Embed Size (px)
Citation preview

WHOQOL-DISABILITIES MODULE
MANUAL
WORLD HEALTH ORGANIZATION
AUGUST 2011

The WHOQOL-
DISABILITIES module – manual
2
This manual was written by Mick Power on behalf of the WHOQOL-DIS Group. The
study was funded by the European Commission Framework 6 Programme, contract
SP23-CT-2005-513723, and was carried out under the auspices of the World Health
Organization Quality of Life Group (WHOQOL Group). The WHOQOL-DIS Group
comprises a coordinating group and collaborating investigators in each of the following
field centres: Professor M. Power, Dr. A. Green, Dr C.Catchpole, and Ms. J.MacLeod,
University of Edinburgh, UK; Dr. Somnath Chatterji, World Health Organization,
Geneva; Dr R. Lucas-Carrasco, Fundacio Insititut Català de l‟Envelliment, Barcelona,
Spain; Professor A. Leplege, University of Paris 7; Dr Eva Dragomirecka, Prague
Psychiatric Centre; Professor Martin Eisemann, University of Tromso; Professor Erhan
Eser and Professor Omer Aydemir Celal Bayar University, Turkey; Dr. Jelena
Ceremnych, Institute of Experimental and Clinical Medicine, Vilnius; Dr. Rosa
Frazzica, Dr. Pasquale Di Mattia and Dr. Marilena Pinco, Centre for Training and
Research in Public Health, Sicily; Professor Monika Bullinger and Dr. Silke Schmidt,
Institute of Medical Psychology, Hamburg; Professor Guus van Heck, Dr Jolanda de
VRies, Ms Brenda Den Oudsten, Tilburg University; Professor L. Kullman, Eötvös
Loránd University, Faculty of Special Education, Budapest, Hungary; Professor Ji-Qian
Fang, Dr Yuantao Hao, Sun Yat-sen University, Guangzhou, China; Professor Marcelo
Fleck Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil; Professor
S.Chaturvedi, National Insitiute for Mental Health and Neurosciences, Bangalore, India;
Professor Laura Schwartzmann, Universidad de la Republica, Montevideo, Uruguay;
Professor Kathryn McPherson, Professor Rex Billington, Auckland University of
Technology; Dr Keith McVilly, RMIT, Dr Graeme Hawthorne, Melbourne University,
Australia.

The WHOQOL-
DISABILITIES module – manual
3
Further information can be obtained from:
Professor Mick Power
Section of Clinical and Health Psychology
University of Edinburgh
Medical School
Teviot Place
Edinburgh EH8 9AG, UK.
Email: [email protected]
This document is not issued to the general public, and all rights are reserved by the
World Health Organization (WHO). This document may not be reviewed, abstracted,
quoted, reproduced, translated, referred to in bibliographical matter or cited, in part or in
whole, without the prior written permission of WHO. No part of this document may be
stored in a retrieval system or transmitted in any form by any means - electronic, me-
chanical or other - without the prior written permission of WHO.

The WHOQOL-
DISABILITIES module – manual
4
Contents Introduction . . . . . . . . 5
The WHOQOL-DIS project. . . . . . . 7
Development of the WHOQOL-DIS module . . . . 7
Overview . . . . . . . . 7
Initial development . . . . . . . 8
Pilot study . . . . . . . . 9
Field Trial . . . . . . . . 11
Summary of results of questionnaire development . . . 13
Description of the instrument . . . . . . 15
Scale structure . . . . . . . 15
Scoring . . . . . . . . 16
Psychometric properties . . . . . . . 19
Interpretation . . . . . . . . 27
Administration – suggested uses . . . . . . 27
Additional New Measures 28
1) Proxy Measures 28
2) Attitudes to Disability Scale 32
3) The Quality of Care Scale 34
References . . . . . . . . 36
Appendix . . . . . . . . 37
I Final set of items for WHOQOL-DIS Module . . . .
II SPSS Syntax File .
III Reference Data . . . . . . .
IV ADS . . . . . . .
V QOCS . . . . . . .
VI List of Centres . . . . .

The WHOQOL-
DISABILITIES module – manual
5
Introduction
The development of the WHOQOL measures of quality of life (QOL) was first carried
out in fifteen different centres worldwide (WHOQOL Group, 1998a) and there are now
over forty centres involved in the project. The two main generic instruments that have
been developed are the WHOQOL-100 and the WHOQOL-BREF (WHOQOL Group,
1998b) which is a shorter 26-item version. The WHOQOL-100 has a hierarchical
structure that includes overall quality of life, a next level of domains, facets within each
domain, and then four specific items for each facet. The shorter WHOQOL-BREF has a
similar hierarchical organisation, except that each facet is represented by a single item
and there are fewer domains. The existence of the WHOQOL as a generic measure of
quality of life, which has been developed cross-culturally and which has good
psychometric properties, makes it ideal for adaptation to the assessment of quality of
life in people with disabilities, in the same way that we have recently produced a
module for use with older adults, the WHOQOL-OLD (Power et al., 2005).
One of the first questions that arise in the generic assessment of quality of life is
whether or not questionnaires that have been developed in adult populations can be used
for people with intellectual disabilities (normally defined by an IQ as less than 70, but
referred to by a variety of terms in different cultures). The earlier focus in intellectual
disabilities research was on objective indicators of quality of life, because of concerns
about the assessment of subjective states in people with intellectual disabilities
(Emerson & Hatton, 1994). Subsequent work for example by Schalock and Keith
(1994) in community settings, and by Cummins (1997) in the adaptation of his own
measure of objective combined with subjective quality of life have shown that it is
possible to develop and adapt measures of quality of life for use both directly with
people with intellectual disability and as proxy measures by relatives and carers.
The rationale for including both physical and intellectual disabilities together comes
from World Health Organization framework for disability, the ICF, which focuses on an
integrative approach to the formulation of health status (WHO, 2001). The ICF is a
Note: Parts of the present manual are adapted from the main publication for the WHOQOL-DIS
module (Power, Green & The WHOQOL-DIS Group, 2010).

The WHOQOL-
DISABILITIES module – manual
6
comprehensive classification system that takes a bio-psychosocial approach to
understanding impairment, handicap and disability. The medical model and the social
model have traditionally been the two main approaches for classifying and measuring
disability (WHO, 2001), but these are integrated in the more recent ICF framework.
A second question arises of whether or not there are specific areas of quality of life that
may be more important for people with either intellectual or physical disabilities and
that therefore should supplement a generic adult questionnaire in order to provide a
broader-band and more valid general assessment. Examples of this problem exist even
for younger adults simply through the comparison of established generic measures. Two
facets (Sensory Problems, and Communication) that were originally included in the
pilot WHOQOL (WHOQOL Group, 1998a), but dropped because of psychometric
problems in a primarily younger adult population, are good examples of facets that may
need to be added to a module for adults with disabilities. This manual will address both
of these questions in relation to the WHOQOL: do the generic forms (in particular, the
WHOQOL-BREF) perform well, on a range of criteria, with adults with disabilities?
And, second, which additional facets need to be added to the adult generic form in order
to assess quality of life adequately in this disabled group?
The manual also considers the question of whether it is possible to have a single cross-
cultural disabilities module or whether each culture requires its own culture-specific
module. Although it has been possible to generate a common generic adult version of
the WHOQOL and this has been supported by empirical analyses (WHOQOL Group,
19998a; 1998b; Power et al., 1999), the possibility remains that diverse attitudes across
cultures towards adults with disabilities may require the production of different adults
modules, especially for people with intellectual disabilities. The feedback from the
focus groups and the data analyses allowed us to ask the question of how well the
existing WHOQOL items perform when used with people with disabilities. That is, one
of the key objectives of the research was to test the question of whether the existing
WHOQOL items only need to be supplemented with an additional module or whether
these generic items also need to be altered in some way or another such as through
simplification of item wording.

The WHOQOL-
DISABILITIES module – manual
7
In summary, the overall aim of the present research was to adapt the generic version of
the WHOQOL for use with adults with physical or intellectual disabilities and then test
its use in a series of cross-cultural field trials. This adaptation consisted of the
development of a supplementary module that can be added to the existing WHOQOL
instruments. The end point of the work however was the production of a Disabilities
WHOQOL module that can be used in conjunction with the WHOQOL-BREF and
WHOQOL-100 in a wide variety of studies including population epidemiology, service
development, and clinical intervention trials in which issues about quality of life are
crucial. The work presented in this manual will focus on the results from each of the
steps in the generation of the WHOQOL-DIS module.
The WHOQOL-DIS Project
The WHOQOL-DIS project aimed at developing and testing a quality of life assessment
for adults with physical disabilities or intelelctual disabilities. It started in 2005, as a
scientific co-operation of several centres. The aim of the project was to develop and test
a generic measure of quality of life in adults with disabilities for international/ cross-
cultural use. The project was funded by the European Commission Sixth Framework,
SP23-CT-2005-513723 and was carried out under the auspices of the World Health
Organization Quality of Life Group (WHOQOL Group). The questionnaire
development was conducted according to the following multi-step procedure: (a) the
initial development of relevant quality of life questions (items) and their translation: fo-
cus group work within the collaborating centres and an iterative Delphi technique pro-
cess between the collaborating centres for item generation; (b) the pilot testing of the
questionnaire with appropriate modification (refinement, item reduction); (c) the field
trial testing of the questionnaire; (d) the final analysis: statistical analysis, project report
and publication of the manual .
Development of the WHOQOL-DIS module
Overview
The WHOQOL-DIS Coordinating Field Centre in Edinburgh produced a draft protocol
based on the previous WHOQOL Group experiences in conducting international

The WHOQOL-
DISABILITIES module – manual
8
collaborative research for the development of the WHOQOL-100 and WHOQOL-BREF
(The WHOQOL Group 1998a, 1998b). Following initial protocol development, it was
circulated to each Field Centre for comment. It was revised using a Delphi technique
until there was agreement among the participating Centres. In summary, the steps for
the development of the WHOQOL-DIS followed the published WHOQOL methodo-
logy, which consisted of focus group work in collaborating centres, item generation, pi-
lot testing, refinement and item reduction, and then field trial testing of the instrument,
as described below. Prior to the focus group exercise the iterative Delphi process was
also used to identify gaps in the coverage of the WHOQOL-100 that might be relevant
for adults with disabilities, and any other issues about the use of the WHOQOL with
older adults. The proposed WHOQOL-DIS module underwent various steps of
instrument development in a simultaneous cross-cultural approach (see Power, Green &
The WHOQOL-DIS Group, 2010). After conducting focus groups and forming an
international item pool, only those items were selected that pertain to people with
disabilities. Further steps included a translation process following international
guidelines (Guillemin et al. 1993) and the pilot testing of the instrument (Bullinger et al.
2002). The field study analysis of the WHOQOL-DIS module comprised additional
psychometric evaluations of both the single items and the scale structure. These analy-
ses lead to the final version of the WHOQOL-OLD module and are reported in detail
elsewhere (Power, Green & The WHOQOL-DIS Group, 2010).
Initial development
The protocol for conducting focus groups established a common framework for inter-
preting and assessing the data reported by each Centre. Once agreed, the protocol was
used in each Centre as the guide for planning and conducting focus groups for the pur-
pose of eliciting the quality of life concerns of adults with disability, and for reporting
the data back to the Edinburgh Coordinating Centre. The focus group discussions
included four parts: (a) a general unstructured discussion on the dimensions of quality
of life that were important for adults with disabilities; (b) a commentary on and
assessment of the facets and items from the WHOQOL-100 instrument; (c) feedback on
additional facets and items that had been previously suggested by Field Centres during
the Delphi exercise described above; and (d) the gathering of ideas from participants for

The WHOQOL-
DISABILITIES module – manual
9
additional areas of quality of life or items that participants felt were not covered during
discussion.
Twelve centres completed focus groups with intellectual disabilities (a total N of 56
individual participants), 10 centres ran focus groups of mixed physical disabilities
(N=45), 10 centres ran focus groups with adults with Parkinson's Disease (N=49), 5
centres ran focus groups with adults with sensory impairment (N=29), one centre ran a
focus group with adults with Multiple Sclerosis (N=5), and all centres ran at least one
focus group with carers and one group with health professionals working with people
with disabilities (see Den Oudsten et al, 2011, for more details of the focus groups).
Suggestions for additional facets and items were translated into English as the working
language; equivalent items were identified across the suggestions from each centre; and
each centre was given feedback about the proposed items. This process led to the
generation of a set of 20 additional pilot items, that consisted of one general item
(impact of disability) and 19 specific items that included issues of discrimination and
social inclusion, communication, and adjustment to disability. The details of the item
generation will be presented in a further paper, but the translation procedure involved
forward and backward translation using bilingual experts and following normal
WHOQOL methodology.
Pilot study
Participants
The pilot testing was carried out in 15 different WHOQOL centres from around the
world (see Table 1). Each centre was asked to test an opportunistic sample of a
minimum of 50 people with intellectual or physical disabilities, though many centres
collected data from more than the minimum numbers (see Table 1). A total of 1400
respondents were included, that consisted of 491 adults with intellectual disabilities and
909 adults with physical disabilities. The inclusion criteria included a minimum age of
18 years plus a verifiable medical diagnosis from the service in which participants were
recruited. Because Centres had already established links with services in order to recruit

The WHOQOL-
DISABILITIES module – manual
10
participants for the focus groups, the range of physical disabilities was very similar for
both the focus groups and for the pilot study.
Measures
Measures The purpose of the pilot testing was to collect data on the WHOQOL-DIS
items for the purpose of item testing and item reduction. The measures included in the
pilot study therefore were the WHOQOL-BREF (1998b), which is an established
measure of quality of life with proven reliability and validity; the set of 20 items for the
pilot WHOQOL-DIS module generated from the focus group work; and a set of
sociodemographic and health-related questions about co-morbid conditions. The
WHOQOL-DIS module has the same time frame (”the past two weeks”) as the
WHOQOL-BREF, and in the pilot version had the same labelled 5-point response
scales. Examples of the items in the WHOQOL-DIS include “Do you feel that other
people accept you?” and “Do you feel in control of your life?” Some additional
examples were included in the Intellectual Disabilities (ID) version in order to help
respondents understand the WHOQOL items more clearly.
Centre ID PD Age ± SD % Female %
Disabled1
Edinburgh 26 48 61.2
(16.3)
65 3
Barcelona 51 49 49.7
(17.2)
54 38
Paris 17 21 40.3
(16.6)
58 14
Prague 46 60 44.7
(18.3)
51 6
Tromso 7 26 45.1
(11.9)
45 6
Izmir 52 57 32.7
(13.1)
56 23
Vilnius 13 62 48.1
(21.1)
51 1
Sicily 28 72 53.3
(21.3)
55 15
Hamburg 26 35 59.6
(18.2)
79 2
Tilburg 13 37 59.9 58 10

The WHOQOL-
DISABILITIES module – manual
11
(16.2)
Guangzhou 53 249 45.9
(14.2)
64 7
Porto Alegre 57 88 39.8
(17.2)
48 20
Montevideo 45 51 39.9
(16.5)
51 17
Auckland 7 4 34.0
(8.8)
55 0
Budapest 50 50 40.9
(17.2)
48 12
Total 491 909 45.9
(18.3)
56 13
Table 1: General Descriptions of the Pilot Study Sample from each of the 15
Centres. Note: ID=Intellectual Disabilities, PD=Physical Disabilities. 1
Disabled or Not-disabled as subjectively defined
Statistical Analysis
The basic approach of the statistical analyses was to combine the strengths of the “clas-
sical” and the modern (“probabilistic”) psychometric approaches for scale development.
Following the earlier WHOQOL analytic guidelines (The WHOQOL Group, 1998b)
analysis examined item response frequency distributions, missing values analysis, item
and facet score correlations and reliability analyses, in particular, the use of the Multi-
trait Analysis Program (MAP; Hays et al., 1988) to identify items loading on predicted
factors versus non-predicted factors, and exploratory and confirmatory factor analyses.
In addition, an Item Response Theory (IRT) approach that used the unidimensional
Rasch measurement model (Andrich 1988) as implemented in the RUMM program
(Andrich 2001) and in the WINMIRA program (von Davier, 2001) was also used. An
iterative approach was taken in which the larger initial set of items was reduced through
a combination of classical and IRT approaches; thus, the earlier focus group and Delphi
work from which the WHOQOL-DIS items had been derived also provided an initial fa-
cet structure for the items which provided the starting point for the subsequent structural
analyses of the module.
Field Trial
The field trial allowed the participating centres to carry out a variety of different types
of studies that ranged from surveys to validity analyses to evaluation of longitudinal

