Embed Size (px)
Citation preview
n e va d a
HeaLTH PLan ReFeRenCe GUIdeFor Brokers
Group Health, dental & vision
Word & Brown simpli�es Large Group sales and service.
• One stop for large group medical, dental, life, vision, LTD and STD
• Turn around from 2-14 business days
• Presentation assistance available
• Underwriting services are dedicated to your timelines
• Broker Services staff available to assist with your service concerns
• Full commissions on all cases
Please contact your Word & Brown
sales representative today!
800.606.4996
10801 West Charleston Blvd., #520, Las Vegas, NV 89135 | Toll Free 800.606.4996 | Fax 800.700.6744 | www.wordandbrown.com
Large Group Services
Helpful Plan Transition Tips for Your Clients ........3Products & Services..........................................5Product Portfolio ..............................................6Health Plan Comparison Chart ..........................8 Medicare Part D Rx &HPV Vaccine Coverages ..................................10Medical Carrier Rating Information &Broker of Record Change Requirements..............11Carrier Online Services & Billing Cycles ..................................................12
WORKSITE VOLUNTARY PRODUCTS ..............13Aflac ............................................................15Allstate Workplace Division ........................21
MEDICAL ........................................................25Aetna ..........................................................27Allied National Companies ..........................33Anthem ......................................................39BEST Life & Health Insurance ......................45Insurers AdministrativeCorporation (IAC) ........................................51Saint Mary’s Health Plans ............................57Starmark......................................................63
CONSUMER DIRECTED PLANS........................69
DENTAL ..........................................................77Dental Plan Comparison Chart ....................78Aetna ..........................................................83Allied National Companies ..........................85Anthem ......................................................87BEST Life & Health Insurance ......................89Delta Dental ................................................91Freedom Dental BEN-E-LECT ......................93GroupLink, Inc. ............................................95Insurers AdministrativeCorporation (IAC) ........................................97 MetLife ........................................................99Principal Financial Group ..........................101Reliance Standard......................................103Saint Mary’s Health Plans ..........................105SecureCare Dental ....................................107SelectDent ................................................109Starmark....................................................111
VISION..........................................................113Anthem......................................................115BEST Life & Health Insurance ....................117Camden Insurance – Affiliate of Vision Plan of America ..........................119Insurers AdministrativeCorporation (IAC) ......................................121Principal Financial Group ..........................123Saint Mary’s Health Plans ..........................125SelectVision ..............................................127
Request forProposal – Small Group (RFP) ....................129
Request forProposal – Large Group (RFP) ....................131
C O N T E N T S
LAS VEGAS OFFICE10801 West Charleston Blvd.
Suite 520Las Vegas, NV 89135
Phone Numbers800-606-4996702-577-9678
Fax Numbers800-700-6744702-577-9684
The Health Plan Reference Guide (HPRG) isa compilation of Carrier Plans and Servicesoffered to you through Word & Brown. TheHPRG provides brokers with information onplan commissions, benefits, enrollment andeligibility requirements and coverage areas.This information is printed on a quarterly basisand the most up to date guidelines are postedon our website.
www.wordandbrown.com
For proposals:[email protected]
TO OUR BROKERS:
The information in this book was collected from carriersmarketed through Word & Brown and is accurate to the bestof our knowledge at the time of printing. However, since thispublication is intended strictly as a guide – and planspecifications may change – we recommend that you verifyany data with your Word & Brown sales representative andthe carrier before basing any decisions on the informationprovided. Word & Brown disclaims any and all liabilityregarding the errors or omissions of the carriers.
Nevada
3
10801 West Charleston Blvd, #520, Las Vegas, NV 89135 | Toll Free 800.606.4996 | www.wordandbrown.com
Helpful transition tips for your clients
Please share these tips with all of your clients changing insurance plans
Until the new insurance plan has been approved, please make sure your clients are aware of the following:
Emergency Care –In case of an emergency situation, your client should call 911 or go to the nearest in-network hospital* for their new plan and pay cashor use a credit card for any incurred fees. Once their group is approved by the carrier, they can request reimbursement (less their plan’semergency room co-payment). Also remind clients to keep a record of their payment for submission to the carrier. Some plans waive theemergency room co-payment if the patient is admitted to the hospital directly from the emergency room. Important: The diagnosis by theemergency room physician must meet the carrier’s definition of a true emergency in order to receive any reimbursement.
* If your client is taken by car or ambulance to a non-network hospital because it’s within closer proximity than an in-network hospital, the new carrier must be notified within24-48 hours. Please have them call their company’s insurance contact person or you, the broker, if they need assistance with this notification process.
Continuity of Care/Completion of Covered Services – If your client or their enrolling spouse is pregnant or your client is undergoing treatment for an acute condition, a serious chronic conditionor terminal illness, it is important that they notify their company’s designated insurance contact person or you as soon as possible soyou can assist them with submitting the continuity of care form to the carrier if their situation meets this law’s criteria and the carrier’sprogram guidelines.
Doctor Office Visit –Some offices will allow the patient to sign a waiver and pay for the visit up front. Remind your client to keep record of their payment forsubmission to the carrier along with their reimbursement form once they have their new ID number. If your client is a current patient, somedoctors will agree to bill the new insurance carrier once the patient gets their new insurance ID number and will have them pay only theoffice visit co-pay for their new plan. It is best to call the office before their appointment and explain their situation so they know what thepayment procedures are in advance. If this visit can be postponed without adverse consequences to their health, they may want to considerrescheduling their appointment for a later date when they have their new ID number.
Prescriptions –Clients should refill maintenance prescriptions prior to the effective date for their new coverage. For example, they should refill a maintenancehigh blood pressure medication no later than 12/31 for new coverage that will be effective 1/1. If they need to fill a prescription on or afterthe effective date for their new coverage, but they do not have their new ID number yet, they can pay for the prescription at the pharmacyand then request reimbursement from the carrier once they receive their new ID number. For reimbursement, they must submit thepharmacy receipt that includes the name of the drug & dosage rather than only the cash register receipt. If they paid for the prescription bycredit or debit card, and return to the pharmacy with their ID number within 7-10 business days, some pharmacies will credit anyoverpayment back to their account. This is the fastest way for them to get their money back. When a medication is expensive, somepharmacies will work with the client by allowing them to buy a smaller amount (Ex: 10-day supply). When the client returns to pick up theremaining balance of their 30-day supply, the appropriate payment adjustment will be made once they show the pharmacy their new IDnumber. Some brand name drugs have generic equivalents that are much more cost effective. You or your client can find out if theirprescription medication is name brand or generic (and the co-pay amount) by using the carrier’s Web site RX search. For your clients’convenience, Web site addresses are included on the other side of this sheet.
Once the plan is approved and your clients’ employees have received their new membership cards:
• They should carry their membership card at all times. It is important for them to show their new ID card to their doctor during theirfirst visit after their new insurance plan becomes effective.
• Your clients should always make sure they use an in-network doctor or an in-network hospital in order to maximize their coverageand prevent significant gaps in coverage and/or higher out of pocket expenses.
• You should encourage your clients to review all of the benefit descriptions they received during enrollment including their Explanationof Benefits booklet (which the carrier mails to their home address) so they are familiar with their co-payments and covered procedures.
• Ensure they are aware of which procedures will require prior authorization in their plan documents. Remember that proceduresauthorized with their previous carrier may require pre-authorization with their new carrier. Each carrier has their own criteria, so anauthorization by one carrier does not guarantee authorization by another carrier in all circumstances.
• For any additional questions, your client should call Member Services (see other side of this sheet or their ID card for the phone number).
4
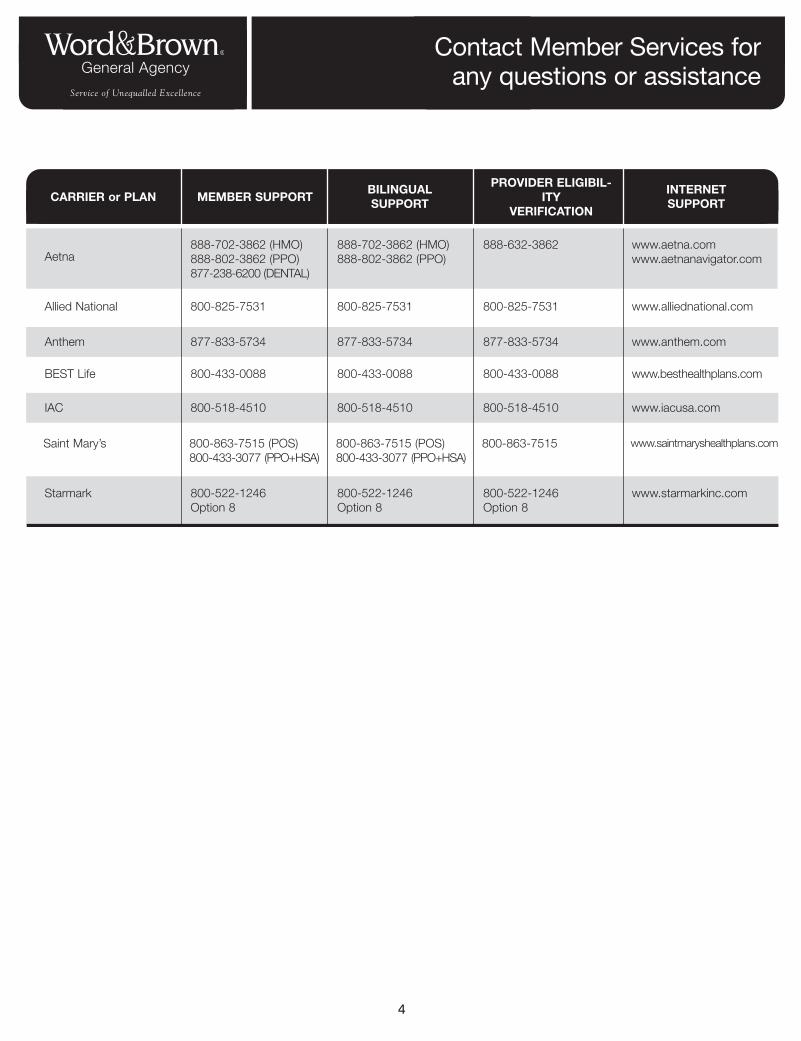
Contact Member Services forany questions or assistance
CARRIER or PLAN MEMBER SUPPORTBILINGUALSUPPORT
PROVIDER ELIGIBIL-ITY
VERIFICATION
INTERNET SUPPORT
Aetna888-702-3862 (HMO)888-802-3862 (PPO)877-238-6200 (DENTAL)
888-702-3862 (HMO)888-802-3862 (PPO)
888-632-3862 www.aetna.comwww.aetnanavigator.com
Allied National 800-825-7531 800-825-7531 800-825-7531 www.alliednational.com
BEST Life 800-433-0088 800-433-0088 800-433-0088 www.besthealthplans.com
Anthem 877-833-5734 877-833-5734 877-833-5734 www.anthem.com
IAC 800-518-4510 800-518-4510 800-518-4510 www.iacusa.com
Starmark 800-522-1246Option 8
800-522-1246Option 8
800-522-1246Option 8
www.starmarkinc.com
Saint Mary’s 800-863-7515 (POS)800-433-3077 (PPO+HSA)
800-863-7515 (POS)800-433-3077 (PPO+HSA)
800-863-7515 www.saintmaryshealthplans.com
5
10801 West Charleston Blvd., #520, Las Vegas, NV 89135 | Toll Free 800.606.4996 | Fax 800.700.6744 | www.wordandbrown.com
Products and ServicesNevada
Carriers
Individual, Small and Large Group Medical
Dental, Vision, Long Term Disability, Short Term Disability and Group Term Life
Flexible Benefits - Section 125, Section 132 (Parking and Transit)
Section 105 HRAs
COBRA and HIPAA Compliance Services
Prevailing Wage Hour Bank Health Plans, Short Term Medical,Travel Insurance, Discount Rx Card and Individual Dental and Medical
Services
Products
Enrollments
Quoting
Supplies
Technical Support
Underwriting
Commissions
6
10801 West Charleston Blvd, #520, Las Vegas, NV 89135 | Toll Free 800.606.4996 | Fax 800.700.6744 | www.wordandbrown.com
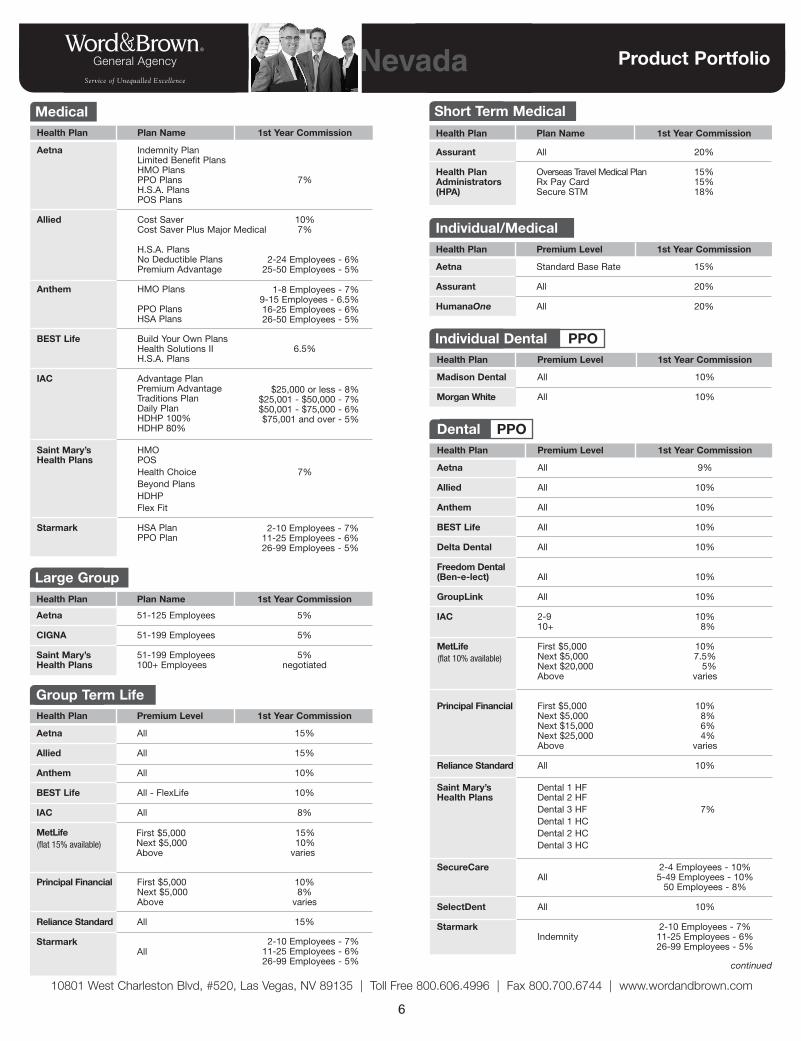
Product PortfolioNevada
Health Plan Premium Level 1st Year Commission
Aetna All 9%
Allied All 10%
Anthem All 10%
BEST Life All 10%
Delta Dental All 10%
Freedom Dental(Ben-e-lect) All 10%
GroupLink All 10%
IAC 2-9 10%10+ 8%
MetLife First $5,000 10%Next $5,000 7.5%Next $20,000 5%Above varies
Principal Financial First $5,000 10%Next $5,000 8%Next $15,000 6%Next $25,000 4%Above varies
Reliance Standard All 10%
Saint Mary’s Dental 1 HFHealth Plans Dental 2 HF
Dental 3 HF 7%Dental 1 HCDental 2 HCDental 3 HC
SecureCare 2-4 Employees - 10%All 5-49 Employees - 10%
50 Employees - 8%
SelectDent All 10%
Starmark 2-10 Employees - 7%Indemnity 11-25 Employees - 6%
26-99 Employees - 5%
Dental PPO
Health Plan Premium Level 1st Year Commission
Madison Dental All 10%
Morgan White All 10%
Individual Dental PPO
Health Plan Plan Name 1st Year Commission
Aetna Indemnity PlanLimited Benefit PlansHMO PlansPPO Plans 7%H.S.A. PlansPOS Plans
Allied Cost Saver 10%Cost Saver Plus Major Medical 7%
H.S.A. Plans No Deductible PlansPremium Advantage
Anthem HMO Plans
PPO PlansHSA Plans
BEST Life Build Your Own PlansHealth Solutions II 6.5%H.S.A. Plans
IAC Advantage Plan Premium AdvantageTraditions PlanDaily PlanHDHP 100%HDHP 80%
Saint Mary’s HMOHealth Plans POS
Health Choice 7%Beyond PlansHDHPFlex Fit
Starmark HSA PlanPPO Plan
Large Group Health Plan Plan Name 1st Year Commission
Aetna 51-125 Employees 5%
CIGNA 51-199 Employees 5%
Saint Mary’s 51-199 Employees 5%Health Plans 100+ Employees negotiated
Short Term Medical Health Plan Plan Name 1st Year Commission
Assurant All 20%
Health Plan Overseas Travel Medical Plan 15%Administrators Rx Pay Card 15%(HPA) Secure STM 18%
Group Term Life Health Plan Premium Level 1st Year Commission
Aetna All 15%
Allied All 15%
Anthem All 10%
BEST Life All - FlexLife 10%
IAC All 8%
MetLife
Principal Financial First $5,000 10%Next $5,000 8%Above varies
Reliance Standard All 15%
StarmarkAll
Medical
Individual/Medical Health Plan Premium Level 1st Year Commission
Aetna Standard Base Rate 15%
Assurant All 20%
HumanaOne All 20%
continued
$25,000 or less - 8%$25,001 - $50,000 - 7%$50,001 - $75,000 - 6%$75,001 and over - 5%
2-10 Employees - 7%11-25 Employees - 6%26-99 Employees - 5%
1-8 Employees - 7%9-15 Employees - 6.5%16-25 Employees - 6%26-50 Employees - 5%
2-24 Employees - 6%25-50 Employees - 5%
2-10 Employees - 7%11-25 Employees - 6%26-99 Employees - 5%
First $5,000Next $5,000Above
15%10%
varies(flat 15% available)
(flat 10% available)
7
10801 West Charleston Blvd, #520, Las Vegas, NV 89135 | Toll Free 800.606.4996 | Fax 800.700.6744 | www.wordandbrown.com
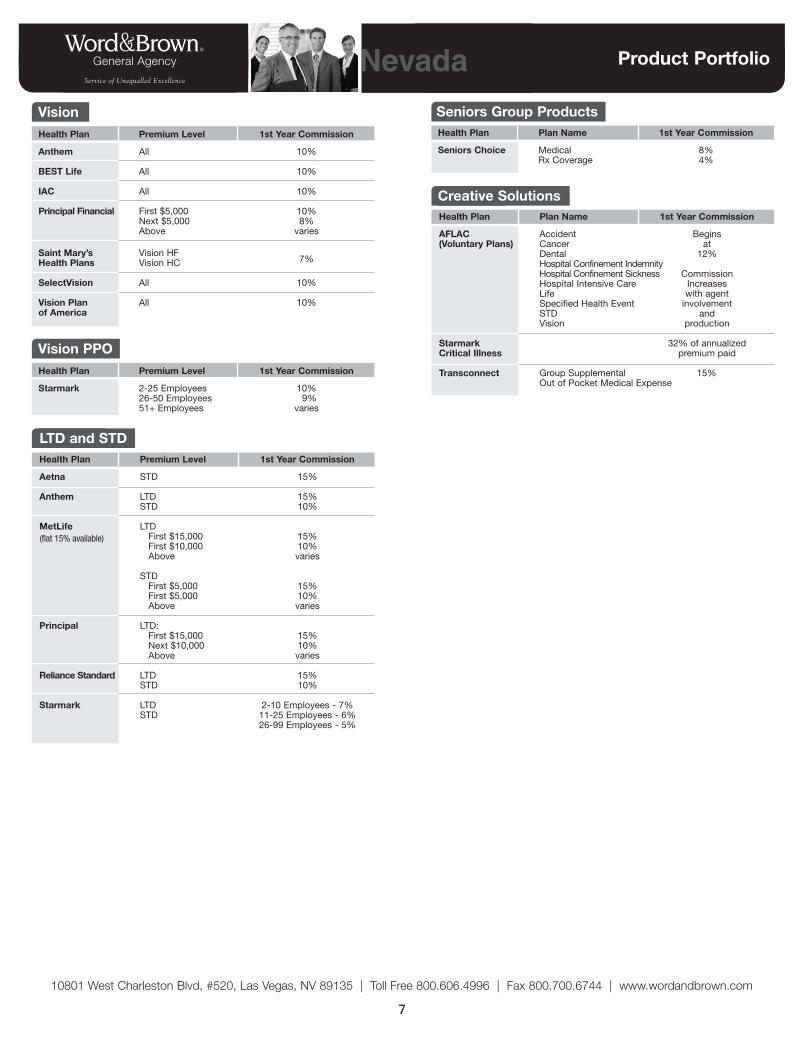
Product PortfolioNevada
Health Plan Plan Name 1st Year Commission
AFLAC Accident Begins (Voluntary Plans) Cancer at
Dental 12%Hospital Confinement IndemnityHospital Confinement Sickness CommissionHospital Intensive Care IncreasesLife with agentSpecified Health Event involvementSTD andVision production
Starmark 32% of annualizedCritical Illness premium paid
Transconnect Group Supplemental 15%Out of Pocket Medical Expense
Creative Solutions
Health Plan Premium Level 1st Year Commission
Aetna STD 15%
Anthem LTD 15%STD 10%
MetLife LTDFirst $15,000 15%First $10,000 10%Above varies
STDFirst $5,000 15%First $5,000 10%Above varies
Principal LTD:First $15,000 15%Next $10,000 10%Above varies
Reliance Standard LTD 15%STD 10%
Starmark LTD 2-10 Employees - 7%STD 11-25 Employees - 6%
26-99 Employees - 5%
LTD and STD
Health Plan Plan Name 1st Year Commission
Seniors Choice Medical 8%Rx Coverage 4%
Seniors Group ProductsVision Health Plan Premium Level 1st Year Commission
Anthem All 10%
BEST Life All 10%
IAC All 10%
Principal Financial First $5,000 10%Next $5,000 8%Above varies
Saint Mary’s Vision HFHealth Plans Vision HC
SelectVision All 10%
Vision Plan All 10%of America
7%
Vision PPO Health Plan Premium Level 1st Year Commission
Starmark 2-25 Employees 10%26-50 Employees 9%51+ Employees varies
(flat 15% available)
8
w w w. w o r d a n d b r o w n . c o m
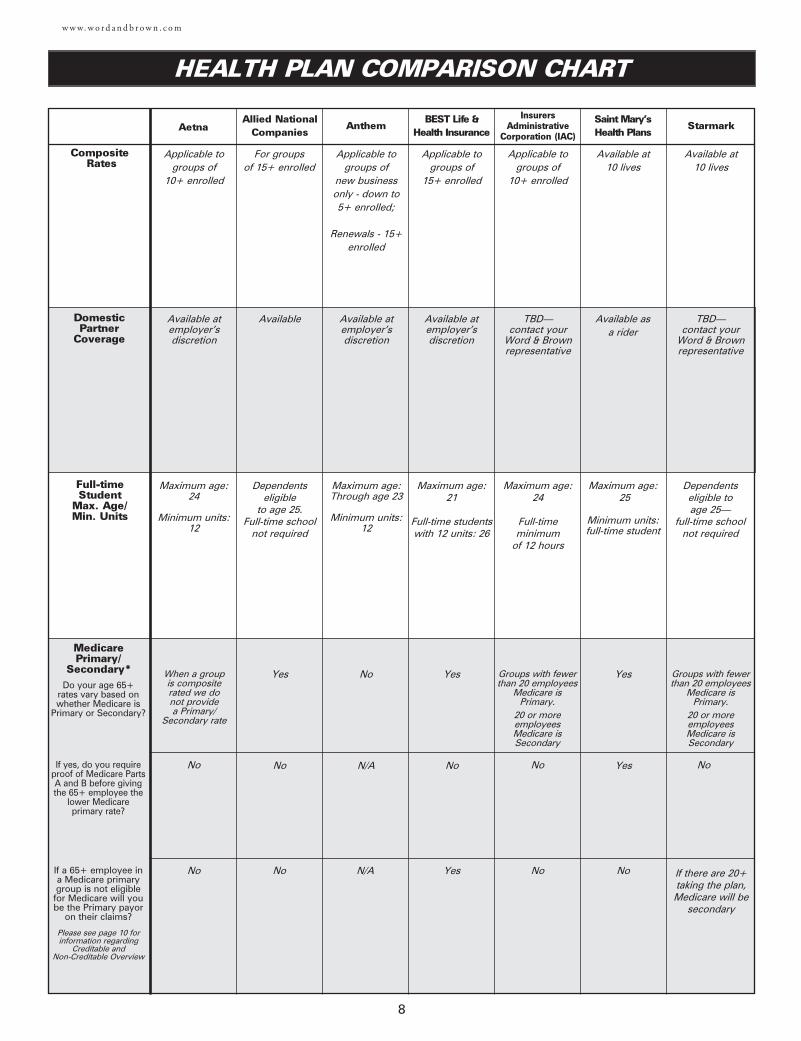
HEALTH PLAN COMPARISON CHART
CompositeRates
Aetna
Domestic Partner
Coverage
Full-time Student
Max. Age/Min. Units
MedicarePrimary/
Secondary*
Allied NationalCompanies
BEST Life & Health Insurance
Applicable to groups of
10+ enrolled
Available atemployer’sdiscretion
Maximum age: 24
Minimum units:12
For groups of 15+ enrolled
Available
Dependents eligible
to age 25. Full-time school
not required
Applicable to groups of
15+ enrolled
Available atemployer’sdiscretion
Maximum age: 21
Full-time students with 12 units: 26
Do your age 65+rates vary based onwhether Medicare is
Primary or Secondary?
If yes, do you requireproof of Medicare PartsA and B before givingthe 65+ employee the
lower Medicare primary rate?
If a 65+ employee ina Medicare primarygroup is not eligiblefor Medicare will yoube the Primary payor
on their claims?
Please see page 10 forinformation regarding
Creditable and Non-Creditable Overview
Yes
No
Yes
Yes
No
No
No
No
Applicable to groups of
10+ enrolled
Maximum age: 24
Full-time minimum
of 12 hours
InsurersAdministrative
Corporation (IAC)
Groups with fewer than 20 employees
Medicare isPrimary.
20 or more employeesMedicare isSecondary
No
No
When a group is composite rated we do not provide a Primary/
Secondary rate
TBD—contact your
Word & Brownrepresentative
Anthem
Applicable to groups of
new business only - down to 5+ enrolled;
Renewals - 15+enrolled
Available atemployer’sdiscretion
Maximum age: Through age 23
Minimum units:12
No
N/A
N/A
Starmark
Available at 10 lives
Dependents eligible to age 25—
full-time school not required
Groups with fewer than 20 employees
Medicare is Primary.
20 or more employeesMedicare isSecondary
No
TBD—contact your
Word & Brownrepresentative
If there are 20+ taking the plan,Medicare will be
secondary
Saint Mary’s Health Plans
Available at 10 lives
Available as a rider
Maximum age: 25
Minimum units:full-time student
Yes
Yes
No
9
w w w. w o r d a n d b r o w n . c o m
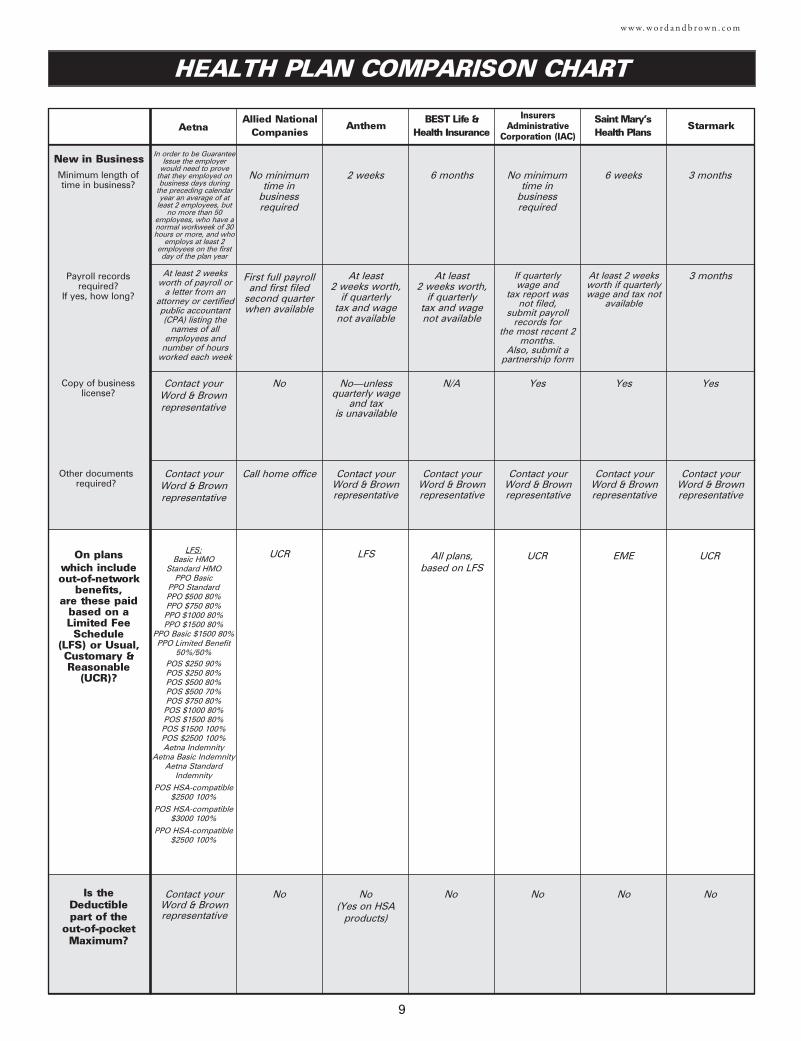
On plans which includeout-of-network
benefits,are these paid
based on aLimited FeeSchedule
(LFS) or Usual,Customary &Reasonable
(UCR)?
LFS:Basic HMO
Standard HMOPPO Basic
PPO StandardPPO $500 80%PPO $750 80%PPO $1000 80%PPO $1500 80%
PPO Basic $1500 80%PPO Limited Benefit
50%/50%POS $250 90%POS $250 80%POS $500 80%POS $500 70%POS $750 80%POS $1000 80%POS $1500 80%POS $1500 100%POS $2500 100%Aetna Indemnity
Aetna Basic IndemnityAetna Standard
Indemnity
POS HSA-compatible $2500 100%
POS HSA-compatible $3000 100%
PPO HSA-compatible $2500 100%
UCR All plans,based on LFS
UCR
Is the Deductible part of the
out-of-pocketMaximum?
Contact yourWord & Brownrepresentative
NoNoNo
New in BusinessMinimum length oftime in business?
Payroll recordsrequired?
If yes, how long?
Copy of businesslicense?
Other documentsrequired?
6 months
At least 2 weeks worth,
if quarterlytax and wage not available
N/A
No minimum time in
business required
First full payroll and first filed
second quarter when available
No
Call home office
In order to be GuaranteeIssue the employer
would need to provethat they employed onbusiness days during
the preceding calendaryear an average of at
least 2 employees, butno more than 50
employees, who have anormal workweek of 30hours or more, and who
employs at least 2employees on the firstday of the plan year
At least 2 weeksworth of payroll or
a letter from anattorney or certifiedpublic accountant(CPA) listing the
names of allemployees and
number of hoursworked each week
Contact your Word & Brown representative
Contact your Word & Brown representative
No minimum time in
business required
If quarterly wage and
tax report was not filed,
submit payroll records for
the most recent 2months.
Also, submit a partnership form
Yes
Contact your Word & Brown representative
Contact your Word & Brown representative
LFS
No(Yes on HSA
products)
2 weeks
No—unless quarterly wage
and tax is unavailable
Contact your Word & Brown representative
At least 2 weeks worth,
if quarterlytax and wage not available
UCR
No
3 months
3 months
Yes
Contact your Word & Brown representative
HEALTH PLAN COMPARISON CHART
AetnaAllied National
CompaniesBEST Life &
Health Insurance
InsurersAdministrative
Corporation (IAC)Anthem Starmark
Saint Mary’s Health Plans
EME
No
6 weeks
At least 2 weeksworth if quarterlywage and tax not
available
Yes
Contact your Word & Brown representative
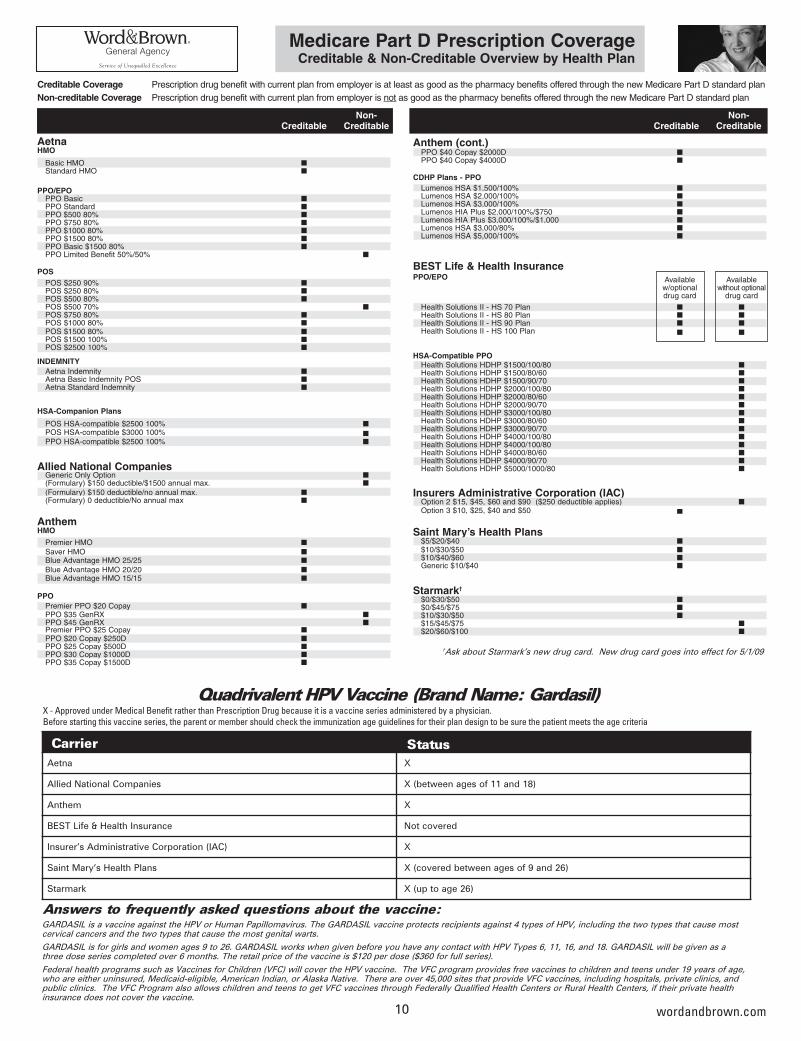
Anthem (cont.)PPO $40 Copay $2000D ■PPO $40 Copay $4000D ■
CDHP Plans - PPOLumenos HSA $1,500/100% ■Lumenos HSA $2,000/100% ■Lumenos HSA $3,000/100% ■Lumenos HIA Plus $2,000/100%/$750 ■Lumenos HIA Plus $3,000/100%/$1,000 ■Lumenos HSA $3,000/80% ■Lumenos HSA $5,000/100% ■
BEST Life & Health InsurancePPO/EPO Available Available
w/optional without optional drug card drug card
Health Solutions II - HS 70 Plan ■ ■Health Solutions II - HS 80 Plan ■ ■Health Solutions II - HS 90 Plan ■ ■Health Solutions II - HS 100 Plan ■ ■
HSA-Compatible PPOHealth Solutions HDHP $1500/100/80 ■Health Solutions HDHP $1500/80/60 ■Health Solutions HDHP $1500/90/70 ■Health Solutions HDHP $2000/100/80 ■Health Solutions HDHP $2000/80/60 ■Health Solutions HDHP $2000/90/70 ■Health Solutions HDHP $3000/100/80 ■Health Solutions HDHP $3000/80/60 ■Health Solutions HDHP $3000/90/70 ■Health Solutions HDHP $4000/100/80 ■Health Solutions HDHP $4000/100/80 ■Health Solutions HDHP $4000/80/60 ■Health Solutions HDHP $4000/90/70 ■Health Solutions HDHP $5000/1000/80 ■
Insurers Administrative Corporation (IAC)Option 2 $15, $45, $60 and $90 ($250 deductible applies) ■Option 3 $10, $25, $40 and $50 ■
Saint Mary’s Health Plans$5/$20/$40 ■$10/$30/$50 ■$10/$40/$60 ■Generic $10/$40 ■
Starmark†
$0/$30/$50 ■$0/$45/$75 ■$10/$30/$50 ■$15/$45/$75 ■$20/$60/$100 ■
10
Non-Creditable Creditable
wordandbrown.com
Medicare Part D Prescription CoverageCreditable & Non-Creditable Overview by Health Plan
Creditable Coverage Prescription drug benefit with current plan from employer is at least as good as the pharmacy benefits offered through the new Medicare Part D standard planNon-creditable Coverage Prescription drug benefit with current plan from employer is not as good as the pharmacy benefits offered through the new Medicare Part D standard plan
Non-Creditable Creditable
AetnaHMO
Basic HMO ■Standard HMO ■
PPO/EPOPPO Basic ■PPO Standard ■PPO $500 80% ■PPO $750 80% ■PPO $1000 80% ■PPO $1500 80% ■PPO Basic $1500 80% ■PPO Limited Benefit 50%/50% ■
POSPOS $250 90% ■POS $250 80% ■POS $500 80% ■POS $500 70% ■POS $750 80% ■POS $1000 80% ■POS $1500 80% ■POS $1500 100% ■POS $2500 100% ■
INDEMNITYAetna Indemnity ■Aetna Basic Indemnity POS ■Aetna Standard Indemnity ■
HSA-Companion Plans
POS HSA-compatible $2500 100% ■POS HSA-compatible $3000 100% ■PPO HSA-compatible $2500 100% ■
Allied National CompaniesGeneric Only Option ■(Formulary) $150 deductible/$1500 annual max. ■
(Formulary) $150 deductible/no annual max. ■(Formulary) 0 deductible/No annual max ■
AnthemHMO
Premier HMO ■
Saver HMO ■Blue Advantage HMO 25/25 ■
Blue Advantage HMO 20/20 ■Blue Advantage HMO 15/15 ■
PPOPremier PPO $20 Copay ■PPO $35 GenRX ■PPO $45 GenRX ■Premier PPO $25 Copay ■PPO $20 Copay $250D ■PPO $25 Copay $500D ■PPO $30 Copay $1000D ■PPO $35 Copay $1500D ■
GARDASIL is a vaccine against the HPV or Human Papillomavirus. The GARDASIL vaccine protects recipients against 4 types of HPV, including the two types that cause mostcervical cancers and the two types that cause the most genital warts.
GARDASIL is for girls and women ages 9 to 26. GARDASIL works when given before you have any contact with HPV Types 6, 11, 16, and 18. GARDASIL will be given as athree dose series completed over 6 months. The retail price of the vaccine is $120 per dose ($360 for full series).
Federal health programs such as Vaccines for Children (VFC) will cover the HPV vaccine. The VFC program provides free vaccines to children and teens under 19 years of age,who are either uninsured, Medicaid-eligible, American Indian, or Alaska Native. There are over 45,000 sites that provide VFC vaccines, including hospitals, private clinics, andpublic clinics. The VFC Program also allows children and teens to get VFC vaccines through Federally Qualified Health Centers or Rural Health Centers, if their private healthinsurance does not cover the vaccine.
Answers to frequently asked questions about the vaccine:
Quadrivalent HPV Vaccine (Brand Name: Gardasil)X - Approved under Medical Benefit rather than Prescription Drug because it is a vaccine series administered by a physician.Before starting this vaccine series, the parent or member should check the immunization age guidelines for their plan design to be sure the patient meets the age criteria
Carrier StatusAetna X
Allied National Companies X (between ages of 11 and 18)
Anthem X
BEST Life & Health Insurance Not covered
Insurer’s Administrative Corporation (IAC) X
Saint Mary’s Health Plans X (covered between ages of 9 and 26)
Starmark X (up to age 26)
†Ask about Starmark’s new drug card. New drug card goes into effect for 5/1/09
11
w w w. w o r d a n d b r o w n . c o m
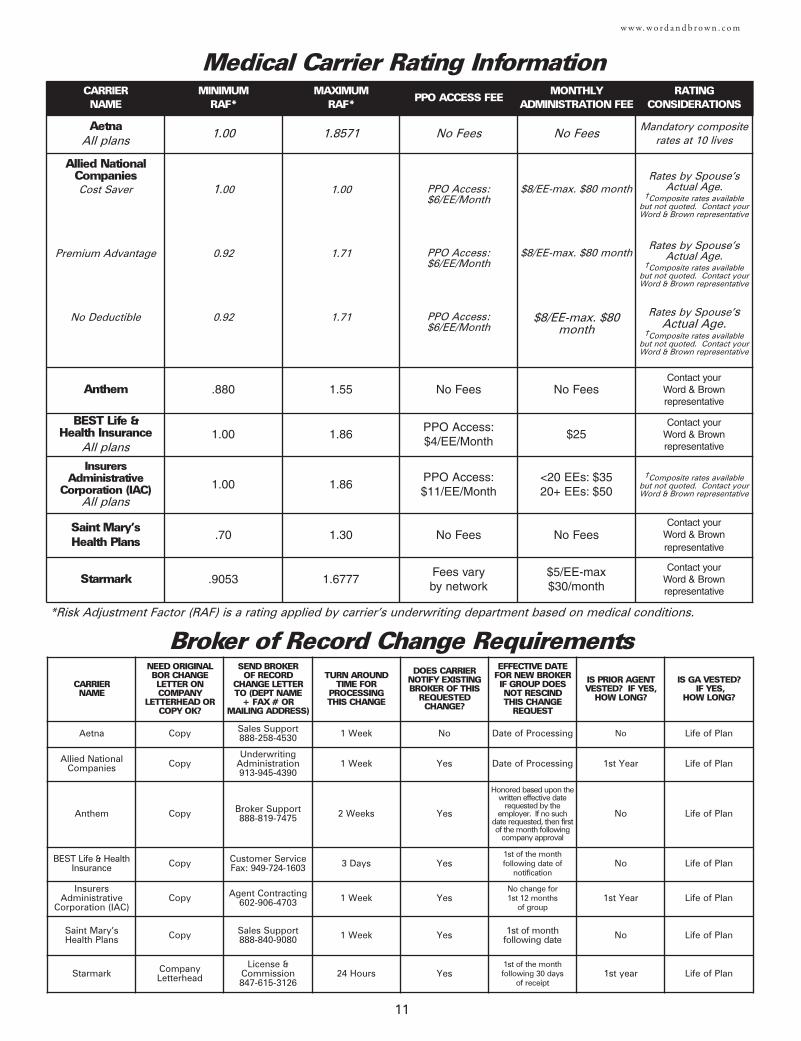
Broker of Record Change Requirements
Medical Carrier Rating Information
*Risk Adjustment Factor (RAF) is a rating applied by carrier’s underwriting department based on medical conditions.
CARRIERNAME
MINIMUMRAF*
MAXIMUMRAF*
PPO ACCESS FEE MONTHLY
ADMINISTRATION FEERATING
CONSIDERATIONS
AetnaAll plans
1.00 1.8571 No Fees No FeesMandatory composite
rates at 10 lives
Allied NationalCompaniesCost Saver
Premium Advantage
No Deductible
1.00
0.92
0.92
1.00
1.71
1.71
PPO Access:$6/EE/Month
PPO Access:$6/EE/Month
PPO Access:$6/EE/Month
$8/EE-max. $80 month
$8/EE-max. $80 month
$8/EE-max. $80month
Rates by Spouse’s Actual Age.
†Composite rates available but not quoted. Contact yourWord & Brown representative
Rates by Spouse’s Actual Age.
†Composite rates available but not quoted. Contact yourWord & Brown representative
Rates by Spouse’s Actual Age.
†Composite rates available but not quoted. Contact yourWord & Brown representative
Anthem .880 1.55 No Fees No FeesContact your
Word & Brown representative
BEST Life & Health Insurance
All plans1.00 1.86
PPO Access:$4/EE/Month
$25Contact your
Word & Brown representative
InsurersAdministrative
Corporation (IAC)All plans
1.00 1.86PPO Access:$11/EE/Month
<20 EEs: $3520+ EEs: $50
†Composite rates available but not quoted. Contact yourWord & Brown representative
Saint Mary’s Health Plans .70 1.30 No Fees No Fees
Contact your Word & Brown representative
Starmark .9053 1.6777Fees vary by network
$5/EE-max$30/month
Contact your Word & Brown representative
CARRIERNAME
NEED ORIGINAL BOR CHANGE LETTER ON COMPANY
LETTERHEAD ORCOPY OK?
SEND BROKER OF RECORD
CHANGE LETTER TO (DEPT NAME
+ FAX # OR MAILING ADDRESS)
TURN AROUNDTIME FOR
PROCESSING THIS CHANGE
DOES CARRIERNOTIFY EXISTINGBROKER OF THIS
REQUESTEDCHANGE?
EFFECTIVE DATEFOR NEW BROKER IF GROUP DOESNOT RESCIND THIS CHANGE
REQUEST
IS PRIOR AGENTVESTED? IF YES,
HOW LONG?
IS GA VESTED? IF YES,
HOW LONG?
Aetna Copy Sales Support888-258-4530 1 Week No Date of Processing No Life of Plan
Allied NationalCompanies Copy
Underwriting Administration913-945-4390
1 Week Yes Date of Processing 1st Year Life of Plan
Anthem Copy Broker Support888-819-7475 2 Weeks Yes
Honored based upon thewritten effective date
requested by theemployer. If no such
date requested, then firstof the month following
company approval
No Life of Plan
BEST Life & HealthInsurance Copy Customer Service
Fax: 949-724-1603 3 Days Yes1st of the month following date of
notificationNo Life of Plan
InsurersAdministrative
Corporation (IAC)Copy Agent Contracting
602-906-4703 1 Week YesNo change for 1st 12 months
of group1st Year Life of Plan
Saint Mary’s Health Plans Copy Sales Support
888-840-9080 1 Week Yes 1st of month following date No Life of Plan
Starmark CompanyLetterhead
License &Commission847-615-3126
24 Hours Yes1st of the month following 30 days
of receipt1st year Life of Plan
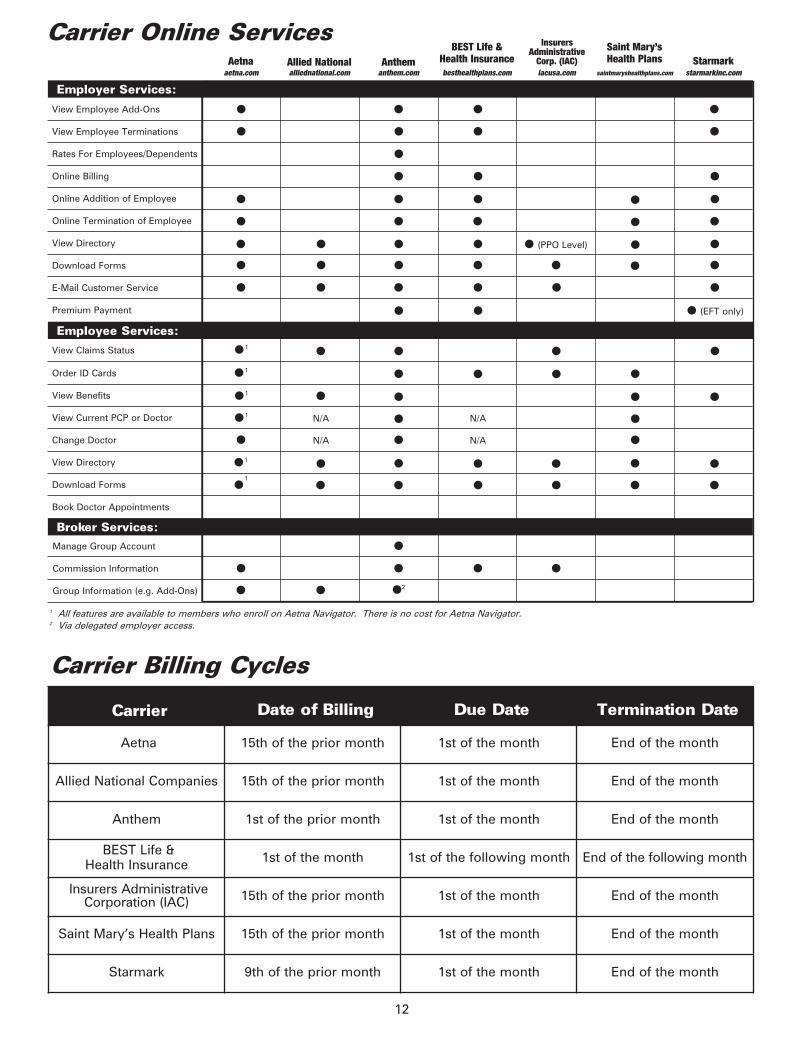
Carrier Date of Billing Due Date Termination Date
Aetna 15th of the prior month 1st of the month End of the month
Allied National Companies 15th of the prior month 1st of the month End of the month
Anthem 1st of the prior month 1st of the month End of the month
BEST Life & Health Insurance 1st of the month 1st of the following month End of the following month
Insurers AdministrativeCorporation (IAC) 15th of the prior month 1st of the month End of the month
Saint Mary’s Health Plans 15th of the prior month 1st of the month End of the month
Starmark 9th of the prior month 1st of the month End of the month
View Employee Add-Ons
View Claims Status
View Employee Terminations
Rates For Employees/Dependents
Online Billing
Online Addition of Employee
Online Termination of Employee
View Directory
Download Forms
E-Mail Customer Service
Premium Payment
Order ID Cards
View Benefits
View Current PCP or Doctor
Change Doctor
View Directory
Download Forms
Book Doctor Appointments
Manage Group Account
Commission Information
Group Information (e.g. Add-Ons)
12
Carrier Billing Cycles
1 All features are available to members who enroll on Aetna Navigator. There is no cost for Aetna Navigator.2 Via delegated employer access.
Employer Services:
Employee Services:
Broker Services:
●
●
●1
●1
●1
●1
●1
●1
Aetnaaetna.com
Allied Nationalalliednational.com
BEST Life & Health Insurancebesthealthplans.com
InsurersAdministrative
Corp. (IAC)iacusa.com
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
N/A
N/A
● (PPO Level)
●
●
●
●
●
●
●
Carrier Online Services
N/A
N/A
Anthemanthem.com
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●2
Starmarkstarmarkinc.com
●
●
●
●
●
●
●
●
● (EFT only)
●
●
●
●
Saint Mary’s Health Plans
saintmaryshealthplans.com
●
●
●
●
●
●
●
●
●
●

13
w w w. w o r d a n d b r o w n . c o m
WORKSITEVOLUNTARYPRODUCTS
15
w w w. w o r d a n d b r o w n . c o m
NY
VAWVA
MD
DE
NJ
MA
ME
NH
VT
CT RI
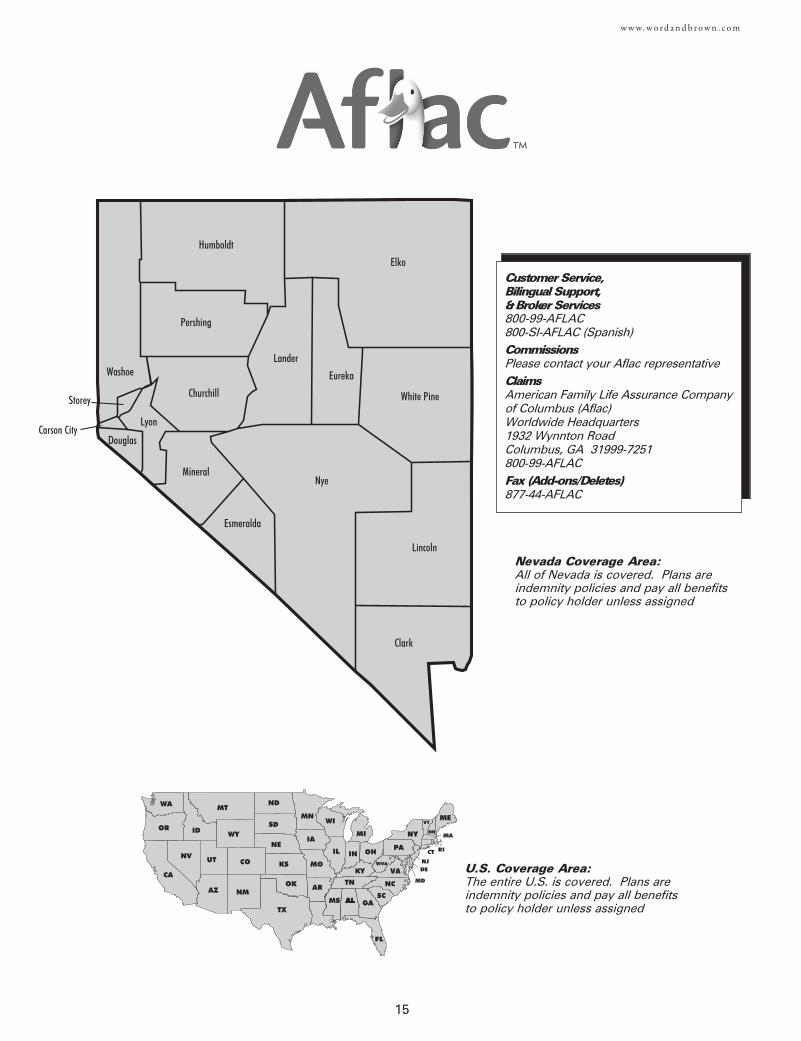
Customer Service, Bilingual Support,& Broker Services800-99-AFLAC800-SI-AFLAC (Spanish)Commissions Please contact your Aflac representativeClaimsAmerican Family Life Assurance Company of Columbus (Aflac)Worldwide Headquarters1932 Wynnton RoadColumbus, GA 31999-7251800-99-AFLACFax (Add-ons/Deletes)877-44-AFLAC
Nevada Coverage Area:All of Nevada is covered. Plans areindemnity policies and pay all benefitsto policy holder unless assigned
U.S. Coverage Area:The entire U.S. is covered. Plans areindemnity policies and pay all benefitsto policy holder unless assigned
Churchill
Clark
Douglas
Elko
Esmeralda
Eureka
Humboldt
Lander
Lincoln
Lyon
MineralNye
Pershing
Storey
Washoe
White Pine
Carson City
16
w w w. w o r d a n d b r o w n . c o m
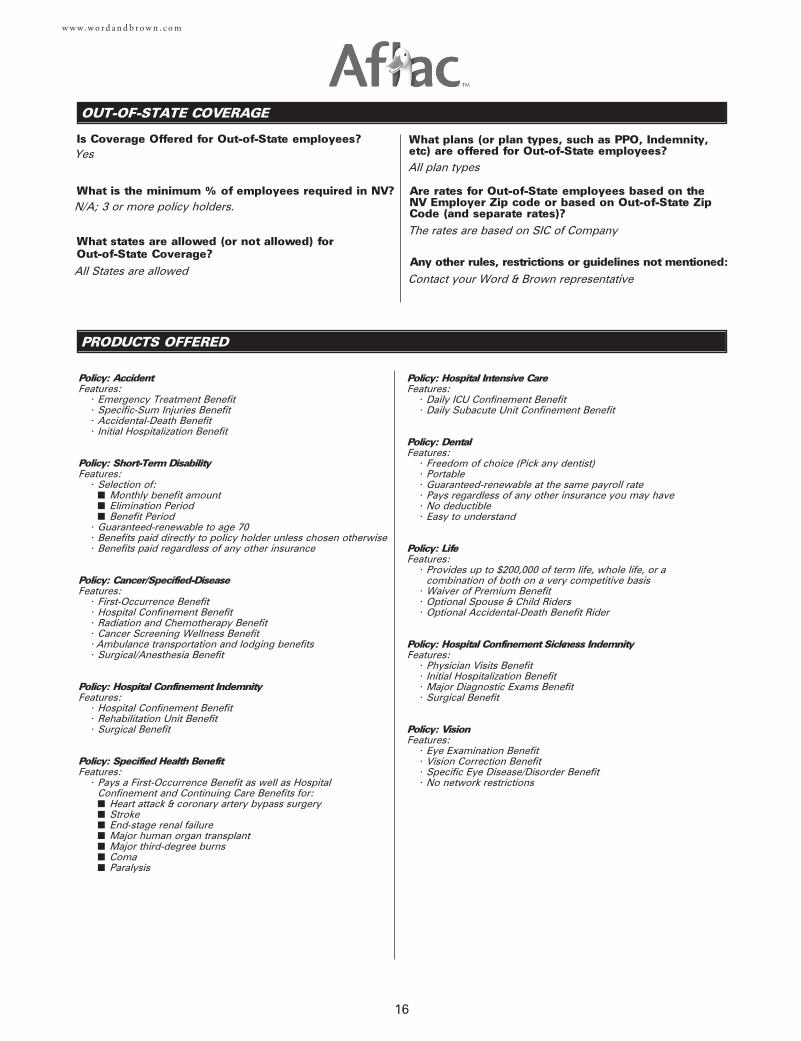
OUT-OF-STATE COVERAGE
PRODUCTS OFFERED
Is Coverage Offered for Out-of-State employees?
What is the minimum % of employees required in NV?
What plans (or plan types, such as PPO, Indemnity,etc) are offered for Out-of-State employees?
What states are allowed (or not allowed) for Out-of-State Coverage?
Are rates for Out-of-State employees based on theNV Employer Zip code or based on Out-of-State ZipCode (and separate rates)?
Any other rules, restrictions or guidelines not mentioned:
Yes
N/A; 3 or more policy holders.
All States are allowedContact your Word & Brown representative
The rates are based on SIC of Company
All plan types
Policy: AccidentFeatures:
• Emergency Treatment Benefit• Specific-Sum Injuries Benefit• Accidental-Death Benefit• Initial Hospitalization Benefit
Policy: Short-Term DisabilityFeatures:
• Selection of:■ Monthly benefit amount■ Elimination Period■ Benefit Period
• Guaranteed-renewable to age 70• Benefits paid directly to policy holder unless chosen otherwise• Benefits paid regardless of any other insurance
Policy: Cancer/Specified-DiseaseFeatures:
• First-Occurrence Benefit• Hospital Confinement Benefit• Radiation and Chemotherapy Benefit• Cancer Screening Wellness Benefit• Ambulance transportation and lodging benefits• Surgical/Anesthesia Benefit
Policy: Hospital Confinement IndemnityFeatures:
• Hospital Confinement Benefit• Rehabilitation Unit Benefit• Surgical Benefit
Policy: Specified Health BenefitFeatures:
• Pays a First-Occurrence Benefit as well as Hospital Confinement and Continuing Care Benefits for:■ Heart attack & coronary artery bypass surgery■ Stroke■ End-stage renal failure■ Major human organ transplant■ Major third-degree burns■ Coma■ Paralysis
Policy: Hospital Intensive CareFeatures:
• Daily ICU Confinement Benefit• Daily Subacute Unit Confinement Benefit
Policy: DentalFeatures:
• Freedom of choice (Pick any dentist)• Portable• Guaranteed-renewable at the same payroll rate• Pays regardless of any other insurance you may have• No deductible• Easy to understand
Policy: LifeFeatures:
• Provides up to $200,000 of term life, whole life, or a combination of both on a very competitive basis
• Waiver of Premium Benefit• Optional Spouse & Child Riders• Optional Accidental-Death Benefit Rider
Policy: Hospital Confinement Sickness IndemnityFeatures:
• Physician Visits Benefit• Initial Hospitalization Benefit• Major Diagnostic Exams Benefit• Surgical Benefit
Policy: VisionFeatures:
• Eye Examination Benefit• Vision Correction Benefit• Specific Eye Disease/Disorder Benefit• No network restrictions
17
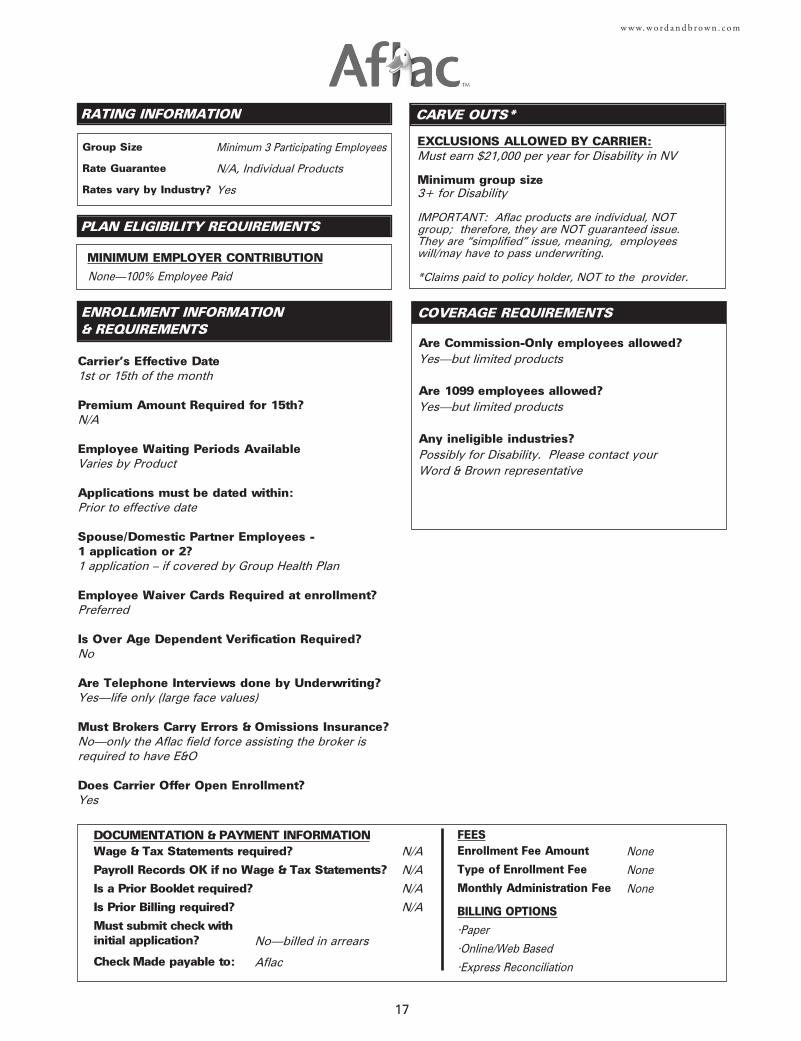
w w w. w o r d a n d b r o w n . c o m
ENROLLMENT INFORMATION & REQUIREMENTS
Are Commission-Only employees allowed?Yes—but limited products
Are 1099 employees allowed?Yes—but limited products
Any ineligible industries?Possibly for Disability. Please contact your Word & Brown representative
RATING INFORMATION
MINIMUM EMPLOYER CONTRIBUTION
EXCLUSIONS ALLOWED BY CARRIER:Must earn $21,000 per year for Disability in NV
Minimum group size3+ for Disability
IMPORTANT: Aflac products are individual, NOTgroup; therefore, they are NOT guaranteed issue.They are “simplified” issue, meaning, employeeswill/may have to pass underwriting.
