Embed Size (px)
Citation preview

www.drsarma.in
1
Dr. R.V.S.N. Sarma., M.D., M.Sc.,
MANAGEMENT OF TYPE 2
DMA Rational Approach

www.drsarma.in
2
Diabetes Mellitus
1. Type 2 DM (No more called NIDDM)
2. Not merely ‘SUGAR DISORDER’
3. Multi system disease – A syndrome
4. Metabolic – Endocrine – Vascular – Neural
5. Cardiac – Cerebral – Renal – Ophthalmi
From Bl. sugar control to blood vessel protection
We should aim for total Metabolic Control
www.drsarma.in
3
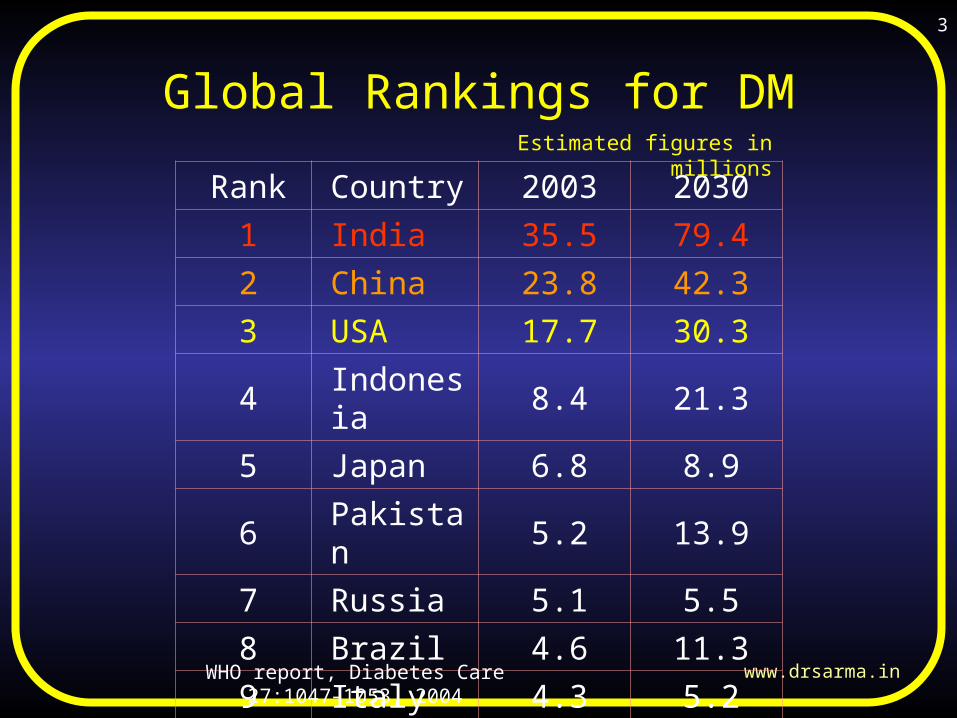
Global Rankings for DM
Rank Country 2003 20301 India 35.5 79.42 China 23.8 42.33 USA 17.7 30.34 Indonesia 8.4 21.35 Japan 6.8 8.96 Pakistan 5.2 13.97 Russia 5.1 5.58 Brazil 4.6 11.39 Italy 4.3 5.2
WHO report, Diabetes Care 27:1047–1053, 2004
Estimated figures in millions

www.drsarma.in
4
Better we all realize !!
1. India is the Diabetic Capitol of the World
2. DM is the leading cause of blindness in < 60 yr
3. Over 60% of ESRD is due to Diabetes
4. 70 % Diabetics die of – CHD, CVD
5. Leading cause of non traumatic LL amputation
6. MAU is the strongest predictor of CHD
7. So, screen all for DM and for risk factors

www.drsarma.in
5
T1DM and T2DMDefects & Differences
Type 1 DiabetesType 1 Diabetes
-cell failure-cell failure
Insulinopenia
Total cell failure
Insulinopenia
Total cell failure
Type 2 DiabetesType 2 Diabetes
IR - Insulin ResistanceIR - Insulin Resistance
ID - Insulin DeficiencyID - Insulin Deficiency
‘More Heterogenous’‘More Heterogenous’
IR ID
ID

www.drsarma.in
6
Normal
Type 2 DM
Type 1 DM

www.drsarma.in
7
DM Deaths – World wide

www.drsarma.in
8
DM Prevalence Developed Countries

www.drsarma.in
9
DM Prevalence Developing Countries
www.drsarma.in
10
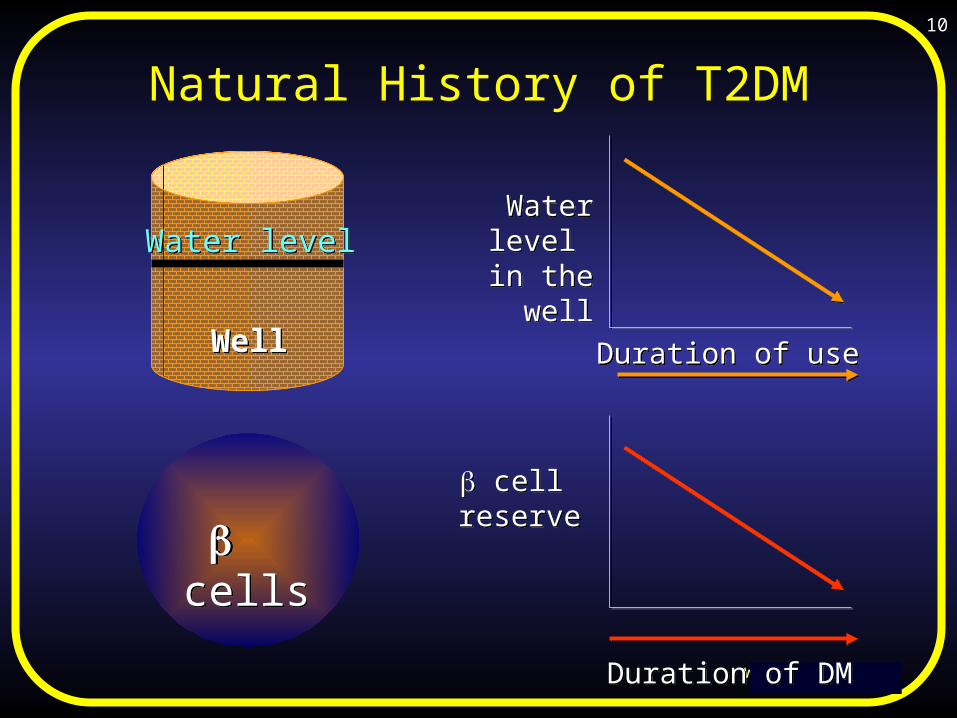
Natural History of T2DM
WellWell
Water levelWater levelWater level in the well
Water level in the well
Duration of useDuration of use
cell reserve cell
reserve
Duration of DMDuration of DM
cells cells