The WHOQOL-
DISABILITIES module – manual
12
trials. Each centre however included a core dataset that could be further analysed to
produce the final version of the WHOQOL-DIS module.
Participants
The field study analyses were conducted on a sample of N=3772 with data coming from
14 national centres (Auckland, Bangalore, and Melbourne were unfortunately unable to
participate in the Field Trial) (see Table 2). Similarly to the pilot study, centres made
use of existing links with intellectual and physical disability services in order to recruit
opportunistic samples of both. The inclusion criteria included minimum age of 18 years
and a confirmable diagnosis with a physical or intellectual disability. The sample size
recruited in each centre varied between N=19 (Paris) and N=1000 (Guangzhou).
Additional data (N=876) were collected in 6 centres from relatives and staff who were
carers of people with ID, but these data will be presented in a later section so are not
included here. The gender rates varied with particularly higher rates of females in the
Vilnius centre, but overall there was a good distribution with 52.6% of respondents
being male and 47.4% being female. Most centres found it easier to collect more data
from people with Physical Disabilities (69.3%) than from people with Intellectual
Disabilities (30.7%), which, in part, reflected the fact all of the ID participants had to be
sufficiently able to give direct self-report, even when they were included in the proxy
study.
Centre PD ID Total
Male Female Total Male Female Total Male Female Total
Edinburgh 66 61 127 51 53 104 117 114 231
Barcelona 74 75 149 59 40 99 133 115 248
Paris 9 9 18 0 1 1 9 10 19
Prague 171 70 241 25 17 42 196 87 283
Tromso 10 20 30 0 0 0 10 20 30
Izmir 86 71 157 93 57 150 179 128 307
Vilnius 74 168 242 25 35 60 99 203 302
Sicily 159 163 322 13 6 19 172 169 341
Hamburg 31 20 51 45 45 90 76 65 141
Tilburg 61 48 109 0 0 0 61 48 109
Guangzhou 468 339 807 103 90 193 571 429 1000 Porto Alegre 64 98 162 102 55 157 166 153 319
Montevideo 26 22 48 25 52 77 51 74 125
Budapest 66 85 151 78 88 166 144 173 317
Totals 1365 1249 2614 619 539 1158 1984 1788 3772
Table 2: General Descriptions of the Field Trial Sample from each of the 14
Centres. Note: ID=Intellectual Disabilities, PD=Physical Disabilities.

The WHOQOL-
DISABILITIES module – manual
13
Measures
The core measures included in the Field Trial were the WHOQOL-BREF (WHOQOL
Group, 1998b), the 13-item WHOQOL-DIS that was generated from the Pilot Study
analyses, sociodemographic and health status questions, and two further measures of
quality of care and attitudes to disability that will be reported briefly at the end of this
manual. The self-report 12-item WHODAS-II was used as a measure of disability
severity (WHO, 2001). The WHODAS-II is a disability assessment schedule that can
provide a profile of functioning and an overall disability score. In the present study, a
simple additive approach to derivation of a summary disability score was used rather
than the alternative item-weighted scoring algorithm. The WHOQOL-BREF was used
in the Field Trial because its shortness allowed centres to include other measures
according to local interests and local availability of questionnaires.
Summary of results of questionnaire development
The two studies presented here summarise the development of an add-on module for the
WHOQOL group of measures for use with adults with disabilities. The studies
demonstrate the development of the module following the WHOQOL methodology
(The WHOQOL Group 1998a) in which a simultaneous approach to instrument
development is employed (Bullinger et al. 1996). That is, the starting point for the
WHOQOL methodology is an intense qualitative phase of cross-cultural focus groups,
which for the WHOQOL-DIS were run in 12 centres throughout the world. The
summary output from these focus groups was used to identify common themes and
issues either absent from or poorly covered in the WHOQOL-100; these themes and
issues were used to generate a set of pilot items for testing with adults with intellectual
or physical disabilities.
The focus group work together with the Delphi exercise with the WHOQOL experts had
suggested two possible approaches to the amendment of the WHOQOL-100 for use
with adults with disabilities. There were some themes that seemed to best form
additional facets, whereas there were other aspects or items that seemed supplementary

The WHOQOL-
DISABILITIES module – manual
14
to existing facets within the WHOQOL-100 such as facets in the Social Domain.
However, the quantitative analyses suggested that the supplementary items were best
included as part of the add-on module rather than being used to supplement or amend
the scoring of an existing facet. One major outcome of the Pilot Study testing was the
indication that for the respondents with Intellectual Disabilities, the original 5-point
scales for the WHOQOL were responded to as if they were 3-point scales (see Fang et
al., 2011, for details of these analyses). In the Field Trial version of the ID module
therefore, 3-point scales were used in place of 5-point scales. There was also some
simplification of wording of both the WHOQOL-BREF and ID module that was
suggested by the Pilot Study (see Appendices).
In terms of psychometric performance, the items selected for the WHOQOL-DIS
module demonstrate good performance both on classical and modern psychometric
grounds. The approach taken here shows that both classical and modern methods can be
fruitfully combined in scale development. Although modern psychometric methods
such as the Rasch modelling approach taken here were primarily developed for use with
unidimensional ability scales, their careful use with attitude scales provides a powerful
methodology for the development of valid comparable measures across key populations,
especially from different cultures.
In the event, the actual module developed focussed primarily on psychosocial aspects
relevant to people with disabilities. Although there are pertinent issues for example that
arise in relation to the personal environment, general agreement was found from the
focus groups that the existing scales of the WHOQOL-100 already covered the personal
environment sufficiently.
The final version of the WHOQOL-DIS module
The final version of the module contained one general item on impact of disability plus
12 items that can be summed together to give a total score; the comparisons between the
WHOQOL-100 and the WHOQOL-BREF used in the pilot and the field trial studies,
respectively, suggest that the Disabilities Module can be used in addition to either the
WHOQOL-100 or the WHOQOL-BREF, whichever is the most appropriate for a study.

The WHOQOL-
DISABILITIES module – manual
15
The scoring of the module can then consist of a profile set of three facet scores, or, as
supported by the existence of a higher order factor in the confirmatory factor analyses
(CFA; see below), there can be a single total score based on a summation of all 12
specific items in the module.
Description of the instrument
In the following section the scale structure and the scoring procedures of the final ver-
sion of the WHOQOL-DIS module are described.
Scale structure
Physical Disabilities The WHOQOL-DIS module consists of 12 Likert-scaled items
assigned to three facets: the facets have between 3 and 6 items, thus for PD facets the
score of possible values can range from 3 to 15 for the three facet scales and 6-30 for
the six facet scale, provided all items of a facet have been completed (see Table 3). The
scores of these three facets or the values of the 12 single items of the WHOQOL-DIS-
PD module can be combined to produce a general (“overall”) score for quality of life in
physically disabled adults, denoted as the WHOQOL-DIS module “total score”. As em-
pirically supported by analyses of the measurement model via structural equation mo-
delling (see below), quality of life is conceived as a higher-order factor, underlying the
structure of the WHOQOL-DIS module.
Facet Abbr. ∑ items Items of facets Possible range of raw score
(Min, Max)
Discrimination DIS 3 2 + 3 + 4 12 (3, 15)
Autonomy AUT 3 5 + 6 + 7 12 (3, 15)
Inclusion INC 6 8+9+10+11+12+13 24 (6, 30)
Table 3 Items included in the facets of the WHOQOL-DIS PD module
Intellectual Disabilities The WHOQOL-DIS module consists of 12 Likert-scaled items
assigned to three facets: the facets have between 3 and 6 items, thus for ID facets the
score of possible values can range from 3 to 9 for the three facet scales and 6-18 for the
six facet scale, provided all items of a facet have been completed (see Table 4). The sco-

The WHOQOL-
DISABILITIES module – manual
16
res of these three facets or the values of the 12 single items of the WHOQOL-DIS-ID
module can be combined to produce a general (“overall”) score for quality of life adults
with intellectual disabilities, denoted as the WHOQOL-DIS-ID module “total score”.
As empirically supported by analyses of the measurement model via structural equation
modelling (see below), quality of life is conceived as a higher-order factor, underlying
the structure of the WHOQOL-DIS module.
Facet Abbr. ∑ items Items of facets Possible range of raw score
(Min, Max)
Discrimination DIS 3 2 + 3 + 4 6 (3, 9)
Autonomy AUT 3 5 + 6 + 7 6 (3, 9)
Inclusion INC 6 8+9+10+11+12+13 12 (6, 18)
Table 4 Items included in the facets of the WHOQOL-DIS ID module
Scoring
To score the questionnaire correctly, the following scoring list has to be administered
(see Table 5). Scoring the WHOQOL-DIS module involves the following steps:
(a) Basically high scores represent high quality of life, low scores represent low quality
of life;
(b) Sorting items into the appropriate scales. For positively worded items, the above
classification can be applied in which higher values represent a higher quality of life.
For negatively worded items, the score has to be recoded (see below);
(c) Recoding negatively worded items, that is, each item identified with a "*" in the
scoring list has to be recoded so that numeric values assigned are reversed: 1 = 5, 2 = 4,
3 = 3, 4 = 2, 5 = 1. The unidirectional values can subsequently be added to yield the
summed scores according to the scoring list of the WHOQOL-DIS module (Table 5);
(d) Using the scoring list (see below) is also necessary for identifying which items be-
long to a facet. Items to be recoded (see step c) are marked with an "*";
(e) Summing the items belonging to a facet yields the raw facet score (RFS). Its range
lies between the lowest possible (number of items (n) x 1) and highest possible (number
of items (n) x 5) value of the respective facet.

The WHOQOL-
DISABILITIES module – manual
17
(f) If the raw facet score is divided by the number of items in the facet, the resulting
standardised (mean) facet score (SFS) can have any decimal value between 1 and 5 for
PD and 1 and 3 for ID. A value of 1 represents the lowest possible quality of life rating
and a value of 5 for PD and 3 for ID the highest possible quality of life rating for the
individual;
(g) Transferring a raw score to a transformed scale score (TFS) between 0 and 100 ma-
kes it possible to express the scale score in percent between the lowest (0) and highest
(100) possible value. To obtain the transformed facet score (0 - 100) the following
transformation rules can be applied:
PD Facets 1 and 2: TFS = 8.3 x (RFS - 3)
PD Facet 3: TFS = 4.2 x (RFS - 6)
ID Facets 1 and 2: TFS = 16.7 x (RFS - 3)
ID Facet 3: TFS = 8.3 x (RFS - 6).
(i) Producing the total score of the WHOQOL-DIS involves the addition of the facet
scores of a person using all items (instead of the facet items only) of the questionnaire
(again paying attention to the recoding procedure – see steps “b” and “c”). Items may be
added to form a total raw score (according to step “e”, but using all items), a total stan-
dardized (mean) score (according to step “g”, but using all items) or a total transformed
(0 - 100) score (according to step “h”, but using all items);
(i) Accumulating the values of more than one person – e g. a special age group – simply
may be done by summarising the facet and/ or total scores of each individual in that
sample (on the level of raw, standardized/ mean or transformed scores) and dividing the
respective result through the number of participants to produce the mean score of the
respective group.
The above manual scoring approach can be made easier by using a scoring mask that
can be easily produced from the scoring list (see step “d”). In addition, the SPSS syntax
file (enclosed in Appendix II) can be used for the automatic computation of facet and
total scores. To work with them, individual data have to be inputted into the computer
and identified by variable names and labels, which are also suggested for the enclosed
program. When analysing the WHOQOL-DIS module, the facet scores and the total

The WHOQOL-
DISABILITIES module – manual
18
score must be calculated according to the following scoring list (including item num-
bers for the WHOQOL-DIS module; see Table 5 following).
Table 5 Scoring list for the WHOQOL-DIS module
Discrimination (DIS) dis_02* dis_03* dis_04*
(3 items)
Autonomy (AUT) dis_05 dis_06 dis_07
(3 items)
Inclusion (INC) dis_08 dis_09 dis_10
dis_11 dis_12 dis_13
(6 items)
Total Score (DIS) dis_02* dis_03* dis_04*
(12 items) dis_05 dis_06 dis_07
dis_08 dis_09 dis_10
dis_11 dis_12 dis_13
Note: * Reverse-scored items.

The WHOQOL-
DISABILITIES module – manual
19
Psychometric properties
The psychometric properties of the WHOQOL-DIS module are based on the results of
the WHOQOL-DIS Field Trial, which have been published in Power et al. (2010), and
in which further details are available.
Descriptives Descriptive data for the WHOQOL-DIS field study are presented in
Tables 6 and 7. The tables present the data for the PD group and the ID group
separately, because the ID items (apart from the three general items 1, 2, and 27 which
were kept as 5-point scales for later comparison purposes) were now scored on the new
3-point scales (range 1 to 3), whereas all of the PD items were scored on the usual 5-
point scale (range 1 to 5). The PD group contained a wide range of physical disabilities
according to the local interests and contacts of each Centre, but the major disorders
included Parkinson's Disease (16.0%), Multiple Sclerosis (6.6%), Visual Impairment
(5.9%), Hearing Impairment (3.8%), and Stroke (3.0%).
Overall the rate of missing data was below 2% except for Item 21, the Sexual Activity
item, which had similar rates of missing values for both the PD group (19.0%) and for
the ID group (18.3%). The skewness and kurtosis of items were typical for quality of
life items, with the majority of the items showing a positive scoring bias.
Internal reliability
Internal consistency as measured with Cronbach‟s alphas of all subscales was
acceptable. The WHQOL-BREF values for the PD group ranged from 0.621 for the
Social Domain to 0.818 for the Psychological Domain, and the values for the ID group
ranged from 0.606 for the Social Domain to 0.792 for the Personal Environment
Domain. It should be noted that alpha values for the WHOQOL-BREF Social Domain
are based on only three items, which is less than the recommended four items for alpha,
and therefore account for the low values normally obtained with this domain.Tables 6
and 7 also show the overall Cronbach alpha values for the WHOQOL-DIS module: for
the PD group, alpha equals 0.852 and all corrected item-total correlation values are