*Claims paid to policy holder, NOT to the provider.
CARVE OUTS*
PLAN ELIGIBILITY REQUIREMENTS
Group Size
Rate Guarantee
Rates vary by Industry?
COVERAGE REQUIREMENTS
Minimum 3 Participating Employees
N/A, Individual Products
Yes
None—100% Employee Paid
Carrier's Effective Date1st or 15th of the month
Premium Amount Required for 15th?N/A
Employee Waiting Periods AvailableVaries by Product
Applications must be dated within:Prior to effective date
Spouse/Domestic Partner Employees - 1 application or 2?1 application – if covered by Group Health Plan
Employee Waiver Cards Required at enrollment?Preferred
Is Over Age Dependent Verification Required?No
Are Telephone Interviews done by Underwriting?Yes—life only (large face values)
Must Brokers Carry Errors & Omissions Insurance?No—only the Aflac field force assisting the broker isrequired to have E&O
Does Carrier Offer Open Enrollment?Yes
DOCUMENTATION & PAYMENT INFORMATIONWage & Tax Statements required?
Payroll Records OK if no Wage & Tax Statements?
Is a Prior Booklet required?
Is Prior Billing required?
Must submit check with initial application?
Check Made payable to:
FEESEnrollment Fee Amount
Type of Enrollment Fee
Monthly Administration Fee
BILLING OPTIONS
•Paper
•Online/Web Based
•Express Reconciliation
N/A
N/A
N/A
N/A
None
None
None
No—billed in arrears
Aflac

18
w w w. w o r d a n d b r o w n . c o m
VALUE ADDED SERVICES
Aflac’s payroll deduction and Section 125 capabilities offer powerful ways to:
• Eliminate or reduce the pressure for future company-paid plans.
• Strengthen benefits packages in a tight labor market.
• Introduce choice and portability at the employee level.
• Let employees access the power of pre-tax dollars.
• Save FICA contributions.
• Communicate the value of total company benefits in real-dollar terms.
Aflac is a premier provider of insurance policies, insuring:
• Over 11,937 state governments (and government agencies) and municipalities (company statistics, December 30, 2006).
• More than 1,108 colleges (company statistics, December 30, 2006).
• Over 1,764 hospitals (December 30, 2006).
• Over 12,083 school districts (December 30, 2006).
• More than 372,000 U.S. payroll accounts (December 30, 2006).
Aflac offers superior enrollment, communications, and claims efficiencies, such as:
• Leading-Edge Technology. Our SmartApp® point-of-sale laptop enrollment system (recognized by the Smithsonian Institution)
provides instant submission of applications via electronic signature capture.
• Employee Benefits Communication System. This people-friendly program is designed to show employees the value of the
benefits their employers provide. It can communicate all benefits, including core benefits and policies sold on a voluntary
basis.
• Info One® Personalized Benefits Statements. Generally free of charge, this service illustrates the “hidden paycheck” by
calculating the total cost of employee benefits by including the employer’s share.
• Flexible Spending Accounts, including Medical Reimbursement (Section 125) and Dependent Day-Care Accounts (Section 129).
• Transit One (Section 132) transportation expense program.
• Internet Billing and Payment Capabilities. Designed for smaller accounts, this system facilitates real-time statement changes
and updates on an easy-to-use basis.
• Single-Point Billing Services. These services are for accounts with 50 or more employees.
• Corporate Alliance Programs. These include COBRA/HIPAA administration and PEO services.
• Comprehensive Call Center. This specially dedicated customer service resource handled over 9.9 million calls in 2006
(December 31, 2006).
• Outstanding Performance in Claims Service. In 2006, Aflac processed more than six million claims in the United States. Aflac
processes most claims within four days (December 31, 2006).
19
w w w. w o r d a n d b r o w n . c o m
FEATURES AND BENEFITS
Benefits to Business Owners:
• Wellness Benefits that help provide an incentive for early detection, helping to mitigate claims costs; having a potentially positive
impact on medical plan experience and employee “return to work” times.
• Eliminate or reduce the pressure for future company-paid plans through “Voluntary, employee funded programs”.
• Revenue generation through FICA and Workers Compensation savings from the pre-taxing of Aflac Benefits.
• Expansion of your benefit program, at “No Cost,” increasing your retention and attraction power of quality employees.
• Ability to reduce “exposure” to Workers Compensation claims through additional programs that pay “Cash Benefits” and provide
“Disability Income” from the 1st day an employee misses work.
Benefits to Employees:
• The power to "choose" the quality of care they desire; while using added benefits to "buffer" the added costs of going outside a
managed care network in order to see a specialist or have a second opinion in time of need.
• Provides insurance products that generate cash to employees to help with out-of-pocket costs associated with illness or injury
that are not covered by traditional medical insurance plans. Allowing them the "choice" of protecting themselves, their families or
their paycheck.
• Access to affordable "Consumer Driven Health Plans" that are "owned" by the consumer, completely portable and guaranteed
renewable
Benefits to Broker:
• A client solution by providing some relief to increasing health insurance premiums by offering products that can help the
employer make decisions to increase deductibles and co-pays, position the company to pass premium expense to the
employee, and reduce an employer’s FICA taxes and potentially, Worker’s Compensation premiums.
• Relief to employees by offering products that reduce out-of-pocket expenses related to higher co-pays, deductibles and other
costs.
• Health Savings Account compatible products.
• The ability to attract and retain employer clients by offering additional products to their employees at no direct premium cost
before a competitive broker does.
• Additional credibility by working with Aflac, a rate-stable, Fortune 500 company with tremendous brand awareness and a 92%
claims satisfaction rate.
• Increased commissions and vesting opportunities with little time commitment.
• Provides the broker with an opportunity to maintain his/her competitive position with his/her employer client.
• Positions the broker to assist the employer with developing a more comprehensive benefit portfolio with no additional premium
cost to the employer.
21
w w w. w o r d a n d b r o w n . c o m
NY
VAWVA
MD
DE
NJ
MA
ME
NH
VT
CT RI
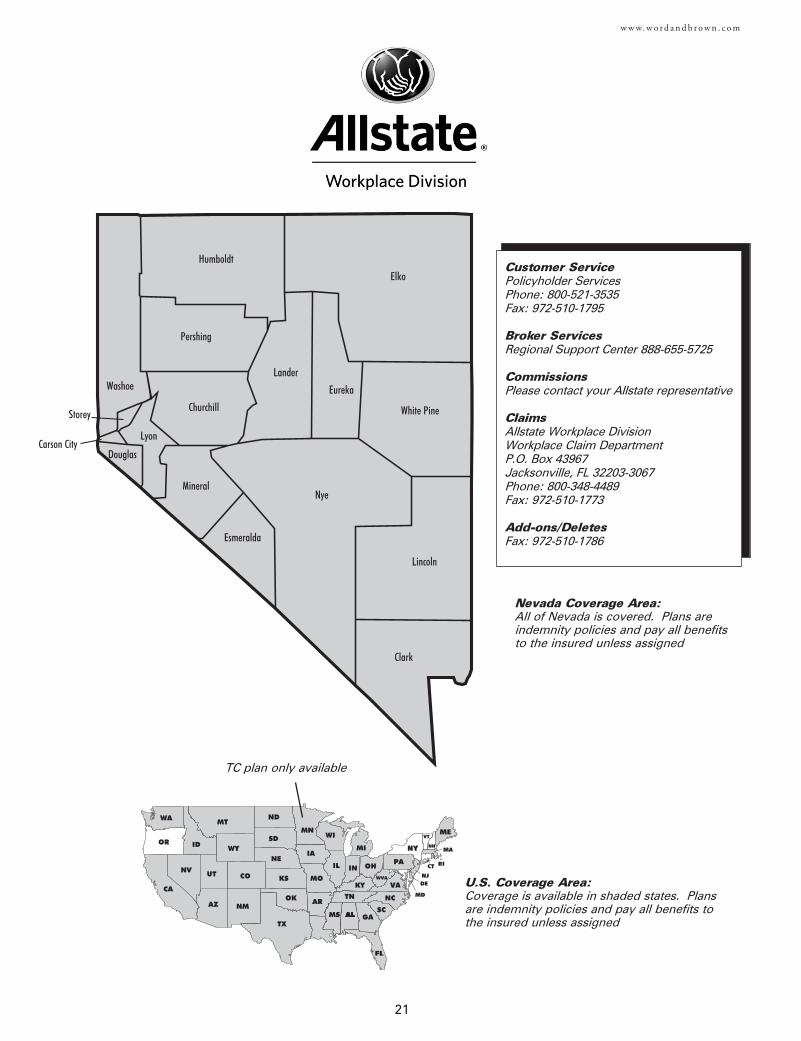
Customer ServicePolicyholder ServicesPhone: 800-521-3535Fax: 972-510-1795
Broker ServicesRegional Support Center 888-655-5725
Commissions Please contact your Allstate representative
ClaimsAllstate Workplace Division Workplace Claim Department P.O. Box 43967 Jacksonville, FL 32203-3067 Phone: 800-348-4489 Fax: 972-510-1773
Add-ons/DeletesFax: 972-510-1786
Nevada Coverage Area:All of Nevada is covered. Plans areindemnity policies and pay all benefitsto the insured unless assigned
U.S. Coverage Area:Coverage is available in shaded states. Plansare indemnity policies and pay all benefits tothe insured unless assigned
Churchill
Clark
Douglas
Elko
Esmeralda
Eureka
Humboldt
Lander
Lincoln
Lyon
MineralNye
Pershing
Storey
Washoe
White Pine
Carson City
TC plan only available
These products are designed to cover some of the things a healthinsurance policy may not and to supplement any coveragereceived through an employer. The products are guaranteed issueat initial enrollment – meaning no medical questions are required.
Group Voluntary Term LifeThis program offers Group Voluntary Term Life for the enrollee,their spouse and dependent children. It is meant to supplementany coverage one may already have through their employer byproviding valuable life insurance coverage at an affordable cost.This coverage is ideal for those who want to protect their families,but may not need a permanent Life Policy. For convenience,premiums are payroll deducted.
Group Voluntary Term Life Insurance is designed to providecoverage for a specified time and provides the ability for anenrollee to choose a plan for themselves or the entire family. Thelump sum benefit can help offset final burial expenses or costsincurred as life events happen.
An insured or their family members may use term life insurance to:
Pay off a mortgage or other outstanding debtsProvide for childcare or educational expensesReplace income to continue the same standard of living
Additional Benefit CoverageThe Waiver of Premium and Accelerated Death Benefit are includedwith the Group Voluntary Term Life coverage. Each benefitenhances the basic coverage and can help with expensesassociated with disability or terminal illness.
Waiver of PremiumIf an insured becomes disabled prior to age 60 and the disabilitylasts for 6 months or longer, they will not be required to paypremiums for as long as the disability lasts or until they reach age65, whichever occurs first, provided the group policy remains inforce.
Accelerated Death BenefitIf an insured or spouse are diagnosed with terminal illness (definedas less than 12 months to live), this benefit pays a portion of thetotal face amount up to 50%. The remaining life insurance benefitis paid upon death of the insured.
Benefit Reduction ScheduleReduction in group insurance amounts will apply at older ages,according to the following schedule:
Insured’s Attained Age Reduction to x% of OriginalCoverage
70 65%75 50%80 35%
If the insured does not enroll during their open enrollment period,they may enroll later during the annual re-enrollment period.However, they must submit evidence of insurability with theirenrollment form.
Continuation of CoverageThe insured has the option, when no longer eligible for coverage,to continue coverage at group rates up to age 70, so long as thegroup policy remains in force.
Group Voluntary Critical IllnessGroup Voluntary Critical Illness insurance pays a lump-sum benefitupon diagnosis of a covered critical illness or condition. Havingsupplemental Critical Illness insurance can help lessen financialimpact to the wallet. It allows the insured to concentrate ongetting better, rather than spending time and energy worryingabout how to pay the bills.
The lump-sum benefit for each category of coverage helps to:
Pay for treatments not covered under medical insuranceSpend precious time with family and friendsPay for mortgage and other expenses
Traditional health insurance is valuable, but often has limits.Because medical treatments and technology are advancing daily,people are living longer with major illnesses or disease. This canbe very costly. Financial hardship can happen, due to indirectmedical expenses that health and disability insurance doesn’tcover. Group Voluntary Critical Illness insurance is a strongsupplement to current health and disability insurance coverage.
The insured may choose either a $5,000 or $10,000 basic benefitamount. Depending on the basic benefit amount selected, up to100% of the basic benefit amount will be payable in each of threebenefit categories; Coronary Artery By-Pass Surgery, Alzheimer’sDisease and Carcinoma in Situ pay 25% of the benefit amount.
Group Voluntary AccidentGroup Voluntary Accident Insurance offers the insured and theirfamily coverage against sudden accidental injuries that can occurwithout warning. It protects the insured and their family 24-hours aday, seven days a week, both on- or off-the-job.
Each pre-packaged plan doesn’t just cover the insured; if theychoose, it also covers their dependents (which can include spouseand dependent children). This valuable coverage can helpsupplement traditional medical insurance. Traditional medicalinsurance is valuable, but may limit coverage during anunexpected accidental injury.
The insured and each covered family member can be sure they willreceive:
· A lump sum benefit, in case the accident leads to death or dismemberment
· 24-7 protection for accidental injuries**· Benefit coverage that goes where you go**
Unexpected accidents can also mean unexpected out-of-pocketexpenses. Hospital stays, medical or surgical treatments,dislocations or fractures, and transportation by air or groundambulance can add up quickly and be very costly. This GroupVoluntary Accident Insurance helps offset some of these expensesso that the insured’s finances remain healthy.
**Treatment must be obtained in the U.S. or its territories.
If a covered person sustains an injury which results in a coveredloss within 90 days from the date of an accident, while coverage isin force, Allstate Workplace Division will pay the benefits as statedin the benefits provisions.
· Accidental Death· Common Carrier Accidental Death· Dismemberment· Dislocation and Fracture· Initial Hospital Confinement· Hospital Confinement· Intensive Care· Ambulance (ground and air)· Medical Expenses· Outpatient Physician’s Treatment
NOTE: This Product Overview is an agent recruitment and trainingdocument and is not intended for consumer use. The insuranceproducts discussed in this document may vary based on state ofissue and may not be available for sale in all states.
22
w w w. w o r d a n d b r o w n . c o m
PRODUCTS OFFERED (High and Low Options)
DOCUMENTATION & PAYMENT INFORMATIONWage & Tax Statements required?
Payroll Records OK if no Wage & Tax Statements?
Is a Prior Booklet required?
Is Prior Billing required?
Must submit check with initial application?
Check Made payable to:
23
w w w. w o r d a n d b r o w n . c o m
ENROLLMENT INFORMATION & REQUIREMENTS
Are Commission-Only employees allowed?Yes
Are 1099 employees allowed?Yes
Any ineligible industries?Please contact your Word & Brown representative
RATING INFORMATION
MINIMUM EMPLOYER CONTRIBUTION
EXCLUSIONS ALLOWED BY CARRIER:
Minimum group size5-200 eligible
CARVE OUTS*
PLAN ELIGIBILITY REQUIREMENTS
Group Size
Rate Guarantee
Rates vary by Industry?
COVERAGE REQUIREMENTS
5-200 eligible
Minimum 1 Year
No
A minimum of 5 participants are required to initiate the SBSprogram. If the total number of participants fall below 5, theemployer has 3 billing cycles (months) to bring the levels up tominimum before the plan will be terminated. Groups with over200 eligible employees will not qualify for participation
Carrier's Effective Date1st of the month
Premium Amount Required for 15th?N/A
Employee Waiting Periods AvailableEmployer Determines Eligibility
Applications must be dated within:Prior to effective date
Spouse/Domestic Partner Employees - 1 application or 2?1 application
Employee Waiver Cards Required at enrollment?Yes
Is Over Age Dependent Verification Required?No
Are Telephone Interviews done by Underwriting?Initial contact to Region, then Broker, then Employer ifnecessary.
Must Brokers Carry Errors & Omissions Insurance?Yes
Does Carrier Offer Open Enrollment?Yes
FEESEnrollment Fee Amount
Type of Enrollment Fee
Monthly Administration Fee
BILLING OPTIONS
Paper only
N/A
N/A
No—billed in arrears
Allstate Workplace Division
N/A
N/A
None
None
None
24
w w w. w o r d a n d b r o w n . c o m
VALUE ADDED SERVICES
• 15% broker commission (1st year and renewal)
• Products are Guarantee Issue
• No participation requirements
• Products are portable as an individual component (not as a package)
• Monthly billing
OUT-OF-STATE COVERAGE
Is Coverage Offered for Out-of-State employees?
What is the minimum % of employees required in NV?
What plans (or plan types, such as PPO, Indemnity,etc) are offered for Out-of-State employees?
What states are allowed (or not allowed) for Out-of-State Coverage?
Are rates for Out-of-State employees based on theNV Employer Zip code or based on Out-of-State ZipCode (and separate rates)?
Any other rules, restrictions or guidelines not mentioned:
Yes
N/A; 5 or more insureds
Contact your Word & Brown representativeContact your Word & Brown representative
The rates are based on SIC of company
All plan types
FEATURES AND BENEFITS
Additional Wellness Screening BenefitAllstate has enhanced the coverage by providing a Wellness Screening Benefit. A $100 benefit will be paid for one of thefollowing screening tests performed while not hospital confined:
· Bone Marrow Testing· CA15-3 (blood test for breast cancer)· CA125 (blood test for ovarian cancer)· CEA (blood test for colon cancer)· Chest X-ray· Colonoscopy· Flexible sigmoidoscopy· Hemocult stool analysis· Mammography, including breast ultrasound· Pap Smear, including Thin Prep Pap Test· PSA (blood test for prostate cancer)· Serum Protein Electrophoresis (test for myeloma)· Biopsy for skin Cancer· Stress test on bike or treadmill· Electrocardiogram· Carotid Doppler· Echocardiogram· Lipid panel (total cholesterol count)· Blood test for triglycerides
There is no limit to the number of years screening tests can be received, and the benefit is paid regardless of the result ofthe test(s). Limited to one test each calendar year for each covered person.

25
MEDICAL
27
w w w. w o r d a n d b r o w n . c o m
Churchill
Clark
Douglas
Elko
Esmeralda
Eureka
Humboldt
Lander
Lincoln
Lyon
MineralNye
Pershing
Storey
Washoe
White Pine
Carson City
HMO/POSAetnaP.O. Box 24019Fresno, CA 93779
PPO/IndemnityAetnaP.O. Box 981204El Paso, TX 79998-1204
CLAIMS REIMBURSEMENT
Member Support 888-702-3862 (HMO)888-802-3862 (PPO/Indemnity)
Broker Service 877-249-2472
Bilingual Support See member supportnumbers above
Commissions 877-249-2472Employer Support 877-249-7235Adds/Terms Fax 888-258-4528Provider Services 888-632-3862
Pharmacy 800-238-6270 (Prompt 2 for Member)
Mail Order Drug 866-612-3862
This may or may not match what is on the employee’s ID card.
PPO Counties
PPO & POS Counties
ME
DI
CA
L
HMO/POS
Any unshaded areas are indemnityonly. Plan may not be available in allzip codes within county. Contact your Word & Brown representative to confirm if coverage is available foryour group location.
LIFE
DENTAL
VISION
INFERTILITY
CHIROPRACTIC
ACUPUNCTURE
MASSAGE THERAPY
PRODUCTS OFFERED
OPTIONAL BENEFITS
GROUP SIZE
PROVIDER INFORMATION
HMO/EPO PPO POS
28
CONSUMER-DIRECTED HEALTHCARE
w w w. w o r d a n d b r o w n . c o m
ALTERNATIVE DISCIPLINES
HMOAetna
CPOSAetna Choice Point of Service
PPOAetna Open Choice PPOwww.aetna.com
Is Workers' Comp required oncorporate officers, partnersand sole proprietors?No
Is on-the-job covered for corporate officers, partnersand sole proprietors?Yes
Is there a premium adjustmentfor 24 hour coverage?No
How often can members change their Primary Care Physician (PCP)?
Can family members eachchoose a PCP from a differentIPA/Medical Group?
Does carrier allow an OB/GYNto be Primary Care Physician?
Self-referral available?
Express referral available?
Not Available
2-50
Aetna
HMO PPO
Aetna IndemnityAetna Basic Indemnity
Aetna Standard Indemnity
Indemnity
Basic HMOStandard HMO
POS HSA-compatible $2500 100%POS HSA-compatible $3000 100%
DUAL OPTION (MIX AND MATCH)
Aetna's multi option program is called Pick-A-Plan 3. Employers ofgroups with 5+ enrolling employees can select up to 3 of the 15 availableplans at the time of initial enrollment. One person must enroll in eachplan chosen.
Aetna
Aetna
No—see self-referral information above
HMO: Yes—OB/GYN well woman exams (including PAP smear),gynecological-related problems, follow-up care & obstetrical carePPO: Yes
SELECTION
SPECIALIST REFERRALS
NETWORKS
HMO: Anytime. Change must berequested by the 15th of the month tobe effective the 1st of the following monthPPO & Indemnity: No PCP selection is required
Yes
Yes—if OB/GYN is listed as a PCP
We offer chiro with some of our medical plans andalongside of our discount program, this benefit isunlimited with the discount program.
PPO BasicPPO StandardPPO $500 80%PPO $750 80%PPO $1000 80%PPO $1500 80%
PPO Basic $1500 80%PPO Limited Benefit 50%/50%
24 HOUR COVERAGE
POSPOS $250 90%POS $250 80%POS $500 80%POS $500 70%POS $750 80%POS $1000 80%POS $1500 80%POS $1500 100%POS $2500 100%
HSA-Compatible POS
PPO HSA-compatible $2500 100%
HSA-Compatible PPO
Available
Available
Discount Included
Discount Included
Not Covered—only the treatment of the underlyingcause. Refer to Infertility section on page 31
w w w. w o r d a n d b r o w n . c o m
AFTERINITIAL ISSUE
ENROLLMENT GROUP SIZE
Employees
Dependents
Employees
Dependents
Employees
For Dependents
% of Total Cost:
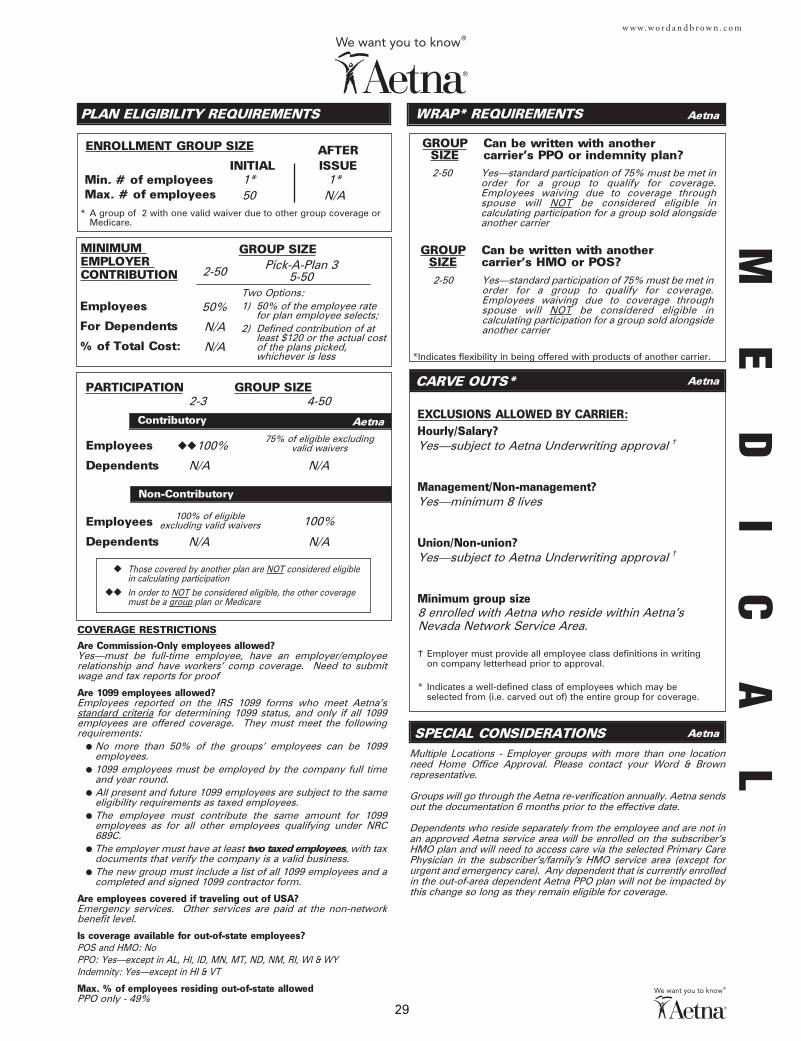
PLAN ELIGIBILITY REQUIREMENTS
MINIMUM EMPLOYER CONTRIBUTION
PARTICIPATION
Contributory
Non-Contributory
GROUP SIZE
GROUP SIZE CARVE OUTS*
WRAP* REQUIREMENTS
*Indicates flexibility in being offered with products of another carrier.
GROUP Can be written with another SIZE carrier's PPO or indemnity plan?
SPECIAL CONSIDERATIONS
29
EXCLUSIONS ALLOWED BY CARRIER:Hourly/Salary?
Management/Non-management?
Union/Non-union?
Minimum group size
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
2-50
50%
N/A
N/A
1* 1*50 N/A
2-50 Yes—standard participation of 75% must be met in order for a group to qualify for coverage.Employees waiving due to coverage throughspouse will NOT be considered eligible incalculating participation for a group sold alongside another carrier
Yes—subject to Aetna Underwriting approval †
Yes—minimum 8 lives
Yes—subject to Aetna Underwriting approval †
8 enrolled with Aetna who reside within Aetna’s Nevada Network Service Area.
Aetna
Aetna
Aetna
Aetna
GROUP Can be written with another SIZE carrier's HMO or POS?
100%
N/A N/A
2-3 4-50
◆◆100%
N/A N/A
† Employer must provide all employee class definitions in writingon company letterhead prior to approval.
Multiple Locations - Employer groups with more than one locationneed Home Office Approval. Please contact your Word & Brownrepresentative.
Groups will go through the Aetna re-verification annually. Aetna sendsout the documentation 6 months prior to the effective date.
Dependents who reside separately from the employee and are not inan approved Aetna service area will be enrolled on the subscriber'sHMO plan and will need to access care via the selected Primary CarePhysician in the subscriber's/family's HMO service area (except forurgent and emergency care). Any dependent that is currently enrolledin the out-of-area dependent Aetna PPO plan will not be impacted bythis change so long as they remain eligible for coverage.
◆ Those covered by another plan are NOT considered eligible in calculating participation
◆◆ In order to NOT be considered eligible, the other coveragemust be a group plan or Medicare
Min. # of employeesMax. # of employees
2-50 Yes—standard participation of 75% must be met inorder for a group to qualify for coverage. Employees waiving due to coverage throughspouse will NOT be considered eligible incalculating participation for a group sold alongside another carrier
COVERAGE RESTRICTIONS
Are Commission-Only employees allowed?Yes—must be full-time employee, have an employer/employeerelationship and have workers' comp coverage. Need to submitwage and tax reports for proof
Are 1099 employees allowed?Employees reported on the IRS 1099 forms who meet Aetna'sstandard criteria for determining 1099 status, and only if all 1099employees are offered coverage. They must meet the followingrequirements:
● No more than 50% of the groups’ employees can be 1099employees.
● 1099 employees must be employed by the company full timeand year round.
● All present and future 1099 employees are subject to the sameeligibility requirements as taxed employees.
● The employee must contribute the same amount for 1099employees as for all other employees qualifying under NRC689C.
● The employer must have at least two taxed employees, with taxdocuments that verify the company is a valid business.
● The new group must include a list of all 1099 employees and acompleted and signed 1099 contractor form.
Are employees covered if traveling out of USA?Emergency services. Other services are paid at the non-networkbenefit level.
Is coverage available for out-of-state employees?POS and HMO: NoPPO: Yes—except in AL, HI, ID, MN, MT, ND, NM, RI, WI & WYIndemnity: Yes—except in HI & VT
Max. % of employees residing out-of-state allowedPPO only - 49%
75% of eligible excludingvalid waivers
100% of eligible excluding valid waivers
* A group of 2 with one valid waiver due to other group coverage or Medicare.
Pick-A-Plan 35-50
Two Options:1) 50% of the employee rate
for plan employee selects;2) Defined contribution of at
least $120 or the actual costof the plans picked,whichever is less
ME
DI
CA
L
w w w. w o r d a n d b r o w n . c o m
MEDICAL UNDERWRITING REQUIREMENTS
Current Employees
TimelyAdd-ons
RAF Increments (2-50 lives)
Composite Rates
Rate Guarantee
Apply Trend Factor?
Use Employee Zips?
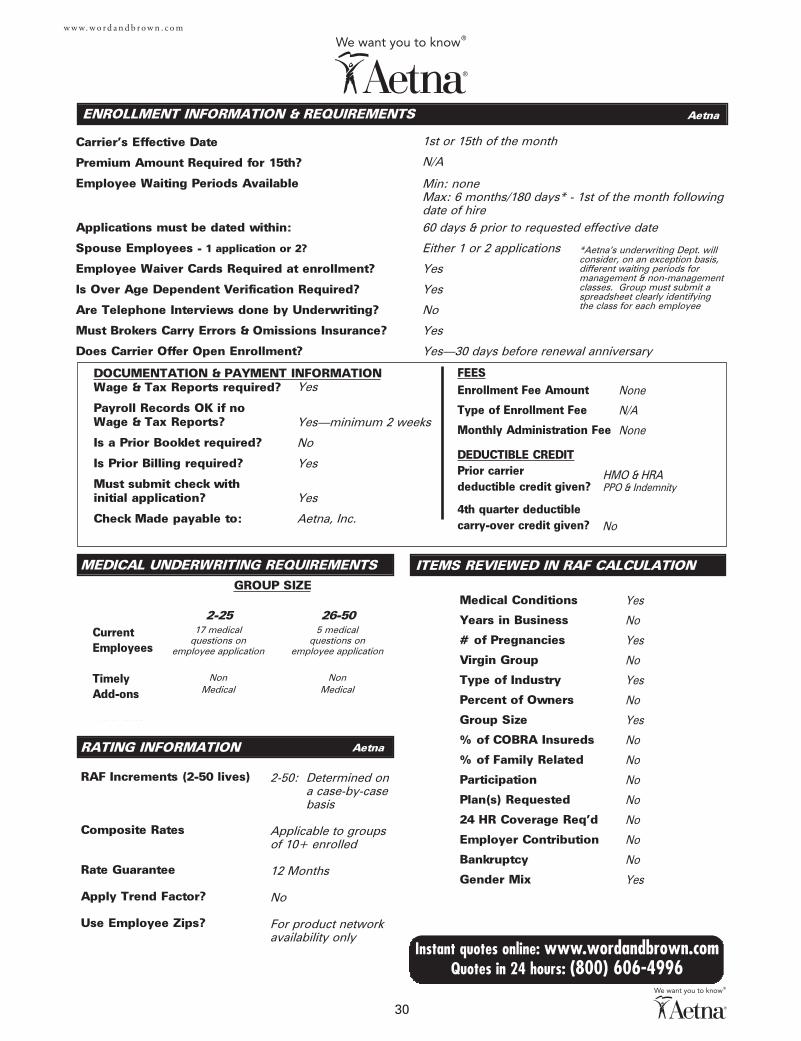
ENROLLMENT INFORMATION & REQUIREMENTS
Carrier's Effective Date
Premium Amount Required for 15th?
Employee Waiting Periods Available
Applications must be dated within:
Spouse Employees - 1 application or 2?
Employee Waiver Cards Required at enrollment?
Is Over Age Dependent Verification Required?
Are Telephone Interviews done by Underwriting?
Must Brokers Carry Errors & Omissions Insurance?
Does Carrier Offer Open Enrollment?
DOCUMENTATION & PAYMENT INFORMATIONWage & Tax Reports required?
Payroll Records OK if no Wage & Tax Reports?
Is a Prior Booklet required?
Is Prior Billing required?
Must submit check with initial application?
Check Made payable to:
FEESEnrollment Fee Amount
Type of Enrollment Fee
Monthly Administration Fee
DEDUCTIBLE CREDITPrior carrier deductible credit given?
4th quarter deductiblecarry-over credit given?
GROUP SIZE
RATING INFORMATION
30
Instant quotes online: www.wordandbrown.comQuotes in 24 hours: (800) 606-4996
ITEMS REVIEWED IN RAF CALCULATION
Medical Conditions
Years in Business
# of Pregnancies
Virgin Group
Type of Industry
Percent of Owners
Group Size
% of COBRA Insureds
% of Family Related
Participation
Plan(s) Requested
24 HR Coverage Req'd
Employer Contribution
Bankruptcy
Gender Mix
Current Employees
TimelyAdd-ons
Yes
Yes—minimum 2 weeks
No
Yes
Yes
Aetna, Inc.
None
N/A
None
Yes
No
Yes
No
Yes
No
Yes
No
No
No
No
No
No
No
Yes
2-50: Determined ona case-by-casebasis
Applicable to groups of 10+ enrolled
12 Months
No
For product network availability only
17 medical 5 medicalquestions on questions on
employee application employee application
Non NonMedical Medical
1st or 15th of the month
N/A
Min: none Max: 6 months/180 days* - 1st of the month followingdate of hire60 days & prior to requested effective date
Either 1 or 2 applications
Yes
Yes
No
Yes
Yes—30 days before renewal anniversary
Aetna
Aetna
GROUP SIZE
HMO & HRAPPO & Indemnity
No
2-25 26-50
*Aetna's underwriting Dept. willconsider, on an exception basis,different waiting periods formanagement & non-managementclasses. Group must submit aspreadsheet clearly identifying the class for each employee
31
w w w. w o r d a n d b r o w n . c o m
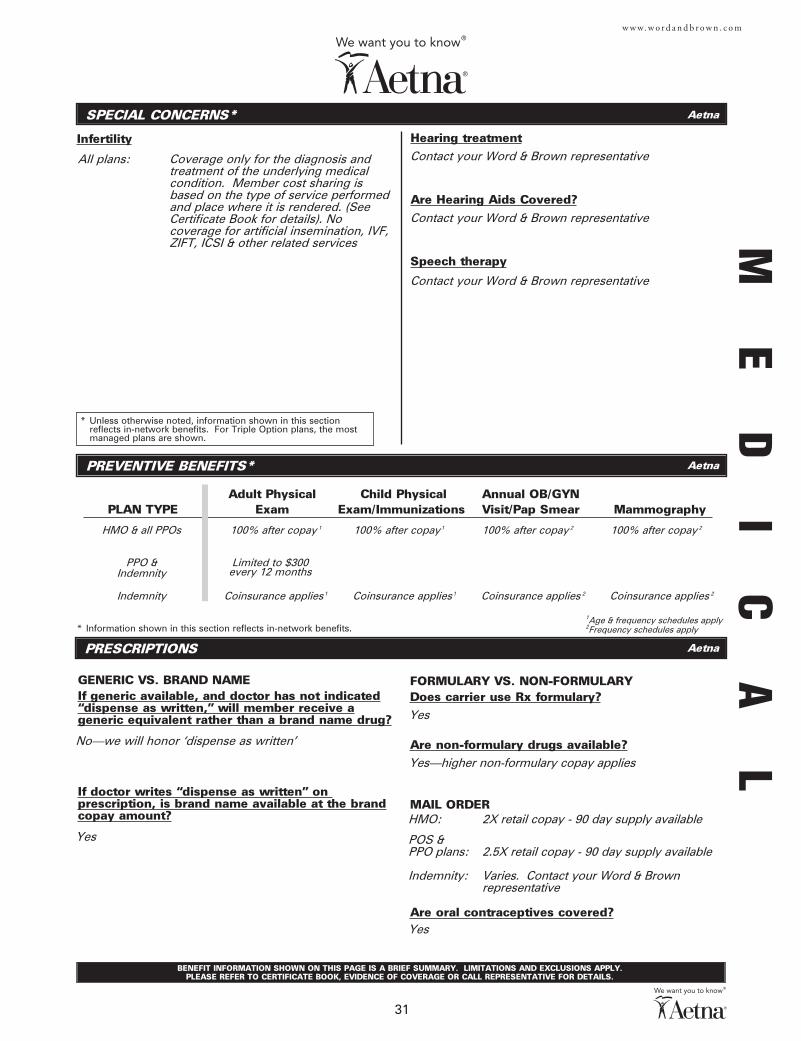
Infertility
Adult Physical Child Physical Annual OB/GYNPLAN TYPE Exam Exam/Immunizations Visit/Pap Smear Mammography
SPECIAL CONCERNS*
Hearing treatment
Are Hearing Aids Covered?
Speech therapy
PREVENTIVE BENEFITS*
PRESCRIPTIONS
* Information shown in this section reflects in-network benefits. For Triple Option plans, the most managed plans are shown.
FORMULARY VS. NON-FORMULARYDoes carrier use Rx formulary?
Are non-formulary drugs available?
MAIL ORDER - 90 DAY SUPPLY
Are oral contraceptives covered?
* Unless otherwise noted, information shown in this section reflects in-network benefits. For Triple Option plans, the most managed plans are shown.
BENEFIT INFORMATION SHOWN ON THIS PAGE IS A BRIEF SUMMARY. LIMITATIONS AND EXCLUSIONS APPLY. PLEASE REFER TO CERTIFICATE BOOK, EVIDENCE OF COVERAGE OR CALL REPRESENTATIVE FOR DETAILS.
FORMULARY VS. NON-FORMULARYDoes carrier use Rx formulary?
Are non-formulary drugs available?
MAIL ORDER
Are oral contraceptives covered?
Contact your Word & Brown representative
No—we will honor ‘dispense as written’
Yes
Yes
Yes—higher non-formulary copay applies
HMO: 2X retail copay - 90 day supply available
POS &PPO plans: 2.5X retail copay - 90 day supply available
Indemnity: Varies. Contact your Word & Brown representative
Yes
* Information shown in this section reflects in-network benefits.
Aetna
Aetna
Aetna
HMO & all PPOs 100% after copay 1 100% after copay 1 100% after copay 2 100% after copay 2
PPO & Indemnity
Limited to $300every 12 months
Indemnity Coinsurance applies 1 Coinsurance applies 1 Coinsurance applies 2 Coinsurance applies 2
GENERIC VS. BRAND NAMEIf generic available, and doctor has not indicated“dispense as written,” will member receive ageneric equivalent rather than a brand name drug?
If doctor writes “dispense as written” on prescription, is brand name available at the brandcopay amount?
1Age & frequency schedules apply2Frequency schedules apply
All plans: Coverage only for the diagnosis andtreatment of the underlying medicalcondition. Member cost sharing isbased on the type of service performedand place where it is rendered. (SeeCertificate Book for details). Nocoverage for artificial insemination, IVF,ZIFT, ICSI & other related services
Contact your Word & Brown representative
Contact your Word & Brown representative ME
DI
CA
L
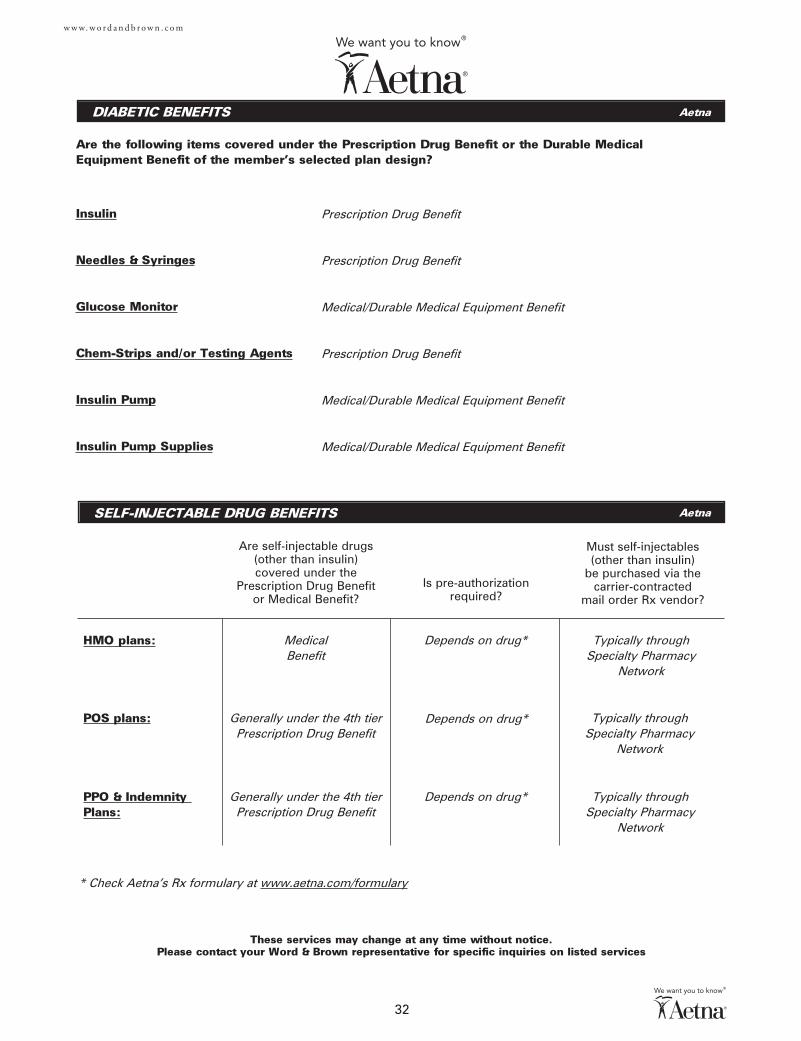
DIABETIC BENEFITS
These services may change at any time without notice. Please contact your Word & Brown representative for specific inquiries on listed services
32
Are the following items covered under the Prescription Drug Benefit or the Durable MedicalEquipment Benefit of the member’s selected plan design?
w w w. w o r d a n d b r o w n . c o m
Insulin
Needles & Syringes
Glucose Monitor
Chem-Strips and/or Testing Agents
Insulin Pump
Insulin Pump Supplies
SELF-INJECTABLE DRUG BENEFITS
Are self-injectable drugs(other than insulin)covered under the
Prescription Drug Benefitor Medical Benefit?
Is pre-authorizationrequired?
Must self-injectables(other than insulin)
be purchased via thecarrier-contracted
mail order Rx vendor?
Aetna
Aetna
Aetna
Prescription Drug Benefit
Prescription Drug Benefit
Medical/Durable Medical Equipment Benefit
Prescription Drug Benefit
Medical/Durable Medical Equipment Benefit
Medical/Durable Medical Equipment Benefit
MedicalBenefit
Generally under the 4th tierPrescription Drug Benefit
Generally under the 4th tierPrescription Drug Benefit
Depends on drug*
Depends on drug*
Depends on drug*
Typically through Specialty Pharmacy
Network
Typically through Specialty Pharmacy
Network
Typically through Specialty Pharmacy
Network
* Check Aetna's Rx formulary at www.aetna.com/formulary
HMO plans:
POS plans:
PPO & Indemnity Plans:
Aetna
33
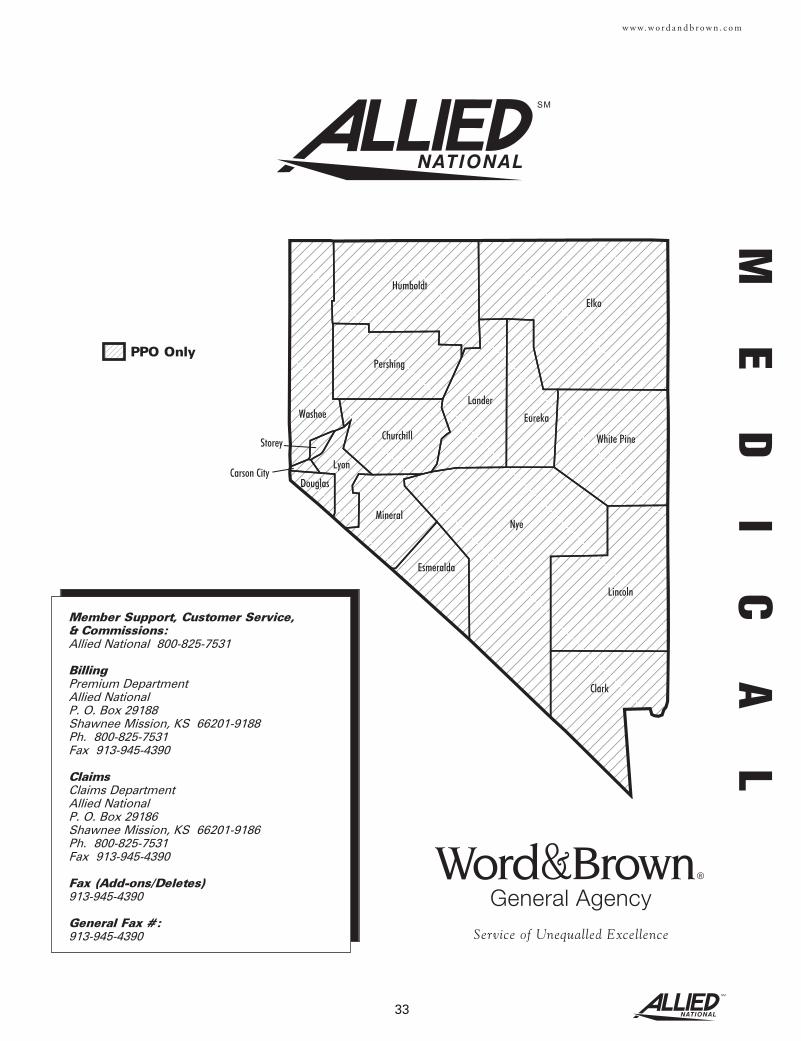
w w w. w o r d a n d b r o w n . c o m
Churchill
Clark
Douglas
Elko
Esmeralda
Eureka
Humboldt
Lander
Lincoln
Lyon
MineralNye
Pershing
Storey
Washoe
White Pine
Carson City
Member Support, Customer Service,& Commissions:Allied National 800-825-7531
BillingPremium DepartmentAllied NationalP. O. Box 29188Shawnee Mission, KS 66201-9188Ph. 800-825-7531Fax 913-945-4390
ClaimsClaims DepartmentAllied NationalP. O. Box 29186Shawnee Mission, KS 66201-9186Ph. 800-825-7531Fax 913-945-4390
Fax (Add-ons/Deletes)913-945-4390
General Fax #:913-945-4390
PPO Only
ME
DI
CA
L
LIFE
DENTAL
VISION
INFERTILITY
CHIROPRACTIC
ACUPUNCTURE
MASSAGE THERAPY
PRODUCTS OFFERED
OPTIONAL BENEFITS
GROUP SIZE
PROVIDER INFORMATION
34
w w w. w o r d a n d b r o w n . c o m
ALTERNATIVE DISCIPLINES
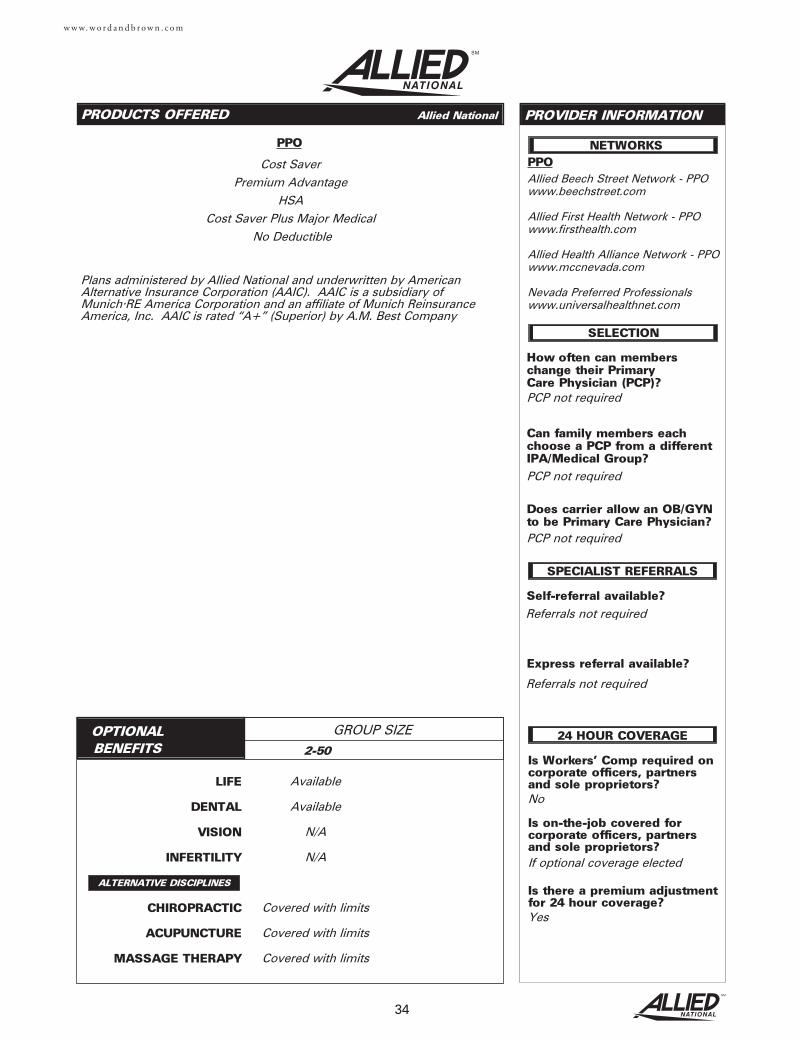
PPO
Is Workers' Comp required oncorporate officers, partnersand sole proprietors?No
Is on-the-job covered for corporate officers, partnersand sole proprietors?If optional coverage elected
Is there a premium adjustmentfor 24 hour coverage?Yes
How often can members change their Primary Care Physician (PCP)?
Can family members eachchoose a PCP from a differentIPA/Medical Group?
Does carrier allow an OB/GYNto be Primary Care Physician?
Self-referral available?
Express referral available?
SELECTION
SPECIALIST REFERRALS
NETWORKS
24 HOUR COVERAGE
PPO
Cost Saver
Premium Advantage
HSA
Cost Saver Plus Major Medical
No Deductible
Referrals not required
PCP not required
Allied Beech Street Network - PPOwww.beechstreet.com
Allied First Health Network - PPOwww.firsthealth.com
Allied Health Alliance Network - PPOwww.mccnevada.com
Nevada Preferred Professionalswww.universalhealthnet.com
Referrals not required
2-50
Available
Available
N/A
N/A
Covered with limits
Covered with limits
Covered with limits
Plans administered by Allied National and underwritten by AmericanAlternative Insurance Corporation (AAIC). AAIC is a subsidiary ofMunich•RE America Corporation and an affiliate of Munich ReinsuranceAmerica, Inc. AAIC is rated “A+” (Superior) by A.M. Best Company
PCP not required
PCP not required
Allied National
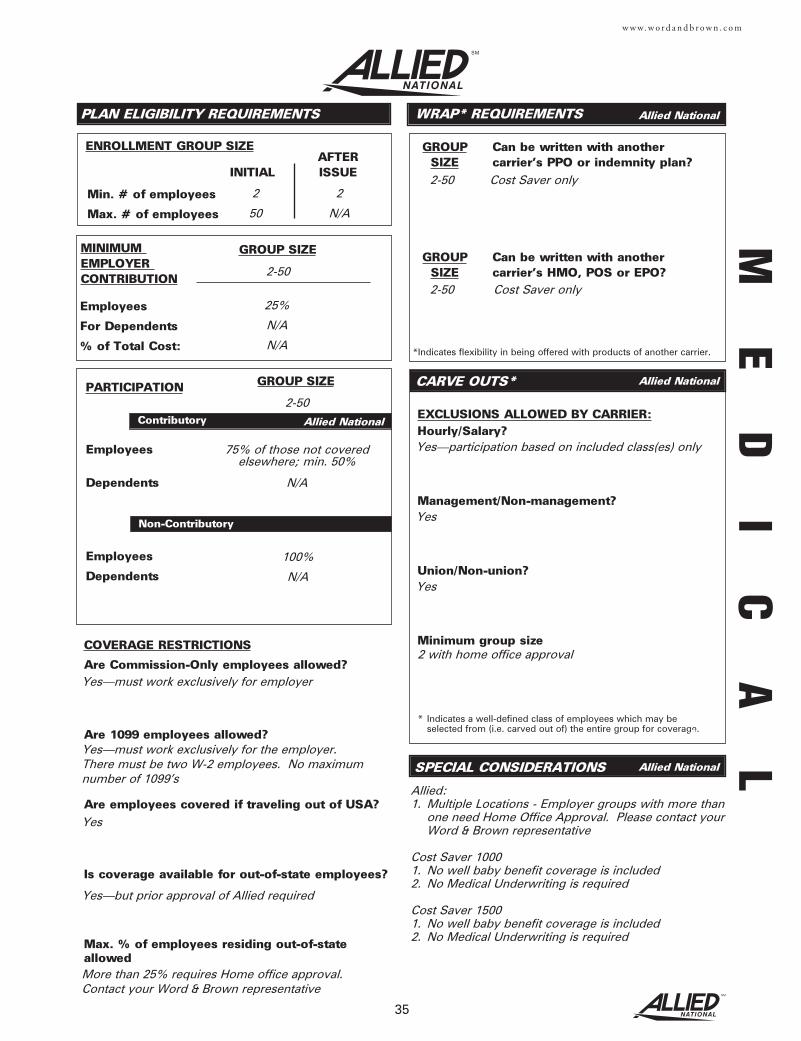
GROUP Can be written with another SIZE carrier's PPO or indemnity plan?
Employees
Dependents
Employees
Dependents
EXCLUSIONS ALLOWED BY CARRIER:Hourly/Salary?
Management/Non-management?
Union/Non-union?
Minimum group size2 with home office approval
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
ENROLLMENT GROUP SIZE
Employees
For Dependents
% of Total Cost:
PLAN ELIGIBILITY REQUIREMENTS
MINIMUM EMPLOYER CONTRIBUTION
PARTICIPATION
Min. # of employees
Max. # of employees
Contributory
Non-Contributory
GROUP SIZE
GROUP SIZE
AFTERINITIAL ISSUE
CARVE OUTS*
WRAP* REQUIREMENTS
*Indicates flexibility in being offered with products of another carrier.
GROUP Can be written with another SIZE carrier's HMO, POS or EPO?
SPECIAL CONSIDERATIONS
35
w w w. w o r d a n d b r o w n . c o m
COVERAGE RESTRICTIONS
Are Commission-Only employees allowed?
Are 1099 employees allowed?
Are employees covered if traveling out of USA?
Is coverage available for out-of-state employees?
Max. % of employees residing out-of-stateallowed
Yes—must work exclusively for employer
Yes—must work exclusively for the employer. There must be two W-2 employees. No maximumnumber of 1099’s
Yes
Yes—but prior approval of Allied required
More than 25% requires Home office approval. Contact your Word & Brown representative
100%
N/A
2-50
2-50 Cost Saver only
2-50 Cost Saver only
25%
N/A
N/A
75% of those not coveredelsewhere; min. 50%
N/A
2-50
2 2
50 N/A
Yes—participation based on included class(es) only
Yes
Yes
Allied:1. Multiple Locations - Employer groups with more than
one need Home Office Approval. Please contact yourWord & Brown representative
Cost Saver 10001. No well baby benefit coverage is included2. No Medical Underwriting is required
Cost Saver 15001. No well baby benefit coverage is included2. No Medical Underwriting is required
ME
DI
CA
LAllied National
Allied National
Allied National
Aetna
Allied National
MEDICAL UNDERWRITING REQUIREMENTS
Current Employees
TimelyAdd-ons
Group Size
Composite Rates
Rate Guarantee
Apply Trend Factor?
Use Employee Zips?
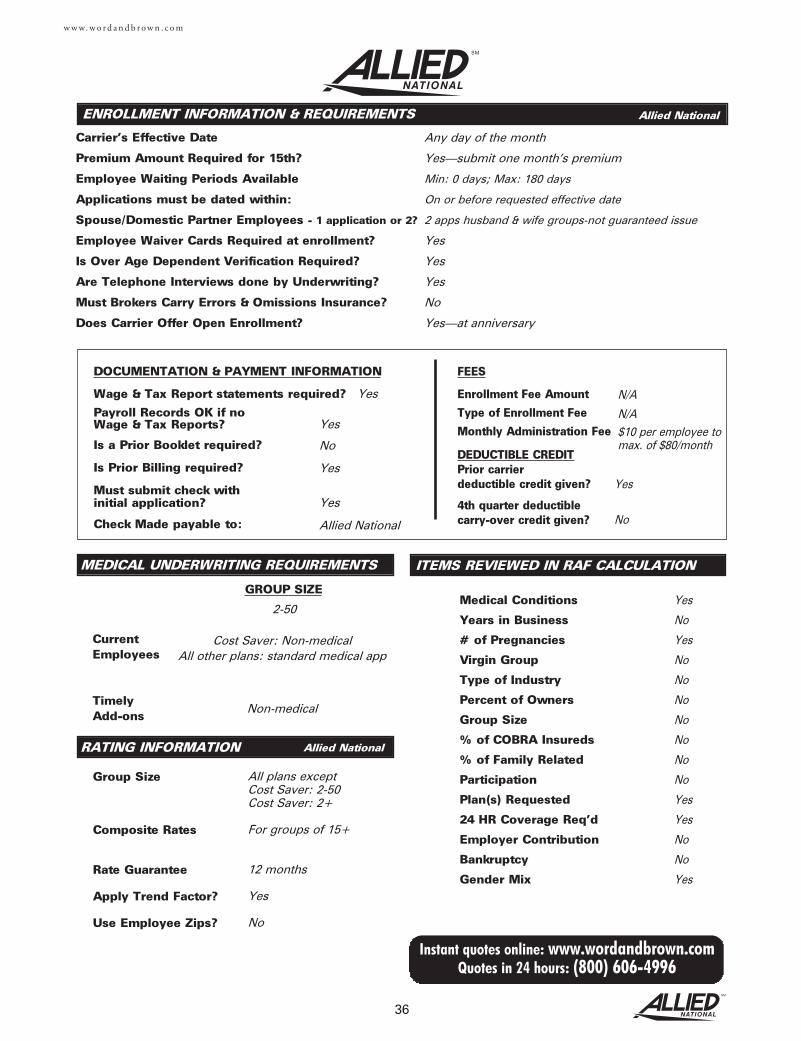
ENROLLMENT INFORMATION & REQUIREMENTS
Carrier's Effective Date
Premium Amount Required for 15th?
