Embed Size (px)
Citation preview

Provided by North American Center forContinuing Medical Education, LLC,
an HMP Communications Holdings Company.
Supported by an educational grant from Shire.
Anthony L. Rostain, MD, MAProfessor of Psychiatry and Pediatrics
Vice Chair for Education, Department of PsychiatryUniversity of Pennsylvania Perelman School of Medicine
Medical Director, Penn Behavioral Health Adult ADHD Treatment & Research Program
Director, Developmental Neuropsychiatry ProgramThe Children’s Hospital of Philadelphia
Philadelphia, Pennsylvania
Faculty
• Dr. Rostain: Book Royalties—Routledge/Taylor Francis Group; Scientific Advisory Board—Shire, Ironshore, Alcobra, Pearson; Consultant—MLB, NFL, SUNY/Upstate (AHRQ grant).
Faculty Disclosures

• The faculty have been informed of their responsibility to disclose to the audience if they will be discussing off-label or investigational use(s) of drugs, products, and/or devices (any use not approved by the US Food and Drug Administration).
– The off-label use of bupropion, tricyclic antidepressants, modafinil, and desipramine combined with methylphenidate for the treatment of ADHD will be discussed.
– The off-label use of mirtazapine and cyproheptadine as an appetite stimulant will be discussed.
– The off-label use of melatonin, clonidine, tricyclic antidepressants, trazodone, mirtazapine, and antihistamines for the treatment of stimulant-induced insomnia will be discussed.
– The off-label use of atomoxetine, α2-adrenergic agonists, and atypical or typical antipsychotics for the treatment of stimulant-exacerbated tics will be discussed.
• Brand names are included in this presentation for participant clarification purposes only. No product promotion should be inferred.
• Applicable CME staff have no relationships to disclose relating to the subject matter of this activity.
• This activity has been independently reviewed for balance.
Disclosure
• Discuss the hallmark features of attention-deficit/hyperactivity disorder (ADHD) in adults, as well as key functional impairments and co-occurring mental health problems that contribute to the clinical and socioeconomic burden
• Describe key steps involved in assessing adults for ADHD incorporating validated screening tools and recent DSM-5criteria
• Differentiate among the current and emerging treatments for adult ADHD in terms of safety, efficacy, duration of activity, and executive function
• Employ evidence-based reasoning in selecting appropriate treatment options for the management of adult patients with ADHD
Learning Objectives
• 19-year-old single white female who first sought help when she was placed on academic probation during her first year at college
• Presenting complaints
– Highly distractible, “spacey”
– Forgetful
– Poor time management, disorganization
– Poor follow through on tasks, overwhelmed
– Very emotional
Case Study: Amanda

• Childhood history
– Outbursts during play with peers
– Parents took responsibility for many tasks (eg, check her assignments, wake her up)
– Learned to read quickly but was a “slow reader”
– Teachers described her as a “daydreamer”
– Diverse examples of immaturity
Case Study: Amanda
• Education history
– Average grades
– Improved status with “extra credit”
– Reliance on other sources to get information missed during lectures
– Required more time to complete tasks
– College – overwhelmed, stopped going to class
• Job history
– Work as waitress – late, forgetful, takes too long to get orders in, however – she is good with customers
– Participated in theater group, internships
Case Study: Amanda
• Medical history – unremarkable
• Substance use history – unremarkable
• Psychiatric history
– Brief counseling in college when she became depressed
Case Study: Amanda

ASRS Symptom Checklist
Inattentive: 33*
Hyper/Imp: 11
Total: 44*
Brown Attention Deficit Disorder Scales
Total T score = 80*
Activation T = 72*
Attention T = 85*
Effort T = 81*
Affect T < 50
Memory T = 85*
Beck Depression Inventory II21*/63 (moderate)
Beck Anxiety Inventory18*/63 (moderate)
Beck Hopelessness Scale13*/20 (moderate)
*Clinically elevated.
Case Study: AmandaInitial Assessment
Pre-Activity Survey
What part of Amanda’s history is most indicative of executive function impairment?
A. Childhood history
B. Education history
C. Job history
D. Psychiatric history
Question 1

If all other explanations are ruled out, what other important information would be helpful to establish a diagnosis of ADHD in this patient?
A. Family psychiatric history
B. Malingering
C. Severity of impairment
D. Transient situational stressors
Question 2
Based on her history and because this class of medication has the best response rate, what pharmacotherapy would you prescribe this patient?
A. Atomoxetine
B. Bupropion
C. Stimulants
D. α2-adrenergic agonists
Question 3
Stimulants may be used in all patients EXCEPT:
A. Patients with bipolar disorder
B. Patients with hypertension
C. Patients with recent myocardial infarction
D. Patients with substance use disorder
Question 4

• ADHD is a valid disorder, most commonly affecting executive functioning and inhibition
• ADHD is found universally
– 7% to 9% of children, 3% to 5% of adults
• ADHD largely results from biological factors
– Genetics, neurology, acquired injuries, and interactions
– 25% to 35% from injuries; 65% to 75% from genetics
• Social factors likely influence degree of impairment, risk for comorbid disorders, and access to resource
Basic Points about Adult ADHD
Froehlich TE, et al. Arch Pediatr Adolesc Med. 2007;161(9):857-864. Kessler RC, et al. Am J Psychiatry. 2006;163(4):716-723. Wilens TE, et al. Postgrad Med. 2010;122(5):97-109.
• ADHD is a complex, heterogeneous neurodevelopmental, lifespan disorder affecting patient, family, and community
– Different trajectories of development
– High degree of overlap with learning difficulties and comorbid psychiatric conditions
– Multiple determinants of clinical course
– Many promising approaches to promoting function/adaptation
• We are still trying to figure out what works for whom and how to combine different paradigms and intervention strategies
Basic Points about Adult ADHD (continued)
Barkley RA (Ed). Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment. New York, NY: Guilford Press; 2015. Ramsay JR, Rostain AL. Cognitive Behavioral Therapy for Adult ADHD: An Integrative Psychosocial and Medical Approach. Second Edition. New York, NY: Routledge Press; 2015.
*According to results from the National Comorbidity Survey Replication in 3199 respondents aged 18 to 44 years.Dulcan M. J Am Acad Child Adolesc Psychiatry. 1997;36(10 Suppl):85S-121S. Kessler RC, et al. Am J Psychiatry. 2006;163(4):716-723.
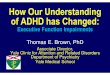
ADHD: A Lifelong Disorder
Estimated prevalence in adult population: 4.4%*
Up to 65% will exhibit symptoms
into adulthood
30%–80% will exhibit symptoms
into adolescence
ADHD in Adolescents
ADHD in Adults
ADHD in Children

