP
Sex
and
year
of
birth
within
10
year
s0.2
6Yes
Yan
get
al.
(25)
2004
Mai
nla
nd
Chin
aA
sian
72
137
mix
edco
ntr
olz
PCR–R
FLP
Age,
gen
der
,ar
ea0.5
2N
oLo
ng
etal
.(2
6)
2004
Mai
nla
nd
Chin
aA
sian
140
536
_PC
R–R
FLP
Age,
sex,
ethnic
ity
0.1
8Yes
Yu
etal
.(2
3)
2003
Taiw
anA
sian
577
_389
PCR–R
FLP
Age,
gen
der
0.2
6Yes
� Contr
ols
ubje
cts
wer
eH
BV
/HC
Vneg
ativ
e(in
cludin
ghea
lthy
volu
nte
eran
dblo
od
donor)
.
wContr
ols
ubje
cts
wer
eH
BV
/HC
Vposi
tive
(incl
udin
ghea
lthy
volu
nte
er,in
pat
ient
and
outp
atie
nt
without
HC
C).
zContr
ols
ubje
cts
incl
uded
am
ixof
HBV
/HC
V-p
osi
tive
and
HBV
/HC
V-n
egat
ive
indiv
idual
s.
HBV,
hep
atitis
Bvi
rus;
HC
V,hep
atitis
Cvi
rus;
HW
E,H
ardy–
Wei
nber
geq
uili
brium
inco
ntr
ol;
MA
F,m
inor
alle
lefr
equen
cy;
NA
,not
avai
lable
;PC
R–R
FLP,
poly
mer
ase
chai
nre
action-r
estr
iction
frag
men
t
length
poly
morp
his
m.
Liver International (2011)804 c� 2011 John Wiley & Sons A/S
XRCC1 polymorphism and HCC risk Liu et al.

Table 2. Stratified analyses of the XRCC1 polymorphism Arg399Gln on hepatocellular carcinoma risk
Variables N�
Gln/Gln vs. Arg/Arg Arg/Gln vs. Arg/Arg Dominant model Recessive model
OR (95% CI) Pw OR (95% CI) Pw OR (95% CI) Pw OR (95% CI) Pw
Total 11 1.01 (0.79, 1.28) 0.19 1.09 (0.81, 1.45) o 0.001 1.12 (0.85, 1.47) o 0.001 0.99 (0.79, 1.25) 0.51
Ethnicity
Asian 9 1.05 (0.82, 1.35) 0.29 1.15 (0.84, 1.59) 0.001 1.19 (0.89, 1.59) o 0.001 1.01 (0.79, 1.29) 0.49
Non-Asian 2 0.64 (0.28, 1.45) 0.10 0.81 (0.32, 2.03) 0.045 0.80 (0.29, 2.19) 0.02 0.80 (0.37, 1.74) 0.21Country/region
Mainland China 6 0.87 (0.58, 1.31) 0.67 1.21 (0.65, 2.28) o 0.001 1.28 (0.81, 2.01) o 0.001 0.82 (0.55, 1.22) 0.90
Others 5 0.96 (0.57, 1.64) 0.06 1.06 (0.89, 1.25) 0.18 0.99 (0.75, 1.31) 0.05 1.09 (0.82, 1.46) 0.22
HWE in controls
Yes 7 1.16 (0.87, 1.53) 0.25 1.04 (0.77, 1.41) 0.005 1.14 (0.84, 1.54) o 0.001 1.15 (0.87, 1.51) 0.67
No 3 0.71 (0.45, 1.12) 0.41 1.25 (0.47, 3.28) 0.003 1.09 (0.48, 2.46) 0.002 0.68 (0.44, 1.06) 0.71
Source of controls
Healthy populationz 6 0.70 (0.45, 1.09) 0.23 1.04 (0.57, 1.88) o 0.001 0.98 (0.55, 1.72) o 0.001 0.69 (0.45, 1.05) 0.51
Hepatitis virus carrier‰ 4 1.17 (0.86, 1.61) 0.19 1.05 (0.88, 1.26) 0.22 0.98 (0.74, 1.31) 0.098 1.16 (0.85, 1.57) 0.43
�Number of comparisons.
wP value of Q-test for heterogeneity test. A random-effects model was used when P value for heterogeneity test o 0.1; otherwise, a fixed-effects model
was used.
zSubjects were chronic hepatitis virus (HBV/HCV) negative.