Employee Waiting Periods Available
Applications must be dated within:
Spouse/Domestic Partner Employees - 1 application or 2?
Employee Waiver Cards Required at enrollment?
Is Over Age Dependent Verification Required?
Are Telephone Interviews done by Underwriting?
Must Brokers Carry Errors & Omissions Insurance?
Does Carrier Offer Open Enrollment?
DOCUMENTATION & PAYMENT INFORMATION
Wage & Tax Report statements required?
Payroll Records OK if no Wage & Tax Reports?
Is a Prior Booklet required?
Is Prior Billing required?
Must submit check with initial application?
Check Made payable to:
FEES
Enrollment Fee Amount
Type of Enrollment Fee
Monthly Administration Fee
DEDUCTIBLE CREDITPrior carrier deductible credit given?
4th quarter deductiblecarry-over credit given?
GROUP SIZE
RATING INFORMATION
36
Instant quotes online: www.wordandbrown.comQuotes in 24 hours: (800) 606-4996
w w w. w o r d a n d b r o w n . c o m
ITEMS REVIEWED IN RAF CALCULATION
Medical Conditions
Years in Business
# of Pregnancies
Virgin Group
Type of Industry
Percent of Owners
Group Size
% of COBRA Insureds
% of Family Related
Participation
Plan(s) Requested
24 HR Coverage Req'd
Employer Contribution
Bankruptcy
Gender Mix
Any day of the month
Yes—submit one month’s premium
Min: 0 days; Max: 180 days
On or before requested effective date
2 apps husband & wife groups-not guaranteed issue
Yes
Yes
Yes
No
Yes—at anniversary
N/A
N/A$10 per employee tomax. of $80/month
Yes
No
Yes
No
No
No
No
No
No
No
Yes
Yes
No
No
Yes
Yes
No
Cost Saver: Non-medicalAll other plans: standard medical app
2-50
Yes
No
Yes
Yes
Allied National
All plans except Cost Saver: 2-50Cost Saver: 2+
For groups of 15+
12 months
Yes
No
Yes
Non-medical
Allied National
Allied National
Infertility
SPECIAL CONCERNS*
PREVENTIVE BENEFITS*
PRESCRIPTIONS
Adult Physical Child Physical Annual OB/GYNPLAN TYPE Exam Exam/Immunizations Visit/Pap Smear Mammography
GENERIC VS. BRAND NAMEIf generic available, and doctor has not indicated“dispense as written,” will member receive ageneric equivalent rather than a brand namedrug?
If doctor writes “dispense as written” on prescription, is brand name available at thebrand copay amount?
* Information shown in this section reflects in-network benefits. For Triple Option plans, the most managed plans are shown.
FORMULARY VS. NON-FORMULARYDoes carrier use Rx formulary?
Are non-formulary drugs available?
MAIL ORDER - 90 DAY SUPPLY
Are oral contraceptives covered?
* Unless otherwise noted, information shown in this section reflects in-network benefits. For Triple Option plans, the most managed plans are shown.
BENEFIT INFORMATION SHOWN ON THIS PAGE IS A BRIEF SUMMARY. LIMITATIONS AND EXCLUSIONS APPLY. PLEASE REFER TO CERTIFICATE BOOK, EVIDENCE OF COVERAGE OR CALL REPRESENTATIVE FOR DETAILS.
37
w w w. w o r d a n d b r o w n . c o m
Hearing treatment
Are Hearing Aids covered?
Speech therapy
Contact home office
Generic offered. If member chooses brand they paythe cost differential between brand and generic
Yes
Yes—at higher copay
2x copay
Yes
Cost Saver N/A Subject to Office Visit Benefit
Physical diagnosis or treatment of infertility: $500 lifetime benefit
20 visits/calendar year
Contact home office
All other plans Subject to OfficeVisit Benefit up to
$250/year
Subject to Office Visit Benefit
Yes
ME
DI
CA
LAllied National
Allied National
Allied National
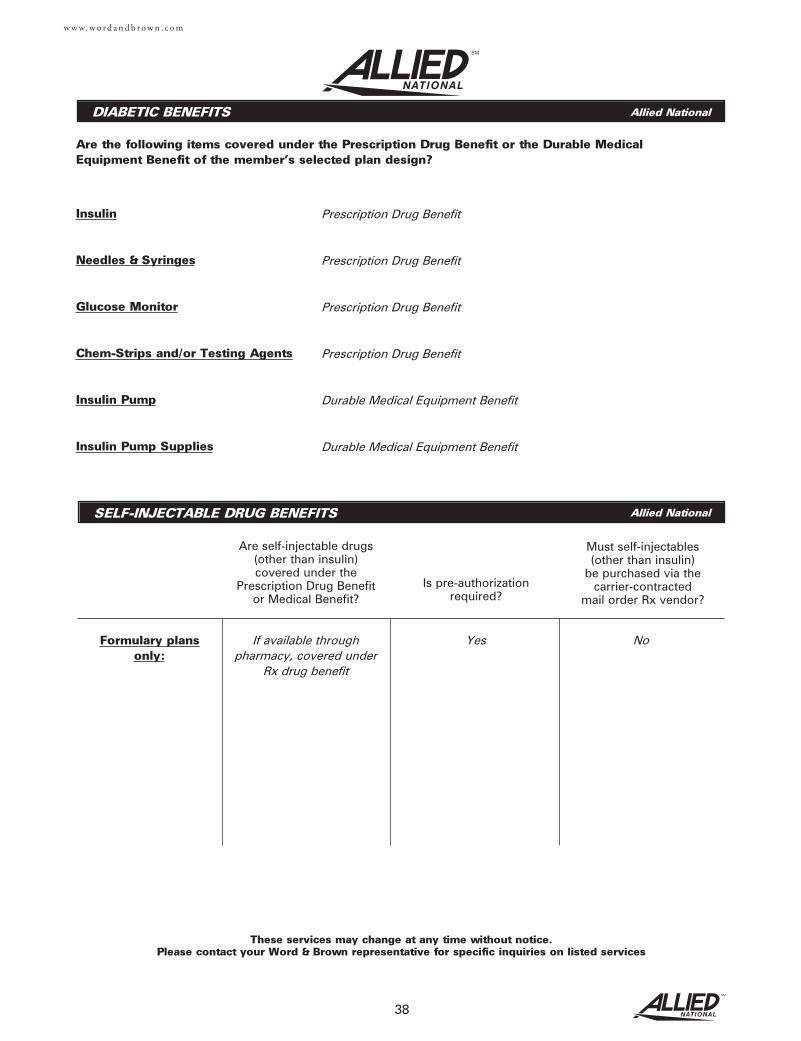
DIABETIC BENEFITS
These services may change at any time without notice. Please contact your Word & Brown representative for specific inquiries on listed services
38
Are the following items covered under the Prescription Drug Benefit or the Durable MedicalEquipment Benefit of the member’s selected plan design?
w w w. w o r d a n d b r o w n . c o m
Insulin
Needles & Syringes
Glucose Monitor
Chem-Strips and/or Testing Agents
Insulin Pump
Insulin Pump Supplies
SELF-INJECTABLE DRUG BENEFITS
Are self-injectable drugs(other than insulin)covered under the
Prescription Drug Benefitor Medical Benefit?
Is pre-authorizationrequired?
Must self-injectables(other than insulin)
be purchased via thecarrier-contracted
mail order Rx vendor?
Prescription Drug Benefit
Prescription Drug Benefit
Prescription Drug Benefit
Prescription Drug Benefit
Durable Medical Equipment Benefit
Durable Medical Equipment Benefit
If available through pharmacy, covered under
Rx drug benefit
Yes NoFormulary plansonly:
Allied National
Allied National
39
w w w. w o r d a n d b r o w n . c o m
Churchill
Clark
Douglas
Elko
Esmeralda
Eureka
Humboldt
Lander
Lincoln
Lyon
MineralNye
Pershing
Storey
Washoe
White Pine
Carson City
Member Support877-833-5734
Broker Support888-445-9236Fax [email protected]
Fax (Adds/Terms)303-831-2399
Commissions888-445-9236
BillingAnthem Blue Cross and Blue Shield P.O. Box 541013 Los Angeles, CA 90054-1013800-922-4770Fax 303-831-2399
ClaimsAnthem Blue Cross and Blue Shield P.O. Box 5747 Denver, CO 80217-5747877-833-5734
www.anthem.com
ME
DI
CA
L
Plan may not be available in all zip codes within county. Contact your Word & Brown representativeto confirm if coverage isavailable for your grouplocation
HMO & PPO Counties
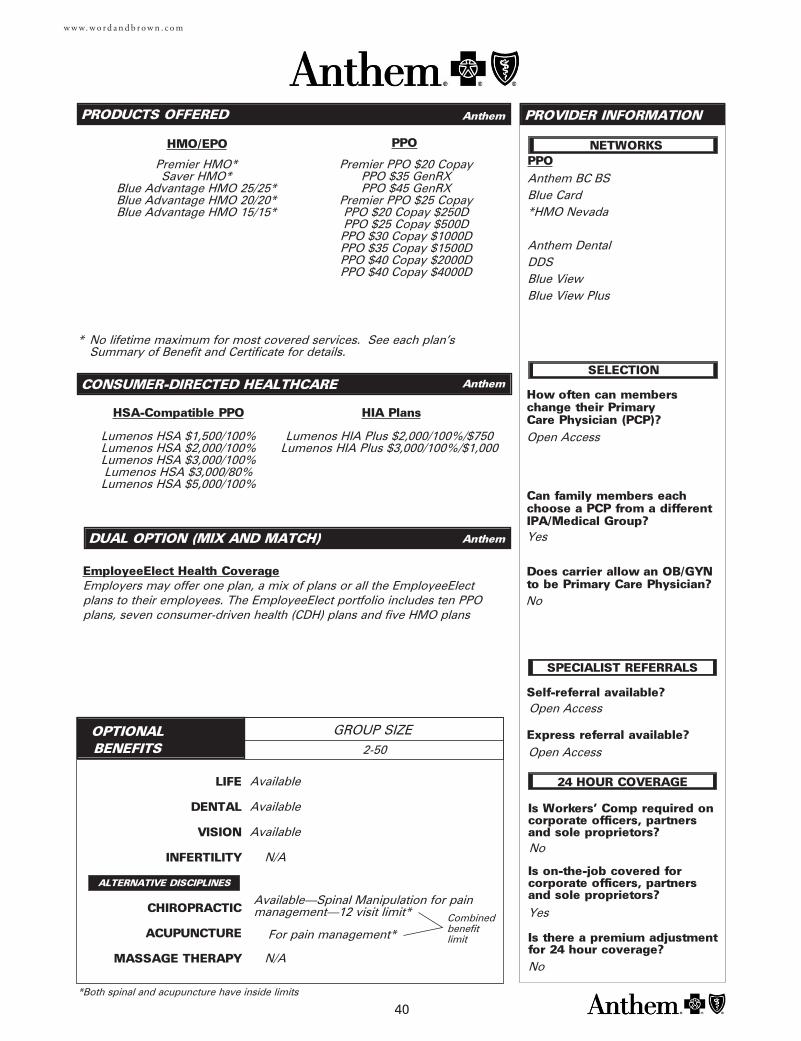
LIFE
DENTAL
VISION
INFERTILITY
CHIROPRACTIC
ACUPUNCTURE
MASSAGE THERAPY
PRODUCTS OFFERED
OPTIONAL BENEFITS
GROUP SIZE
PROVIDER INFORMATION
HMO/EPO
40
CONSUMER-DIRECTED HEALTHCARE
HSA-Compatible PPO
w w w. w o r d a n d b r o w n . c o m
ALTERNATIVE DISCIPLINES
Premier HMO*Saver HMO*
Blue Advantage HMO 25/25*Blue Advantage HMO 20/20*Blue Advantage HMO 15/15*
PPO
Premier PPO $20 CopayPPO $35 GenRXPPO $45 GenRX
Premier PPO $25 CopayPPO $20 Copay $250DPPO $25 Copay $500DPPO $30 Copay $1000DPPO $35 Copay $1500DPPO $40 Copay $2000DPPO $40 Copay $4000D
Lumenos HSA $1,500/100%Lumenos HSA $2,000/100%Lumenos HSA $3,000/100%Lumenos HSA $3,000/80%Lumenos HSA $5,000/100%
HIA Plans
Lumenos HIA Plus $2,000/100%/$750Lumenos HIA Plus $3,000/100%/$1,000
PPO
Is Workers' Comp required oncorporate officers, partnersand sole proprietors?
Is on-the-job covered for corporate officers, partnersand sole proprietors?
Is there a premium adjustmentfor 24 hour coverage?
How often can members change their Primary Care Physician (PCP)?
Can family members eachchoose a PCP from a differentIPA/Medical Group?
Does carrier allow an OB/GYNto be Primary Care Physician?
Self-referral available?
Express referral available?Open Access
Open Access
SELECTION
SPECIALIST REFERRALS
NETWORKS
Open Access
24 HOUR COVERAGE
Anthem BC BS Blue Card*HMO Nevada
Anthem DentalDDSBlue ViewBlue View Plus
Yes
No
Available
Available
Available
N/A
N/A
2-50
Yes
No
No
Available—Spinal Manipulation for painmanagement—12 visit limit*
For pain management*
*Both spinal and acupuncture have inside limits
Combinedbenefitlimit
* No lifetime maximum for most covered services. See each plan’s Summary of Benefit and Certificate for details.
DUAL OPTION (MIX AND MATCH)
EmployeeElect Health CoverageEmployers may offer one plan, a mix of plans or all the EmployeeElectplans to their employees. The EmployeeElect portfolio includes ten PPOplans, seven consumer-driven health (CDH) plans and five HMO plans
Anthem
Anthem
Anthem
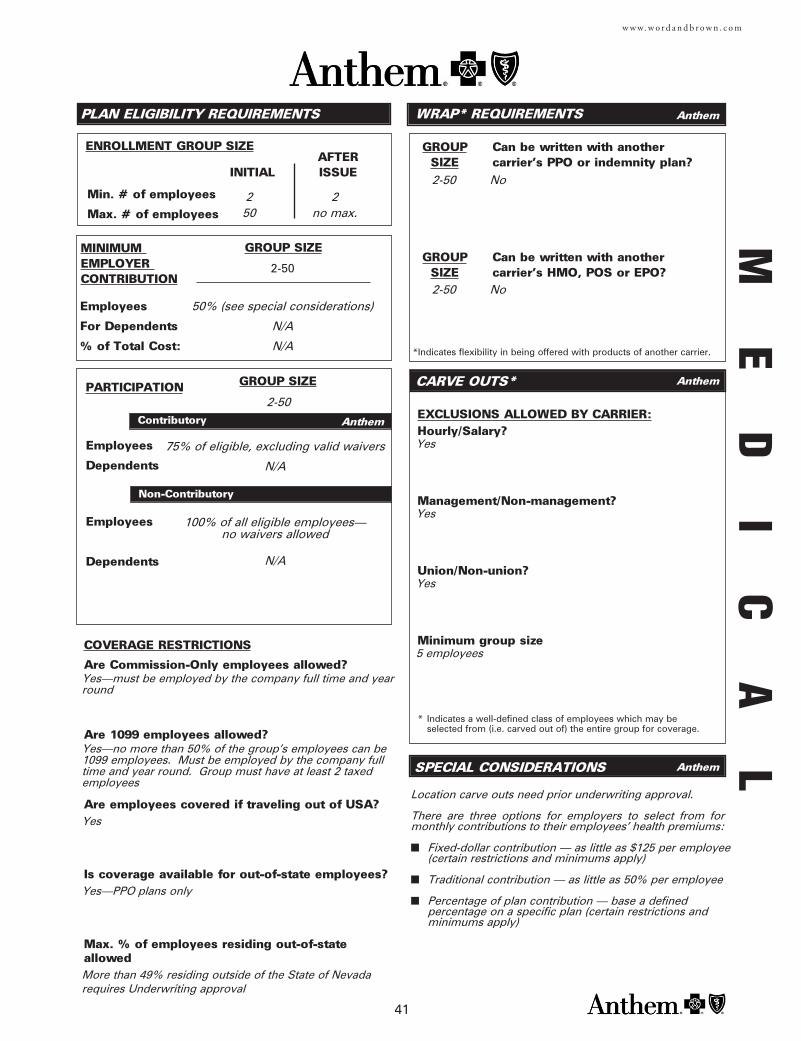
GROUP Can be written with another SIZE carrier's PPO or indemnity plan?
Employees
Dependents
Employees
Dependents
EXCLUSIONS ALLOWED BY CARRIER:Hourly/Salary?
Management/Non-management?
Union/Non-union?
Minimum group size
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
ENROLLMENT GROUP SIZE
Employees
For Dependents
% of Total Cost:
PLAN ELIGIBILITY REQUIREMENTS
MINIMUM EMPLOYER CONTRIBUTION
PARTICIPATION
Min. # of employees
Max. # of employees
Contributory
Non-Contributory
GROUP SIZE
GROUP SIZE
AFTERINITIAL ISSUE
CARVE OUTS*
WRAP* REQUIREMENTS
*Indicates flexibility in being offered with products of another carrier.
GROUP Can be written with another SIZE carrier's HMO, POS or EPO?
SPECIAL CONSIDERATIONS
41
w w w. w o r d a n d b r o w n . c o m
COVERAGE RESTRICTIONS
Are Commission-Only employees allowed?
Are 1099 employees allowed?
Are employees covered if traveling out of USA?
Is coverage available for out-of-state employees?
Max. % of employees residing out-of-stateallowed
Yes—must be employed by the company full time and yearround
Yes—no more than 50% of the group’s employees can be1099 employees. Must be employed by the company fulltime and year round. Group must have at least 2 taxedemployees
Yes
Yes—PPO plans only
More than 49% residing outside of the State of Nevadarequires Underwriting approval
2-50
2-50 No
2-50 No
50% (see special considerations)
N/A
N/A
75% of eligible, excluding valid waivers
N/A
Yes
Yes
Yes
5 employees
Location carve outs need prior underwriting approval.
There are three options for employers to select from formonthly contributions to their employees’ health premiums:
■ Fixed-dollar contribution — as little as $125 per employee(certain restrictions and minimums apply)
■ Traditional contribution — as little as 50% per employee
■ Percentage of plan contribution — base a defined percentage on a specific plan (certain restrictions and minimums apply)
2 250 no max.
2-50
100% of all eligible employees—no waivers allowed
N/A
ME
DI
CA
LAnthem
Anthem
Anthem
Anthem
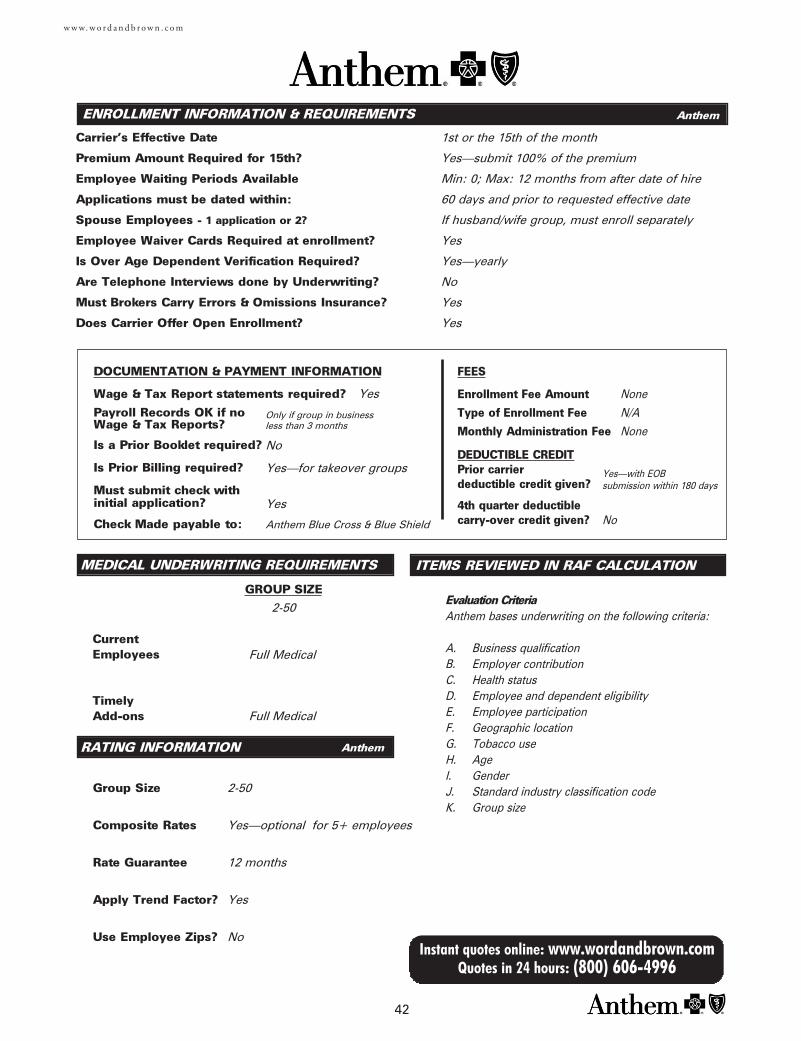
MEDICAL UNDERWRITING REQUIREMENTS
Current Employees
TimelyAdd-ons
Group Size
Composite Rates
Rate Guarantee
Apply Trend Factor?
Use Employee Zips?
ENROLLMENT INFORMATION & REQUIREMENTS
Carrier's Effective Date
Premium Amount Required for 15th?
Employee Waiting Periods Available
Applications must be dated within:
Spouse Employees - 1 application or 2?
Employee Waiver Cards Required at enrollment?
Is Over Age Dependent Verification Required?
Are Telephone Interviews done by Underwriting?
Must Brokers Carry Errors & Omissions Insurance?
Does Carrier Offer Open Enrollment?
DOCUMENTATION & PAYMENT INFORMATION
Wage & Tax Report statements required?
Payroll Records OK if no Wage & Tax Reports?
Is a Prior Booklet required?
Is Prior Billing required?
Must submit check with initial application?
Check Made payable to:
FEES
Enrollment Fee Amount
Type of Enrollment Fee
Monthly Administration Fee
DEDUCTIBLE CREDITPrior carrier deductible credit given?
4th quarter deductiblecarry-over credit given?
GROUP SIZE
RATING INFORMATION
42
Instant quotes online: www.wordandbrown.comQuotes in 24 hours: (800) 606-4996
w w w. w o r d a n d b r o w n . c o m
ITEMS REVIEWED IN RAF CALCULATION
1st or the 15th of the month
Yes—submit 100% of the premium
Min: 0; Max: 12 months from after date of hire
60 days and prior to requested effective date
If husband/wife group, must enroll separately
Yes
Yes—yearly
No
Yes
Yes
Full Medical
No
Yes—for takeover groups
Yes
Anthem Blue Cross & Blue Shield
Full Medical
2-50
Yes—optional for 5+ employees
12 months
Yes
No
Yes
2-50
Only if group in businessless than 3 months
None
N/A
None
Yes—with EOB submission within 180 days
No
Evaluation CriteriaAnthem bases underwriting on the following criteria:
A. Business qualification B. Employer contribution C. Health status D. Employee and dependent eligibilityE. Employee participationF. Geographic locationG. Tobacco useH. AgeI. GenderJ. Standard industry classification codeK. Group size
Anthem
Anthem
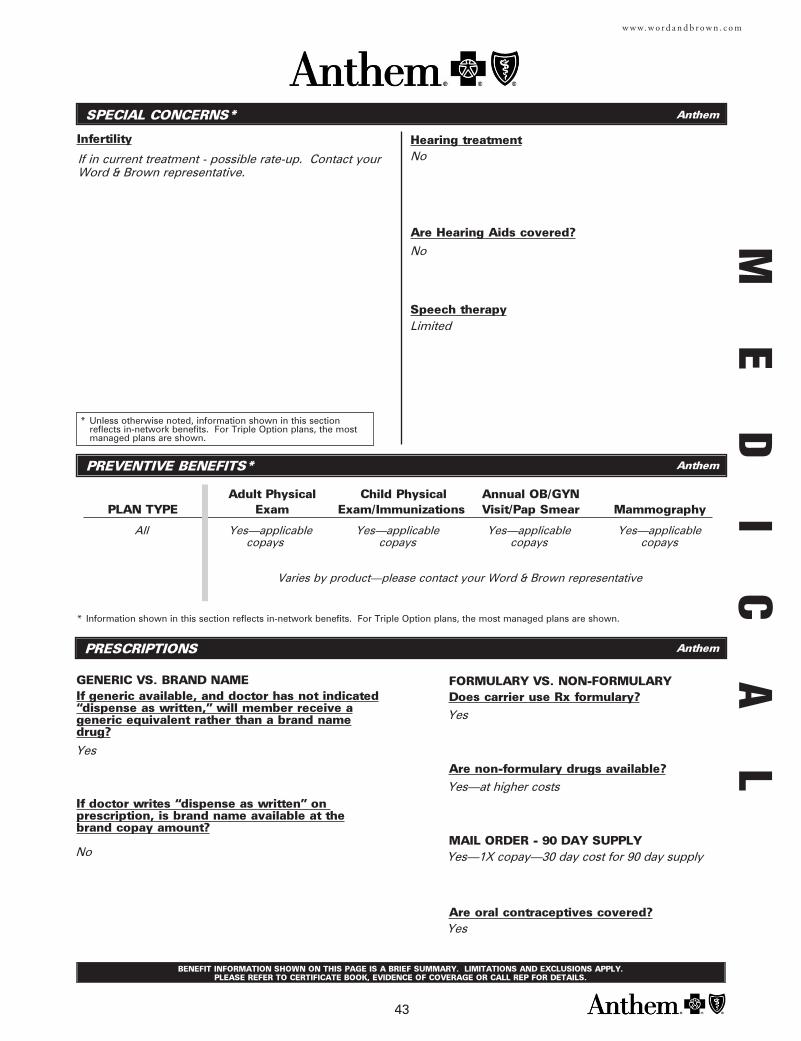
SPECIAL CONCERNS*
Infertility
PREVENTIVE BENEFITS*
PRESCRIPTIONS
Adult Physical Child Physical Annual OB/GYNPLAN TYPE Exam Exam/Immunizations Visit/Pap Smear Mammography
GENERIC VS. BRAND NAMEIf generic available, and doctor has not indicated“dispense as written,” will member receive ageneric equivalent rather than a brand namedrug?
If doctor writes “dispense as written” on prescription, is brand name available at thebrand copay amount?
* Information shown in this section reflects in-network benefits. For Triple Option plans, the most managed plans are shown.
FORMULARY VS. NON-FORMULARYDoes carrier use Rx formulary?
Are non-formulary drugs available?
MAIL ORDER - 90 DAY SUPPLY
Are oral contraceptives covered?
* Unless otherwise noted, information shown in this section reflects in-network benefits. For Triple Option plans, the most managed plans are shown.
BENEFIT INFORMATION SHOWN ON THIS PAGE IS A BRIEF SUMMARY. LIMITATIONS AND EXCLUSIONS APPLY. PLEASE REFER TO CERTIFICATE BOOK, EVIDENCE OF COVERAGE OR CALL REP FOR DETAILS.
43
w w w. w o r d a n d b r o w n . c o m
Hearing treatment
Are Hearing Aids covered?
Speech therapy
No
Yes
Yes—at higher costs
Yes—1X copay—30 day cost for 90 day supply
Yes
All Yes—applicablecopays
If in current treatment - possible rate-up. Contact yourWord & Brown representative.
Yes
No
Yes—applicablecopays
Yes—applicablecopays
Yes—applicablecopays
No
Limited
Varies by product—please contact your Word & Brown representative
ME
DI
CA
LAnthem
Anthem
Anthem
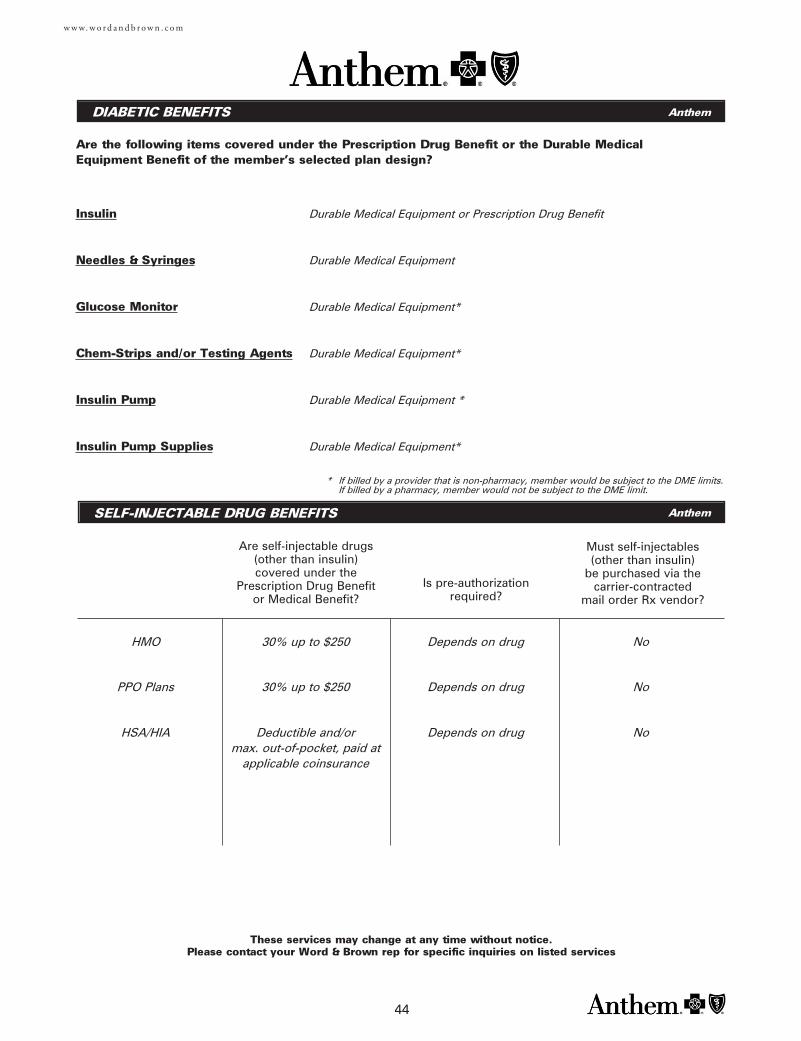
DIABETIC BENEFITS
These services may change at any time without notice. Please contact your Word & Brown rep for specific inquiries on listed services
44
Are the following items covered under the Prescription Drug Benefit or the Durable MedicalEquipment Benefit of the member’s selected plan design?
w w w. w o r d a n d b r o w n . c o m
Insulin
Needles & Syringes
Glucose Monitor
Chem-Strips and/or Testing Agents
Insulin Pump
Insulin Pump Supplies
SELF-INJECTABLE DRUG BENEFITS
Are self-injectable drugs(other than insulin)covered under the
Prescription Drug Benefitor Medical Benefit?
Is pre-authorizationrequired?
Must self-injectables(other than insulin)
be purchased via thecarrier-contracted
mail order Rx vendor?
Durable Medical Equipment or Prescription Drug Benefit
Durable Medical Equipment
Durable Medical Equipment*
Durable Medical Equipment*
Durable Medical Equipment *
Durable Medical Equipment*
30% up to $250 Depends on drug NoPPO Plans
30% up to $250 Depends on drug NoHMO
Deductible and/or max. out-of-pocket, paid at
applicable coinsurance
Depends on drug NoHSA/HIA
* If billed by a provider that is non-pharmacy, member would be subject to the DME limits. If billed by a pharmacy, member would not be subject to the DME limit.
Anthem
Anthem
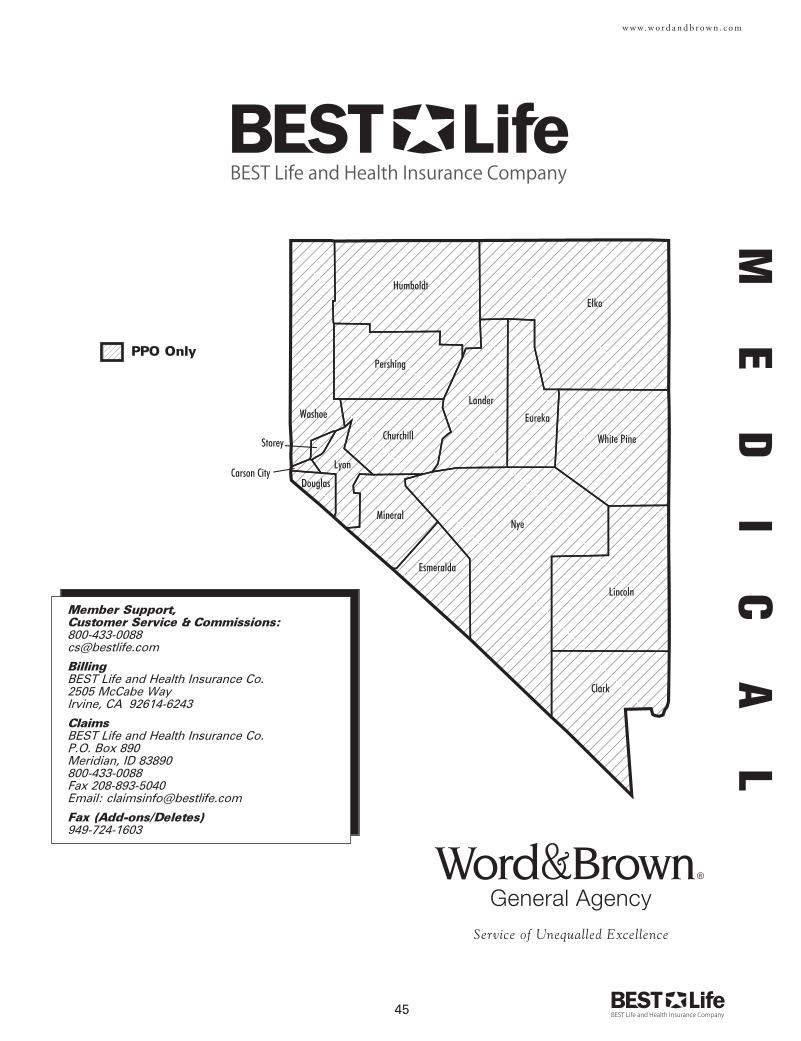
45
w w w. w o r d a n d b r o w n . c o m
Churchill
Clark
Douglas
Elko
Esmeralda
Eureka
Humboldt
Lander
Lincoln
Lyon
MineralNye
Pershing
Storey
Washoe
White Pine
Carson City
Member Support, Customer Service & Commissions:[email protected]
BillingBEST Life and Health Insurance Co. 2505 McCabe WayIrvine, CA 92614-6243
ClaimsBEST Life and Health Insurance Co. P.O. Box 890Meridian, ID 83890800-433-0088Fax 208-893-5040Email: [email protected]
Fax (Add-ons/Deletes)949-724-1603
ME
DI
CA
L
PPO Only
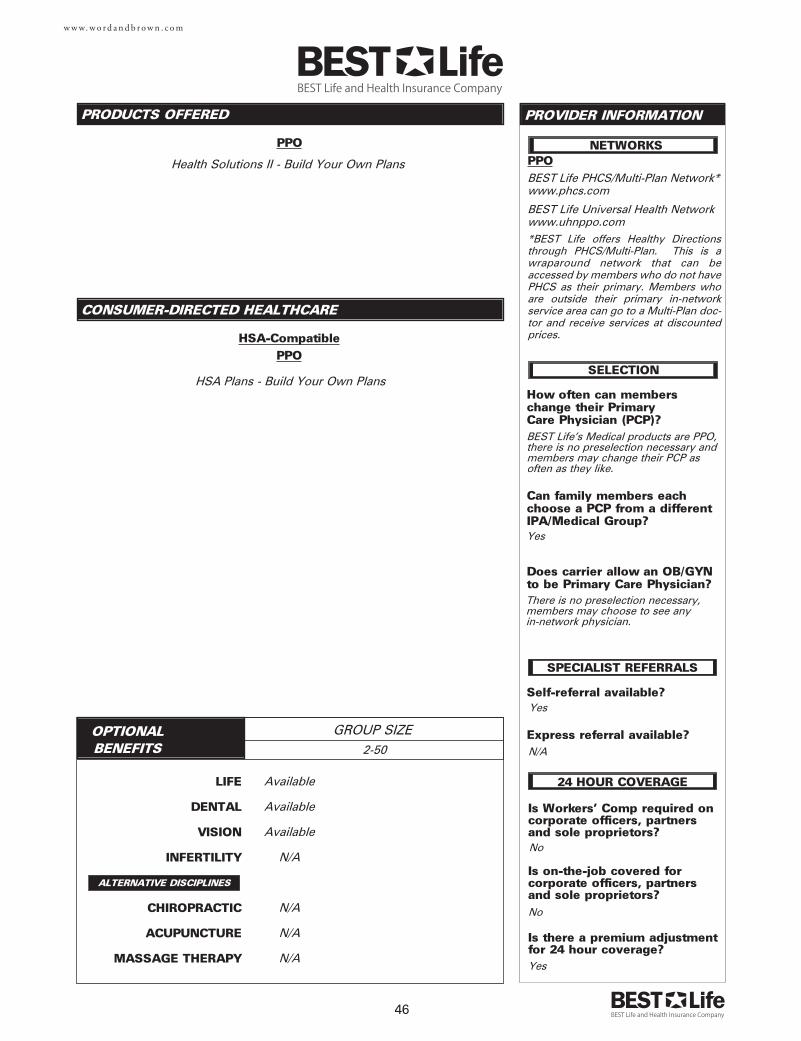
LIFE
DENTAL
VISION
INFERTILITY
CHIROPRACTIC
ACUPUNCTURE
MASSAGE THERAPY
PRODUCTS OFFERED
OPTIONAL BENEFITS
GROUP SIZE
PROVIDER INFORMATION
46
CONSUMER-DIRECTED HEALTHCARE
w w w. w o r d a n d b r o w n . c o m
ALTERNATIVE DISCIPLINES
PPO
Is Workers' Comp required oncorporate officers, partnersand sole proprietors?
Is on-the-job covered for corporate officers, partnersand sole proprietors?
Is there a premium adjustmentfor 24 hour coverage?
How often can members change their Primary Care Physician (PCP)?
Can family members eachchoose a PCP from a differentIPA/Medical Group?
Does carrier allow an OB/GYNto be Primary Care Physician?
Self-referral available?
Express referral available?N/A
Yes
SELECTION
SPECIALIST REFERRALS
NETWORKS
BEST Life's Medical products are PPO,there is no preselection necessary andmembers may change their PCP asoften as they like.
24 HOUR COVERAGE
BEST Life PHCS/Multi-Plan Network*www.phcs.com
BEST Life Universal Health Networkwww.uhnppo.com*BEST Life offers Healthy Directionsthrough PHCS/Multi-Plan. This is awraparound network that can beaccessed by members who do not havePHCS as their primary. Members whoare outside their primary in-networkservice area can go to a Multi-Plan doc-tor and receive services at discountedprices.
Yes
There is no preselection necessary,members may choose to see any in-network physician.
Available
Available
Available
N/A
N/A
N/A
N/A
2-50
Health Solutions II - Build Your Own Plans
HSA Plans - Build Your Own Plans
No
No
Yes
PPO
HSA-CompatiblePPO
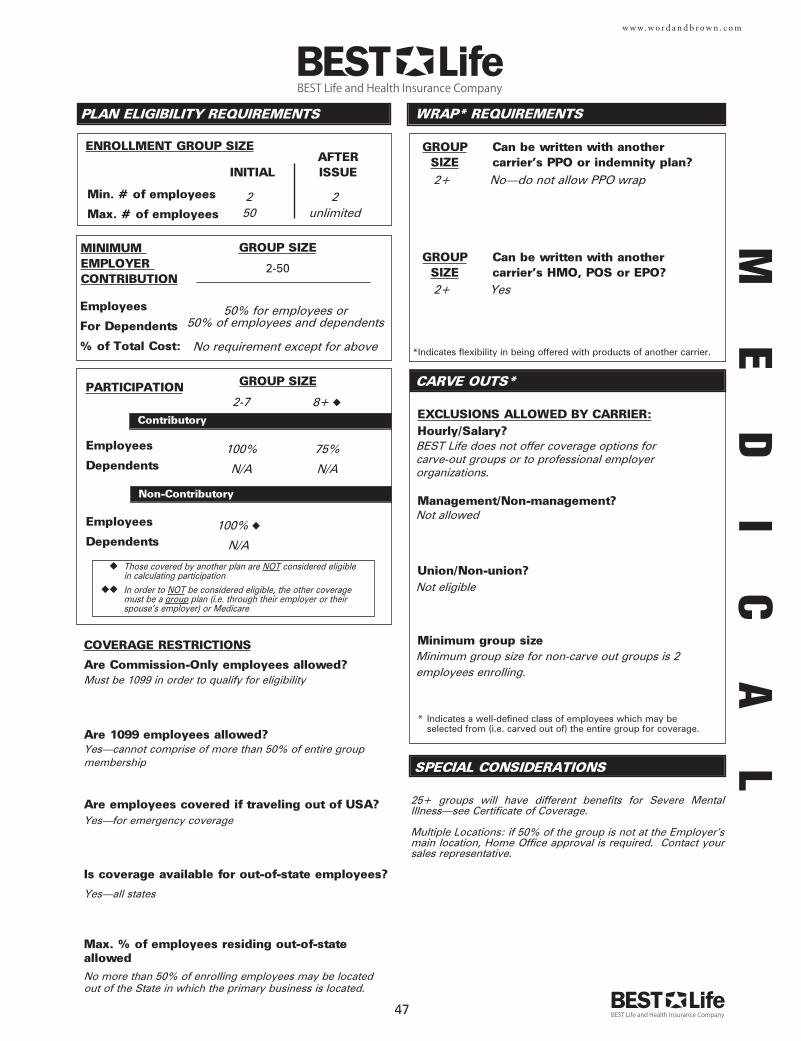
GROUP Can be written with another SIZE carrier's PPO or indemnity plan?
Employees
Dependents
Employees
Dependents
EXCLUSIONS ALLOWED BY CARRIER:Hourly/Salary?
Management/Non-management?
Union/Non-union?
Minimum group size
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
ENROLLMENT GROUP SIZE
Employees
For Dependents
% of Total Cost:
PLAN ELIGIBILITY REQUIREMENTS
MINIMUM EMPLOYER CONTRIBUTION
PARTICIPATION
Min. # of employees
Max. # of employees
Contributory
Non-Contributory
GROUP SIZE
GROUP SIZE
AFTERINITIAL ISSUE
CARVE OUTS*
WRAP* REQUIREMENTS
*Indicates flexibility in being offered with products of another carrier.
GROUP Can be written with another SIZE carrier's HMO, POS or EPO?
SPECIAL CONSIDERATIONS
47
w w w. w o r d a n d b r o w n . c o m
COVERAGE RESTRICTIONS
Are Commission-Only employees allowed?
Are 1099 employees allowed?
Are employees covered if traveling out of USA?
Is coverage available for out-of-state employees?
Max. % of employees residing out-of-stateallowed
Must be 1099 in order to qualify for eligibility
Yes—cannot comprise of more than 50% of entire group membership
Yes—for emergency coverage
Yes—all states
No more than 50% of enrolling employees may be located out of the State in which the primary business is located.
100% ◆
N/A
2-7
2+ Yes
2+ No—do not allow PPO wrap
50% for employees or50% of employees and dependents
100%
N/A
BEST Life does not offer coverage options for carve-out groups or to professional employerorganizations.
Not allowed
Not eligible
Minimum group size for non-carve out groups is 2employees enrolling.
25+ groups will have different benefits for Severe MentalIllness—see Certificate of Coverage.
Multiple Locations: if 50% of the group is not at the Employer’smain location, Home Office approval is required. Contact yoursales representative.
No requirement except for above
8+ ◆
75%
N/A
◆ Those covered by another plan are NOT considered eligible in calculating participation
◆◆ In order to NOT be considered eligible, the other coveragemust be a group plan (i.e. through their employer or their spouse's employer) or Medicare
2 250 unlimited
2-50
ME
DI
CA
L
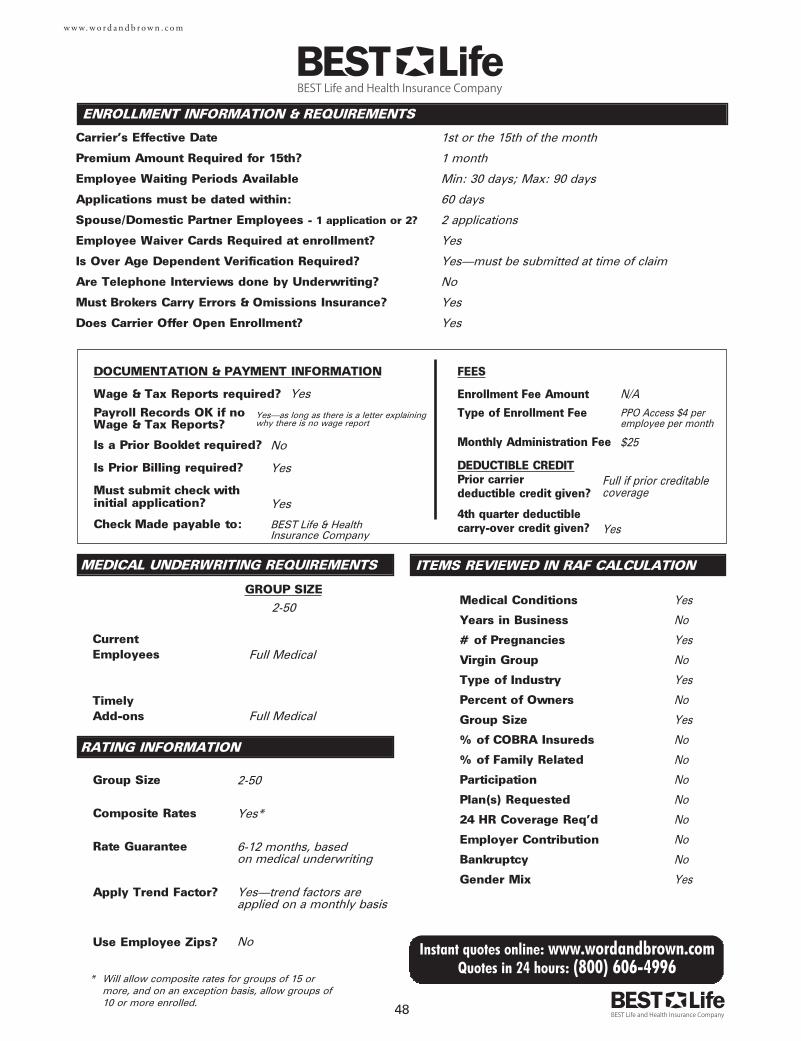
MEDICAL UNDERWRITING REQUIREMENTS
Current Employees
TimelyAdd-ons
Group Size
Composite Rates
Rate Guarantee
Apply Trend Factor?
Use Employee Zips?
ENROLLMENT INFORMATION & REQUIREMENTS
Carrier's Effective Date
Premium Amount Required for 15th?
Employee Waiting Periods Available
Applications must be dated within:
Spouse/Domestic Partner Employees - 1 application or 2?
Employee Waiver Cards Required at enrollment?
Is Over Age Dependent Verification Required?
Are Telephone Interviews done by Underwriting?
Must Brokers Carry Errors & Omissions Insurance?
Does Carrier Offer Open Enrollment?
DOCUMENTATION & PAYMENT INFORMATION
Wage & Tax Reports required?
Payroll Records OK if no Wage & Tax Reports?
Is a Prior Booklet required?
Is Prior Billing required?
Must submit check with initial application?
Check Made payable to:
FEES
Enrollment Fee Amount
Type of Enrollment Fee
Monthly Administration Fee
DEDUCTIBLE CREDITPrior carrier deductible credit given?
4th quarter deductiblecarry-over credit given?
GROUP SIZE
RATING INFORMATION
48
Instant quotes online: www.wordandbrown.comQuotes in 24 hours: (800) 606-4996
w w w. w o r d a n d b r o w n . c o m
ITEMS REVIEWED IN RAF CALCULATION
Medical Conditions
Years in Business
# of Pregnancies
Virgin Group
Type of Industry
Percent of Owners
Group Size
% of COBRA Insureds
% of Family Related
Participation
Plan(s) Requested
24 HR Coverage Req'd
Employer Contribution
Bankruptcy
Gender Mix
1st or the 15th of the month
1 month
Min: 30 days; Max: 90 days
60 days
2 applications
Yes
Yes—must be submitted at time of claim
No
Yes
Yes
N/A
PPO Access $4 peremployee per month
$25
Yes
No
Yes
No
Yes
No
Yes
No
No
No
No
No
No
No
Yes
Full if prior creditablecoverage
Full Medical
No
Yes
Yes
BEST Life & Health Insurance Company
Full Medical
2-50
Yes*
6-12 months, based on medical underwriting
Yes—trend factors areapplied on a monthly basis
No
Yes
Yes—as long as there is a letter explainingwhy there is no wage report
Yes
* Will allow composite rates for groups of 15 or more, and on an exception basis, allow groups of10 or more enrolled.
2-50
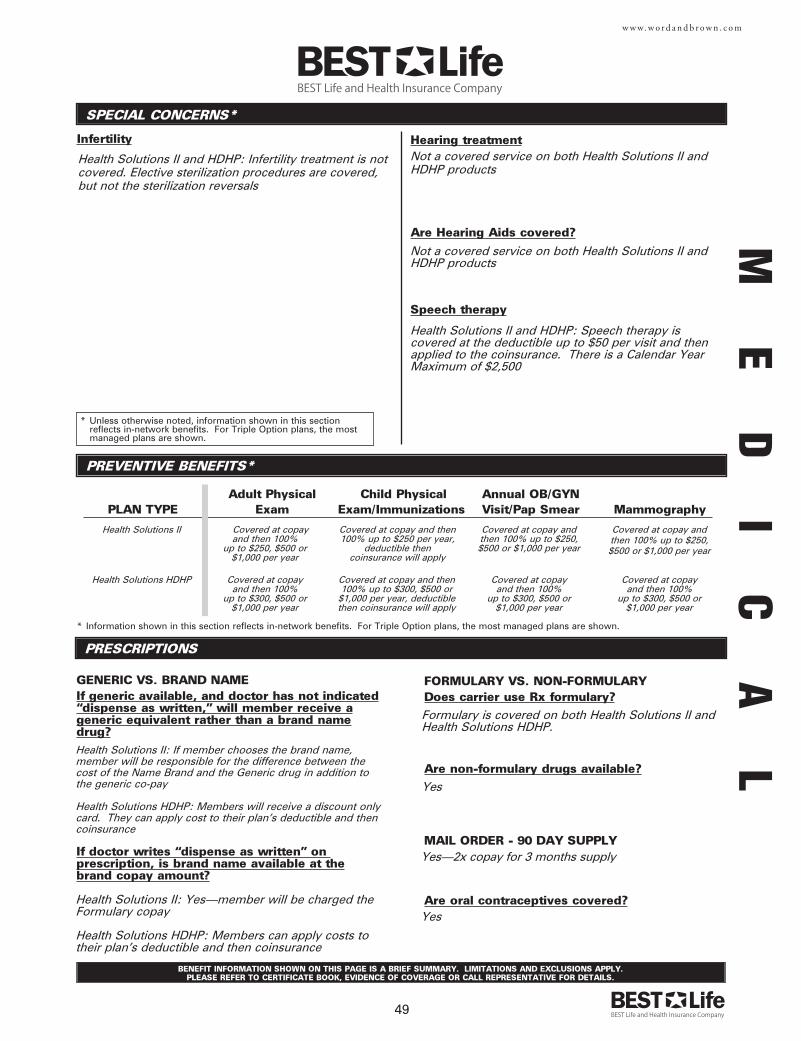
SPECIAL CONCERNS*
Infertility
PREVENTIVE BENEFITS*
PRESCRIPTIONS
Adult Physical Child Physical Annual OB/GYNPLAN TYPE Exam Exam/Immunizations Visit/Pap Smear Mammography
GENERIC VS. BRAND NAMEIf generic available, and doctor has not indicated“dispense as written,” will member receive ageneric equivalent rather than a brand namedrug?
If doctor writes “dispense as written” on prescription, is brand name available at thebrand copay amount?
* Information shown in this section reflects in-network benefits. For Triple Option plans, the most managed plans are shown.
FORMULARY VS. NON-FORMULARYDoes carrier use Rx formulary?
Are non-formulary drugs available?
MAIL ORDER - 90 DAY SUPPLY
Are oral contraceptives covered?
* Unless otherwise noted, information shown in this section reflects in-network benefits. For Triple Option plans, the most managed plans are shown.
BENEFIT INFORMATION SHOWN ON THIS PAGE IS A BRIEF SUMMARY. LIMITATIONS AND EXCLUSIONS APPLY. PLEASE REFER TO CERTIFICATE BOOK, EVIDENCE OF COVERAGE OR CALL REPRESENTATIVE FOR DETAILS.
49
w w w. w o r d a n d b r o w n . c o m
Hearing treatment
Are Hearing Aids covered?
Speech therapy
Not a covered service on both Health Solutions II andHDHP products
Formulary is covered on both Health Solutions II andHealth Solutions HDHP.
Yes
Yes—2x copay for 3 months supply
Yes
Health Solutions II Covered at copay and then 100%
up to $250, $500 or$1,000 per year
Health Solutions II and HDHP: Infertility treatment is notcovered. Elective sterilization procedures are covered,but not the sterilization reversals
Health Solutions II: If member chooses the brand name,member will be responsible for the difference between thecost of the Name Brand and the Generic drug in addition tothe generic co-pay
Health Solutions HDHP: Members will receive a discount onlycard. They can apply cost to their plan's deductible and thencoinsurance
Not a covered service on both Health Solutions II andHDHP products
Covered at copay and then100% up to $250 per year,
deductible then coinsurance will apply
Covered at copay andthen 100% up to $250,$500 or $1,000 per year
Covered at copay andthen 100% up to $250,$500 or $1,000 per year
Health Solutions II: Yes—member will be charged theFormulary copay
Health Solutions HDHP: Members can apply costs totheir plan's deductible and then coinsurance
Health Solutions II and HDHP: Speech therapy iscovered at the deductible up to $50 per visit and thenapplied to the coinsurance. There is a Calendar YearMaximum of $2,500
ME
DI
CA
L
Health Solutions HDHP Covered at copay and then 100%
up to $300, $500 or $1,000 per year
Covered at copay and then100% up to $300, $500 or
$1,000 per year, deductiblethen coinsurance will apply
Covered at copay and then 100%
up to $300, $500 or $1,000 per year
Covered at copay and then 100%
up to $300, $500 or $1,000 per year
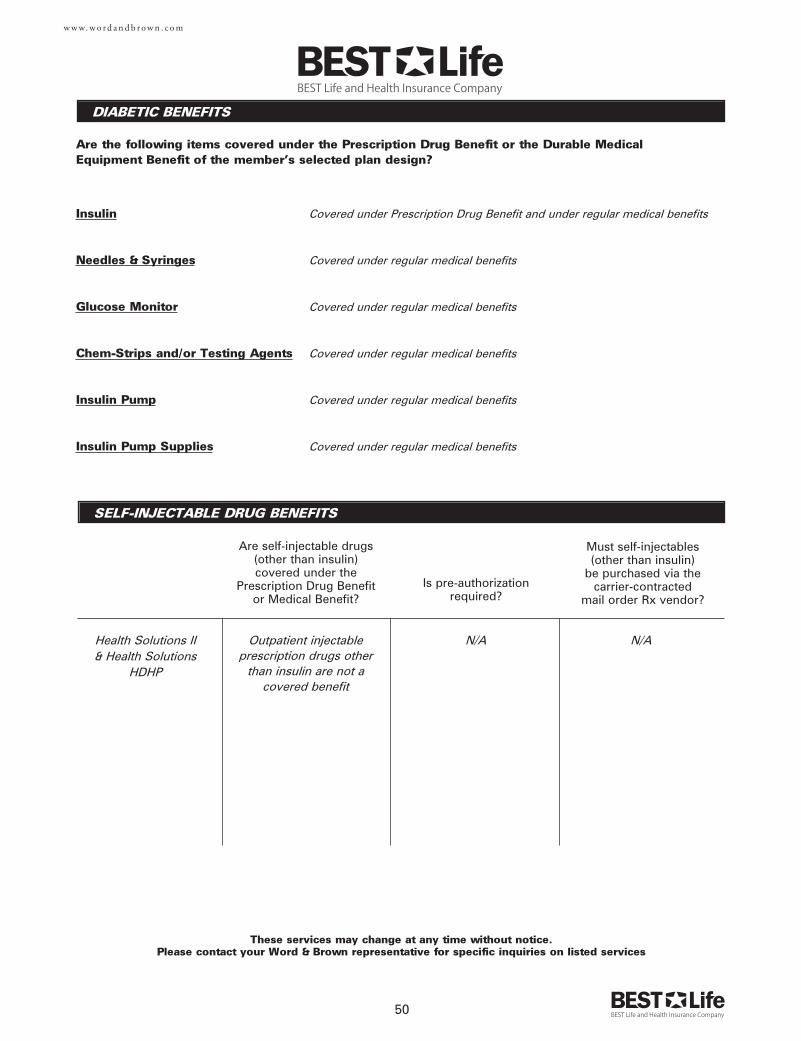
DIABETIC BENEFITS
These services may change at any time without notice. Please contact your Word & Brown representative for specific inquiries on listed services
50
Are the following items covered under the Prescription Drug Benefit or the Durable MedicalEquipment Benefit of the member’s selected plan design?
w w w. w o r d a n d b r o w n . c o m
Insulin
Needles & Syringes
Glucose Monitor
Chem-Strips and/or Testing Agents
Insulin Pump
Insulin Pump Supplies
SELF-INJECTABLE DRUG BENEFITS
Are self-injectable drugs(other than insulin)covered under the
Prescription Drug Benefitor Medical Benefit?
Is pre-authorizationrequired?
Must self-injectables(other than insulin)
be purchased via thecarrier-contracted
mail order Rx vendor?