The WHOQOL-
DISABILITIES module – manual
20
above 0.35 (range 0.373 to 0.613); for the ID group, alpha equals 0.808 though the
corrected item-total correlations for three of the items (28, 29, and 30) are below 0.35.
Nevertheless, these data suggest that the WHOQOL-DIS module works well as a single
domain.
Table 6 Selected psychometric properties for the items and total score of the
WHOQOL-DIS PD module (Field Trial sample; N = 2614)
Domain / Facet N MV % Mean SD (±) Skew p (Skew) Kurtosis p
(Kurtosis) r(corrected)
1 Overall QOL 2593 0.8 3.08 0.952 -0.257 <0.001 -0.225 <0.01
2 General Health 2602 0.5 2.74 1.028 0.063 NS -0.756 <0.001
Physical
3 Pain 2580 1.3 2.84 1.217 -0.062 NS -1.061 <0.001 0.549
4 Medication 2583 1.2 3.16 1.263 -0.295 <0.001 -0.971 <0.001 0.439
10 Energy 2599 0.6 3.06 1.061 -0.060 NS -0.700 <0.001 0.640
15 Mobility 2595 0.7 2.89 1.181 0.043 NS -0.900 <0.001 0.533
16 Sleep 2595 0.7 3.21 1.100 -0.248 <0.001 -0.731 <0.001 0.375
17 ADS 2596 0.7 2.96 1.020 -0.127 <0.005 -0.629 <0.001 0.734
18 Work 2538 2.9 2.79 1.077 0.043 NS -0.782 <0.001 0.674
0.816
Psychological
5 Positive feelings 2594 0.8 3.17 1.008 -0.277 <0.001 -0.259 <0.005 0.681
6 Spirituality 2583 1.2 3.33 1.026 -0.217 <0.001 -0.435 <0.001 0.685
7 Thinking 2597 0.7 3.28 0.958 -0.098 <0.05 -0.367 <0.001 0.474
11 Body image 2599 0.6 3.30 1.106 -0.287 <0.001 -0.533 <0.001 0.538
19 Self esteem 2584 1.1 3.18 0.990 -0.229 <0.001 -0.486 <0.001 0.632
26 Negative feelings 2596 0.7 2.76 0.987 0.290 <0.001 -0.390 <0.001 0.492
0.818
Social
20 Personal relationships 2587 1.0 3.56 0.969 -0.629 <0.001 0.195 <0.05 0.542
21 Sexual activity 2117 19.0 2.93 1.137 -0.215 <0.001 -0.717 <0.001 0.305
22 Social support 2581 1.3 3.54 1.010 -0.521 <0.001 -0.122 NS 0.467
0.621
Environment
8 Safety 2589 1.0 3.27 0.959 -0.322 <0.001 -0.029 NS 0.442
9 Physical environment 2585 1.1 3.34 0.944 -0.389 <0.001 0.131 NS 0.484
12 Finance 2592 0.8 2.74 1.138 0.187 <0.001 -0.711 <0.001 0.553
13 Information 2588 1.0 3.30 1.027 -0.212 <0.001 -0.441 <0.001 0.554
14 Leisure activities 2583 1.2 2.97 1.169 0.021 NS -0.952 <0.001 0.497
23 Home 2587 1.0 3.55 0.983 -0.460 <0.001 -0.154 NS 0.544
24 Health/social care 2592 0.8 3.35 0.931 -0.321 <0.001 -0.124 NS 0.508
25 Transport 2587 1.0 3.28 1.039 -0.411 <0.001 -0.333 <0.001 0.422
0.792
Disabilities Module
27 Impact of disability 2589 1.0 3.37 1.123 -0.312 <0.001 -0.669 <0.001
28 Discrimination 2581 1.3 2.24 1.106 0.540 <0.001 -0.585 <0.001 0.401
29 Advocacy 2585 1.1 2.77 1.293 -0.017 NS -1.247 <0.001 0.447
30 Future prospects 2588 1.0 3.23 1.249 -0.325 <0.001 -0.932 <0.001 0.373
31 Control 2587 1.0 3.43 1.120 -0.456 <0.001 -0.521 <0.001 0.537
32 Choice 2591 0.9 3.80 1.057 -0.788 <0.001 0.040 NS 0.599
33 Autonomy 2587 1.0 3.72 1.123 -0.709 <0.001 -0.263 <0.01 0.579

The WHOQOL-
DISABILITIES module – manual
21
34 Communication ability 2598 0.6 3.72 1.044 -0.635 <0.001 -0.083 NS 0.589
35 Social acceptance 2572 1.6 3.72 0.913 -0.530 <0.001 0.156 NS 0.594
36 Respect 2588 1.0 3.73 0.891 -0.568 <0.001 0.271 <0.01 0.577
37 Social network and interaction 2589 1.0 3.09 1.188 -0.092 <0.05 -0.915 <0.001 0.613
38 Social inclusion and contribution 2561 2.0 2.92 1.183 -0.015 NS -0.922 <0.001 0.556
39 Personal potential 2586 1.1 2.84 1.134 0.064 NS -0.734 <0.001 0.496
0.852
Table 7 Selected psychometric properties for the items and total score of the
WHOQOL-DIS ID module (Field Trial sample; N = 1158)
Domain / Facet N MV % Mean SD (±) Skew p (Skew) Kurtosis p
(Kurtosis) r(corrected)
1 Overall QOL 1153 0.4 3.63 1.298 -0.500 <0.001 -0.878 <0.001
2 General Health 1146 1.0 3.57 1.318 -0.464 <0.001 -0.881 <0.001 Physical 3 Pain 1140 1.6 1.61 0.721 0.754 <0.001 -0.736 <0.001 0.369
4 Medication 1148 0.9 2.06 0.885 -0.121 <0.05 -1.714 <0.001 0.210
10 Energy 1149 0.8 2.43 0.702 -0.799 <0.001 -0.584 <0.001 0.508
15 Mobility 1146 1.0 2.63 0.632 -1.453 <0.001 0.921 <0.001 0.413
16 Sleep 1145 1.1 2.58 0.654 -1.273 <0.001 0.376 <0.05 0.347
17 ADS 1145 1.1 2.61 0.622 -1.336 <0.001 0.680 <0.001 0.611
18 Work 1140 1.6 2.41 0.768 -0.837 <0.001 -0.793 <0.001 0.541
0.705
Psychological 5 Positive feelings 1151 0.6 2.49 0.685 -0.985 <0.001 -0.285 <0.05 0.659
6 Spirituality 1137 1.8 2.46 0.695 -0.897 <0.001 -0.454 <0.005 0.604
7 Thinking 1146 1.0 2.35 0.736 -0.663 <0.001 -0.887 <0.001 0.432
11 Body image 1148 0.9 2.51 0.679 -1.044 <0.001 -0.166 NS 0.530
19 Self esteem 1147 0.9 2.55 0.667 -1.193 <0.001 0.158 NS 0.619
26 Negative feelings 1140 1.6 1.86 0.683 0.179 <0.05 -0.868 <0.001 0.197
0.759
Social 20 Personal relationships 1147 0.9 2.50 0.682 -0.996 <0.001 -0.228 NS 0.492
21 Sexual activity 946 18.3 2.14 0.867 -0.263 <0.005 -1.599 <0.001 0.345
22 Social support 1129 2.5 2.45 0.712 -0.902 <0.001 -0.489 <0.001 0.440
0.606
Environment 8 Safety 1152 0.5 2.48 0.687 -0.967 <0.001 -0.322 <0.05 0.519
9 Physical environment 1140 1.6 2.37 0.720 -0.677 <0.001 -0.788 <0.001 0.455
12 Finance 1149 0.8 2.09 0.815 -0.159 <0.05 -1.477 <0.001 0.441
13 Information 1135 2.0 2.30 0.757 -0.555 <0.001 -1.041 <0.001 0.452
14 Leisure activities 1136 1.9 2.47 0.730 -0.969 <0.001 -0.461 <0.005 0.577
23 Home 1145 1.1 2.59 0.637 -1.255 <0.001 0.438 <0.005 0.570
24 Health/social care 1134 2.1 2.52 0.648 -0.990 <0.001 -0.114 NS 0.549
25 Transport 1142 1.4 2.52 0.656 -1.035 <0.001 -0.097 NS 0.456
0.792
Disabilities Module
27 Impact of disability
1097 5.3 2.60 1.347 0.322 <0.001 -1.053 <0.001 28 Discrimination 1143 1.3 1.84 0.750 0.266 <0.001 -1.184 <0.001 0.196
29 Advocacy 1142 1.4 2.12 0.811 -0.221 <0.005 -1.446 <0.001 0.209
30 Future prospects 1141 1.5 2.05 0.845 -0.091 NS -1.576 <0.001 0.206

The WHOQOL-
DISABILITIES module – manual
22
31 Control 1138 1.7 2.32 0.763 -0.610 <0.001 -1.018 <0.001 0.526
32 Choice 1145 1.1 2.33 0.770 -0.627 <0.001 -1.032 <0.001 0.584
33 Autonomy 1139 1.6 2.07 0.818 -0.112 NS -1.476 <0.001 0.516
34 Communication ability 1145 1.1 2.47 0.704 -0.939 <0.001 -0.404 <0.005 0.662
35 Social acceptance 1144 1.2 2.34 0.706 -0.587 <0.001 -0.814 <0.001 0.525
36 Respect 1140 1.6 2.40 0.672 -0.666 <0.001 -0.619 <0.001 0.534
37 Social network and interaction 1148 0.9 2.38 0.764 -0.753 <0.001 -0.877 <0.001 0.582
38 Social inclusion and contribution 1136 1.9 2.29 0.774 -0.549 <0.001 -1.111 <0.001 0.541
39 Personal potential 1140 1.6 2.19 0.786 -0.341 <0.001 -1.283 <0.001 0.482
0.808
Confirmatory Factor Analyses
In combination with other so-called classical and modern psychometric techniques,
confirmatory factor analyses (CFA) were used both to test the structure of the
WHOQOL-DIS module and as part of the item-reduction procedure. Initial CFA
analyses that used the Maximum Likelihood estimation method showed that the overall
12-item single scale had a better CFI (CFI= 0.786, NFI=0.785, RMSEA=0.166,
X2=5559.7, df=53, p<0.001) than the 3-factor solution (CFI=0.689, NFI=0.687,
RMSEA=0.204, X2=8080.9, df=51, p<0.001). Only when a higher-order factor was
included to the 3-factor solution did the fit improve above that of the 1-factor solution
(CFI=0.870, NFI=0.869, RMSEA=0.132, X2=3396.0, df=51, p<0.001). This pattern of
results was also obtained when the PD and the ID samples were analysed separately.
Because of the non-normality of distribution for some of the items, as with the pilot
study, CFAs were also run using the Maximum Likelihood Robust estimation method.
Fit levels improved with the one-factor solution showing better fit than the three factor
solution, but the best fit being found for the three-factor with the addition of a higher
order factor (CFI=0.900, NFI=0.898, RMSEA=0.110, Satorra-Bentler X2=2365.5,
df=51, p<0.001) (see Figure 1 for a summary of this model). These results suggest that
the WHOQOL-DIS module may be best analysed as one general item (item 27) together
with 12 specific items that can be added together to give a single summative scale, but
which can also be used as three subscales for more detailed analysis.

The WHOQOL-
DISABILITIES module – manual
23
Discrim. .760
Advocacy .714
F1
Future .541
Control .733
Choice .896
.817
Autonomy .874
.847 F4
F2
Communic. .787
Acceptance .856
.946
Respect .844
Interaction .626
F3
. Inclusion .571
Potential .536
Figure 1 Best fitting CFA Model for 12-item Disability Module

The WHOQOL-
DISABILITIES module – manual
24
IRT Analyses Analyses on the basis of item-response-theory were again carried out
using the RUMM2020 (Andrich, 2005) program. The analyses suggested that the 12
specific items for the WHOQOL-DIS formed a good scale, but if Item 27 (the general
Impact of Disability item) was included this showed the poorest item-fit, high residuals,
and a disordered threshold both when analysed for the complete dataset and for ID and
PD separately. Further IRT analyses were therefore carried out for a possible three scale
structure for the 12 specific items, but for both the ID and the PD sample, one of the
factors (consisting of items 28, 29, and 30) performed very poorly with for example PSI
(the IRT equivalent of Cronbach alpha) values of 0.594 and 0.447, respectively.
The RUMM2020 analyses showed no disordered thresholds and good item fits (when
examining fit residuals and X2 values) for the 12-item overall analysis, but numerous
disordered thresholds occurred with the subscale approach. The 12-item scale had an
excellent PSI=0.905, and good overall item fit residual (0.518), and person fit residual
(-0.513), with the total scale X2=1592.2, df=108, p<0.001.
Further analyses indicated a good performance of the items in terms of absence of
Differential Item Functioning (DIF) (using the logistic regression approach for detecting
DIF) when analysed across gender and centre. No item showed gender or centre DIF
with respect to the "cut-off" criterion for practical meaningful DIF of 2 % pseudo R2-
difference, though the centre DIF was simply a comparison of "European" versus "Non-
European" centres because sample sizes were too small for individual centre
comparisons.
Validity
Although all participants had been diagnosed with one or more physical or intellectual
disabilities, each participant was also asked a simple yes-no question on whether or not
they considered themselves to be disabled. In addition to this subjective self-report of
disability, the completion of the 12-item WHODAS-II by the interviewers provided a
relatively more objective assessment of disability. The analyses that are summarised
here were carried out therefore to test whether or not subjective self-report of disability

The WHOQOL-
DISABILITIES module – manual
25
and objective level of disability were correlated with quality of life as measured by the
WHOQOL-BREF and the new WHOQOL-DIS module.
For the ID sample 353 (30.8%) of respondents stated that they did not have a disability.
Those who stated that they did not have a disability reported a significantly higher
overall quality of life on the module (mean=28.3 sd=4.6) than those who stated that they
did have a disability (mean=26.2 sd=5.3) (t, df=779.4, = 2.07, p<0.001; please note that
the decimal point for the df value indicates a corrected df following a significant Levene
Test showing heterogeneity of variances). This pattern was also found across each of the
four domains for the WHOQOL-BREF (range of values of t from 4.3 to 7.9, all
ps<0.001).
A similar set of findings was obtained for the PD sample, although a much smaller
proportion of this sample (N=178, equal to 7.3%) stated that they were not disabled.
The not disabled group scored higher for quality of life on the module (mean=45.6,
sd=7.7) compared to those who stated that they were disabled (mean=40.4, sd=8.1)
(please note, these values appear higher than for the ID sample because these are scored
on the 5-point scales whereas the ID values are scored on the 3-point scales) (t,
df=2602, = 8.3, p<0.001). For the WHOQOL-BREF domains the not disabled group
reported higher values than did the disabled group (range of ts from 5.1 to 8.3, all
ps<0.001).
In relation to the objective WHODAS-II scores, there were significant negative
correlations between total WHODAS scores and the five QOL domains for the ID
sample (range of Pearson r = -0.399 to -0.629) and for the PD sample (range of Pearson
r = -0.247 to -0.616) indicating that as disability increased so quality of life decreased.
One of the interpretations of the subjective report of disability effect on QOL is that
perhaps those who reported themselves to be not disabled simply scored less on
objective disability on the WHODAS. If such an interpretation were the case, then
partialling out the variance accounted for by objective disability, should leave the effect
on subjective disability non-significant. A number of multiple regression equations were
run therefore that included subjective and objective reports of disability as predictors of
domains of the WHOQOL-BREF or of the WHOQOL-DIS score. For example, for the
ID sample there were four significant predictors of WHOQOL-DIS score that included

The WHOQOL-
DISABILITIES module – manual
26
Age (final equation standardised beta = 0.071), Income (beta= -0.148), subjective
disability status (beta = 0.099) and total WHODAS score (beta = -0.489). The
equivalent regression equation for the PD group was very similar, though Age was no
longer a significant predictor. Similar equations occurred for each of the four
WHOQOL-BREF domains for subjective and objective disability status, the only
exception being for Personal Environment in the ID group where subjective status was
no longer a significant predictor once the total WHODAS score was entered. Apart from
this single exception therefore, out of the 10 regression equations that were run, 9 of
them showed that both subjective and objective disability status uniquely accounted for
variance in quality of life independent of each other and of other sociodemographic
factors.

The WHOQOL-
DISABILITIES module – manual
27
Interpretation The values achieved on the individual facet scores of the WHOQOL-DIS PD and ID
modules and on the total score of the WHOQOL-DIS module represent an empirical
assessment of adults with disabilities quality of life from the respondent‟s point of
view. Until the data from representative national standard samples are available for the
WHOQOL-DIS modules, the results of the WHOQOL-DIS Field Trial should be used
as preliminary reference data for adults with physical disabilities and adults with
intellectual disabilities. For the reference values of the WHOQOL-DIS facet scores and
the WHOQOL-DIS total score, all scores can be linearly transformed to a range of 0 to
100 or can be retained as scale scores (see Appendices II and III). The scores are shown
separately for the physically disabled and the intellectually disabled.
How to use the questionnaire
Upon completion, comprehensiveness of questionnaire completion should be checked
and the identification of the form should be noted. Use of the data for research purposes
is not recommended when more than 20% of the items are missing (see WHOQOL
Group, 1998a, 1998b). Data can be computer inputted for easy scoring (in research
projects) or can be scored by hand according to the scoring procedure described above.
The questionnaires are available in the different project languages. Translations into a
number of further languages are in preparation. Proposals for further language versions
should first be sent via the Edinburgh Co-ordinating Centre to the WHOQOL-DIS
Steering Group.
Administration – suggested uses
The WHOQOL-DIS modules can be used in a wide variety of studies including cross-
cultural investigations, population epidemiology, health monitoring, service develop-
ment, and clinical intervention trials in which issues about quality of life are crucial.
The WHOQOL-DIS modules will permit the assessment of the impact of service provi-
sion and of different health and social care structures on quality of life, especially in the
identification of the possible consequences of policies on quality of life for adults with

The WHOQOL-
DISABILITIES module – manual
28
disabilities and a clearer understanding of investment areas to achieve best gains in
quality of life. A related issue is the estimation of the impact of physical and
psychological interventions in a range of physical and psychiatric conditions related to
disability. Cross-sectional studies between different services or treatments and
longitudinal studies of interventions can be assessed with the WHOQOL-DIS.
Moreover, the unique cross-cultural approach to the development of the measure, means
that comparisons can be made between different cultures (Power et al., 1999). The
exacting standards of instrument development used for the WHOQOL-DIS mean that
such comparisons run less risk of cultural bias; the WHOQOL methodology
(WHOQOL Group 1998a) provides a unique approach to instrument development that
provides for cross-cultural validity for the assessment of quality of life across the adult
lifespan.
Additional New Measures Developed Alongside the WHOQOL-DIS In addition to the WHOQOL-DIS, the project team took the opportunity to consider the
issue of proxy measurement of quality of life for people with physical or intellectual
disabilities, but also took the opportunity to develop two further measures, the first
being an Attitudes to Disability Scale (ADS), and the second being a Quality of Care
Scale (QOCS). Each of these will be very briefly summarised here, but further details
are available from the various papers that have been published or that are in preparation
in relation to these measures.
1) Proxy Measurement of Quality of Life
A paper that presents detailed results of the proxy analyses has now been published
(Schmidt et al., 2010), so the reader is referred to this paper for a more detailed account
of the proxy study.