‰Subjects were chronic hepatitis virus (HBV/HCV) positive.
CI, confidence interval; HBV, hepatitis B virus; HCV, hepatitis C virus; HWE, Hardy–Weinberg equilibrium; OR, odds ratio.
Fig. 1. Forest plots of odds ratios (ORs) with 95% confidence interval (CI) for XRCC1 codon 399 polymorphism and risk for hepatocellular carcinoma.The centre of each square represents the OR, the area of the square is the number of sample and thus the weight used in the meta-analysis, and thehorizontal line indicates the 95% CI. (a) Gln/Gln vs. Arg/Arg. (b) Arg/Gln vs. Arg/Arg. (c) Gln/Gln+Arg/Gln vs. Arg/Arg. (d) Gln/Gln vs. Arg/Gln+ Arg/Arg.
Liver International (2011)c� 2011 John Wiley & Sons A/S 805
Liu et al. XRCC1 polymorphism and HCC risk

comparison (Arg/Gln vs. Arg/Arg) and the dominantmodel. To explore sources of heterogeneity across stu-dies, we assessed heterozygote comparison and dominantmodel comparison by ethnicity, HWE in controls,matched controls, genotyping methods and study samplesize. As a result, matched controls (Arg/Gln vs. Arg/Arg:P = 0.016; dominant model: P = 0.006), but not ethnicity,HWE in controls, genotyping methods or study samplesize, were found to contribute to substantial heterogene-ity. Moreover, meta-regression analyses indicated thatmatched controls could explain 67.30% (Arg/Gln vs.Arg/Arg) and 70.08% (dominant model) of the t2.
Sensitivity analysis
In the sensitivity analysis, the influence of each study onthe pooled OR was examined by repeating the meta-analysis while omitting each study, one at a time. Thisprocedure confirmed the stability of our overall results.In addition, when excluding the studies that were not inHWE, the results were persistent and robust (Table 2).
Publication bias
Funnel plot, Begg’s and Egger’s tests were performed toevaluate publication bias of the literature on HCC. Figure2 displays a funnel plot that examined the XRCC1polymorphism and overall HCC risk included in themeta-analysis in the homozygote comparison. The shapeof funnel plots did not reveal any evidence of funnel plotasymmetry. The statistical results still did not showpublication bias (Gln/Gln vs. Arg/Arg: Begg’s testP = 0.93, Egger’s test P = 0.26; Arg/Gln vs. Arg/Arg: Begg’stest P = 0.18, Egger’s test P = 0.39; dominant model:Begg’s test P = 0.33, Egger’s test P = 0.15; recessive model:Begg’s test P = 1.00, Egger’s test P = 0.36).
Discussion
A wide variety of DNA damage may be induced bynormal endogenous metabolic processes or by environ-mental carcinogens. Most of these alterations, if notrepaired, may result in genetic instability, mutagenesisand cell death. DNA repair mechanisms are importantfor maintaining genome integrity and preventing carci-nogenesis. BER is the predominant DNA damage repairpathway for the processing of small base lesions, derivedfrom oxidation and alkylation’s damage. XRCC1 is one ofthe most important proteins in BER and is closelyassociated with BER pathway coordination by interactingwith most components of the BER short-patch pathway.Mutations of XRCC1 may increase the risk of cancers byimpairing the interaction of XRCC1 with other enzy-matic proteins and consequently altering DNA repairactivity (32, 33). In recent years, a large number ofmolecular epidemiological studies have been conductedto evaluate the role of polymorphisms Arg399Gln in theDNA repair gene XRCC1 on cancer risk; however, theresults remain conflicting rather than conclusive (34–42),including HCC (18–28).