PFC = prefrontal cortex.
Tripp G, et al. Neuropharmacology. 2009;57(7-8):579-589.
Summary: Neurobiology of ADHD
Noradrenalin Dopamine Serotonin
Genes
PFC Basal ganglia Cerebellum
NeuralMechanisms
DBH HTR1B DAT1 D4 D5 SER T SNAP-25
BasicProcesses
ADHD
Executive Function
Workingmemory
Behavioralinhibition
Motivation
Delayaversion
Reinforcement
Predominantlyinattentive
Predominantlyhyperactive–impulsive
Combined
Symptoms
Shaw P, et al. Proc Natl Acad Sci U S A. 2007;104(49):19649-19654.
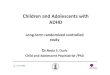
Delayed Cortical Maturation in ADHD
Kaplan–Meier curves illustrating the proportion of cortical points that had attained peak thickness at each age for all cerebral cortical points (Left) and the prefrontal cortex
(Right). The median age by which 50% of cortical points had attained their peak differed significantly between the groups.
0.4
1.0
0.2
Pro
po
rtio
n R
each
ing
Pea
k T
hic
knes
s
0.8
0.6
Age (years)20.00 25.000
All Cortical Points
ADHD
0
Typically Developing
15.005.00 10.00
Group:
Age (years)12.50 15.000
Prefrontal Cortex
10.005.00 7.50
Faraone SV, et al. Nat Rev Dis Primers. 2015;1:15020.
Clinical Progression PathophysiologyEtiology
Frontal–subcortical–cerebellar dysfunction via structural and functional brain abnormalities and downregulation of catecholamine systems that regulate attention, reward, executive control and motor functions
Different genetic risk factors affect the course of ADHD at different stages of the lifespan
Psychosocial influences, chaotic family environments, peer influences and mismatch with school and/or work environments
Inattention persists and hyperactive–impulsive symptoms wane
Substance abuse, low self-esteem and social disability
Behavioral disinhibition, emotional ability and emergence of diagnosis in preschool years
Full expression of ADHD, psychiatric comorbidity, school failure, peer rejection and neurocognitive dysfunction
Sm
oki
ng
in
itia
tio
n
Genetic predisposition
Fetal exposures and epigenetic changes
Prodrome: hyperactivity; and speech, language and motor coordination problems
In utero Adolescence AdulthoodChildhood
Persistence of cortical thickness, default-mode network and white matter tract abnormalities

Faraone SV, et al. Nat Rev Dis Primers. 2015;1:15020.
Childhood Adolescence Adulthood
Health problems and psychiatric comorbidities Psychological dysfunction
Academic and occupational failureSocial disabilityRisky behaviors
Unplanned pregnancies
Accidents and injuries, traffic accidents and violation, and license suspensions
Emotional dysregulation and lack of motivation
Lower quality of life and low self-esteem
Suicidal ideation, suicide attempts and suicide
Poor social skills, impaired family relationships, poor peer relationships and rejection by peers
Disruptive behavior, mood, anxiety, elimination, tic and autism spectrum disorders
Specific learning disabilities and executive dysfunction
Delinquency and criminality, smoking and addictions
Overweight, obesity and hypertension
Premature mortality
Developmental coordination disorder, andspeech and language disorders
Marital discord, separation and divorce, parenting problems, and legal problems, arrests and incarcerations
Underachievement, grade repetition, special education needs, school expulsion and dropping out
Reduced occupational performance, unemployment and lower socioeconomic status
• Behavioral activation difficulties– Disorganization– Poor planning skills
• Information processing problems– Inattention– Distractibility– Poor time management
• Inconsistent effort, follow through– More sensitive to interruption– Slower to resume task once interrupted– Slower processing speed
Adult ADHD: Domains of Impairment
Ramsay JR, Rostain AL. Cognitive Behavioral Therapy for Adult ADHD: An Integrative Psychosocial and Medical Approach. Second Edition. New York, NY: Routledge Press; 2015.
• Restlessness / Impatience / “Delay aversion” • Affect regulation difficulties (Emotional dysregulation)
– Anger, temper outbursts– Anxiety– Emotional lability / instability
• Memory deficits– Forgetfulness– Impaired verbal memory, recall
• Impairments in problem-solving, “synthesis” • Deficient self-control, judgment• Interpersonal (social) problems
Adult ADHD: Domains of Impairment (continued)
Ramsay JR, Rostain AL. Cognitive Behavioral Therapy for Adult ADHD: An Integrative Psychosocial and Medical Approach. Second Edition. New York, NY: Routledge Press; 2015.

Assessment of Adult ADHD
• Thorough and comprehensive – not mere symptom counts
• Include collateral informants when possible
• Obtain historical records when possible
• Attempt to establish childhood onset, chronicity, severity, and pervasiveness of impairment
• Rule outs
ADHD Assessment Principles
Canadian Attention Deficit Hyperactivity Disorder Resource Alliance (CADDRA): Canadian ADHD Practice Guidelines, Third Edition, Toronto ON; CADDRA, 2011. www.caddra.ca/pdfs/caddraGuidelines2011.pdf. Accessed September 8, 2016.
29
1. Is there credible evidence the patient experienced ADHD symptoms in early childhood, and that by middle school (ie, 12 years of age), these led to substantial and chronic impairment across settings?
2. Is there credible evidence that ADHD symptoms currently cause significant impairment across settings?
3. Are there explanations other than ADHD that better account for the clinical picture?
4. For patients who meet criteria for ADHD, is there evidence for the existence of comorbid conditions?
An Adult ADHD Assessment should be able to answer 4 fundamental questions:

• Transient situational stressors (divorce, career change, grief, family/lifestyle changes, etc.)
• Medical conditions (chronic fatigue, thyroid conditions, diabetes, aging/menopause, medication side effects)
• Other psychiatric disorders (bipolar, substance abuse, depression, anxiety disorders, personality disorders)
• Malingering
Ruling Out Alternative Explanations for ADHD Symptoms
Canadian Attention Deficit Hyperactivity Disorder Resource Alliance (CADDRA): Canadian ADHD Practice Guidelines, Third Edition, Toronto ON; CADDRA, 2011. www.caddra.ca/pdfs/caddraGuidelines2011.pdf. Accessed September 8, 2016.
• Mood disorders
– Recurrent depression
– Bipolar disorder
– Cyclothymia
– Dysthymia
– Depressive disorder NOS
• Anxiety disorders
– Generalized anxiety
– Anxiety disorder NOS
• Substance use disorders
• Learning disabilities
• Intermittent explosive disorder
• Tourette syndrome
• Antisocial personality
• Borderline personality
• Dependent personality
NOS = not otherwise specified.
Barkley RA (Ed). Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment. New York, NY: Guilford Press; 2015. Ramsay JR, Rostain AL. Cognitive Behavioral Therapy for Adult ADHD: An Integrative Psychosocial and Medical Approach. Second Edition. New York, NY: Routledge Press; 2015.
Psychiatric Comorbidity in Adult ADHD
• Head injury (traumatic brain injury) – including mild concussions, repetitive injuries
• Sleep apnea• Chronic obstructive
pulmonary disease• Anoxic encephalopathy• Mild cognitive impairment• Dementia• Delirium
• Hypothyroidism
• Hyperthyroidism
• Renal insufficiency
• Hepatic insufficiency
• Vitamin deficient states
• Iron deficiency
• Lead poisoning
• Medication induced
Barkley RA (Ed). Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment. New York, NY: Guilford Press; 2015. Ramsay JR, Rostain AL. Cognitive Behavioral Therapy for Adult ADHD: An Integrative Psychosocial and Medical Approach. Second Edition. New York, NY: Routledge Press; 2015.
Medical Comorbidity in Adult ADHD

• Determine the specific current ADHD symptoms
• Determine presence of ADHD in childhood
• Determine level of daily impairments in multiple life domains
• Assess family psychiatric history
• Assess for history of and concurrent psychiatric comorbidities
• Assess medical history and current medications
• Evaluate risks for the use of ADHD medications
Components of ADHD Diagnostic Evaluation
Barkley RA (Ed). Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment. New York, NY: Guilford Press; 2015. Ramsay JR, Rostain AL. Cognitive Behavioral Therapy for Adult ADHD: An Integrative Psychosocial and Medical Approach. Second Edition. New York, NY: Routledge Press; 2015.
• DSM-5 diagnosis of ADHD
– 4 key elements
• Current symptoms: 5/9 inattentive and/or 5/9 hyperactive-impulsive persistent for at least 6 months
• Impairment in multiple settings
• Childhood onset before age 12
• Symptoms not better accounted for by another mental health disorder
Assessment Methodology
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Fifth Edition. Arlington, VA: American Psychiatric Publishing, Inc.; 2013.
• Symptom assessment is important, but chronicity, pervasiveness, and impairment are critical to diagnosis
• Clear evidence of clinically significant impairment in social, academic, or occupational functioning
• Symptoms not accounted for by another mental disorder (eg, pervasive developmental disorder, schizophrenia,mood disorder, anxiety disorder, dissociative disorder, or a personality disorder)
• Autism spectrum disorder can be a comorbid condition
Clinical Diagnosis of DSM-5 ADHD
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Fifth Edition. Arlington, VA: American Psychiatric Publishing, Inc.; 2013.

• WHO Adult ADHD Self-Report Scale (ASRS)
– Self questionnaire, adapted for adults
• Validated
• User friendly; multiple languages
• Free, downloadable
• Screener: Part A, 6 items
– Positive if ≥ 4 items checked in gray zones
• Part B: 12 items
Screening for ADHD in Adults
WHO = World Health Organization.Harvard Medical School. www.hcp.med.harvard.edu/ncs/asrs.php. Accessed September 8, 2016.
WHO ASRS ScreenerInattention Never Rarely Sometimes Often
Very Often
1. How often do you have trouble wrapping up the fine details of a project once the challenging parts have been done?
0 1 2* 3* 4*
2. How often do you have difficulty getting things in order when you have to do a task that requires organization?
0 1 2* 3* 4*
3. When you have a task that requires a lot of thought, how often do you avoid or delay getting started?
0 1 2 3* 4*
4. How often do you have problems remembering appointments or obligations?
0 1 2* 3* 4*
Hyperactivity-Impulsivity Never Rarely Sometimes OftenVery Often
5. How often do you fidget or squirm with your hands or your feet when you have to sit down for a long time?
0 1 2 3* 4*
6. How often do you feel overly active and compelled to do things, like you were driven by a motor?
0 1 2 3* 4*
• Presenting problems
• Childhood history of ADHD symptoms
• Education / Job history
• Medical history (esp. neurologic and cardiac function)
• Family history (especially learning and school problems, disorganization, impulse control problems, substance and alcohol abuse, and “personality disorders”)
• Comorbid conditions
• Corroborative information
Clinical Interview

• Intense frustration
• Demoralization
• Learned helplessness
• Trouble finishing tasks
• Underachievement
• Feeling chronically misunderstood
• “I would if I could, but I can’t.”
Internal Experience of Adult ADHD
• Conners’ Adult ADHD Rating Scale (CAARS)• Barkley Current and Childhood Symptom Scales
– (includes self and “other” measures)• Barkley Adult ADHD Rating Scale–IV (BAARS-IV)• ADHD Rating Scale IV with Adult Prompts (ADHD-RS-IV)• Brown Attention Deficit Disorder Scale (BADDS) • Wender-Utah Rating Scale (WURS)--------------------------------------------------------------------• Barkley Deficits in Executive Functioning Scale (BDEFS)• Weiss Functional Impairment Rating Scale (WFIRS) • Mood and Anxiety Scales (eg, BDI, BAI, BHS)• Personality Measures (eg, NEO-PI)
Clinical Rating Scales
BDI = Beck Depression Inventory; BAI = Beck Anxiety Inventory; BHS = Beck Hopelessness Scale; NEO-PI = NEO Personality Inventory.
• Differential Diagnosis
• Problem List
• Case Conceptualization
– Readiness for Treatment (Stages of Change)
– Patient Preferences and Priorities
• Treatment Planning
Putting It All Together

• Review findings and diagnostic impression
• Educate about both ADHD and comorbid disorders
• Consider both protective and risk factors
• Elicit patient preferences and priorities
• Emphasize need for multimodal approach
• Help patient to get ready to take next steps
Treatment Planning
Pliszka S; AACAP Work Group on Quality Issues. J Am Acad Child Adolesc Psychiatry. 2007;46(7):894-921. Murphy K. J Clin Psychol. 2005;61(5):607-619.
Dulcan M. J Am Acad Child Adolesc Psychiatry. 1997;36(10 Suppl):85S-121S.
Treatment Modalities for ADHD
Medical Interventions
Educational / Workplace Interventions
Psychosocial Interventions
• Psycho-educational session – present findings, treatment options
• Self-education RE: ADHD (books, videos, DVDs, online resources)
• Environmental restructuring• Coaching (life skills, organization, time management)• Problem-focused support groups• Medications• CBT / Supportive psychotherapy / Insight-oriented therapy• Social skills groups • Vocational counseling
Multimodal Treatment Approach
CBT = cognitive-behavioral therapy.