www.drsarma.in
11
FPG in T2DM (untreated DM)
FPG in T2DM (untreated DM)
500
400
300
200
100
0
500
400
300
200
100
0
Duration of Diabetes in yearsDuration of Diabetes in years
FP
G in
mg
%F
PG
in m
g %
7 207 20

www.drsarma.in
12
Insulin Defects in T2DMInsulin Defects in T2DM
1. ‘Selective Unresponsiveness’ 2. ‘Secretory Rigidity’ - Defective
glucose recognition3. ‘Gluco-toxicity’ to cells
1. Absence or delay in 1st Phase- a primary defect of T2DM
2. Blunting of 2nd Phase- secondary to high blood sugar Basal Steady StateBasal Steady State
TimeTimeIn
sulin
ou
tput
Insu
lin
outp
ut
2nd Phase2nd Phase
1st phase1st phase
Cell defect
Normal Cell

www.drsarma.in
13
Mandatory Examinations
1. Family H/o DM
2. H/o Angina, IHD, IC
3. H/o Smoking
4. H/o Hypoglycemia
5. Exam for all pulses
6. B.P recording
7. Foot exam - Trophic
8. PNP and ANP
9. Fungal, Infect, Pruritus
1. Fasting and PP BG
2. HbA1c on Dx. & 3-6 months
3. Lipid profile, Lp(a), hs-CRP
4. CHD Risk factors
5. MAU - ACR
6. ECG for LVH, IHD
7. Echo for LVD, LVH
8. Stress test in equivocal cases
9. Fundus exam for DR

www.drsarma.in
14
Type 2 DMDiagnosisType 2 DMDiagnosis

www.drsarma.in
15
Diagnosis – O-GTT
DM
IGT
Normal
126 mg%
100 mg%
126 mg%
100 mg%
200 mg%
140 mg%
200 mg%
140 mg%
PPG75g of oral glucose – 2 hrs. after
DM
IFG
Normal
FPG

www.drsarma.in
16
Diagnosis – Criteria
FBG > 126 & PPBG > 200 - same day RBG > 200 mg % on 2 occasions or Never make a diagnosis on single test Never diagnose based on glycosuria Glucometer is not ideal for diagnosis For Diagnosis Plasma Glucose only For Screening or Monitoring BGM

www.drsarma.in
17
Diagnosis - Practical Points
1. Do not label one a diabetic by glycosuria alone
For, one may have renal glycosuria
2. Benedict’s less accurate; shows any reducing substance.
Glucose oxidase test strips confirm glucosuria
3. Urine test is useful – Albumin, MAU, Ketones
4. Never make a Dx. based on a single blood sugar test
5. O-GTT (2 sample) is the gold standard for Dx. of DM
6. HbA1c – Not for Dx. Follow up once in 3 to 6 months
7. Majority of diabetics are not symptomatic – so screen
One may present first time with complications – too late

www.drsarma.in
18
Fasting Hyperglycemia
Due to↑ Hepatic Glucose Output - HGO
Glycogenolysis – breakdown of glycogen
Lipolysis – breakdown of fats
Gluconeogenesis – breakdown of proteins
Because of ↓in basal insulin secretion
More important than postprandial spikes
Develops after some time in T2DM

www.drsarma.in
19
Post Prandial Hyperglycemia
Blood sugar can rise above normal if1.↓ Decreased peripheral utilization
2.↓ In insulin secretion after meal
3. Delay in insulin secretion – No 1st phase
4.↓ In insulin sensitivity (resistance)
5. Excessive CHO consumption
6. A combination of any of the above

www.drsarma.in
20
Metformin SU, Repag.
Acarbose, Miglitol
Pio glit, Rosi.

www.drsarma.in
21
Type 2 DMMonitoringType 2 DMMonitoring
A Paradigm Shift from Blood Glucose to HbA1CA Paradigm Shift from Blood Glucose to HbA1C

www.drsarma.in
22
Different Hemoglobins
Fetal Hemoglobin – Hb F Adult Hemoglobin – Hb A Sickle cell disease – Hb S Hemoglobinopathies – Hb C, Hb E
Glucose in the blood reacts with the
Hemoglobin A to form Glycated Hb.

www.drsarma.in
23
Different types of Glycation products are formed from the HbA depending on the carbohydrate moiety – namely
HbA1a1 - Fr 1,6 diphos –N-term. valine
HbA1a2 - Gl 6 phos –N-terminal valine
HbA1b - Other CHO – N-term. valine
HbA1c - Glucose – N-terminal valine
Normally less than 6% of Hb is HbA1c
Glycated Hb - GHb
(Previously called glycosylated Hb.)

www.drsarma.in
24
Estimation of HbA1c
There are many methods of estimation
HPLC (High Performance Liquid Chromatography) – Gold standard.
Immuno-turbimetric meth. – HbA1cAb Affinity chromatography Electrophoretic methods Method based on chemical reactions.
www.drsarma.in
25
Advantages of HbA1c
• Index of long-term control over 120 days
• It is not a snap shot like FBG/PPBG
• Can be done at any time of day
• Not influenced by diet, exercise, emotional disturbances on test day
• The index of control for clinical practice
• Useful if missed drugs / default on diet
• Useful in DD of stress hyperglycemia

www.drsarma.in
26
Limitations of HbA1c
• Should not be used for Dx. of Diabetes
• Cannot be an emergency room test to titrate Insulin or ODA dosage
• Can not register hypoglycaemia
• Not sensitive enough for use in GDM Anaemia, Uraemia, Pregnancy

www.drsarma.in
27
HbA1c is ‘weighted’

www.drsarma.in
28
Correlation of MPG - HbA1c
Mean Plasma Glucose =
(35.6 x HbA1c %) – 77.3
HbA1C % MPG mg%
5 100
6 135
7 1708 2059 240
10 27511 31012 34513 380
Diabetes Care
Vol.26 (S), P33, 2003
HbA1c =
(MPG mg% + 77.3) / 35.6

www.drsarma.in
29
Which is the best measure of monitor control of DM
Fasting Blood Glucose (FBG) ? 2 hour Postprandial Glucose
(PPBG) ?Answer is
Mean Amplitude of Glucose Excursions (MAGE) –
This is best reflected by HbA1c

www.drsarma.in
30
Any Diabetes Related Endpoint
Updated mean HbA1c
Haz
ard
ratio
UKPDS 35. BMJ 2000; 321: 405-12
0.5
1
5
0 5 6 7 8 9 10 11
21% decrease per 1% decrement in HbA1c
p<0.0001