Covered under Prescription Drug Benefit and under regular medical benefits
Covered under regular medical benefits
Covered under regular medical benefits
Covered under regular medical benefits
Covered under regular medical benefits
Covered under regular medical benefits
Outpatient injectableprescription drugs other
than insulin are not acovered benefit
N/A N/AHealth Solutions II& Health Solutions
HDHP
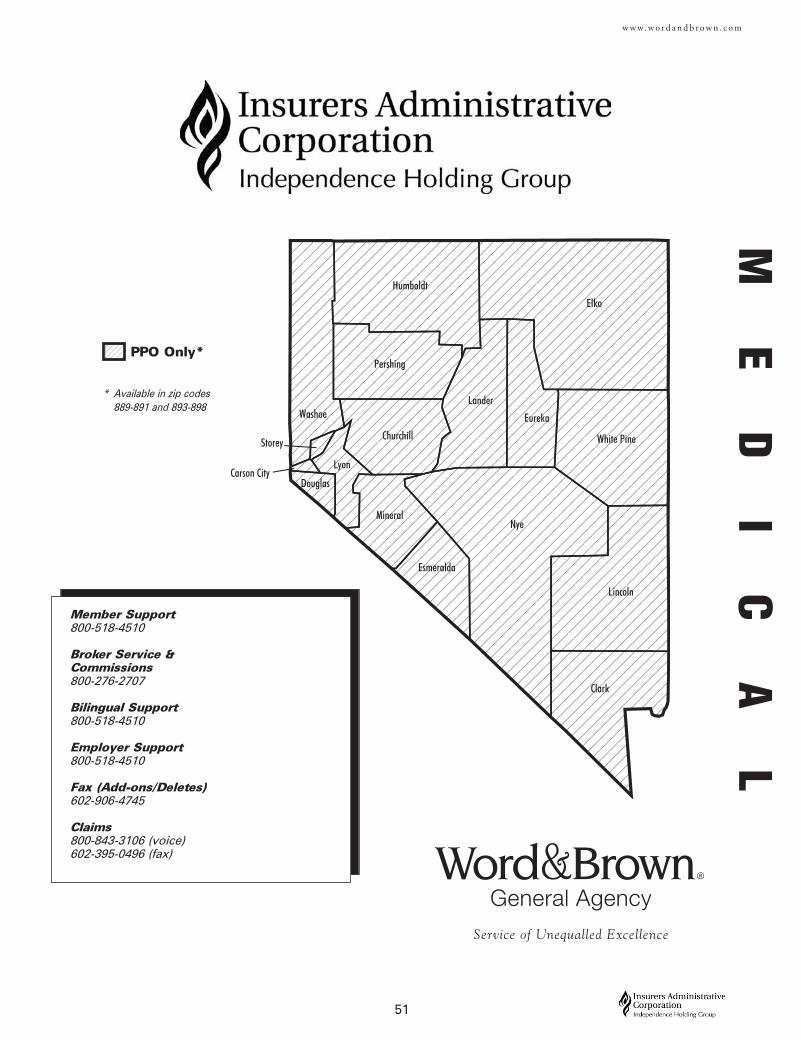
51
w w w. w o r d a n d b r o w n . c o m
Churchill
Clark
Douglas
Elko
Esmeralda
Eureka
Humboldt
Lander
Lincoln
Lyon
MineralNye
Pershing
Storey
Washoe
White Pine
Carson City
Member Support800-518-4510
Broker Service &Commissions800-276-2707
Bilingual Support800-518-4510
Employer Support800-518-4510
Fax (Add-ons/Deletes)602-906-4745
Claims800-843-3106 (voice)602-395-0496 (fax)
PPO Only*
* Available in zip codes 889-891 and 893-898
ME
DI
CA
L
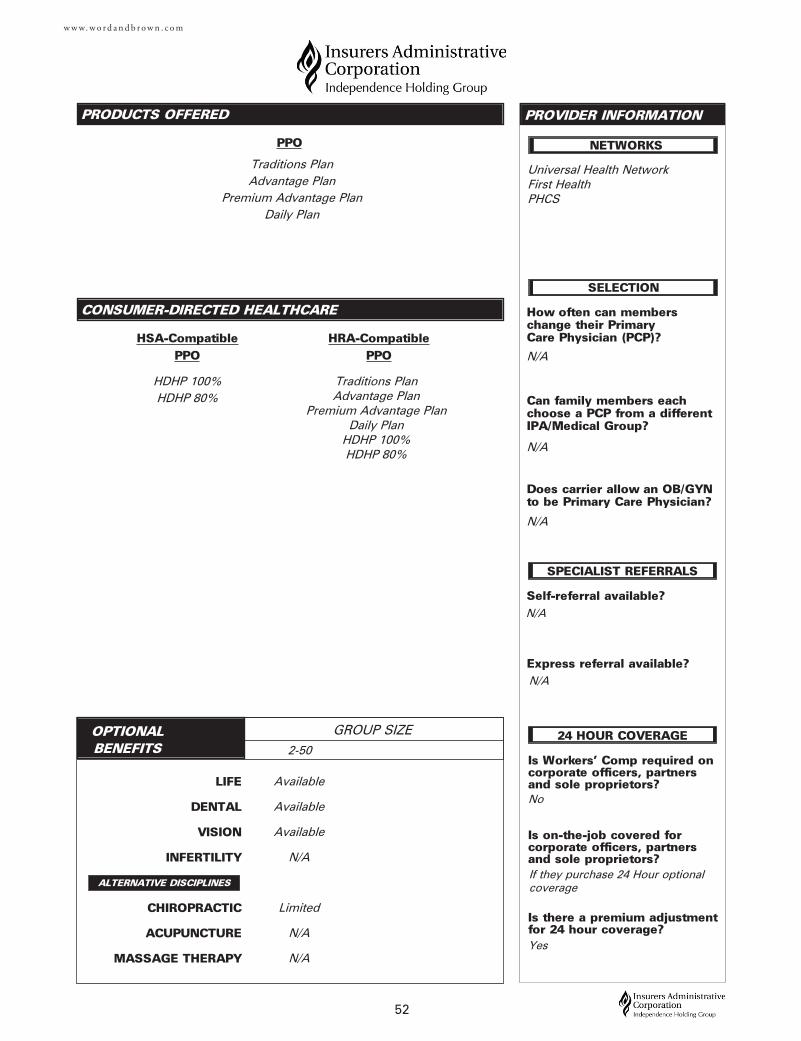
LIFE
DENTAL
VISION
INFERTILITY
CHIROPRACTIC
ACUPUNCTURE
MASSAGE THERAPY
PRODUCTS OFFERED
OPTIONAL BENEFITS
GROUP SIZE
PROVIDER INFORMATION
52
CONSUMER-DIRECTED HEALTHCARE
w w w. w o r d a n d b r o w n . c o m
ALTERNATIVE DISCIPLINES
Is Workers' Comp required oncorporate officers, partnersand sole proprietors?
Is on-the-job covered for corporate officers, partnersand sole proprietors?
Is there a premium adjustmentfor 24 hour coverage?
How often can members change their Primary Care Physician (PCP)?
Can family members eachchoose a PCP from a differentIPA/Medical Group?
Does carrier allow an OB/GYNto be Primary Care Physician?
Self-referral available?
Express referral available?
SELECTION
SPECIALIST REFERRALS
NETWORKS
24 HOUR COVERAGE
No
N/A
N/A
Universal Health NetworkFirst HealthPHCS
N/A
N/A
Available
Available
Available
N/A
Limited
N/A
N/A
Traditions PlanAdvantage Plan
Premium Advantage PlanDaily Plan
HDHP 100%HDHP 80%
If they purchase 24 Hour optional coverage
Yes
Traditions PlanAdvantage Plan
Premium Advantage Plan Daily Plan
HDHP 100%HDHP 80%
2-50
N/A
PPO
HSA-CompatiblePPO
HRA-CompatiblePPO
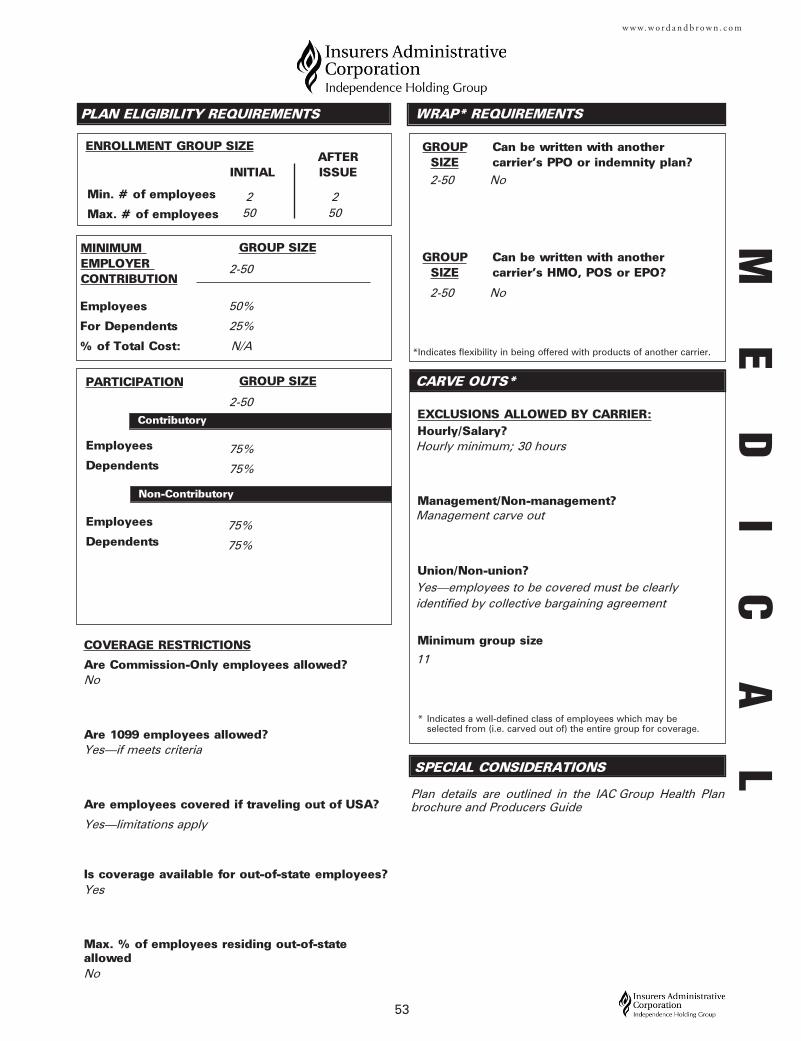
GROUP Can be written with another SIZE carrier's PPO or indemnity plan?
Employees
Dependents
Employees
Dependents
EXCLUSIONS ALLOWED BY CARRIER:Hourly/Salary?
Management/Non-management?
Union/Non-union?
Minimum group size
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
ENROLLMENT GROUP SIZE
Employees
For Dependents
% of Total Cost:
PLAN ELIGIBILITY REQUIREMENTS
MINIMUM EMPLOYER CONTRIBUTION
PARTICIPATION
Min. # of employees
Max. # of employees
Contributory
Non-Contributory
GROUP SIZE
GROUP SIZE
AFTERINITIAL ISSUE
CARVE OUTS*
WRAP* REQUIREMENTS
*Indicates flexibility in being offered with products of another carrier.
GROUP Can be written with another SIZE carrier's HMO, POS or EPO?
SPECIAL CONSIDERATIONS
53
w w w. w o r d a n d b r o w n . c o m
COVERAGE RESTRICTIONS
Are Commission-Only employees allowed?
Are 1099 employees allowed?
Are employees covered if traveling out of USA?
Is coverage available for out-of-state employees?
Max. % of employees residing out-of-stateallowed
No
Yes—if meets criteria
Yes—limitations apply
Yes
No
75%
75%
2-50
75%
75%
Hourly minimum; 30 hours
Management carve out
Yes—employees to be covered must be clearlyidentified by collective bargaining agreement
11
Plan details are outlined in the IAC Group Health Planbrochure and Producers Guide
2 250 50
2-50
50%
25%
N/A
2-50 No
2-50 No
ME
DI
CA
L
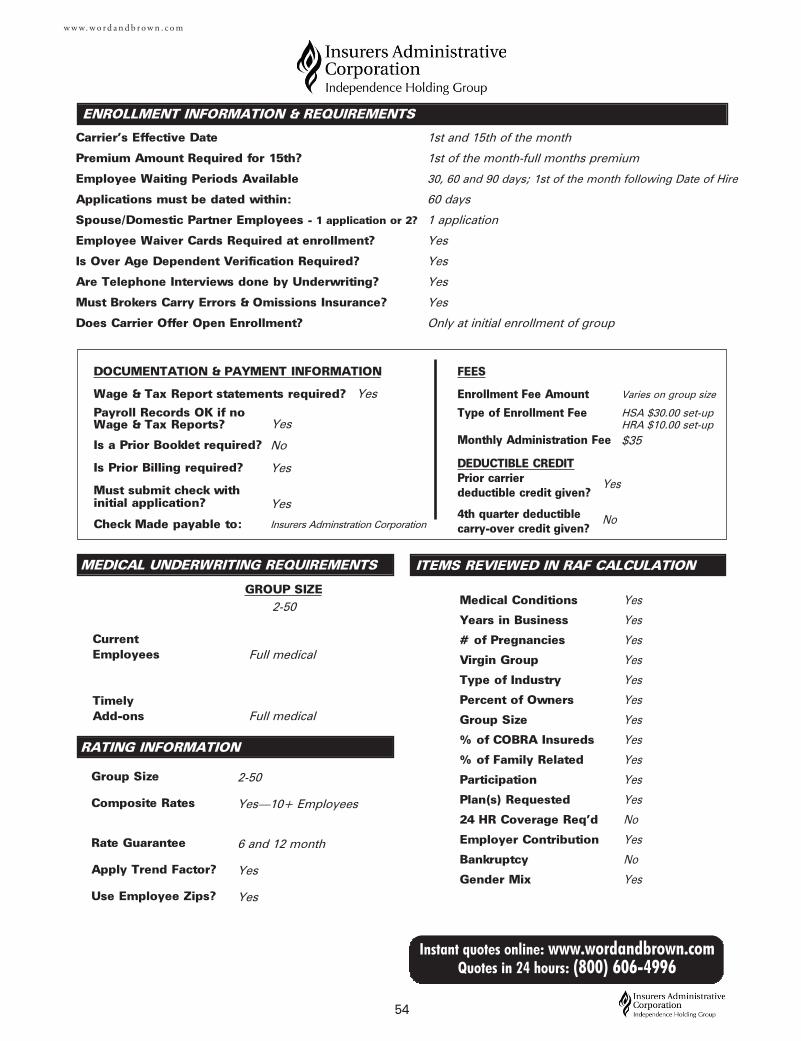
MEDICAL UNDERWRITING REQUIREMENTS
Current Employees
TimelyAdd-ons
Group Size
Composite Rates
Rate Guarantee
Apply Trend Factor?
Use Employee Zips?
ENROLLMENT INFORMATION & REQUIREMENTS
Carrier's Effective Date
Premium Amount Required for 15th?
Employee Waiting Periods Available
Applications must be dated within:
Spouse/Domestic Partner Employees - 1 application or 2?
Employee Waiver Cards Required at enrollment?
Is Over Age Dependent Verification Required?
Are Telephone Interviews done by Underwriting?
Must Brokers Carry Errors & Omissions Insurance?
Does Carrier Offer Open Enrollment?
DOCUMENTATION & PAYMENT INFORMATION
Wage & Tax Report statements required?
Payroll Records OK if no Wage & Tax Reports?
Is a Prior Booklet required?
Is Prior Billing required?
Must submit check with initial application?
Check Made payable to:
FEES
Enrollment Fee Amount
Type of Enrollment Fee
Monthly Administration Fee
DEDUCTIBLE CREDITPrior carrier deductible credit given?
4th quarter deductiblecarry-over credit given?
GROUP SIZE
RATING INFORMATION
54
Instant quotes online: www.wordandbrown.comQuotes in 24 hours: (800) 606-4996
w w w. w o r d a n d b r o w n . c o m
ITEMS REVIEWED IN RAF CALCULATION
Medical Conditions
Years in Business
# of Pregnancies
Virgin Group
Type of Industry
Percent of Owners
Group Size
% of COBRA Insureds
% of Family Related
Participation
Plan(s) Requested
24 HR Coverage Req'd
Employer Contribution
Bankruptcy
Gender Mix
1st and 15th of the month
1st of the month-full months premium
30, 60 and 90 days; 1st of the month following Date of Hire
60 days
1 application
Yes
Yes
Yes
Yes
Only at initial enrollment of group
Varies on group size
HSA $30.00 set-upHRA $10.00 set-up
$35
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
No
Yes
No
Yes
Yes
Full medical
No
Yes
Yes
Insurers Adminstration Corporation
Full medical
2-50
Yes—10+ Employees
6 and 12 month
Yes
Yes
Yes
No
Yes
2-50
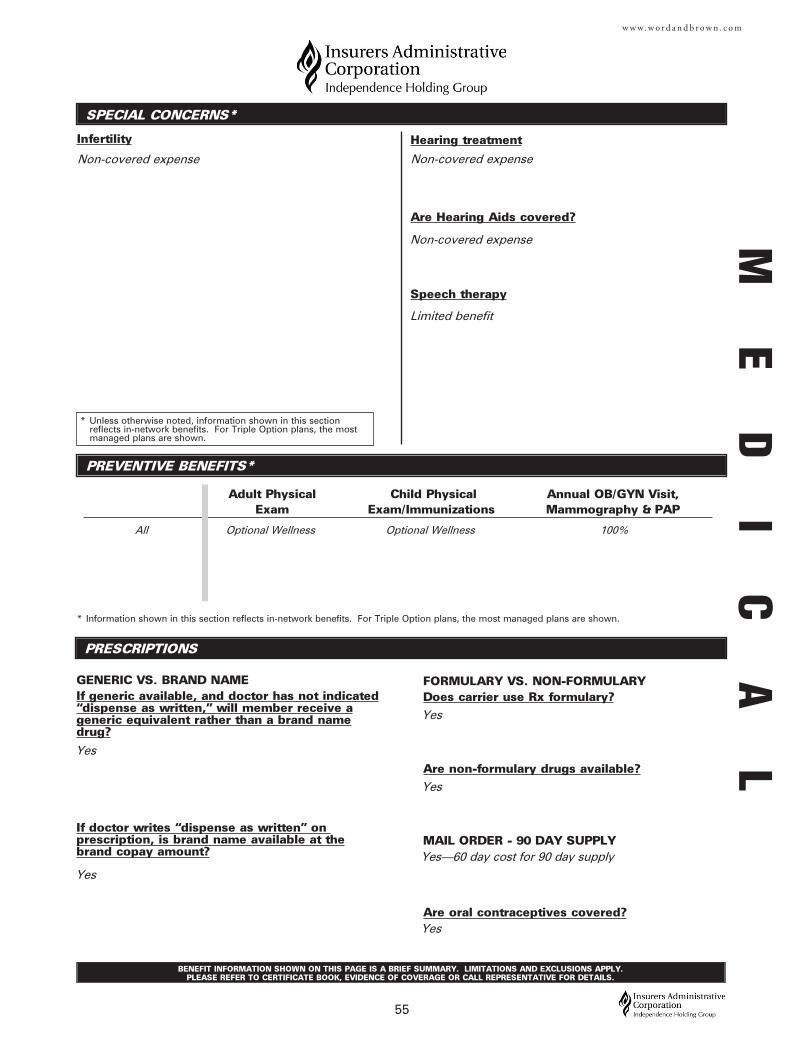
SPECIAL CONCERNS*
Infertility
PREVENTIVE BENEFITS*
PRESCRIPTIONS
Adult Physical Child Physical Annual OB/GYN Visit, Exam Exam/Immunizations Mammography & PAP
GENERIC VS. BRAND NAMEIf generic available, and doctor has not indicated“dispense as written,” will member receive ageneric equivalent rather than a brand namedrug?
If doctor writes “dispense as written” on prescription, is brand name available at thebrand copay amount?
* Information shown in this section reflects in-network benefits. For Triple Option plans, the most managed plans are shown.
FORMULARY VS. NON-FORMULARYDoes carrier use Rx formulary?
Are non-formulary drugs available?
MAIL ORDER - 90 DAY SUPPLY
Are oral contraceptives covered?
* Unless otherwise noted, information shown in this section reflects in-network benefits. For Triple Option plans, the most managed plans are shown.
BENEFIT INFORMATION SHOWN ON THIS PAGE IS A BRIEF SUMMARY. LIMITATIONS AND EXCLUSIONS APPLY. PLEASE REFER TO CERTIFICATE BOOK, EVIDENCE OF COVERAGE OR CALL REPRESENTATIVE FOR DETAILS.
55
w w w. w o r d a n d b r o w n . c o m
Hearing treatment
Are Hearing Aids covered?
Speech therapy
Non-covered expense
Yes
Yes
Yes—60 day cost for 90 day supply
Yes
All Optional Wellness
Non-covered expense
Limited benefit
Yes
Non-covered expense
Optional Wellness 100%
Yes
ME
DI
CA
L
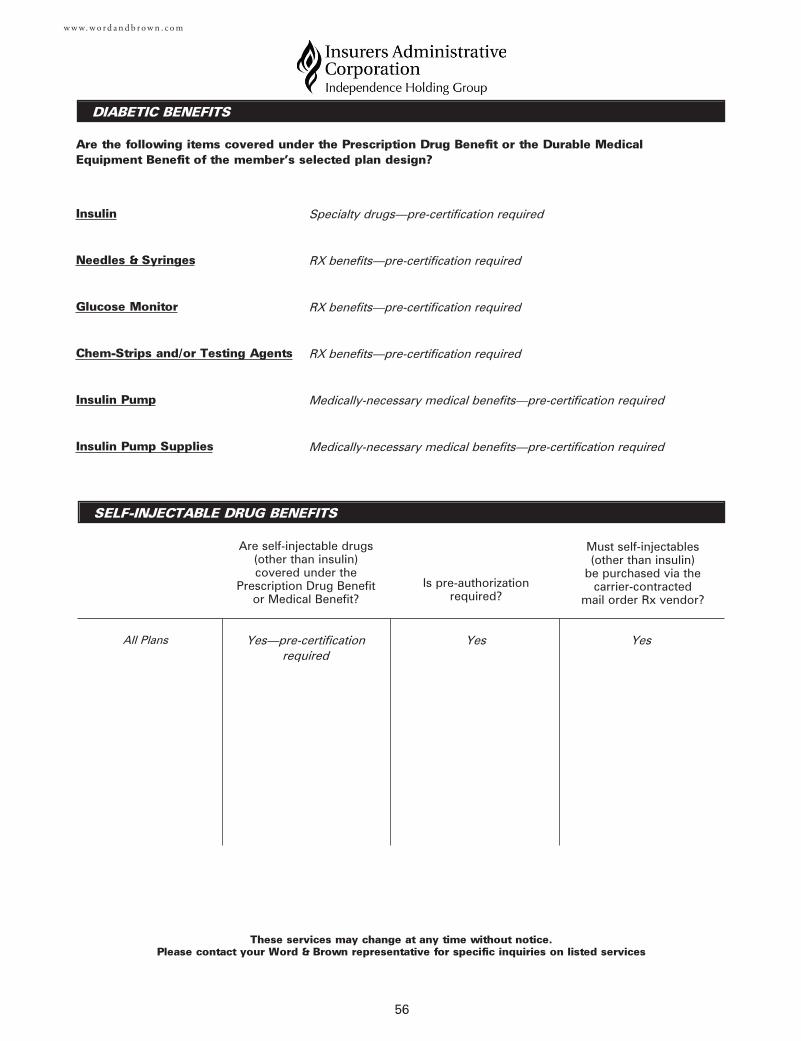
DIABETIC BENEFITS
These services may change at any time without notice. Please contact your Word & Brown representative for specific inquiries on listed services
56
Are the following items covered under the Prescription Drug Benefit or the Durable MedicalEquipment Benefit of the member’s selected plan design?
w w w. w o r d a n d b r o w n . c o m
Insulin
Needles & Syringes
Glucose Monitor
Chem-Strips and/or Testing Agents
Insulin Pump
Insulin Pump Supplies
SELF-INJECTABLE DRUG BENEFITS
Are self-injectable drugs(other than insulin)covered under the
Prescription Drug Benefitor Medical Benefit?
Is pre-authorizationrequired?
Must self-injectables(other than insulin)
be purchased via thecarrier-contracted
mail order Rx vendor?
Specialty drugs—pre-certification required
RX benefits—pre-certification required
RX benefits—pre-certification required
RX benefits—pre-certification required
Medically-necessary medical benefits—pre-certification required
Medically-necessary medical benefits—pre-certification required
Yes—pre-certificationrequired
Yes YesAll Plans
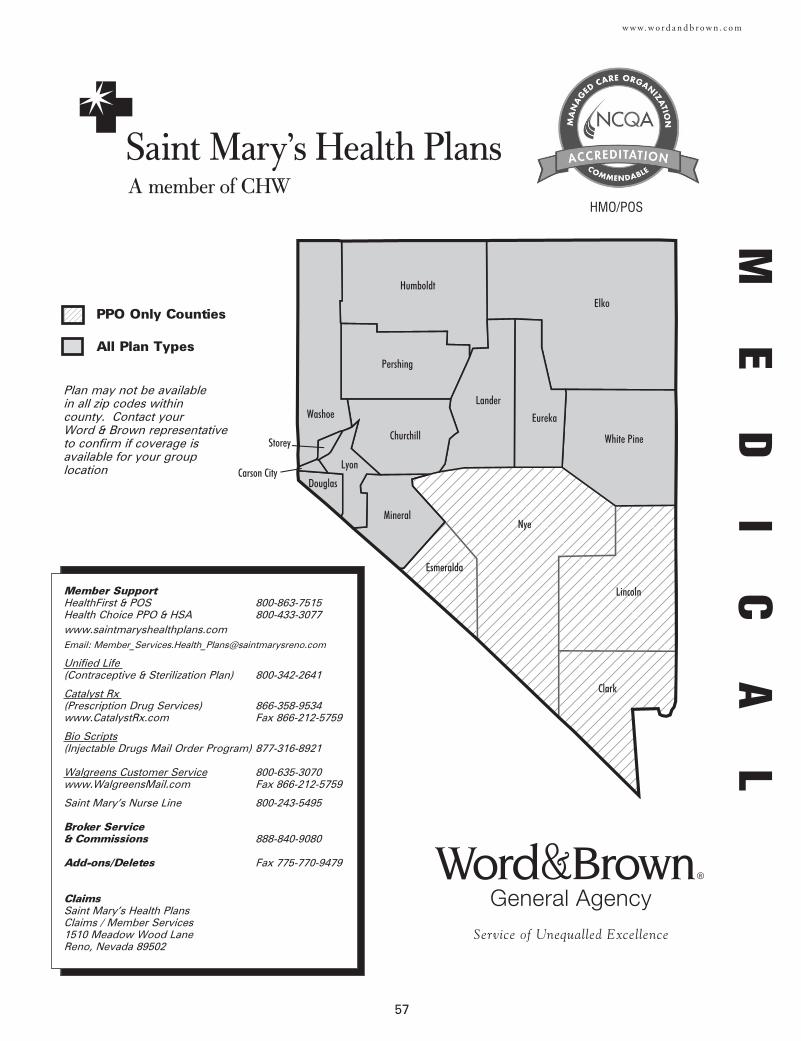
57
w w w. w o r d a n d b r o w n . c o m
Churchill
Clark
Douglas
Elko
Esmeralda
Eureka
Humboldt
Lander
Lincoln
Lyon
MineralNye
Pershing
Storey
Washoe
White Pine
Carson City
Member SupportHealthFirst & POS 800-863-7515Health Choice PPO & HSA 800-433-3077www.saintmaryshealthplans.comEmail: [email protected]
Unified Life (Contraceptive & Sterilization Plan) 800-342-2641
Catalyst Rx (Prescription Drug Services) 866-358-9534www.CatalystRx.com Fax 866-212-5759
Bio Scripts(Injectable Drugs Mail Order Program) 877-316-8921
Walgreens Customer Service 800-635-3070www.WalgreensMail.com Fax 866-212-5759
Saint Mary’s Nurse Line 800-243-5495
Broker Service & Commissions 888-840-9080
Add-ons/Deletes Fax 775-770-9479
ClaimsSaint Mary’s Health PlansClaims / Member Services1510 Meadow Wood LaneReno, Nevada 89502
HMO/POS
Plan may not be available in all zip codes within county. Contact your Word & Brown representativeto confirm if coverage isavailable for your grouplocation
ME
DI
CA
L
PPO Only Counties
All Plan Types
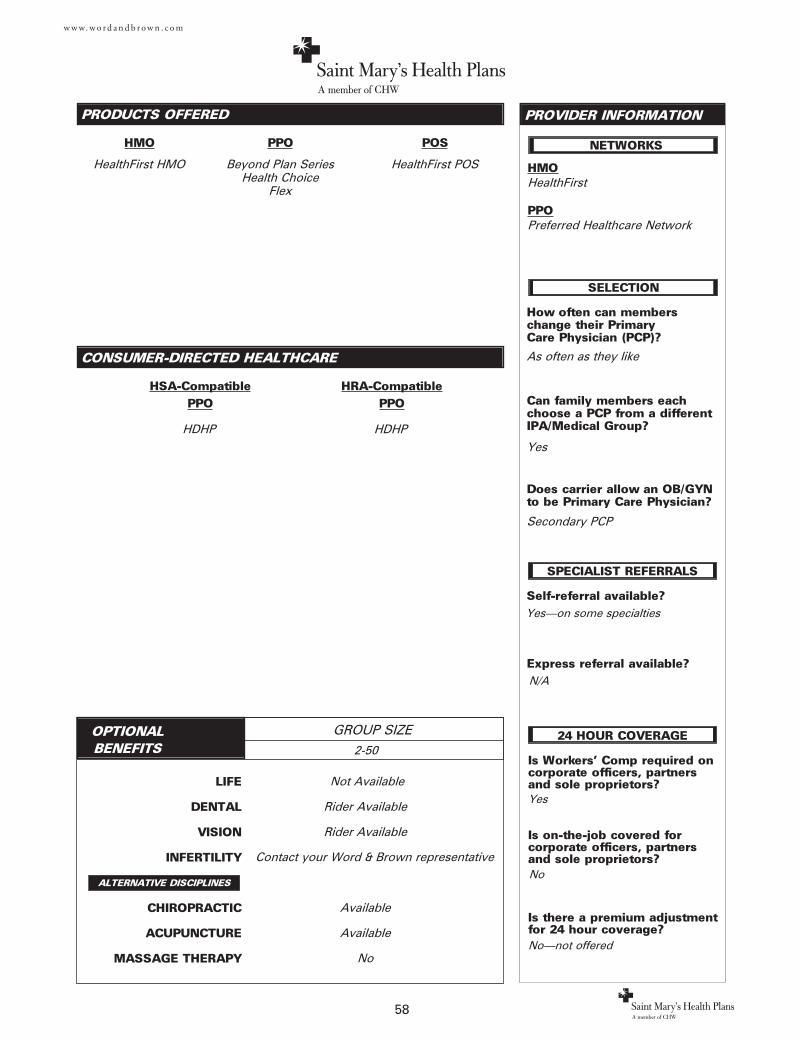
LIFE
DENTAL
VISION
INFERTILITY
CHIROPRACTIC
ACUPUNCTURE
MASSAGE THERAPY
PRODUCTS OFFERED
OPTIONAL BENEFITS
GROUP SIZE
PROVIDER INFORMATION
HMO
58
CONSUMER-DIRECTED HEALTHCARE
HSA-CompatiblePPO
w w w. w o r d a n d b r o w n . c o m
ALTERNATIVE DISCIPLINES
Is Workers' Comp required oncorporate officers, partnersand sole proprietors?
Is on-the-job covered for corporate officers, partnersand sole proprietors?
Is there a premium adjustmentfor 24 hour coverage?
How often can members change their Primary Care Physician (PCP)?
Can family members eachchoose a PCP from a differentIPA/Medical Group?
Does carrier allow an OB/GYNto be Primary Care Physician?
Self-referral available?
Express referral available?
SELECTION
SPECIALIST REFERRALS
NETWORKS
24 HOUR COVERAGE
Yes
N/A
Yes
Secondary PCP
Yes—on some specialties
Not Available
Rider Available
Rider Available
Available
Available
No
HealthFirst HMO
HDHP
No
No—not offered
As often as they like
PPO
Beyond Plan SeriesHealth Choice
Flex
POS
HealthFirst POS
2-50
Contact your Word & Brown representative
HMOHealthFirst
PPOPreferred Healthcare Network
HRA-CompatiblePPO
HDHP
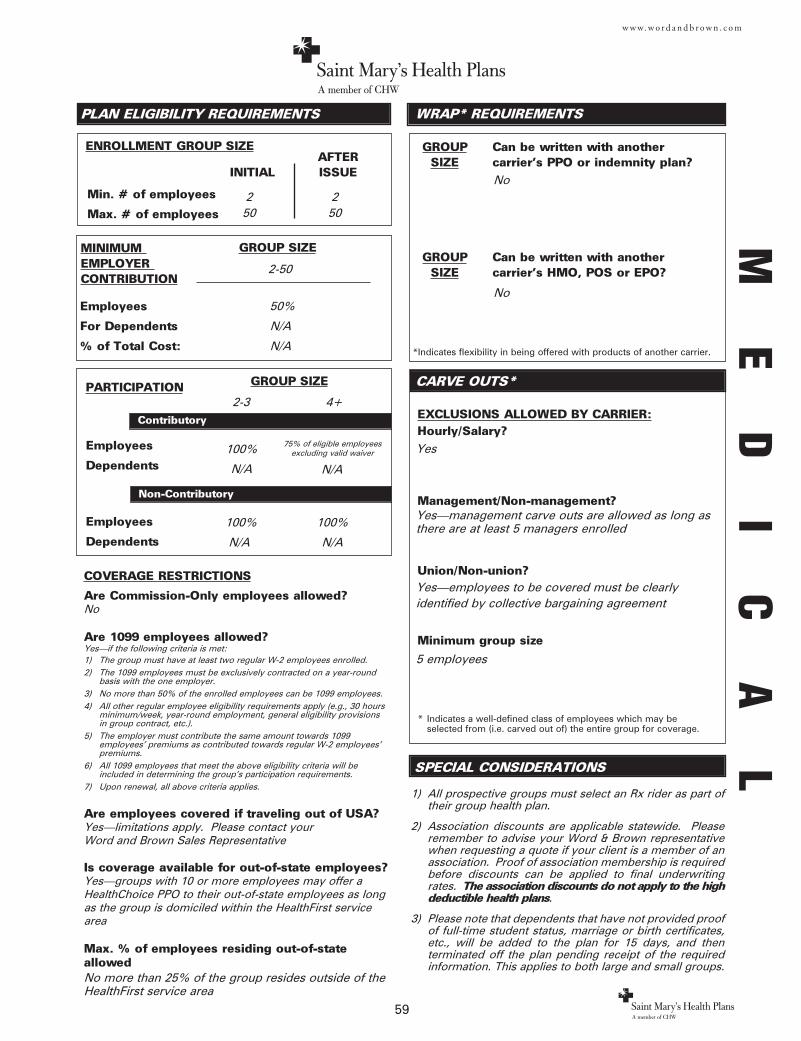
GROUP Can be written with another SIZE carrier's PPO or indemnity plan?
Employees
Dependents
Employees
Dependents
EXCLUSIONS ALLOWED BY CARRIER:Hourly/Salary?
Management/Non-management?
Union/Non-union?
Minimum group size
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
ENROLLMENT GROUP SIZE
Employees
For Dependents
% of Total Cost:
PLAN ELIGIBILITY REQUIREMENTS
MINIMUM EMPLOYER CONTRIBUTION
PARTICIPATION
Min. # of employees
Max. # of employees
Contributory
Non-Contributory
GROUP SIZE
GROUP SIZE
AFTERINITIAL ISSUE
CARVE OUTS*
WRAP* REQUIREMENTS
*Indicates flexibility in being offered with products of another carrier.
GROUP Can be written with another SIZE carrier's HMO, POS or EPO?
SPECIAL CONSIDERATIONS
59
w w w. w o r d a n d b r o w n . c o m
COVERAGE RESTRICTIONS
Are Commission-Only employees allowed?No
Are 1099 employees allowed?Yes—if the following criteria is met:1) The group must have at least two regular W-2 employees enrolled.2) The 1099 employees must be exclusively contracted on a year-round
basis with the one employer.3) No more than 50% of the enrolled employees can be 1099 employees. 4) All other regular employee eligibility requirements apply (e.g., 30 hours
minimum/week, year-round employment, general eligibility provisionsin group contract, etc.).
5) The employer must contribute the same amount towards 1099 employees' premiums as contributed towards regular W-2 employees'premiums.
6) All 1099 employees that meet the above eligibility criteria will beincluded in determining the group's participation requirements.
7) Upon renewal, all above criteria applies.
Are employees covered if traveling out of USA?Yes—limitations apply. Please contact your Word and Brown Sales Representative
Is coverage available for out-of-state employees?Yes—groups with 10 or more employees may offer aHealthChoice PPO to their out-of-state employees as longas the group is domiciled within the HealthFirst servicearea
Max. % of employees residing out-of-stateallowedNo more than 25% of the group resides outside of theHealthFirst service area
100%
N/A
2-3
100%
N/A
Yes
Yes—management carve outs are allowed as long asthere are at least 5 managers enrolled
Yes—employees to be covered must be clearlyidentified by collective bargaining agreement
5 employees
1) All prospective groups must select an Rx rider as part oftheir group health plan.
2) Association discounts are applicable statewide. Pleaseremember to advise your Word & Brown representativewhen requesting a quote if your client is a member of anassociation. Proof of association membership is requiredbefore discounts can be applied to final underwritingrates. The association discounts do not apply to the highdeductible health plans.
3) Please note that dependents that have not provided proofof full-time student status, marriage or birth certificates,etc., will be added to the plan for 15 days, and thenterminated off the plan pending receipt of the requiredinformation. This applies to both large and small groups.
2 250 50
2-50
50%
N/A
N/A
No
No
100%
N/A
4+
75% of eligible employeesexcluding valid waiver
N/A
ME
DI
CA
L
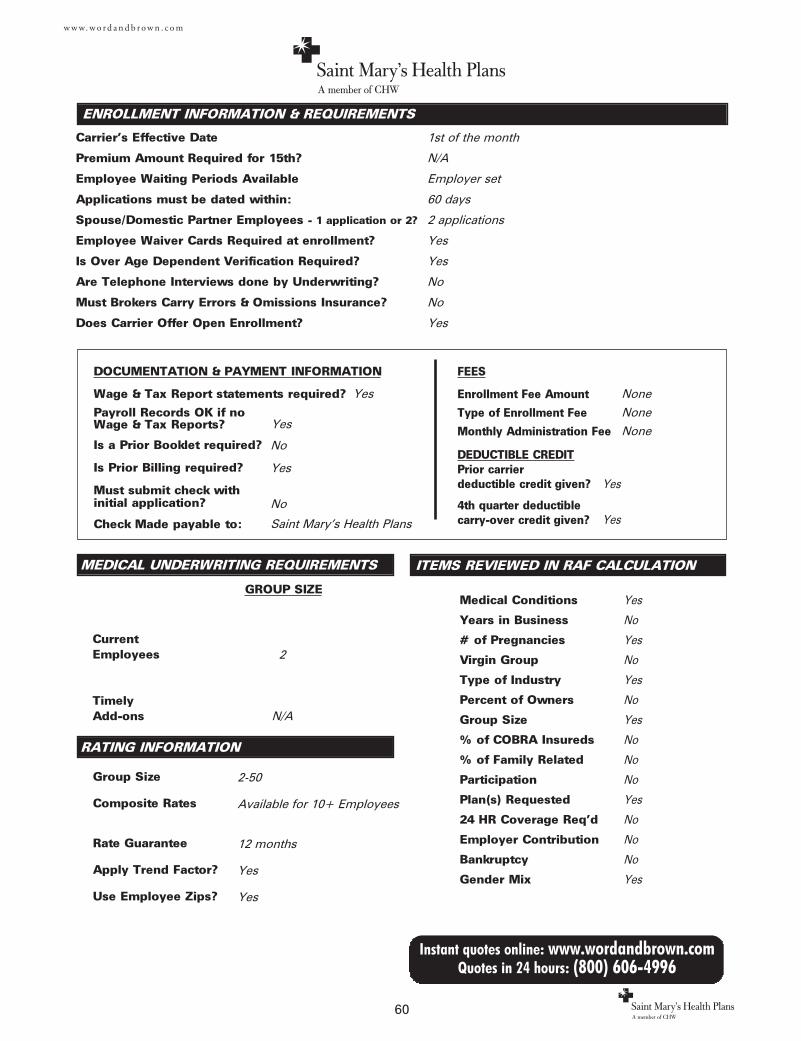
MEDICAL UNDERWRITING REQUIREMENTS
Current Employees
TimelyAdd-ons
Group Size
Composite Rates
Rate Guarantee
Apply Trend Factor?
Use Employee Zips?
ENROLLMENT INFORMATION & REQUIREMENTS
Carrier's Effective Date
Premium Amount Required for 15th?
Employee Waiting Periods Available
Applications must be dated within:
Spouse/Domestic Partner Employees - 1 application or 2?
Employee Waiver Cards Required at enrollment?
Is Over Age Dependent Verification Required?
Are Telephone Interviews done by Underwriting?
Must Brokers Carry Errors & Omissions Insurance?
Does Carrier Offer Open Enrollment?
DOCUMENTATION & PAYMENT INFORMATION
Wage & Tax Report statements required?
Payroll Records OK if no Wage & Tax Reports?
Is a Prior Booklet required?
Is Prior Billing required?
Must submit check with initial application?
Check Made payable to:
FEES
Enrollment Fee Amount
Type of Enrollment Fee
Monthly Administration Fee
DEDUCTIBLE CREDITPrior carrier deductible credit given?
4th quarter deductiblecarry-over credit given?
GROUP SIZE
RATING INFORMATION
60
Instant quotes online: www.wordandbrown.comQuotes in 24 hours: (800) 606-4996
w w w. w o r d a n d b r o w n . c o m
ITEMS REVIEWED IN RAF CALCULATION
Medical Conditions
Years in Business
# of Pregnancies
Virgin Group
Type of Industry
Percent of Owners
Group Size
% of COBRA Insureds
% of Family Related
Participation
Plan(s) Requested
24 HR Coverage Req'd
Employer Contribution
Bankruptcy
Gender Mix
1st of the month
N/A
Employer set
60 days
2 applications
Yes
Yes
No
No
Yes
None
None
None
Yes
No
Yes
No
Yes
No
Yes
No
No
No
Yes
No
No
No
Yes
Yes
2
No
Yes
No
Saint Mary’s Health Plans
N/A
2-50
Available for 10+ Employees
12 months
Yes
Yes
Yes
Yes
Yes
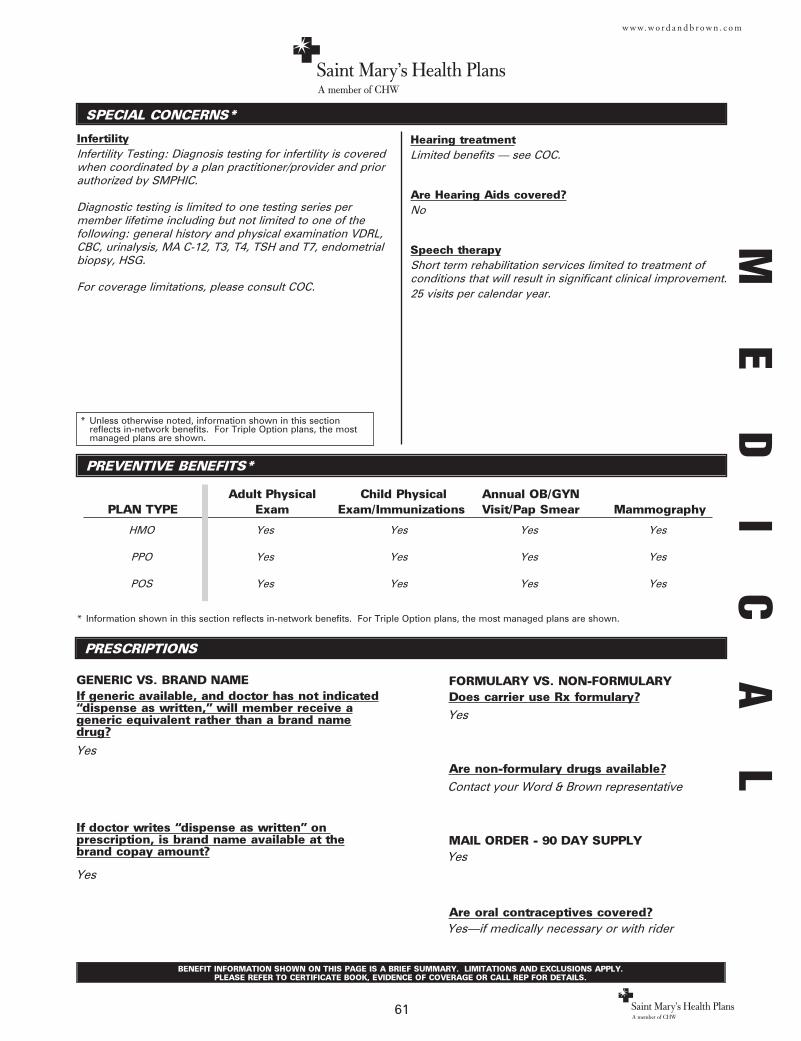
FORMULARY VS. NON-FORMULARYDoes carrier use Rx formulary?
Are non-formulary drugs available?
MAIL ORDER - 90 DAY SUPPLY
Are oral contraceptives covered?
SPECIAL CONCERNS*
InfertilityInfertility Testing: Diagnosis testing for infertility is coveredwhen coordinated by a plan practitioner/provider and priorauthorized by SMPHIC.
Diagnostic testing is limited to one testing series permember lifetime including but not limited to one of thefollowing: general history and physical examination VDRL,CBC, urinalysis, MA C-12, T3, T4, TSH and T7, endometrialbiopsy, HSG.
For coverage limitations, please consult COC.
PREVENTIVE BENEFITS*
PRESCRIPTIONS
Adult Physical Child Physical Annual OB/GYNPLAN TYPE Exam Exam/Immunizations Visit/Pap Smear Mammography
GENERIC VS. BRAND NAMEIf generic available, and doctor has not indicated“dispense as written,” will member receive ageneric equivalent rather than a brand namedrug?
If doctor writes “dispense as written” on prescription, is brand name available at thebrand copay amount?
* Information shown in this section reflects in-network benefits. For Triple Option plans, the most managed plans are shown.
* Unless otherwise noted, information shown in this section reflects in-network benefits. For Triple Option plans, the most managed plans are shown.
BENEFIT INFORMATION SHOWN ON THIS PAGE IS A BRIEF SUMMARY. LIMITATIONS AND EXCLUSIONS APPLY. PLEASE REFER TO CERTIFICATE BOOK, EVIDENCE OF COVERAGE OR CALL REP FOR DETAILS.
61
w w w. w o r d a n d b r o w n . c o m
Hearing treatmentLimited benefits — see COC.
Are Hearing Aids covered?No
Speech therapyShort term rehabilitation services limited to treatment ofconditions that will result in significant clinical improvement.25 visits per calendar year.
ME
DI
CA
L
HMO Yes Yes Yes Yes
PPO Yes Yes Yes Yes
POS Yes Yes Yes Yes
Yes
Contact your Word & Brown representative
Yes
Yes—if medically necessary or with rider
Yes
Yes
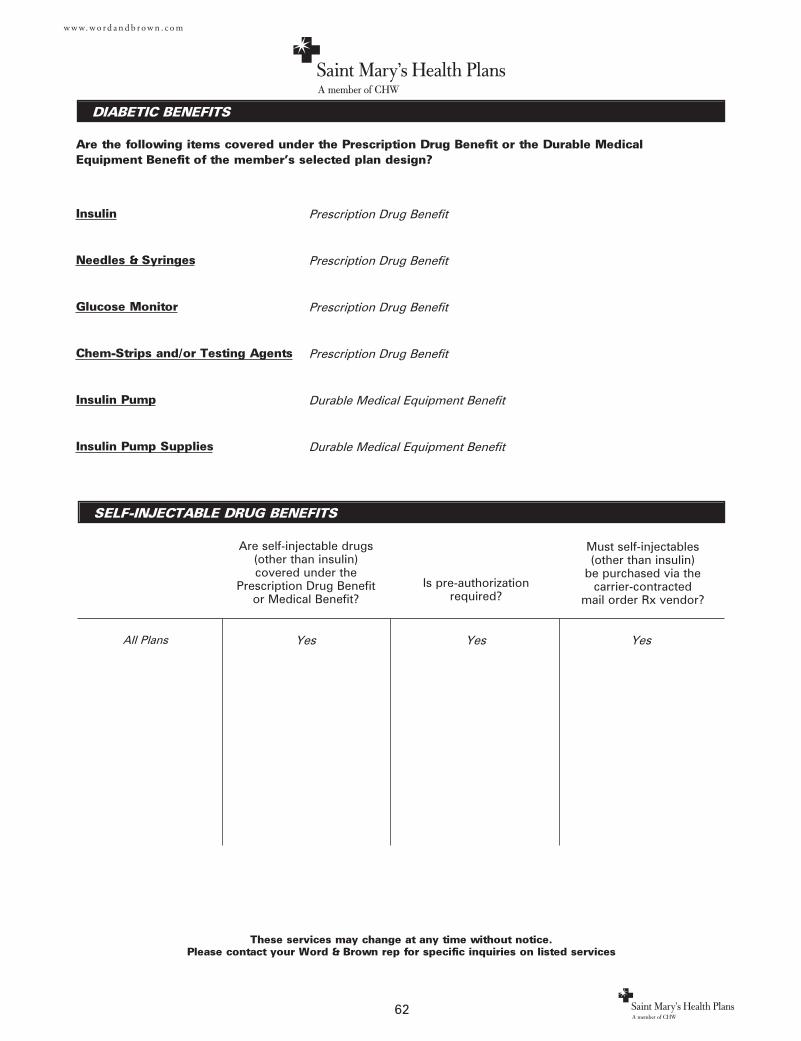
DIABETIC BENEFITS
These services may change at any time without notice. Please contact your Word & Brown rep for specific inquiries on listed services
62
Are the following items covered under the Prescription Drug Benefit or the Durable MedicalEquipment Benefit of the member’s selected plan design?
w w w. w o r d a n d b r o w n . c o m
Insulin
Needles & Syringes
Glucose Monitor
Chem-Strips and/or Testing Agents
Insulin Pump
Insulin Pump Supplies
SELF-INJECTABLE DRUG BENEFITS
Are self-injectable drugs(other than insulin)covered under the
Prescription Drug Benefitor Medical Benefit?
Is pre-authorizationrequired?
Must self-injectables(other than insulin)
be purchased via thecarrier-contracted
mail order Rx vendor?
Prescription Drug Benefit
Prescription Drug Benefit
Prescription Drug Benefit
Prescription Drug Benefit
Durable Medical Equipment Benefit
Durable Medical Equipment Benefit
Yes Yes Yes All Plans
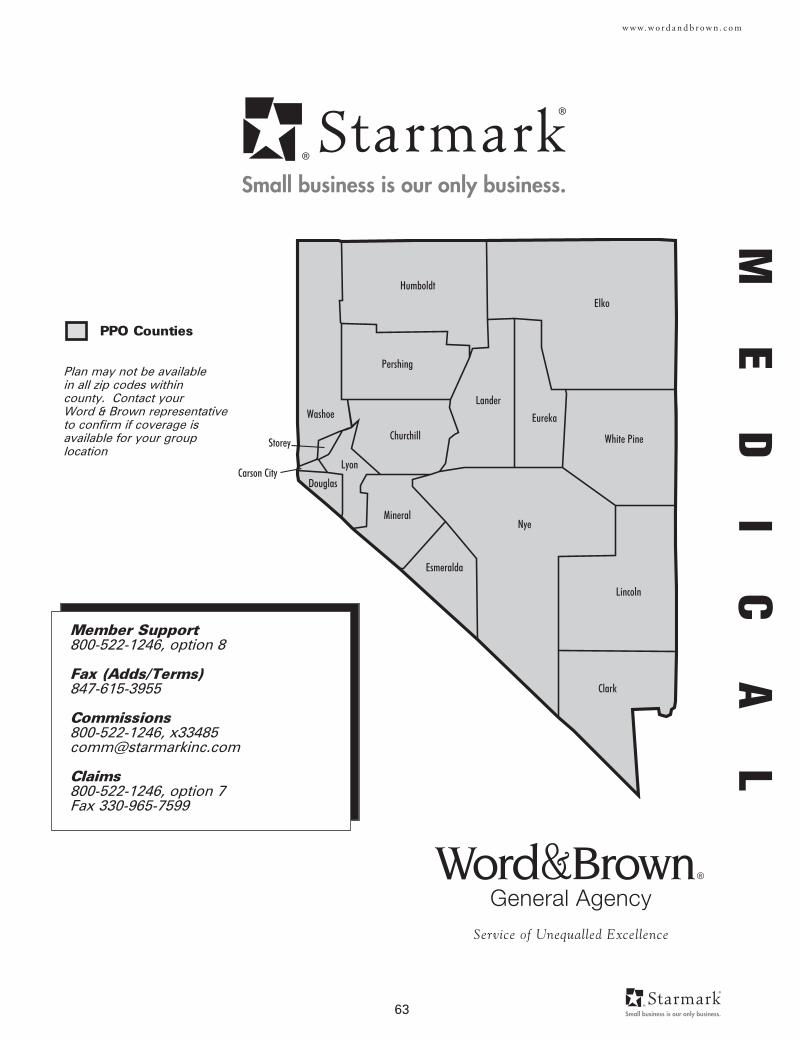
63
w w w. w o r d a n d b r o w n . c o m
Churchill
Clark
Douglas
Elko
Esmeralda
Eureka
Humboldt
Lander
Lincoln
Lyon
MineralNye
Pershing
Storey
Washoe
White Pine
Carson City
Member Support800-522-1246, option 8
Fax (Adds/Terms)847-615-3955
Commissions800-522-1246, [email protected]
Claims800-522-1246, option 7Fax 330-965-7599
ME
DI
CA
L
Plan may not be available in all zip codes within county. Contact your Word & Brown representativeto confirm if coverage isavailable for your grouplocation
PPO Counties
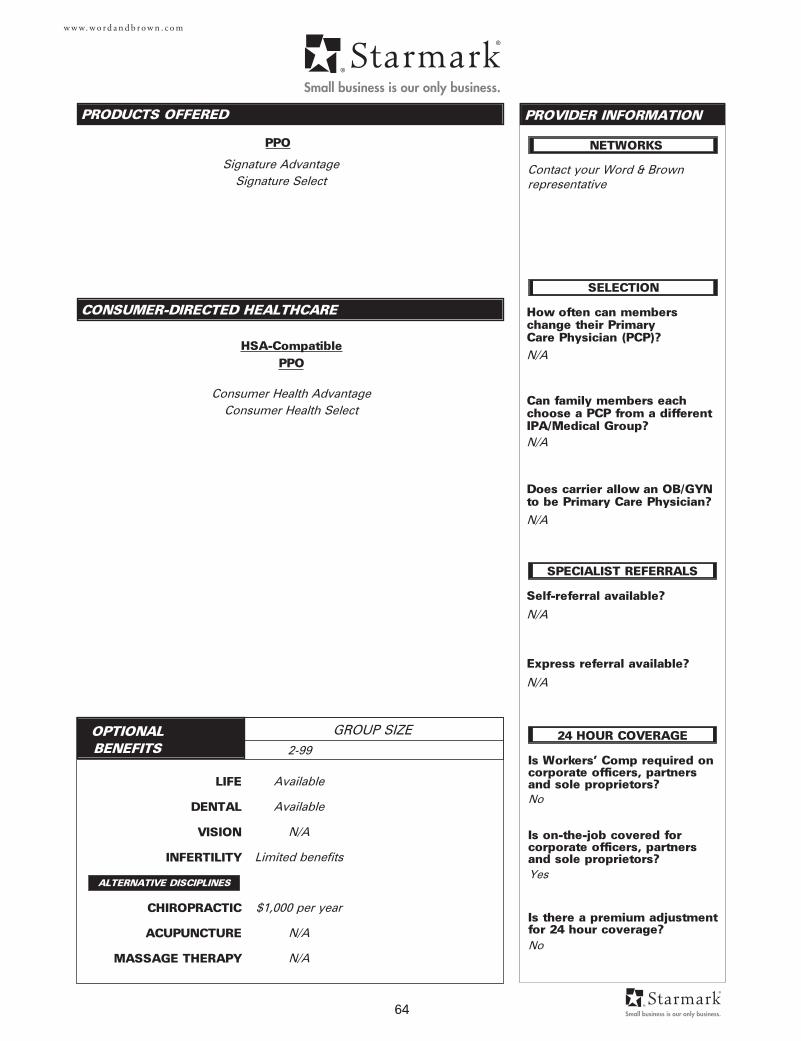
LIFE
DENTAL
VISION
INFERTILITY
CHIROPRACTIC
ACUPUNCTURE
MASSAGE THERAPY
PRODUCTS OFFERED
OPTIONAL BENEFITS
GROUP SIZE
PROVIDER INFORMATION
64
CONSUMER-DIRECTED HEALTHCARE
w w w. w o r d a n d b r o w n . c o m
ALTERNATIVE DISCIPLINES
Is Workers' Comp required oncorporate officers, partnersand sole proprietors?
Is on-the-job covered for corporate officers, partnersand sole proprietors?
Is there a premium adjustmentfor 24 hour coverage?
How often can members change their Primary Care Physician (PCP)?
Can family members eachchoose a PCP from a differentIPA/Medical Group?
Does carrier allow an OB/GYNto be Primary Care Physician?
Self-referral available?
Express referral available?
SELECTION
SPECIALIST REFERRALS
NETWORKS
N/A
24 HOUR COVERAGE
No
Contact your Word & Brown representative
Yes
No
Available
Available
N/A
Limited benefits
$1,000 per year
N/A
N/A
Signature AdvantageSignature Select
2-99
PPO
Consumer Health AdvantageConsumer Health Select
HSA-CompatiblePPO
N/A
N/A
N/A
N/A
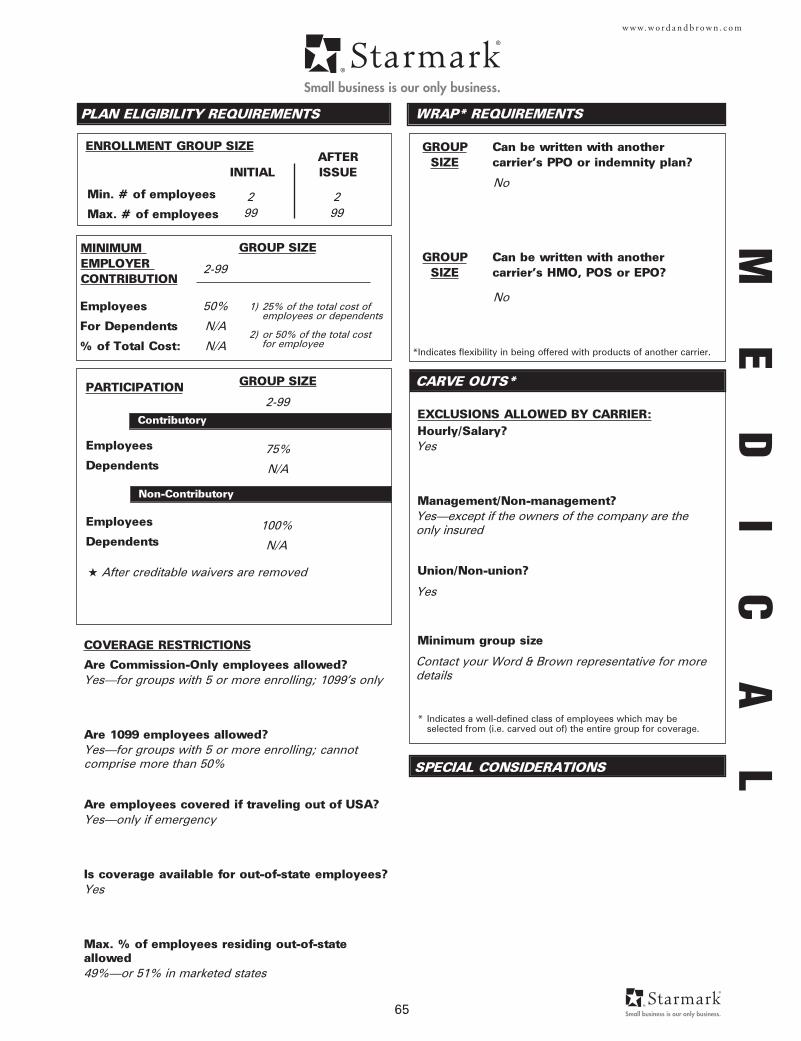
GROUP Can be written with another SIZE carrier's PPO or indemnity plan?
Employees
Dependents
Employees
Dependents
EXCLUSIONS ALLOWED BY CARRIER:Hourly/Salary?
Management/Non-management?
Union/Non-union?
Minimum group size
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
ENROLLMENT GROUP SIZE
Employees
For Dependents
% of Total Cost:
PLAN ELIGIBILITY REQUIREMENTS
MINIMUM EMPLOYER CONTRIBUTION
PARTICIPATION
Min. # of employees
Max. # of employees
Contributory
Non-Contributory
GROUP SIZE
GROUP SIZE
AFTERINITIAL ISSUE
CARVE OUTS*
WRAP* REQUIREMENTS
*Indicates flexibility in being offered with products of another carrier.
GROUP Can be written with another SIZE carrier's HMO, POS or EPO?
SPECIAL CONSIDERATIONS
65
w w w. w o r d a n d b r o w n . c o m
COVERAGE RESTRICTIONS
Are Commission-Only employees allowed?
Are 1099 employees allowed?
Are employees covered if traveling out of USA?
Is coverage available for out-of-state employees?