• Met diagnostic criteria for ADHD, Inattentive presentation and Unspecified Depressive Disorder
• Assigned Amanda task of visiting Web sites (NIMH, CHADD), reading up on ADHD, and reporting back on what she learned
• Conducted a psychoeducational session reviewing diagnosis and treatment options
• Elicited patient’s preferences for treatment
• Treatment recommended:
– CBT
– Pharmacotherapy – lisdexamfetamine 30 mg – duration sufficient to help her focus better at work where she is struggling
Case Study: Amanda
Principles of Pharmacotherapy of Adult ADHD (Brief Review)
Arnsten AF, et al. J Am Acad Child Adolesc Psychiatry. 2012;51(4):356-367.
Regulation of Attention and Emotion

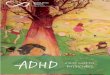
Arnsten AF. J Pediatr. 2009;154(5):I-S43.
The Prefrontal Cortex Requires a Proper Level of Catecholamines for Optimal Function
Increasing Levels of Catecholamine Release
Drowsy Alert Stressed
Unguided attention / responsesDistracted, poor impulse control
(eg, Untreated ADHD)
Misguided attention / responsesMental inflexibility, stimulus bound(eg, Excessive dose of stimulant)
Guided attention and responsesFocused, organized and flexible
(eg, Optimally treated ADHD)
NE 2A
Moderate D1
Too little2A/D1
NE 1, 1
Excess D1
Shaw M, et al. BMC Med. 2012;10:99.
Treatment Benefit by Outcome Group Compared with Untreated ADHD
No Benefit
Benefit
100
10
0
Ou
tco
mes
in
Eac
h O
utc
om
e G
rou
p (
%)
70
30
20
90
50
60
80
40
Outcome Groups
LA = long-acting.Faraone SV. Understanding the Effect Size of ADHD Medications: Implications for Clinical Care. September 18, 2003. www.medscape.com/viewarticle/461543_5. Accessed September 8, 2016.
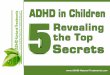
Effect Size for Classes of ADHD Medications
Eff
ect
Siz
e
Nonstimulant Stimulant LA StimulantClass of Medication
Represents the mean effect size for each class of medication.
P <.05 for stimulants vs nonstimulants.
3
2
1
0
-1

Wilens TE, et al. Postgrad Med. 2010;122(5):97-109. Stevens JR, et al. In: Adler LA, et al (Eds). Attention-Deficit Disorder in Adults and Children. Cambridge University Press: Cambridge, UK; 2015:245-258.
Pharmacologic Treatments Approved for ADHDAmphetamine-based Formulations Duration of Effect Peds/Adult
Adderall® (mixed amphetamine salts) 4-6 hours -/-
Adderall XR® (mixed amphetamine salts XR) ~12 hours +/+
Dexedrine® Spansule (dextroamphetamine) 6-8 hours +/-
VyvanseTM (lisdexamfetamine) ~12 hours +/+
Methylphenidate-based Formulations
Concerta® (MPH) ~12 hours +/+
Daytrana® (MPH patch) ~12 hours (worn for 9) +/-
Focalin® (dexMPH capsule) ~5 hours +/-
Focalin® XR (dexMPH XR capsule) 10-12 hours +/+
Metadate® CD (MPH controlled-release capsule) 8-10 hours +/-
Ritalin® (MPH) ~4 hours +/-
Ritalin® LA (MPH XR capsule) 8-10 hours +/-
Quillivant XRTM (MPH XR liquid) ~12 hours +/-
Nonstimulants
Strattera® (atomoxetine) 8-24 hours +/+
Intuniv® (guanfacine XR) ~12 hours +/-
Kapvay® (clonidine XR) ~12 hours +/-
• Aptensio-XR® (MPH extended-release capsules): approved for ages ≥ 6 (no adult studies available)
• Evekeo® (AMPH sulphate): 5 and 10 mg tablets
• Adzenys XR-ODT™ (AMPH extended-release orally disintegrating tablet)
• Several other new options for treatment of ADHD thought to be arriving soon
Recent FDA Approvals in ADHD
AMPH = amphetamine; MPH = methylphenidate.
US Food and Drug Administration. www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm.
Developed for children and adolescents.
Pliszka SR, et al. J Am Acad Child Adolesc Psychiatry. 2006;45(6):642-657.
ADHD Treatment Algorithm
0. Assessment/family consultation/treatment planning
1. MPH or AMPH
2. Stimulant not used in Step 1
3. Atomoxetine
4. Bupropion or tricyclic antidepressants
5. Agent not used in Step 4
6. α2-adrenergic agonist
Non-medtreatments
1a. AMPHnot used in Step 1
2a. AMPHnot used in Step 2
3a. Combine atomoxetine and stimulant
Consultation

• Stimulants [MPH, AMPH]
• Atomoxetine
• Bupropion*
• α2-adrenergic agonists
• Tricyclic antidepressants*
• Modafinil*
Medications
*The use of bupropion, tricyclic antidepressants, and modafinil for the treatment of ADHD is off-label.
• Stimulants: 75% – 85%
– Of responders, 1/3 do better on MPH, 1/3 do better on AMPH, and 1/3 do equally well on MPH or AMPH
• Atomoxetine: 65% – 70%
– Different mechanism of action may be beneficial or may be seen as not as effective for those used to stimulants
– Combination with stimulants is safe, but should be closely monitored
• Bupropion: 65% – 75%
– Not as well studied as other agents
Overall Response Rates for Pharmacotherapy
Rostain AL. Postgrad Med. 2008;120(3):27-38. Wilens TE, et al. Expert Rev Neurother. 2011;11(10):1443-1465. Maneeton N, et al. Psychiatry Clin Neurosci. 2011;65(7):611-617.
• Assess response and tolerability separately
– If mild side effects (eg, insomnia, low appetite, tension) consider switch to similar class stimulant or alternate stimulant
– If partial/lack response, consider alternate stimulant
– If moderate or greater side effects or lack of response to both stimulant classes, consider trial of nonstimulant
• Also, if relative contraindication is present, eg, active substance abuse
Clinical Prescribing: Tolerability
Rostain AL. Postgrad Med. 2008;120(3):27-38. Wilens TE, et al. Expert Rev Neurother. 2011;11(10):1443-1465. Prince JB, et al. In: Barkley RA (Ed). Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment. New York, NY: Guilford Press; 2015.