To the best of our knowledge, this is the first systematicreview that has investigated the association of XRCC1codon 399 polymorphisms and HCC, and no evidencehas shown any association between Arg399Gln poly-morphism and HCC susceptibility. When stratifying forethnicity, country/region, HWE in controls and source ofcontrols, the results were similar. Our results were con-sistent with previous meta-analyses based on othercancer. For example, previous three meta-analyses hadconfirmed that Arg399Gln polymorphism was not asso-ciated with a risk of gastric cancer (43), colorectal cancer(44) and bladder cancer (45). However, Saadat andAnsari-Lari (46) concluded that Arg399Gln polymorph-ism had an association with breast cancer, Geng et al. (47)found that the Arg399Gln polymorphism was associatedwith a risk of prostate cancer among Asians and Kiyoharaet al. (48) found that the 399Gln/Gln genotype of theXRCC1 Arg399Gln polymorphism was associated withan increased risk of lung cancer among Asians but notamong Caucasians. Although the reasons for this appar-ent difference in risk with different tumours are as yetunknown, some possibilities should be considered.Firstly, those gene–variant associations vary in differentkinds of cancer and may result from the differentmechanisms of carcinogenesis among different kinds ofcancer. Secondly, different ethnic composition may con-tribute to the discrepancy. Different meta-analyses in-cluded different original studies that were performed indifferent races and the ethnic composition in differentmeta-analyses may be diverse. Thirdly, some methodolo-gical diversity, such as inclusion criteria, the quality oforiginal studies, selection bias, Type – error and smallsample size, can also contribute to the discrepancy.
Because the allele frequencies of polymorphismsand their effects on the cancer risk were diverse in the
Fig. 2. Funnel plot for publication bias test (Gln/Gln vs. Arg/Arg ).Each point represents a separate study for the indicated association.
Liver International (2011)806 c� 2011 John Wiley & Sons A/S
XRCC1 polymorphism and HCC risk Liu et al.

different ethnicities, we carried out subgroup analysis byethnicity. The results demonstrated that there was noassociation between XRCC1 Arg399Gln polymorphismand HCC risk in different ethnicities. The null result maybe because of the limited number of studies, with onlytwo studies from non-Asian (one Caucasian and oneAfrican) available in this meta-analysis. It is critical thatlarger and well-designed multicentric studies based onCaucasian and African-American patients should beperformed to re-evaluate the association.
It seemed that selection bias could have played a rolebecause the genotype distribution of Arg399Gln poly-morphism among control subjects disobeyed the law ofHWE in three studies (18, 25, 27). It is widely believedthat deviation from HWE may be as a result of geneticreasons including non-random mating, or the allelesreflect recent mutations that have not reached equili-brium, as well as methodological reasons includingbiased selection of subjects from the population orgenotyping errors (49, 50). Despite the reasons of dis-equilibrium, the results of genetic association studiesmight be spurious if the distribution of genotypes in thecontrol groups were not in HWE (51, 52). Hence, wecarried out subgroup analysis by HWE in controls. Whenexcluding the studies that were not in HWE, the resultswere persistent and robust, suggesting that this factorprobably had little effect on the overall estimates.
The results of meta-analyses often depend on controlselection procedures (53). Different control sources maybe a confounding factor that may impact the conclusionof our study because of case–control studies. For in-stance, some studies used a healthy population as thereference group; whereas, others selected chronic hepati-tis virus carriers without HCC as the reference group. Inorder to eliminate interference from the confoundingfactor, we performed subgroup analysis by the source ofcontrols. Our results showed that there was no significantassociation between XRCC1 Arg399Gln polymorphismand HCC risk in different controls, which confirmed thereliability of our overall results.
One of the major concerns in a sound meta-analysis isthe degree of heterogeneity that exists between the compo-nent studies because non-homogeneous data are liable toresult in misleading results. In the present study, the Q-testand I2 statistics were carried out to test the significanceof heterogeneity. Obvious heterogeneity between studieswas observed in overall comparisons and also some sub-group analyses for some models, and then meta-regressionanalysis was used to explore the sources of heterogeneity.We found that matched controls did contribute to poten-tial heterogeneity. Another important issue for any meta-analysis is publication bias because of selective publicationof reports. In the current study, Funnel plot, Begg’s andEgger’s tests were performed to evaluate this problem.Both the shape of funnel plots and the statistical results didnot show publication bias. It is worth mentioning that theresults held when the sensitivity analysis was performed,which implied that the results were reliable.