www.drsarma.in
31
Diabetes Related Deaths
21% decrease per 1% decrement in HbA1c
p<0.0001
0.5
1
5
0 5 6 7 8 9 10 11Updated mean HbA1c
Haz
ard
ratio
UKPDS 35. BMJ 2000; 321: 405-12

www.drsarma.in
32
Microvascular Endpoints
0.5
1
10
15
0 5 6 7 8 9 10 11
37% decrease per 1% decrement in HbA1c
p<0.0001
Updated mean HbA1c
Haz
ard
ratio
UKPDS 35. BMJ 2000; 321: 405-12

www.drsarma.in
33
Amputation or Death from PVD
0.1
1
10
20
0 5 6 7 8 9 10 11
43% decrease per 1% decrement in HbA1c
p<0.0001
Updated mean HbA1c
Haz
ard
ratio
UKPDS 35. BMJ 2000; 321: 405-12
www.drsarma.in
34
Blood Sample – Practical Points
The whole blood glucose is 15% higher We need to estimate plasma glucose Na F is to be used as the anti-coagulant Centrifuge and separate plasma within 1 hour For HbA1c – we need EDTA added blood – HbA1c measurement – No fasting is required C-Peptide or Serum Insulin – Only on fasting Shouldn’t add any anti-coagulant for C peptide

www.drsarma.in
35
Indian Diabetic Risk Score (IDRS)Parameter Classification PointsAge 1. < 35 yrs
2. 35 – 49 yrs3. 50 yrs
02030
Abdominal Obesity
1. < 90 cm for ♂; < 80 cm for ♀2. 90-99 cm for ♂; 80-89 cm for ♀ 3. 100 cm for ♂; > 90 cm for ♀
01020
Physical Inactivity
1. Regular Exercise + Strenuous work2. Regular Exercise or Strenuous work3. No Exercise and Sedentary work
02030
Family H/o Diabetes
1. No family history of DM2. Either parent / sibling DM3. Both parents / sibling DM
01020
Interpretation < 20 Least risk; 20 to 50 Moderate risk;50 to 70 High risk; > 70 Very high risk.
Range0 to 100

www.drsarma.in
36
Prevention of Type 2
Diabetes
Prevention of Type 2
Diabetes

0 1 2 3 4
0
10
20
30
40Placebo (n=1082)Metformin (n=1073, p<0.001 vs. Plac)Lifestyle (n=1079, p<0.001 vs. Met , p<0.001 vs. Plac )
Percent developing diabetes
All participants
All participants
Years from randomization
Cum
ulat
ive
inci
denc
e (%
)
Placebo (n=1082)
Metformin (n=1073, p<0.001 vs. Placebo)
Lifestyle (n=1079, p<0.001 vs. Metformin , p<0.001 vs. Placebo)
Incidence of Diabetes Incidence of Diabetes
Risk reductionRisk reduction31% by metformin31% by metformin58% by lifestyle58% by lifestyle
The DPP Research Group, NEJM 346:393-403, 2002

www.drsarma.in
38
Exercise
Question is not what ? – We need exercise
Do 45 minutes of aerobic exercise at least 5 times a week.
•Swimming
•Brisk walking
•Dancing
•Running
•Biking
• Jogging

www.drsarma.in
39
ManagementStrategies
ManagementStrategies

www.drsarma.in
40
Insulin
Monitoring
Education
Diet
Exercise
Oral Agents
3
T2DM Treatment
www.drsarma.in
41
Life StyleModifications
Life StyleModifications

www.drsarma.in
42
WHO recommendation -Diet
CARBOHYDRATES : 50-60%
- mainly from complex carbohydrates
FATS : 25%
- saturated 7%
- poly-unsaturated 9%
- mono-unsaturated 9%
- cholesterol < 300 mg/day
PROTEINS : 12-20%
SODIUM : < 6 g/day
- hypertensive diabetic, < 3 g/day

www.drsarma.in
43
Managing Diabetes Follow a Healthy Meal Plan
Eat More Carbohydrate Foods
Eat Least Sugar, Fat, Alcohol, Salt
Eat Moderately Protein Foods
Eat Most Vegetables

www.drsarma.in
44
The New Food Pyramid

www.drsarma.in
45
EXERCISEBenefits
• Reduces weight• Improves cardiovascular function• Increases fitness • Increases physical working capacity• Improves sense of well-being
/quality of life

www.drsarma.in
46
Management of T2DM
Old Paradigm
Old Paradigm
Diet +
Exercise
Diet +
Exercise
Oral drugsOral drugs
InsulinInsulin
11
22
33
‘‘Step-Care’Step-Care’‘‘Step-Care’Step-Care’
1. Glycemic targets not met
2. Monotherapy is not durable
3. Fails to address dual defect
4. Perpetuates failure of Rx.
5. Glucotoxicity ↓ response

www.drsarma.in
47
Stages of T2DM
Insulin Resistance
Insulin Deficiency1. Insulin Resistance
2. Hyper Insulinemia3. Normal Glucose
Tolerance1. Insulin Resistance2. Declining Insulin levels3. Abnormal Glucose
Tolerance1. Insulin Resistance2. Very low Insulin levels3. Hyperglycemia round
the clock
Stage 1
Stage 2
Stage 3
IR
IR + ID
ID

www.drsarma.in
48
T2DM – Cardiometabolic Basis

www.drsarma.in
49
Stage Management
Today’s ParadigmToday’s
Paradigm
IR AloneIR Alone
IR + IDIR + ID
Frank IDFrank ID
11
22
33
Metabolic BasisMetabolic Basis
1. Metformin is the sheet anchor2. Early insulin therapy, Basal
Insulin3. HbA1c target of < 7, OAD
Combina.4. OAD choice based on patient
type 5. ABC control; not glycemia
alone6. Prevention of complications - a
must

www.drsarma.in
50
What is new in Rx. of T2DM
• The step-care therapy is not advocated now.• Choice of OAD/Insulin to be individualized• Glycemic targets must be achieved quickly• Multiple therapies may be needed• A1c is the target now - within 6 months• Diet alone is not the option now - difficulties• Even prediabetes needs Rx. Aggressively• Total ABC control – not glycemia alone• Combination of OAD + Insulin, early insulin• Avoid hypoglycemia by proper drug choice

www.drsarma.in
51
Stage Based Management
Stage 1 Stage 2 Stage 3
Pre Diabetic State N FBG, ↑ PPBG ↑ FBG, ↑ PPBG
Weight Reduction Diet and Exercise Diet and Exercise
Physical Activity Metformin, -GI !! Metformin
May be Metformin SU, GLT TZD, SU (↓ effect)
No drug app. FDA TZD, RA insulin Basal In, AM PM In.
7% per yr - DM Amylinomimetics Exenatide, Pramlin.