Max. % of employees residing out-of-stateallowed
Yes—for groups with 5 or more enrolling; 1099’s only
Yes—for groups with 5 or more enrolling; cannot comprise more than 50%
Yes—only if emergency
Yes
49%—or 51% in marketed states
100%
N/A
2-99
75%
N/A
Yes
Yes—except if the owners of the company are the only insured
Yes
Contact your Word & Brown representative for moredetails
2 99
2-99
50%
N/A
N/A
1) 25% of the total cost of employees or dependents
2) or 50% of the total cost for employee
ME
DI
CA
L
2 99
★ After creditable waivers are removed
No
No
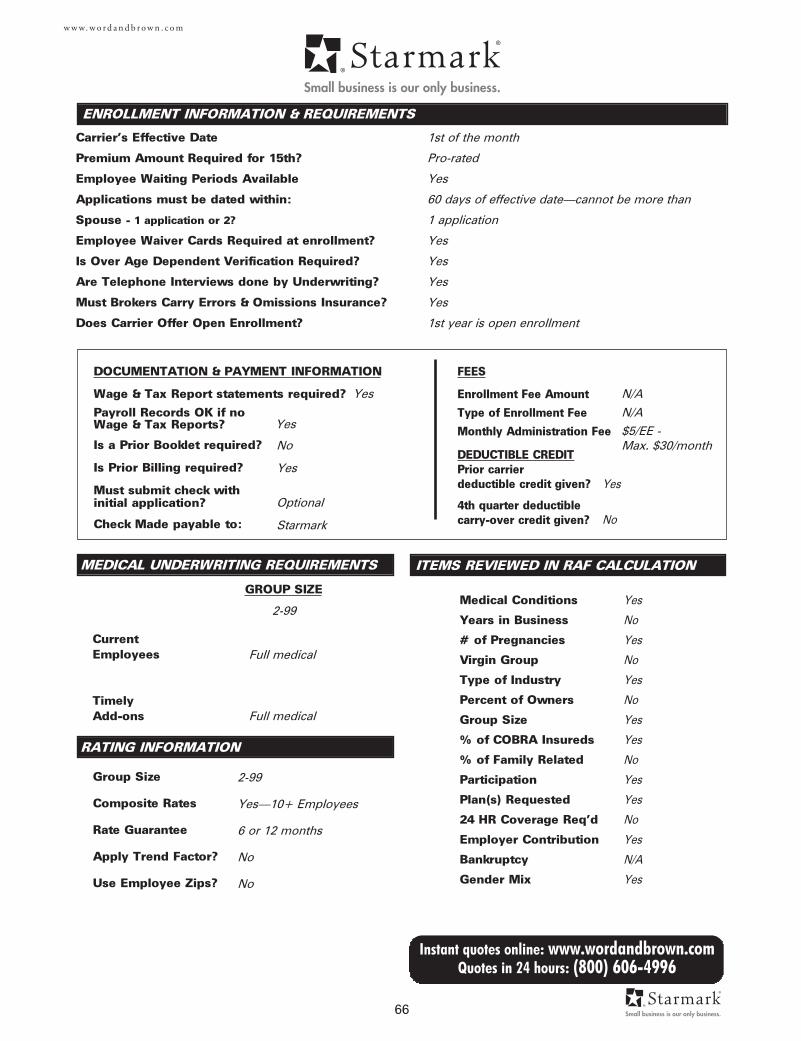
DOCUMENTATION & PAYMENT INFORMATION
Wage & Tax Report statements required?
Payroll Records OK if no Wage & Tax Reports?
Is a Prior Booklet required?
Is Prior Billing required?
Must submit check with initial application?
Check Made payable to:
MEDICAL UNDERWRITING REQUIREMENTS
Current Employees
TimelyAdd-ons
Group Size
Composite Rates
Rate Guarantee
Apply Trend Factor?
Use Employee Zips?
ENROLLMENT INFORMATION & REQUIREMENTS
Carrier's Effective Date
Premium Amount Required for 15th?
Employee Waiting Periods Available
Applications must be dated within:
Spouse - 1 application or 2?
Employee Waiver Cards Required at enrollment?
Is Over Age Dependent Verification Required?
Are Telephone Interviews done by Underwriting?
Must Brokers Carry Errors & Omissions Insurance?
Does Carrier Offer Open Enrollment?
FEES
Enrollment Fee Amount
Type of Enrollment Fee
Monthly Administration Fee
DEDUCTIBLE CREDITPrior carrier deductible credit given?
4th quarter deductiblecarry-over credit given?
GROUP SIZE
RATING INFORMATION
66
Instant quotes online: www.wordandbrown.comQuotes in 24 hours: (800) 606-4996
w w w. w o r d a n d b r o w n . c o m
ITEMS REVIEWED IN RAF CALCULATION
Medical Conditions
Years in Business
# of Pregnancies
Virgin Group
Type of Industry
Percent of Owners
Group Size
% of COBRA Insureds
% of Family Related
Participation
Plan(s) Requested
24 HR Coverage Req'd
Employer Contribution
Bankruptcy
Gender Mix
1st of the month
Pro-rated
Yes
60 days of effective date—cannot be more than
1 application
Yes
Yes
Yes
Yes
1st year is open enrollment
N/A
N/A
$5/EE - Max. $30/month
Yes
No
Yes
No
Yes
No
Yes
Yes
No
Yes
Yes
No
Yes
N/A
Yes
Yes
No
Yes
Optional
Starmark
2-99
Yes—10+ Employees
6 or 12 months
No
No
Yes
No
Yes
Full medical
Full medical
2-99
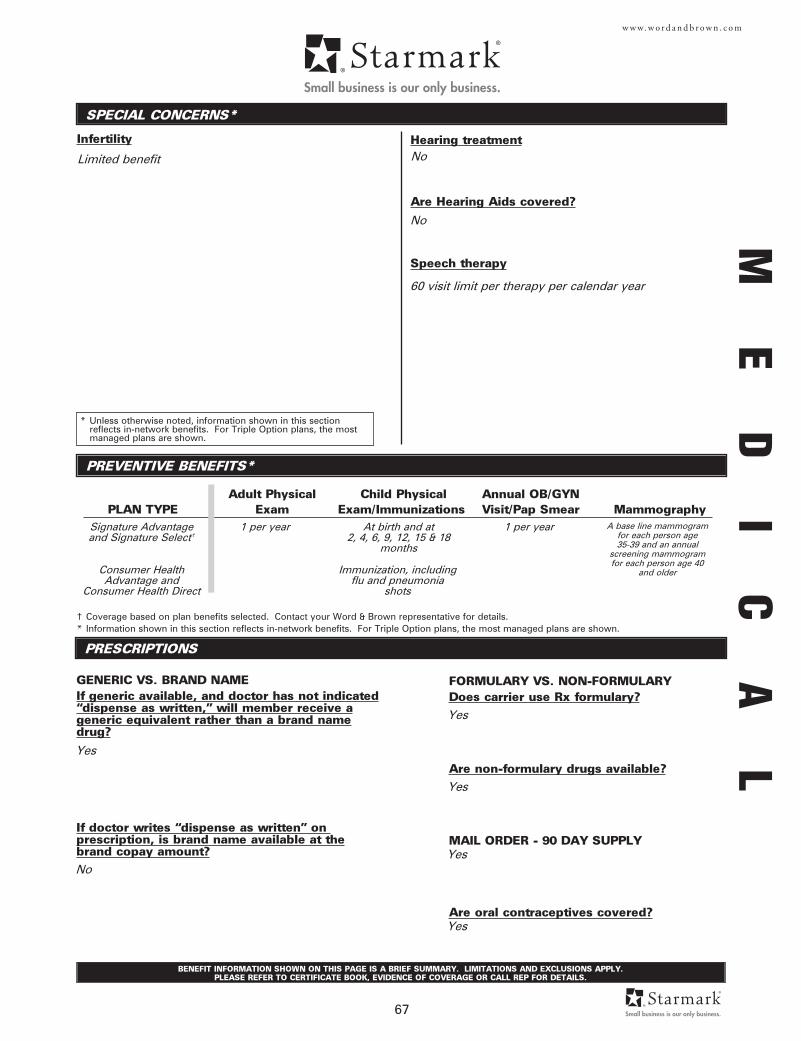
Infertility
SPECIAL CONCERNS*
PREVENTIVE BENEFITS*
PRESCRIPTIONS
Adult Physical Child Physical Annual OB/GYNPLAN TYPE Exam Exam/Immunizations Visit/Pap Smear Mammography
GENERIC VS. BRAND NAMEIf generic available, and doctor has not indicated“dispense as written,” will member receive ageneric equivalent rather than a brand namedrug?
If doctor writes “dispense as written” on prescription, is brand name available at thebrand copay amount?
† Coverage based on plan benefits selected. Contact your Word & Brown representative for details.* Information shown in this section reflects in-network benefits. For Triple Option plans, the most managed plans are shown.
FORMULARY VS. NON-FORMULARYDoes carrier use Rx formulary?
Are non-formulary drugs available?
MAIL ORDER - 90 DAY SUPPLY
Are oral contraceptives covered?
* Unless otherwise noted, information shown in this section reflects in-network benefits. For Triple Option plans, the most managed plans are shown.
BENEFIT INFORMATION SHOWN ON THIS PAGE IS A BRIEF SUMMARY. LIMITATIONS AND EXCLUSIONS APPLY. PLEASE REFER TO CERTIFICATE BOOK, EVIDENCE OF COVERAGE OR CALL REP FOR DETAILS.
67
w w w. w o r d a n d b r o w n . c o m
Hearing treatment
Are Hearing Aids covered?
Speech therapy
ME
DI
CA
L
Limited benefit
Yes
Yes
Yes
Yes
Signature Advantageand Signature Select†
1 per year
No
60 visit limit per therapy per calendar year
Yes
No
At birth and at 2, 4, 6, 9, 12, 15 & 18
months
1 per year A base line mammogramfor each person age35-39 and an annual
screening mammogramfor each person age 40
and older
No
Consumer HealthAdvantage and
Consumer Health Direct
Immunization, includingflu and pneumonia
shots
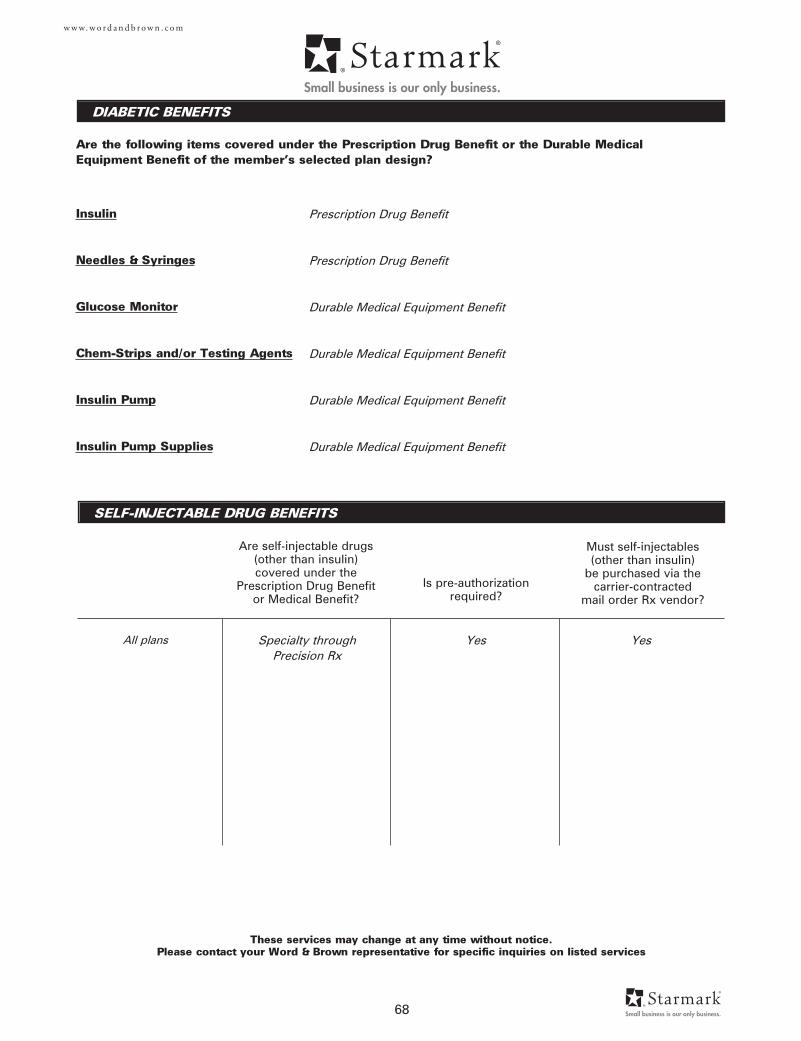
DIABETIC BENEFITS
These services may change at any time without notice. Please contact your Word & Brown representative for specific inquiries on listed services
68
Are the following items covered under the Prescription Drug Benefit or the Durable MedicalEquipment Benefit of the member’s selected plan design?
w w w. w o r d a n d b r o w n . c o m
Insulin
Needles & Syringes
Glucose Monitor
Chem-Strips and/or Testing Agents
Insulin Pump
Insulin Pump Supplies
SELF-INJECTABLE DRUG BENEFITS
Are self-injectable drugs(other than insulin)covered under the
Prescription Drug Benefitor Medical Benefit?
Is pre-authorizationrequired?
Must self-injectables(other than insulin)
be purchased via thecarrier-contracted
mail order Rx vendor?
Prescription Drug Benefit
Prescription Drug Benefit
Durable Medical Equipment Benefit
Durable Medical Equipment Benefit
Durable Medical Equipment Benefit
Durable Medical Equipment Benefit
Specialty throughPrecision Rx
Yes YesAll plans

69
w w w. w o r d a n d b r o w n . c o m
CONSUMERDIRECTED
PLANS
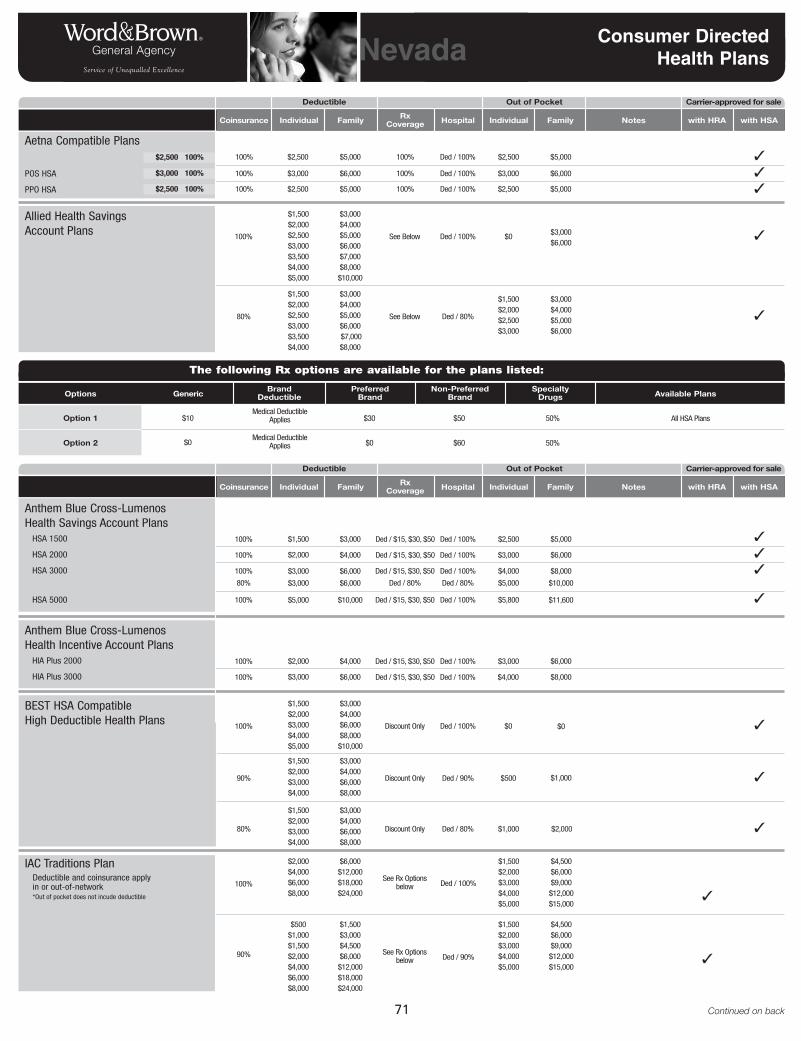
71 Continued on back
Nevada Consumer Directed Health Plans
Coinsurance Rx Coverage Hospital
Ded / 100% $2,500 $5,000100%$5,000$2,500100%
Out of Pocket Carrier-approved for sale
✓
Individual Family Individual Family Notes with HRA with HSA
Deductible
Ded / 100% $0 $3,000$6,000
See Below100%
$1,500$2,000$2,500$3,000$3,500$4,000$5,000
$3,000$4,000$5,000$6,000$7,000$8,000$10,000
✓
Ded / 80%
$3,000$4,000$5,000$6,000
$1,500$2,000$2,500$3,000
See Below80%
$1,500$2,000$2,500$3,000$3,500$4,000
$3,000$4,000$5,000$6,000$7,000$8,000
✓
Ded / 100% $3,000 $6,000100%$6,000$3,000100% ✓Ded / 100% $2,500 $5,000100%$5,000$2,500100% ✓
Allied Health SavingsAccount Plans
Ded / 100% $2,500 $5,000Ded / $15, $30, $50100% ✓
Anthem Blue Cross-LumenosHealth Savings Account Plans
HSA 1500
HSA 2000
HSA 3000
HSA 5000
$1,500 $3,000
Ded / 100% $3,000 $6,000Ded / $15, $30, $50100% ✓$2,000 $4,000
Ded / 100%
Ded / 80%
$4,000
$5,000
$8,000
$10,000
Ded / $15, $30, $50
Ded / 80%
100%
80%
✓$3,000
$3,000
$6,000
$6,000
Ded / 100% $3,000 $6,000Ded / $15, $30, $50100%
Anthem Blue Cross-LumenosHealth Incentive Account Plans
HIA Plus 2000
HIA Plus 3000
$2,000 $4,000
Ded / 100% $4,000 $8,000Ded / $15, $30, $50100% $3,000 $6,000
Aetna Compatible Plans
POS HSA
PPO HSA
$2,500 100%
$3,000 100%
$2,500 100%
Ded / 100% $0 $0Discount Only100%
$1,500$2,000$3,000$4,000$5,000
$3,000$4,000$6,000$8,000$10,000
✓
Ded / 90% $500 $1,000Discount Only90%
$1,500$2,000$3,000$4,000
$3,000$4,000$6,000$8,000
✓
Ded / 80% $1,000 $2,000Discount Only80%
$1,500$2,000$3,000$4,000
$3,000$4,000$6,000$8,000
✓
BEST HSA Compatible High Deductible Health Plans
Ded / 100% $5,800 $11,600Ded / $15, $30, $50100% ✓$5,000 $10,000
Options
Option 1
Generic
Option 2 $60$0Medical Deductible
Applies $0
BrandDeductible
PreferredBrand
Non-PreferredBrand
SpecialtyDrugs Available Plans
All HSA Plans
All HSA Plans
The following Rx options are available for the plans listed:
$50$10Medical Deductible
Applies $30 50%
50%
Ded / 100%See Rx Options
below100%
$2,000$4,000$6,000$8,000
$6,000$12,000$18,000$24,000
$1,500$2,000$3,000$4,000$5,000
$4,500$6,000$9,000$12,000$15,000
✓
Ded / 90%See Rx Options
below
$500$1,000$1,500$2,000$4,000$6,000$8,000
$1,500$3,000$4,500$6,000$12,000$18,000$24,000
$1,500$2,000$3,000$4,000$5,000
$4,500$6,000$9,000$12,000$15,000
✓90%
IAC Traditions PlanDeductible and coinsurance apply in or out-of-network*Out of pocket does not incude deductible
Coinsurance Rx Coverage Hospital
Out of Pocket Carrier-approved for sale
Individual Family Individual Family Notes with HRA with HSA
Deductible
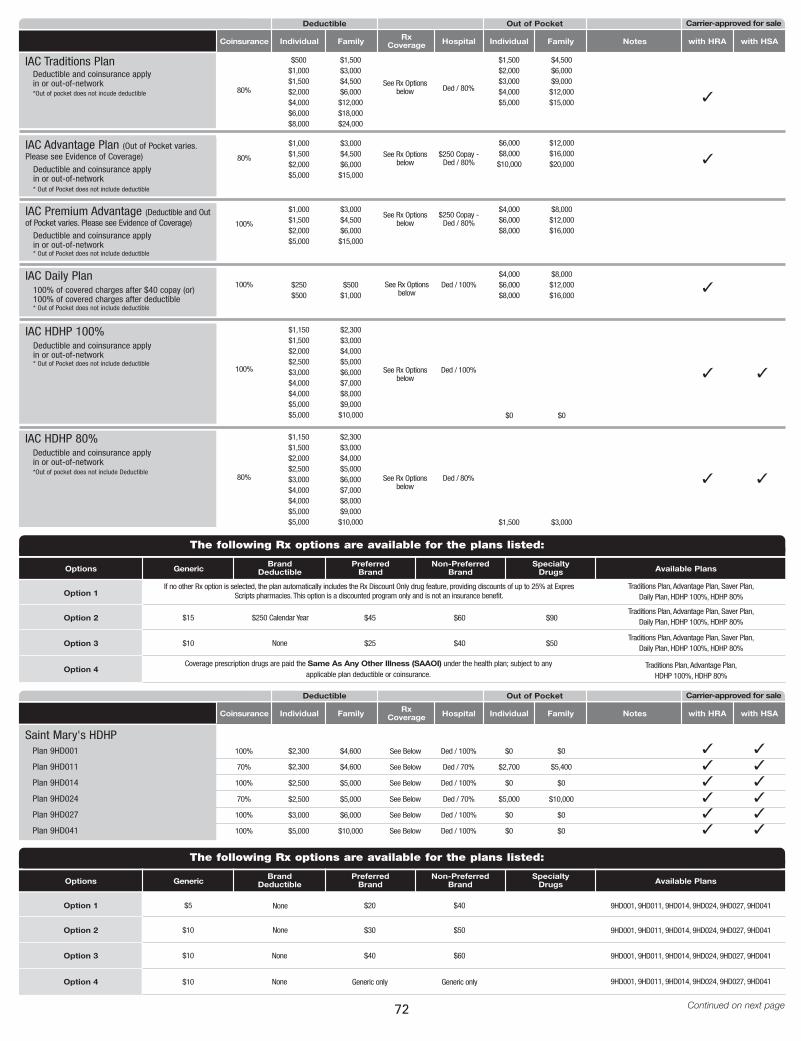
72 Continued on next page
Coinsurance Rx Coverage Hospital
Out of Pocket Carrier-approved for sale
Individual Family Individual Family Notes with HRA with HSA
Deductible
$250 Copay -Ded / 80%
See Rx Optionsbelow
80%
$1,000$1,500$2,000$5,000
$3,000$4,500$6,000$15,000
$6,000$8,000$10,000
$12,000$16,000$20,000 ✓
IAC Advantage Plan (Out of Pocket varies.Please see Evidence of Coverage)
Ded / 100%See Rx Optionsbelow
100%
$1,150$1,500$2,000$2,500$3,000$4,000 $4,000$5,000$5,000
$2,300$3,000$4,000$5,000$6,000$7,000 $8,000$9,000$10,000 $0 $0
✓
IAC HDHP 100%Deductible and coinsurance apply in or out-of-network* Out of Pocket does not include deductible
Ded / 80%See Rx Optionsbelow
80%
$1,150$1,500$2,000$2,500$3,000$4,000 $4,000$5,000$5,000
$2,300$3,000$4,000$5,000$6,000$7,000 $8,000$9,000$10,000 $1,500 $3,000
✓
✓
✓
IAC HDHP 80%Deductible and coinsurance apply in or out-of-network*Out of pocket does not include Deductible
Ded / 100%See Rx Optionsbelow
100% $250$500
$500$1,000
$4,000$6,000$8,000
$8,000$12,000$16,000
✓IAC Daily Plan
100% of covered charges after $40 copay (or)100% of covered charges after deductible* Out of Pocket does not include deductible
Options
Option 1
Generic
Option 2 $60 $90$15
If no other Rx option is selected, the plan automatically includes the Rx Discount Only drug feature, providing discounts of up to 25% at ExpresScripts pharmacies. This option is a discounted program only and is not an insurance benefit.
$250 Calendar Year $45
BrandDeductible
PreferredBrand
Non-PreferredBrand
SpecialtyDrugs Available Plans
Option 3 $40 $50$10 None $25
Option 4
Traditions Plan, Advantage Plan, Saver Plan, Daily Plan, HDHP 100%, HDHP 80%
Traditions Plan, Advantage Plan, Saver Plan, Daily Plan, HDHP 100%, HDHP 80%
Traditions Plan, Advantage Plan, Saver Plan, Daily Plan, HDHP 100%, HDHP 80%
Traditions Plan, Advantage Plan, HDHP 100%, HDHP 80%
Coverage prescription drugs are paid the Same As Any Other Illness (SAAOI) under the health plan; subject to anyapplicable plan deductible or coinsurance.
The following Rx options are available for the plans listed:
Ded / 100% $0 $0See Below100% ✓Saint Mary's HDHP
Plan 9HD001
Plan 9HD011
Plan 9HD014
Plan 9HD024
Plan 9HD027
Plan 9HD041
$2,300 $4,600
Ded / 70% $2,700 $5,400See Below70% ✓$2,300 $4,600
Ded / 100% $0 $0See Below100% ✓$2,500 $5,000
Ded / 70% $5,000 $10,000See Below70% ✓$2,500 $5,000
Coinsurance Rx Coverage Hospital
Out of Pocket Carrier-approved for sale
Individual Family Individual Family Notes with HRA with HSA
Deductible
✓
✓
✓
✓Ded / 100% $0 $0See Below100% ✓$3,000 $6,000
Ded / 100% $0 $0See Below100% ✓$5,000 $10,000
✓✓
Options
Option 1
Generic
Option 2 $50$10 None $30
BrandDeductible
PreferredBrand
Non-PreferredBrand
SpecialtyDrugs Available Plans
Option 3 $60$10 None $40
Option 4
9HD001, 9HD011, 9HD014, 9HD024, 9HD027, 9HD041
9HD001, 9HD011, 9HD014, 9HD024, 9HD027, 9HD041
9HD001, 9HD011, 9HD014, 9HD024, 9HD027, 9HD041
9HD001, 9HD011, 9HD014, 9HD024, 9HD027, 9HD041
The following Rx options are available for the plans listed:
$40$5 None $20
Generic only$10 None Generic only
Ded / 80%See Rx Options
below
$500$1,000$1,500$2,000$4,000$6,000$8,000
$1,500$3,000$4,500$6,000$12,000$18,000$24,000
$1,500$2,000$3,000$4,000$5,000
$4,500$6,000$9,000$12,000$15,000 ✓
80%
IAC Traditions PlanDeductible and coinsurance apply in or out-of-network*Out of pocket does not incude deductible
$250 Copay -Ded / 80%
See Rx Optionsbelow100%
$1,000$1,500$2,000$5,000
$3,000$4,500$6,000$15,000
$4,000$6,000$8,000
$8,000$12,000$16,000
IAC Premium Advantage (Deductible and Outof Pocket varies. Please see Evidence of Coverage)
Deductible and coinsurance apply in or out-of-network* Out of Pocket does not include deductible
Deductible and coinsurance apply in or out-of-network* Out of Pocket does not include deductible
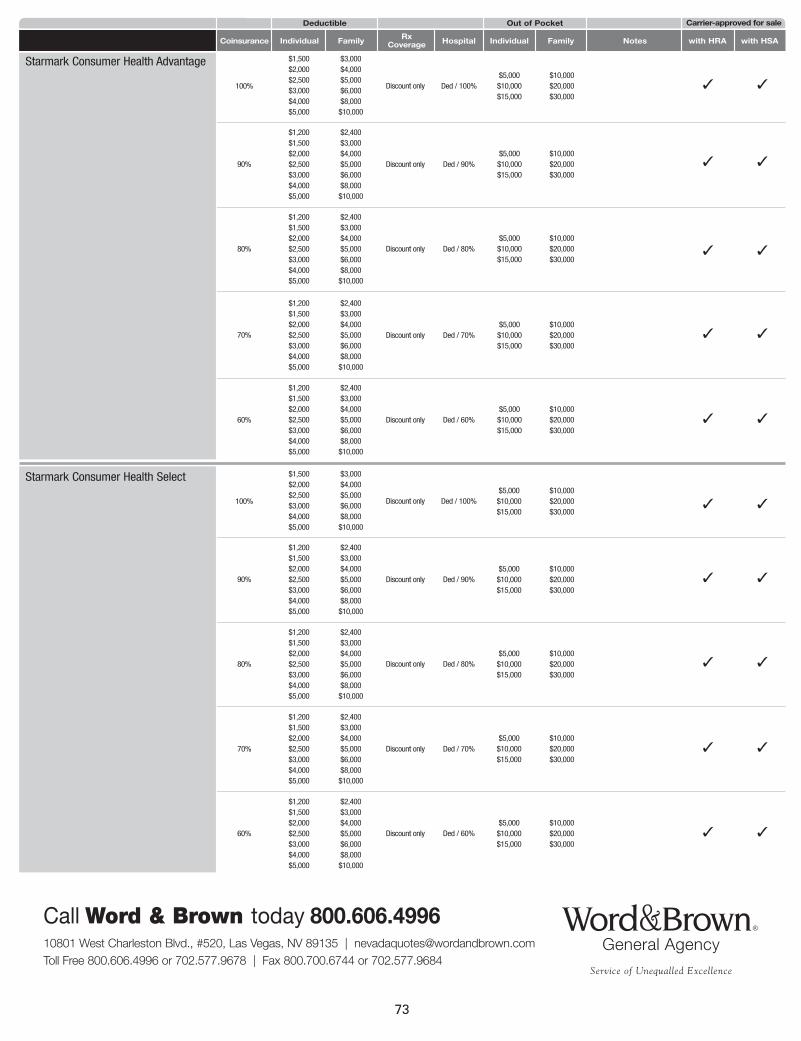
73
10801 West Charleston Blvd., #520, Las Vegas, NV 89135 | [email protected] Free 800.606.4996 or 702.577.9678 | Fax 800.700.6744 or 702.577.9684
Call Word & Brown today 800.606.4996
Coinsurance Rx Coverage Hospital
Out of Pocket Carrier-approved for sale
Individual Family Individual Family Notes with HRA with HSA
Deductible
70%
60%
Ded / 70%Discount only
$1,200$1,500$2,000$2,500$3,000$4,000$5,000
$2,400$3,000$4,000$5,000$6,000$8,000$10,000
✓
Ded / 60%Discount only
$1,200$1,500$2,000$2,500$3,000$4,000$5,000
$2,400$3,000$4,000$5,000$6,000$8,000$10,000
✓
$5,000$10,000$15,000
$10,000$20,000$30,000
$5,000$10,000$15,000
$10,000$20,000$30,000
Ded / 100%Discount only100%
$1,500$2,000$2,500$3,000$4,000$5,000
$3,000$4,000$5,000$6,000$8,000$10,000
$5,000$10,000$15,000
$10,000$20,000$30,000
✓
Ded / 90%Discount only
$1,200$1,500$2,000$2,500$3,000$4,000$5,000
$2,400$3,000$4,000$5,000$6,000$8,000$10,000
✓
Ded / 80%Discount only
$1,200$1,500$2,000$2,500$3,000$4,000$5,000
$2,400$3,000$4,000$5,000$6,000$8,000$10,000
✓
90%
80%
Starmark Consumer Health Advantage
$5,000$10,000$15,000
$10,000$20,000$30,000
$5,000$10,000$15,000
$10,000$20,000$30,000
✓
✓
✓
✓
✓
70%
100%
90%
80%
60%
Starmark Consumer Health Select
Ded / 100%Discount only
$1,500$2,000$2,500$3,000$4,000$5,000
$3,000$4,000$5,000$6,000$8,000$10,000
✓
Ded / 90%Discount only
$1,200$1,500$2,000$2,500$3,000$4,000$5,000
$2,400$3,000$4,000$5,000$6,000$8,000$10,000
✓
Ded / 80%Discount only
$1,200$1,500$2,000$2,500$3,000$4,000$5,000
$2,400$3,000$4,000$5,000$6,000$8,000$10,000
✓
Ded / 70%Discount only
$1,200$1,500$2,000$2,500$3,000$4,000$5,000
$2,400$3,000$4,000$5,000$6,000$8,000$10,000
✓
Ded / 60%Discount only
$1,200$1,500$2,000$2,500$3,000$4,000$5,000
$2,400$3,000$4,000$5,000$6,000$8,000$10,000
✓
$5,000$10,000$15,000
$10,000$20,000$30,000
$5,000$10,000$15,000
$10,000$20,000$30,000
$5,000$10,000$15,000
$10,000$20,000$30,000
$5,000$10,000$15,000
$10,000$20,000$30,000
$5,000$10,000$15,000
$10,000$20,000$30,000
✓
✓
✓
✓
✓
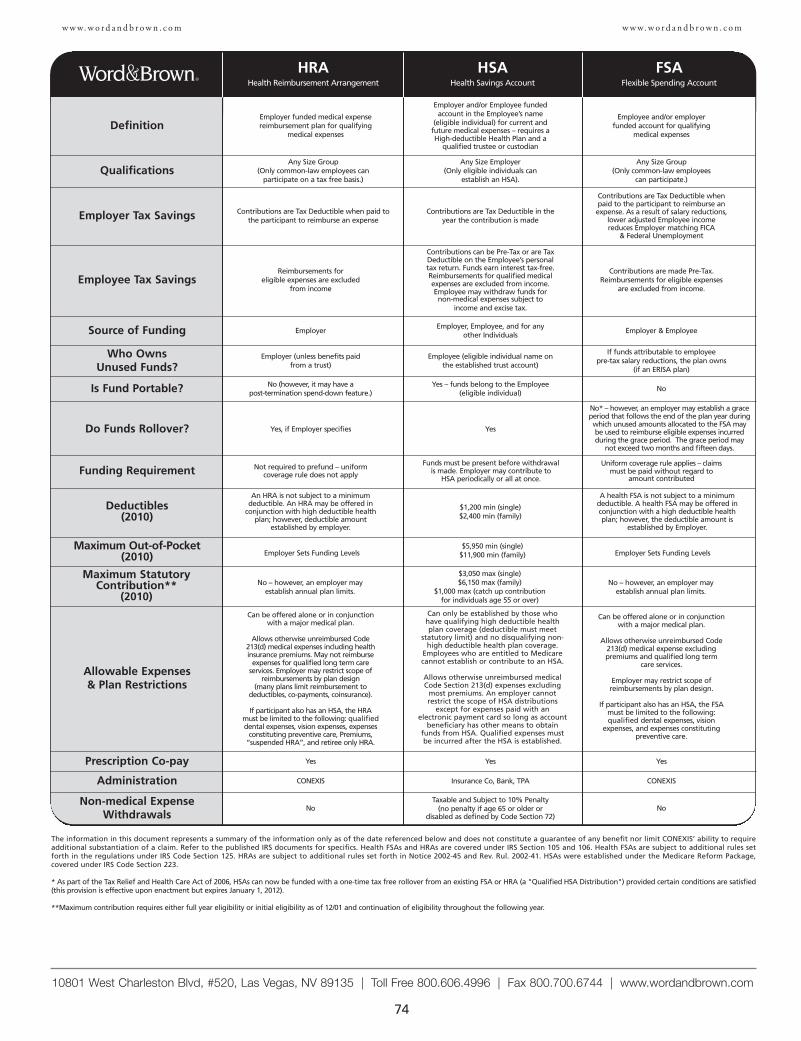
74
w w w. w o r d a n d b r o w n . c o m
10801 West Charleston Blvd, #520, Las Vegas, NV 89135 | Toll Free 800.606.4996 | Fax 800.700.6744 | www.wordandbrown.com
Employer funded medical expensereimbursement plan for qualifying
medical expenses
Employer and/or Employee fundedaccount in the Employee’s name
(eligible individual) for current and future medical expenses – requires aHigh-deductible Health Plan and a
qualified trustee or custodian
DefinitionEmployee and/or employer
funded account for qualifying medical expenses
Any Size Group (Only common-law employees can
participate on a tax free basis.)
Any Size Employer(Only eligible individuals can
establish an HSA).Qualifications
Any Size Group(Only common-law employees
can participate.)
Contributions are Tax Deductible when paid tothe participant to reimburse an expense
Contributions are Tax Deductible in theyear the contribution is madeEmployer Tax Savings
Contributions are Tax Deductible whenpaid to the participant to reimburse anexpense. As a result of salary reductions,
lower adjusted Employee income reduces Employer matching FICA
& Federal Unemployment
An HRA is not subject to a minimum deductible. An HRA may be offered in
conjunction with high deductible healthplan; however, deductible amount
established by employer.
$1,200 min (single)$2,400 min (family)
Deductibles(2010)
A health FSA is not subject to a minimumdeductible. A health FSA may be offered inconjunction with a high deductible healthplan; however, the deductible amount is
established by Employer.
Employer Sets Funding Levels$5,950 min (single)
$11,900 min (family)Maximum Out-of-Pocket
(2010) Employer Sets Funding Levels
Employer Employer, Employee, and for any
other IndividualsSource of Funding Employer & Employee
Employer (unless benefits paid from a trust)
Employee (eligible individual name onthe established trust account)
Who Owns Unused Funds?
If funds attributable to employee pre-tax salary reductions, the plan owns
(if an ERISA plan)
Can be offered alone or in conjunctionwith a major medical plan.
Allows otherwise unreimbursed Code213(d) medical expenses including healthinsurance premiums. May not reimburse
expenses for qualified long term careservices. Employer may restrict scope of
reimbursements by plan design (many plans limit reimbursement to
deductibles, co-payments, coinsurance).
If participant also has an HSA, the HRAmust be limited to the following: qualifieddental expenses, vision expenses, expenses
constituting preventive care, Premiums,“suspended HRA”, and retiree only HRA.
Can only be established by those whohave qualifying high deductible healthplan coverage (deductible must meet
statutory limit) and no disqualifying non-high deductible health plan coverage.
Employees who are entitled to Medicarecannot establish or contribute to an HSA.
Allows otherwise unreimbursed medicalCode Section 213(d) expenses excluding
most premiums. An employer cannotrestrict the scope of HSA distributions
except for expenses paid with anelectronic payment card so long as account
beneficiary has other means to obtainfunds from HSA. Qualified expenses mustbe incurred after the HSA is established.
Allowable Expenses & Plan Restrictions
Can be offered alone or in conjunctionwith a major medical plan.
Allows otherwise unreimbursed Code213(d) medical expense excludingpremiums and qualified long term
care services.
Employer may restrict scope ofreimbursements by plan design.
If participant also has an HSA, the FSA must be limited to the following:qualified dental expenses, vision
expenses, and expenses constitutingpreventive care.
No (however, it may have a post-termination spend-down feature.)
Yes – funds belong to the Employee(eligible individual)Is Fund Portable? No
Yes YesPrescription Co-pay Yes
CONEXIS Insurance Co, Bank, TPAAdministration CONEXIS
Yes, if Employer specifies YesDo Funds Rollover?
No* – however, an employer may establish a graceperiod that follows the end of the plan year duringwhich unused amounts allocated to the FSA maybe used to reimburse eligible expenses incurredduring the grace period. The grace period may
not exceed two months and fifteen days.
Not required to prefund – uniformcoverage rule does not apply
Funds must be present before withdrawal is made. Employer may contribute to
HSA periodically or all at once.Funding Requirement
Uniform coverage rule applies – claims must be paid without regard to
amount contributed
NoTaxable and Subject to 10% Penalty
(no penalty if age 65 or older or disabled as defined by Code Section 72)
Non-medical ExpenseWithdrawals
No
Reimbursements for eligible expenses are excluded
from income
Contributions can be Pre-Tax or are TaxDeductible on the Employee’s personaltax return. Funds earn interest tax-free.Reimbursements for qualified medicalexpenses are excluded from income.Employee may withdraw funds for non-medical expenses subject to
income and excise tax.
Employee Tax SavingsContributions are made Pre-Tax.
Reimbursements for eligible expenses are excluded from income.
The information in this document represents a summary of the information only as of the date referenced below and does not constitute a guarantee of any benefit nor limit CONEXIS’ ability to requireadditional substantiation of a claim. Refer to the published IRS documents for specifics. Health FSAs and HRAs are covered under IRS Section 105 and 106. Health FSAs are subject to additional rules setforth in the regulations under IRS Code Section 125. HRAs are subject to additional rules set forth in Notice 2002-45 and Rev. Rul. 2002-41. HSAs were established under the Medicare Reform Package,covered under IRS Code Section 223.
* As part of the Tax Relief and Health Care Act of 2006, HSAs can now be funded with a one-time tax free rollover from an existing FSA or HRA (a "Qualified HSA Distribution") provided certain conditions are satisfied(this provision is effective upon enactment but expires January 1, 2012).
**Maximum contribution requires either full year eligibility or initial eligibility as of 12/01 and continuation of eligibility throughout the following year.
No – however, an employer may establish annual plan limits.
$3,050 max (single)$6,150 max (family)
$1,000 max (catch up contribution for individuals age 55 or over)
Maximum StatutoryContribution**
(2010)
No – however, an employer may establish annual plan limits.
HRAHealth Reimbursement Arrangement
HSAHealth Savings Account
FSAFlexible Spending Account
w w w. w o r d a n d b r o w n . c o m
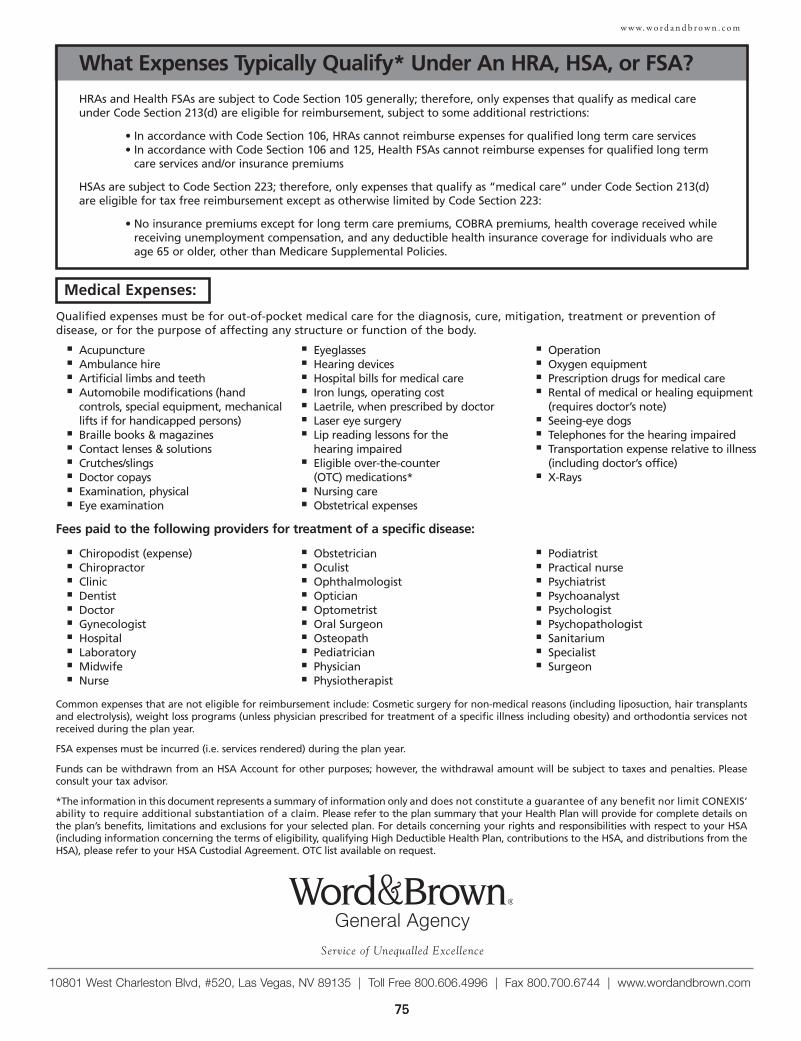
75
w w w. w o r d a n d b r o w n . c o m
10801 West Charleston Blvd, #520, Las Vegas, NV 89135 | Toll Free 800.606.4996 | Fax 800.700.6744 | www.wordandbrown.com
75
What Expenses Typically Qualify* Under An HRA, HSA, or FSA?
HRAs and Health FSAs are subject to Code Section 105 generally; therefore, only expenses that qualify as medical careunder Code Section 213(d) are eligible for reimbursement, subject to some additional restrictions:
• In accordance with Code Section 106, HRAs cannot reimburse expenses for qualified long term care services• In accordance with Code Section 106 and 125, Health FSAs cannot reimburse expenses for qualified long term
care services and/or insurance premiums
HSAs are subject to Code Section 223; therefore, only expenses that qualify as “medical care” under Code Section 213(d)are eligible for tax free reimbursement except as otherwise limited by Code Section 223:
• No insurance premiums except for long term care premiums, COBRA premiums, health coverage received whilereceiving unemployment compensation, and any deductible health insurance coverage for individuals who areage 65 or older, other than Medicare Supplemental Policies.
Medical Expenses:
Fees paid to the following providers for treatment of a specific disease:
■ Acupuncture■ Ambulance hire■ Artificial limbs and teeth■ Automobile modifications (hand
controls, special equipment, mechanicallifts if for handicapped persons)
■ Braille books & magazines■ Contact lenses & solutions■ Crutches/slings■ Doctor copays■ Examination, physical■ Eye examination
■ Eyeglasses■ Hearing devices■ Hospital bills for medical care■ Iron lungs, operating cost■ Laetrile, when prescribed by doctor■ Laser eye surgery■ Lip reading lessons for the
hearing impaired■ Eligible over-the-counter
(OTC) medications*■ Nursing care■ Obstetrical expenses
■ Operation■ Oxygen equipment■ Prescription drugs for medical care■ Rental of medical or healing equipment
(requires doctor’s note)■ Seeing-eye dogs■ Telephones for the hearing impaired■ Transportation expense relative to illness
(including doctor’s office)■ X-Rays
■ Chiropodist (expense)■ Chiropractor■ Clinic■ Dentist■ Doctor■ Gynecologist■ Hospital■ Laboratory■ Midwife■ Nurse
■ Obstetrician■ Oculist■ Ophthalmologist■ Optician■ Optometrist■ Oral Surgeon■ Osteopath■ Pediatrician■ Physician■ Physiotherapist
■ Podiatrist■ Practical nurse■ Psychiatrist■ Psychoanalyst■ Psychologist■ Psychopathologist■ Sanitarium■ Specialist■ Surgeon
Common expenses that are not eligible for reimbursement include: Cosmetic surgery for non-medical reasons (including liposuction, hair transplantsand electrolysis), weight loss programs (unless physician prescribed for treatment of a specific illness including obesity) and orthodontia services notreceived during the plan year.
FSA expenses must be incurred (i.e. services rendered) during the plan year.
Funds can be withdrawn from an HSA Account for other purposes; however, the withdrawal amount will be subject to taxes and penalties. Pleaseconsult your tax advisor.
*The information in this document represents a summary of information only and does not constitute a guarantee of any benefit nor limit CONEXIS’ability to require additional substantiation of a claim. Please refer to the plan summary that your Health Plan will provide for complete details onthe plan’s benefits, limitations and exclusions for your selected plan. For details concerning your rights and responsibilities with respect to your HSA(including information concerning the terms of eligibility, qualifying High Deductible Health Plan, contributions to the HSA, and distributions from theHSA), please refer to your HSA Custodial Agreement. OTC list available on request.
Qualified expenses must be for out-of-pocket medical care for the diagnosis, cure, mitigation, treatment or prevention ofdisease, or for the purpose of affecting any structure or function of the body.
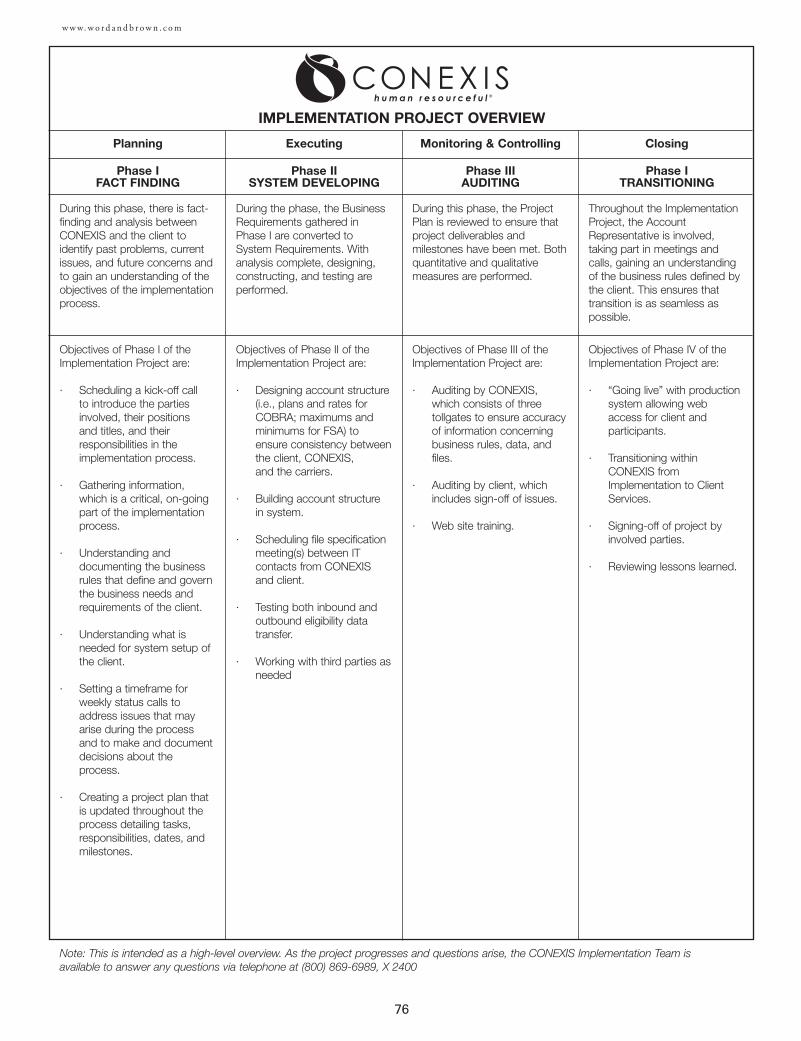
76
w w w. w o r d a n d b r o w n . c o m
Planning
During this phase, there is fact-finding and analysis betweenCONEXIS and the client toidentify past problems, currentissues, and future concerns andto gain an understanding of theobjectives of the implementationprocess.
IMPLEMENTATION PROJECT OVERVIEW
Phase IFACT FINDING
Executing
Phase IISYSTEM DEVELOPING
Monitoring & Controlling
Phase IIIAUDITING
Closing
Phase ITRANSITIONING
Objectives of Phase I of theImplementation Project are:
· Scheduling a kick-off call to introduce the partiesinvolved, their positions and titles, and theirresponsibilities in theimplementation process.
· Gathering information,which is a critical, on-goingpart of the implementationprocess.
· Understanding anddocumenting the businessrules that define and governthe business needs andrequirements of the client.
· Understanding what isneeded for system setup ofthe client.
· Setting a timeframe forweekly status calls toaddress issues that mayarise during the processand to make and documentdecisions about theprocess.
· Creating a project plan thatis updated throughout theprocess detailing tasks,responsibilities, dates, andmilestones.
During the phase, the BusinessRequirements gathered inPhase I are converted toSystem Requirements. Withanalysis complete, designing,constructing, and testing areperformed.
Objectives of Phase II of theImplementation Project are:
· Designing account structure(i.e., plans and rates forCOBRA; maximums andminimums for FSA) toensure consistency between the client, CONEXIS, and the carriers.
· Building account structurein system.
· Scheduling file specificationmeeting(s) between ITcontacts from CONEXISand client.
· Testing both inbound andoutbound eligibility datatransfer.
· Working with third parties asneeded
During this phase, the ProjectPlan is reviewed to ensure thatproject deliverables andmilestones have been met. Bothquantitative and qualitativemeasures are performed.
Objectives of Phase III of theImplementation Project are:
· Auditing by CONEXIS,which consists of threetollgates to ensure accuracyof information concerningbusiness rules, data, andfiles.
· Auditing by client, whichincludes sign-off of issues.
· Web site training.
Throughout the ImplementationProject, the AccountRepresentative is involved,taking part in meetings andcalls, gaining an understandingof the business rules defined bythe client. This ensures thattransition is as seamless aspossible.
Objectives of Phase IV of theImplementation Project are:
· “Going live” with productionsystem allowing webaccess for client andparticipants.
· Transitioning withinCONEXIS fromImplementation to ClientServices.
· Signing-off of project byinvolved parties.
· Reviewing lessons learned.
Note: This is intended as a high-level overview. As the project progresses and questions arise, the CONEXIS Implementation Team isavailable to answer any questions via telephone at (800) 869-6989, X 2400
77
DENTAL
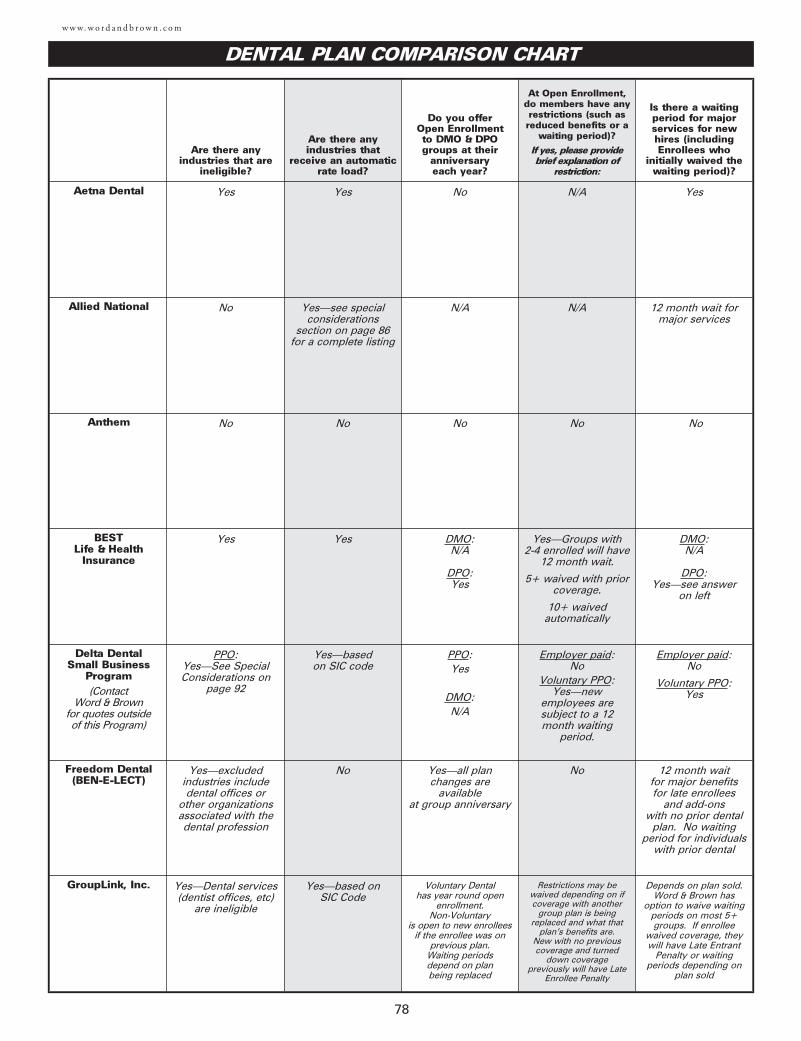
w w w. w o r d a n d b r o w n . c o m
78
DENTAL PLAN COMPARISON CHART
Are there anyindustries that are
ineligible?
Are there anyindustries that
receive an automaticrate load?
Do you offer Open Enrollment to DMO & DPOgroups at their
anniversary each year?
At Open Enrollment,do members have anyrestrictions (such asreduced benefits or a
waiting period)?
If yes, please providebrief explanation of
restriction:
Is there a waitingperiod for majorservices for newhires (includingEnrollees who
initially waived thewaiting period)?
Aetna Dental Yes Yes No N/A Yes
Allied National No Yes—see specialconsiderations
section on page 86for a complete listing
N/A N/A 12 month wait for major services
Anthem No No No No No
BEST Life & Health
Insurance
Yes Yes DMO:N/A
DPO:Yes
Yes—Groups with 2-4 enrolled will have
12 month wait.
5+ waived with priorcoverage.
10+ waivedautomatically
DMO:N/A
DPO:Yes—see answer
on left
Delta DentalSmall Business
Program(Contact
Word & Brown for quotes outside of this Program)
PPO:Yes—See SpecialConsiderations on
page 92
Yes—based on SIC code
PPO:Yes
DMO:N/A
Employer paid: No
Voluntary PPO:Yes—new
employees aresubject to a 12month waiting
period.
Employer paid:No
Voluntary PPO:Yes
Freedom Dental(BEN-E-LECT)
Yes—excludedindustries includedental offices or
other organizationsassociated with thedental profession
No Yes—all plan changes are
available at group anniversary
No 12 month wait for major benefits for late enrollees
and add-ons with no prior dental
plan. No waitingperiod for individuals
with prior dental
GroupLink, Inc. Yes—Dental services(dentist offices, etc)
are ineligible
Yes—based on SIC Code
Voluntary Dental has year round open
enrollment. Non-Voluntary
is open to new enrollees if the enrollee was on
previous plan. Waiting periods depend on plan being replaced
Restrictions may bewaived depending on ifcoverage with another
group plan is beingreplaced and what that
plan’s benefits are. New with no previouscoverage and turned
down coveragepreviously will have Late
Enrollee Penalty
Depends on plan sold. Word & Brown has
option to waive waitingperiods on most 5+groups. If enrollee
waived coverage, theywill have Late Entrant
Penalty or waitingperiods depending on
plan sold
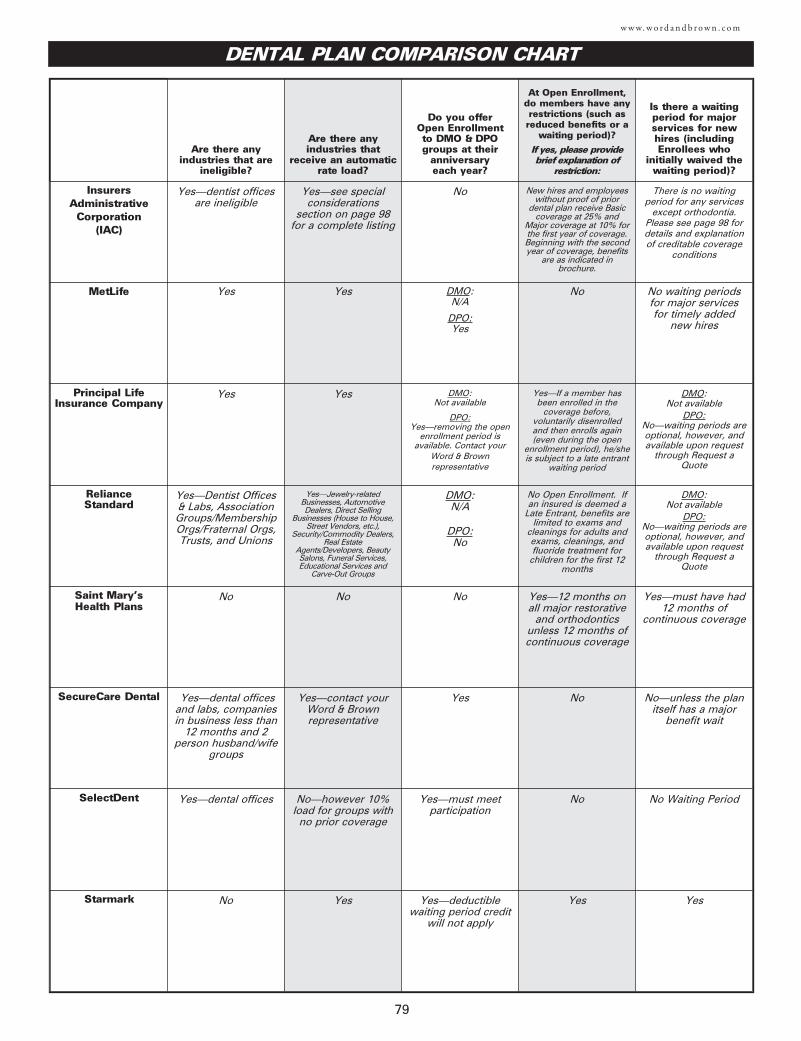
79
w w w. w o r d a n d b r o w n . c o m
DENTAL PLAN COMPARISON CHART
Are there anyindustries that are
ineligible?
Are there anyindustries that
receive an automaticrate load?
Do you offer Open Enrollment to DMO & DPOgroups at their
anniversary each year?
At Open Enrollment,do members have anyrestrictions (such asreduced benefits or a
waiting period)?
If yes, please providebrief explanation of
restriction:
Is there a waitingperiod for majorservices for newhires (includingEnrollees who
initially waived thewaiting period)?
InsurersAdministrative
Corporation (IAC)
Yes—dentist offices are ineligible
Yes—see specialconsiderations
section on page 98for a complete listing
No New hires and employeeswithout proof of prior
dental plan receive Basiccoverage at 25% and
Major coverage at 10% forthe first year of coverage.Beginning with the secondyear of coverage, benefits
are as indicated inbrochure.