• Stimulants [MPH, AMPH]
• Atomoxetine
• Bupropion
• α2-adrenergic agonists
• Tricyclic antidepressants
• Modafinil
Medications
• Psychostimulants first-line agents
– Multiple FDA approved agents (adult)
• Long-acting preparations preferable
– Better adherence, treat through the day
– Minimize potential for misuse or abuse
• May be useful to orient according to weight
– eg, 1–1.5 mg/kg/day MPH ~ 70–100 mg/day;
– 0.5–1.0 mg/kg/day MAS
First-Line Pharmacotherapy
MAS = mixed amphetamine salts.
Canadian Attention Deficit Hyperactivity Disorder Resource Alliance (CADDRA): Canadian ADHD Practice Guidelines, Third Edition, Toronto ON; CADDRA, 2011. www.caddra.ca/pdfs/caddraGuidelines2011.pdf. Accessed September 8, 2016.
• Trust your patient – if you are concerned about potential substance abuse or misuse do not prescribe stimulants
• Explain the principle of a “medication trial” and the need for patient to keep a medication response log
• Up to 30% of patients respond better to either AMPH or MPH, while 30% respond equally well to both
• Start with MPH at varying doses – once the optimal dose is determined, can adjust the schedule with longer acting preparations
• If MPH is not optimally effective, switch to AMPH and determine responses to variable doses
Psychostimulant Use Guidelines
Daughton J, et al. In: Martin A, et al (Eds). Pediatric Psychopharmacology: Principles and Practice. Second Edition. New York, NY: Oxford Press; 2011. Prince JB, et al. In: Barkley RA (Ed). Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment. New York, NY: Guilford Press; 2015.

• Adverse effects are generally well tolerated
– Reduced appetite and consequent weight loss
– Abdominal pain, nausea, constipation
– Difficulty falling asleep
– Mild increase in heart rate and blood pressure
– Jitteriness, jumpiness
– Motor tics
– Dysphoria, moodiness, irritability
– Rebound effects
Psychostimulants: Overview
Pliszka SR. J Am Acad Child Adolesc Psychiatry. 2006;46(7):894-921. Daughton J, et al. In: Martin A, et al (Eds). Pediatric Psychopharmacology: Principles and Practice. Second Edition. New York, NY: Oxford Press; 2011.
• Some patients report a need for additional medication at specific times
– Stimulant dose may be increased when there is a need for increased focus
– Patients who need evening treatment may benefit from
• Combination of extended-release and immediate-release stimulant
• Atomoxetine or a combination of atomoxetine and a daytime stimulant
Adjusting Medication
Adler LA, et al. Curr Psychiatry Rep. 2006;8(5):409-415. Hazell P. CNS Drugs. 2007;21(1):37-46.
Extended-release stimulants, lisdexamfetamine, MPH transdermal system
Atomoxetine, bupropion, tricyclic antidepressant
0800 1200 1600 2000 2400Time (h)
Combination treatment: long-acting stimulant and nonstimulant
Long-acting stimulant Immediate-release stimulant
Morning Evening
Stimulants may be prescribed in combination with a nonstimulant to ensure coverage into the evening
Long-acting stimulant
Long-acting stimulant (1/2 AM dose)
Adapted from Hazell P. CNS Drugs. 2007;21(1):37-46.
Medication Dosing Options

• Dietary caffeine: recommend decrease in consumption to avoid over-stimulation
• Nicotine: similar caution
• Alcohol: no toxic interactions seen at moderate doses, but normal response to alcohol may be altered
• Decongestants (eg, pseudoephedrine): should reduce dosage or stop stimulant for duration of use
• Diet: should be adjusted to avoid significant weight loss [ie, this is not a good diet drug!]
Psychostimulants: Other Issues
Managing Common Side Effects
• Patience
• Usually improves after a few days
• Eat a big breakfast and dinner
• Absorption ?
• Adjust timing of medication
• Adjust timing of meals
• Encourage snacks (including bedtime)
• Consider changing dose, regimen, or medication
Managing Common Side Effects: Appetite Loss
Pliszka SR. J Am Acad Child Adolesc Psychiatry. 2006;46(7):894-921. Daughton J, et al. In: Martin A, et al (Eds). Pediatric Psychopharmacology: Principles and Practice. Second Edition. New York, NY: Oxford Press; 2011.

• For stimulant-induced insomnia
– Melatonin
– Clonidine
– Tricyclic antidepressant
– Trazodone
– Mirtazapine
– Antihistamine (acutely)
Managing Common Side Effects: Insomnia
The use of these medications for this indication is off-label.
Pliszka S; AACAP Work Group on Quality Issues. J Am Acad Child Adolesc Psychiatry. 2007;46(7):894-921. Weiss MD, et al. J Am Acad Child Adolesc Psychiatry. 2006;45(5):512-519. Tjon Pian Gi CV, et al. Eur J Pediatr. 2003;162(7-8):554-555. Kratochvil CJ, et al. J Am Acad Child AdolescPsychiatry. 2005;44(5):499-501.
• Direct vs indirect effect
– Medication vs hunger
– Determine time of day
• Patience
– Often resolve after the first few days of treatment
• Lower daily dose
• Try a different medication
Managing Common Side Effects: Stomachaches
• Stimulant-exacerbated tics
– Examine severity of tics
– Re-challenge to examine if tics are stimulant-induced
– Switch to atomoxetine, α2-adrenergic agonists, or atypical or typical antipsychotics (pimozide – FDA approved)
– Combination therapies
• Atomoxetine plus stimulant
• Clonidine plus methylphenidate (3 studies)
• Atypical plus other treatment
Managing Common Side Effects: Tics
The use of these medications for this indication is off-label.
Pliszka S; AACAP Work Group on Quality Issues. J Am Acad Child Adolesc Psychiatry. 2007;46(7):894-921. Palumbo DR, et al. J Am Acad Child Adolesc Psychiatry. 2008;47(2):180-188. Hazell PL, et al. J Am Acad Child Adolesc Psychiatry. 2003;42(8):886-94. The Tourette’s Syndrome Study Group. Neurology. 2002;58(4):527-536.