www.drsarma.in
52
Today’s Treatment Goals
Keeping HbA1c and FBG, PPBG with in limits1. Exercise – Diet – Weight reduction
2. OHAs and Insulin
Correction of all metabolic abnormalities1. Normalizing lipids, BP Goal < 130/80
2. Reducing Obesity and Waist Circumference
Prevention and Rx. of complications1. Macrovascular, 2. Microvascular, 3.
Metabolic
Special emphasis on Prevention of CHD

www.drsarma.in
53
Complications of T2DM
1. Metabolic Complications1. IR; Obesity, Lipids – ↑TG, ↓HDL, ↑ sLDL
2. Thrombogenic ( ↑PAI-1, ↑ fibrinogen) profile
2. Micro-vascular Complications1. Diabetic Retinopathy (DR)
2. Diabetic Kidney Disease (DKD) – Nephropathy
3. Diabetic Neuropathy – DPN, DAN
3. Macro-vascular Complication1. Coronary Artery Disease (CAD)
2. Stroke, CVD, TIA, HT
3. Peripheral Vascular Disease (PVD)

www.drsarma.in
54
Ticking Clock of T2DM
1. Micro-vascular Complications At the onset of hyperglycemia Control of hyperglycemia essential The A1c target of less than 7 must
(A)
2. Macro-vascular Complication At the onset of insulin resistance Blood pressure goal of 130/80 (B) Control of lipid abnormalities (C)

www.drsarma.in
55
How to Identify IR ??
Features Insulin Resistance
Hyperglycemia ↑ PPBG, Usually FBG is N
Obesity, ↑ WC, ACN BMI > 23, WC > 90, ACN+
↑ TG, ↓ HDL, ↑ sLDL Dyslipidemia Present
Cluster of metabolic factors Metabolic Syndrome
Hypertension (>130/80) Usually is a feature
Recent weight change Increase
Fasting C peptide / Insulin Increased (HOMA)
Treatment OAD – Met, TZD, Exercise

www.drsarma.in
56
Insulin is a dimer of two peptides. Each peptide consists of A and B chains
A has 21 amino acids; B has 30 amino acids; The two chains are linked by pair of S – S bonds
C peptide has 35 amino acids and is cleaved
Insulin – C peptide

www.drsarma.in
57
Measures of Insulin Resistance
Can we measure insulin resistance ? Yes ! It is useful in special situations as follows: It will be of use to confirm IR (Stage 1) C Peptide is useful detect SU failure What are the measures ? – F-C-Peptide, FBG CISI – Composite Insulin Sensitivity Index QUICKI – Quantitative Insulin Sensitivity
Index HOMA IR – Homeostasis Model Assessment
•HOMA calculator is available

www.drsarma.in
58
How to treat Insulin Resistance ?
IDID IRIR
Diet, Exercise, TLC
Weight reduction, Waist reduction
Metformin – unmasks Insulin receptors
Insulin sensitizers – TZDs - PPARγ
Abolition of Glucotoxicity
Control of hypertension
Control of Metabolic abnormalities
Diet, Exercise, TLC
Weight reduction, Waist reduction
Metformin – unmasks Insulin receptors
Insulin sensitizers – TZDs - PPARγ
Abolition of Glucotoxicity
Control of hypertension
Control of Metabolic abnormalities

www.drsarma.in
59
ABC - The Target Values
Hb A1c – Target less than 7% better 6.0% Blood Pressure - < 130/ 80 Blood Glucose must not go below 60 mg% BMI < 23, WC < 36” (32”) Cholesterol - LDL < 100 mg HDL > 40 (50) TG < 150 mg Lp(a) < 25 mg hs-CRP < 3

www.drsarma.in
60
Major Classes of Medications
1. Drugs that sensitize the body to insulin and/or control HGO
2. Drugs that stimulate the pancreas to make more insulin
3. Drugs that slow the absorption of starches
TZD – Glitazones And Metformin
Sulfonylureas and Meglitinides
-GI – Acarbose, Miglitol,Voglibose

www.drsarma.in
61
Site & Mode of Action of OADs
Adapted from DeFronzo R. Ann Intern Med 1999;131:281
Site of action MOA Agents
Insulinsecretion
SulfonylureasRepaglinideNateglinide
HGOproduction
BiguanidesGlitazones
Slow CHODigestion
- glucosidaseinhibitors
Peripheralinsulin sensitivity
GlitazonesBiguanides

www.drsarma.in
62
© International Diabetes Center. From Kendall D, Bergenstal R.
Timeline for Utilization of Therapies
Glucose
Relative
Function
0
50
100
150
200
250
-10 -5 0 5 10 15 20 25 30
50100150200250300350
Years of Diabetes
Insulin Resistance
Insulin Level
Fasting Glucose
Beta cell failure
Post Meal Glucose
At riskfor Diabetes
Lifestyle Insulin
Metformin, TZD, (-GI add on)
SUMeglitinide

www.drsarma.in
63
MetforminEfficacy
1. Decreases HGO – Reduces FBG mainly.2. ↑ insulin-mediated peripheral glucose uptake3. Improves Insulin sensitivity, No hypoglycemia4. Decreases micro-vascular complications
(UKPDS)5. Take 2 to 3 weeks for the effect to be seen
Side Effects1. Diarrhea & Abdominal Pain; Lactic acidosis ?2. Causes small decrease in LDL and TG3. No effect on Blood Pressure; Modest weight
loss4. Don’t use if > 80 yrs; or Impaired renal
function (Serum Cr > 1.4 mg/dL for ♀ or 1.5 mg/dL ♂)

www.drsarma.in
64
Sulfonylureas (SU)Glimepiride, Gliclazide, Glipizide,
GlybenclamideEfficacy
1. Stimulate pancreatic Insulin Secretion
2. Reduces FBG mainly – less effect on PPBG
3. Effects are seen almost from day one
Side Effects1. Hypoglycemia - more with Glybenclamide
2. Weight gain may be a problem (may ↑ IR)
3. Skin rashes and urticaria – Sulfa like allergy
4. Lipid neutral; No effect on Blood Pressure
5. Least expensive class of medication

www.drsarma.in
65
Which SU to choose ??
1. Glybenclamide (Daonil) is a long acting SU
2. Incidence of hypoglycemia is high with Daonil
3. The continuously stimulate the -cell – ↑ apoptosis
4. Glipizide and Gliclazide need to be used twice a day
5. Glimepiride is the best among the SU – OD
6. Its action on -cell is short lived –less hypoglycemia

