Embed Size (px)
Citation preview
2016-202016-20
Evolving CDI
WSLHD’s Journey to Clinical Documentation Integrity
Nina LeanWSLHD District Clinical Coding ManagerHealth Informatics I Directorate of Finance
2The Early Days of CDIWhy the CDS structure?
WSLHD:
• Population growth at twice the rate of rest of NSW
• Growing burden of disease; patients living longer; chronic illness
• Multimillion dollar capital redevelopments at our inpatient facilities
• Increased bed numbers and separations
• Increased separations relates directly to the workload of the clinical coding team
• Already significantly under resourced (coders; coding educators; auditors)
• ABM Environment
• Documentation clarity extremely important to reflect complexity & ultimately appropriate funding
2012: Serious concern about Westmead financial status
• Large A1, tertiary referral facility but complexity lower than Blacktown (then a small metropolitan facility)
• New Coding Manager: Serious coding quality concern
• External Coding Audit evidenced a 29% DRG error rate
• Significant loss in revenue
• CE initiated “Recoding Exercise” recovered $5M
LEARNINGS:
Coding & Documentation Needed improvement
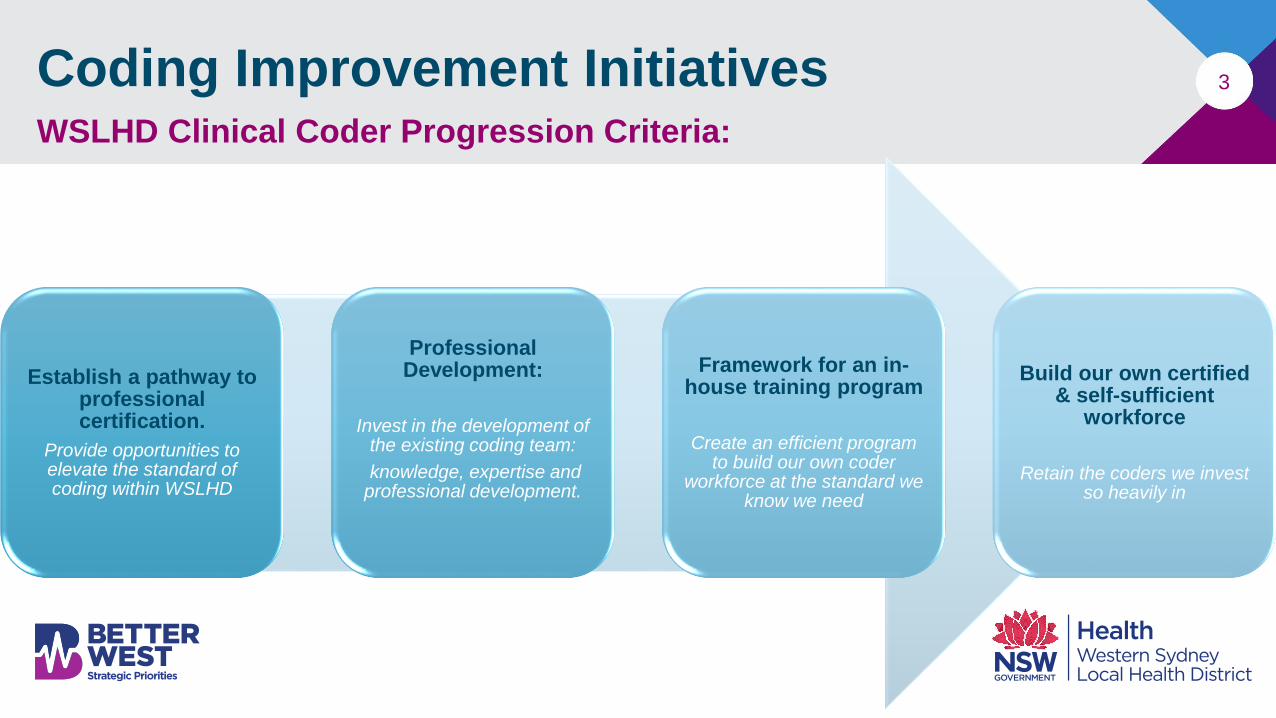
3Coding Improvement InitiativesWSLHD Clinical Coder Progression Criteria:
Establish a pathway to professional certification.
Provide opportunities to elevate the standard of coding within WSLHD
Professional Development:
Invest in the development of the existing coding team:
knowledge, expertise and professional development.
Framework for an in-house training program
Create an efficient program to build our own coder
workforce at the standard we know we need
Build our own certified & self-sufficient
workforce
Retain the coders we invest so heavily in
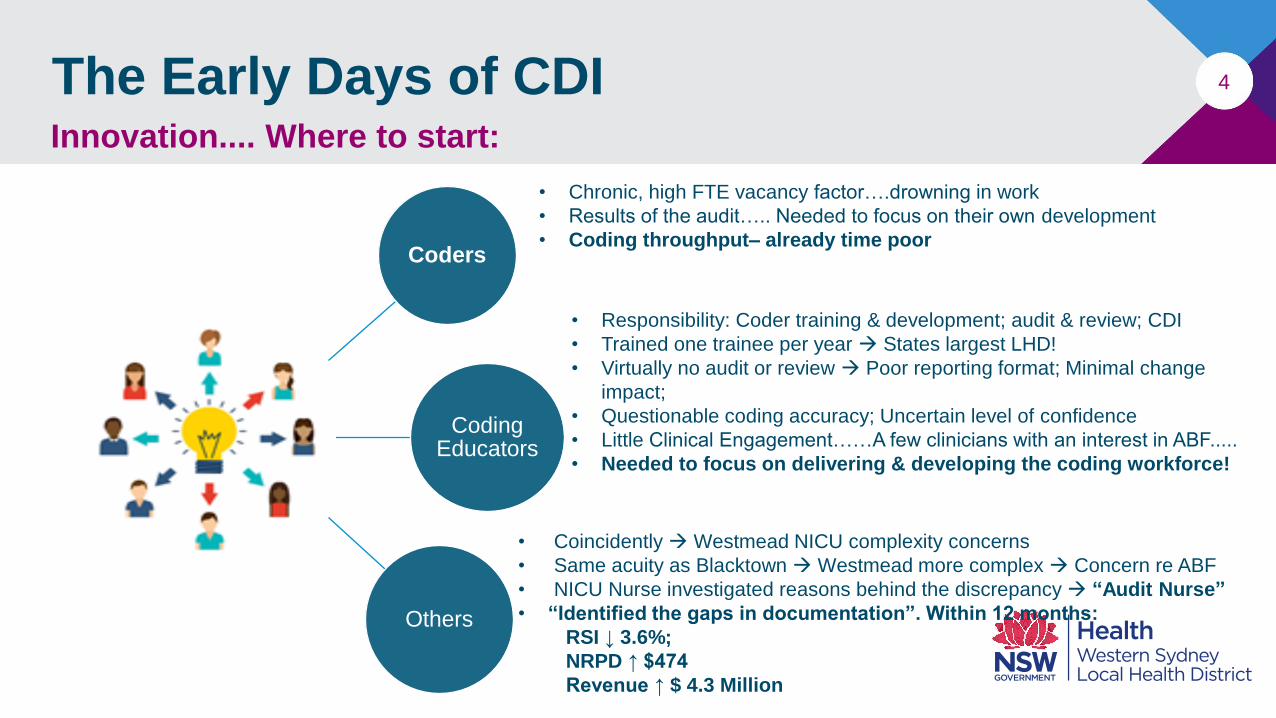
4The Early Days of CDIInnovation.... Where to start:
Coders
Coding Educators
Others
• Responsibility: Coder training & development; audit & review; CDI
• Trained one trainee per year States largest LHD!