Health and Safety Concerns
• Current FDA language stipulates that sudden death can occur at usual doses in patients with a pre-existing structural cardiac abnormality or other serious heart problem
• Careful history of heart-related problems must be obtained and documented before starting stimulant medication
Recent Concerns about Stimulants and Cardiac Disease
Important screening questions:
• Patient-related factors: history of murmur, syncope, or other CVD illness
• Family-related factors: history of early or sudden cardiac death
• Other health considerations that increase CVD risk
– Smoking history, caffeine use, over-the-counter sympathomimetic medications
• If cardiac screening is negative, EKG is NOT required prior to initiating treatment
Screening Adults with ADHD for Cardiovascular Safety
CVD = cardiovascular disease; EKG = electrocardiogram.

• Spontaneous syncope
• Exercise-induced syncope
• Exercise-induced chest pain
• Sudden death in family member under age 30
• History of cardiac abnormalities (structural or electrical) in self or family members
• EKGs are not routinely required
Clinical Assessment of Cardiac Risk
Cava JR, et al. Pediatr Clin N Am. 2004;51(5):1401-1420. Paterick TE, et al. JAMA. 2005;294(23):3011-3018.
• Possible causes for concern– History of palpitations or arrhythmia– Recent myocardial infarction– Syncopal episodes, dizziness– Multiple risk factors, such as smoking, high body mass
index, hypertension, metabolic syndrome• Maximize cardiac medications and address risk factors;
patients with ADHD may find it difficult to make necessary lifestyle changes
• Introduce ADHD medication at a low dose and titrate up slowly
• Monitor symptoms, blood pressure/heart rate regularly• Longer term effects of ADHD medications on cardiovascular
status unclear
Treating ADHD Patients with Heart Disease
Gutgesell H, et al. Circulation. 1999;99(7):979-982.
• Evaluate blood pressure/pulse prior to initiating ADHD treatment
• Address hypertension before treating ADHD
• Once hypertension is controlled, treat ADHD and monitor blood pressure
• Stimulants have a clinically insignificant effect on blood pressure in treated, normotensive adults
Treating ADHD Patients with Hypertension
Wilens TE, et al. J Clin Psychiatry. 2006;67(5):696-702. Pliszka S; AACAP Work Group on Quality Issues. J Am Acad Child Adolesc Psychiatry. 2007;46(7):894-921. Nutt DJ, et al. J Psychopharmacol. 2007;21(1):10-41. Canadian Attention Deficit Hyperactivity Disorder Resource Alliance (CADDRA): Canadian ADHD Practice Guidelines, Third Edition, Toronto ON; CADDRA, 2011. www.caddra.ca/pdfs/caddraGuidelines2011.pdf. Accessed September 8, 2016.

Stimulant Misuse/Abuse/Addiction
• Diversion behaviors: selling, forging, stealing prescriptions
• Past or current abuse of other substances
• Non-adherent behaviors, including escalation of usage despite warnings
• Injecting oral formulations
• Losing and seeking prescriptions from multiple clinicians
• Showing signs of declining social functioning
Signs and Symptoms of Prescription Drug Misuse/Abuse
Kollins SH. J Atten Disord. 2008;12(2):115-125. Harstad E, et al. Pediatrics. 2014;134(1):e293-e301. Wilens TE, et al. Curr Psychiatry Rep. 2007;9(5):408-414.
• Make an accurate diagnosis of ADHD
• Evaluate patients for risk of medication misuse
• Rule out faking or simulation of ADHD symptoms
• Choose most appropriate treatment given clinical circumstances
• Educate patient and family about their responsibility for avoiding misuse of medication
• Use consent forms to document these discussions
• Record your actions and patient’s responses in the medical record
Clinical Strategies
Kollins SH. J Atten Disord. 2008;12(2):115-125. Harstad E, et al. Pediatrics. 2014;134(1):e293-e301. Wilens TE, et al. Curr Psychiatry Rep. 2007;9(5):408-414.

• Atomoxetine
• α2-adrenergic agonists
– Guanfacine
– Clonidine
• Bupropion
• Tricyclic antidepressants
• Nicotinic agonists
• Methylphenidate
– Long-acting
– Transdermal patch
• Lisdexamfetamine
• Modafinil
• Amphetamine
– Long-acting
NONSTIMULANTS STIMULANTS
SUD = substance use disorder.
Kollins SH. J Atten Disord. 2008;12(2):115-125. Harstad E, et al. Pediatrics. 2014;134(1):e293-e301. Wilens TE, et al. Curr Psychiatry Rep. 2007;9(5):408-414.
Pharmacologic Treatments for ADHD with Suspected or Proven Comorbid SUD
• Consider nonstimulants for high risk, current/recent substance abusers; those with histories of diversion or misuse of stimulants
• Introduce non-pharmacologic approaches
• CBT, cognitive-remediation, self-help, group and individual psychotherapy
• Family therapy for adolescents and young adults
Clinical Strategies
Kollins SH. J Atten Disord. 2008;12(2):115-125. Harstad E, et al. Pediatrics. 2014;134(1):e293-e301. Wilens TE, et al. Curr Psychiatry Rep. 2007;9(5):408-414.
• Keep track of pills and refills
• Use extended-release formulations
• Obtain urine toxicology frequently
• Discuss safe storage and not sharing medications
• Pre-discuss “renewal” guidelines
– Use of 14- or 30-day Rx
– “Lost prescriptions”
• State/Commonwealth Web sites tracking patient controlled substance administration
Clinical Strategies
Kollins SH. J Atten Disord. 2008;12(2):115-125. Harstad E, et al. Pediatrics. 2014;134(1):e293-e301. Wilens TE, et al. Curr Psychiatry Rep. 2007;9(5):408-414.