However, there are still some limitations in this meta-analysis. Firstly, this paper was limited by analysing a singleSNPs site and lack of haplotype analyses. As mentionedabove, there are three common SNPs sites (Arg399Gln,Arg280His and Arg194Trp) in the XRCC1 gene. Data frommultiple polymorphisms within a gene can be combined tocreate haplotypes, the set of multiple alleles on a singlechromosome. The analysis of haplotype can increase thepower to detect disease associations because of higherheterozygosity and stronger linkage disequilibrium withdisease-causing mutations (54–56). However, only onestudy (18) in this meta-analysis reported haplotype ana-lyses, although several studies analysed the three commonSNPs sites in the XRCC1 gene. Secondly, we did not test forgene-to-environment interactions because of the issue ofmultiple testing and the lack of sufficient studies. It ispossible for specific environmental and lifestyle factors toalter those associations between gene polymorphisms andcancer risk. For example, Lao et al. (57) concluded that theGln/Gln genotype of Arg399Gln was associated with adecreased risk of bladder cancer among ever smokers whilethe Arg399Gln polymorphism was not associated withbladder cancer risk in the total population. Thirdly, therewas significant between-study heterogeneity from studiesin overall comparisons and also subgroup analyses in theheterozygote comparison and the dominant model, andthe genotype distribution in the control group also showeddeviation from HWE in some studies.
In conclusion, this meta-analysis evaluates the relation-ship between genetic polymorphisms and HCC risk andreveals that the XRCC1 polymorphism Arg399Gln is notassociated with altered susceptibility to HCC. Becauselimited studies were from non-Asian populations, it iscritical that larger and well-designed multicentric studiesbased on Caucasian and African-American patients shouldbe performed to re-evaluate the association. Moreover,further studies estimating the effect of haplotypes andgene–environment interactions may eventually provide abetter, comprehensive understanding of the associationbetween the XRCC1 polymorphisms and HCC risk.
Acknowledgements
Fei Liu designed research/study, performed research/study, collected data, analysed data, wrote the paper,reviewed/edited the manuscript. Bo Li performed re-search/study, collected data, analyzed data, reviewed/edited the manuscript. Yonggang Wei collected data,analysed data, reviewed/edited the manuscript. LvnanYan, Tianfu Wen, Jichun Zhao designed research/study,reviewed/edited the manuscript. Mingqing Xu reviewed/edited the manuscript.
Conflict of interest statement: none declared.
References
1. Parkin DM, Bray F, Ferlay J, Pisani P. Global cancerstatistics, 2002. CA Cancer J Clin 2005; 55: 74–108.
Liver International (2011)c� 2011 John Wiley & Sons A/S 807
Liu et al. XRCC1 polymorphism and HCC risk

2. Michielsen PP, Francque SM, van Dongen JL. Viral hepati-tis and hepatocellular carcinoma. World J Surg Oncol 2005;3: 27.
3. Faivre S, Bouattour M, Raymond E. Novel moleculartherapies in hepatocellular carcinoma. Liver Int 2011;31(Suppl. 1): 151–60.
4. Bowen DG, Walker CM. Adaptive immune responses inacute and chronic hepatitis C virus infection. Nature 2005;436: 946–52.
5. Smith TR, Miler MS, Lohman KK, et al. Polymorphisms ofXRCC1 and XRCC3 genes and susceptibility to breastcancer. Cancer Lett 2003; 190: 183–90.
6. Seeberg E, Eide L, Bjoras M. The base excision repairpathway. Trends Biochem Sci 1995; 20: 397–401.
7. Lee JM, Lee YC, Yang SY, et al. Genetic polymorphisms ofXRCC1 and risk of the esophageal cancer. Int J Cancer 2001;95: 240–6.