• Virtually no audit or review Poor reporting format; Minimal change
impact;
• Questionable coding accuracy; Uncertain level of confidence
• Little Clinical Engagement……A few clinicians with an interest in ABF.....
• Needed to focus on delivering & developing the coding workforce!
• Chronic, high FTE vacancy factor….drowning in work
• Results of the audit….. Needed to focus on their own development
• Coding throughput– already time poor
• Coincidently Westmead NICU complexity concerns
• Same acuity as Blacktown Westmead more complex Concern re ABF
• NICU Nurse investigated reasons behind the discrepancy “Audit Nurse”
• “Identified the gaps in documentation”. Within 12 months:
RSI ↓ 3.6%;
NRPD ↑ $474
Revenue ↑ $ 4.3 Million
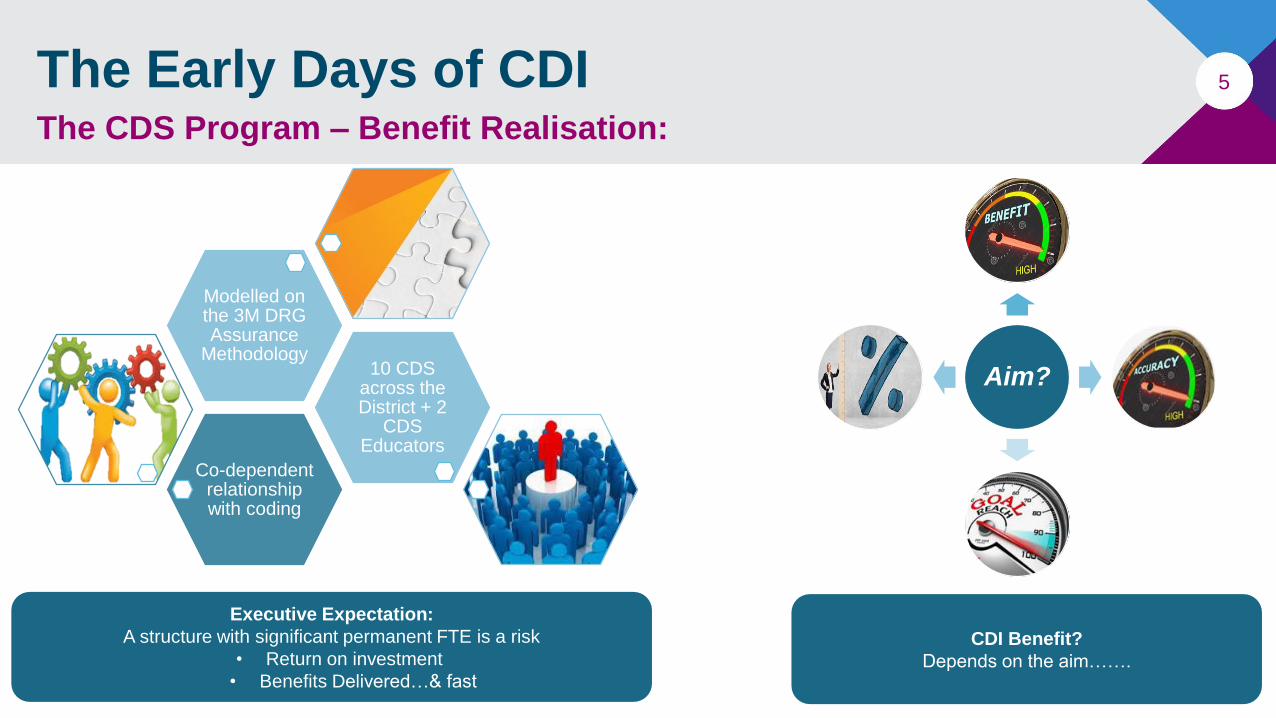
5The Early Days of CDIThe CDS Program – Benefit Realisation:
Co-dependent relationship with coding
10 CDS across the District + 2
CDS Educators
Modelled on the 3M DRG Assurance
Methodology
Executive Expectation:
A structure with significant permanent FTE is a risk
• Return on investment
• Benefits Delivered…& fast!
Aim?
CDI Benefit?
Depends on the aim…….
6The Early Days of CDIThe Aim:
Capture the highest specificity from improved clinical documentation to support accurate and appropriate reimbursement.