www.drsarma.in
66
Which Sulfonylurea to choose ?
Sulfonylurea Effectiveness Dosage Hypogly Metabolite
Glimepiride (III) * Potent - OD 1 to 8 mg Least. Inactive
Gliclazide (II) Potent - BID 40 to 80 mg Less Inactive
Glipizide (II) Most potent -BID 5 to 15 mg Less Active
Glibenclamide (II) Long acting OD 2.5 to 15 mg More Active
Chlorpropamide (I) Long acting Not in use Most Active
Tolbutamide (I) Intermediate Not in use More Active
* No action on KATP of Heart

www.drsarma.in
67
Thiazolidinediones (TZD)Pioglitazone & Rosiglitazone (PPARγ
modulators)1. Target insulin resistance – the core defect
2. Muscle and adipose cells made sensitive to insulin
3. Suppress HGO also, No hypoglycemia
4. Preserve cells and improve CV outcomes
5. Take 6 weeks for the maximum effect
Side Effects1. Weight gain, edema, some ↓ in B.P
2. Hypoglycemia (if taken with insulin or SU, GLT)
3. Contraindicated in - abnormal liver function or CHF
4. Improves HDL cholesterol and plasma TG

www.drsarma.in
68
Which Glitazone to choose ?
Effects Pioglitazone Rosiglitazone
LDL Neutral Increases
TG Decreases Neutral
HDL Increases more Increases
Dosage 15 - 30 mg OD 2 - 4 mg BID
HbA1c reduction 0.8 – 1.5 % 0.5 – 1.2 %
Cost per day Rs. 2 to 4 Rs. 8 to 16

www.drsarma.in
69
Glinides (GLT)
Repaglinide and Netaglinide
Efficacy Short rapid stimulation of Insulin from
pancreas Decrease the peak of postprandial glucose No effect on FBG and Insulin Resistance
Other Effects1. Hypoglycemia (less than with SU)
2. No meal – no tablet – effect instantaneous
3. Weight gain
4. No effect on plasma lipid levels
5. Safer at higher levels of serum creatine > SU

www.drsarma.in
70
Alpha-glucosidase InhibitorsAcarbose, Miglitol, VogliboseEfficacy
1. Inhibit the enzyme -glucosidase in the gut2. Prevent conversion of complex CHO to simple
CHO3. Thus delay the absorption of CHO4. Hence, reduced PPBG excursions5. Very modest in efficacy, usually take 6-8
weeks
Side Effects1. Flatulence or abdominal discomfort common2. No effect on lipids or blood pressure3. No weight gain or loss4. Contraindicated in IBD or Cirrhosis
www.drsarma.in
71
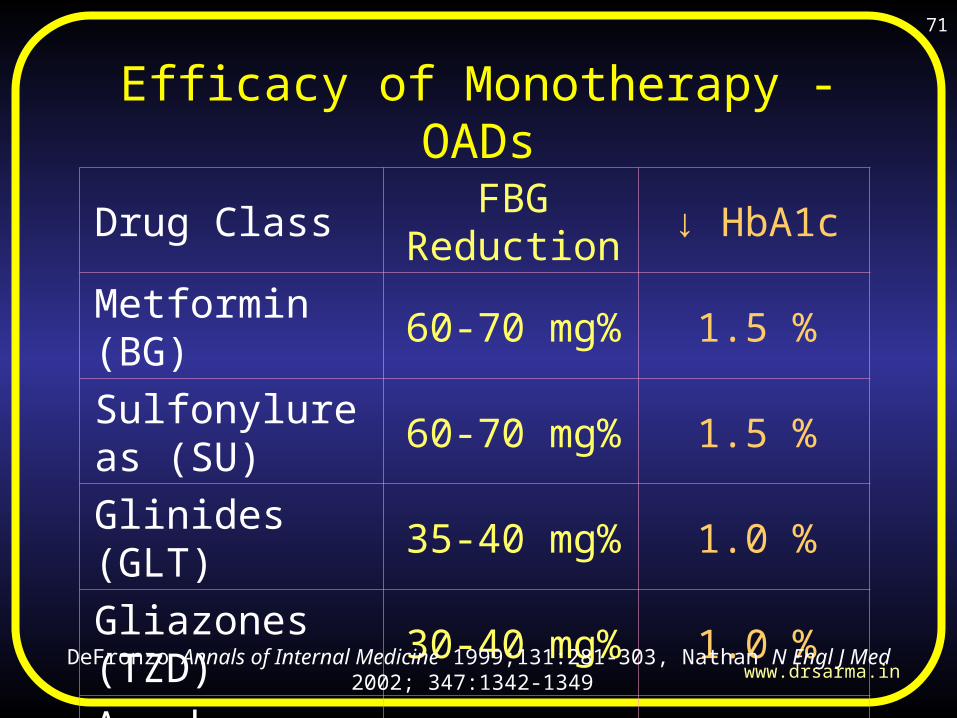
Efficacy of Monotherapy - OADs
Drug Class FBG Reduction ↓ HbA1c
Metformin (BG) 60-70 mg% 1.5 %
Sulfonylureas (SU) 60-70 mg% 1.5 %
Glinides (GLT) 35-40 mg% 1.0 %
Gliazones (TZD) 30-40 mg% 1.0 %
Acarbose (-GI) 20-30 mg% 0.6 %
DeFronzo Annals of Internal Medicine 1999;131:281-303, Nathan N Engl J Med 2002; 347:1342-1349

www.drsarma.in
72
Durability of OADs
N Engl J Med 355; 23 December 7, 2006

www.drsarma.in
73
Summary of all effects of Rx.
Intervention Glycemia Lipids B.P. B.V Weight
Diet + + + + ++Excercise +/- + + + ++Metformin + + + + +Sulfonylureas + No No No ↑
Glitazones + + + + ↑
Insulin ++ + No + ↑ ↑
Diabetes Spectrum Vol. 5, # 3, 103-108

www.drsarma.in
74
Basis of Treatment DecisionsL
IFE
ST
YL
E
Dx. of T 2 DM (2 readings) Test Hb A1c %
Hb A1c < 9.0 % Hb A1c > 9.0 %
No IR Features IR Features +
RF N / Abn.
N FBG, ↑ PPBG ↑FBG, PPBG N
OAD = BG, SU, TZD, RG, AGI,
CHF +/- LFT N /↑ SU aller. lipid
OAD + In. + Amy + Ex
DM 5 yr / 5+ yrs
↑FBG, ↑ PPBG
Early Insulin +/- OAD
HT
Acute/ DKA