8. Lamerdin J, Montegomery M, Stilwagen S, et al. Genomicsequence comparison of human and mouse XRCC1 DNArepair gene regions. Genomics 1995; 25: 547–54.
9. Lindahl T, Wood RD. Quality control by DNA repair.Science 1999; 286: 1897–905.
10. Shen MR, Jones LM, Mohrenweiser H. Nonconservativeamino acid substitution variants exist at polymorphicfrequency in DNA repair genes in healthy humans. CancerRes 1998; 58: 604–8.
11. Cochran WG. The combination of estimates from differentexperiments. Biometrics 1954; 10: 101–29.
12. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measur-ing inconsistency in meta-analyses. BMJ 2003; 327: 557–60.
13. Mantel N, Haenszel W. Statistical aspects of the analysis ofdata from retrospective studies of disease. J Natl Cancer Inst1959; 22: 719–48.
14. DerSimonian R, Laird N. Meta-analysis in clinical trials.Control Clin Trials 1986; 7: 177–88.
15. Begg CB, Mazumdar M. Operating characteristics of a rankcorrelation test for publication bias. Biometrics 1994; 50:1088–101.
16. Egger M, Davey Smith G, Schneider M, Minder C. Bias inmeta-analysis detected by a simple, graphical test. BMJ1997; 315: 629–34.
17. Kiran M, Chawla YK, Jain M, Kaur J. Haplotypes ofmicrosomal epoxide hydrolase and x-ray cross-comple-menting group 1 genes in Indian hepatocellular carcinomapatients. DNA Cell Biol 2009; 28: 573–7.
18. Kiran M, Saxena R, Chawla YK, Kaur J. Polymorphism ofDNA repair gene XRCC1 and hepatitis-related hepatocel-lular carcinoma risk in Indian population. Mol Cell Bio-chem 2009; 327: 7–13.
19. Borentain P, Gerolami V, Ananian P, et al. DNA-repair andcarcinogen-metabolising enzymes genetic polymorphismsas an independent risk factor for hepatocellular carcinomain Caucasian liver-transplanted patients. Eur J Cancer 2007;43: 2479–86.
20. Long XD, Ma Y, Wei YP, Deng ZL. The polymorphisms ofGSTM1, GSTT1, HYL1�2, and XRCC1, and aflatoxin B1-related hepatocellular carcinoma in Guangxi population,China. Hepatol Res 2006; 36: 48–55.
21. Chen CC, Yang SY, Liu CJ, et al. Association of cytokineand DNA repair gene polymorphisms with hepatitis B-related hepatocellular carcinoma. Int J Epidemiol 2005; 34:1310–8.
22. Kirk GD, Turner PC, Gong Y, et al. Hepatocellular carcino-ma and polymorphisms in carcinogen-metabolizing andDNA repair enzymes in a population with aflatoxin ex-posure and hepatitis B virus endemicity. Cancer EpidemiolBiomark Prev 2005; 14: 373–9.
23. Yu MW, Yang SY, Pan IJ, et al. Polymorphisms in XRCC1 andglutathione S-transferase genes and hepatitis B-related hepa-tocellular carcinoma. J Natl Cancer Inst 2003; 95: 1485–8.
24. Ren Y, Wang DS, Li Z, et al. Study on the relationshipbetween Gene XRCC1 Codon 399 S ingle NucleotidePolymorphisms and Primary Hepatic Carcinoma in HanNationality. Chin J Clin Hepatol 2008; 24: 361–4 (article inChinese).
25. Yang JL, Han YN, Zheng SG. Influence of human XRCC1-399 single nucleotide polymorphism on primary hepatocy-tic carcinoma. Zhong Liu 2004; 24: 322–4 (article inChinese).
26. Long XD, Ma Y, Wei YP, Deng ZL. Polymorphism of DNArepair gene XRCC1 and risk of hepatocellular carcinoma.J Guang Xi Med. Univ. 2004; 21: 313–5 (article in Chinese).