Improve data validity to reflect true organisational complexity
And ultimately……
Deliver information that supports informed decision making
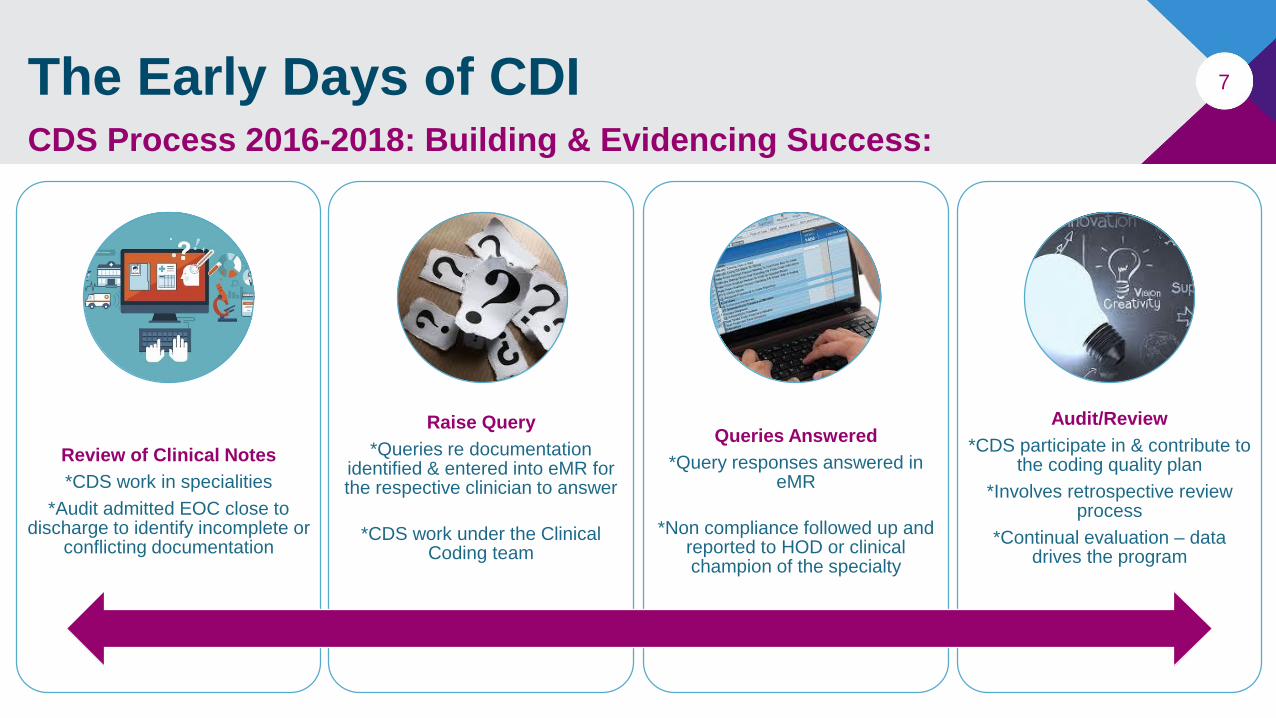
7The Early Days of CDI
Review of Clinical Notes
*CDS work in specialities
*Audit admitted EOC close to discharge to identify incomplete or
conflicting documentation
Raise Query
*Queries re documentation identified & entered into eMR for the respective clinician to answer
*CDS work under the Clinical Coding team
Queries Answered
*Query responses answered in eMR
*Non compliance followed up and reported to HOD or clinical champion of the specialty
Audit/Review
*CDS participate in & contribute to the coding quality plan
*Involves retrospective review process
*Continual evaluation – data drives the program
CDS Process 2016-2018: Building & Evidencing Success:
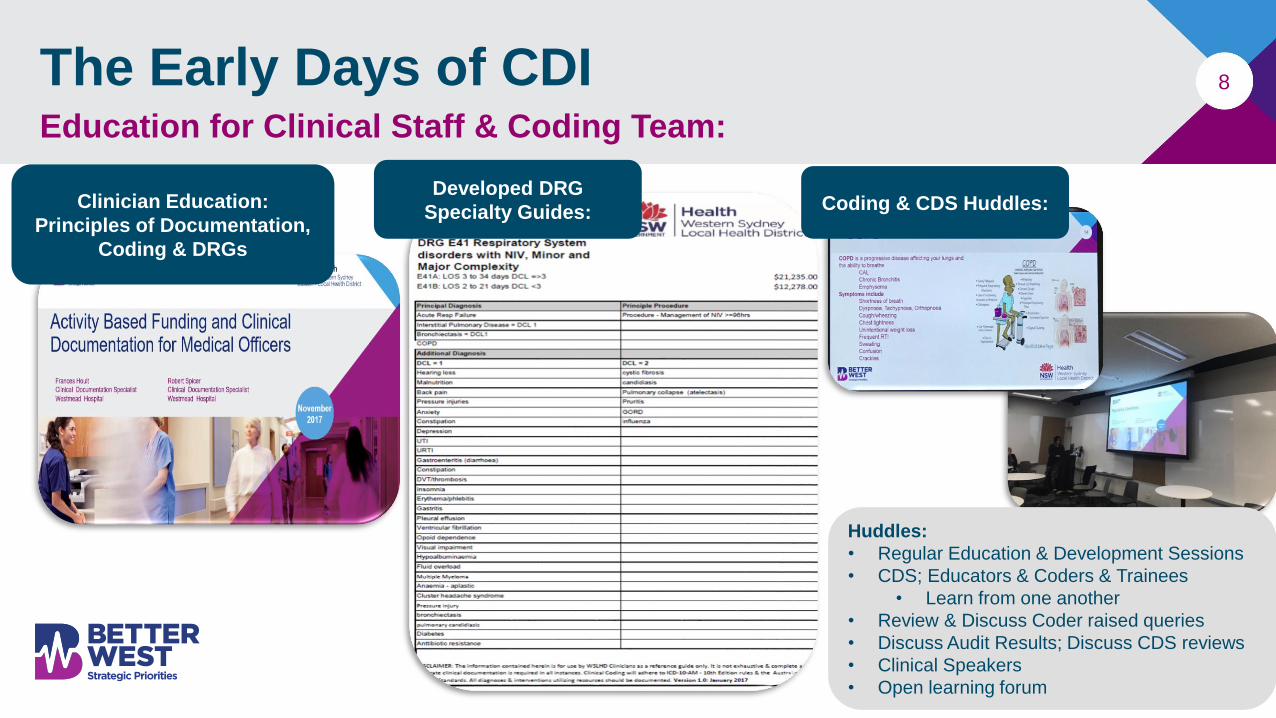
8The Early Days of CDIEducation for Clinical Staff & Coding Team:
Clinician Education:
Principles of Documentation,
Coding & DRGs
Developed DRG
Specialty Guides:
Huddles:
• Regular Education & Development Sessions
• CDS; Educators & Coders & Trainees
• Learn from one another
• Review & Discuss Coder raised queries
• Discuss Audit Results; Discuss CDS reviews
• Clinical Speakers
• Open learning forum
Coding & CDS Huddles:
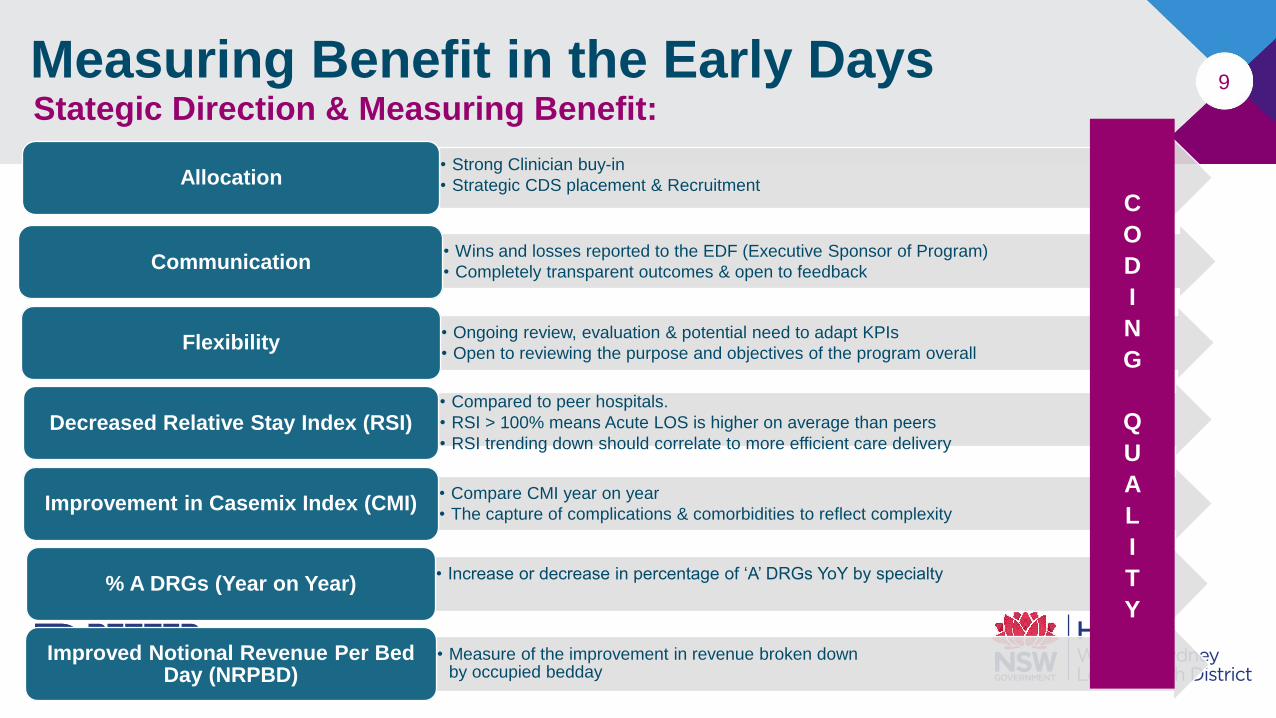