There is no waitingperiod for any services
except orthodontia.Please see page 98 fordetails and explanationof creditable coverage
conditions
MetLife Yes Yes DMO:N/A
DPO:Yes
No No waiting periodsfor major services for timely added
new hires
Principal LifeInsurance Company
Yes Yes DMO:Not available
DPO:Yes—removing the open
enrollment period isavailable. Contact your
Word & Brownrepresentative
Yes—If a member hasbeen enrolled in the
coverage before,voluntarily disenrolledand then enrolls again(even during the open
enrollment period), he/sheis subject to a late entrant
waiting period
DMO:Not available
DPO:No—waiting periods areoptional, however, and available upon request
through Request aQuote
Reliance Standard
Yes—Dentist Offices & Labs, AssociationGroups/MembershipOrgs/Fraternal Orgs,Trusts, and Unions
Yes—Jewelry-relatedBusinesses, AutomotiveDealers, Direct Selling
Businesses (House to House,Street Vendors, etc.),
Security/Commodity Dealers,Real Estate
Agents/Developers, BeautySalons, Funeral Services,Educational Services and
Carve-Out Groups
DMO:N/A
DPO:No
No Open Enrollment. Ifan insured is deemed a
Late Entrant, benefits arelimited to exams and
cleanings for adults andexams, cleanings, andfluoride treatment for
children for the first 12months
DMO:Not available
DPO:No—waiting periods areoptional, however, and available upon request
through Request aQuote
Saint Mary’sHealth Plans
No No No Yes—12 months onall major restorative
and orthodonticsunless 12 months ofcontinuous coverage
Yes—must have had12 months of
continuous coverage
SecureCare Dental Yes—dental offices and labs, companiesin business less than
12 months and 2person husband/wife
groups
Yes—contact your Word & Brownrepresentative
Yes No No—unless the planitself has a major
benefit wait
SelectDent Yes—dental offices No—however 10% load for groups with
no prior coverage
Yes—must meetparticipation
No No Waiting Period
Starmark No Yes Yes—deductiblewaiting period credit
will not apply
Yes Yes
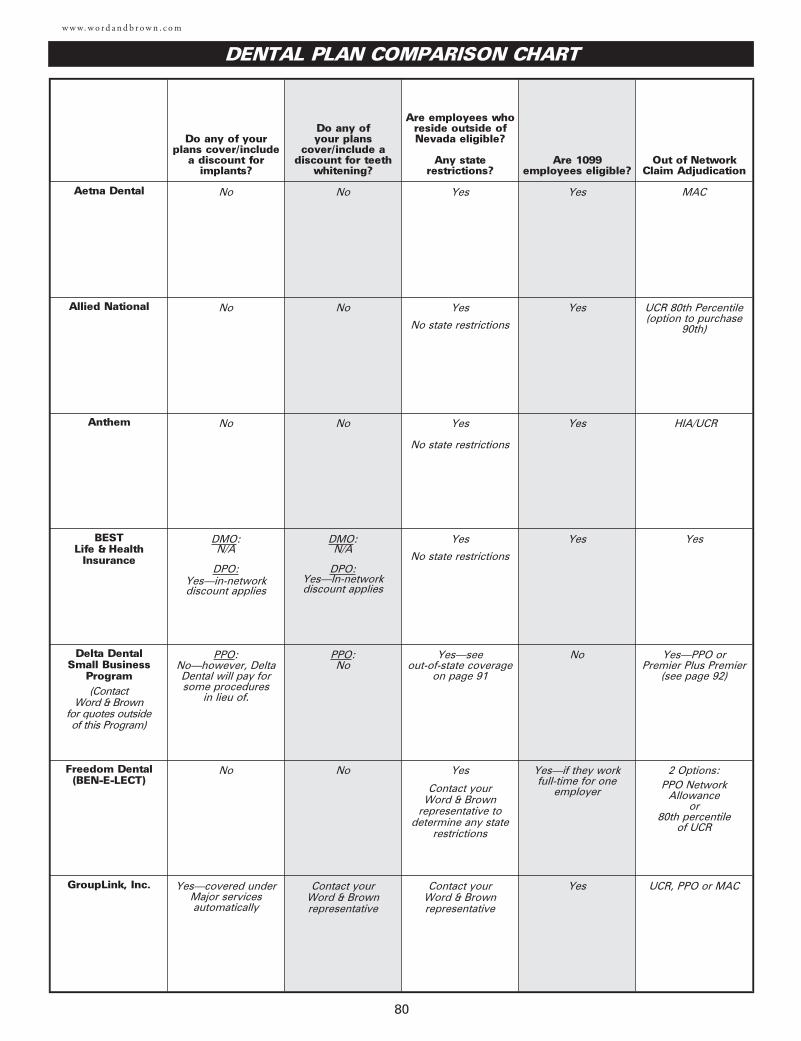
80
Do any of your plans cover/include
a discount forimplants?
Do any of your plans
cover/include adiscount for teeth
whitening?
Are employees whoreside outside ofNevada eligible?
Any staterestrictions?
Are 1099employees eligible?
Out of NetworkClaim Adjudication
Aetna Dental No No Yes Yes MAC
Allied National No No Yes
No state restrictions
Yes UCR 80th Percentile(option to purchase
90th)
Anthem No No Yes
No state restrictions
Yes HIA/UCR
BEST Life & Health
Insurance
DMO:N/A
DPO:Yes—in-networkdiscount applies
DMO:N/A
DPO:Yes—In-network discount applies
Yes
No state restrictions
Yes Yes
Delta DentalSmall Business
Program(Contact
Word & Brown for quotes outside of this Program)
PPO:No—however, DeltaDental will pay forsome procedures
in lieu of.
PPO:No
Yes—see out-of-state coverage
on page 91
No Yes—PPO orPremier Plus Premier
(see page 92)
Freedom Dental(BEN-E-LECT)
No No Yes
Contact your Word & Brown
representative to determine any state
restrictions
Yes—if they work full-time for one
employer
2 Options:PPO Network
Allowance or
80th percentile of UCR
GroupLink, Inc. Yes—covered underMajor servicesautomatically
Contact your Word & Brownrepresentative
Contact your Word & Brownrepresentative
Yes UCR, PPO or MAC
w w w. w o r d a n d b r o w n . c o m
DENTAL PLAN COMPARISON CHART
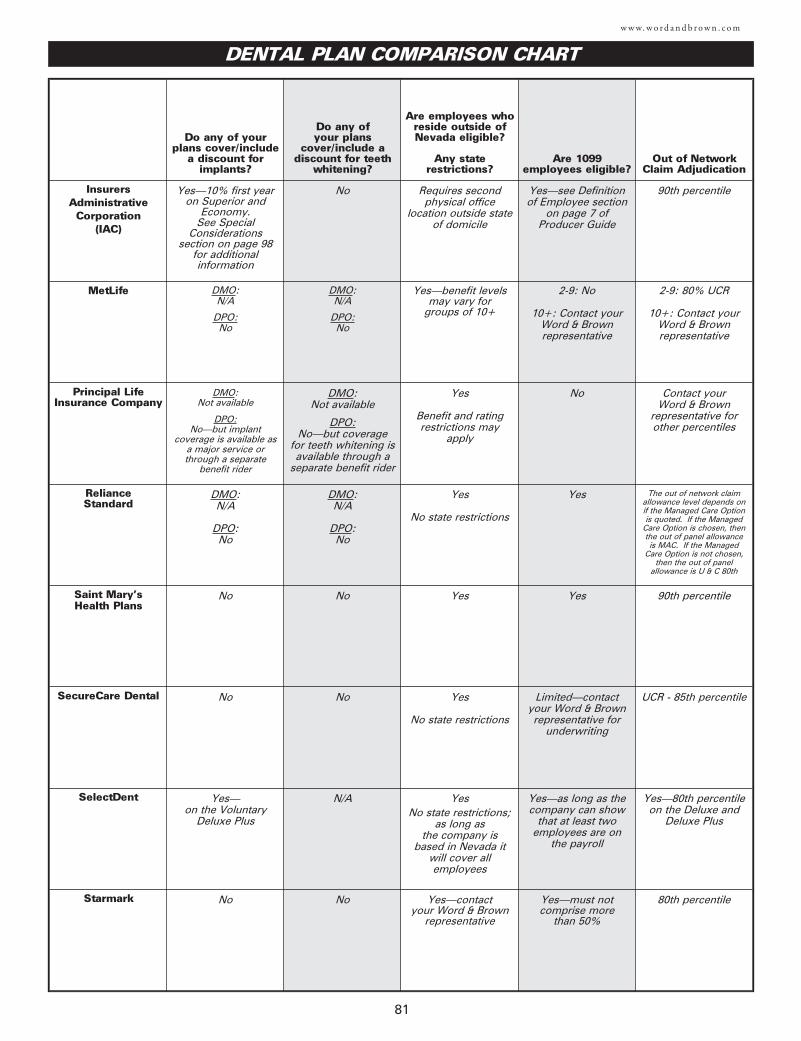
81
w w w. w o r d a n d b r o w n . c o m
Do any of your plans cover/include
a discount forimplants?
Do any of your plans
cover/include adiscount for teeth
whitening?
Are employees whoreside outside ofNevada eligible?
Any staterestrictions?
Are 1099employees eligible?
Out of NetworkClaim Adjudication
InsurersAdministrative
Corporation (IAC)
Yes—10% first year on Superior and
Economy. See Special
Considerationssection on page 98
for additional information
No Requires secondphysical office
location outside stateof domicile
Yes—see Definitionof Employee section
on page 7 ofProducer Guide
90th percentile
MetLife DMO:N/A
DPO:No
DMO:N/A
DPO:No
Yes—benefit levelsmay vary for
groups of 10+
2-9: No
10+: Contact yourWord & Brownrepresentative
2-9: 80% UCR
10+: Contact yourWord & Brownrepresentative
Principal LifeInsurance Company
DMO:Not available
DPO:No—but implant
coverage is available asa major service orthrough a separate
benefit rider
DMO:Not available
DPO:No—but coverage
for teeth whitening isavailable through a
separate benefit rider
Yes
Benefit and ratingrestrictions may
apply
No Contact your Word & Brown
representative for other percentiles
Reliance Standard
DMO:N/A
DPO:No
DMO:N/A
DPO:No
Yes
No state restrictions
Yes The out of network claimallowance level depends onif the Managed Care Optionis quoted. If the Managed
Care Option is chosen, thenthe out of panel allowanceis MAC. If the Managed
Care Option is not chosen,then the out of panel
allowance is U & C 80th
Saint Mary’sHealth Plans
No No Yes Yes 90th percentile
SecureCare Dental No No Yes
No state restrictions
Limited—contactyour Word & Brownrepresentative for
underwriting
UCR - 85th percentile
SelectDent Yes—on the Voluntary
Deluxe Plus
N/A YesNo state restrictions;
as long as the company is
based in Nevada itwill cover allemployees
Yes—as long as thecompany can show
that at least twoemployees are on
the payroll
Yes—80th percentile on the Deluxe and
Deluxe Plus
Starmark No No Yes—contactyour Word & Brown
representative
Yes—must notcomprise more
than 50%
80th percentile
DENTAL PLAN COMPARISON CHART
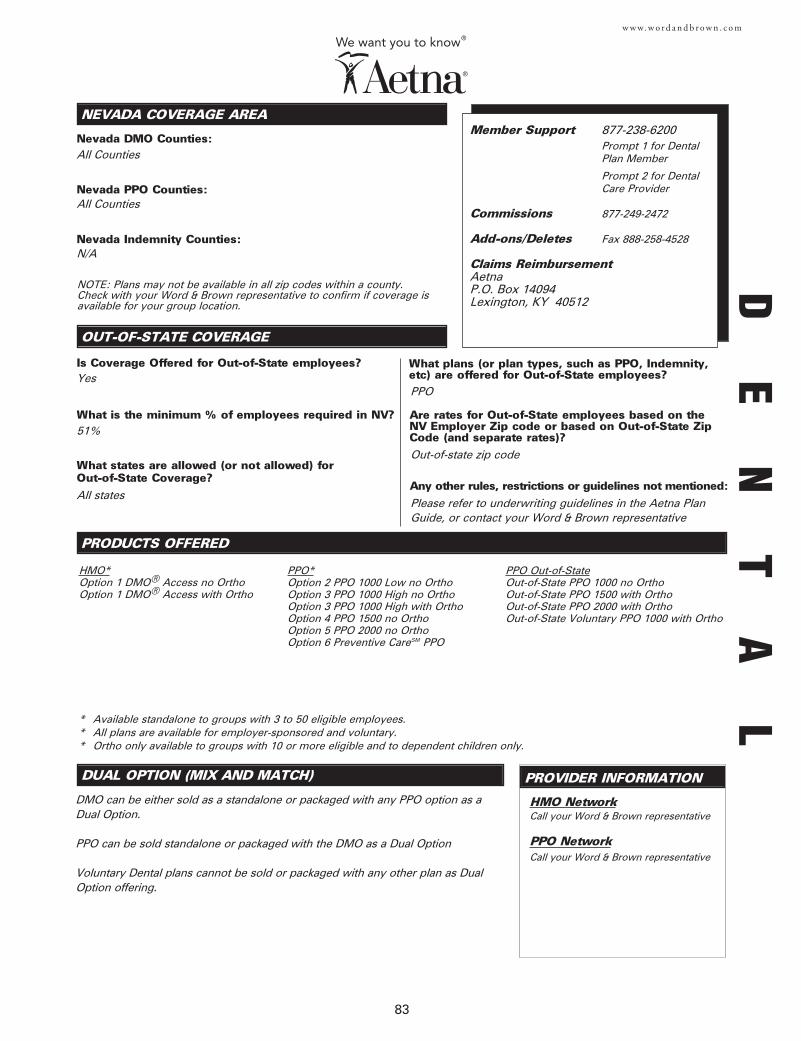
OUT-OF-STATE COVERAGE
NEVADA COVERAGE AREA
Nevada DMO Counties:
PRODUCTS OFFERED
Nevada PPO Counties:
Is Coverage Offered for Out-of-State employees?
What is the minimum % of employees required in NV?
What plans (or plan types, such as PPO, Indemnity,etc) are offered for Out-of-State employees?
What states are allowed (or not allowed) for Out-of-State Coverage?
Are rates for Out-of-State employees based on theNV Employer Zip code or based on Out-of-State ZipCode (and separate rates)?
Any other rules, restrictions or guidelines not mentioned:
83
w w w. w o r d a n d b r o w n . c o m
Member Support 877-238-6200Prompt 1 for Dental Plan Member
Prompt 2 for Dental Care Provider
Commissions 877-249-2472
Add-ons/Deletes Fax 888-258-4528
Claims ReimbursementAetnaP.O. Box 14094Lexington, KY 40512
All Counties
All Counties
HMO*Option 1 DMO® Access no OrthoOption 1 DMO® Access with Ortho
NOTE: Plans may not be available in all zip codes within a county. Check with your Word & Brown representative to confirm if coverage isavailable for your group location.
Yes
51%
All statesPlease refer to underwriting guidelines in the Aetna PlanGuide, or contact your Word & Brown representative
Out-of-state zip code
PPO
DE
NT
AL
DUAL OPTION (MIX AND MATCH)
DMO can be either sold as a standalone or packaged with any PPO option as aDual Option.
PPO can be sold standalone or packaged with the DMO as a Dual Option
Voluntary Dental plans cannot be sold or packaged with any other plan as DualOption offering.
PROVIDER INFORMATION
HMO Network
PPO Network
Call your Word & Brown representative
Call your Word & Brown representative
PPO*Option 2 PPO 1000 Low no OrthoOption 3 PPO 1000 High no OrthoOption 3 PPO 1000 High with OrthoOption 4 PPO 1500 no OrthoOption 5 PPO 2000 no OrthoOption 6 Preventive CareSM PPO
PPO Out-of-StateOut-of-State PPO 1000 no OrthoOut-of-State PPO 1500 with OrthoOut-of-State PPO 2000 with OrthoOut-of-State Voluntary PPO 1000 with Ortho
* Available standalone to groups with 3 to 50 eligible employees.* All plans are available for employer-sponsored and voluntary.* Ortho only available to groups with 10 or more eligible and to dependent children only.
Nevada Indemnity Counties:N/A
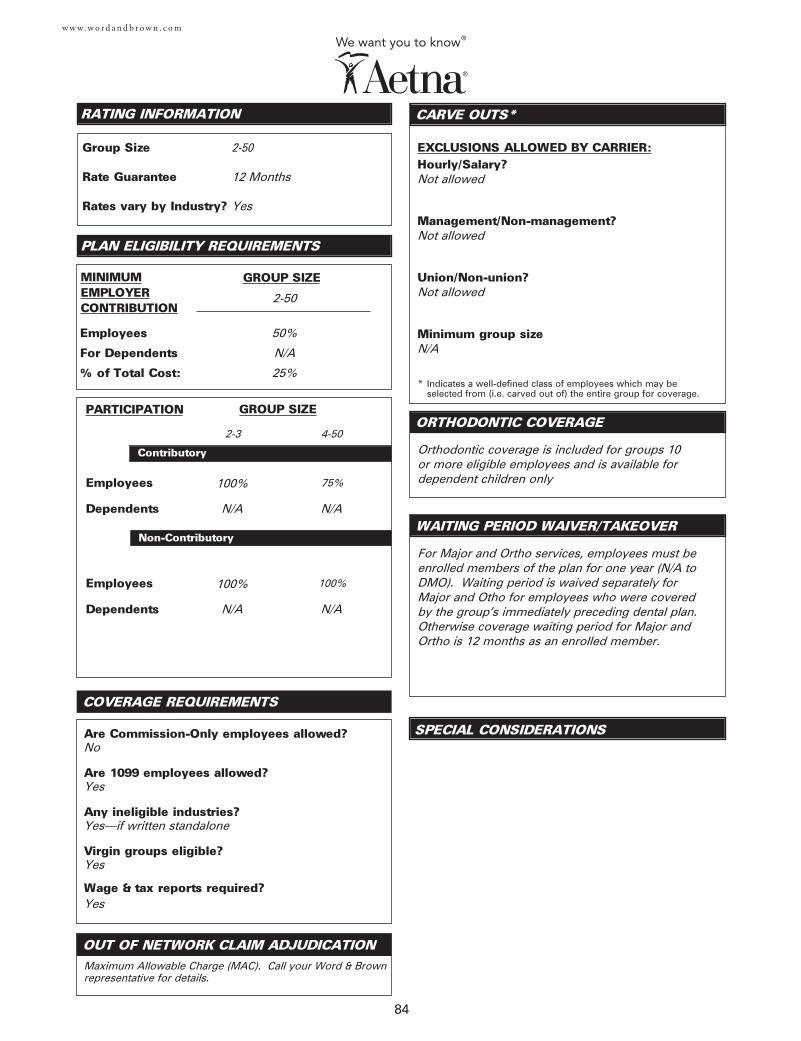
84
w w w. w o r d a n d b r o w n . c o m
Employees
Are Commission-Only employees allowed?
Are 1099 employees allowed?
Any ineligible industries?
Virgin groups eligible?
Wage & tax reports required?
Employees
For Dependents
% of Total Cost:
RATING INFORMATION
PARTICIPATION
Contributory
Non-Contributory
GROUP SIZE
GROUP SIZE
EXCLUSIONS ALLOWED BY CARRIER:Hourly/Salary?Not allowed
Management/Non-management?Not allowed
Union/Non-union?Not allowed
Minimum group sizeN/A
CARVE OUTS*
SPECIAL CONSIDERATIONS
ORTHODONTIC COVERAGE
WAITING PERIOD WAIVER/TAKEOVER
PLAN ELIGIBILITY REQUIREMENTS
OUT OF NETWORK CLAIM ADJUDICATION
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
Group Size
Rate Guarantee
Rates vary by Industry?
COVERAGE REQUIREMENTS
MINIMUMEMPLOYERCONTRIBUTION
2-50
2-50
12 Months
Yes
100%
No
Yes
Yes—if written standalone
Yes
Yes
Orthodontic coverage is included for groups 10 or more eligible employees and is available fordependent children only
2-3
Maximum Allowable Charge (MAC). Call your Word & Brownrepresentative for details.
4-50
75%
Dependents N/A N/A
50%
N/A
25%
Employees 100% 100%
Dependents N/A N/A
For Major and Ortho services, employees must beenrolled members of the plan for one year (N/A toDMO). Waiting period is waived separately forMajor and Otho for employees who were coveredby the group’s immediately preceding dental plan.Otherwise coverage waiting period for Major andOrtho is 12 months as an enrolled member.
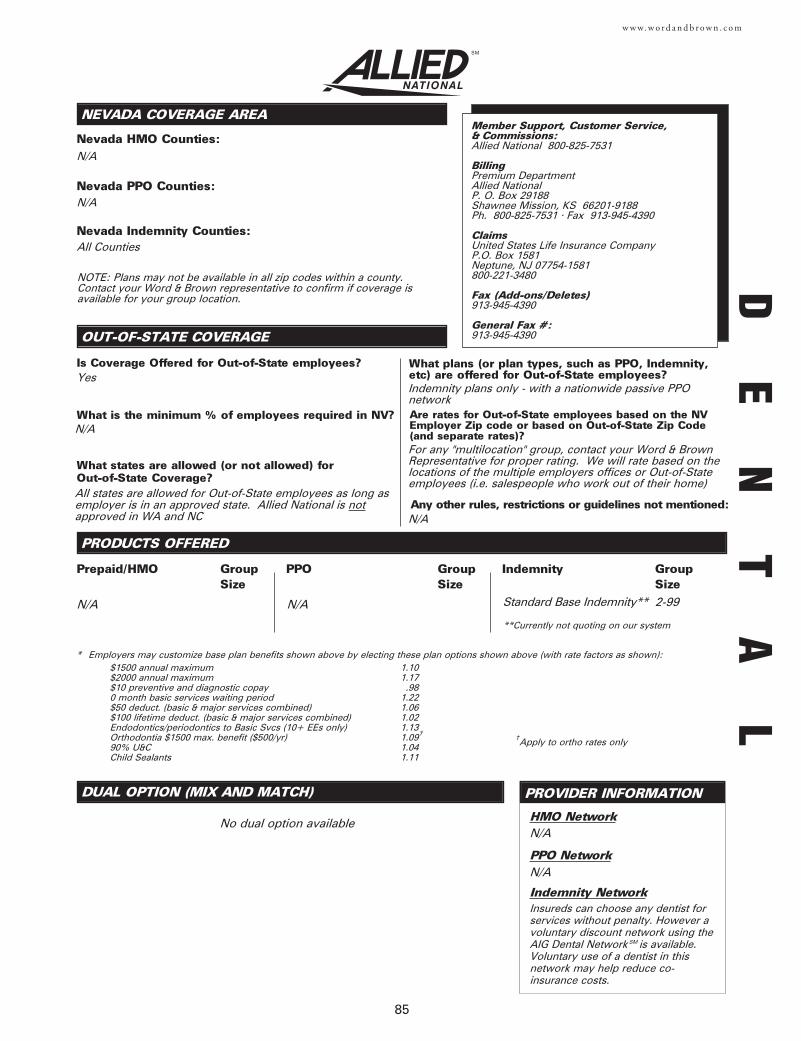
OUT-OF-STATE COVERAGE
NEVADA COVERAGE AREA
DUAL OPTION (MIX AND MATCH)
Nevada HMO Counties:
PROVIDER INFORMATION
PRODUCTS OFFERED
Nevada PPO Counties:
Nevada Indemnity Counties:
Is Coverage Offered for Out-of-State employees?
What is the minimum % of employees required in NV?
What plans (or plan types, such as PPO, Indemnity,etc) are offered for Out-of-State employees?
What states are allowed (or not allowed) for Out-of-State Coverage?
Are rates for Out-of-State employees based on the NVEmployer Zip code or based on Out-of-State Zip Code(and separate rates)?
Any other rules, restrictions or guidelines not mentioned:
85
w w w. w o r d a n d b r o w n . c o m
N/A
N/A
All Counties
N/A Standard Base Indemnity** 2-99
N/A
N/A
* Employers may customize base plan benefits shown above by electing these plan options shown above (with rate factors as shown):$1500 annual maximum 1.10$2000 annual maximum 1.17$10 preventive and diagnostic copay .980 month basic services waiting period 1.22$50 deduct. (basic & major services combined) 1.06$100 lifetime deduct. (basic & major services combined) 1.02Endodontics/periodontics to Basic Svcs (10+ EEs only) 1.13Orthodontia $1500 max. benefit ($500/yr) 1.09†
90% U&C 1.04Child Sealants 1.11
No dual option available
NOTE: Plans may not be available in all zip codes within a county. Contact your Word & Brown representative to confirm if coverage isavailable for your group location.
Yes
Insureds can choose any dentist forservices without penalty. However avoluntary discount network using theAIG Dental Network SM is available.Voluntary use of a dentist in thisnetwork may help reduce co-insurance costs.
HMO Network
PPO Network
Indemnity Network
Member Support, Customer Service, & Commissions:Allied National 800-825-7531
BillingPremium DepartmentAllied NationalP. O. Box 29188Shawnee Mission, KS 66201-9188Ph. 800-825-7531 • Fax 913-945-4390
ClaimsUnited States Life Insurance Company P.O. Box 1581 Neptune, NJ 07754-1581 800-221-3480
Fax (Add-ons/Deletes)913-945-4390
General Fax #:913-945-4390
Prepaid/HMO Group Size
PPO Group Size
Indemnity Group Size
†Apply to ortho rates only
**Currently not quoting on our system
N/A
All states are allowed for Out-of-State employees as long asemployer is in an approved state. Allied National is notapproved in WA and NC
Indemnity plans only - with a nationwide passive PPO network
For any "multilocation" group, contact your Word & BrownRepresentative for proper rating. We will rate based on thelocations of the multiple employers offices or Out-of-Stateemployees (i.e. salespeople who work out of their home)
N/A
N/A
DE
NT
AL
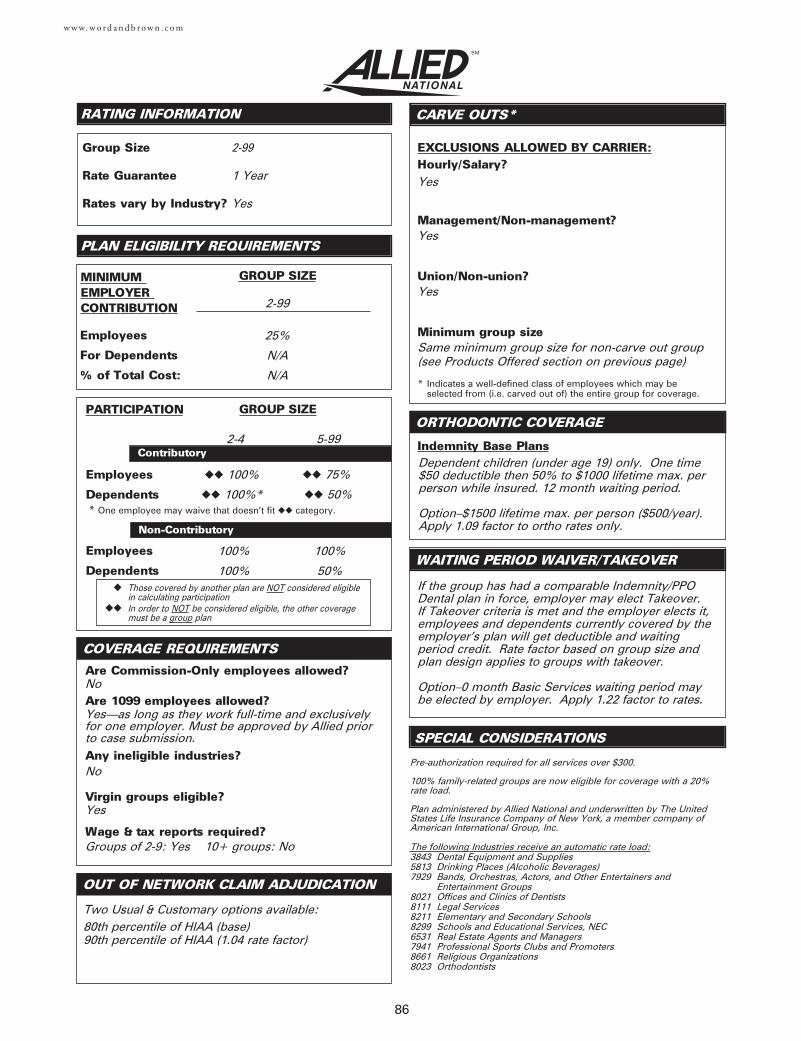
Employees
Dependents
Employees
Dependents
Employees
For Dependents
% of Total Cost:
RATING INFORMATION
MINIMUM EMPLOYER CONTRIBUTION
PARTICIPATION
Contributory
Non-Contributory
GROUP SIZE
GROUP SIZE
◆ Those covered by another plan are NOT considered eligible in calculating participation
◆◆ In order to NOT be considered eligible, the other coveragemust be a group plan
EXCLUSIONS ALLOWED BY CARRIER:Hourly/Salary?
Management/Non-management?
Union/Non-union?
Minimum group size
CARVE OUTS*
SPECIAL CONSIDERATIONS
ORTHODONTIC COVERAGE
PLAN ELIGIBILITY REQUIREMENTS
OUT OF NETWORK CLAIM ADJUDICATION
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
Group Size
Rate Guarantee
Rates vary by Industry?
COVERAGE REQUIREMENTS
86
w w w. w o r d a n d b r o w n . c o m
Are Commission-Only employees allowed?
Are 1099 employees allowed?
Any ineligible industries?
Virgin groups eligible?
Wage & tax reports required?
If the group has had a comparable Indemnity/PPODental plan in force, employer may elect Takeover. If Takeover criteria is met and the employer elects it,employees and dependents currently covered by theemployer’s plan will get deductible and waitingperiod credit. Rate factor based on group size andplan design applies to groups with takeover.
Option–0 month Basic Services waiting period maybe elected by employer. Apply 1.22 factor to rates.
Indemnity Base Plans
Are Commission-Only employees allowed?
Are 1099 employees allowed?
Any ineligible industries?
Virgin groups eligible?
NUCS 4072/NUCS 4073 statements required?
Yes
Yes
Yes
Same minimum group size for non-carve out group(see Products Offered section on previous page)
2-4
2-99
25%
N/A
N/A
2-99
1 Year
Yes
5-99
◆◆ 75%
◆◆ 50%
100%
100%
100%
50%
Pre-authorization required for all services over $300.
100% family-related groups are now eligible for coverage with a 20%rate load.
Plan administered by Allied National and underwritten by The UnitedStates Life Insurance Company of New York, a member company ofAmerican International Group, Inc.
The following Industries receive an automatic rate load:3843 Dental Equipment and Supplies5813 Drinking Places (Alcoholic Beverages)7929 Bands, Orchestras, Actors, and Other Entertainers and
Entertainment Groups8021 Offices and Clinics of Dentists8111 Legal Services8211 Elementary and Secondary Schools8299 Schools and Educational Services, NEC6531 Real Estate Agents and Managers7941 Professional Sports Clubs and Promoters8661 Religious Organizations8023 Orthodontists
No
Yes—as long as they work full-time and exclusivelyfor one employer. Must be approved by Allied priorto case submission.
No
Yes
Groups of 2-9: Yes 10+ groups: No
Two Usual & Customary options available:80th percentile of HIAA (base)90th percentile of HIAA (1.04 rate factor)
◆◆ 100%
◆◆ 100%** One employee may waive that doesn’t fit ◆◆ category.
SPECIAL CONSIDERATIONS
ORTHODONTIC COVERAGE
WAITING PERIOD WAIVER/TAKEOVER
Are Commission-Only employees allowed?
Are 1099 employees allowed?
Any ineligible industries?
Virgin groups eligible?
Wage & tax reports required?
Dependent children (under age 19) only. One time$50 deductible then 50% to $1000 lifetime max. perperson while insured. 12 month waiting period.
Option–$1500 lifetime max. per person ($500/year).Apply 1.09 factor to ortho rates only.
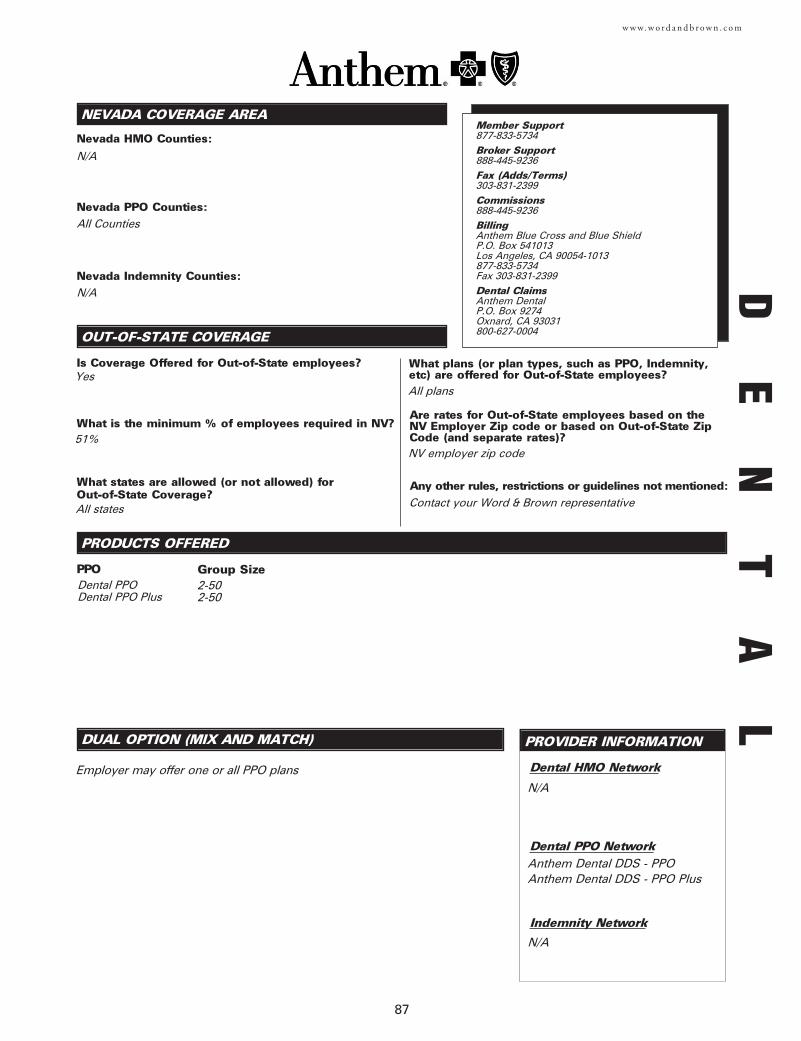
OUT-OF-STATE COVERAGE
NEVADA COVERAGE AREA
DUAL OPTION (MIX AND MATCH)
Nevada HMO Counties:
PROVIDER INFORMATION
PRODUCTS OFFERED
Nevada PPO Counties:
Nevada Indemnity Counties:
Is Coverage Offered for Out-of-State employees?
What is the minimum % of employees required in NV?
What plans (or plan types, such as PPO, Indemnity,etc) are offered for Out-of-State employees?
What states are allowed (or not allowed) for Out-of-State Coverage?
Are rates for Out-of-State employees based on theNV Employer Zip code or based on Out-of-State ZipCode (and separate rates)?
Any other rules, restrictions or guidelines not mentioned:
87
w w w. w o r d a n d b r o w n . c o m
N/A
All Counties
N/A
PPO Group SizeDental PPODental PPO Plus
2-502-50
Employer may offer one or all PPO plans Dental HMO Network
Dental PPO Network
Indemnity Network
N/A
Anthem Dental DDS - PPOAnthem Dental DDS - PPO Plus
N/A
Yes
51%
All states
All plans
NV employer zip code
Contact your Word & Brown representative
Member Support877-833-5734Broker Support888-445-9236Fax (Adds/Terms)303-831-2399Commissions888-445-9236BillingAnthem Blue Cross and Blue Shield P.O. Box 541013 Los Angeles, CA 90054-1013877-833-5734Fax 303-831-2399Dental ClaimsAnthem DentalP.O. Box 9274Oxnard, CA 93031800-627-0004
DE
NT
AL
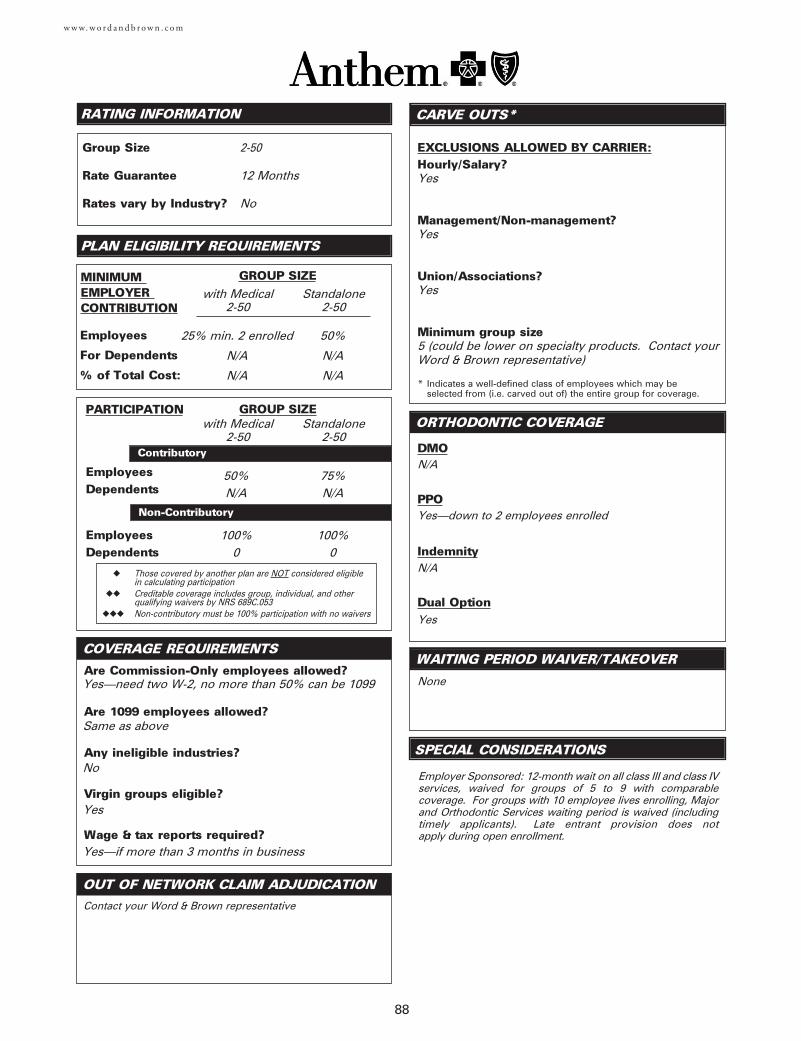
EmployeesDependents
EmployeesDependents
Employees
For Dependents
% of Total Cost:
RATING INFORMATION
MINIMUM EMPLOYER CONTRIBUTION
PARTICIPATION
Contributory
Non-Contributory
GROUP SIZE
GROUP SIZE
◆ Those covered by another plan are NOT considered eligible in calculating participation
◆◆ Creditable coverage includes group, individual, and other qualifying waivers by NRS 689C.053
◆◆◆ Non-contributory must be 100% participation with no waivers
CARVE OUTS*
SPECIAL CONSIDERATIONS
DMO
ORTHODONTIC COVERAGE
WAITING PERIOD WAIVER/TAKEOVER
PLAN ELIGIBILITY REQUIREMENTS
OUT OF NETWORK CLAIM ADJUDICATION
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
Group Size
Rate Guarantee
Rates vary by Industry?
Indemnity
Dual Option
COVERAGE REQUIREMENTS
88
w w w. w o r d a n d b r o w n . c o m
Are Commission-Only employees allowed?
Are 1099 employees allowed?
Any ineligible industries?
Virgin groups eligible?
Wage & tax reports required?
with Medical2-50
2-50
12 Months
No
25% min. 2 enrolled
N/A
N/A
Standalone2-50
50%
N/A
N/A
with Medical2-50
75%N/A
Standalone2-50
50%N/A
100%0
100%0
EXCLUSIONS ALLOWED BY CARRIER:Hourly/Salary?
Management/Non-management?
Union/Associations?
Minimum group size
Yes—need two W-2, no more than 50% can be 1099
Same as above
No
Yes
Yes—if more than 3 months in business
Contact your Word & Brown representative
Employer Sponsored: 12-month wait on all class III and class IVservices, waived for groups of 5 to 9 with comparablecoverage. For groups with 10 employee lives enrolling, Majorand Orthodontic Services waiting period is waived (includingtimely applicants). Late entrant provision does not apply during open enrollment.
N/A
Yes
Yes
Yes
5 (could be lower on specialty products. Contact yourWord & Brown representative)
PPOYes—down to 2 employees enrolled
N/A
Yes
None
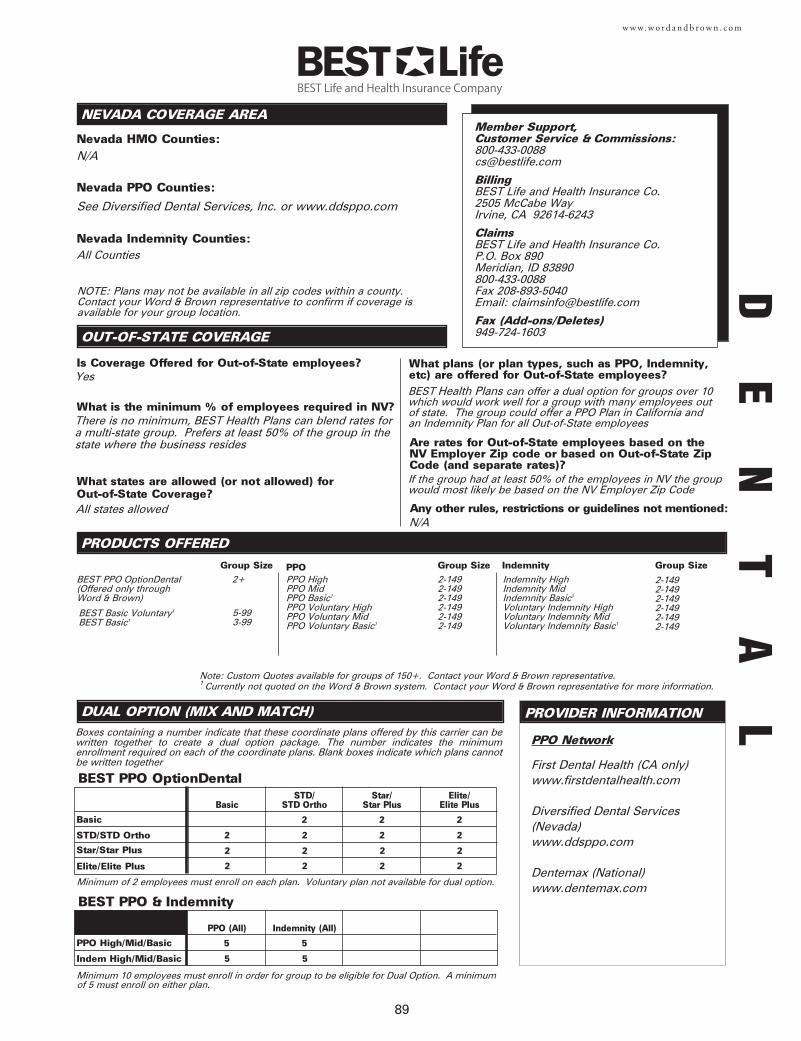
OUT-OF-STATE COVERAGE
NEVADA COVERAGE AREA
DUAL OPTION (MIX AND MATCH)
Nevada HMO Counties:
Boxes containing a number indicate that these coordinate plans offered by this carrier can bewritten together to create a dual option package. The number indicates the minimumenrollment required on each of the coordinate plans. Blank boxes indicate which plans cannotbe written together
PROVIDER INFORMATION
PRODUCTS OFFERED
Nevada PPO Counties:
Nevada Indemnity Counties:
Is Coverage Offered for Out-of-State employees?
What is the minimum % of employees required in NV?
What plans (or plan types, such as PPO, Indemnity,etc) are offered for Out-of-State employees?
What states are allowed (or not allowed) for Out-of-State Coverage?
Are rates for Out-of-State employees based on theNV Employer Zip code or based on Out-of-State ZipCode (and separate rates)?
Any other rules, restrictions or guidelines not mentioned:
89
w w w. w o r d a n d b r o w n . c o m
PPO Network
N/A
See Diversified Dental Services, Inc. or www.ddsppo.com
All Counties
BEST PPO OptionDental(Offered only through Word & Brown)
2+ PPO HighPPO MidPPO Basic1
PPO Voluntary HighPPO Voluntary MidPPO Voluntary Basic1
2-1492-1492-1492-1492-1492-149
Indemnity HighIndemnity MidIndemnity Basic1
Voluntary Indemnity HighVoluntary Indemnity MidVoluntary Indemnity Basic1
2-1492-1492-1492-1492-1492-149
First Dental Health (CA only)www.firstdentalhealth.com
Diversified Dental Services(Nevada)www.ddsppo.com
Dentemax (National)www.dentemax.com
Member Support, Customer Service & Commissions:[email protected]
BillingBEST Life and Health Insurance Co. 2505 McCabe WayIrvine, CA 92614-6243
ClaimsBEST Life and Health Insurance Co. P.O. Box 890Meridian, ID 83890800-433-0088Fax 208-893-5040Email: [email protected]
Fax (Add-ons/Deletes)949-724-1603
Basic
NOTE: Plans may not be available in all zip codes within a county.Contact your Word & Brown representative to confirm if coverage isavailable for your group location.
Group Size PPO Group Size Indemnity Group Size
Note: Custom Quotes available for groups of 150+. Contact your Word & Brown representative.1 Currently not quoted on the Word & Brown system. Contact your Word & Brown representative for more information.
BasicSTD/
STD OrthoStar/
Star PlusElite/
Elite Plus
STD/STD Ortho 2
2
Elite/Elite Plus 2
2
2
2
2
2
2
2
2
2
BEST Basic Voluntary1
BEST Basic15-993-99
Minimum of 2 employees must enroll on each plan. Voluntary plan not available for dual option.
BEST PPO OptionDental
Star/Star Plus
PPO High/Mid/Basic
PPO (All) Indemnity (All)
Indem High/Mid/Basic 5
5
Minimum 10 employees must enroll in order for group to be eligible for Dual Option. A minimumof 5 must enroll on either plan.
BEST PPO & Indemnity
5
5
2
2
2
Yes
There is no minimum, BEST Health Plans can blend rates fora multi-state group. Prefers at least 50% of the group in thestate where the business resides
All states allowed
BEST Health Plans can offer a dual option for groups over 10which would work well for a group with many employees outof state. The group could offer a PPO Plan in California andan Indemnity Plan for all Out-of-State employees
If the group had at least 50% of the employees in NV the groupwould most likely be based on the NV Employer Zip Code
N/A
DE
NT
AL
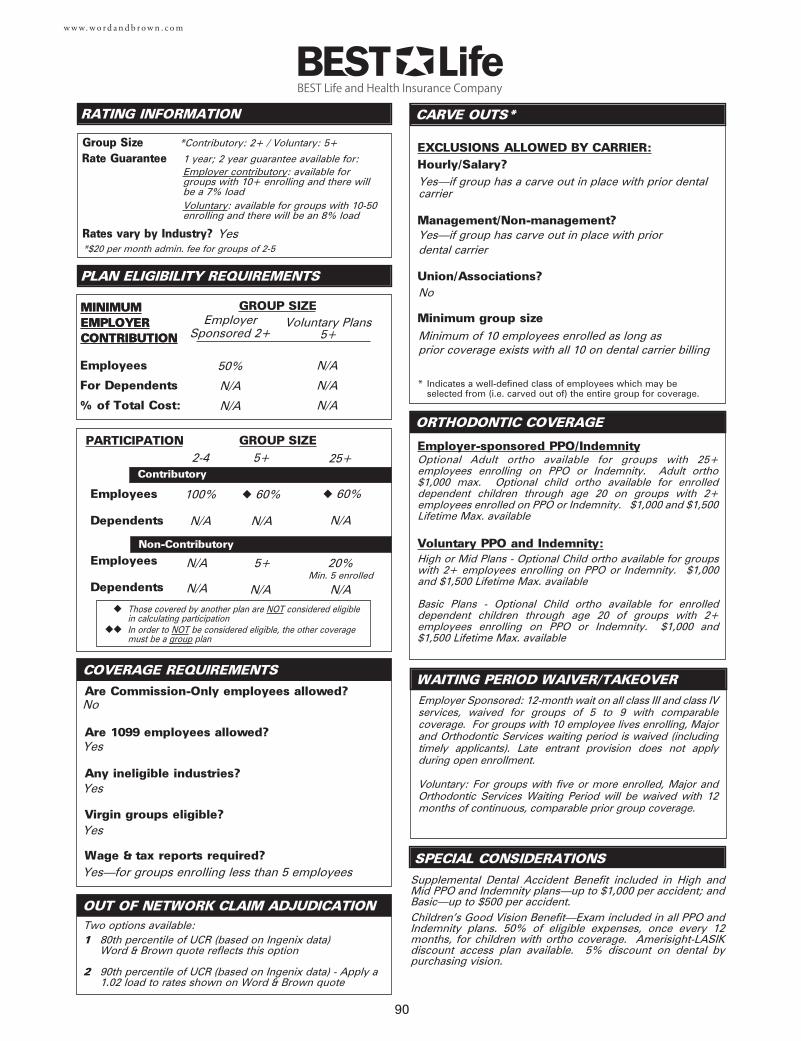
Yes—if group has a carve out in place with prior dental carrier
Yes—if group has carve out in place with prior dental carrier
No
Minimum of 10 employees enrolled as long as prior coverage exists with all 10 on dental carrier billing
w w w. w o r d a n d b r o w n . c o m
Employer-sponsored PPO/Indemnity
RATING INFORMATION
EXCLUSIONS ALLOWED BY CARRIER:Hourly/Salary?
Management/Non-management?
Union/Associations?
Minimum group size
CARVE OUTS*
ORTHODONTIC COVERAGE
WAITING PERIOD WAIVER/TAKEOVER
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
90
Are Commission-Only employees allowed?
Are 1099 employees allowed?
Any ineligible industries?
Virgin groups eligible?
Wage & tax reports required?
No
Yes
Yes
Yes
Yes—for groups enrolling less than 5 employees
Employer Sponsored: 12-month wait on all class III and class IVservices, waived for groups of 5 to 9 with comparablecoverage. For groups with 10 employee lives enrolling, Majorand Orthodontic Services waiting period is waived (includingtimely applicants). Late entrant provision does not apply during open enrollment.
Voluntary: For groups with five or more enrolled, Major andOrthodontic Services Waiting Period will be waived with 12months of continuous, comparable prior group coverage.
Optional Adult ortho available for groups with 25+employees enrolling on PPO or Indemnity. Adult ortho$1,000 max. Optional child ortho available for enrolleddependent children through age 20 on groups with 2+employees enrolled on PPO or Indemnity. $1,000 and $1,500Lifetime Max. available
SPECIAL CONSIDERATIONS
ORTHODONTIC COVERAGE
WAITING PERIOD WAIVER/TAKEOVER
Supplemental Dental Accident Benefit included in High andMid PPO and Indemnity plans—up to $1,000 per accident; andBasic—up to $500 per accident. Children’s Good Vision Benefit—Exam included in all PPO andIndemnity plans. 50% of eligible expenses, once every 12months, for children with ortho coverage. Amerisight-LASIKdiscount access plan available. 5% discount on dental bypurchasing vision.
Voluntary PPO and Indemnity:High or Mid Plans - Optional Child ortho available for groupswith 2+ employees enrolling on PPO or Indemnity. $1,000and $1,500 Lifetime Max. available
Basic Plans - Optional Child ortho available for enrolleddependent children through age 20 of groups with 2+employees enrolling on PPO or Indemnity. $1,000 and$1,500 Lifetime Max. available
Employees
Dependents
Employees
Dependents
Employees
For Dependents
% of Total Cost:
MINIMUMEMPLOYERCONTRIBUTION
PARTICIPATION
Contributory
Non-Contributory
GROUP SIZE
GROUP SIZE
◆ Those covered by another plan are NOT considered eligible in calculating participation
◆◆ In order to NOT be considered eligible, the other coveragemust be a group plan
PLAN ELIGIBILITY REQUIREMENTS
OUT OF NETWORK CLAIM ADJUDICATION
Group Size
COVERAGE REQUIREMENTS
MINIMUMEMPLOYERCONTRIBUTION
EmployerSponsored 2+
50%
N/A
N/A
*Contributory: 2+ / Voluntary: 5+
N/A
N/A
N/A
◆ 60%
N/A
◆ 60%
N/A
5+
N/A
20%
N/A
Two options available:1 80th percentile of UCR (based on Ingenix data)
Word & Brown quote reflects this option
2 90th percentile of UCR (based on Ingenix data) - Apply a1.02 load to rates shown on Word & Brown quote
5+ 25+
Voluntary Plans5+
Yes
Min. 5 enrolled
100%
N/A
2-4
*$20 per month admin. fee for groups of 2-5
N/A
N/A
Rate Guarantee
Rates vary by Industry?
1 year; 2 year guarantee available for:Employer contributory: available forgroups with 10+ enrolling and there willbe a 7% loadVoluntary: available for groups with 10-50enrolling and there will be an 8% load
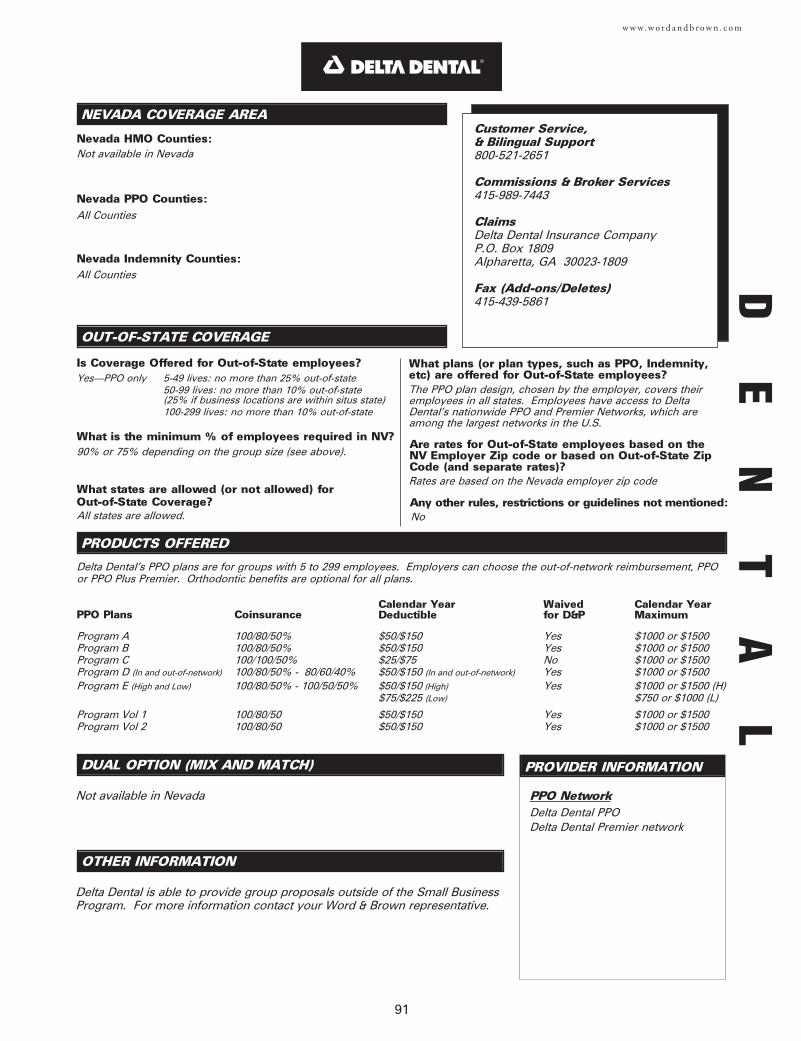
OUT-OF-STATE COVERAGE
NEVADA COVERAGE AREA
DUAL OPTION (MIX AND MATCH)
Nevada HMO Counties:
Not available in Nevada
PROVIDER INFORMATION
PRODUCTS OFFERED
Nevada PPO Counties:
Nevada Indemnity Counties:
Is Coverage Offered for Out-of-State employees?
What is the minimum % of employees required in NV?
What plans (or plan types, such as PPO, Indemnity,etc) are offered for Out-of-State employees?
What states are allowed (or not allowed) for Out-of-State Coverage?
Are rates for Out-of-State employees based on theNV Employer Zip code or based on Out-of-State ZipCode (and separate rates)?
Any other rules, restrictions or guidelines not mentioned:
PPO Network
91
w w w. w o r d a n d b r o w n . c o m
Program AProgram BProgram CProgram D (In and out-of-network)
Program E (High and Low)
Program Vol 1Program Vol 2
PPO Plans
Not available in Nevada
All Counties
All Counties
Yes—PPO only 5-49 lives: no more than 25% out-of-state50-99 lives: no more than 10% out-of-state(25% if business locations are within situs state)100-299 lives: no more than 10% out-of-state
Delta Dental PPO Delta Dental Premier network
Customer Service, & Bilingual Support800-521-2651
Commissions & Broker Services415-989-7443
ClaimsDelta Dental Insurance CompanyP.O. Box 1809Alpharetta, GA 30023-1809
Fax (Add-ons/Deletes)415-439-5861
All states are allowed.
Rates are based on the Nevada employer zip code
The PPO plan design, chosen by the employer, covers theiremployees in all states. Employees have access to DeltaDental’s nationwide PPO and Premier Networks, which areamong the largest networks in the U.S.
No
90% or 75% depending on the group size (see above).
Delta Dental’s PPO plans are for groups with 5 to 299 employees. Employers can choose the out-of-network reimbursement, PPOor PPO Plus Premier. Orthodontic benefits are optional for all plans.
100/80/50%100/80/50%100/100/50%100/80/50% - 80/60/40%100/80/50% - 100/50/50%
100/80/50 100/80/50
Coinsurance
YesYesNoYesYes
YesYes
Waived for D&P
OTHER INFORMATION
Delta Dental is able to provide group proposals outside of the Small BusinessProgram. For more information contact your Word & Brown representative.
$50/$150$50/$150$25/$75$50/$150 (In and out-of-network)
$50/$150 (High)$75/$225 (Low)
$50/$150$50/$150
Calendar Year Deductible
$1000 or $1500$1000 or $1500$1000 or $1500$1000 or $1500$1000 or $1500 (H)$750 or $1000 (L)
$1000 or $1500$1000 or $1500
Calendar Year Maximum
DE
NT
AL
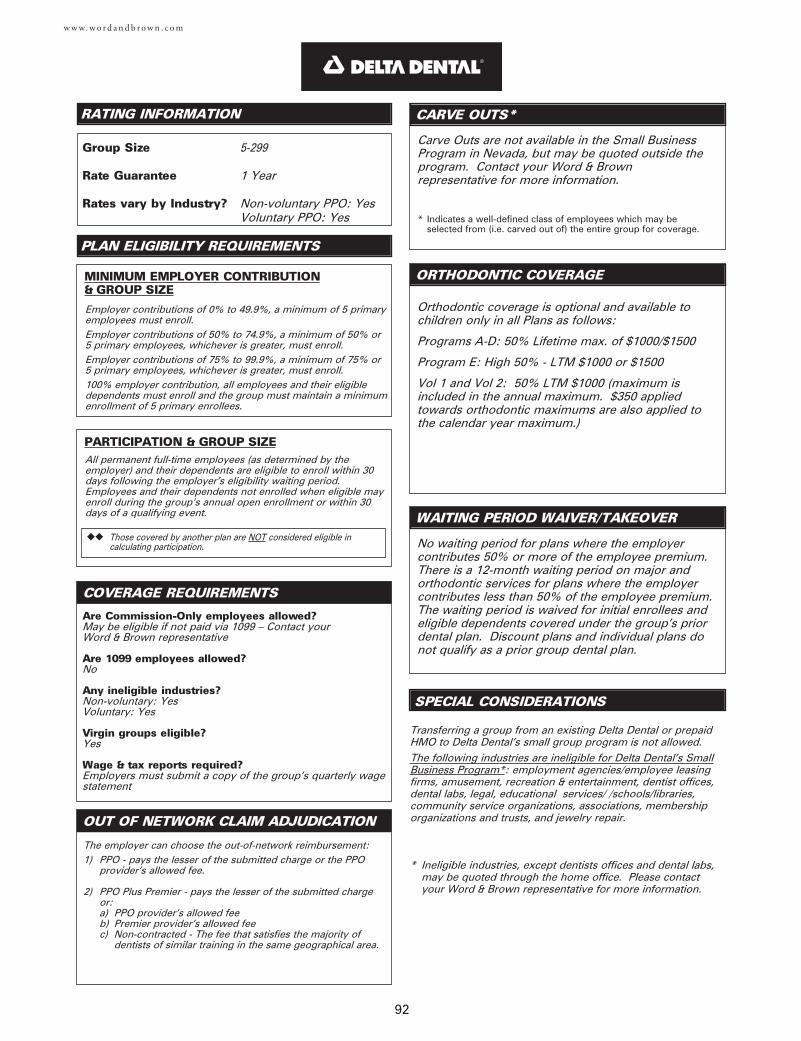
RATING INFORMATION
MINIMUM EMPLOYER CONTRIBUTION& GROUP SIZE
CARVE OUTS*
SPECIAL CONSIDERATIONS
ORTHODONTIC COVERAGE
WAITING PERIOD WAIVER/TAKEOVER
PLAN ELIGIBILITY REQUIREMENTS
OUT OF NETWORK CLAIM ADJUDICATION
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
Group Size
Rate Guarantee
Rates vary by Industry?