The WHOQOL-
DISABILITIES module – manual
29
Table 8. Summary of proxy respondents from the six centres that took part in the
proxy study.
Altogether 617 participants with intellectual disabilities as well 867 proxies participated
in the study (see Table 8). Concerning living circumstances, in most national centres
there was a mix of residential and community based care settings on the one hand and
(paid or unpaid) home care on the other hand, however to varying degrees. Participants
were institutionalized in hospitals only in one centre (Izmir). Concerning the
educational level most participants did not reach higher level and primary school. It is
interesting to note that 30% of the sample did not subjectively consider themselves
being disabled.
In relation to the correlations between individual items of the WHOQOL-BREF and the
disabilities supplementary module with both types of proxy samples, there were high to
moderate significant positive associations between the person and the proxy assessment
in most of the items as demonstrated both by the Pearson correlation coefficient (r) and
as well as the Intraclass Correlation coefficient (ICC). There was no association in
respect to the item on satisfaction with safety in the first proxy sample and no difference
with satisfaction with transport in the second proxy sample.
The differences in means were tested between both assessments and showed significant
differences in all of the items in proxy assessment 1 as well as proxy assessment 2.
Centre
Relatives Staff Total
Edinburgh 23 131 154
Barcelona 69 84 153
Prague 37 47 84
Izmir 32 118 150
Hamburg 30 60 90
Porto Alegre 85 151 236
Totals 276 591 867
Proxy Cases

The WHOQOL-
DISABILITIES module – manual
30
Concerning the scale differences (see Table 9), scale differences were significant
between the patient and the proxy assessment in the proxy sample 1 as well as in the
proxy sample 2, however, not in the Physical scale in both proxy samples. For all other
scales, the proxies significantly underestimated quality of life for the ID person, but
were in agreement with each other in terms of mean values (see Table 9).
We tested whether there were differences between national centres in terms of the
directional differences between persons and proxies. ANOVA results showed some
selective significant cross-centre differences in respect to disagreement between person
and proxy. Post-hoc tests showed that across all centres it was the Porto Allegre centre
which showed some particular differences. In terms of the Social and the Personal
Environment domains, there were differences between the Porto Allegre centre and all
other centres. In general, the discrepancy between participant and proxy response was
higher in the Porto Allegre sample. The Edinburgh sample showed differences with
three other centres in the Personal Environment scale, indicating a higher agreement in
the Edinburgh centre than in the other three samples. The tables for these comparisons
are presented in Schmidt et al. (2010).

The WHOQOL-DISABILITIES module – manual
31
Table 9: Correlations and mean differences in scales across Person –Proxy 1, Person–Proxy 2, and Proxy – Proxy pairs
Domain Person - Proxy 1 Person - Proxy 2 Proxy 1 – Proxy 2
Descriptives Correlations Directional Difference
Descriptives Correlations Directional Difference
Descriptives Correlations Directional Difference
Com-plete Pairs
Person Mean (SD)
Proxy 1 Mean (SD)
Pearson ICCa Mean (SD)b Effect Size
Com-plete Pairs
Person Mean (SD)
Proxy 2 Mean (SD)
Pearson ICCa Mean (SD)b
Effect Size
Com-plete Pairs
Proxy 1 Mean (SD)
Proxy 2 Mean (SD)
Pearson ICCa Mean (SD)b
Effect Size
Physical
601 3.82 (.60)
3.83 (.67)
.21*** .21*** -.01 (.81)
-.02 250 3.93 (.54)
3.92 (.68)
.01 .01 .01
(.86) 0.02 249
3.88 (.65)
3.92 (.68)
.43*** .43*** -.04 (.71)
-.06
Psychological 599 3.94 (.69)
3.63 (.69)
.25*** .19*** .31
(.85)*** .45 248
4.07 (.57)
3.79 (.68)
.17** .12* .28
(.81)*** .45 249
3.72 (.62)
3.78 (.68)
.48*** .48*** -.06 (.67)
-.09
Social 602 4.03
(1.02) 3.49 (.95)
.25*** .16*** .54
(1.20)*** .55 250
4.20 (.93)
3.46 (.91)
.18** .01 .75
(1.18)*** .80 245
3.43 (.88)
3.44 (.91)
.46*** .46*** -.01 .93
-.01
Personal Environment
610 3.88 (.67)
3.76 (.68)
.29*** .28*** .12
(.80)*** .18 255
4.00 (.56)
3.89 (.63)
.18** .17** .11
(.77)* .18 254
3.84 (.66)
3.89 (.63)
.42*** .42*** -.04 (.69)
-.08
Disabilities Module
602 3.70 (.73)
3.17 (.57)
.30*** .12** .53
(.78)*** .81 250
3.85 (.67)
3.23 (.53)
.20** -.06 .63
(.76)*** 1.03 250
3.16 (.52)
3.21 (.52)
.48*** .47*** -.06 (.53)
-.10
a ICC one-way random b tested for significance with two-sided paired t-test (* significant at the 5% level, ** significant at the 1% level, *** significant at the 0,1% level) c d = (x1 – x2)/(√(s1 + s2)/2)

The WHOQOL-
DISABILITIES module – manual
32
2) Attitudes to Disability Scale
One of the additional measures that was developed alongside the WHOQOL-DIS was an
Attitudes to Disability Scale (ADS). The development of the scale is described in detail in
Power et al. (2010), so will not be described here. Basically, the development mirrored the
approach taken to the development of the WHOQOL-DIS and included initial focus group
work, pilot testing and revision of an initial scale, and then the field trial testing of the final
16-item measure. The 16 items form four subscales that cover issues of inclusion,
discrimination, gains, and prospects. Similar to the WHOQOL-DIS, the final versions of the
scale include 5-point scales for general (any respondent) and personal (for a person with a
disability) formats, but also include 3-point scales for people with intellectual disabilities.
The full set of scales have been included in the appendices (see Appendix IV).
The field study analyses were conducted on a sample of N=3772 with data coming from 14
national centres (Auckland, Bangalore, and Melbourne were unfortunately unable to
participate in the Field Trial). The sample size recruited in each centre varied between N=19
(Paris) and N=1000 (Guangzhou) (see Table 4). The gender rates varied with particularly
higher rates of females in the Vilnius centre, but overall there was a good distribution with
52.6% of respondents being male and 47.4% being female. Table 4 also shows that most
centres found it easier to collect more data from people with Physical Disabilities (69.3%)
than from people with Intellectual Disabilities (30.7%), which, in part, reflected the fact all of
the ID participants had to be sufficiently able to give direct self-report, because we did not
use any proxy information in the main Field Trial study.
Item N MV % Mean SD (±) Skew p (Skew) Kurtosis
p
(Kurtosis)
r
(corrected)
1 Relationships 2493 4.6 3.00 1.205 -0.105 <0.05 -1.097 <0.001 0.553
2 Inclusion 2491 4.7 3.23 1.162 -0.394 <0.001 -0.894 <0.001 0.534
3 Ridicule 2480 5.1 2.75 1.212 0.077 NS -1.101 <0.001 0.405
4 Exploitation 2483 5.0 2.88 1.224 -0.028 NS -1.136 <0.001 0.458
5 Burden-society 2490 4.7 2.80 1.218 0.045 NS -1.118 <0.001 0.529
6 Burden-family 2484 5.0 2.95 1.234 -0.133 <0.01 -1.117 <0.001 0.507
7 Emotional strength 2486 4.9 3.24 1.090 -0.372 <0.001 -0.629 <0.001 0.179
8 Maturity 2491 4.7 3.23 1.043 -0.291 <0.001 -0.515 <0.001 0.197
9 Achievement 2491 4.7 2.84 1.046 -0.005 NS -0.598 <0.001 0.046
10 Determination 2485 4.9 3.25 1.023 -0.314 <0.001 -0.379 <0.001 0.119
11 Irritation 2483 5.0 2.96 1.106 -0.083 <0.05 -0.956 <0.001 0.480
12 Ignorance 2486 4.9 2.62 1.066 0.337 <0.001 -0.706 <0.001 0.480
13 Sexuality 2450 6.3 2.34 1.008 0.462 <0.001 -0.278 <0.005 0.426
14 Underestimation 2480 5.1 2.60 1.063 0.287 <0.001 -0.780 <0.001 0.476
15 Optimism 2481 5.1 2.39 1.097 0.480 <0.001 -0.580 <0.001 0.412
16 Future prospects 2480 5.1 2.65 1.146 0.209 <0.001 -0.912 <0.001 0.440

The WHOQOL-
DISABILITIES module – manual
33
0.795
TABLE 10 : ADS Descriptives and Reliability Analysis (PD - Max N=2614)
The CFA analyses for the overall combined data using a Maximum Likelihood estimation
model showed that the 1-factor solution did not fit the data well (CFI=0.618, NFI=0.617,
X2=11,740.9, df=104, p<.001, RMSEA=0.175). The 3-factor (CFI=0.799, NFI=0.796,
X2=6239.1, df=104, p<.001, RMSEA=0.127) and 4-factor (CFI=0.741, NFI=0.738,
X2=8012.7, df=104, p<.001, RMSEA=0.144) solutions both show significant improved fit in
comparison to the 1-factor solution, but the addition of a higher-order factor in the CFA
model on which all lower order factors load improves both the 3-factor model (CFI=0.868,
NFI=0.866, X2=4115.8, df=101, p<.001, RMSEA=0.104) and the 4-factor model
(CFI=0.882, NFI=0.879, X2=3709.6, df=99, RMSEA=0.099). However, the improvement in
fit for the 4-factor correlated model in comparison to the 3-factor correlated model is highly
significant (X2=406.2, df=2, p<.001) and consistent across other levels of analysis and
therefore the 4-factor correlated model provides the preferred structure for the ADS. A
further comparison of note however was that the personal version of the ADS showed better
fit for both the PD respondents and the ID respondents than did the general version. EQS
offers a Maximum Likelihood Robust estimation model which corrects for non-normal data
distribution. Using this estimation model improved the fit of the 4-factor correlated model
(CFI=0.901, NFI=0.898, RMSEA=0.084, Satorra-Bentler X2=2696.2, df=100, p<.001).
Allowing Item 13 (“Sex should not be discussed with people with disabilities”) to cross-load
onto Factor 2 further improved the fit of this model (CFI=0.907, NFI=0.904, RMSEA=0.082,
Satorra-Bentler X2=2535.9, df=99, p<0.001) and additional cross-loadings further improved
the fit of the model.
Item N MV % Mean SD (±) Skew p (Skew) Kurtosis
p
(Kurtosis)
r
(corrected)
1 Relationships 1134 2.1 2.07 0.885 -0.145 <0.05 -1.710 <0.005 0.458
2 Inclusion 1129 2.5 2.09 0.873 -0.174 <0.01 -1.667 <0.005 0.472
3 Ridicule 1126 2.8 2.01 0.882 -0.024 NS -1.716 <0.005 0.437
4 Exploitation 1119 3.4 1.98 0.871 0.036 NS -1.683 <0.005 0.489
5 Burden-society 1101 4.9 1.82 0.859 0.358 <0.005 -1.553 <0.005 0.506
6 Burden-family 1098 5.2 1.81 0.865 0.377 <0.005 -1.561 <0.005 0.421
7 Emotional strength 1124 2.9 2.19 0.825 -0.362 <0.005 -1.439 <0.005 0.121
8 Maturity 1123 3.0 2.13 0.824 -0.247 <0.005 -1.485 <0.005 0.156
9 Achievement 1119 3.4 2.06 0.829 -0.117 NS -1.534 <0.005 0.058
10 Determination 1118 3.5 2.23 0.809 -0.442 <0.005 -1.339 <0.005 0.048

The WHOQOL-
DISABILITIES module – manual
34
11 Irritation 1125 2.8 2.11 0.823 -0.210 <0.005 -1.495 <0.005 0.433
12 Ignorance 1122 3.1 1.90 0.849 0.197 <0.005 -1.584 <0.005 0.445
13 Sexuality 1106 4.5 1.78 0.794 0.420 <0.005 -1.294 <0.005 0.363
14 Underestimation 1113 3.9 1.86 0.809 0.266 <0.001 -1.426 <0.005 0.423
15 Optimism 1114 3.8 1.75 0.800 0.485 <0.005 -1.276 <0.005 0.398
16 Future prospects 1120 3.3 1.82 0.819 0.336 <0.005 -1.432 <0.005 0.488
0.764
Table 11: ADS Descriptives and Reliability Analysis (ID - Max N=1158)
3) The Quality of Care Scale (QOCS)
A second scale that was developed alongside the WHOQOL-DIS and the ADS was the
Quality of Care Scale (QOCS). The scale followed the same procedures for the development
of the WHOQOL-DIS and the ADS. A paper that describes its development in detail has now
been published (Lucas-Carrasco et al., 2011).
Table 12. Descriptive statistics and reliability analysis of QOCS Field Trial Physical
Disability sample data.
Facet N MV % Mean SD (±) Skew p (Skew) Kurtosis p (Kurtosis) r(corrected)
1 Competence of care providers 2558 2,1 3,83 0,984 -0,716 < 0.001 0,287 < 0.01 0,529
2 Knowledge of care providers 2558 2,1 3,80 1,029 -0,691 < 0.001 0,008 NS 0,495
3 Person centred care 2558 2,1 3,73 0,996 -0,583 < 0.001 0,046 NS 0,581
4 Autonomy 2558 2,1 3,47 1,070 -0,295 < 0.001 -0,275 < 0.01 0,513
5 Availability of services 2558 2,1 3,37 1,180 -0,191 < 0.001 -0,874 < 0.001 0,401
6 Access to services 2558 2,1 3,55 1,182 -0,397 < 0.001 -0,798 < 0.001 0,346
7 Rights to care 2558 2,1 3,46 1,238 -0,293 < 0.001 -0,888 < 0.001 0,423
8 Cost of care 2558 2,1 3,41 1,210 -0,181 < 0.001 -0,826 < 0.001 0,398
9
Support for ADL (activities of daily
living) 2558 2,1 3,73 1,284 -0,903 < 0.001 -0,262 < 0.01 0,442
10 Support for leisure activities 2558 2,1 3,21 1,308 -0,256 < 0.001 -1,077 < 0.001 0,515
11 Support for social activities 2558 2,1 3,19 1,333 -0,178 < 0.001 -1,154 < 0.001 0,548
12 Standards of care 2558 2,1 3,64 1,127 -0,684 < 0.001 -0,230 < 0.01 0,608
13 Safety of care 2558 2,1 3,71 1,096 -0,655 < 0.001 -0,164 < 0.05 0,599
14 Information about disability 2558 2,1 3,43 1,219 -0,330 < 0.001 -0,928 < 0.001 0,578
15 Information about services 2558 2,1 3,15 1,234 -0,162 < 0.001 -0,978 < 0.001 0,575
16 Information about benefits 2558 2,1 3,04 1,299 -0,047 NS -1,090 < 0.001 0,461
17 Clarity of information 2558 2,1 3,41 1,154 -0,231 < 0.001 -0,763 < 0.001 0,546
0,873
MV Tilburg PD = 56 / 109 cases (replacement by centre median not appropriate)