9Measuring Benefit in the Early DaysStategic Direction & Measuring Benefit:
• Strong Clinician buy-in
• Strategic CDS placement & Recruitment Allocation
• Wins and losses reported to the EDF (Executive Sponsor of Program)
• Completely transparent outcomes & open to feedbackCommunication
• Ongoing review, evaluation & potential need to adapt KPIs
• Open to reviewing the purpose and objectives of the program overallFlexibility
• Compared to peer hospitals.
• RSI > 100% means Acute LOS is higher on average than peers
• RSI trending down should correlate to more efficient care deliveryDecreased Relative Stay Index (RSI)
• Compare CMI year on year
• The capture of complications & comorbidities to reflect complexityImprovement in Casemix Index (CMI)
• Increase or decrease in percentage of ‘A’ DRGs YoY by specialty% A DRGs (Year on Year)
• Measure of the improvement in revenue broken down by occupied bedday
Improved Notional Revenue Per Bed Day (NRPBD)
C
O
D
I
N
G
Q
U
A
L
I
T
Y
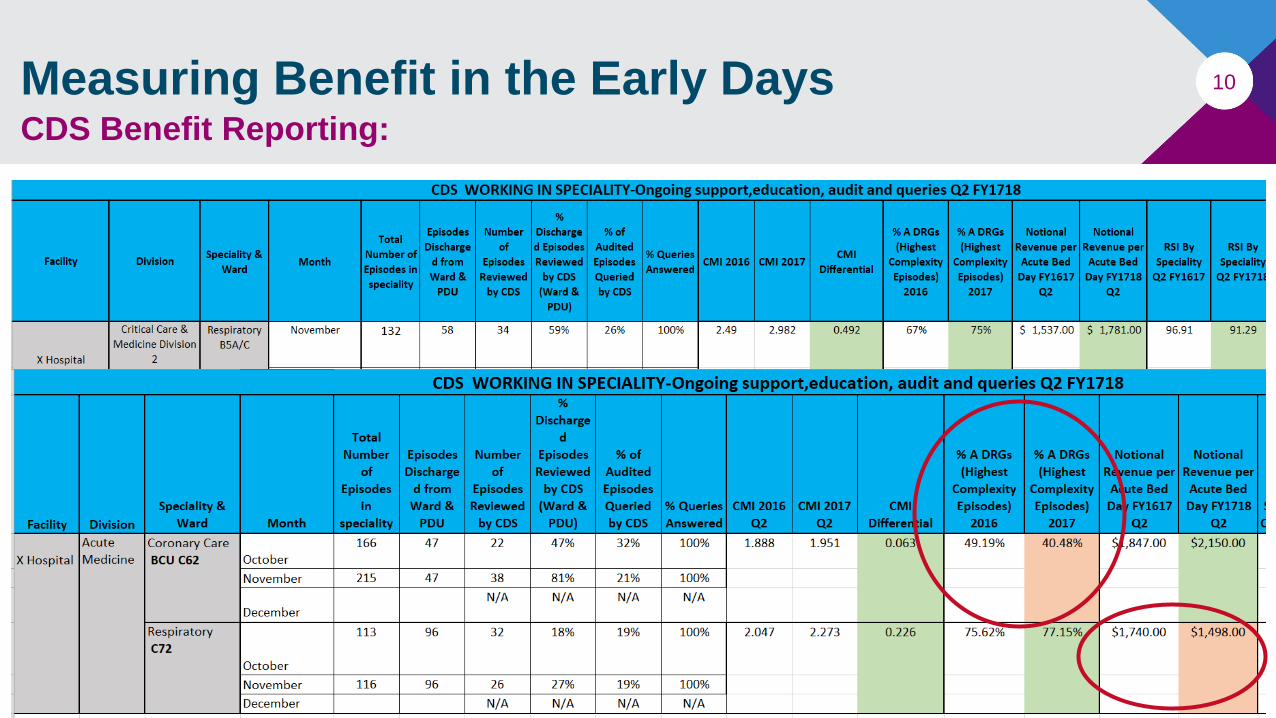
10Measuring Benefit in the Early DaysCDS Benefit Reporting:
11
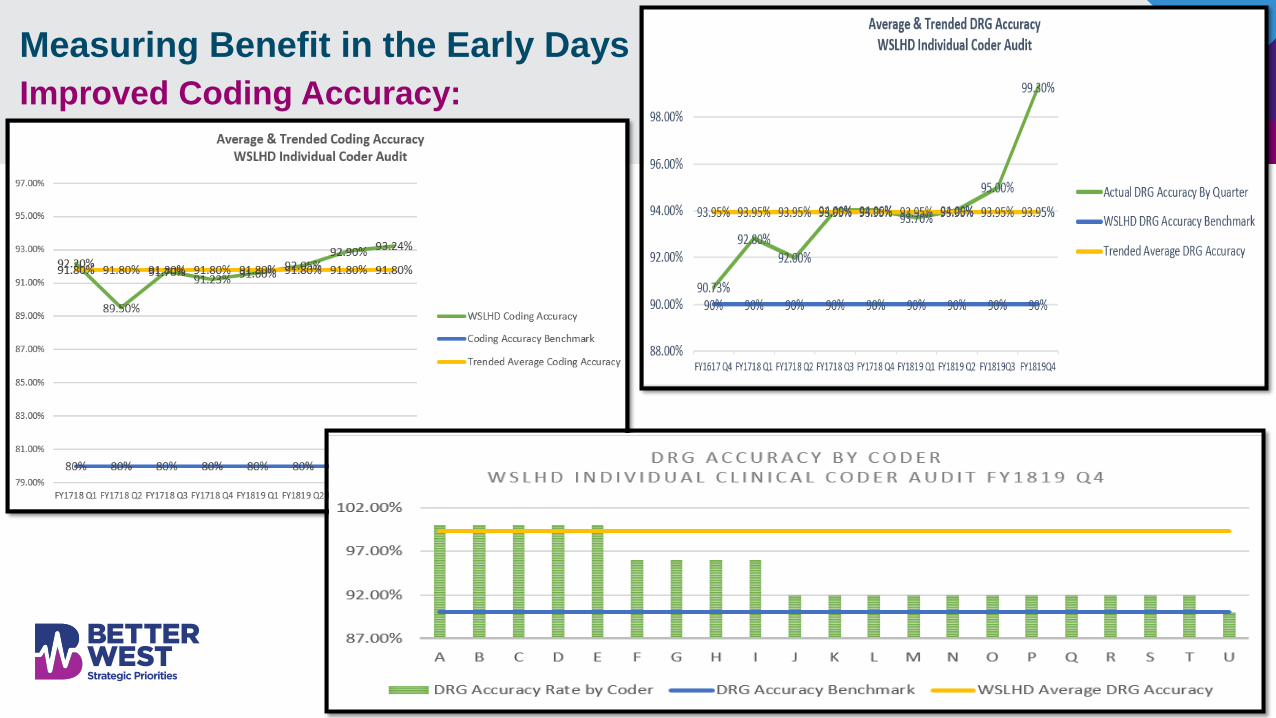
Measuring Benefit in the Early Days
Improved Coding Accuracy:

Better
CDI strategies…..
What to do when the benefits
start to flatten….
13The need for better CDI processes:
Remembering….Benefit is directly related to our aim
The need for concurrent audit and review:
• While robust, our audit practices were largely retrospective
• “Confidence Point” for informed decision making Often 6+ months post coding
• Querying doctors (many had moved on); FP&A meetings look at financial status of the organisation a week into the new month!
ICD-10-AM, 11th Edition & CCPF:
• We knew we were coding and applying CDS process ethically & we knew our coding accuracy was high (internal audit results matched large scale external coding audit) but it was evident that:
• Conditions that met criteria for code assignment as per ACS0002 & ACS0010 would decrease
• It would affect DCLs that drive case complexity
• ???? Decrease in NWAU
The impact of EMR Integration on Documentation Integrity……
• Regardless of being paper or electronic good record keeping should:Enable continuity of care…Enhance communication between healthcare professionals…Accurately reflect the patient journey
By early 2019: It was apparent the “aim” was quickly changing….
While we were confident that EOCs we had a “touch point” to were highly accurate (documentation & coding)….
The time had come to ensure that accuracy extended to culture change within our Organisation……
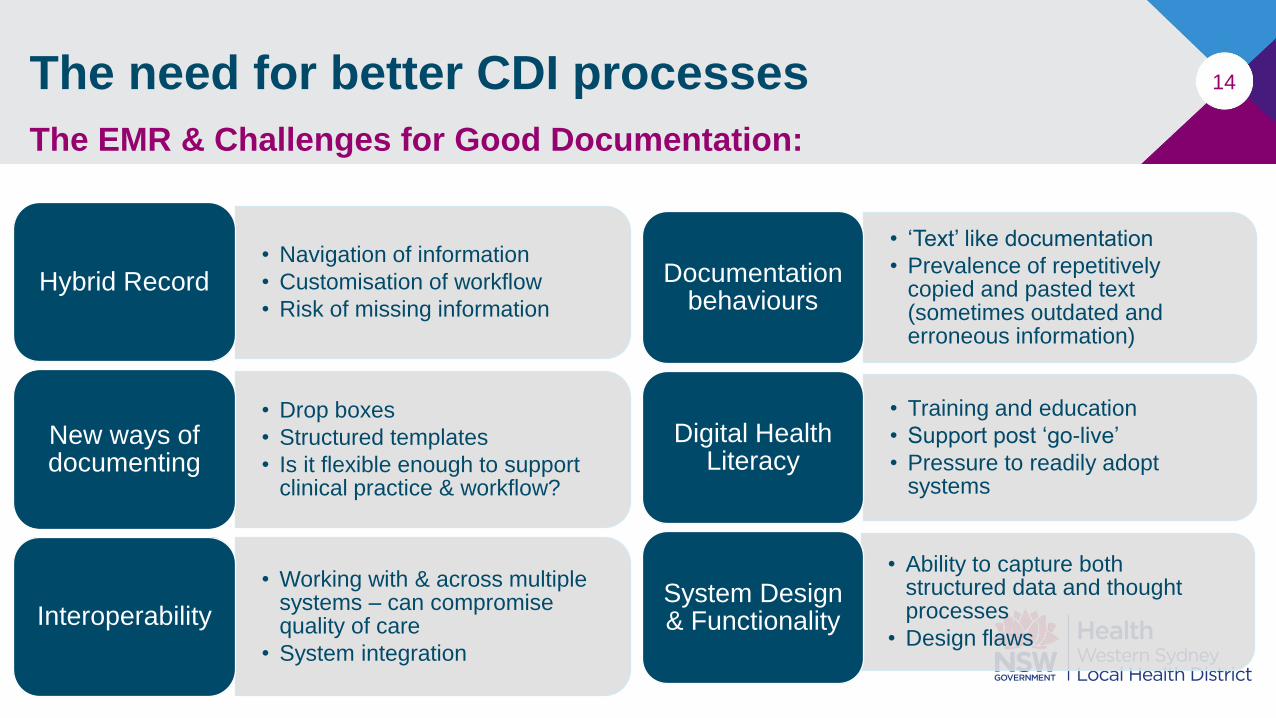
14
• Navigation of information
• Customisation of workflow
• Risk of missing informationHybrid Record
• Drop boxes
• Structured templates
• Is it flexible enough to support clinical practice & workflow?