27. Su HY. A case–control study on association between geneticpolymorphisms of DNA repair and hepatic cell cancersusceptibility, 2008 (article in Chinese). Available at http://dlib3.edu.cnki.net/kns50/detail.aspx?dbname=CDFD2008&filename=2008083042.nh (accessed 10 March 2011).
28. Wu H. Correlation between DNA repair gene XRCC1 singlenucleotide polymorphism and susceptibility to hepatocellu-lar carcinoma in Fusui County of Guangxi, 2009 (article inChinese). Available at http://dlib3.edu.cnki.net/kns50/detail.aspx?dbname=CMFD2009&filename=2009132690.nh (ac-cessed 10 March 2011).
29. Long XD. Polymorphism of DNA repair gene XRCC1 andrisk of aflatoxin B1-related hepatocellular carcinoma, 2004(article in Chinese). Available at http://dlib3.edu.cnki.net/kns50/detail.aspx?dbname=CMFD2004&filename=2004080557.nh (accessed 10 March 2011).
30. Wang DS. Serological diagnosis and DNA repair gene XRCC1polymorphism in patients with primary liver cancer, 2006(article in Chinese). Available at http://dlib3.edu.cnki.net/kns50/detail.aspx?dbname=CMFD2007&filename=2007101142.nh (accessed 10 March 2011).
31. Han YN, Yang JL, Zheng SG, Wu YQ. Study on theassociation of human XRCC1-399 single nucleotide poly-morphism and primary hepatocytic carcinoma. Gan Zang2004; 9: 235–7 (article in Chinese).
32. Basso D, Navaglia F, Fogar P, et al. DNA repair pathwaysand mitochondrial DNA mutations in gastrointestinalcarcinogenesis. Clin Chim Acta 2007; 381: 50–5.
33. Tudek B. Base excision repair modulation as a risk factorfor human cancers. Mol Aspects Med 2007; 28: 258–75.
34. Xing D, Qi J, Miao X, et al. Polymorphisms of DNA repairgenes XRCC1 and XPD and their associations with risk ofesophageal squamous cell carcinoma in a Chinese popula-tion. Int J Cancer 2002; 100: 600–5.
Liver International (2011)808 c� 2011 John Wiley & Sons A/S
XRCC1 polymorphism and HCC risk Liu et al.

35. Divine KK, Gilliland FD, Crowell RE, et al. The XRCC1 399glutamine allele is a risk factor for adenocarcinoma of thelung. Mutat Res 2001; 461: 273–8.
36. Olshan AF, Watson MA, Weissler MC, Bell DA. XRCC1polymorphisms and head and neck cancer. Cancer Lett2002; 178: 181–6.
37. Duell EJ, Holly EA, Bracci PM, Wiencke JK, Kelsey KT. Apopulation-based study of the Arg399Gln polymorphismin X-ray repair cross-complementing group 1 (XRCC1)and risk of pancreatic adenocarcinoma. Cancer Res 2002;62: 4630–6.
38. van Gils CH, Bostick RM, Stern MC, Taylor JA. Differencesin base excision repair capacity may modulate the effect ofdietary antioxidant intake on prostate cancer risk: anexample of polymorphisms in the XRCC1 gene. CancerEpidemiol Biomarkers Prev 2002; 11: 1279–84.
39. Shen M, Hung RJ, Brennan P, et al. Polymorphisms of theDNA repair genes XRCC1. XRCC3, XPD, interaction withenvironmental exposures, and bladder cancer risk in acase–control study in northern Italy. Cancer EpidemiolBiomarkers Prev 2003; 12: 1234–40.
40. Shu XO, Cai Q, Gao YT, et al. A population based case–control study of the Arg399Gln polymorphism in DNArepair gene XRCC1 and risk of breast cancer. CancerEpidemiol Biomarkers Prev 2003; 12: 1462–7.
41. Matsuo K, Hamajima N, Suzuki R, et al. Lack of associationbetween DNA base excision repair gene XRCC1 Gln399Argpolymorphism and risk of malignant lymphoma in Japan.Cancer Genet Cytogenet 2004; 149: 77–80.