www.drsarma.in
75
Treatment AlgorithmTreatment Algorithm
Dx. of T 2 DM (2 readings) HbA1c > 9%
TLC + Metformin 3 mon.HbA1c < 7 Y
No
Add Basal Insulin Add SU Add TZD
HbA1c < 7 HbA1c < 7 HbA1c < 7%
↑ Insulin + OAD
Y No Y No YNo
Add TZD Add SUBasal Insulin
I+OAD
HbA1c < 9%
3 M 3 M
NEJM 355; 2478 23 December 7, 2006
www.drsarma.in
76
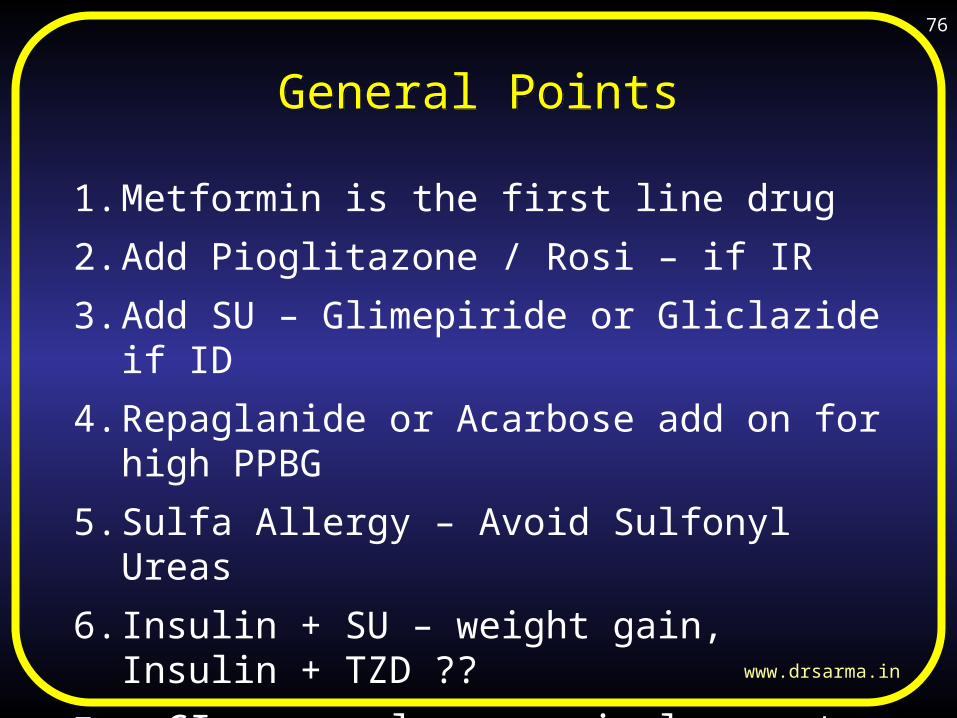
General PointsGeneral Points
1. Metformin is the first line drug
2. Add Pioglitazone / Rosi – if IR
3. Add SU – Glimepiride or Gliclazide if ID
4. Repaglanide or Acarbose add on for high PPBG
5. Sulfa Allergy – Avoid Sulfonyl Ureas
6. Insulin + SU – weight gain, Insulin + TZD ??
7. -GI never alone as single agents (pre DM – ? yes)
8. DM over 10 yrs – OAD alone may not work

www.drsarma.in
77
Key ContraindicationsKey Contraindications
1. Liver Disease, Ch. Alcoholism – TZD, Met, SU
2. Renal insufficiency – Metformin, SU
3. CHF and fluid overload – TZD, Metformin
4. Advanced age – Metformin, Glybenclamide
5. Sulfa Allergy – Sulfonyl ureas
6. Insulin + SU – Obesity, Insulin + TZD ??
7. -GI in Inflammatory bowel disease, Liver dis.
8. Pregnancy and Acute states – No OHAs

www.drsarma.in
78
Insulin inType 2 DMInsulin in
Type 2 DM

www.drsarma.in
79
Central PointCentral Point
Problem
In T2DM, a disordered regulation of Hepatic Glucose Output (HGO) is the crucial defect
Solution
Insulin is the primary regulator of overnight Hepatic Glucose Output

www.drsarma.in
80
Insulin in T2DM - Certain MythsInsulin in T2DM - Certain Myths
1. Type 2 diabetics are non-insulin dependent Hence it is incorrect to use insulin for them - No
2. Secondary sulfonylurea failure is a misnomer Remember it is the pancreas & not the drug that fails – ‘Secondary Secretory failure’
3. Type-2 DM is characterized by Insulin Resistance – So why use Insulin ?
4. Insulin is atherogenic – isn’t it ? – No

www.drsarma.in
81
Barriers to Insulin useBarriers to Insulin use
Patient Barriers Solutions
Fear of injections Fear of hypoglycemia Fear of weight gain Only for ‘Severe DM’
Improved comfort & convenience Sever hypoglycemia is rare Weight gain seen with most Rxs. Glucose normalization is the key
Provider Barriers Solutions
Insulin is atherogenic? Difficulty in convincing Complex to adjust dose
No !!, DIGAMI, UKPDS, DCCT Improved devices, Dr education Simplify regimens and dosing

www.drsarma.in
82
Benefits of Insulin TherapyBenefits of Insulin Therapy
1. Prevention of acute metabolic crises
2. Quick return to ‘health’
3. ↓ ↓ symptoms of glucosuria and hyperglycemia
4. Sense of well-being
5. Anabolic & anti–catabolic effects of insulin
6. Restoration of -cell function
7. -cell protection from apoptosis & preservation
8. Postponement of ‘Secretory Failure’

www.drsarma.in
83
Insulin – Adverse EffectsInsulin – Adverse Effects
1. Hypoglycemia
2. Weight gain – It is rather restoration of lost weight than true weight gain
3. Atherogenicity hypothesis is disproved.

www.drsarma.in
84
Insulin RegimensInsulin Regimens1. Temporary Insulin Therapy – TIT
2. Basal Interm. Action Insulin Therapy - BIAIT
3. Basal Insulin + Day time SU – BIDS
4. Convention Insulin Therapy – CIT
5. Intensive Insulin Therapy – IIT (Pumps)
6. Insulin + OAD combination
7. Analogs versus conventional
8. Inhaled Insulin, Insulin snuff, Oral HIM
Annals of Internal Medicine Volume 145 • Number 2, July 2006

www.drsarma.in
85
Insulin PreparationsInsulin Preparations
Rapidity of Action Insulin preparationUltra- rapid-actionOnset 10’ -20’ Peak 30 min
Lispro (Humalog), Glulisin (Apidra)Aspart (Novolog)
Short ActingOnset 30’ to 60’, Peak 2 hr
Regular (Human) InsulinHumulin R, Novolin R
Intermediate Acting (Human) or Analog 1 -4 h, Peak 4 -10 h
NPH (Human) Humulin N, Novolin NInsulin Detemir (analog) - Levemir
Long Acting 1-3 No Peak 24 h Insulin Glargine (Lantus)Mixtures (Human)1 h, P 3-12 h 70/30 or 50/50 Humulin, 70/30 NovolinMixtures (Analog)Onset 30’-1h, Peak 3-12 h
75/25 or 50/50 Humalog (NPL + Lispro)70/30 Novolog neutral (Protamin + Aspart