The WHOQOL-
DISABILITIES module – manual
35
Domain / Facet N MV % Mean SD (±) Skew p (Skew) Kurtosis p (Kurtosis) r(corrected)
1 Competence of care providers 1158 0 2,66 0,574 -1,428 < 0.001 1,080 < 0.001 0,478
2 Knowledge of care providers 1158 0 2,58 0,651 -1,253 < 0.001 0,377 < 0.01 0,428
3 Person centred care 1158 0 2,58 0,617 -1,152 < 0.001 0,286 < 0.05 0,504
4 Autonomy 1158 0 2,31 0,718 -0,517 < 0.001 -0,910 < 0.001 0,363
5 Availability of services 1157 0,1 2,10 0,759 -0,163 < 0.05 -1,247 < 0.001 0,191
6 Access to services 1157 0,1 2,27 0,754 -0,490 < 0.001 -1,099 < 0.001 0,156
7 Rights to care 1157 0,1 2,27 0,747 -0,474 < 0.001 -1,081 < 0.001 0,240
8 Cost of care 1157 0,1 2,30 0,739 -0,544 < 0.001 -1,001 < 0.001 0,287
9
Support for ADL (activities of daily
living) 1158 0 2,58 0,712 -1,301 < 0.001 0,367 < 0.01 0,299
10 Support for leisure activities 1158 0 2,39 0,771 -0,765 < 0.001 -0,774 < 0.001 0,458
11 Support for social activities 1158 0 2,28 0,823 -0,525 < 0.001 -1,214 < 0.001 0,454
12 Standards of care 1158 0 2,58 0,648 -1,197 < 0.001 0,480 < 0.001 0,472
13 Safety of care 1157 0,1 2,57 0,650 -1,137 < 0.001 0,350 < 0.01 0,469
14 Information about disability 1158 0 2,11 0,823 -0,198 < 0.01 -1,477 < 0.001 0,500
15 Information about services 1158 0 2,09 0,811 -0,151 < 0.05 -1,444 < 0.001 0,437
16 Information about benefits 1158 0 2,06 0,843 -0,116 NS -1,585 < 0.001 0,347
17 Clarity of information 1158 0 2,31 0,761 -0,581 < 0.001 -1,038 < 0.001 0,508
0,795
Table 13. Descriptive statistics and reliability analysis of Field Trial Intellectual
Disability sample data.
Data from the field trial version of the QOCS have been summarised in Tables 12 and 13.
The final version of the measure has four subscales and the internal consistencies measured
with Cronbach‟s alphas for the PD group were acceptable, ranging from 0.59 for the Meeting
Needs Domain to 0.84 for the Staff Quality Domain, and the values ranged from 0.63 for the
Accessibility of Care Domain, to 0.75 for the Information Domain for the ID group. Overall
alpha values for both PD (0.87) and ID (0.79) groups were acceptable as well. Cronbach
alpha values calculated when each of the items deleted revealed that none of the items were
problematic for both of the PD and ID groups. All corrected item-total correlation values
were above 0.35 for the PD group (range 0.46 to 0.76), and the ID group (range 0.35 to 0.62).
The items 4, 5 and 8 were borderline for item-total correlation values (=0.35) for the ID
group. If item deleted alpha values for each of the domain were also obtained to demonstrate
the contribution of each of the individual item to the variance, which was very satisfactory for
the entire items except for item 4 (Autonomy item) for both PD and ID persons. Nevertheless
MAP analyses revealed 100% item success based on the item scale correlations indicated that
item 4 should not be excluded.
The final 17-item version of the QOCS has been included in the appendix (see Appendices
….).

The WHOQOL-
DISABILITIES module – manual
36
References
Andrich D (2005). RUMM2020: Rasch unidimensional measurement models. Perth: RUMM Laboratory.
Bullinger M, Power MJ, Aaronson NK, Cella DF, Anderson RT (1996). Creating and evaluating cross-cultural
instruments. In B Spilker B (ed), Quality of life and pharmacoeconomics in clinical trials (2nd ed).
Hagerstown, MD: Lippincott-Raven.
Den Oudsten BL, Lucas-Carrasco R, Green AM, The WHOQOL-DIS Group (2011). Perceptions of persons
with Parkinson's disease, family and professionals on quality of life: An international focus group study.
Disability and Rehabilitation, May 6.
Fang J, Fleck MP, Green A, McVilly K, Hao Y, Tan W, Fu R, Power M. (2011). The response scale for the
intellectual disability module of the WHOQOL: 5-point or 3-point? J Intellect Disabil Res. Jun;55(6):537-
49. doi: 10.1111/j.1365-2788.2011.01401.x. Epub 2011 Mar 25
Hays RD, Hayashi T, Carson S, Ware JE (1988). User’s Guide for the Multitrait Analysis Program (MAP).
Santa Monica, CA: The RAND Corporation, N-2786-RC.
Lucas-Carrasco, R., Eser, E., Hao, Y. McPherson, K. Green, A.M. Kullman, L., The WHOQOL-DIS Group
(2011). The Quality of Care and Support (QOCS) for people with disability scale: Development and
Psychometric properties. Research in Developmental Disabilities, 32, 1212-1225.
Power MJ, Bullinger M, Harper A, The WHOQOL Group (1999). The World Health Organization WHOQOL-
100: tests of the universality of quality of life in fifteen different cultural groups world-wide. Health
Psychology, 18: 495 - 505.
Schmidt S, Power M, Green A, Lucas-Carrasco R, Eser E, Dragomirecka E, Fleck M. (2010). Self and proxy
rating of quality of life in adults with intellectual disabilities: Results from the DISQOL study. Res Dev
Disabil. 2010 Sep-Oct;31(5):1015-26. Epub 2010 May 15.
Von Davier M (2001). WINMIRA User Manual. Kiel: IPN (Institute for Science Education).
The WHOQOL Group (1998a). Development of The World Health Organization WHOQOL-BREF quality of
life assessment. Psychological Medicine, 28: 551 - 558.
The WHOQOL Group (1998b). The World Health Organization quality of life assessment (WHOQOL): de-
velopment and general psychometric properties. Social Science & Medicine, 46: 1569 - 1585.
The WHOQOL-OLD Group (2005). Development of the WHOQOL-OLD module. Quality of Life Research,
14, 2197-2214.

The WHOQOL-
DISABILITIES module – manual
Appendix
I Final sets of items for WHOQOL-DIS Modules
II SPSS syntax file
III Reference data
IV ADS
V QOCS
VI List of Centres

The WHOQOL-
DISABILITIES module – manual
APPENDIX 1: WHOQOL-BREF-ID & DISABILITIES MODULE (3-POINT SCALES)
INSTRUCTIONS
This assessment asks how you feel about your quality of life, health or other areas of your life. It is just about you
– you and your life.
Please keep in mind what is important to you; what makes you happy; your hopes and dreams, and your worries
or concerns.
Please answer all the questions. If you are unsure about which answer to give to a question - if it is hard to pick an
answer - please choose the one that seems nearest or most appropriate. This can often be the first thing that comes into
your mind. Some questions include an example to help you think about your answer.
There are no right or wrong answers – just answer what is true for you. Please think about your life in the last two
weeks.
For example, thinking about the last two weeks, a question might ask:
EXAMPLE
Not at all Moderately Totally
Do you get the kind of support that you need from others? For example, do you get the kind of help you need from other people?
1
2
3
In this item, the question has an example. You should circle the number that best fits your opinion about the kind of
support (or help) you got from others over the last two weeks. So you would circle the number 2 if the support (or help)
you got met your needs moderately, as follows:
EXAMPLE
Not at all Moderately Totally
Do you get the kind of support that you need from others? For example, do you get the kind of help you need from other people?
1
3
Alternatively, you would circle number 1 if the support you got over the last two weeks did not meet your needs at all.
Please read each question, think about your feelings, and circle the number on the scale for each question that gives the
best answer for you.
You may find it helpful to look at the „smiley faces‟ that add a visual guide (a picture) to the number scales. These are
available printed on separate cards also.
If you would like some help to write your answers on the form, it is OK to ask someone to do this for you.
Please think about your life in the last two weeks:
The first two questions ask about your life and health overall.
2

The WHOQOL-
DISABILITIES module – manual
Not at all A Little Moderately Mostly Totally
1G
Are you satisfied with your life?
1
2
3
4
5
2G
Are you satisfied with your health?
1
2
3
4
5
The following questions ask about how you have felt about certain things, how much you have been able to do certain
things, or how satisfied you have been about various aspects of your life over the last two weeks.
Not at all Moderately Totally
3
Does (physical) pain stop you from doing what you need to do?
1
2
3
4
Do you need any medical treatment to help you in your daily life? For example, medicines.
1
2
3
Not at all Moderately Totally
5
Do you enjoy your life?
1
2
3
6
Do you feel your life has meaning? For example, do you feel your life is important and has a purpose?
1
2
3
7
Are you able to think clearly? For example, are you able to pay attention, and think carefully about things?
1
2
3
8
Do you feel safe in your daily life? For example, at home and in the places you go to during the day.
1
2
3
9
Do you feel the local area you live in is healthy? For example, thinking about the noise, the traffic, the pollution, the weather.
1
2
3
10
Do you have enough energy for everyday life? For example, are you able to do things through the day without feeling tired?
1
2
3
11
Are you able to accept the way your body looks?
1
2
3
12
Do you have enough money for the things you need?
1
2
3

The WHOQOL-
DISABILITIES module – manual
Not at all Moderately Totally
13
Are you able to get the information that you need in your day-to-day life? For example, is it easy to find out about things you need to know in your daily life?
1
2
3
14
Do you get the chance to do leisure activities?
For example, do you get the chance to do things you enjoy in your spare time?
1
2
3
15
Are you able to get around OK in the house and outside?
1
2
3
16
Are you satisfied with your sleep?
1
2
3
17
Are you satisfied with your ability to do your daily activities? For example, looking after yourself, washing, dressing, eating
1
2
3
18
Are you satisfied with your ability to work? For example, to do your job, or your daily activities.
1
2
3
19
Are you satisfied with yourself as a person? For example, with the kind of person you are, in what you do, how you spend your time, your friendships, your achievements.
1
2
3
20
Are you satisfied with your personal relationships? For example, how you get along with the people in your life, your friends, your family, the people you live with.
1
2
3
21
Are you satisfied with your sex life, or your relationship with your partner? For example, your husband/wife, boyfriend/girlfriend.
1
2
3
22
Are you satisfied with the support you get from your friends?
1
2
3
23
Are you satisfied with what your home is like? For example, thinking about your home and the place you live in.
1
2
3
24
Are you satisfied with your access to health services? For example, is it easy to see the doctors, nurses or other staff who look after you when you are unwell?
1
2
3
25
Are you satisfied with the transport you can use? For example, how you get to the places you go to (e.g. by bus, car, taxi etc.).
1
2
3
Not at all Moderately Totally
26
Do you feel very unhappy, sad, worried or depressed?
1
2
3

The WHOQOL-
DISABILITIES module – manual
DISABILITIES MODULE
The next question asks about your disability overall.
Not at all A Little Moderately Mostly Totally
27G Does your disability have a negative (bad) effect on your day-to-day life?
1
2
3
4
5
The following questions ask about how you have felt about certain things, how much certain things have applied to you,
and how satisfied you have been about various parts of your life over the last two weeks
Not at all Moderately Totally
28
Do you feel that some people treat you unfairly?
1
2
3
29
Do you need someone to stand up for you when you have problems?
1
2
3
30
Do you worry about what might happen to you in the future? For example, thinking about not being able to look after yourself, or being a burden to others in the future.
1
2
3
Not at all Moderately Totally
31
Do you feel in control of your life? For example, do you feel in charge of your life?
1
2
3
32
Do you make your own choices about your day-to-day life? For example, where to go, what to do, what to eat.
1
2
3
33
Do you get to make the big decisions in your life? For example, like deciding where to live, or who to live with, how to spend your money.
1
2
3
34
Are you satisfied with your ability to communicate with other people? For example, how you say things or get your point across, the way you understand others, by words or signs.
1
2
3
35
Do you feel that other people accept you?
1
2
3
36
Do you feel that other people respect you? For example, do you feel that others value you as a person, and listen to what you have to say?
1
2
3

The WHOQOL-
DISABILITIES module – manual
Not at all Moderately Totally
37
Are you satisfied with your chances to be involved in social activities?
For example, meeting friends, going out for a meal, going to a party etc.
1
2
3
38
Are you satisfied with your chances to be involved in local activities? For example, being part of what is happening in your local area or neighbourhood.
1
2
3
39
Do you feel that your dreams, hopes and wishes will happen? For example, do you feel you will get the chance to do the things you want, or get the things you wish for, in your life?
1
2
3
Do you have any comments about the questionnaire?
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
THANK YOU FOR YOUR HELP

The WHOQOL-
DISABILITIES module – manual
WHOQOL-BREF & DISABILITIES MODULE (5 POINT SCALES) INSTRUCTIONS
This assessment asks how you feel about your quality of life, health or other areas of your life. It is just about you
– you and your life.
Please keep in mind what is important to you; what makes you happy; your hopes and dreams, and your worries
or concerns.
Please answer all the questions. If you are unsure about which answer to give to a question - if it is hard to pick an
answer - please choose the one that seems nearest or most appropriate. This can often be the first thing that comes into
your mind. Some questions include an example to help you think about your answer.
There are no right or wrong answers – just answer what is true for you. Please think about your life in the last two
weeks.
For example, thinking about the last two weeks, a question might ask:
EXAMPLE
Not at all A Little Moderately Mostly Totally
Do you get the kind of support from others that you need? For example, do you get the kind of help you need from other people?
1
2
3
4
5
In this item, the question has an example. You should circle the number that best fits your opinion about the kind of
support (or help) you got from others over the last two weeks. So you would circle the number 2 if the support (or help)
you got met your needs a little, as follows:
EXAMPLE
Not at all
A Little Moderately Mostly Totally
Do you get the kind of support from others that you need? For example, do you get the kind of help you need from other people?
1
3
4
5
Alternatively, you would circle number 1 if the support you got over the last two weeks did not meet your needs at all.
Please read each question, think about your feelings, and circle the number on the scale for each question that gives the
best answer for you.
You may find it helpful to look at the „smiley faces‟ that add a visual guide (a picture) to the number scales for some
items. These are available printed on separate cards also.
If you would like some help to write your answers on the form, it is OK to ask someone to do this for you.
Please think about your life in the last two weeks:
The first two questions ask about your life and health overall.
2

The WHOQOL-
DISABILITIES module – manual
Very poor Poor Neither poor nor
good Good Very good
1G
How would you rate your quality of life?
1
2
3
4
5
Very dissatisfied
Dissatisfied
Neither satisfied
nor dissatisfied
Satisfied Very
satisfied
2G
How satisfied are you with your health?
1
2
3
4
5
The following questions ask about how much you have experienced certain things in the last two weeks.
Not at all A little A
moderate amount
Very much An extreme
amount
3
To what extent do you feel that (physical) pain prevents you from doing what you need to do?
1
2
3
4
5
4
How much do you need any medical treatment to function in your daily life?
1
2
3
4
5
5
How much do you enjoy life?
1
2
3
4
5
6
To what extent do you feel your life to be meaningful?
1
2
3
4
5
Not at all A little A
moderate amount
Very much Extremely
7
How well are you able to concentrate?
1
2
3
4
5
8
How safe do you feel in your daily life?
1
2
3
4
5
9
How healthy is your physical environment?
1
2
3
4
5
The following questions ask about how completely you experienced or were able to do certain things in the last two weeks.
Not at all
A Little
Moderately
Mostly
Completely
10
Do you have enough energy for everyday life?
1
2
3
4
5
11
Are you able to accept your bodily appearance?
1
2
3
4
5
12
Have you enough money to meet your needs?
1
2
3
4
5