42. Figueiredo JC, Knight JA, Briollais L, Andrulis IL, OzcelikH. Polymorphisms XRCC1-R399Q and XRCC3-T241Mand the risk of breast cancer at the ontario site of the breastcancer family registry. Cancer Epidemiol Biomarkers Prev2004; 13: 583–91.
43. Geng J, Zhang YW, Huang GC, Chen LB. XRCC1 geneticpolymorphism Arg399Gln and gastric cancer risk: a meta-analysis. World J Gastroenterol 2008; 14: 6733–7.
44. Wang B, Wang D, Huang G, et al. XRCC1 polymorphismsand risk of colorectal cancer: a meta-analysis. Int J Color-ectal Dis 2010; 25: 313–21.
45. Wang C, Sun Y, Han R. XRCC1genetic polymorphisms andbladder cancer susceptibility: a meta-analysis. Urology 2008;72: 869–72.
46. Saadat M, Ansari-Lari M. Polymorphism of XRCC1 (atcodon 399) and susceptibility to breast cancer, a meta-analysis of the literatures. Breast Cancer Res Treat 2009; 115:137–44.
47. Geng J, Zhang Q, Zhu C, Wang J, Chen L. XRCC1 geneticpolymorphism Arg399Gln and prostate cancer risk: a meta-analysis. Urology 2009; 72: 4648–53.
48. Kiyohara C, Takayama K, Nakanishi Y. Association ofgenetic polymorphisms in the base excision repair pathwaywith lung cancer risk: a meta-analysis. Lung Cancer 2006;54: 267–83.
49. Mitchell AA, Cutler DJ, Chakravarti A. Undetected geno-typing errors cause apparent overtransmission of commonalleles in the transmission/disequilibrium test. Am J HumGenet 2003; 72: 598–610.
50. Hosking L, Lumsden S, Lewis K, et al. Detection ofgenotyping errors by Hardy–Weinberg equilibrium testing.Eur J Hum Genet 2004; 12: 395–9.
51. Salanti G, Amountza G, Ntzani EE, Ioannidis JP.Hardy–Weinberg equilibrium in genetic association stu-dies: an empirical evaluation of reporting, deviations, andpower. Eur J Hum Genet 2005; 13: 840–8.
52. Trikalinos TA, Salanti G, Khoury MJ, Ioannidis JP. Impactof violations and deviations in Hardy–Weinberg equili-brium on postulated gene–disease associations. Am J Epi-demiol 2006; 163: 300–9.
53. Benhamou S, Lee WJ, Alexandrie AK, et al. Meta- andpooled analyses of the effects of glutathione S-transferaseM1 polymorphisms and smoking on lung cancer risk.Carcinogenesis 2002; 23: 1343–50.
54. Stephens JC, Schneider JA, Tanguay DA, et al. Haplotypevariation and linkage disequilibrium in 313 human genes.Science 2001; 293: 489–93.
55. Juson R, Stephens JC, Windemuth A. The predictive powerof haplotypes in clinical response. Pharmacogenomics 2000;1: 15–26.
56. Fallin D, Cohen A, Essioux L, et al. Genetic analysis of case/control data using estimated haplotype frequencies: appli-cation to APOE locus variation and Alzheimer’s disease.Genome Res 2001; 11: 143–51.
57. Lao T, Gu W, Huang Q. A meta-analysis on XRCC1 R399Qand R194W polymorphisms, smoking and bladder cancerrisk. Mutagenesis 23: 523–32.
Liver International (2011)c� 2011 John Wiley & Sons A/S 809
Liu et al. XRCC1 polymorphism and HCC risk






![Research Paper Reappraisal of XRCC1 Arg194Trp polymorphism ...€¦ · [7–20] published to estimate the association between XRCC1 Arg194Trp polymorphism and glioma risk, but the](https://img.pdfslide.us/doc/110x75/5f2c5b6030f7cb7aad7c10ff/research-paper-reappraisal-of-xrcc1-arg194trp-polymorphism-7a20-published.jpg)




