New ways of documenting
• Working with & across multiple systems – can compromise quality of care
• System integration
Interoperability
• ‘Text’ like documentation
• Prevalence of repetitively copied and pasted text (sometimes outdated and erroneous information)
Documentation behaviours
• Training and education
• Support post ‘go-live’
• Pressure to readily adopt systems
Digital Health Literacy
• Ability to capture both structured data and thought processes
• Design flaws
System Design & Functionality
The need for better CDI processes
The EMR & Challenges for Good Documentation:
15The need for better CDI processesThe Impact of Clinical Documentation:
Clinical Documentation is used in:
• Patient Care & Safety
• Communication / Handover
• Research, Teaching & Health Care Planning
• Legal document – Complaints; Subpoenas
• Healthcare Funding (Activity Based Funding)
16Aim of Modern CDI Initiatives:Documentation with Integrity!
Documentation that accurately reflects the inpatient journey!
• Clear
• Legible
• Complete
• Highly Specific
• Non-Ambiguous
• Non-Conflicting
• High quality
• Demonstrates the safe and high quality care provided
And ultimately:
A record that meets the need of all its uses, and exists as the
source of recall long after the patient leaves hospital
17Aim of Modern CDI InitiativesThe need to refocus Coding & CDS Responsibility:Mandated & significant
changes to coding & DRG classification
systems
•Coding Educators must be involved in documentation improvement initiatives… they are the experts
•CDS role needed to diversify to facilitate clinical documentation to meet the needs of all its uses & not funding alone
ICD-10-AM, 11th Edition
• Most significant impact is on the ability to assign additional diagnosis codes
• Evident that there would be a decrease in coding of conditions that met criteria for code assignment as per ACS0002 & ACS0010 pre 11th
edition
• Same concerns raised by LHD peers
AR-DRG Version 10.0 (Impending)
• DCLs dropped from many conditions considered clinically insignificant…….
• Although that’s open to interpretation!
Concurrent Coding Audits
• Change: Retrospective to concurrent audit
• Episodes coded the week prior meeting targeted NWAU or DRGs selection are reviewed by coding auditors the next week
• Queries raised while the doctor remembers the patient!
• This demonstrates the benefit of CDS interaction better than anything else!
18
CDI Process 2020Complete Documentation that demonstrates high quality care:
Review Clinical Notes to identify gaps & Raise queries
Take coder queries to clinicians
Retrospectively Raise Queries or directly interact with clinician
involved in care following ward rounds
Don’t only query if it carries a DCL!
CDS resources are now spread further across the organisation!
Ward Rounding
Record reviewed first; questions ready; interacts with clinical team at the point of documentation
entry!
Capture clear, complete, non-ambiguous & non-misleading
clinical documentation at the point of entry
Clinicians must document the ward round. Can’t be delegated
Documentation that reflects the patient journey with no need for further clarification at the time
of coding
Facilitate Basic EMR Support
Capturing the PDx!
One on one interaction with the junior clinicians documenting in the record…… timely reminder
about the need to document appropriately
Documentation Roadshows
Presented by the most senior members of the Health
Informatics team. Sponsored by EDF & EDMS
Highlight clinical responsibility
Demonstrate the difference between low & high quality
documentation….. Impact of poor documentation.
19CDS RoundingSetup & Process:
Executive Support & Engagement
Engage HOD: Explain need & purpose of rounding
Commitment to round at convenient times
Adapt rounding to suit individual speciality
requirements
Rounding Process
Often > one team per Specialty. Rounding
undertaken strategically to ensure interaction with all
teams within specialty (spread the message
further)
Consultants & Advanced Trainees run the ward
round….
If they are “speaking” the right terminology, the junior medical team will document
it!
CDS Review of ward inpatient documentation
the day prior
Record (in a data collection spreadsheet) where
clarification is required *(Unclear, incomplete,
conflicting or misleading….eg. PDx unclear)
Query written if appropriate or note made to clarify
verbally (at round)
During Ward Round
Resolved “issues” requiring clarification CDS clarify with JMO post ward round so as not to slow it down
(ward round only discusses current issues)
CDS listens at round Issues discussed that are documented fully CDS raises it and explains the
need for it to be documented in medical progress note
Rounding at agreed times on a hospital wide basis
All education occurs away from the patient bedside
Queries on resolved issues (depending on time
limitation) may occur after the round
Rounding process is fluid.
What works on one ward doesn’t work on another.
Adapt to the needs of the clinical team….Initiation of CDS Peer
Review……

Measuring
“modern” CDI Benefit…..