www.drsarma.in
86
Classification based on FBGClassification based on FBG
• LADA-Latent Autoimmune Diabetes of Adults
• MODY – Maturity Onset Diabetes of Young
1. Mild – FBG < 140 mg%
• Insulin virtually not needed
2. Moderate – FBG 141 to 250 mg%
• BIAIT – Basal IA Insulin Therapy
3. Severe – FBG > 250 but < 300 mg%
• AM – PM Insulin – Mix. SA & IA, I Pump
4. Very Severe – FBG > 300 mg%
• Treat as though it is Type 1 Diabetes

www.drsarma.in
87
Three Types of ProfilesThree Types of Profiles
Patient Profile Choice of Regimen Choice of Insulin
↑ PPG, N FBG, RA Insulin Pre Meal Human Regular or Lispro or Aspart
↑ FBG, Day time Euglycemia
Bed time IA Insulin +/- OAD
Insulin NPH or Detemir
↑ FBG, ↑ PPG ‘Round the clock hyperglycemia’
IA insulin BID orLA Insulin HS + OAD
NPH Detemir BID or 70:30 BID, or Glargine HS
Annals of Internal Medicine Volume 145 • Number 2, July 2006

www.drsarma.in
88
Insulin in T2DM
Single insulin regimen
Single insulin regimen
Single mixed insulin regimenSingle mixed
insulin regimen11
22
33
Mixed insulin regimen
Mixed insulin regimen
mixed & split insulin regimenmixed & split
insulin regimen
44
Bed time IA Insulin + OHA AMBed time IA Insulin + OHA AM
SA + IA Insulin AMSA + IA Insulin AM
AM IA insulin PM SA InsulinAM IA insulin PM SA Insulin
AM SA + IA PM SA + IA AM SA + IA PM SA + IA

www.drsarma.in
89
T2DM – NewTherapies
T2DM – NewTherapies

www.drsarma.in
90
Exubera (Inhaled Insulin)
Insulin Blisters for Aerosol

www.drsarma.in
91
Pramlintide
Amylin -a hormone secreted by the -cells of pancreas
It is very similar to Insulin in its action – Structure dif.
Amylin handles 20% of our glucose metabolism Pramlintide is an analog of natural hormone - Amylin It is available only as s.c inj. like insulin It slows gastric empting; It suppresses Glucagon;
It reduces HGO – all like insulin It is available as SYMLIN inj. For both forms of DM

www.drsarma.in
92
Exenatide
We have two hormones in intestines - Incretins
•GLP-1 (Glucagon Like Peptide-1) and
•GIP (Glucose dependent Insulinotropic Polypetide)
Normally Incretins are degraded by DPP IV enzyme Exenatide is a synthetic analog of GLP-1 – Mimetic It is very similar to the GLP-1 in venom of Gila mon. This is resistant to degradation by DPP IV enzyme Exenatide inj. enhances postprandial insulin secretion

www.drsarma.in
93
Gila (Hee-la) Monster
Lizard Spit

www.drsarma.in
94
Exenatide (Byetta)
www.drsarma.in
95
Liraglutide
Modified GLP-1 Binds to albumin Injection form only Can reduce fasting and PP
hyperglycemia It is an additional Rx. option Can be combined with OADs Does not cause hypoglycemia.

www.drsarma.in
96
Sitag‘Liptin’
Normally Incretins are degraded by DPP IV enzyme Liptins are compounds which inhibit the DDP IV Liptins increase the action of natural GLP-1 These are oral drugs – hence advantageous These ↑ postprandial insulin secretion via GLP-1 Sitag-liptin, Vildag-liptin, Sexag-liptin are useful Rx They are 2nd line agents. Combined with OADs Do not cause hypoglycemia.
www.drsarma.in
97
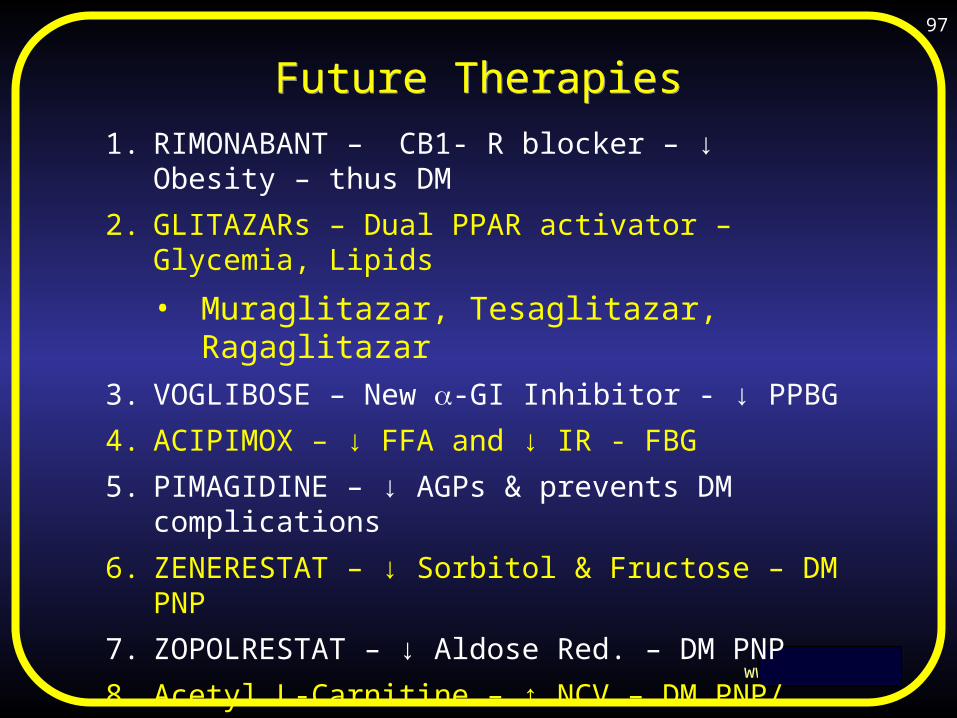
Future TherapiesFuture Therapies1. RIMONABANT – CB1- R blocker – ↓ Obesity –
thus DM
2. GLITAZARs – Dual PPAR activator – Glycemia, Lipids
• Muraglitazar, Tesaglitazar, Ragaglitazar
3. VOGLIBOSE – New -GI Inhibitor - ↓ PPBG
4. ACIPIMOX – ↓ FFA and ↓ IR - FBG
5. PIMAGIDINE – ↓ AGPs & prevents DM complications
6. ZENERESTAT – ↓ Sorbitol & Fructose – DM PNP
7. ZOPOLRESTAT – ↓ Aldose Red. – DM PNP
8. Acetyl L-Carnitine – ↑ NCV – DM PNP/ ANP
9. BIMOCLOMOL – ↑ Heat Shock Proteins – DR & DKD
10.EXO- 226 – ↓ Glycation of Proteins – DKD
11.Insu. Like GF, HIM 2 (oral), Englitazone – New TZD