The WHOQOL-
DISABILITIES module – manual
Not at all
A Little
Moderately
Mostly
Completely
13 How available to you is the information that you need in your day-to-day life?
1
2
3
4
5
14
To what extent do you have the opportunity for leisure activities?
1
2
3
4
5
Very poor Poor Neither poor nor
good Good Very good
15
How well are you able to get around?
1
2
3
4
5
The following questions ask you to say how good or satisfied you have felt about various aspects of your life over the
last two weeks.
Very dissatisfied
Dissatisfied
Neither satisfied
nor dissatisfied
Satisfied Very
satisfied
16
How satisfied are you with your sleep?
1
2
3
4
5
17
How satisfied are you with your ability to perform your daily living activities?
1
2
3
4
5
18
How satisfied are you with your capacity for work?
1
2
3
4
5
19
How satisfied are you with yourself?
1
2
3
4
5
20
How satisfied are you with your personal relationships?
1
2
3
4
5
21
How satisfied are you with your sex life?
1
2
3
4
5
22
How satisfied are you with the support you get from your friends?
1
2
3
4
5
23
How satisfied are you with the conditions of your living place?
1
2
3
4
5
24
How satisfied are you with your access to health services?
1
2
3
4
5
25
How satisfied are you with your transport?
1
2
3
4
5
The following question refers to how often you have felt or experienced certain things in the last two weeks.
Never Seldom Quite often Very often Always
26
How often do you have negative feelings such as blue mood, despair, anxiety, depression?
1
2
3
4
5

The WHOQOL-
DISABILITIES module – manual
DISABILITIES MODULE
The next question asks about your disability overall.
Not at all A Little Moderately Mostly Totally
27G Does your disability have a negative (bad) effect on your day-to-day life?
1
2
3
4
5
The following questions ask about how you have felt about certain things, how much certain things have applied to you,
and how satisfied you have been about various parts of your life over the last two weeks
Not at all A Little Moderately Mostly Totally
28 Do you feel that some people treat you unfairly?
1
2
3
4
5
29
Do you need someone to stand up for you when you have problems?
1
2
3
4
5
30
Do you worry about what might happen to you in the future? For example, thinking about not being able to look after yourself, or being a burden to others in the future.
1
2
3
4
5
Not at all A Little Moderately Mostly Totally
31 Do you feel in control of your life? For example, do you feel in charge of your life?
1
2
3
4
5
32
Do you make your own choices about your day-to-day life? For example, where to go, what to do, what to eat.
1
2
3
4
5
33
Do you get to make the big decisions in your life? For example, like deciding where to live, or who to live with, how to spend your money.
1
2
3
4
5
34
Are you satisfied with your ability to communicate with other people? For example, how you say things or get your point across, the way you understand others, by words or signs.
1
2
3
4
5
35
Do you feel that other people accept you?
1
2
3
4
5
36
Do you feel that other people respect you?
1
2
3
4
5

The WHOQOL-
DISABILITIES module – manual
For example, do you feel that others value you as a person and listen to what you have to say?
Not at all A Little Moderately Mostly Totally
37 Are you satisfied with your chances to be involved in social activities?
For example, meeting friends, going out for a meal, going to a party etc.
1
2
3
4
5
38
Are you satisfied with your chances to be involved in local activities? For example, being part of what is happening in your local area or neighbourhood.
1
2
3
4
5
39
Do you feel that your dreams, hopes and wishes will happen? For example, do you feel you will get the chance to do the things you want, or get the things you wish for, in your life?
1
2
3
4
5
Do you have any comments about the questionnaire?
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
THANK YOU FOR YOUR HELP

The WHOQOL-
DISABILITIES module – manual
WHOQOL-BREF & DISABILITIES MODULE (PROXY) INSTRUCTIONS You are being asked to complete this assessment on behalf of someone else (a proxy assessment). This may be
because that person cannot answer the questions (e.g. as a result of illness or disability), or because the views of
another individual who knows the person well are being sought also.
In order to complete a proxy assessment, you must know well the person for whom you are responding. For
example, you might be the person‟s partner, a member of their family, a close friend, a health or social care
worker, a health professional or their advocate (a person formally or legally appointed to help them). You should
answer the questions as you think the person for whom you are responding would answer, using all your
knowledge and experience of that person and their life.
If you do not know the person well enough to answer questions on their behalf, you should not complete the
assessment. (In this case, please return the questionnaire and explain that you are unable to act as a proxy for this
person.) This assessment asks how the person for whom you are responding feels about their quality of life,
health or other areas of their life. It is about them, and their life, rather than about you.
Please keep in mind what is important to the person for whom you are responding; what makes them happy;
their hopes and dreams, and their worries or concerns.
Please answer all the questions. If you are unsure about which answer to give to a question - if it is hard to pick an
answer - please choose the one that seems nearest or most appropriate. This can often be the first thing that comes into
your mind. Some questions include an example to help you think about your answer.
There are no right or wrong answers – just answer what you believe is true. Please think about the life of the person in
the last two weeks.
For example, thinking about the last two weeks, a question might ask:
EXAMPLE
Not at all A Little Moderately Mostly Totally
Does he/she get the kind of support that he/she needs from others? For example, does he/she get the kind of help he/she needs from other people?
1
2
3
4
5
In this item, the question has an example. You should circle the number that best fits what the person for whom you are
responding would say about the kind of support (or help) they got from others over the last two weeks. So you would
circle the number 3 if the support (or help) the person got met their needs moderately, as follows:
EXAMPLE
Not at all A Little Moderately Mostly Totally
Does he/she get the kind of support that he/she needs from others? For example, does he/she get the kind of help he/she needs from other people?
1
2
3
4
5
Alternatively, you would circle number 1 if the person for whom you are responding would say that the support they got
over the last two weeks did not meet his/her needs at all.
Please read each question, think about the feelings of the person for whom you are responding, and circle the number on
the scale for each question that gives the best answer for him/her.
You may find it helpful to look at the „smiley faces‟ that add a visual guide (a picture) to the number scales. These are
printed on separate cards also. Please think about the life of the person for whom you are responding in the last two
weeks:
The first two questions ask about his/her life and health overall.
3

The WHOQOL-
DISABILITIES module – manual
Not at all A Little Moderately Mostly Totally
1G
Is he/she satisfied with his/her life?
1
2
3
4
5
2G
Is he/she satisfied with his/her health?
1
2
3
4
5
The following questions ask about how he/she has felt about certain things, how much he/she has been able to do
certain things, or how satisfied he/she has been about various aspects of his/her life over the last two weeks.
Not at all A Little Moderately Mostly Totally
3
Does (physical) pain stop him/her from doing what he/she needs to do?
1
2
3
4
5
4
Does he/she need any medical treatment to help him/her in his/her daily life? For example, medicines.
1
2
3
4
5
Not at all A Little Moderately Mostly Totally
5
Does he/she enjoy his/her life?
1
2
3
4
5
6
Does he/she feel his/her life has meaning? For example, does he/she feel his/her life is important and has a purpose?
1
2
3
4
5
7
Is he/she able to think clearly? For example, is he/she able to pay attention, and think carefully about things?
1
2
3
4
5
8
Does he/she feel safe in his/her daily life? For example, at home and in the places he/she goes to during the day.
1
2
3
4
5
9
Does he/she feel the local area he/she lives in is healthy? For example, thinking about the noise, the traffic, the pollution, the weather.
1
2
3
4
5
10
Does he/she have enough energy for everyday life? For example, is he/she able to do things through the day without feeling tired?
1
2
3
4
5
11
Is he/she able to accept the way his/her body looks?
1
2
3
4
5
12
Does he/she have enough money for the things he/she needs?
1
2
3
4
5

The WHOQOL-
DISABILITIES module – manual
Not at all A Little Moderately Mostly Totally
13
Is he/she able to get the information that he/she needs in his/her day-to-day life?
For example, is it easy to find out about things he/she needs to know in his/her daily life?
1
2
3
4
5
14
Does he/she get the chance to do leisure activities?
For example, does he/she get the chance to do things he/she enjoys in his/her spare time?
1
2
3
4
5
15
Is he/she able to get around OK in the house and outside?
1
2
3
4
5
16
Is he/she satisfied with his/her sleep?
1
2
3
4
5
17
Is he/she satisfied with his/her ability to do his/her daily activities?
For example, looking after himself/herself, washing, dressing, eating.
1
2
3
4
5
18
Is he/she satisfied with his/her ability to work?
For example, to do his/her job, or his/her daily activities.
1
2
3
4
5
19
Is he/she satisfied with himself/herself as a person?
For example, with the kind of person he/she is, in what he/she does, how he/she spends his/her time, his/her friendships, his/her achievements.
1
2
3
4
5
20
Is he/she satisfied with his/her personal relationships?
For example, how he/she gets along with the people in his/her life, his/her friends, his/her family, the people he/she lives with.
1
2
3
4
5
21
Is he/she satisfied with his/her sex life, or his/her relationship with his/her partner?
For example, his/her husband/wife, boyfriend/girlfriend.
1
2
3
4
5
22
Is he/she satisfied with the support he/she gets from his/her friends?
1
2
3
4
5
23
Is he/she satisfied with what his/her home is like?
For example, thinking about his/her home and the place he/she lives in.
1
2
3
4
5
24
Is he/she satisfied with his/her access to health services?
For example, is it easy to see the doctors, nurses or other staff who look after him/her when he/she is unwell?
1
2
3
4
5
25
Is he/she satisfied with the transport he/she can use?
For example, how he/she gets to the places he/she goes to (e.g. by bus, car, taxi etc.).
1
2
3
4
5
Not at all A Little Moderately Mostly Totally
26
Does he/she feel very unhappy, sad, worried or depressed?
1
2
3
4
5

The WHOQOL-
DISABILITIES module – manual
DISABILITIES MODULE
The next question asks about his/her disability overall.
Not at all A Little Moderately Mostly Totally
27G Does he/she feel that his/her disability has a negative (bad) effect on his/her day-to-day life?
1
2
3
4
5
The following questions ask about how he/she has felt about certain things, how much certain things have applied to
him/her, and how satisfied he/she has been about various parts of his/her life over the last two weeks
Not at all A Little Moderately Mostly Totally
28
Does he/she feel that some people treat him/her unfairly?
1
2
3
4
5
29
Does he/she feel that he/she needs someone to stand up for him/her when he/she has problems?
1
2
3
4
5
30
Does he/she worry about what might happen to him/her in the future? For example, thinking about not being able to look after him/herself, or being a burden to others in the future.
1
2
3
4
5
Not at all A Little Moderately Mostly Totally
31
Does he/she feel in control of his/her life? For example, does he/she feel in charge of his/her life?
1
2
3
4
5
32
Does he/she make his/her own choices about his/her day-to-day life? For example, where to go, what to do, what to eat.
1
2
3
4
5
33
Does he/she get to make the big decisions in his/her life? For example, like deciding where to live, or who to live with, how to spend his/her money.
1
2
3
4
5
34
Is he/she satisfied with his/her ability to communicate with other people? For example, how he/she says things or gets his/her point across, the way he/she understands others, by words or signs.
1
2
3
4
5
35
Does he/she feel that other people accept him/her?
1
2
3
4
5
36
Does he/she feel that other people respect him/her?
1
2
3
4
5

The WHOQOL-
DISABILITIES module – manual
For example, does he/she feel that others value him/her as a person and listen to what he/she has to say?
Not at all A Little Moderately Mostly Totally
37
Is he/she satisfied with his/her chances to be involved in social activities?
For example, meeting friends, going out for a meal, going to a party
etc.
1
2
3
4
5
38
Is he/she satisfied with his/her chances to be involved in local activities? For example, being part of what is happening in his/her local area or neighbourhood.
1
2
3
4
5
39
Does he/she feel that his/her dreams, hopes and wishes will happen? For example, does he/she feel he/she will get the chance to do the things he/she wants, or get the things he/she wishes for, in his/her life?
1
2
3
4
5
Do you have any comments about the questionnaire?
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………

The WHOQOL-
DISABILITIES module – manual
ABOUT YOU
Finally, we would like to ask you to answer a few general questions about yourself. Please answer by putting a cross
like this X in the box beside the correct answer OR write in the space provided.
Gender Male Female
Age (in years) Date of Birth
(dd / mm / yy)
Education: What is the highest level of education you received?
None at all
Primary school
Secondary school / High school
College / University
Other (please tell us what)…………………………………………………………………
Your relationship to the person for whom you have responded:
Partner
Parent
Sibling
Other family member (please specify relationship)………………………………………..
Friend
Paid Carer / Staff
Professional
Other (please tell us what)…………………………………………………………………
How long have you known the person? ………………………………………………………..…(years / months)
How much contact do you have with the person?
Monthly Fortnightly Weekly Daily 24 hours
How well do you think you know the person?
Not very well A Little Quite well Well Very well
Your view of the Quality of Life of the person for whom you have responded:
How do you think his/her quality of life compares with that of other people who live in the
same local area?
Much worse A bit worse About the same A bit better Much better
How do you think his/her quality of life compares with that of other people with similar disabilities?
Much worse A bit worse About the same A bit better Much better
Overall, how easy or difficult did you find it to answer quality of life questions on his/her behalf?
Very difficult Difficult Neither easy
nor difficult Easy Very easy

The WHOQOL-
DISABILITIES module – manual
APPENDIX 2 - STEPS FOR CHECKING AND CLEANING DATA WHOQOL ID and PD
Modules
Steps for ID Module SPSS syntax for carrying out data checking, cleaning and
computing total scores
Check all 12 items from
assessment have a range of 1-3
RECODE f28 f29 f30 f31 f32 f33 f34 f35 f36 f37 f38 f39
(1=1) (2=2) (3=3) (ELSE=SYSMIS).
(This recodes all data outside the range 1-3 to system missing.)
Reverse negatively phrased
items
RECODE f28 f29 f30 (1=3) (2=2) (3=1).
(This transforms negatively framed questions to positively framed
questions.)
Compute total module score COMPUTE DIS12sum
=(MEAN.10(f28,f29,f30,f31,f32,f33,f34,f35,f36,f37,f38,f39))*12.
(These equations calculate the DIS total scores. Mean scores are
multiplied by 12 so as to provide total scores while permitting up to
two items to be missing. The „.10‟ in „mean.10‟ specifies that at
least 10 items must be endorsed or not missing for the score to be
calculated.)
Transform scores to a 0-100
scale if needed
COMPUTE DIS100 = (DIS12sum - 12)*(100/24).
Steps for PD Module SPSS syntax for carrying out data checking, cleaning and
computing total scores
Check all 12 items from
assessment have a range of 1-5
RECODE f28 f29 f30 f31 f32 f33 f34 f35 f36 f37 f38 f39
(1=1) (2=2) (3=3) (4=4) (5=5) (ELSE=SYSMIS).
(This recodes all data outside the range 1-5 to system missing.)
Reverse negatively phrased
items
RECODE f28 f29 f30 (1=5) (2=4) (3=3) (4=2) (5=1).
(This transforms negatively framed questions to positively framed
questions.)
Compute total module score COMPUTE DIS12sum
=(MEAN.10(f28,f29,f30,f31,f32,f33,f34,f35,f36,f37,f38,f39))*12.
(These equations calculate the DIS total scores. Mean scores are
multiplied by 12 so as to provide total scores while permitting up to
two items to be missing. The „.10‟ in „mean.10‟ specifies that at
least 10 items must be endorsed or not missing for the score to be
calculated.)
Transform scores to a 0-100
scale if needed
COMPUTE DIS100 = (DIS12sum - 12)*(100/48).