COVERAGE REQUIREMENTS
92
w w w. w o r d a n d b r o w n . c o m
Carve Outs are not available in the Small BusinessProgram in Nevada, but may be quoted outside theprogram. Contact your Word & Brownrepresentative for more information.
Are Commission-Only employees allowed?May be eligible if not paid via 1099 – Contact yourWord & Brown representative
Are 1099 employees allowed?No
Any ineligible industries?Non-voluntary: YesVoluntary: Yes
Virgin groups eligible?Yes
Wage & tax reports required?Employers must submit a copy of the group's quarterly wagestatement
Employer contributions of 0% to 49.9%, a minimum of 5 primaryemployees must enroll.Employer contributions of 50% to 74.9%, a minimum of 50% or5 primary employees, whichever is greater, must enroll. Employer contributions of 75% to 99.9%, a minimum of 75% or5 primary employees, whichever is greater, must enroll.100% employer contribution, all employees and their eligibledependents must enroll and the group must maintain a minimumenrollment of 5 primary enrollees.
5-299
1 Year
Non-voluntary PPO: YesVoluntary PPO: Yes
The employer can choose the out-of-network reimbursement:1) PPO - pays the lesser of the submitted charge or the PPO
provider's allowed fee.
2) PPO Plus Premier - pays the lesser of the submitted chargeor:a) PPO provider's allowed feeb) Premier provider's allowed feec) Non-contracted - The fee that satisfies the majority of
dentists of similar training in the same geographical area.
Orthodontic coverage is optional and available tochildren only in all Plans as follows:
Programs A-D: 50% Lifetime max. of $1000/$1500
Program E: High 50% - LTM $1000 or $1500
Vol 1 and Vol 2: 50% LTM $1000 (maximum isincluded in the annual maximum. $350 appliedtowards orthodontic maximums are also applied tothe calendar year maximum.)
No waiting period for plans where the employercontributes 50% or more of the employee premium.There is a 12-month waiting period on major andorthodontic services for plans where the employercontributes less than 50% of the employee premium.The waiting period is waived for initial enrollees andeligible dependents covered under the group's priordental plan. Discount plans and individual plans donot qualify as a prior group dental plan.
Transferring a group from an existing Delta Dental or prepaidHMO to Delta Dental’s small group program is not allowed.The following industries are ineligible for Delta Dental's SmallBusiness Program*: employment agencies/employee leasingfirms, amusement, recreation & entertainment, dentist offices,dental labs, legal, educational services/ /schools/libraries,community service organizations, associations, membershiporganizations and trusts, and jewelry repair.
* Ineligible industries, except dentists offices and dental labs,may be quoted through the home office. Please contactyour Word & Brown representative for more information.
◆◆ Those covered by another plan are NOT considered eligible in calculating participation.
PARTICIPATION & GROUP SIZEAll permanent full-time employees (as determined by theemployer) and their dependents are eligible to enroll within 30days following the employer’s eligibility waiting period.Employees and their dependents not enrolled when eligible mayenroll during the group’s annual open enrollment or within 30days of a qualifying event.
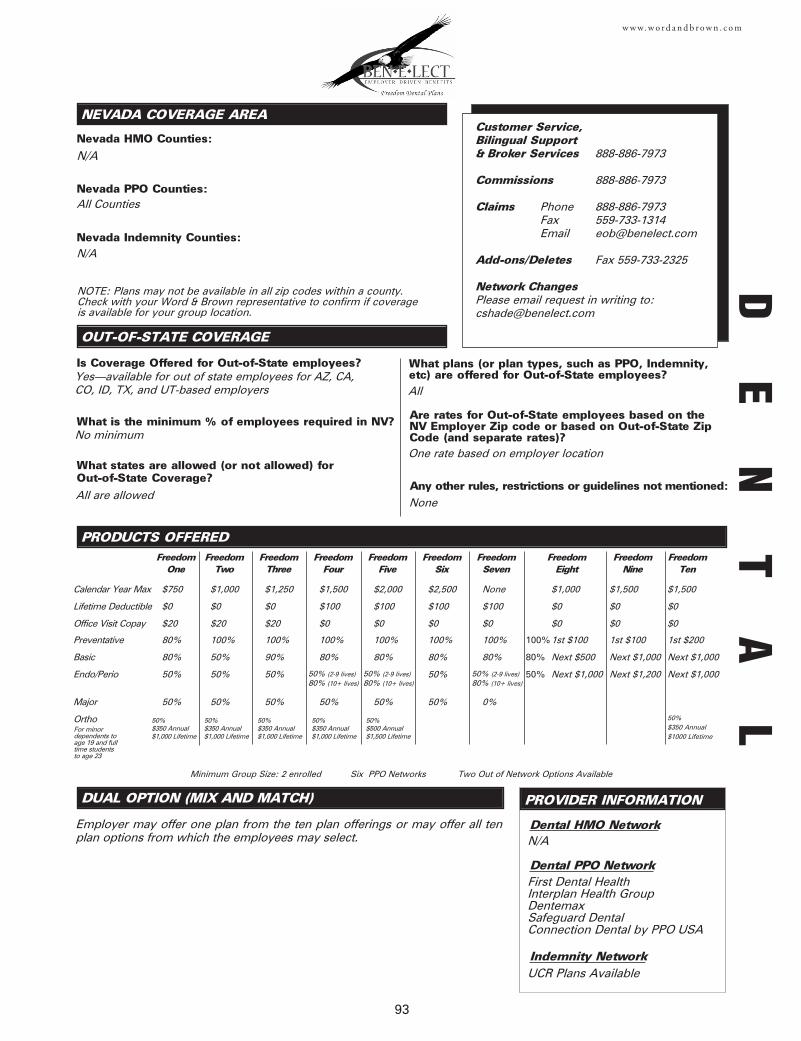
OUT-OF-STATE COVERAGE
NEVADA COVERAGE AREA
DUAL OPTION (MIX AND MATCH)
Nevada HMO Counties:
Employer may offer one plan from the ten plan offerings or may offer all tenplan options from which the employees may select.
PROVIDER INFORMATION
PRODUCTS OFFERED
Nevada PPO Counties:
Nevada Indemnity Counties:
Is Coverage Offered for Out-of-State employees?
What is the minimum % of employees required in NV?
What plans (or plan types, such as PPO, Indemnity,etc) are offered for Out-of-State employees?
What states are allowed (or not allowed) for Out-of-State Coverage?
Are rates for Out-of-State employees based on theNV Employer Zip code or based on Out-of-State ZipCode (and separate rates)?
Any other rules, restrictions or guidelines not mentioned:
93
w w w. w o r d a n d b r o w n . c o m
N/A
All Counties
NOTE: Plans may not be available in all zip codes within a county.Check with your Word & Brown representative to confirm if coverageis available for your group location.
Yes—available for out of state employees for AZ, CA,CO, ID, TX, and UT-based employers
No minimum
All are allowed
All
One rate based on employer location
None
N/A
Dental HMO Network
Dental PPO Network
Indemnity Network
N/A
First Dental HealthInterplan Health GroupDentemaxSafeguard DentalConnection Dental by PPO USA
UCR Plans Available
Calendar Year Max
Lifetime Deductible
Preventative
Basic
Endo/Perio
Major
Ortho
$750
$0
80%
80%
50%
50%
FreedomOne
$1,000
$0
100%
50%
50%
50%
FreedomTwo
$1,250
$0
100%
90%
50%
50%
FreedomThree
$1,500
$100
100%
80%
50% (2-9 lives)80% (10+ lives)
50%
FreedomFour
$2,000
$100
100%
80%
50%
FreedomFive
$2,500
$100
100%
80%
50%
50%
FreedomSix
None
$100
100%
80%
0%
FreedomSeven
$1,000
$0
1st $100
Next $500
Next $1,000
FreedomEight
$1,500
$0
1st $100
Next $1,000
Next $1,200
FreedomNine
$1,500
$0
1st $200
Next $1,000
Next $1,000
FreedomTen
50%$350 Annual$1000 Lifetime
100%
80%
50%
Office Visit Copay $20 $20 $20 $0 $0 $0 $0 $0 $0 $0
50%$350 Annual$1,000 Lifetime
For minordependents to age 19 and fulltime students to age 23
50%$350 Annual$1,000 Lifetime
50%$350 Annual$1,000 Lifetime
50%$350 Annual$1,000 Lifetime
50%$500 Annual$1,500 Lifetime
Minimum Group Size: 2 enrolled Six PPO Networks Two Out of Network Options Available
DE
NT
AL
50% (2-9 lives)80% (10+ lives)
50% (2-9 lives)80% (10+ lives)
Customer Service, Bilingual Support & Broker Services 888-886-7973
Commissions 888-886-7973
Claims Phone 888-886-7973 Fax 559-733-1314 Email [email protected]
Add-ons/Deletes Fax 559-733-2325
Network ChangesPlease email request in writing to:[email protected]
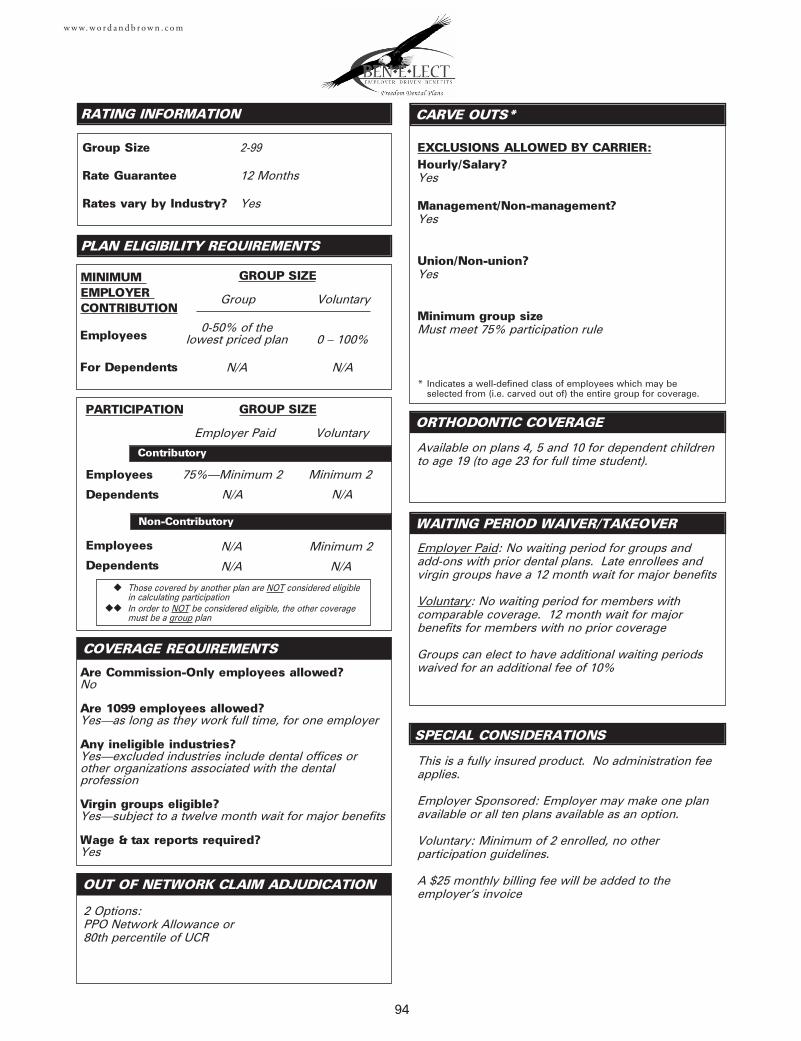
Employees
Dependents
Employees
Dependents
Employees
For Dependents
RATING INFORMATION
MINIMUM EMPLOYER CONTRIBUTION
PARTICIPATION
Contributory
Non-Contributory
GROUP SIZE
GROUP SIZE
◆ Those covered by another plan are NOT considered eligible in calculating participation
◆◆ In order to NOT be considered eligible, the other coveragemust be a group plan
EXCLUSIONS ALLOWED BY CARRIER:Hourly/Salary?Yes
Management/Non-management?Yes
Union/Non-union?Yes
Minimum group sizeMust meet 75% participation rule
CARVE OUTS*
SPECIAL CONSIDERATIONS
ORTHODONTIC COVERAGE
WAITING PERIOD WAIVER/TAKEOVER
PLAN ELIGIBILITY REQUIREMENTS
OUT OF NETWORK CLAIM ADJUDICATION
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
Group Size
Rate Guarantee
Rates vary by Industry?
COVERAGE REQUIREMENTS
94
w w w. w o r d a n d b r o w n . c o m
Are Commission-Only employees allowed?No
Are 1099 employees allowed?Yes—as long as they work full time, for one employer
Any ineligible industries?Yes—excluded industries include dental offices orother organizations associated with the dentalprofession
Virgin groups eligible?Yes—subject to a twelve month wait for major benefits
Wage & tax reports required?Yes
Employer Paid
Group
0-50% of the lowest priced plan
N/A
2-99
12 Months
Yes
Voluntary
Minimum 2
N/A
N/A
N/A
Minimum 2
N/A
2 Options:PPO Network Allowance or80th percentile of UCR
75%—Minimum 2
N/A
Voluntary
0 – 100%
N/A
Available on plans 4, 5 and 10 for dependent childrento age 19 (to age 23 for full time student).
Employer Paid: No waiting period for groups and add-ons with prior dental plans. Late enrollees andvirgin groups have a 12 month wait for major benefits
Voluntary: No waiting period for members withcomparable coverage. 12 month wait for majorbenefits for members with no prior coverage
Groups can elect to have additional waiting periodswaived for an additional fee of 10%
This is a fully insured product. No administration feeapplies.
Employer Sponsored: Employer may make one planavailable or all ten plans available as an option.
Voluntary: Minimum of 2 enrolled, no otherparticipation guidelines.
A $25 monthly billing fee will be added to theemployer’s invoice
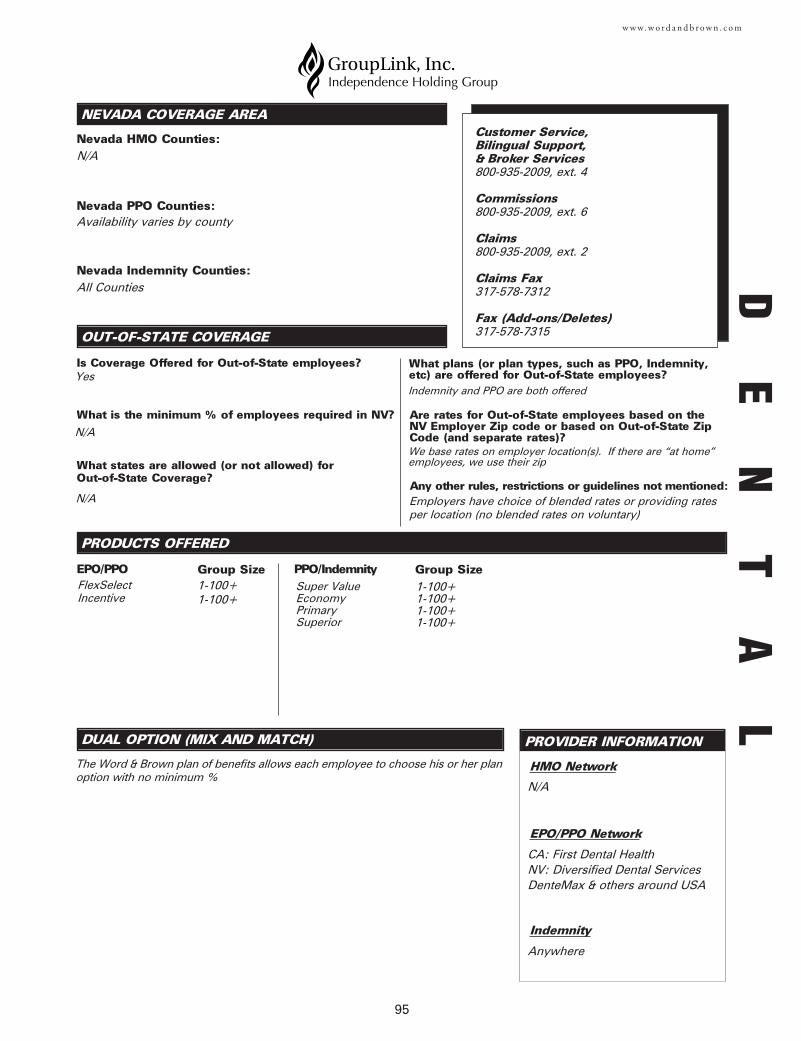
OUT-OF-STATE COVERAGE
NEVADA COVERAGE AREA
DUAL OPTION (MIX AND MATCH)
The Word & Brown plan of benefits allows each employee to choose his or her planoption with no minimum %
PROVIDER INFORMATION
PRODUCTS OFFERED
Is Coverage Offered for Out-of-State employees?
What is the minimum % of employees required in NV?
What plans (or plan types, such as PPO, Indemnity,etc) are offered for Out-of-State employees?
What states are allowed (or not allowed) for Out-of-State Coverage?
Are rates for Out-of-State employees based on theNV Employer Zip code or based on Out-of-State ZipCode (and separate rates)?
Any other rules, restrictions or guidelines not mentioned:
95
w w w. w o r d a n d b r o w n . c o m
N/A
Availability varies by county
All Counties
PPO/Indemnity
Incentive
N/A
Yes
N/A
N/A
Indemnity and PPO are both offered
We base rates on employer location(s). If there are “at home”employees, we use their zip
Employers have choice of blended rates or providing rates per location (no blended rates on voluntary)
CA: First Dental HealthNV: Diversified Dental ServicesDenteMax & others around USA
Anywhere
Group Size
Nevada HMO Counties:
Nevada PPO Counties:
Nevada Indemnity Counties:
HMO Network
EPO/PPO Network
Indemnity
Super ValueEconomyPrimarySuperior
1-100+1-100+1-100+1-100+
EPO/PPO Group SizeFlexSelect 1-100+
1-100+
Customer Service, Bilingual Support,& Broker Services800-935-2009, ext. 4
Commissions 800-935-2009, ext. 6
Claims800-935-2009, ext. 2
Claims Fax317-578-7312
Fax (Add-ons/Deletes)317-578-7315
DE
NT
AL
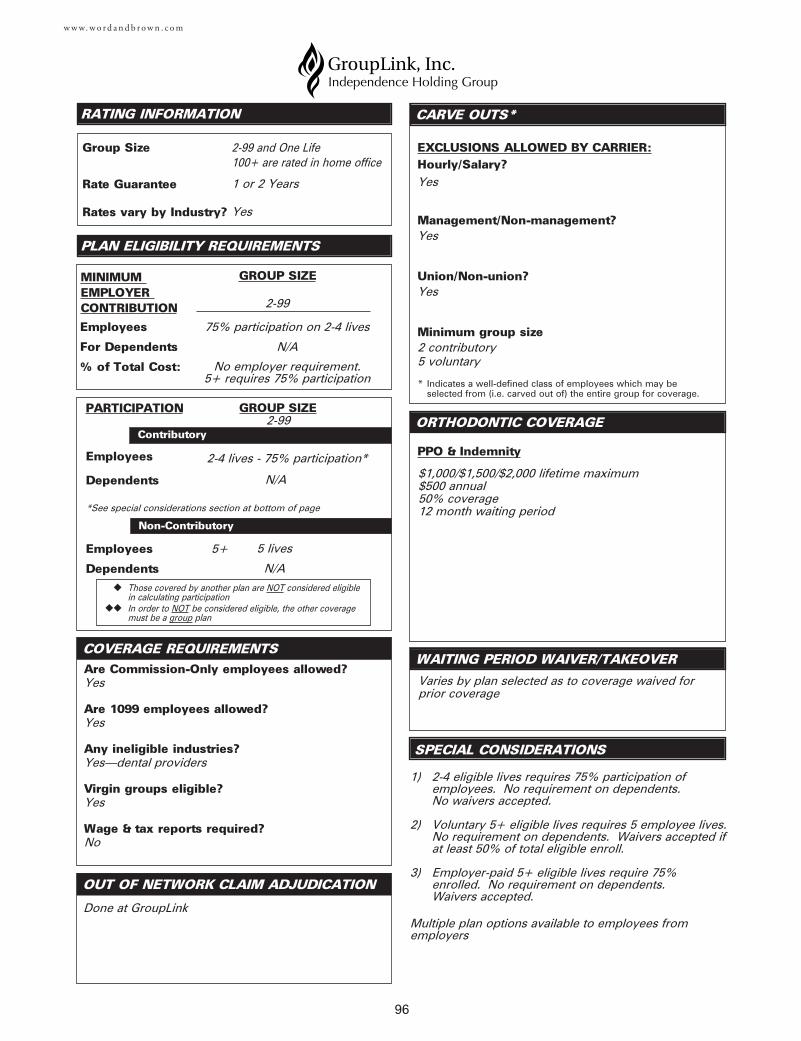
Employees
Dependents
Employees
Dependents
Are Commission-Only employees allowed?
Are 1099 employees allowed?
Any ineligible industries?
Virgin groups eligible?
Wage & tax reports required?
Employees
For Dependents
% of Total Cost:
RATING INFORMATION
PARTICIPATION
Contributory
Non-Contributory
GROUP SIZE
◆ Those covered by another plan are NOT considered eligible in calculating participation
◆◆ In order to NOT be considered eligible, the other coveragemust be a group plan
EXCLUSIONS ALLOWED BY CARRIER:Hourly/Salary?
Management/Non-management?
Union/Non-union?
Minimum group size
CARVE OUTS*
SPECIAL CONSIDERATIONS
ORTHODONTIC COVERAGE
WAITING PERIOD WAIVER/TAKEOVER
PLAN ELIGIBILITY REQUIREMENTS
OUT OF NETWORK CLAIM ADJUDICATION
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
Group Size
Rate Guarantee
Rates vary by Industry?
PPO & Indemnity
COVERAGE REQUIREMENTS
96
w w w. w o r d a n d b r o w n . c o m
$1,000/$1,500/$2,000 lifetime maximum$500 annual50% coverage12 month waiting period
Yes
Yes
Yes
2 contributory5 voluntary
2-99
75% participation on 2-4 lives
N/A
No employer requirement. 5+ requires 75% participation
2-99 and One Life100+ are rated in home office
1 or 2 Years
Yes
1) 2-4 eligible lives requires 75% participation ofemployees. No requirement on dependents. No waivers accepted.
2) Voluntary 5+ eligible lives requires 5 employee lives.No requirement on dependents. Waivers accepted ifat least 50% of total eligible enroll.
3) Employer-paid 5+ eligible lives require 75%enrolled. No requirement on dependents. Waivers accepted.
Multiple plan options available to employees fromemployers
Done at GroupLink
2-4 lives - 75% participation*
N/A
5 lives
N/A
Varies by plan selected as to coverage waived forprior coverage
*See special considerations section at bottom of page
Yes
Yes
Yes—dental providers
Yes
No
MINIMUM EMPLOYER CONTRIBUTION
2-99GROUP SIZE
5+
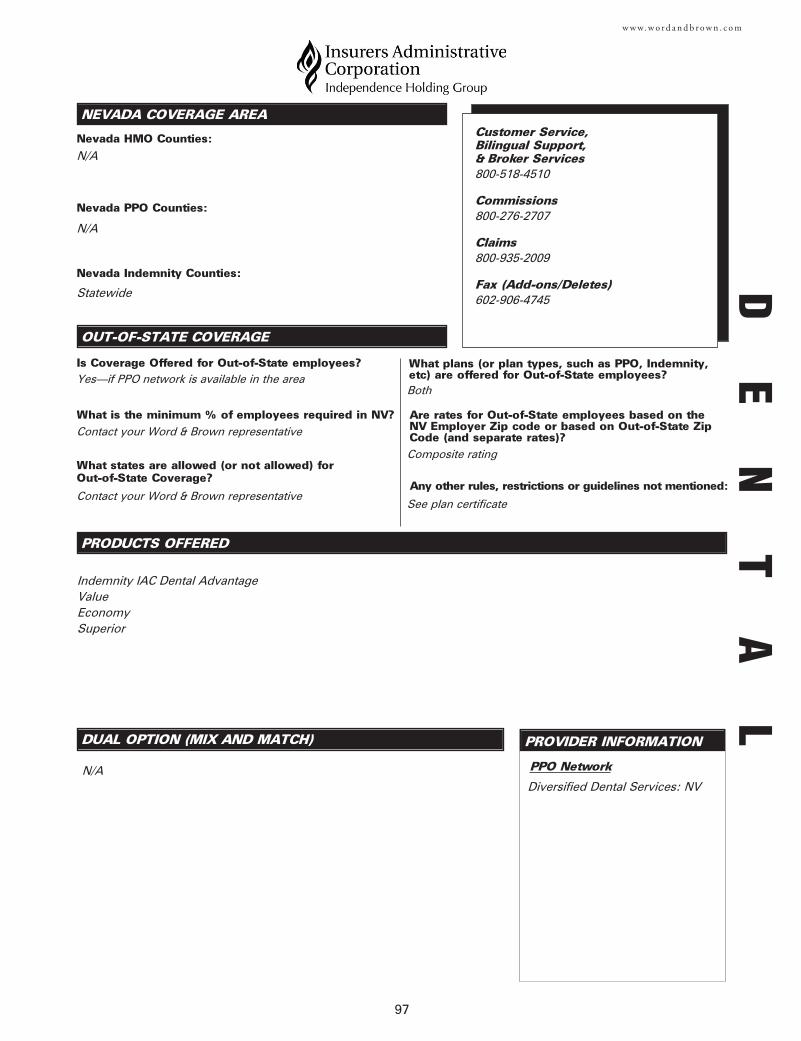
OUT-OF-STATE COVERAGE
NEVADA COVERAGE AREA
DUAL OPTION (MIX AND MATCH)
Nevada HMO Counties:
PROVIDER INFORMATION
PRODUCTS OFFERED
Nevada PPO Counties:
Nevada Indemnity Counties:
Is Coverage Offered for Out-of-State employees?
What is the minimum % of employees required in NV?
What plans (or plan types, such as PPO, Indemnity,etc) are offered for Out-of-State employees?
What states are allowed (or not allowed) for Out-of-State Coverage?
Are rates for Out-of-State employees based on theNV Employer Zip code or based on Out-of-State ZipCode (and separate rates)?
Any other rules, restrictions or guidelines not mentioned:
PPO Network
97
w w w. w o r d a n d b r o w n . c o m
Customer Service, Bilingual Support,& Broker Services800-518-4510
Commissions 800-276-2707
Claims800-935-2009
Fax (Add-ons/Deletes)602-906-4745
N/A
N/A
Statewide
Indemnity IAC Dental AdvantageValueEconomySuperior
Diversified Dental Services: NVN/A
Yes—if PPO network is available in the area
Contact your Word & Brown representative
Contact your Word & Brown representative
Both
Composite rating
See plan certificate
DE
NT
AL
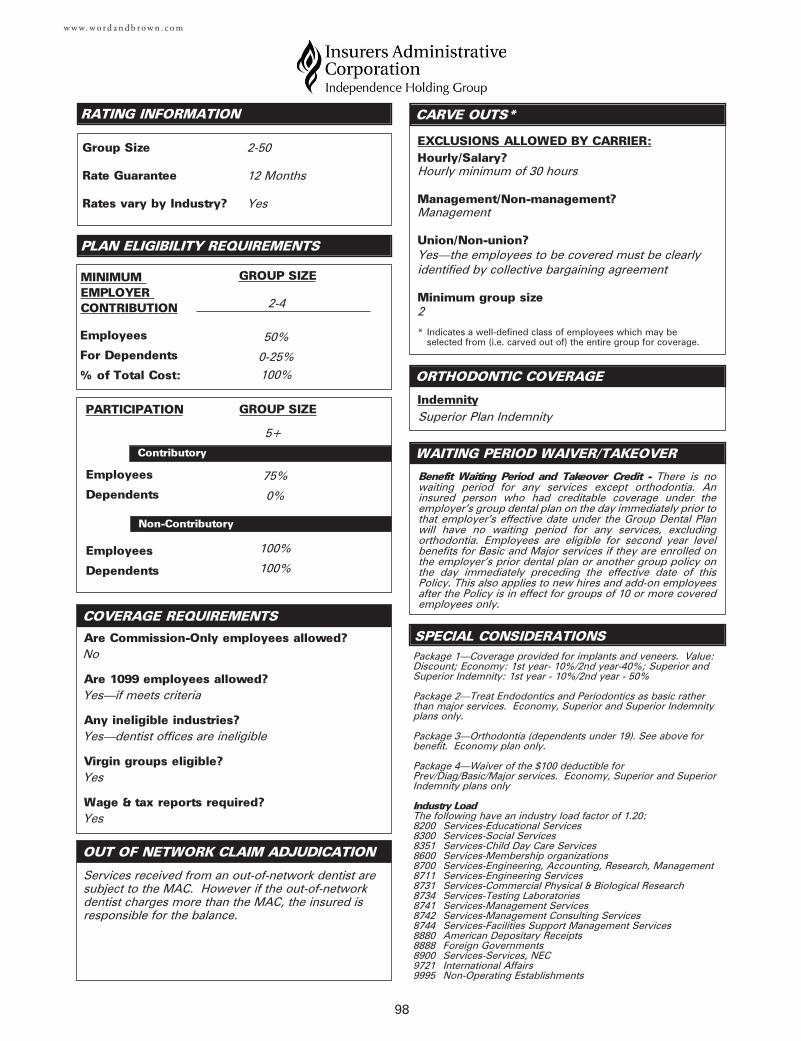
Employees
Dependents
Employees
Dependents
Employees
For Dependents
% of Total Cost:
RATING INFORMATION
MINIMUM EMPLOYER CONTRIBUTION
PARTICIPATION
Contributory
Non-Contributory
GROUP SIZE
GROUP SIZE
EXCLUSIONS ALLOWED BY CARRIER:Hourly/Salary?Hourly minimum of 30 hours
Management/Non-management?Management
Union/Non-union?Yes—the employees to be covered must be clearlyidentified by collective bargaining agreement
Minimum group size2
CARVE OUTS*
SPECIAL CONSIDERATIONS
ORTHODONTIC COVERAGE
WAITING PERIOD WAIVER/TAKEOVER
PLAN ELIGIBILITY REQUIREMENTS
OUT OF NETWORK CLAIM ADJUDICATION
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
Group Size
Rate Guarantee
Rates vary by Industry?
Indemnity
COVERAGE REQUIREMENTS
98
w w w. w o r d a n d b r o w n . c o m
Are Commission-Only employees allowed?
Are 1099 employees allowed?
Any ineligible industries?
Virgin groups eligible?
Wage & tax reports required?
Superior Plan Indemnity
2-4
100%
2-50
12 Months
Yes
No
Yes—if meets criteria
Yes—dentist offices are ineligible
Yes
Yes
Services received from an out-of-network dentist aresubject to the MAC. However if the out-of-networkdentist charges more than the MAC, the insured isresponsible for the balance.
75%
0%
Benefit Waiting Period and Takeover Credit - There is nowaiting period for any services except orthodontia. Aninsured person who had creditable coverage under theemployer’s group dental plan on the day immediately prior tothat employer’s effective date under the Group Dental Planwill have no waiting period for any services, excludingorthodontia. Employees are eligible for second year levelbenefits for Basic and Major services if they are enrolled onthe employer’s prior dental plan or another group policy onthe day immediately preceding the effective date of thisPolicy. This also applies to new hires and add-on employeesafter the Policy is in effect for groups of 10 or more coveredemployees only.
5+
50%
0-25%
100%
100%
Package 1—Coverage provided for implants and veneers. Value:Discount; Economy: 1st year- 10%/2nd year-40%; Superior andSuperior Indemnity: 1st year - 10%/2nd year - 50%
Package 2—Treat Endodontics and Periodontics as basic ratherthan major services. Economy, Superior and Superior Indemnityplans only.
Package 3—Orthodontia (dependents under 19). See above forbenefit. Economy plan only.
Package 4—Waiver of the $100 deductible forPrev/Diag/Basic/Major services. Economy, Superior and SuperiorIndemnity plans only
Industry LoadThe following have an industry load factor of 1.20:8200 Services-Educational Services8300 Services-Social Services8351 Services-Child Day Care Services8600 Services-Membership organizations8700 Services-Engineering, Accounting, Research, Management8711 Services-Engineering Services8731 Services-Commercial Physical & Biological Research8734 Services-Testing Laboratories8741 Services-Management Services8742 Services-Management Consulting Services8744 Services-Facilities Support Management Services8880 American Depositary Receipts8888 Foreign Governments8900 Services-Services, NEC9721 International Affairs9995 Non-Operating Establishments
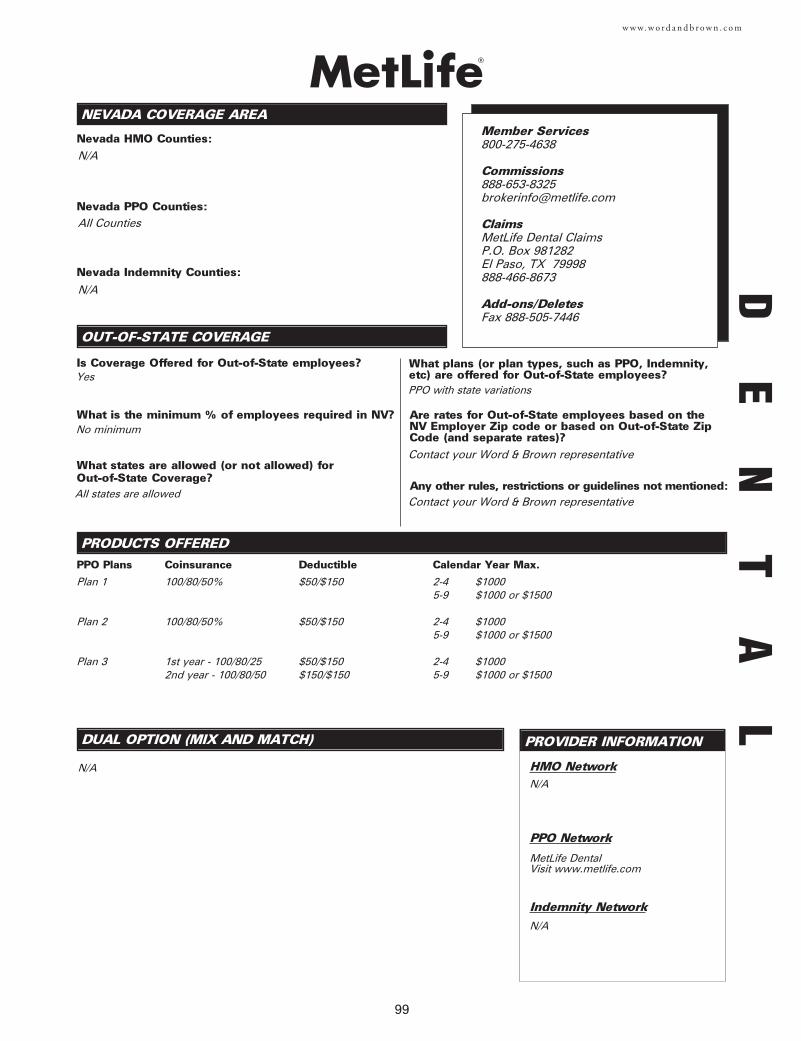
OUT-OF-STATE COVERAGE
NEVADA COVERAGE AREA
DUAL OPTION (MIX AND MATCH)
Nevada HMO Counties:
PROVIDER INFORMATION
PRODUCTS OFFERED
Nevada PPO Counties:
Nevada Indemnity Counties:
Is Coverage Offered for Out-of-State employees?
What is the minimum % of employees required in NV?
What plans (or plan types, such as PPO, Indemnity,etc) are offered for Out-of-State employees?
What states are allowed (or not allowed) for Out-of-State Coverage?
Are rates for Out-of-State employees based on theNV Employer Zip code or based on Out-of-State ZipCode (and separate rates)?
Any other rules, restrictions or guidelines not mentioned:
HMO Network
PPO Network
Indemnity Network
99
w w w. w o r d a n d b r o w n . c o m
DE
NT
AL
Plan 1
Plan 2
Plan 3
N/A
No minimum
PPO Plans
100/80/50%
100/80/50%
1st year - 100/80/252nd year - 100/80/50
Coinsurance
$50/$150
$50/$150
$50/$150$150/$150
Deductible
2-4 $10005-9 $1000 or $1500
2-4 $10005-9 $1000 or $1500
2-4 $10005-9 $1000 or $1500
Calendar Year Max.
Member Services800-275-4638
ClaimsMetLife Dental ClaimsP.O. Box 981282El Paso, TX 79998888-466-8673
Add-ons/DeletesFax 888-505-7446
Yes
All states are allowed
PPO with state variations
Contact your Word & Brown representative
Contact your Word & Brown representative
All Counties
N/A
N/A
N/A
N/A
MetLife DentalVisit www.metlife.com
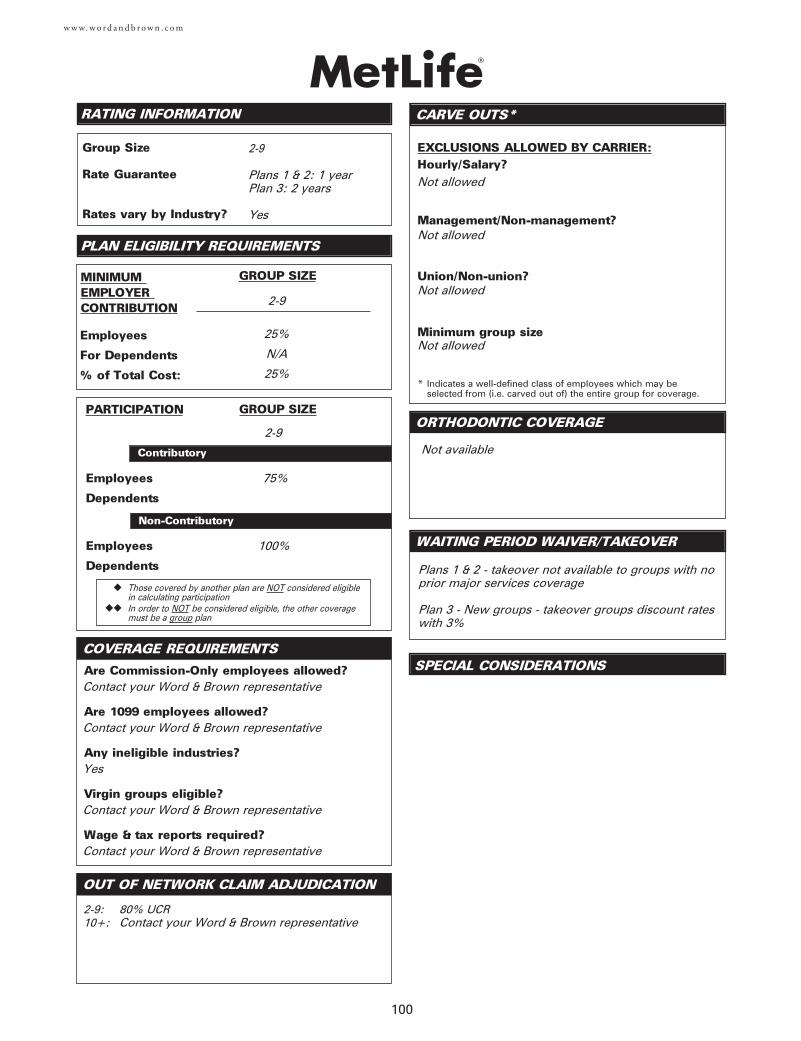
Employees
Dependents
Employees
For Dependents
% of Total Cost:
RATING INFORMATION
MINIMUM EMPLOYER CONTRIBUTION
PARTICIPATION
Contributory
Non-Contributory
GROUP SIZE
GROUP SIZE
◆ Those covered by another plan are NOT considered eligible in calculating participation
◆◆ In order to NOT be considered eligible, the other coveragemust be a group plan
EXCLUSIONS ALLOWED BY CARRIER:Hourly/Salary?
Management/Non-management?
Union/Non-union?
Minimum group size
CARVE OUTS*
SPECIAL CONSIDERATIONS
ORTHODONTIC COVERAGE
WAITING PERIOD WAIVER/TAKEOVER
PLAN ELIGIBILITY REQUIREMENTS
OUT OF NETWORK CLAIM ADJUDICATION
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
Group Size
Rate Guarantee
Rates vary by Industry?
COVERAGE REQUIREMENTS
100
w w w. w o r d a n d b r o w n . c o m
Are Commission-Only employees allowed?
Are 1099 employees allowed?
Any ineligible industries?
Virgin groups eligible?
Wage & tax reports required?
Not available
Not allowed
Not allowed
Not allowed
Not allowed
2-9
2-9
Plans 1 & 2: 1 yearPlan 3: 2 years
Yes
Contact your Word & Brown representative
Contact your Word & Brown representative
Yes
Contact your Word & Brown representative
Contact your Word & Brown representative
2-9: 80% UCR10+: Contact your Word & Brown representative
Plans 1 & 2 - takeover not available to groups with noprior major services coverage
Plan 3 - New groups - takeover groups discount rateswith 3%
2-9
25%
N/A
25%
Employees
Dependents
75%
100%
101
OUT-OF-STATE COVERAGE
NEVADA COVERAGE AREA
DUAL OPTION (MIX AND MATCH)
Nevada PPO Counties:
PROVIDER INFORMATION
PRODUCTS OFFERED
Nevada Indemnity Counties:
PPO Network
Indemnity Network
w w w. w o r d a n d b r o w n . c o m
Contact your Word & Brown representative
All counties
N/A
Diversified Dental Services-Las Vegas
Diversified Dental Services-Reno
The Principal Plan Dental
N/A
Customer & Broker Services949-553-1616
Adds/TermsFax 949-553-1898
Commissions800-388-4793
BOR ChangesFax 515-235-5538
Claims800-247-4695
Is Coverage Offered for Out-of-State employees?
What is the minimum % of employees required in NV?
What plans (or plan types, such as PPO, Indemnity,etc) are offered for Out-of-State employees?
What states are allowed (or not allowed) for Out-of-State Coverage?
Are rates for Out-of-State employees based on theNV Employer Zip code or based on Out-of-State ZipCode (and separate rates)?
Any other rules, restrictions or guidelines not mentioned:
Yes—contact your Word & Brown representative
Contact your Word & Brown representative
All states available through Request-a-Quote. Contact your Word & Brown representative
PPO & Indemnity—contact your Word & Brown representative
Contact your Word & Brown representative
Contact your Word & Brown representative
DE
NT
AL
Principal Dental Series II (PDS II)Group SizePPO
3-150
w w w. w o r d a n d b r o w n . c o m
50th percentile60th percentile70th percentile75th percentile80th percentile
85th percentile 90th percentile95th percentile99th percentile
OUT OF NETWORK CLAIM ADJUDICATION
Employees
Dependents
Employees
For Dependents
% of Total Cost:
RATING INFORMATION
MINIMUM EMPLOYER CONTRIBUTION
GROUP SIZE
EXCLUSIONS ALLOWED BY CARRIER:Hourly/Salary?
Management/Non-management?
Union/Non-union?
Minimum group size
CARVE OUTS*
SPECIAL CONSIDERATIONS
ORTHODONTIC COVERAGE
WAITING PERIOD WAIVER/TAKEOVER
PLAN ELIGIBILITY REQUIREMENTS
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
COVERAGE REQUIREMENTS
102
Are Commission-Only employees allowed?
Are 1099 employees allowed?
Any ineligible industries?
Virgin groups eligible?
Wage & tax reports required?
COVERAGE REQUIREMENTS
Yes
Yes
Yes
10 enrolled lives
Yes
No
Yes
Yes
No
Dental - 10 enrolled lives for child ortho, 25 lives foradult or adult/child ortho
Voluntary Dental – Contact your Word & Brown representative
Benefit Waiting Period will not apply to Preventativeservices. You may elect a benefit waiting period forBasic services, Major services and Additional BenefitRiders.
25%
N/A
GROUP SIZE
Employees
For Dependents
% of Total Cost:
MINIMUM EMPLOYER CONTRIBUTION
Contributory
Voluntary
GROUP SIZEPARTICIPATION
75%
50%
Employees
Dependents
100%
0%
N/A
Non-contributory
50–99%
0%
N/A
Contributory
0-49%
0%
N/A
Voluntary
Employees
Dependents
100%
50%
Non-Contributory
Group Size
Rate Guarantee
Rates vary by Industry?
3-150 employer paid 10-150 voluntary
Voluntary w/o prior<20 lives: 1 year>20 lives: 1 or 2 year
Dental or Vol w/prior<10 lives: 1 year>10 lives: 1 or 2 year
Yes
3-150 employer paid10-150 voluntary
3-150 employer paid10-150 voluntary
1. For Retiree coverage, please contact your Word & Brown representative.
2. Annual enrollment period options are available.
3. Domestic Partner coverage is available.
4. Additional Benefit Riders are available.
5. For groups over 150 lives, please contact your Word & Brown representative.
6. 3 & 4 life groups must quote 2 or more coverages.
7 Voluntary coverage is not available for groups under 10 lives.
OUT-OF-STATE COVERAGE
NEVADA COVERAGE AREA
DUAL OPTION (MIX AND MATCH)
Nevada HMO Counties:
PROVIDER INFORMATION
PRODUCTS OFFERED
Nevada PPO Counties:
Nevada Indemnity Counties:
Is Coverage Offered for Out-of-State employees?
What is the minimum % of employees required in NV?
What plans (or plan types, such as PPO, Indemnity,etc) are offered for Out-of-State employees?
What states are allowed (or not allowed) for Out-of-State Coverage?
Are rates for Out-of-State employees based on theNV Employer Zip code or based on Out-of-State ZipCode (and separate rates)?
Any other rules, restrictions or guidelines not mentioned:
HMO Network
PPO Network
103
w w w. w o r d a n d b r o w n . c o m
Member Support,Customer Service, Commissions800-659-2223, ext. 0-82149
ClaimsP.O. Box 82510Lincoln, NE 68501800-497-7044
Fax (Add-ons/Deletes)402-309-2583
N/A
N/A
All Counties
Indemnity3-19*
N/A
Yes
No minimum
All states allowed
Indemnity with nationwide passive PPO
Rates are based on the firm’s home office (i.e. wherebilled)
No
Ameritas PPO
Group Size
N/A
Plan A: 100/80/50$1000 max., $50 deductible (3 per family)Vision Care option available
Plan B: 100/80-90/100 step-up in Basic/50$1500 max., $50 deductible (3 per family)Ortho benefit (all insureds)Vision Care option available * Large Group available upon request
DE
NT
AL
Employees
Dependents
Employees
Dependents
Employees
For Dependents
% of Total Cost:
RATING INFORMATION
MINIMUM EMPLOYER CONTRIBUTION
PARTICIPATION
Contributory
Non-Contributory
GROUP SIZE
GROUP SIZE
◆ Those covered by another plan are NOT considered eligible in calculating participation
◆◆ In order to NOT be considered eligible, the other coveragemust be a group plan
EXCLUSIONS ALLOWED BY CARRIER:Hourly/Salary?
Management/Non-management?
Union/Non-union?
Minimum group size
CARVE OUTS*
SPECIAL CONSIDERATIONS
ORTHODONTIC COVERAGE
WAITING PERIOD WAIVER/TAKEOVER
PLAN ELIGIBILITY REQUIREMENTS
OUT OF NETWORK CLAIM ADJUDICATION
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
Group Size
Rate Guarantee
Rates vary by Industry?
COVERAGE REQUIREMENTS
104
w w w. w o r d a n d b r o w n . c o m
Are Commission-Only employees allowed?
Are 1099 employees allowed?
Any ineligible industries?
Virgin groups eligible?
Wage & tax reports required?
All insureds eligible. 50% to $1000 lifetime benefitwith a 24 month elimination period.
Yes
Yes
Yes
Down to 3 insured employees
3-19
25% of the total
cost
3-19
2 Years
No, some loaded industries considered higher risk
Yes
Yes
Yes
Yes
No
Indemnity:Insureds can choose any dentist with 90% of dentists in-network. Reimbursement outside of network is 80% ofUCR. Maximum Allowable Charge (MAC) option available for plans A and B and pays out-of-network dentist basedon Reliance Standard negotiated fee.
Groups of 3-5 eligible employees: 100%Groups of 6-9 eligible employees: all but one
Groups of 10-19 eligible employees: 75%
100% of eligible employees
12 month Basic Services elimination period waivedand credit given for calendar year deductibles paidfor groups that had a similar coverage in force for atleast 18 months prior to effective date. A rate factorof 10% is applied to takeover groups.
3-19
OUT-OF-STATE COVERAGE
NEVADA COVERAGE AREA
DUAL OPTION (MIX AND MATCH)
Nevada HMO Counties:
PROVIDER INFORMATION
Customer Service, Bilingual Support,& Broker Services 800-863-7515
Commissions 888-840-9080
Add-ons/Deletes Fax 775-770-9479
ClaimsSaint Mary’s Health PlansClaims/Member Services1510 Meadow Wood LaneReno, NV 89502
PRODUCTS OFFERED
Nevada PPO Counties:
Is Coverage Offered for Out-of-State employees?
What is the minimum % of employees required in NV?
What plans (or plan types, such as PPO, Indemnity,etc) are offered for Out-of-State employees?
What states are allowed (or not allowed) for Out-of-State Coverage?
Are rates for Out-of-State employees based on theNV Employer Zip code or based on Out-of-State ZipCode (and separate rates)?
Any other rules, restrictions or guidelines not mentioned:
HMO Network
PPO Network
Indemnity Network
105
w w w. w o r d a n d b r o w n . c o m
DE
NT
AL
Dental Rider Plan 1Dental Rider Plan 2Dental Rider Plan 3
Group SizePPO
2+2+2+
N/A
Diversified Dental Serviceswww.ddsppo.com
N/A
Must be sold with medical HMO
Must be sold with medical PPO
Nevada Indemnity Counties:N/A
Yes
75%
N/A
Yes
Out-of-State Zip code
N/A
N/A
Employees
Dependents
Employees
Dependents
Employees
For Dependents
% of Total Cost:
RATING INFORMATION
MINIMUM EMPLOYER CONTRIBUTION
PARTICIPATION
Contributory
Non-Contributory
GROUP SIZE
GROUP SIZE
◆ Those covered by another plan are NOT considered eligible in calculating participation
◆◆ In order to NOT be considered eligible, the other coveragemust be a group plan
EXCLUSIONS ALLOWED BY CARRIER:Hourly/Salary?
Management/Non-management?
Union/Non-union?
Minimum group size
CARVE OUTS*
SPECIAL CONSIDERATIONS
DMO
ORTHODONTIC COVERAGE
WAITING PERIOD WAIVER/TAKEOVER
PLAN ELIGIBILITY REQUIREMENTS
OUT OF NETWORK CLAIM ADJUDICATION
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
Group Size
Rate Guarantee
Rates vary by Industry?
DPO
Indemnity
Dual Option
COVERAGE REQUIREMENTS
106
w w w. w o r d a n d b r o w n . c o m
Are Commission-Only employees allowed?
Are 1099 employees allowed?
Any ineligible industries?
Virgin groups eligible?
Wage & tax reports required?
None
None
None
None
2
12 months
No
No
Yes
No
Yes
Yes
90th percentile
12 months on all major restorative and orthodonticsunless 12 months of continuous coverage
None
N/A
N/A
N/A
2-50
100%
N/A
100%
N/A
Yes
Yes
Yes
Yes
OUT-OF-STATE COVERAGE
NEVADA COVERAGE AREA
DUAL OPTION (MIX AND MATCH)
Nevada HMO Counties:
PROVIDER INFORMATION
PRODUCTS OFFERED
Nevada PPO Counties:
Nevada Indemnity Counties:
Is Coverage Offered for Out-of-State employees?
What is the minimum % of employees required in NV?
What plans (or plan types, such as PPO, Indemnity,etc) are offered for Out-of-State employees?
What states are allowed (or not allowed) for Out-of-State Coverage?
Are rates for Out-of-State employees based on theNV Employer Zip code or based on Out-of-State ZipCode (and separate rates)?
Any other rules, restrictions or guidelines not mentioned:
HMO Network
PPO Network
Indemnity Network
107
w w w. w o r d a n d b r o w n . c o m
N/A
Las Vegas and Henderson
Las Vegas and Henderson
The Copay Plan- Scheduled PPO (MAC)- No annual maximums- No network waiting periods- No deductibles (employer sponsored)
The PPO Plan- Annual maximums ($1,000, $1,500, $2,000)- UCR out of network reimbursement
The Indemnity Plan- Annual maximums ($1,000, $1,500, $2,000)- See any dentist- UCR out of network reimbursement
Custom plans for large groups available through Word & Brown
N/A
Yes—for all plans including The Copay Plan. Employeesout-of-state enroll on the same Copay Plan as employeesin Nevada and pay the same copays.
51%
All states allowed
The Copay Plan, The PPO Plan, The Indemnity Plan;National PPO Network available in states outside Nevada
Employer zip code
No
Southwest PreferredDental Organization
Yes—groups of 5+
Customer Service, BilingualSupport & Broker Services888-429-0914
Commissions602-241-0914 x2504
Claims602-241-0914 x2505
Fax (Add-ons/Deletes)602-285-0121
Southwest PreferredDental Organization
National NetworkDenteMax
DE
NT
AL
The Copay Plans have no in-network waiting periods.
The PPO and Indemnity employer sponsored plans do nothave waiting periods.
For plans with waiting periods insureds received month-to-month prior coverage credit for satisfaction of waiting periodmet under employer’s prior qualifying group dental plan
EXCLUSIONS ALLOWED BY CARRIER:
Hourly/Salary?Yes
Management/Non-management?Yes
Union/Non-union?Yes
Minimum group size2
Employees
Dependents
Employees
Dependents
Employees
For Dependents
% of Total Cost:
RATING INFORMATION
MINIMUM EMPLOYER CONTRIBUTION
PARTICIPATION
Contributory
Non-Contributory
GROUP SIZE
GROUP SIZE
◆ Those covered by another plan are NOT considered eligible in calculating participation
◆◆ In order to NOT be considered eligible, the other coveragemust be a group plan
CARVE OUTS*
SPECIAL CONSIDERATIONS
PPO & Indemnity
ORTHODONTIC COVERAGE
WAITING PERIOD WAIVER/TAKEOVER
PLAN ELIGIBILITY REQUIREMENTS
OUT OF NETWORK CLAIM ADJUDICATION
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
COVERAGE REQUIREMENTS
108
w w w. w o r d a n d b r o w n . c o m
Are Commission-Only employees allowed?No
Are 1099 employees allowed?Yes—as long as they work full-time and exclusively for the group
Any ineligible industries?Yes
Virgin groups eligible?Yes—12 months in business
Wage & tax reports required?State
ER Sponsored5+
N/A
2-50*
12 months
No
85th percentile
75%
N/A
5+
50%
N/A
N/A
N/A
All plans include a scheduled (discounted) orthodonticbenefit for adults and children.
Insured orthodontia also available to 10 or more enrolledemployees:
Child only$1,000 lifetime maximum$500 annual50% coverage12 month waiting period
Voluntary2+
N/A
N/A
N/A
* 51 or more - Large group available upon request. Please contactyour Word & Brown Representative for details.
Group Size
Rate Guarantee
Rates vary by Industry?
* Employer sponsored groups may also contribute 100% of theemployee only cost of The Copay Plan and employees can buyup to The PPO Plan and/or The Indemnity Plan.
Benefit Highlights
- Flexible Triple and Dual choice plans for groups of 5 or more enrolled
- White fillings on molars are standard- Endo & Perio in Basic or Major- 4 cleanings with perio surgery is standard- No age limit on pediatric care- No 6 month limit on cleaning frequency- Missing teeth covered after 36 months
Annual open enrollment for all plans
Monthly administrative fees per group:Groups with 2-24 insured: $15.00 per monthGroups with 25-49 insured: $20.00 per monthGroups with 50+ insured: $30.00 per monthAll PEOs Groups (Employee leasing companies): $50.00 per month
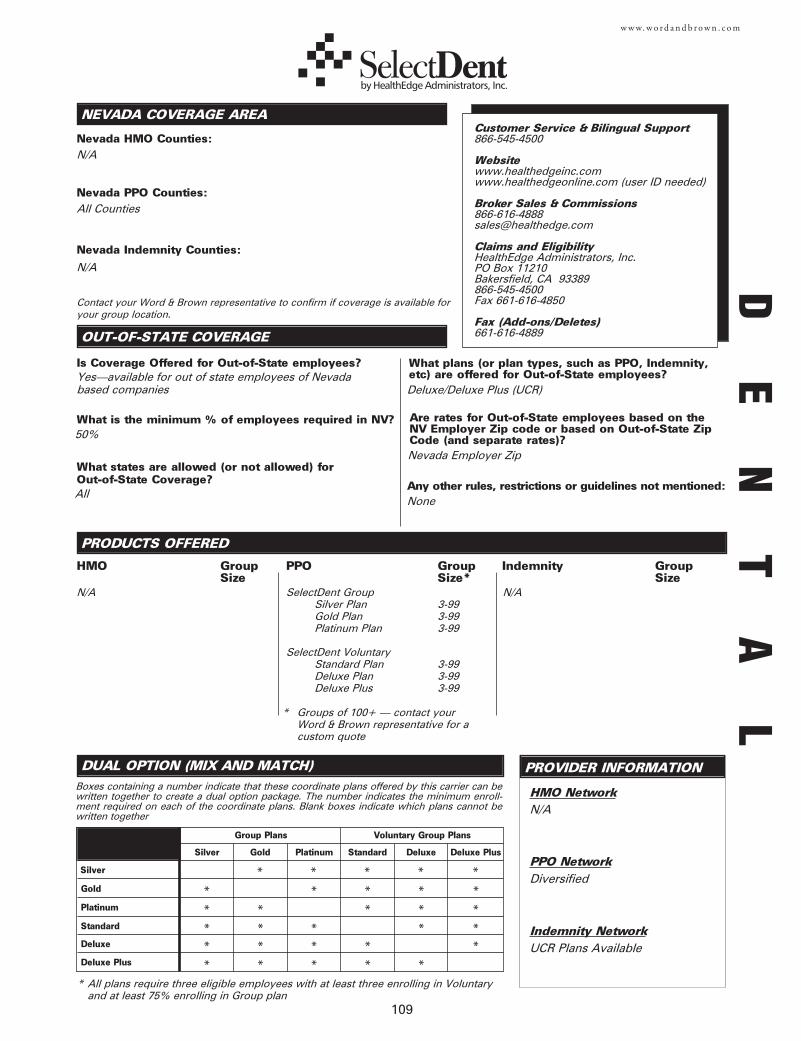
109
w w w. w o r d a n d b r o w n . c o m
OUT-OF-STATE COVERAGE
NEVADA COVERAGE AREA
DUAL OPTION (MIX AND MATCH)
Nevada HMO Counties:
Boxes containing a number indicate that these coordinate plans offered by this carrier can bewritten together to create a dual option package. The number indicates the minimum enroll-ment required on each of the coordinate plans. Blank boxes indicate which plans cannot bewritten together
PROVIDER INFORMATION
PRODUCTS OFFERED
Nevada PPO Counties:
Nevada Indemnity Counties:
Is Coverage Offered for Out-of-State employees?
What is the minimum % of employees required in NV?
What plans (or plan types, such as PPO, Indemnity,etc) are offered for Out-of-State employees?
What states are allowed (or not allowed) for Out-of-State Coverage?
Are rates for Out-of-State employees based on theNV Employer Zip code or based on Out-of-State ZipCode (and separate rates)?