www.drsarma.in
98
Future Diagnostic TestsFuture Diagnostic Tests
Glucose sensors – to be applied on to skin
Peel of patch tests – Read the Sugar in sweat
Micro needle inserted continuous monitors
Antibodies to insulin for insulin resistance
HbA1c monitors – like glucose monitors

www.drsarma.in
99
Glycosylation of hair
• Hair glycosylation using thiobarbituric acid TBA
• Glycosylation of hair is in diabetes mellitus
• Both insulin dependent , non-insulin dependent
• Glycosylation of hair is proportionate to HbA1c
• Due to the presence of hexosyl lysome in hair
• Long hair sample provides a long term record.
• May have forensic application & in population
studies.
BMJ, 1996, vol. 288 pp. 669-670

www.drsarma.in
100
Prevention ofComplicationsPrevention ofComplications

www.drsarma.in
101
How to prevention Complications of Diabetes ?
1. Weight reduction, Exercise
2. Strict control hyperglycemia
3. Achieving lipid profile targets
4. Smoking cessation
5. Rx. of Hypertension with ACEi/ ARB
6. Low dose aspirin therapy
7. Statin therapy for all T2DM
8. ACEi or ARB for all with MAU
9. Early detection and evaluation

www.drsarma.in
102
HT Rx. Algorithm in DMHT Rx. Algorithm in DM
BP > 130/80 (2 readings) No TOD / Al-
ACE/ARB + TLC 1 M
Goal BP 130/80Yes No
Add Diuretic
Add Verapamil
Add blocker
Yes
Yes
No
TLC cont.
>140/90/MAU/TOD
1 Month
Sub Amlodepine
No
No
No
Yes
Yes
1 Month
1 Month
1 Month ?
Diabetes Spectrum Vol. 5, # 3, 103-108

www.drsarma.in
103
Treatment of DyslipidemiaTreatment of Dyslipidemia
Every T2DM must get 10 mg of Atorvastatin LDL is raised – Statin or Statin+ Ezetemibe TG is raised – Fenofibrate HDL is low – Niacin Combined dyslipidemia – Combinations Lp(a) is raised – Niacin hs-CRP is raised – Aspirin & Statin (already)

www.drsarma.in
104
Take Home – A B C D ETake Home – A B C D E
A A1c – target of < 7%; Better 6% Aspirin for all DM ACEi or ARB for all DM
B Blood Pressure target of 130/80 Blood Glucose monitoring
C Cholesterol LDL <100, Statin for all DM
D Diet modifications, Do not smoke E Exercise 45’ every day, Education
on DM Equivalent to having CAD is DM
www.drsarma.in
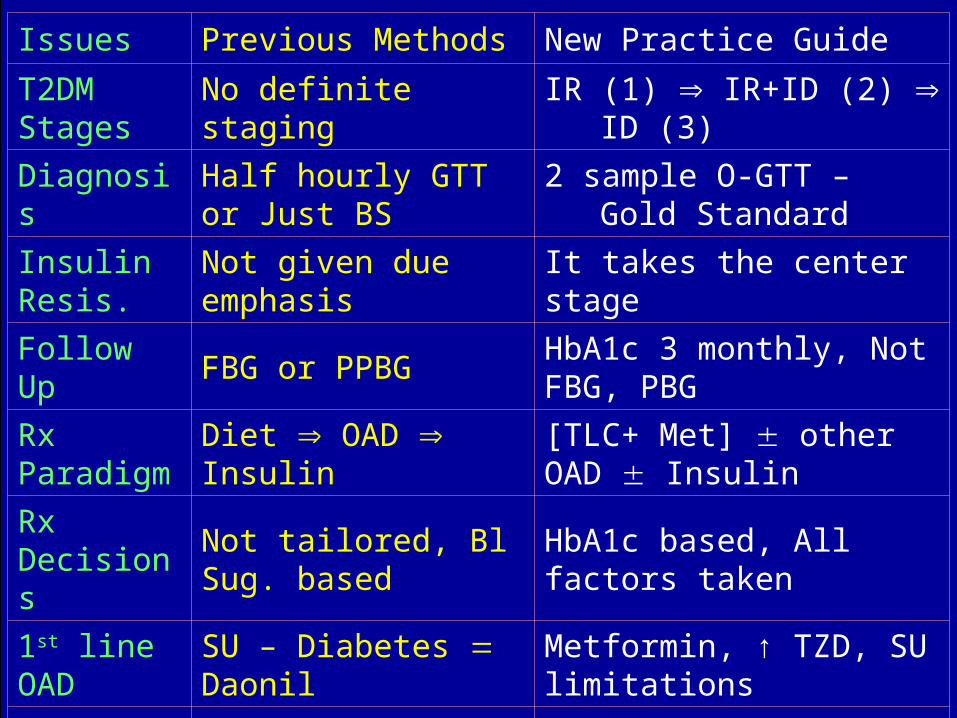
105Issues Previous Methods New Practice GuideT2DM Stages No definite staging IR (1) IR+ID (2) ID (3)Diagnosis Half hourly GTT or Just BS 2 sample O-GTT – Gold StandardInsulin Resis. Not given due emphasis It takes the center stageFollow Up FBG or PPBG HbA1c 3 monthly, Not FBG, PBG
Rx Paradigm Diet OAD Insulin [TLC+ Met] other OAD Insulin
Rx Decisions Not tailored, Bl Sug. based HbA1c based, All factors taken1st line OAD SU – Diabetes Daonil Metformin, ↑ TZD, SU limitationsInsulin use Delayed until pt is burnt out Early basal Insulin or intens. InsulFocus on Glycemic control alone Total Metabolic control A,B,CPrescriptions Limited to OAD and Insulin Aspirin, Statin, ACEi + DM Rx.Prevention Was not the emphasis Prevent DM & prevent complicati.Emphasis Not worried for apoptosis Preserve the cell at all costs

www.drsarma.in
106
Let us together
win the waragainst
Diabetes
Let us together
win the waragainst
Diabetes

www.drsarma.in
107
Wish You All A Happy New Year