The WHOQOL-
DISABILITIES module – manual
APPENDIX III - REFERENCE DATA FOR WHOQOL-DIS MODULE
i) Field Trial ID Data by Centre (variable DIS12sum - summary scores)
ii) Field Trial PD Data by Centre (variable DIS12sum - summary scores)
Valid N Mean Std Deviation
Name of centre
Edinburgh N=124 44.85 7.57
Barcelona N=148 42.12 7.87
Paris N=18 39.34 4.80
Prague N=240 43.58 7.42
Tromso N=30 44.27 7.90
Izmir N=156 40.71 8.66
Vilnius N=238 41.02 7.19
Sicily N=309 40.62 8.44
Hamburg N=51 44.60 7.65
Tilburg N=108 43.39 8.18
Guangzhou N=805 36.45 7.02
Porto Alegre N=161 44.37 7.33
Montevideo N=43 43.27 7.53
Budapest N=150 46.13 7.64
Total N=2581 40.75 8.23
Valid N Mean Std Deviation
Name of centre
Edinburgh N=93 29.28 3.79
Barcelona N=99 27.48 4.32
Prague N=40 27.78 3.38
Izmir N=150 26.30 4.93
Vilnius N=60 21.88 4.97
Sicily N=17 24.76 4.96
Hamburg N=90 29.57 3.39
Guangzhou N=193 21.59 5.10
Porto Alegre N=157 28.51 4.29
Montevideo N=76 29.26 3.97
Budapest N=163 28.08 3.43
Total N=1138 26.66 5.16

The WHOQOL-
DISABILITIES module – manual
iii) Field Trial ID Data by Centre (variable DIS100 - 0-100 transformed scores)
Valid N Mean Std Deviation
Name of centre
Edinburgh N=93 72.00 15.80
Barcelona N=99 64.52 17.99
Prague N=40 65.73 14.07
Izmir N=150 59.58 20.52
Vilnius N=60 41.18 20.70
Sicily N=17 53.19 20.65
Hamburg N=90 73.19 14.12
Guangzhou N=193 39.94 21.24
Porto Alegre N=157 68.79 17.86
Montevideo N=76 71.93 16.56
Budapest N=163 67.00 14.28
Total N=1138 61.07 21.51
iv) Field Trial PD Data by Centre (variable DIS100 - 0-100 transformed scores)
Valid N Mean Std Deviation
Name of centre
Edinburgh N=124 68.44 15.77
Barcelona N=148 62.76 16.39
Paris N=18 56.95 10.00
Prague N=240 65.80 15.46
Tromso N=30 67.23 16.47
Izmir N=156 59.80 18.04
Vilnius N=238 60.45 14.97
Sicily N=309 59.63 17.59
Hamburg N=51 67.92 15.93
Tilburg N=108 65.39 17.04
Guangzhou N=805 50.95 14.63
Porto Alegre N=161 67.44 15.28
Montevideo N=43 65.15 15.69
Budapest N=150 71.11 15.92
Total N=2581 59.91 17.14

The WHOQOL-
DISABILITIES module – manual
APPENDIX IV - ATTITUDES TO DISABILITY SCALE (GENERAL) INSTRUCTIONS
This questionnaire asks you how you feel about disabilities and people with disabilities in general.
Please keep in mind your standards; what makes you happy; your hopes and dreams, and your worries or
concerns.
Please answer all the questions. If you are unsure about which answer to give to a question - if it is hard to pick an
answer - please choose the one that seems nearest or most appropriate. This can often be the first thing that comes into
your mind.
There are no right or wrong answers – just answer what is true for you. Please think about your life and your
experience of disabilities in general.
For example, thinking about your life and your experience of disabilities in general, a statement might say:
EXAMPLE
Strongly disagree
Disagree Uncertain Agree Strongly agree
People with a disability can be as happy as anyone else.
1
2
3
4
5
You should circle the number that best fits how much you agree with the statement. So you would circle the number 5 if
you strongly agree that people with a disability can be as happy as anyone else, as follows:
EXAMPLE
Strongly disagree
Disagree Uncertain Agree Strongly agree
People with a disability can be as happy as anyone else.
1
2
3
4
Alternatively, you would circle number 1 if you strongly disagree that people with a disability can be as happy as
anyone else.
Please read each statement, think about your feelings, and circle the number on the scale for each question that gives the
best answer for you.
You may find it helpful to look at the „smiley faces‟ that add a visual guide (a picture) to the number scales. These are
available printed on separate cards also.
If you would like some help to write your answers on the form, it is OK to ask someone to do this for you.
5

The WHOQOL-
DISABILITIES module – manual
These questions ask how much you agree with the following statements.
If you agree with the statements an extreme amount (a great deal) circle the number 5 next to “Strongly agree”. If you
do not agree with the statements at all, circle the number 1 next to “Strongly disagree”. Alternatively, if your answer
lies somewhere between “Strongly disagree” and “Strongly agree”, you should circle one of the numbers 2, 3 or 4 in
between.
Please think about disability and people with disabilities in general.
Strongly disagree
Disagree Uncertain Agree Strongly agree
1
People with a disability find it harder than others to make new friends.
1
2
3
4
5
2
People with a disability have problems getting involved in society.
1
2
3
4
5
3
People often make fun of disabilities.
1
2
3
4
5
4
People with a disability are easier to take advantage of (exploit or treat badly) compared with other people.
1
2
3
4
5
5
People with a disability are a burden on society.
1
2
3
4
5
6
People with a disability are a burden on their family.
1
2
3
4
5
Strongly disagree
Disagree Uncertain Agree Strongly agree
7
Having a disability can make someone a stronger person.
1
2
3
4
5
8
Having a disability can make someone a wiser person.
1
2
3
4
5
9
Some people achieve more because of their disability (e.g. they are more successful).
1
2
3
4
5
10
People with a disability are more determined than others to reach their goals.
1
2
3
4
5

The WHOQOL-
DISABILITIES module – manual
Strongly disagree
Disagree Uncertain Agree Strongly agree
11
People tend to become impatient with those with a disability.
1
2
3
4
5
12
People tend to treat those with a disability as if they have no feelings.
1
2
3
4
5
13
Sex should not be discussed with people with disabilities.
1
2
3
4
5
14
People should not expect too much from those with a disability.
1
2
3
4
5
15
People with a disability should not be optimistic (hopeful) about their future.
1
2
3
4
5
16
People with a disability have less to look forward to than others.
1
2
3
4
5
Do you have any comments about the questionnaire?
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
THANK YOU FOR YOUR HELP

The WHOQOL-
DISABILITIES module – manual
ATTITUDES TO DISABILITY SCALE (PERSONAL) INSTRUCTIONS
This questionnaire asks you how you feel about your own disability.
Please keep in mind your standards; what makes you happy; your hopes and dreams, and your worries or
concerns.
Please answer all the questions. If you are unsure about which answer to give to a question - if it is hard to pick an
answer - please choose the one that seems nearest or most appropriate. This can often be the first thing that comes into
your mind.
There are no right or wrong answers – just answer what is true for you. Please think about your life and your
experience of your disability.
For example, thinking about your life and your disability, a statement might say:
EXAMPLE
Strongly disagree
Disagree Uncertain Agree Strongly agree
I can be as happy as anyone else, even though I have a disability.
1
2
3
4
5
You should circle the number that best fits how much you agree with the statement. So you would circle the number 5 if
you strongly agree that you can be as happy as anyone else, in spite of your disability, as follows:
EXAMPLE
Strongly disagree
Disagree Uncertain Agree Strongly agree
I can be as happy as anyone else, even though I have a disability.
1
2
3
4
Alternatively, you would circle number 1 if you strongly disagree that you can be as happy as anyone else.
Please read each statement, think about your feelings, and circle the number on the scale for each question that gives the
best answer for you.
You may find it helpful to look at the „smiley faces‟ that add a visual guide (a picture) to the number scales. These are
available printed on separate cards also.
If you would like some help to write your answers on the form, it is OK to ask someone to do this for you.
5

The WHOQOL-
DISABILITIES module – manual
These questions ask how much you agree with the following statements.
If you agree with the statements an extreme amount (a great deal) circle the number 5 next to “Strongly agree”. If you
do not agree with the statements at all, circle the number 1 next to “Strongly disagree”. Alternatively, if your answer
lies somewhere between “Strongly disagree” and “Strongly agree”, you should circle one of the numbers 2, 3 or 4 in
between.
Please think about your life and your disability.
Strongly disagree
Disagree Uncertain Agree Strongly agree
1
Because of my disability, I find it harder than others to make new friends.
1
2
3
4
5
2
Because of my disability, I have problems getting involved in society.
1
2
3
4
5
3
People often make fun of my disability.
1
2
3
4
5
4
Because of my disability, I am easier to take advantage of (exploit or treat badly) compared with other people.
1
2
3
4
5
5
Because of my disability, I feel I am a burden on society.
1
2
3
4
5
6
Because of my disability, I feel I am a burden on my family.
1
2
3
4
5
Strongly disagree
Disagree Uncertain Agree Strongly agree
7
I feel I am a stronger person, because of my disability.
1
2
3
4
5
8
I feel I am a wiser person (I have learned a lot about life) because of my disability.
1
2
3
4
5
9 I achieve more because of my disability (e.g. I am more
successful).
1
2
3
4
5
10
Because of my disability, I am more determined than others to reach my goals.
1
2
3
4
5

The WHOQOL-
DISABILITIES module – manual
Strongly disagree
Disagree Uncertain Agree Strongly agree
11
Because of my disability, people tend to become impatient with me.
1
2
3
4
5
12
Because of my disability, people tend to treat me as if I have no feelings.
1
2
3
4
5
13
People think they should not discuss sex with me, because of my disability.
1
2
3
4
5
14
Because of my disability, people should not expect too much from me.
1
2
3
4
5
15
Because of my disability, I am not optimistic (hopeful) about my future.
1
2
3
4
5
16
Because of my disability, I have less to look forward to than others.
1
2
3
4
5
Do you have any comments about the questionnaire?
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
……………………………………………………………………………………………………………………………
THANK YOU FOR YOUR HELP

The WHOQOL-
DISABILITIES module – manual
ATTITUDES TO DISABILITY SCALE (ID - GENERAL) INSTRUCTIONS
This questionnaire asks you how you feel about disabilities and people with disabilities in general.
Please keep in mind your standards; what makes you happy; your hopes and dreams, and your worries or
concerns.
Please answer all the questions. If you are unsure about which answer to give to a question - if it is hard to pick an
answer - please choose the one that seems nearest or most appropriate. This can often be the first thing that comes into
your mind.
There are no right or wrong answers – just answer what is true for you. Please think about your life, and your
experience of disabilities, in general.
For example, thinking about your life and your experience of disabilities in general, a statement might say:
EXAMPLE
Disagree Uncertain Agree
People with a disability can be as happy as anyone else.
1
2
3
You should circle the number that best fits how much you agree with the statement. So you would circle the number 3 if
you agree that people with a disability can be as happy as anyone else, as follows:
EXAMPLE
Disagree Uncertain Agree
People with a disability can be as happy as anyone else.
1
2
Alternatively, you would circle number 1 if you disagree that people with a disability can be as happy as anyone else.
Please read each statement, think about your feelings, and circle the number on the scale for each question that gives the
best answer for you.
You may find it helpful to look at the „smiley faces‟ that add a visual guide (a picture) to the number scales. These are
available printed on separate cards also.
If you would like some help to write your answers on the form, it is OK to ask someone to do this for you.
3

The WHOQOL-
DISABILITIES module – manual
These questions ask how much you agree with the following statements.
If you agree with the statements circle the number 3 next to “Agree”. If you do not agree with the statements, circle the
number 1 next to “Disagree”. Alternatively, if your answer lies somewhere between “Disagree” and “Agree”, you
should circle the number 2 in between.
Please think about disability and people with disabilities in general.
Disagree Uncertain Agree
1
People with a disability find it harder than others to make new friends.
1
2
3
2
People with a disability have problems getting involved in society.
1
2
3
3
People often make fun of disabilities.
1
2
3
4
People with a disability are easier to take advantage of (exploit or treat badly) compared with other people.
1
2
3
5
People with a disability are a burden on society.
1
2
3
6
People with a disability are a burden on their family.
1
2
3
Disagree Uncertain Agree
7 Having a disability can make someone a stronger person.
1
2
3
8 Having a disability can make someone a wiser person.
1
2
3
9 Some people achieve more because of their disability (e.g. they are more
successful).
1
2
3
10
People with a disability are more determined than others to reach their goals.
1
2
3

The WHOQOL-
DISABILITIES module – manual
Disagree Uncertain Agree
11
People tend to become impatient with those with a disability.
1
2
3
12
People tend to treat those with a disability as if they have no feelings.
1
2
3
13
Sex should not be discussed with people with disabilities.
1
2
3
14
People should not expect too much from those with a disability.
1
2
3
15
People with a disability should not be optimistic (hopeful) about their future.
1
2
3
16
People with a disability have less to look forward to than others.
1
2
3
Do you have any comments about the questionnaire?
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
THANK YOU FOR YOUR HELP

The WHOQOL-
DISABILITIES module – manual
ATTITUDES TO DISABILITY SCALE (ID - PERSONAL) INSTRUCTIONS
This questionnaire asks you how you feel about your own disability.
Please keep in mind your standards; what makes you happy; your hopes and dreams, and your worries or
concerns.
Please answer all the questions. If you are unsure about which answer to give to a question - if it is hard to pick an
answer - please choose the one that seems nearest or most appropriate. This can often be the first thing that comes into
your mind.
There are no right or wrong answers – just answer what is true for you. Please think about your life and your
experience of your disability.
For example, thinking about your life and your disability, a statement might say:
EXAMPLE
Disagree Uncertain Agree
I can be as happy as anyone else, even though I have a disability.
1
2
3
You should circle the number that best fits how much you agree with the statement. So you would circle the number 3 if
you agree that you can be as happy as anyone else, in spite of your disability, as follows:
EXAMPLE
Disagree Uncertain Agree
I can be as happy as anyone else, even though I have a disability.
1
2
3
Alternatively, you would circle number 1 if you disagree that you can be as happy as anyone else.
Please read each statement, think about your feelings, and circle the number on the scale for each question that gives the
best answer for you.
You may find it helpful to look at the „smiley faces‟ that add a visual guide (a picture) to the number scales. These are
available printed on separate cards also.
If you would like some help to write your answers on the form, it is OK to ask someone to do this for you.
3

The WHOQOL-
DISABILITIES module – manual
These questions ask how much you agree with the following statements.
If you agree with the statements circle the number 3 next to “Agree”. If you do not agree with the statements, circle the
number 1 next to “Disagree”. Alternatively, if your answer lies somewhere between “Disagree” and “Agree”, you
should circle the number 2 in between.
Please think about your life and your disability.
Disagree Uncertain Agree
1
Because of my disability, I find it harder than others to make new friends.
1
2
3
2
Because of my disability, I have problems getting involved in society.
1
2
3
3
People often make fun of my disability.
1
2
3
4
Because of my disability, I am easier to take advantage of (exploit or treat badly) compared with other people.
1
2
3
5
Because of my disability, I feel I am a burden on society.
1
2
3
6
Because of my disability, I feel I am a burden on my family.
1
2
3
Disagree Uncertain Agree
7
I feel I am a stronger person, because of my disability.
1
2
3
8 I feel I am a wiser person (I have learned a lot about life) because of my disability.
1
2
3
9 I achieve more because of my disability (e.g. I am more successful).
1
2
3
10
Because of my disability, I am more determined than others to reach my goals.
1
2
3

The WHOQOL-
DISABILITIES module – manual
Disagree Uncertain Agree
11
Because of my disability, people tend to become impatient with me.
1
2
3
12
Because of my disability, people tend to treat me as if I have no feelings.
1
2
3
13
People think they should not discuss sex with me, because of my disability.
1
2
3
14
Because of my disability, people should not expect too much from me.
1
2
3
15
Because of my disability, I am not optimistic (hopeful) about my future.
1
2
3
16
Because of my disability, I have less to look forward to than others.
1
2
3
Do you have any comments about the questionnaire?
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………
……………………………………………………………………………………………………………………………
THANK YOU FOR YOUR HELP