• Red Flags
– Demand for immediate-release stimulants
– Repeatedly discordant pill counts
– Frequently lost prescriptions
– Requests to increase dosage
– Signs of stimulant toxicity
Clinical Strategies
Kollins SH. J Atten Disord. 2008;12(2):115-125. Harstad E, et al. Pediatrics. 2014;134(1):e293-e301. Wilens TE, et al. Curr Psychiatry Rep. 2007;9(5):408-414.
• Stimulants
• Atomoxetine
• Bupropion
• α2-adrenergic agonists
• Tricyclic antidepressants
• Modafinil
Medications
• Posterior Attention System
– Increased NE
• Improved alerting and orienting
• Reduced “startle” and over-reactivity
• Anterior Attention System
– Increased NE and DA
• Improved focusing
• Improved executive functioning
Atomoxetine: Mechanism of Action
DA = dopamine; NE = norepinephrine.
Bymaster FP, et al. Neuropsychopharmacology. 2002;27(5):699-711. Arnsten AF, et al. PharmacolBiochem Behav. 2011;99(2):211-216.

• Downstream increase in DA activity in the prefrontal cortex
– Consistent with improved executive functioning
• No increase in DA activity in the nucleus accumbens
– Not associated with abuse liability
• No increase in DA in the striatum
– Not associated with motor activity (tics)
Atomoxetine: Effects on Dopamine
Bymaster FP, et al. Neuropsychopharmacology. 2002;27(5):699-711. Arnsten AF, et al. PharmacolBiochem Behav. 2011;99(2):211-216.
• Dizziness, high blood pressure
• Headache, irritability, nervousness
• Abdominal pain, nausea, vomiting, loss of appetite, weight loss
• Dry mouth, constipation, urinary hesitancy
• Decreased sexual desire
• Very slight chance of hepatic insufficiency
Atomoxetine: Side Effects
US Food and Drug Administration. www.accessdata.fda.gov/scripts/cder/drugsatfda/. Michelson D, et al. Biol Psychiatry. 2003;53(2):112-120.
• Stimulants
• Atomoxetine
• Bupropion
• α2-adrenergic agonists
• Tricyclic antidepressants
• Modafinil
Medications

• DA (and NE) reuptake blocker
• Similar to phenylethylamine (aminoketone)
• Hydroxylated metabolite is active agent
• Half-life = 14 hours
• Generally activating or even stimulating
• Less sexual dysfunction than other antidepressants
Bupropion: Mechanism of Action
US Food and Drug Administration. www.accessdata.fda.gov/scripts/cder/drugsatfda/. Prince JB, et al. In: Barkley RA (Ed). Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment. New York, NY: Guilford Press; 2015. Maneeton N, et al. Psychiatry Clin Neurosci. 2011;65(7):611-617.
• Dry mouth, constipation, nausea, vomiting
• Anorexia, weight loss
• Headache, dizziness, fainting spells
• Increased incidence of seizures (0.4%)
• Insomnia, tremor, restlessness, excitability
• Mood swings, irritability
Bupropion: Side Effects
US Food and Drug Administration. www.accessdata.fda.gov/scripts/cder/drugsatfda/. Prince JB, et al. In: Barkley RA (Ed). Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment. New York, NY: Guilford Press; 2015. Maneeton N, et al. Psychiatry Clin Neurosci. 2011;65(7):611-617.
• Stimulants
• Atomoxetine
• Bupropion
• α2-adrenergic agonists
• Tricyclic antidepressants
• Modafinil
Medications

• Mechanism of action: partial agonist of NE
• Decreases erratic activity of locus coeruleus
• Increases neurotransmission in prefrontal cortex
• First introduced as anti-hypertensive agents
• Helpful for patients who are highly aroused, impulsive, emotionally labile, irritable and explosive
• Reduces anxiety, defiance, and aggression
• Useful in controlling tics
α2-Adrenergic Agonists(Clonidine, Guanfacine)
US Food and Drug Administration. www.accessdata.fda.gov/scripts/cder/drugsatfda/. Newcorn JH, et al. In: Martin A, et al (Eds). Pediatric Psychopharmacology: Principles and Practice. Second Edition. New York, NY: Oxford Press; 2011. Prince JB, et al. In: Barkley RA (Ed). Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment. New York, NY: Guilford Press; 2015.
• Sedation, fatigue
• Dizziness
• Dry mouth, indigestion, nausea
• Nightmares, insomnia
• Anxiety, depression
• Hypertensive crisis with sudden discontinuation
α2-Adrenergic Agonists: Side Effects(Clonidine, Guanfacine)
US Food and Drug Administration. www.accessdata.fda.gov/scripts/cder/drugsatfda/. Newcorn JH, et al. In: Martin A, et al (Eds). Pediatric Psychopharmacology: Principles and Practice. Second Edition. New York, NY: Oxford Press; 2011. Prince JB, et al. In: Barkley RA (Ed). Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment. New York, NY: Guilford Press; 2015.
• Start with ½ tablet at bedtime (0.05 mg clonidine, 0.5 mg guanfacine)
• Add ½ tablet in the morning as tolerated (5–15 days)
• Continue incremental increases by ½ tablet q weekly
• Titrate upwards as tolerated to maximum of 0.4/4 mg daily
• Extended-release preparation is approved for children and adolescents; need to increase dose by 33%
α2-Adrenergic Agonists: Dosing(Clonidine, Guanfacine)
US Food and Drug Administration. www.accessdata.fda.gov/scripts/cder/drugsatfda/. Newcorn JH, et al. In: Martin A, et al (Eds). Pediatric Psychopharmacology: Principles and Practice. Second Edition. New York, NY: Oxford Press; 2011. Prince JB, et al. In: Barkley RA (Ed). Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment. New York, NY: Guilford Press; 2015.