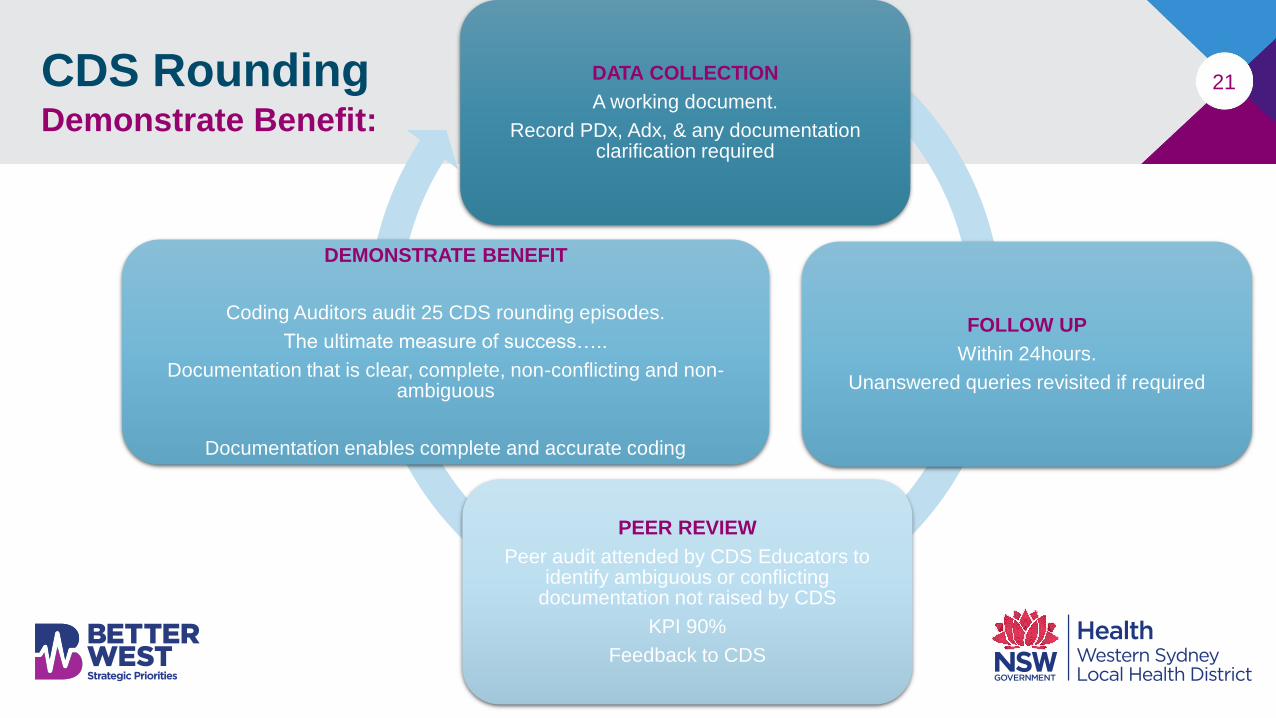
21CDS RoundingDemonstrate Benefit:
DATA COLLECTION
A working document.
Record PDx, Adx, & any documentation clarification required
FOLLOW UP
Within 24hours.
Unanswered queries revisited if required
PEER REVIEW
Peer audit attended by CDS Educators to identify ambiguous or conflicting
documentation not raised by CDS
KPI 90%
Feedback to CDS
DEMONSTRATE BENEFIT
Coding Auditors audit 25 CDS rounding episodes.
The ultimate measure of success…..
Documentation that is clear, complete, non-conflicting and non-ambiguous
Documentation enables complete and accurate coding
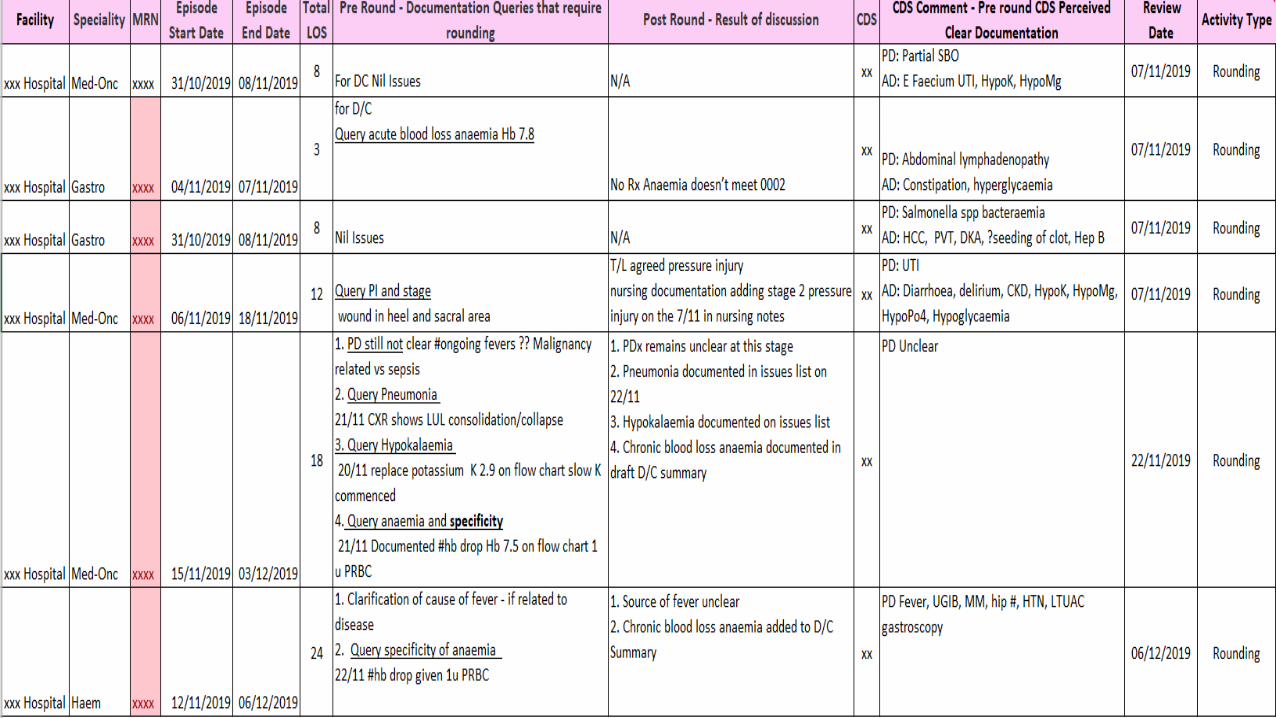
22CDS Rounding
Demonstrate Benefit:
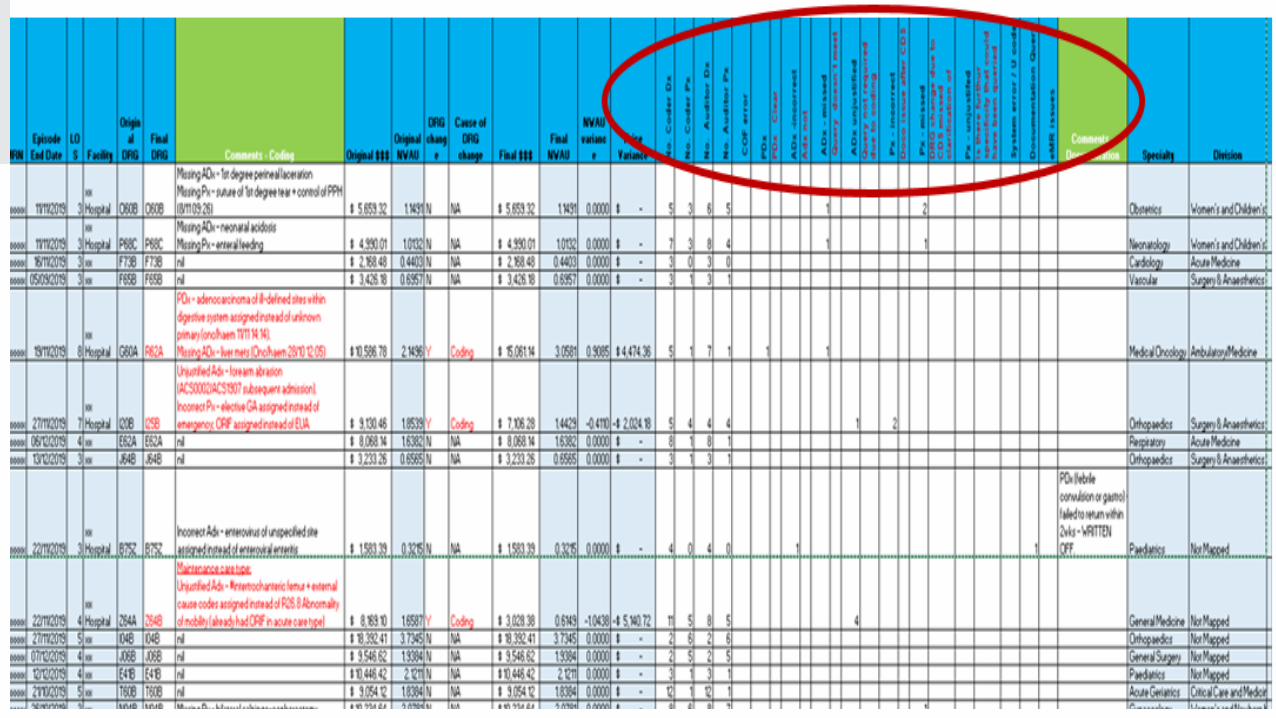
23
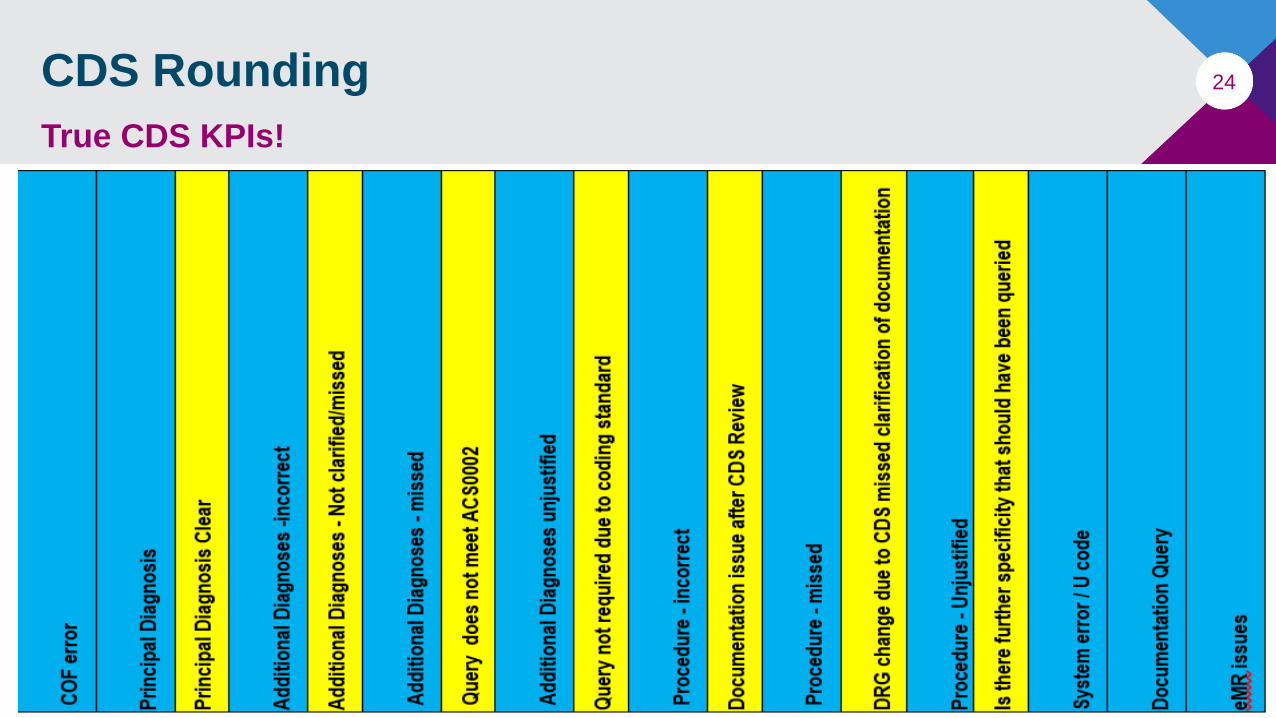
24CDS Rounding
True CDS KPIs!
25Clinical Documentation IntegrityWhat Works… What Doesn’t?
True Documentation Integrity:
• Identify the “Real” Gaps….. EMR Forms, Clinical Workflow
• Data Enhances Models of Care
• Refined Processes & Minimal Clinical Variation
• Professional Development
• Safe Practice - HAC Awareness & Risk Mitigation
• End to End Assessment Capture
• Improved Communication
• Improved Patient Experience
• Comprehensive & Continuity of Care
• Accountability
• Data Quality
• EMR Documentation & Workflow Efficiency
26Clinical Documentation Integrity
The Ultimate Aim: Better Value Care
Bridge the gap eMROpportunities
Quality and Safety….HACs
Understand the Impact of Clinical Variation
Drives Benchmarking & Operational Efficiency
Leading Better Value Care
Thank youNina Lean
WSLHD District Clinical Coding Manager,
Health Informatics WSLHD
M:0418 234 625