The WHOQOL-
DISABILITIES module – manual
APPENDIX V QOCS - ID INSTRUCTIONS
This assessment asks how you feel about the quality of the care and support you receive. This includes health
(medical) care, social care and family support. This care could come from any source e.g. care that is free, or care
you have to pay for. It is just about you – you and your care.
Please keep in mind your standards, what makes you happy, your hopes and dreams, and your worries or concerns.
Please answer all the questions. If you are unsure about which answer to give to a question - if it is hard to pick an
answer - please choose the one that seems nearest or most appropriate. This can often be the first thing that comes into
your mind. Some questions include an example to help you think about your answer.
There are no right or wrong answers – just answer what is true for you. Please think about your care over the last six
months.
For example, thinking about the last six months, a question might ask:
EXAMPLE
Not at all Moderately Totally
Do your care providers give you the kind of care and support you need?
1
2
3
You should circle the number that best fits your opinion about whether you got the kind of care and support you needed
from your care providers over the last six months. So you would circle the number 3 if you got the care and support you
needed totally, as follows:
EXAMPLE
Not at all Moderately Totally
Do your care providers give you the kind of care and support you need?
1
2
3
Alternatively, you would circle number 1 if you did not get the kind of care and support you needed at all over the last
six months.
Please read each question, think about your feelings, and circle the number on the scale for each question that gives the
best answer for you.
You may find it helpful to look at the „smiley faces‟ that add a visual guide (a picture) to the number scales. These are
available printed on separate cards also.
If you would like some help to write your answers on the form, it is OK to ask someone to do this for you.
3

The WHOQOL-
DISABILITIES module – manual
Please think about your life, and the care and support you have received, over the last six months.
These questions ask about your health and social care, and the professionals and support staff who provide your care.
This may include services provided by doctors, psychologists, nurses, physiotherapists, social workers etc.
Not at all Moderately Totally
1
Are the people who provide your care (the professional staff) good at their jobs?
1
2
3
2
Do the people who provide your care know enough about your condition or disability? For example, do they know enough about the problems or difficulties you experience?
1
2
3
3
Do the people who provide your care meet your needs?
1
2
3
4
Do the people who provide your care involve you in decisions about your health and/or social care?
1
2
3
These questions ask about how easy it is for you to get health and social care services, and to get to see the
professionals who provide your care.
Not at all Moderately Totally
5
Do you have to wait a long time to see the people who provide your care? For example, does it take long to get appointments with doctors, psychologists, nurses, physiotherapists, social workers etc?
1
2
3
6
Do you have to do a lot of paperwork to get the services you need? For example, do you have to fill in lots of forms?
1
2
3
7
Do you have to fight for the care and support you need?
1
2
3
8
Does a lack of services where you live limit the care and support you get? For example, if there is a lack of facilities, staff, or money for medicines or other treatments.
1
2
3

The WHOQOL-
DISABILITIES module – manual
These questions ask about how well all the care and support you receive (from health and social care services, and from
your family) meets your needs.
Not at all Moderately Totally
9
Do you get the help you need to live in your home? For example, help with washing, dressing, cooking, cleaning etc
1
2
3
10
Can you get help to take part in leisure activities? For example, things you like to do for fun, your hobbies and interests.
1
2
3
11
Can you get help to take part in social activities? For example, meeting friends or going out for a meal.
1
2
3
12
Do you get enough care and support? For example, do you have enough people looking after you to meet your needs?
1
2
3
13
Do you feel safe about the care you get? For example, do you feel secure and protected, that you will not have an accident or get hurt, that you will not suffer abuse etc?
1
2
3
These questions ask about the information you have been given about your disability and about the care and support
available to help you.
Not at all Moderately Totally
14
Have you been given enough information about your disability? For example, has someone talked to you about your disability or health problems?
1
2
3
15
Do you know about the services and support you can get to help you? For example, treatments, therapies, medicines, support associations, aids and equipment.
1
2
3
16
Do you know about the money and other benefits you can get to help you? For example, a pension, free transport, day services.
1
2
3
17
Are you given information in a way that you can understand easily? For example, do people tell you things in a way you can understand and explain things clearly to you; is any written material easy to understand?
1
2
3

The WHOQOL-
DISABILITIES module – manual
QOCS -ID (PROXY) INSTRUCTIONS
You are being asked to complete this assessment on behalf of someone else (a proxy assessment). This may be
because that person cannot answer the questions (e.g. as a result of illness or disability), or because the views of
another individual who knows the person well are being sought also.
In order to complete a proxy assessment, you must know well the person for whom you are responding. For
example, you might be the person‟s partner, a member of their family, a close friend, a health or social care
worker, a health professional or their advocate (a person formally or legally appointed to help them). You should
answer the questions as you think the person for whom you are responding would answer, using all your
knowledge and experience of that person and their life.
If you do not know the person well enough to answer questions on their behalf, you should not complete the
assessment. (In this case, please return the questionnaire and explain that you are unable to act as a proxy for this
person.)
This assessment asks how the person for whom you are responding feels about the quality of care and support
they receive. This includes health (medical) care, social care and family support. This care could come from any
source e.g. care that is free, or care they have to pay for. It is about them, and their care, rather than about you.
Please keep in mind what is important to the person for whom you are responding; their standards, what
makes them happy; their hopes and dreams, and their worries or concerns.
Please answer all the questions. If you are unsure about which answer to give to a question - if it is hard to pick an
answer - please choose the one that seems nearest or most appropriate. This can often be the first thing that comes into
your mind. Some questions include an example to help you think about your answer.
There are no right or wrong answers – just answer what you believe is true. Please think about the care of the person
over the last six months.
For example, thinking about the last six months, a question might ask:
EXAMPLE
Not at all A Little Moderately Mostly Totally
Do his/her care providers give him/her the kind of care and support he/she needs?
1
2
3
4
5
You should circle the number that best fits what the person for whom you are responding would say about whether
he/she got the kind of care and support he/she needed from his/her care providers over the last six months. So you
would circle the number 5 if the person got the care and support he/she needed totally, as follows:
EXAMPLE
Not at all A Little Moderately Mostly Totally
Do his/her care providers give him/her the kind of care and support he/she needs?
1
2
3
4
5
Alternatively, you would circle number 1 if the person for whom you are responding would say he/she did not get the
kind of care and support he/she needed over the last six months.
Please read each question, think about the feelings of the person for whom you are responding, and circle the number on
the scale for each question that gives the best answer for him/her.
5

The WHOQOL-
DISABILITIES module – manual
You may find it helpful to look at the „smiley faces‟ that add a visual guide (a picture) to the number scales. These are
printed on separate cards also.
Please think about the life of the person for whom you are responding, and the care and support he/she has received,
over the last six months.
These questions ask about his/her health and social care, and the professionals and support staff who provide his/her
care. This may include services provided by doctors, psychologists, nurses, physiotherapists, social workers etc.
Not at all A Little Moderately Mostly Totally
1
Are the people who provide his/her care (the professional staff) good at their jobs?
1
2
3
4
5
2
Do the people who provide his/her care know enough about his/her condition or disability? For example, do they know enough about the problems or difficulties he/she experiences?
1
2
3
4
5
3
Do the people who provide his/her care meet his/her needs?
1
2
3
4
5
4
Do the people who provide his/her care involve him/her in decisions about his/her health and/or social care?
1
2
3
4
5
These questions ask about how easy it is for him/her to get health and social care services, and to get to see the
professionals who provide his/her care.
Not at all A Little Moderately Mostly Totally
5
Does he/she have to wait a long time to see the people who provide his/her care? For example, does it take long to get appointments with doctors, psychologists, nurses, physiotherapists, social workers etc?
1
2
3
4
5
6
Does he/she have to do a lot of paperwork to get the services he/she needs? For example, does he/she have to fill in lots of forms?
1
2
3
4
5
7
Does he/she have to fight for the care and support he/she needs?
1
2
3
4
5
8
Does a lack of services where he/she lives limit the care and support he/she gets? For example, if there is a lack of facilities, staff, or money for medicines or other treatments.
1
2
3
4
5

The WHOQOL-
DISABILITIES module – manual
These questions ask about how well all the care and support he/she receives (from health and social care services, and
from his/her family) meets his/her needs.
Not at all A Little Moderately Mostly Totally
9
Does he/she get the help he/she needs to live in his/her home? For example, help with washing, dressing, cooking, cleaning etc
1
2
3
4
5
10
Can he/she get help to take part in leisure activities? For example, things he/she likes to do for fun, his/her hobbies and interests.
1
2
3
4
5
11
Can he/she get help to take part in social activities? For example, meeting friends or going out for a meal.
1
2
3
4
5
12
Does he/she get enough care and support? For example, does he/she have enough people looking after him/her to meet his/her needs?
1
2
3
4
5
13
Does he/she feel safe about the care he/she gets? For example, does he/she feel secure and protected, that he/she will not have an accident or get hurt, that he/she will not suffer abuse etc?
1
2
3
4
5
These questions ask about the information he/she has been given about his/her disability and about the care and support
available to help him/her.
Not at all A Little Moderately Mostly Totally
14
Has he/she been given enough information about his/her disability? For example, has someone talked to him/her about his/her disability or health problems?
1
2
3
4
5
15
Does he/she know about the services and support he/she can get to help him/her? For example, treatments, therapies, medicines, support associations, aids and equipment.
1
2
3
4
5
16
Does he/she know about the money and other benefits he/she can get to help him/her? For example, a pension, free transport, day services.
1
2
3
4
5
17
Is he/she given information in a way that he/she can understand easily? For example, do people tell him/her things in a way he/she can understand and explain things clearly to him/her; is any written material easy to understand?
1
2
3
4
5

The WHOQOL-DISABILITIES module – manual
No. Centre APPENDIX VI - CENTRES Project Personnel Telephone Fax E-mail
1 Edinburgh Clinical & Health Psychology Prof Mick Power 44-131-651-3943 44-131-651-3971 [email protected]
University of Edinburgh Dr Ann Green 44-131-466-1756 44-131-651-3971 [email protected]
Teviot Place
Edinburgh
EH8 9AG
2 WHO (Geneva) 20 Avenue Appia Dr Somnath Chatterji 41-22-791-3202 41-22-791-4328 [email protected]
Geneva 27
Switzerland
CH 1211
3 Barcelona Fundacio Institut Català de l´Envelliment Dr Ramona Lucas 34-93-433-50-69 34-93-4464505 [email protected]
Universitat Autonoma de Barcelona
Sant Antoni Maria Claret, 171
08041 Barcelona
4 Paris REHSEIS (CNRS UMR 7596) Prof. Alain Leplège 33 6 64 64 14 33 33 1 44 27 86 47 [email protected]
Université Paris 7 - Denis Diderot Dr Isabelle Ville 33 1 49 58 36 32 33 1 49 58 34 38 [email protected]
2, place Jussieu Ms Laure Cartron [email protected]
75251 Paris cedex 05 Dr Michele Cammelli [email protected]
France
5 Prague Prague Psychiatric Center Dr Eva Dragomirecka 420-2-66-003142 420-2-66-003143 [email protected]
Social Psychiatry Unit Ms Jitka Prajsova 420-2-66-003274 420-2-66-003143 [email protected]
Ustavni 91 Dr Dagmar Dzurova 420-2-21 951390 420-2-24 920657 [email protected]
181 03 Praha 8 - Bohnice
Czech Republic
6 Tromsø Department of Psychology Prof. Martin Eisemann 47-776-46279 47-776-45610 [email protected]
University of Tromsø Ms Linn Kristensen [email protected]
N-9037 Tromsø
Norway

The WHOQOL-DISABILITIES module – manual
8 Izmir Faculty of Medicine, Dept. of Public Health Prof Erhan Eser 90-236-231 83 73 90-236-232-0058 [email protected]
Celal Bayar University (alternatives) 90-232-375 42 38 [email protected]
45020 Manisa Dr Beyhan Cengiz Ozyurt 90-236-239 13 19 [email protected]
Turkey Prof Omer Aydemir [email protected]
Mr Cenaletti Ayik
Dr Sultan Eser [email protected]
9 Vilnius Scientfic Department of Gerontology Problems Dr Jelena Ceremnych 370-5-2697972 370-5-2123073 [email protected]
Institute of Experimental and Clinical Medicine Dr Vaineta Valeikiene 370-5-2777726 370-5-2123073 [email protected]
Zygimantu 9 Dr Vidmantas Alekna 370-5-2777745 370-5-2123073 [email protected]
LT- 01102 Vilnius
Lithuania
10 Sicily Centre for Training and Research in Public Health Dr Rosa Frazzica 39-0934-505204 39-0934-594310 [email protected]
Via G. Mule n.1 Dr Roberta Arnone 39-0934-505381 39-0934-594310 [email protected]
Caltanissetta Dr Marilena Pinco 39-0934-505134 39-0934-594310 [email protected]
Sicily, 93100 Dr Pasquale Di Mattia 39-0934-594310 [email protected]
Italy Dr. Danilo Greco 39-0934-505230 39-0934-594310 [email protected]
12 Hamburg Centre for Psychosocial Medicine Dr Silke Schmidt
Institute of Medical Psychology Ms Christina Bajer 49-40-42803-7723
49-04-42803-4940 [email protected]
Martinistrasse 52 Mr. Kai Kossow 49-40-42803-6207
49-04-42803-4940 [email protected]
Hamburg, 20246 Prof. Monika Bullinger 49-40-42803-6430 [email protected]
Germany
13 Tilburg Department of Psychology and Health Prof. Guus Van Heck 31-13-466-2522 31-13-466-2370 [email protected]
Faculty of Social Sciences Prof. Jolanda De Vries 31-13-466-2705 31-13-466-2067 [email protected]
Tilburg University Ms Brenda Den Oudsten 31-13-466-2940 31-13-466-2067 [email protected]
Warandalaan 2
Tilburg, 5000LE
The Netherlands
14 Guangzhou Dept. of Medical Statistics and Epidemiology Prof Jiqian Fang 86-20-87330671 86-20-87331605 [email protected]
Sun Yat-Sen University Dr Yuantao Hao 86-20-87331587 86-20-87331587 [email protected]
74 Zhongshan Road II

The WHOQOL-DISABILITIES module – manual
Guangzhou 510080
China
15 Porto Alegre Universidade Federal do Rio Grande do Sul Prof Marcelo Pio de Almeida Fleck 55-51-2101-8413 55-51-3330-8965 [email protected]
Rua Ramiro Barcelos 2350 4º andar Dr Juliana Bredemeir [email protected]
Porto Alegre Dr Betina Suñé Mattevi [email protected]
Brazil Cláudia Fam [email protected]
16 Bangalore National Institute for Mental Health and Neurosciences Prof. Santosh K. Chaturvedi 91-80-2699 5264 91-80-2656 4830 [email protected]
Bangalore 560029
India
17 Montevideo Departamento de Psicología Médica Facultad de Medicina Dr Laura Schwartzmann 598-2-4983423 598-2- 6222683 [email protected]
Universidad de la República Dr Eliana Ripa [email protected]
Calabria 3969 Dr. Adriana Suarez [email protected]
CP 11300 Dr. Maria Otero [email protected]
Montevideo Mrs Magdalena Alvarez [email protected]
Uruguay Mrs Ma. Del C. Abreu [email protected]
18 Auckland Division of Rehabilitation and Occupation Studies Prof. Kathryn McPherson 64-9-921-9999 64-9-921-9620 [email protected]
Akoranga Drive Campus (ext 7110)
Auckland University of Technology Prof Rex Billington
AA Building, Room 263 AssPro William Taylor
Private Bag 92006 Auckland Mr Philip Patston
New Zealand Ms Kate Diesfeld
19 Melbourne RMIT University Dr Keith McVilly 61-3-9925-7362 61-3-9925-7303 [email protected]
School of Health Science (Disability Studies) PO Box 71
BUNDOORA 3083
Victoria, Australia
University of Melbourne Dr Graeme Hawthorne 61-0-8344-5467 61-3-9349-2792 [email protected]
Dept. of Psychiatry, Royal Melbourne Hospital
Main Building - Level 1, North
Grattan Street

The WHOQOL-DISABILITIES module – manual
PARKVILLE 3052
Victoria, Australia
20 Hungary G. Barczi Faculty of Special Education Prof Lajos Kullmann 36-30-962-3314 36-1-358-5532 [email protected]
Ecseri ut 3, (mobile)
1097 Budapest,
Hungary
Note: No centre 7 or 11










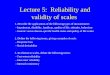



![Guides.chap 01 [001-016]FINAL Guides 5th-min.pdf · Chapter 1 1 1.1 History 1.2 Impairment, Disability, and Handicap 1.3 The Organ System and Whole Body Approach to Impairment 1.4](https://img.pdfslide.us/doc/110x75/5ed97273eb09c069957f64a7/01-001-016final-guides-5th-minpdf-chapter-1-1-11-history-12-impairment-disability.jpg)