• Stimulants
• Atomoxetine
• Bupropion
• α2-adrenergic agonists
• Tricyclic antidepressants
• Modafinil
Medications
Prince JB, et al. In: Barkley RA (Ed). Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment. New York, NY: Guilford Press; 2015.
• Stimulants may be combined with atomoxetine when patients do not respond adequately to either medication alone
• Clinical trials have been conducted on the following combination therapies:
– Atomoxetine and MPH
– Clonidine and MPH
– Guanfacine and MPH
– Desipramine and MPH
Combining Agents
The use of desipramine combined with MPH for the treatment of ADHD is off-label.
Wilens TE, et al. Presented at: 159th Annual Meeting of the American Psychiatric Association; May 2006; Toronto, Canada. Palumbo DR, et al. J Am Acad Child Adolesc Psychiatry. 2008;47(2):180-188. Hazell PL, et al. J Am Acad Child Adolesc Psychiatry. 2003;42(8):886-94. The Tourette’s Syndrome Study Group. Neurology. 2002;58(4):527-536. Cohen LG, et al. Pharmacotherapy. 1999;19(6):746-752. Rapport MD, et al. J Am Acad Child Adolesc Psychiatry. 1993;32(2):333-342.
• With adult patients, medication may lead to remission of symptoms, but functional impairment remains
– Medication effects may vary from time to time, and from setting to setting
– Patients may still lack organizational skills, social skills, academic and workplace skills; their adaptive behavior remains a problem
Functional Remission
Gibbins C, et al. Curr Psychiatry Rep. 2007;9(5):420-426.

• Newly diagnosed patients may take 2 to 3 months to be stabilized on medication
• Adjust the dose or consider switching medications
• Ensure that comorbid conditions are treated
• Try combination treatment
• Manage side effects
• Reconsider the diagnosis and possible presence of confounding comorbid psychiatric conditions
Managing Inadequate Response
Pliszka S; AACAP Work Group on Quality Issues. J Am Acad Child Adolesc Psychiatry. 2007;46(7):894-921.
• “It’s a magic pill – it will cure all my problems”
• “It’s bad to be dependent on medications – I’m like a drug addict”
• “If I do better, it’s not me doing it.”
• “If I don’t do better, it’s the medication’s fault.”
• “It’s all in the meds, there’s nothing I can do.”
Distorted Beliefs about Medications
• Patient was very adherent with treatment
– Came regularly to CBT sessions and was engaged in therapy
– Took medication as prescribed – needed higher dose to maintain symptom remission (50 mg)
– Started to work part-time in order to take courses at community college – got excellent grades
– Reapplied and was accepted back to a 4-year college
• Family very pleased with outcomes
Case Study: AmandaTreatment Outcome

ASRS Symptom Checklist
Inattentive: 16 (33)
Hyper/Imp: 4 (11)
Total: 20 (44)
Brown Attention Deficit Disorder Scales
Total T = 50 80*
Activation T = 51 72*
Attention T = 53 85*
Effort T < 50 81*
Affect T < 50 < 50
Memory T = 58 85*
Beck Depression Inventory II
7 (minimal) 21/63 (moderate)
Beck Anxiety Inventory
7 (minimal) 18/63 (moderate)
Beck Hopelessness Scale
2 (minimal) 13/20 (moderate)
*Clinically elevated.
Case Study: AmandaTreatment Outcome
• Depression
– Active depression should be controlled first
• Bupropion and duloxetine often improve ADHD symptoms
– When depression stabilized, add ADHD medications
• Stimulants can have adjuvant effect to antidepressants
• Atomoxetine titration should be slowed (½ target dose) if added to SNRI, fluoxetine, or paroxetine
– Dysthymia may respond to ADHD medications alone without need for antidepressant
Managing Comorbidities
SNRI = serotonin-norepinephrine reuptake inhibitor.Pliszka SR, et al. J Am Acad Child Adolesc Psychiatry. 2006;45(6):642-657. Goodman DW, et al. Postgrad Med. 2009;121(5):20-30.
Bond DJ, et al. Ann Clin Psychiatry. 2012;24(1):23-37. Goodman DW, et al. Postgrad Med. 2009;121(5):20-30.
Treatment Recommendations for the Management of ADHD in Adults with MDD + ADHD
Lines of Evidence Treatment Recommendation
First-Line Bupropion, Antidepressant + Extended Delivery Stimulant;Antidepressant + CBT
Second-Line Venlafaxine, Nortriptyline, Desipramine
Third-Line Antidepressant + Short-Acting Stimulant, Antidepressant + Atomoxetine, Antidepressant + Lisdexamfetamine

• Bipolar Disorder – Mood stability is primary – ADHD medications can be trialed if impairing
symptoms persist despite mood stabilizer therapy• Bupropion• Low-dose atomoxetine• Low-dose stimulants• Modafinil• Tricyclic antidepressants
– Begin low and titrate ADHD medications cautiously– Follow closely. All ADHD medications can induce
switches or rapid cycling
Managing Comorbidities
Wilens TE, et al. Biol Psychiatry. 2003;54(1):9-16. Goodman DW, et al. Postgrad Med. 2009;121(5):20-30. Chang K, et al. J Child Adolesc Psychopharmacol. 2009;19(5):547-551.
Bond DJ, et al. Ann Clin Psychiatry. 2012;24(1):23-37. Goodman DW, et al. Postgrad Med. 2009;121(5):20-30.
Treatment Recommendations for the Management of ADHD in Adults with BD + ADHD
Lines of Evidence Treatment Recommendation
First-Line Bupropion
Second-Line MAS, MPH, Modafinil, CBT
Third-Line Atomoxetine, Venlafaxine, Nortriptyline, Desipramine,Lisdexamfetamine
• ADHD in adults is highly impairing and often associated with major psychiatric and medical comorbidities
• Assessing adults for ADHD includes use of standardized screening tools, self-report scales, and diagnostic interview schedule. Diagnosis requires symptom counts, pervasiveness of symptoms, and impairment as well as evidence of difficulties dating back to early adolescence
• Multimodal treatment is the most appropriate approach to intervention. Medications are most effective when combined with educational/workplace interventions and psychosocial approaches
• Stimulant and nonstimulant medications have shown promise in relieving the symptoms and reducing impairments in adults with ADHD
Key Points

Post-Activity Survey
What part of Amanda’s history is most indicative of executive function impairment?
A. Childhood history
B. Education history
C. Job history
D. Psychiatric history
Question 1
If all other explanations are ruled out, what other important information would be helpful to establish a diagnosis of ADHD in this patient?
A. Family psychiatric history
B. Malingering
C. Severity of impairment
D. Transient situational stressors
Question 2

Based on her history and because this class of medication has the best response rate, what pharmacotherapy would you prescribe this patient?
A. Atomoxetine
B. Bupropion
C. Stimulants
D. α2-adrenergic agonists
Question 3
Stimulants may be used in all patients EXCEPT:
A. Patients with bipolar disorder
B. Patients with hypertension
C. Patients with recent myocardial infarction
D. Patients with substance use disorder
Question 4
Q&A