Any other rules, restrictions or guidelines not mentioned:
HMO Network
Indemnity Network
N/A3-993-993-99
3-993-993-99
N/A
DiversifiedSilver
Gold *
SelectDent Group Silver PlanGold PlanPlatinum Plan
SelectDent Voluntary Standard PlanDeluxe PlanDeluxe Plus
N/A
N/A
All Counties
N/A
Yes—available for out of state employees of Nevadabased companies
Platinum *Standard *Deluxe *
HMO Group Size
PPO Group Size*
Indemnity Group Size
* Groups of 100+ — contact your Word & Brown representative for a custom quote
Silver Gold Platinum Standard Deluxe
UCR Plans Available
* All plans require three eligible employees with at least three enrolling in Voluntary and at least 75% enrolling in Group plan
Group Plans Voluntary Group Plans
Customer Service & Bilingual Support866-545-4500
Websitewww.healthedgeinc.comwww.healthedgeonline.com (user ID needed)
Broker Sales & Commissions866-616-4888 [email protected]
Claims and EligibilityHealthEdge Administrators, Inc.PO Box 11210Bakersfield, CA 93389866-545-4500Fax 661-616-4850
Fax (Add-ons/Deletes)661-616-4889
Nevada Employer Zip
Deluxe/Deluxe Plus (UCR)
PPO Network
50%
All None
Deluxe Plus
Deluxe Plus *
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
* * * * *
Contact your Word & Brown representative to confirm if coverage is available foryour group location.
DE
NT
AL
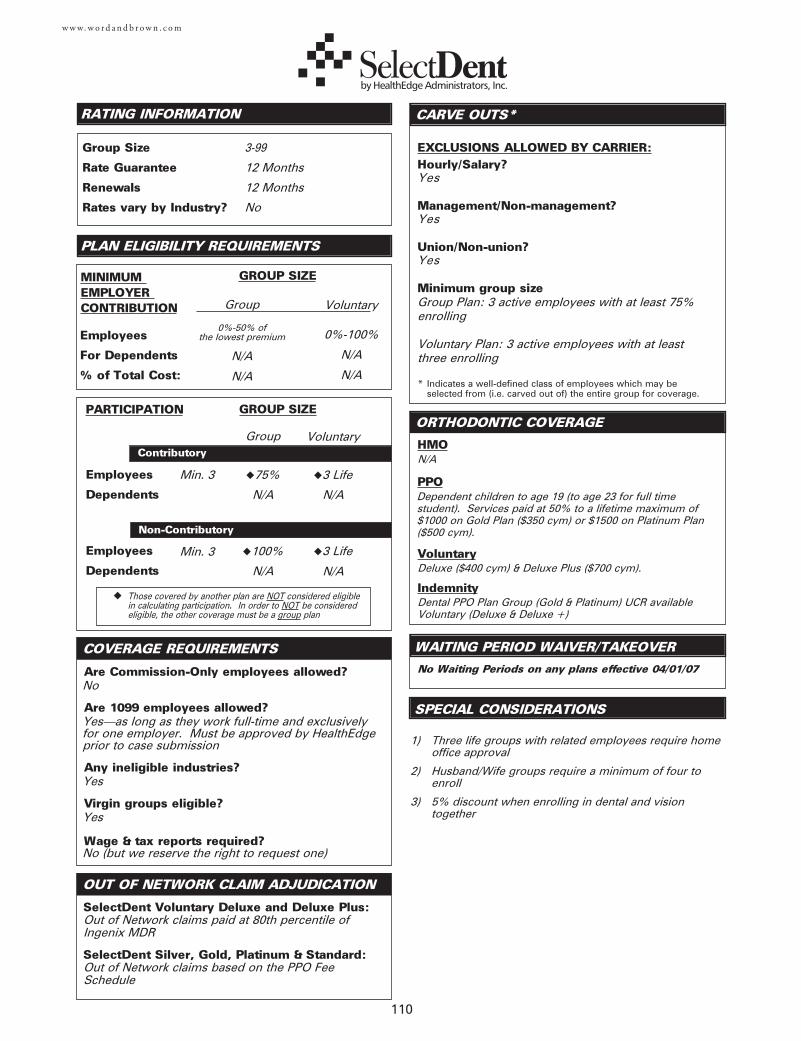
Are Commission-Only employees allowed?
Are 1099 employees allowed?
Any ineligible industries?
Virgin groups eligible?
Wage & tax reports required?
110
w w w. w o r d a n d b r o w n . c o m
SPECIAL CONSIDERATIONS
No Waiting Periods on any plans effective 04/01/07
No
Yes—as long as they work full-time and exclusivelyfor one employer. Must be approved by HealthEdgeprior to case submission
Yes
Yes
No (but we reserve the right to request one)
Employees
Dependents
Employees
Dependents
RATING INFORMATION
PARTICIPATION
Contributory
Non-Contributory
GROUP SIZE
GROUP SIZE
◆ Those covered by another plan are NOT considered eligible in calculating participation. In order to NOT be considered eligible, the other coverage must be a group plan
EXCLUSIONS ALLOWED BY CARRIER:Hourly/Salary?Yes
Management/Non-management?Yes
Union/Non-union?Yes
Minimum group sizeGroup Plan: 3 active employees with at least 75%enrolling
Voluntary Plan: 3 active employees with at leastthree enrolling
CARVE OUTS*
HMO
ORTHODONTIC COVERAGE
WAITING PERIOD WAIVER/TAKEOVER
PLAN ELIGIBILITY REQUIREMENTS
OUT OF NETWORK CLAIM ADJUDICATION
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
Group Size
Rate Guarantee
Renewals
Rates vary by Industry?
PPO
Voluntary
COVERAGE REQUIREMENTS
3-99
12 Months
12 Months
No
SelectDent Voluntary Deluxe and Deluxe Plus:Out of Network claims paid at 80th percentile ofIngenix MDR
SelectDent Silver, Gold, Platinum & Standard:Out of Network claims based on the PPO FeeSchedule
N/A
Group
0%-50% of the lowest premium
N/A
N/A
Voluntary
0%-100%
N/A
N/A
Dependent children to age 19 (to age 23 for full timestudent). Services paid at 50% to a lifetime maximum of$1000 on Gold Plan ($350 cym) or $1500 on Platinum Plan($500 cym).
Group Voluntary
Min. 3
◆100%
N/A
◆3 Life
N/A
Min. 3
◆75%
N/A
◆3 Life
N/A
Deluxe ($400 cym) & Deluxe Plus ($700 cym).
Employees
For Dependents
% of Total Cost:
MINIMUM EMPLOYER CONTRIBUTION
IndemnityDental PPO Plan Group (Gold & Platinum) UCR availableVoluntary (Deluxe & Deluxe +)
WAITING PERIOD WAIVER/TAKEOVER
1) Three life groups with related employees require home office approval
2) Husband/Wife groups require a minimum of four to enroll
3) 5% discount when enrolling in dental and vision together
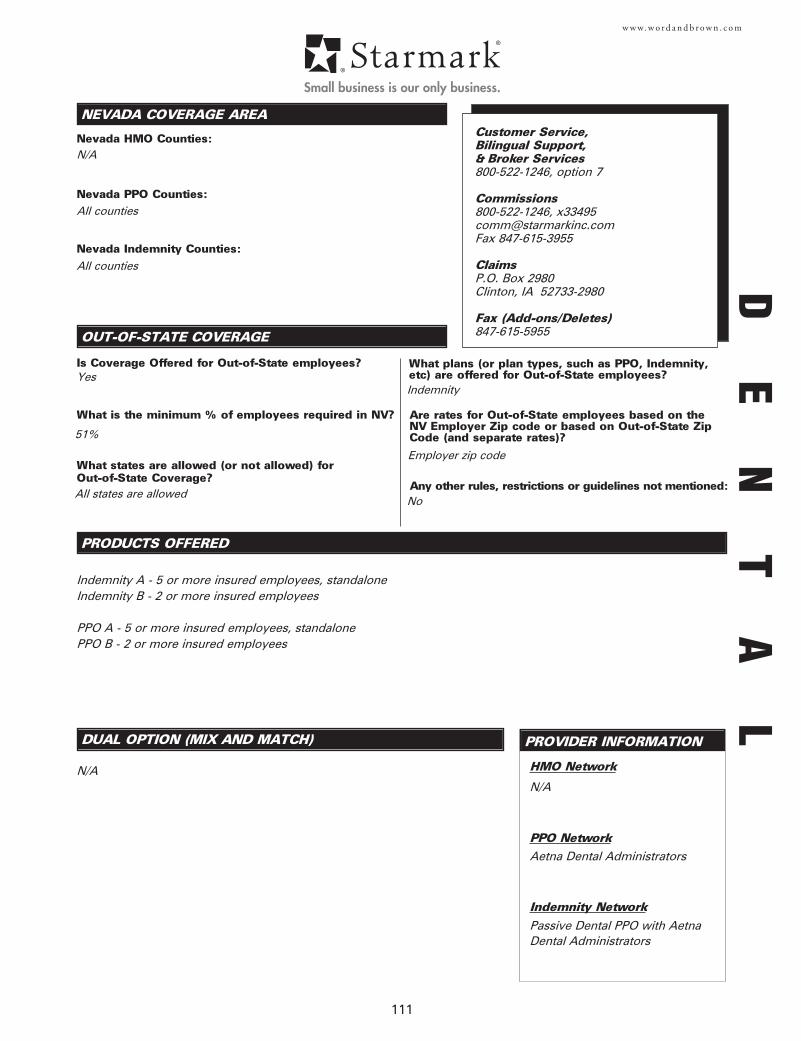
OUT-OF-STATE COVERAGE
NEVADA COVERAGE AREA
DUAL OPTION (MIX AND MATCH)
Nevada HMO Counties:
PROVIDER INFORMATION
Customer Service, Bilingual Support,& Broker Services800-522-1246, option 7
Commissions 800-522-1246, [email protected] 847-615-3955
ClaimsP.O. Box 2980Clinton, IA 52733-2980
Fax (Add-ons/Deletes)847-615-5955
PRODUCTS OFFERED
Nevada PPO Counties:
Nevada Indemnity Counties:
Is Coverage Offered for Out-of-State employees?
What is the minimum % of employees required in NV?
What plans (or plan types, such as PPO, Indemnity,etc) are offered for Out-of-State employees?
What states are allowed (or not allowed) for Out-of-State Coverage?
Are rates for Out-of-State employees based on theNV Employer Zip code or based on Out-of-State ZipCode (and separate rates)?
Any other rules, restrictions or guidelines not mentioned:
HMO Network
PPO Network
Indemnity Network
111
w w w. w o r d a n d b r o w n . c o m
N/A
Aetna Dental Administrators
Indemnity A - 5 or more insured employees, standaloneIndemnity B - 2 or more insured employees
PPO A - 5 or more insured employees, standalonePPO B - 2 or more insured employees
N/A
All counties
All counties
Yes
Passive Dental PPO with AetnaDental Administrators
Employer zip code
Indemnity
51%
All states are allowedNo
N/A
DE
NT
AL
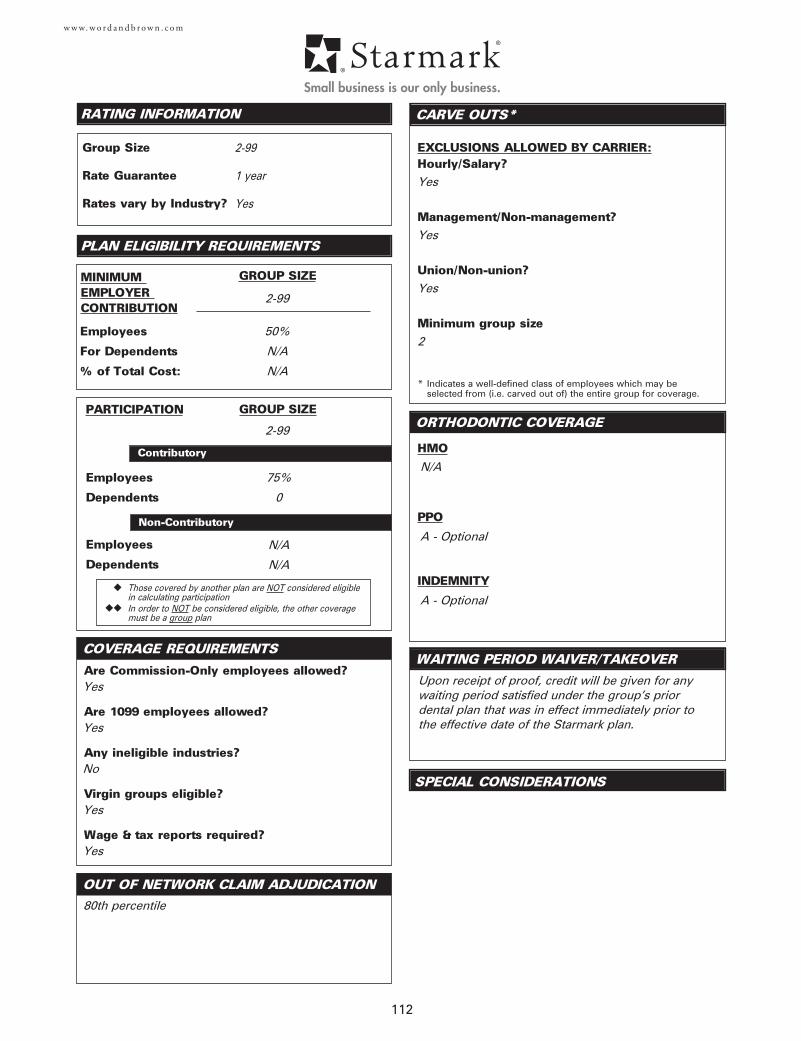
Employees
Dependents
Employees
Dependents
Employees
For Dependents
% of Total Cost:
RATING INFORMATION
MINIMUM EMPLOYER CONTRIBUTION
PARTICIPATION
Contributory
Non-Contributory
GROUP SIZE
GROUP SIZE
◆ Those covered by another plan are NOT considered eligible in calculating participation
◆◆ In order to NOT be considered eligible, the other coveragemust be a group plan
EXCLUSIONS ALLOWED BY CARRIER:Hourly/Salary?
Management/Non-management?
Union/Non-union?
Minimum group size
CARVE OUTS*
SPECIAL CONSIDERATIONS
HMO
ORTHODONTIC COVERAGE
WAITING PERIOD WAIVER/TAKEOVER
PLAN ELIGIBILITY REQUIREMENTS
OUT OF NETWORK CLAIM ADJUDICATION
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
Group Size
Rate Guarantee
Rates vary by Industry?
PPO
COVERAGE REQUIREMENTS
112
w w w. w o r d a n d b r o w n . c o m
Are Commission-Only employees allowed?
Are 1099 employees allowed?
Any ineligible industries?
Virgin groups eligible?
Wage & tax reports required?
Yes
Yes
Yes
2
2-99
1 year
Yes
Yes
Yes
No
Yes
Yes
80th percentile
Upon receipt of proof, credit will be given for anywaiting period satisfied under the group’s priordental plan that was in effect immediately prior to the effective date of the Starmark plan.
2-99
50%
N/A
N/A
2-99
75%
0
N/A
N/A
N/A
A - Optional
INDEMNITY
A - Optional

113
VISION
OUT-OF-STATE COVERAGE
NEVADA COVERAGE AREA
PRODUCTS OFFERED
Is Coverage Offered for Out-of-State employees?
What is the minimum % of employees required in NV?
What plans (or plan types, such as PPO, Indemnity,etc) are offered for Out-of-State employees?
What states are allowed (or not allowed) for Out-of-State Coverage?
Are rates for Out-of-State employees based on theNV Employer Zip code or based on Out-of-State ZipCode (and separate rates)?
Any other rules, restrictions or guidelines not mentioned:
115
w w w. w o r d a n d b r o w n . c o m
PROVIDER INFORMATION
Nevada Prepaid HMO Counties:
Nevada PPO Counties:
Nevada Indemnity Counties:
N/A
N/A
All
2-50Blue ViewBlue View Plus
Yes
51%
All
All plans - PPO
NV Employer Zip Code
Contact your Word & Brown representative
Member Support877-833-5734Broker Support888-445-9236Fax (Adds/Terms)303-831-2399Commissions888-445-9236BillingAnthem Blue Cross and Blue Shield P.O. Box 541013 Los Angeles, CA 90054-1013877-833-5734Fax 303-831-2399Vision Claims (out-of-network only)Blue View VisionAttn: OON ClaimsP.O. Box 8504Mason, OH 45040-7111866-723-0515
Contact your Word & Brown representative
VI
SI
ON
Employees
Dependents
Employees
Dependents
Are Commission-Only employees allowed?
Are 1099 employees allowed?
Any ineligible industries?
Virgin groups eligible?
Wage & tax reportstatements required?
Employees
For Dependents
% of Total Cost:
RATING INFORMATION
MINIMUMEMPLOYERCONTRIBUTION
PARTICIPATION
Contributory
Non-Contributory
GROUP SIZE
GROUP SIZE
◆ Those covered by another plan are NOT considered eligible in calculating participation
◆◆ Creditable coverage includes group, individual, and other qualifying waivers by NRS 689C.053
EXCLUSIONS ALLOWED BY CARRIER:Hourly/Salary?
Management/Non-management?
Union/Non-union?
Minimum group size
CARVE OUTS*
SPECIAL CONSIDERATIONS
WAITING PERIOD WAIVER/TAKEOVER
PLAN ELIGIBILITY REQUIREMENTS
OUT OF NETWORK CLAIM ADJUDICATION
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
Group Size
Rate Guarantee
Rates vary by Industry?
COVERAGE REQUIREMENTS
116
w w w. w o r d a n d b r o w n . c o m
2-50
2-50
12 Months
No
50%
N/A
N/A
2-50
75%
Yes
Yes
Yes
5 (could be lower on specialty products. Contactyour Word & Brown representative)
Contact your Word & Brown representative
Contact your Word & Brown representative
Contact your Word & Brown representative
Contact your Word & Brown representative
Contact your Word & Brown representative
Yes—need two W-2’s, no more than 50% and 1099
Same as above
No
Yes
Yes—if more than 3 months in business
Contact your Word & Brown representative
OUT-OF-STATE COVERAGE
NEVADA COVERAGE AREA
PROVIDER INFORMATION
PRODUCTS OFFERED
Nevada Vision Indemnity Counties:
Is Coverage Offered for Out-of-State employees?
What is the minimum % of employees required in NV?
What plans (or plan types, such as PPO, Indemnity,etc) are offered for Out-of-State employees?
What states are allowed (or not allowed) for Out-of-State Coverage?
Are rates for Out-of-State employees based on theNV Employer Zip code or based on Out-of-State ZipCode (and separate rates)?
Any other rules, restrictions or guidelines not mentioned:
Indemnity Network
117
w w w. w o r d a n d b r o w n . c o m
Outlook Vision Services (National)www.outlookvision.com
The BEST Life Stand Alone Vision plans are available either as stand alonefor groups with 5 or more employees enrolling, or bundled with anotherBEST Life product for groups with 2 or more employees enrolling.
All counties
There is no minimum
Yes—BEST Life's Vision Indemnity plan is available to allstates in the country
There are no restrictions on which states can receive out-of-state coverage. BEST Life's Stand Alone Vision plan is available to all states within the country
Out-of-State employees can enroll on the Stand AloneVision plan, which is an Indemnity plan availablethroughout the United States.
Rates are based on the NV Employer Zip code
None
PlanExam/Lenses/Frames/ContactsPlan A 12/12/12/12 monthsPlan B 12/12/24/12 monthsPlan C12/12/24/24 monthsPlan D12/24/24/24 monthsPlans come with the choice of $0, $10 or $25 deductible, and contact lenses maybe covered in lieu of frames and lenses or in addition to frames and lenses.
PROVIDER INFORMATION
Member Support, Customer Service & Commissions:[email protected]
BillingBEST Life and Health Insurance Co. 2505 McCabe WayIrvine, CA 92614-6243
ClaimsBEST Life and Health Insurance Co. P.O. Box 890Meridian, ID 83890800-433-0088Fax 208-893-5040Email: [email protected]
Fax (Add-ons/Deletes)949-724-1603
VI
SI
ON
Employees
Dependents
Employees
Dependents
Are Commission-Only employees allowed?
Are 1099 employees allowed?
Any ineligible industries?
Virgin groups eligible?
Wage & tax reports required?
Employees
For Dependents
% of Total Cost:
RATING INFORMATION
MINIMUM EMPLOYER CONTRIBUTION
PARTICIPATION
Contributory
Non-Contributory
GROUP SIZE
GROUP SIZE
EXCLUSIONS ALLOWED BY CARRIER:Hourly/Salary?
Management/Non-management?
Union/Non-union?
Minimum group size
CARVE OUTS*
SPECIAL CONSIDERATIONS
WAITING PERIOD WAIVER/TAKEOVER
PLAN ELIGIBILITY REQUIREMENTS
OUT OF NETWORK CLAIM ADJUDICATION
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
Group Size
Rate Guarantee
Rates vary by Industry?
COVERAGE REQUIREMENTS
118
w w w. w o r d a n d b r o w n . c o m
EmployerSponsored 5+
50%
N/A
N/A
Bundled: 2+, Stand alone: 5+
0%
N/A
N/A
Claims payments are based on a per service maximum
Voluntary Plans5+
Yes
60% participation of eligible employees. On groupswhere employer contributes 100% requires 100%
participation of eligible employees.
5+
1 year
N/A
20% participation of eligible employees
N/A
Yes—if group has a carve out in place with prior vision carrier
Yes—if group has a carve out in place with prior vision carrier
No
Minimum of 10 employees or more enrolling, if previously insured this way
There are no waiting periods for BEST Life's StandAlone Vision plan
No
These employees are not eligible unless written with medical
No
Yes
Yes—for groups enrolling less than 5 employees
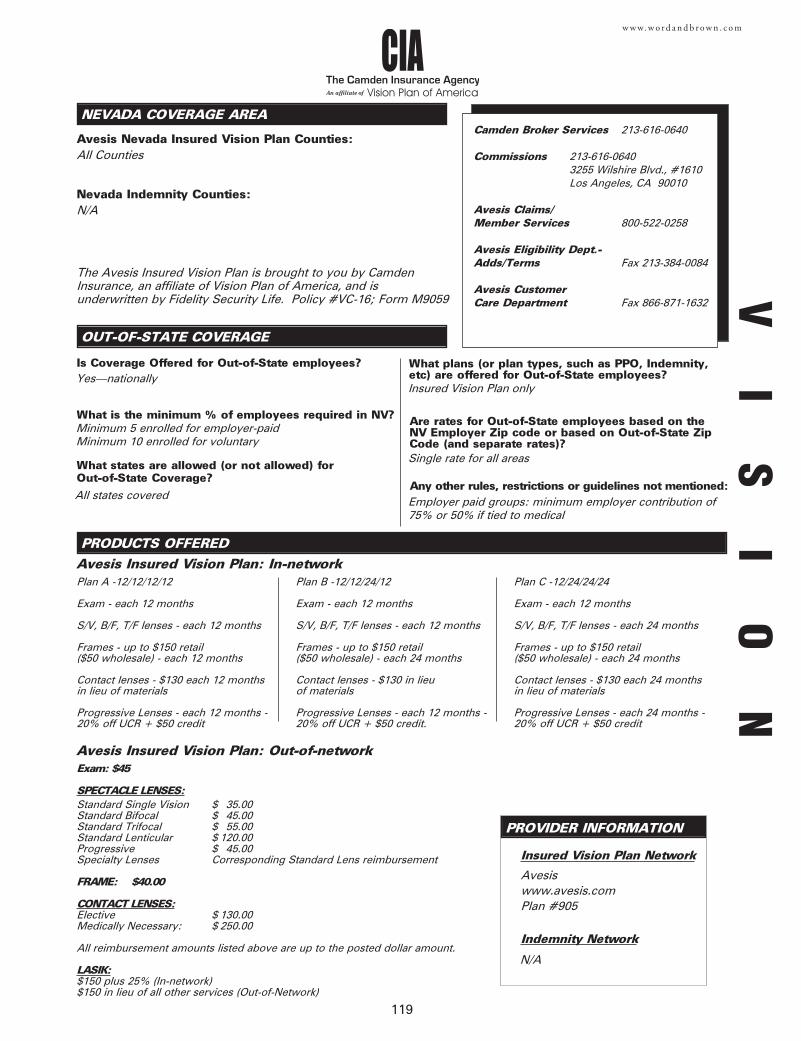
119
w w w. w o r d a n d b r o w n . c o m
The Camden Insurance AgencyVision Plan of AmericaAn affiliate of
OUT-OF-STATE COVERAGE
NEVADA COVERAGE AREA
Avesis Nevada Insured Vision Plan Counties:
PRODUCTS OFFERED
Nevada Indemnity Counties:
Is Coverage Offered for Out-of-State employees?
What is the minimum % of employees required in NV?
What plans (or plan types, such as PPO, Indemnity,etc) are offered for Out-of-State employees?
What states are allowed (or not allowed) for Out-of-State Coverage?
Are rates for Out-of-State employees based on theNV Employer Zip code or based on Out-of-State ZipCode (and separate rates)?
Any other rules, restrictions or guidelines not mentioned:
Avesiswww.avesis.comPlan #905
Plan A -12/12/12/12
Exam - each 12 months
S/V, B/F, T/F lenses - each 12 months
Frames - up to $150 retail ($50 wholesale) - each 12 months
Contact lenses - $130 each 12 months in lieu of materials
Progressive Lenses - each 12 months -20% off UCR + $50 credit
All Counties
N/A
Minimum 5 enrolled for employer-paidMinimum 10 enrolled for voluntary
Yes—nationally
All states covered
Insured Vision Plan only
Single rate for all areas
Employer paid groups: minimum employer contribution of75% or 50% if tied to medical
Avesis Insured Vision Plan: In-networkPlan B -12/12/24/12
Exam - each 12 months
S/V, B/F, T/F lenses - each 12 months
Frames - up to $150 retail ($50 wholesale) - each 24 months
Contact lenses - $130 in lieu of materials
Progressive Lenses - each 12 months -20% off UCR + $50 credit.
Plan C -12/24/24/24
Exam - each 12 months
S/V, B/F, T/F lenses - each 24 months
Frames - up to $150 retail ($50 wholesale) - each 24 months
Contact lenses - $130 each 24 monthsin lieu of materials
Progressive Lenses - each 24 months -20% off UCR + $50 credit
Insured Vision Plan Network
Indemnity Network
Exam: $45
SPECTACLE LENSES:Standard Single Vision $ 35.00Standard Bifocal $ 45.00Standard Trifocal $ 55.00Standard Lenticular $ 120.00Progressive $ 45.00Specialty Lenses Corresponding Standard Lens reimbursement
FRAME: $40.00
CONTACT LENSES:Elective $ 130.00Medically Necessary: $ 250.00
All reimbursement amounts listed above are up to the posted dollar amount.
LASIK:$150 plus 25% (In-network)$150 in lieu of all other services (Out-of-Network)
Avesis Insured Vision Plan: Out-of-network
PROVIDER INFORMATION
The Avesis Insured Vision Plan is brought to you by CamdenInsurance, an affiliate of Vision Plan of America, and isunderwritten by Fidelity Security Life. Policy #VC-16; Form M9059
N/A
VI
SI
ON
Camden Broker Services 213-616-0640
Commissions 213-616-06403255 Wilshire Blvd., #1610Los Angeles, CA 90010
Avesis Claims/Member Services 800-522-0258
Avesis Eligibility Dept.-Adds/Terms Fax 213-384-0084
Avesis Customer Care Department Fax 866-871-1632
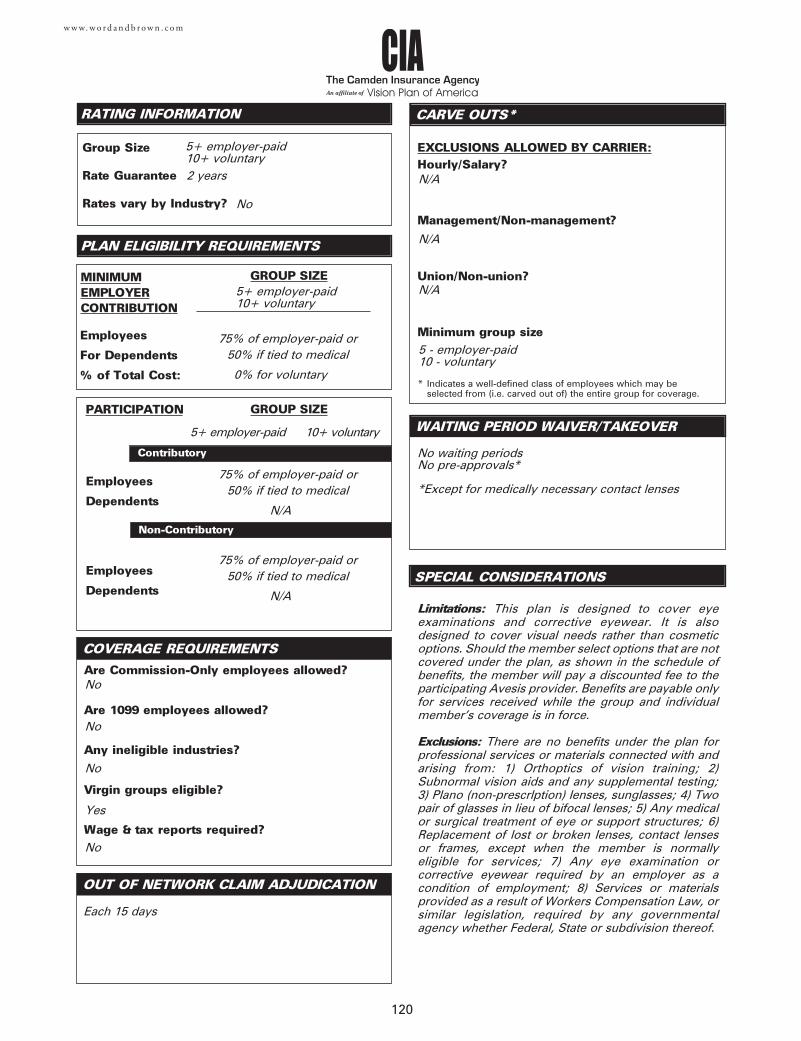
120
w w w. w o r d a n d b r o w n . c o m
The Camden Insurance AgencyVision Plan of AmericaAn affiliate of
Employees
Dependents
Employees
Dependents
Are Commission-Only employees allowed?
Are 1099 employees allowed?
Any ineligible industries?
Virgin groups eligible?
Wage & tax reports required?
Employees
For Dependents
% of Total Cost:
RATING INFORMATION
MINIMUMEMPLOYERCONTRIBUTION
PARTICIPATION
Contributory
Non-Contributory
GROUP SIZE
GROUP SIZE
EXCLUSIONS ALLOWED BY CARRIER:Hourly/Salary?
Management/Non-management?
Union/Non-union?
Minimum group size
CARVE OUTS*
SPECIAL CONSIDERATIONS
WAITING PERIOD WAIVER/TAKEOVER
PLAN ELIGIBILITY REQUIREMENTS
OUT OF NETWORK CLAIM ADJUDICATION
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
Group Size
Rate Guarantee
Rates vary by Industry?
COVERAGE REQUIREMENTS
N/A
N/A
N/A
5 - employer-paid10 - voluntary
75% of employer-paid or 50% if tied to medical
0% for voluntary
75% of employer-paid or 50% if tied to medical
N/A
75% of employer-paid or 50% if tied to medical
N/A
No
No
No
Yes
No
5+ employer-paid10+ voluntary
5+ employer-paid10+ voluntary
Each 15 days
10+ voluntary
No waiting periodsNo pre-approvals*
*Except for medically necessary contact lenses
No
5+ employer-paid
2 years
Limitations: This plan is designed to cover eyeexaminations and corrective eyewear. It is alsodesigned to cover visual needs rather than cosmeticoptions. Should the member select options that are notcovered under the plan, as shown in the schedule ofbenefits, the member will pay a discounted fee to theparticipating Avesis provider. Benefits are payable onlyfor services received while the group and individualmember's coverage is in force.
Exclusions: There are no benefits under the plan forprofessional services or materials connected with andarising from: 1) Orthoptics of vision training; 2)Subnormal vision aids and any supplemental testing;3) Plano (non-prescrlption) lenses, sunglasses; 4) Twopair of glasses in lieu of bifocal lenses; 5) Any medicalor surgical treatment of eye or support structures; 6)Replacement of lost or broken lenses, contact lensesor frames, except when the member is normallyeligible for services; 7) Any eye examination orcorrective eyewear required by an employer as acondition of employment; 8) Services or materialsprovided as a result of Workers Compensation Law, orsimilar legislation, required by any governmentalagency whether Federal, State or subdivision thereof.
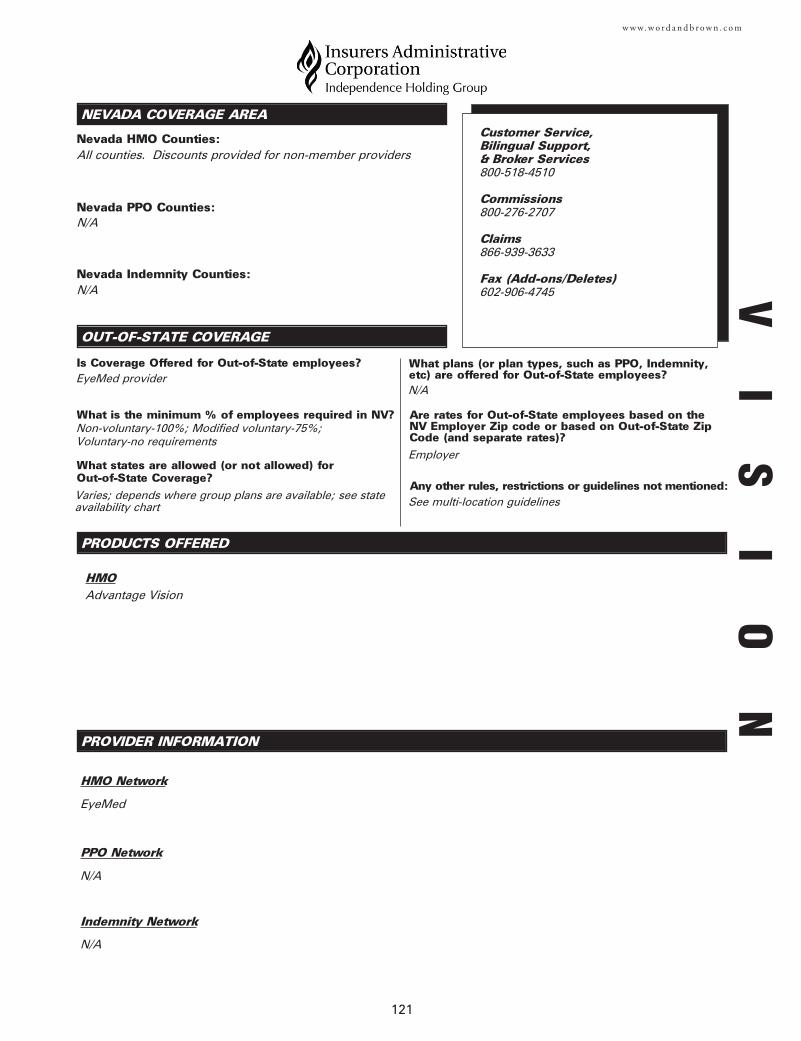
OUT-OF-STATE COVERAGE
NEVADA COVERAGE AREA
PRODUCTS OFFERED
Is Coverage Offered for Out-of-State employees?
What is the minimum % of employees required in NV?
What plans (or plan types, such as PPO, Indemnity,etc) are offered for Out-of-State employees?
What states are allowed (or not allowed) for Out-of-State Coverage?
Are rates for Out-of-State employees based on theNV Employer Zip code or based on Out-of-State ZipCode (and separate rates)?
Any other rules, restrictions or guidelines not mentioned:
HMO Network
PPO Network
Indemnity Network
121
w w w. w o r d a n d b r o w n . c o m
PROVIDER INFORMATION
Nevada HMO Counties:
Nevada PPO Counties:
Nevada Indemnity Counties:
All counties. Discounts provided for non-member providers
N/A
N/A
Non-voluntary-100%; Modified voluntary-75%; Voluntary-no requirements
EyeMed provider
Varies; depends where group plans are available; see stateavailability chart
N/A
Employer
See multi-location guidelines
Customer Service, Bilingual Support,& Broker Services800-518-4510
Commissions 800-276-2707
Claims866-939-3633
Fax (Add-ons/Deletes)602-906-4745
EyeMed
N/A
N/A
HMOAdvantage Vision
VI
SI
ON
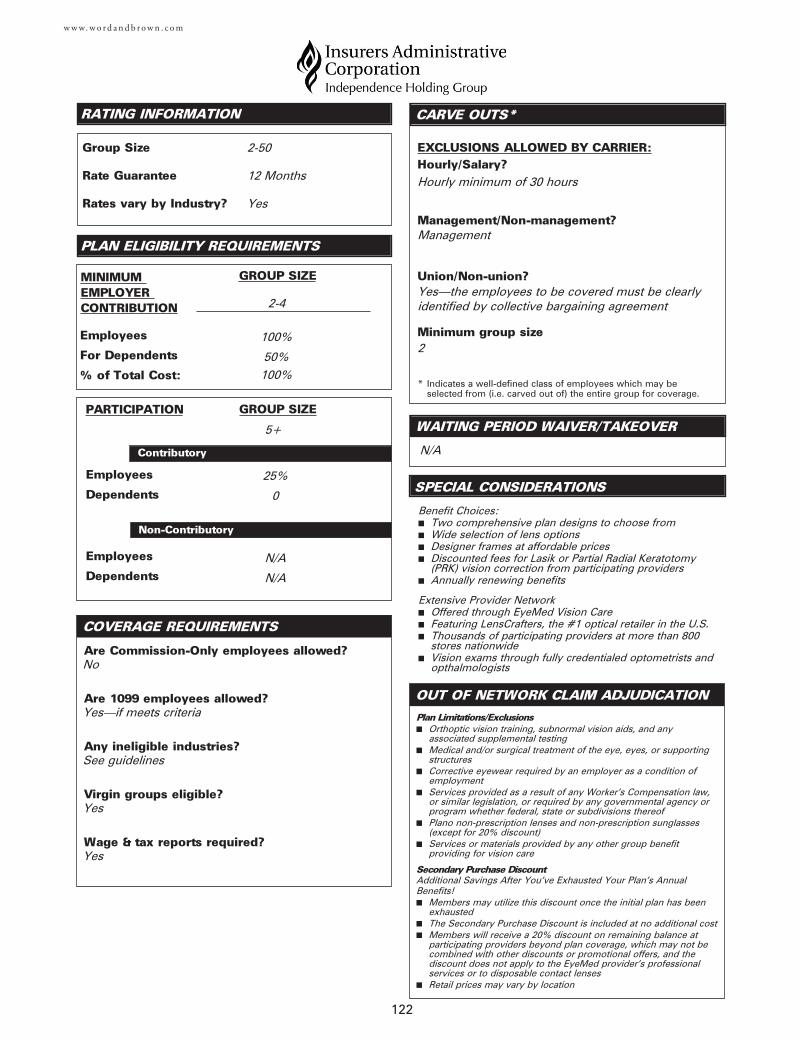
122
w w w. w o r d a n d b r o w n . c o m
Employees
Dependents
Employees
Dependents
Are Commission-Only employees allowed?
Are 1099 employees allowed?
Any ineligible industries?
Virgin groups eligible?
Wage & tax reports required?
Employees
For Dependents
% of Total Cost:
RATING INFORMATION
MINIMUM EMPLOYER CONTRIBUTION
PARTICIPATION
Contributory
Non-Contributory
GROUP SIZE
GROUP SIZE
EXCLUSIONS ALLOWED BY CARRIER:Hourly/Salary?
Management/Non-management?
Union/Non-union?
Minimum group size
CARVE OUTS*
SPECIAL CONSIDERATIONS
WAITING PERIOD WAIVER/TAKEOVER
PLAN ELIGIBILITY REQUIREMENTS
OUT OF NETWORK CLAIM ADJUDICATION
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
Group Size
Rate Guarantee
Rates vary by Industry?
COVERAGE REQUIREMENTS
N/A
Hourly minimum of 30 hours
Management
Yes—the employees to be covered must be clearlyidentified by collective bargaining agreement
2
2-4
100%
2-50
12 Months
Yes
No
Yes—if meets criteria
See guidelines
Yes
Yes
Plan Limitations/Exclusions■ Orthoptic vision training, subnormal vision aids, and any
associated supplemental testing■ Medical and/or surgical treatment of the eye, eyes, or supporting
structures■ Corrective eyewear required by an employer as a condition of
employment■ Services provided as a result of any Worker's Compensation law,
or similar legislation, or required by any governmental agency orprogram whether federal, state or subdivisions thereof
■ Plano non-prescription lenses and non-prescription sunglasses(except for 20% discount)
■ Services or materials provided by any other group benefitproviding for vision care
Secondary Purchase DiscountAdditional Savings After You’ve Exhausted Your Plan’s Annual Benefits!■ Members may utilize this discount once the initial plan has been
exhausted■ The Secondary Purchase Discount is included at no additional cost■ Members will receive a 20% discount on remaining balance at
participating providers beyond plan coverage, which may not becombined with other discounts or promotional offers, and thediscount does not apply to the EyeMed provider’s professionalservices or to disposable contact lenses
■ Retail prices may vary by location
25%
0Benefit Choices:■ Two comprehensive plan designs to choose from■ Wide selection of lens options■ Designer frames at affordable prices■ Discounted fees for Lasik or Partial Radial Keratotomy
(PRK) vision correction from participating providers■ Annually renewing benefits
Extensive Provider Network■ Offered through EyeMed Vision Care■ Featuring LensCrafters, the #1 optical retailer in the U.S.■ Thousands of participating providers at more than 800
stores nationwide■ Vision exams through fully credentialed optometrists and
opthalmologists
5+
100%
50%
N/A
N/A
OUT-OF-STATE COVERAGE
NEVADA COVERAGE AREA
PRODUCTS OFFERED
123
w w w. w o r d a n d b r o w n . c o m
PROVIDER INFORMATION
www.vsp.com
Vision and Voluntary Vision
Is Coverage Offered for Out-of-State employees?
What is the minimum % of employees required in NV?
What plans (or plan types, such as PPO, Indemnity,etc) are offered for Out-of-State employees?
What states are allowed (or not allowed) for Out-of-State Coverage?
Are rates for Out-of-State employees based on theNV Employer Zip code or based on Out-of-State ZipCode (and separate rates)?
Any other rules, restrictions or guidelines not mentioned:
Vision coverage is available throughout the state
Yes—contact your Word & Brown representative
Customer & Broker Services949-553-1616
Adds/TermsFax 949-553-1898
Commissions800-388-4793
BOR ChangesFax 515-235-5538
Claims800-247-4695
Contact your Word & Brown representative
All states available through Request-A-Quote except forMaryland and Vermont. Contact your Word & Brown representative
Indemnity. Vision is not available in Maryland or Vermont.
Rates are based on NV employer zip code with nodifference in rates for other locations
Yes—see Special Considerations
VI
SI
ON
Employees
Dependents
Are Commission-Only employees allowed?
Are 1099 employees allowed?
Any ineligible industries?
Virgin groups eligible?
Wage & tax reports required?
Employees
For Dependents
% of Total Cost:
RATING INFORMATION
MINIMUM EMPLOYER CONTRIBUTION
PARTICIPATION
Contributory
Voluntary
GROUP SIZE
GROUP SIZE
EXCLUSIONS ALLOWED BY CARRIER:Hourly/Salary?
Management/Non-management?
Union/Non-union?
Minimum group size
CARVE OUTS*
SPECIAL CONSIDERATIONS
WAITING PERIOD WAIVER/TAKEOVER
PLAN ELIGIBILITY REQUIREMENTS
OUT OF NETWORK CLAIM ADJUDICATION
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
Group Size
Rate Guarantee
Rates vary by Industry?
COVERAGE REQUIREMENTS
124
w w w. w o r d a n d b r o w n . c o m
Yes
Yes
Yes
10 enrolled lives
Yes
No
Yes
Yes
No
10 to 150
N/A
Waiting periods do not apply.
No
12 months
25%
N/A
25%
N/A
10-150
0 to 100%
0 to 100%
N/A
10-150
Employees
Dependents
Non-Contributory
100%
N/A
Employees
Dependents1. Contacts are only available if medically necessary.
2. Contact lens benefit is in lieu of the lens and frame,when contacts are chosen.
3. Annual enrollment period applies.
4. For groups over 150 lives, please contact yourWord & Brown representative.
5. Retirees are not eligible for coverage.
6. Members are eligible for a vision discount plan, theVSP Access Program, at no extra cost.
OUT-OF-STATE COVERAGE
NEVADA COVERAGE AREA
DUAL OPTION (MIX AND MATCH)
Nevada HMO Counties:
PROVIDER INFORMATION
PRODUCTS OFFERED
Nevada PPO Counties:
Nevada Indemnity Counties:
Is Coverage Offered for Out-of-State employees?
What is the minimum % of employees required in NV?
What plans (or plan types, such as PPO, Indemnity,etc) are offered for Out-of-State employees?
What states are allowed (or not allowed) for Out-of-State Coverage?
Are rates for Out-of-State employees based on theNV Employer Zip code or based on Out-of-State ZipCode (and separate rates)?
Any other rules, restrictions or guidelines not mentioned:
HMO Network
PPO Network
Indemnity Network
125
w w w. w o r d a n d b r o w n . c o m
VI
SI
ON
Vision Rider
N/A
Yes
75%
N/A
N/A
NV Zip code
No
N/A
N/A
N/A
N/A
N/A
N/A
Customer Service, Bilingual Support,& Broker Services 800-863-7515
Commissions 888-840-9080
Add-ons/Deletes Fax 775-770-9479
ClaimsSaint Mary’s Health PlansClaims/Member Services1510 Meadow Wood LaneReno, NV 89502
Employees
Dependents
Employees
Dependents
Employees
For Dependents
% of Total Cost:
RATING INFORMATION
MINIMUM EMPLOYER CONTRIBUTION
PARTICIPATION
Contributory
Non-Contributory
GROUP SIZE
GROUP SIZE
◆ Those covered by another plan are NOT considered eligible in calculating participation
◆◆ In order to NOT be considered eligible, the other coveragemust be a group plan
CARVE OUTS*
SPECIAL CONSIDERATIONS
WAITING PERIOD WAIVER/TAKEOVER
PLAN ELIGIBILITY REQUIREMENTS
OUT OF NETWORK CLAIM ADJUDICATION
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
Group Size
Rate Guarantee
Rates vary by Industry?
COVERAGE REQUIREMENTS
126
w w w. w o r d a n d b r o w n . c o m
Are Commission-Only employees allowed?No
Are 1099 employees allowed?Yes
Any ineligible industries?No
Virgin groups eligible?Yes
Wage & tax reports required?Yes
EXCLUSIONS ALLOWED BY CARRIER:
Hourly/Salary?None
Management/Non-management?None
Union/Non-union?None
Minimum group sizeNone
2
No
12 months
100%
N/A
2-50
N/A
N/A
N/A
None
100%
N/A
90th percentile
None
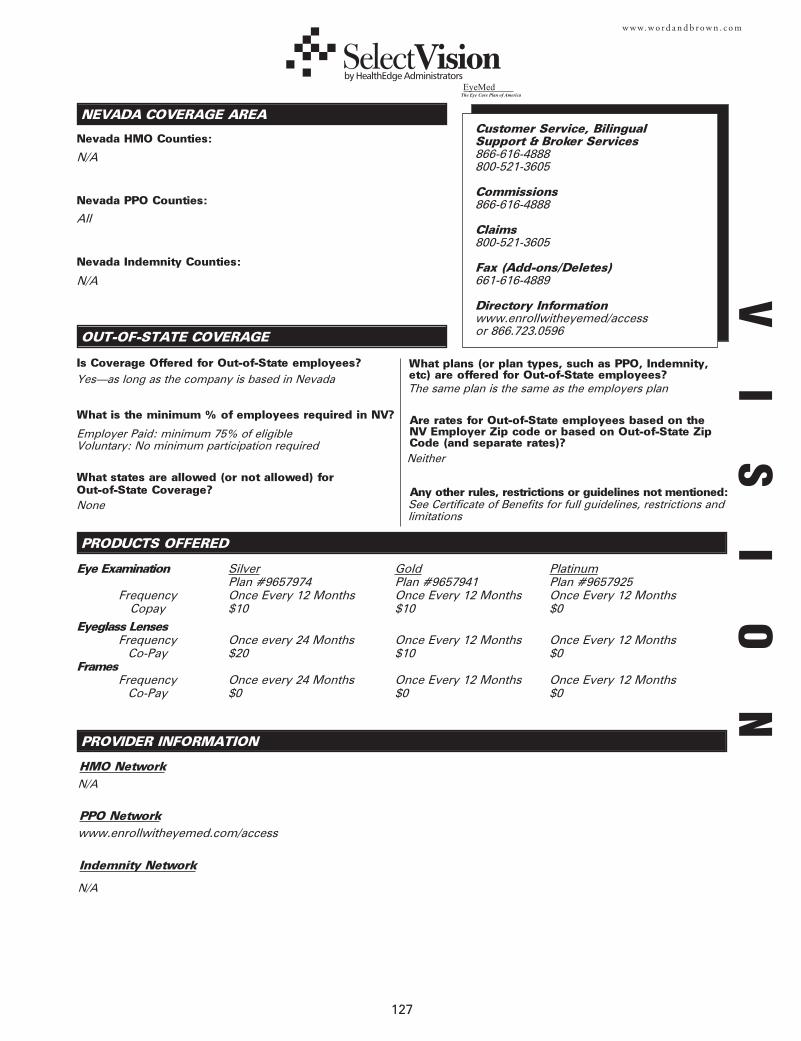
127
w w w. w o r d a n d b r o w n . c o m
OUT-OF-STATE COVERAGE
NEVADA COVERAGE AREA
Nevada HMO Counties:
PRODUCTS OFFERED
Nevada PPO Counties:
Nevada Indemnity Counties:
Is Coverage Offered for Out-of-State employees?
What is the minimum % of employees required in NV?
What plans (or plan types, such as PPO, Indemnity,etc) are offered for Out-of-State employees?
What states are allowed (or not allowed) for Out-of-State Coverage?
Are rates for Out-of-State employees based on theNV Employer Zip code or based on Out-of-State ZipCode (and separate rates)?
Any other rules, restrictions or guidelines not mentioned:
PPO Network
Indemnity Network
HMO Network
N/A
Yes—as long as the company is based in Nevada
Customer Service, BilingualSupport & Broker Services866-616-4888800-521-3605
Commissions866-616-4888
Claims800-521-3605
Fax (Add-ons/Deletes)661-616-4889
Directory Informationwww.enrollwitheyemed/access or 866.723.0596
Employer Paid: minimum 75% of eligible Voluntary: No minimum participation required
None
The same plan is the same as the employers plan
Neither
See Certificate of Benefits for full guidelines, restrictions andlimitations
All
N/A
www.enrollwitheyemed.com/access
N/A
N/A
PROVIDER INFORMATION
VI
SI
ON
Eye Examination Silver Gold PlatinumPlan #9657974 Plan #9657941 Plan #9657925
Frequency Once Every 12 Months Once Every 12 Months Once Every 12 MonthsCopay $10 $10 $0
Eyeglass LensesFrequency Once every 24 Months Once Every 12 Months Once Every 12 Months
Co-Pay $20 $10 $0 Frames
Frequency Once every 24 Months Once Every 12 Months Once Every 12 MonthsCo-Pay $0 $0 $0
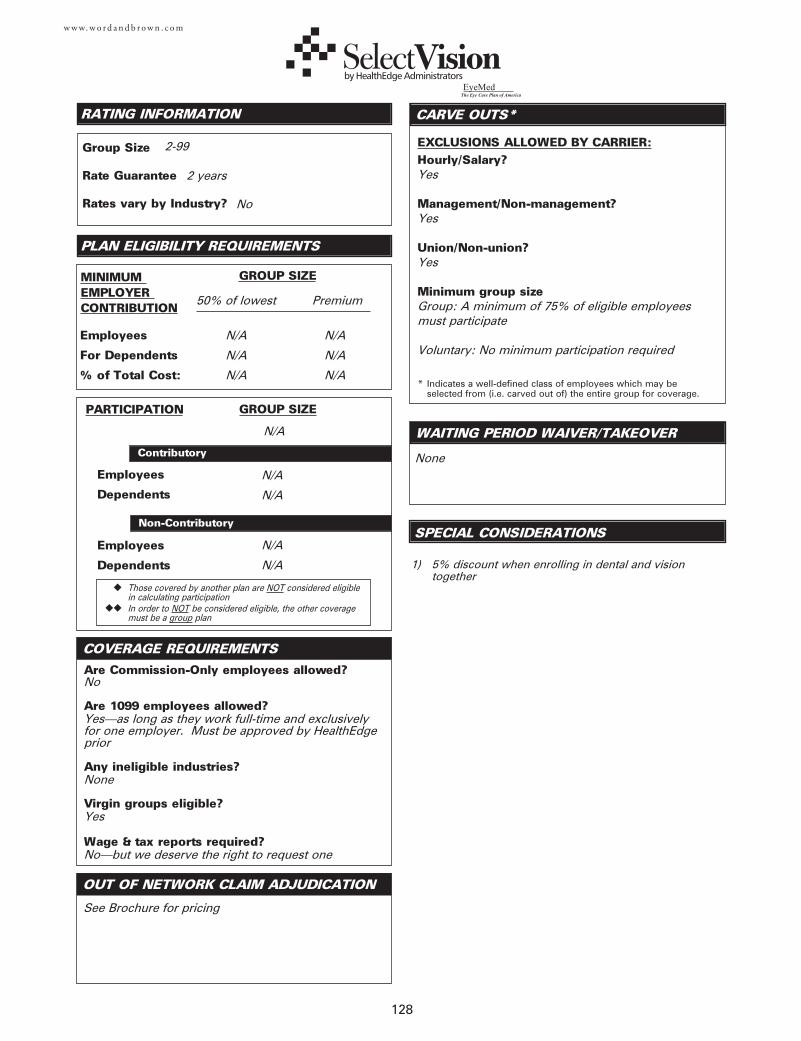
128
w w w. w o r d a n d b r o w n . c o m
Employees
Dependents
Employees
Dependents
Are Commission-Only employees allowed?No
Are 1099 employees allowed?Yes—as long as they work full-time and exclusivelyfor one employer. Must be approved by HealthEdgeprior
Any ineligible industries?None
Virgin groups eligible?Yes
Wage & tax reports required?No—but we deserve the right to request one
Employees
For Dependents
% of Total Cost:
RATING INFORMATION
MINIMUM EMPLOYER CONTRIBUTION
PARTICIPATION
Contributory
Non-Contributory
GROUP SIZE
GROUP SIZE
◆ Those covered by another plan are NOT considered eligible in calculating participation
◆◆ In order to NOT be considered eligible, the other coveragemust be a group plan
EXCLUSIONS ALLOWED BY CARRIER:Hourly/Salary?Yes
Management/Non-management?Yes
Union/Non-union?Yes
Minimum group sizeGroup: A minimum of 75% of eligible employeesmust participate
Voluntary: No minimum participation required
CARVE OUTS*
SPECIAL CONSIDERATIONS
WAITING PERIOD WAIVER/TAKEOVER
PLAN ELIGIBILITY REQUIREMENTS
OUT OF NETWORK CLAIM ADJUDICATION
* Indicates a well-defined class of employees which may be selected from (i.e. carved out of) the entire group for coverage.
Group Size
Rate Guarantee
Rates vary by Industry?
COVERAGE REQUIREMENTS
2-99
See Brochure for pricing
No
2 years
NoneN/A
N/A
N/A
N/A
N/A
N/A
50% of lowest Premium
N/A
N/A
N/A
N/A
N/A 1) 5% discount when enrolling in dental and vision together
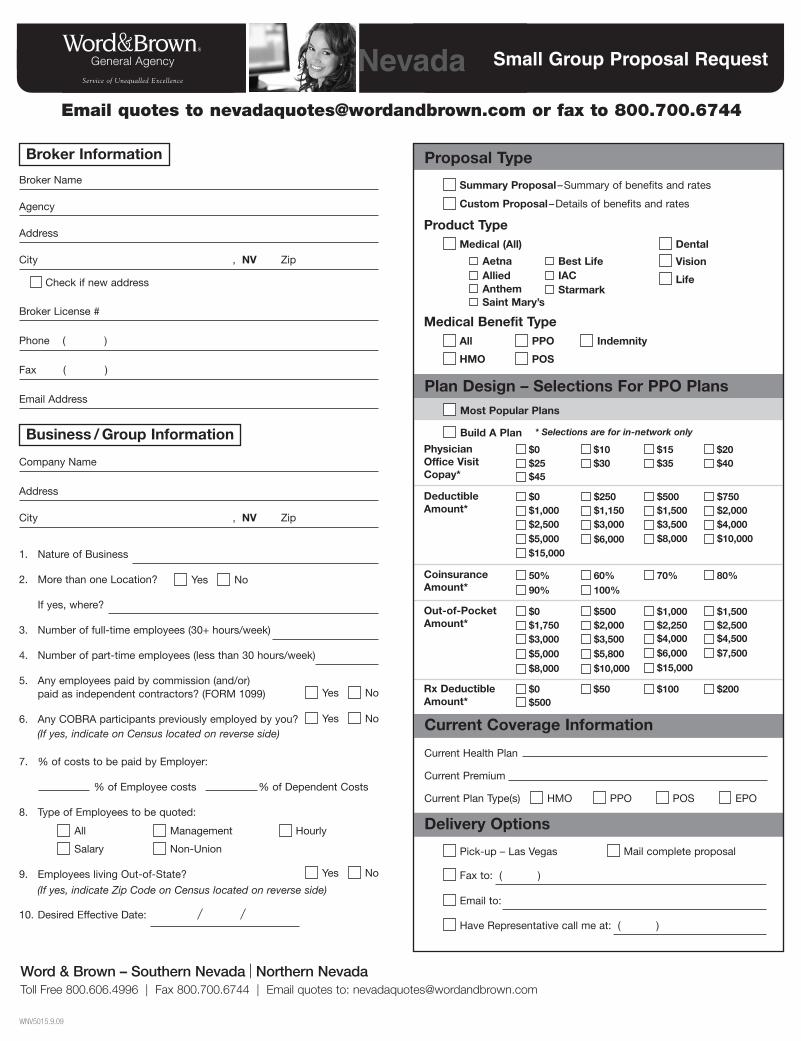
Small Group Proposal RequestNevadaEmail quotes to [email protected] or fax to 800.700.6744
$5,000
Broker Name
Agency
Address
City , NV Zip
Broker License #
Phone ( )
Fax ( )
Email Address
Check if new address
Company Name
Address
City , NV Zip
1. Nature of Business
2. More than one Location?
If yes, where?
3. Number of full-time employees (30+ hours/week)
4. Number of part-time employees (less than 30 hours/week)
5. Any employees paid by commission (and/or) paid as independent contractors? (FORM 1099)
6. Any COBRA participants previously employed by you?
7. % of costs to be paid by Employer:
% of Employee costs % of Dependent Costs
8. Type of Employees to be quoted:
9. Employees living Out-of-State?
10. Desired Effective Date:
Yes No
Yes No
Yes No
Yes No
(If yes, indicate on Census located on reverse side)
All Management Hourly
Salary Non-Union
(If yes, indicate Zip Code on Census located on reverse side)
Broker Information
Business / Group Information
WNV5015.9.09
Word & Brown – Southern Nevada | Northern NevadaToll Free 800.606.4996 | Fax 800.700.6744 | Email quotes to: [email protected]
Proposal Type
Plan Design – Selections For PPO PlansMost Popular Plans
$0$25$45
DeductibleAmount*
CoinsuranceAmount*
Out-of-Pocket Amount*
Rx Deductible Amount*
$10$30
$15$35
$20$40
$0$1,000$2,500
$250$1,150$3,000
$500$1,500$3,500
$750$2,000$4,000
$6,000 $8,000 $10,000
$0$1,750$3,000
$500$2,000$3,500
$1,000$2,250
$1,500$2,500
$4,000 $4,500
$5,000 $5,800 $6,000 $7,500
Current Health Plan
Current Premium
Current Plan Type(s)
Current Coverage Information
HMO PPO POS EPO
Delivery Options
Pick-up – Las Vegas
50% 60% 70% 80%90% 100%
Fax to: ( )
Email to:
Have Representative call me at: ( )
Mail complete proposal
$0$500
$50 $100 $200
PhysicianOffice VisitCopay*
Build A Plan * Selections are for in-network only
Summary Proposal–Summary of benefits and rates
Medical Benefit TypeAll
Custom Proposal–Details of benefits and rates
HMO
PPO
POS
Indemnity
$8,000 $10,000 $15,000
$15,000
Product TypeMedical (All) Dental
Vision
Life
AetnaAllied
Best LifeIACStarmark
Saint Mary’sAnthem
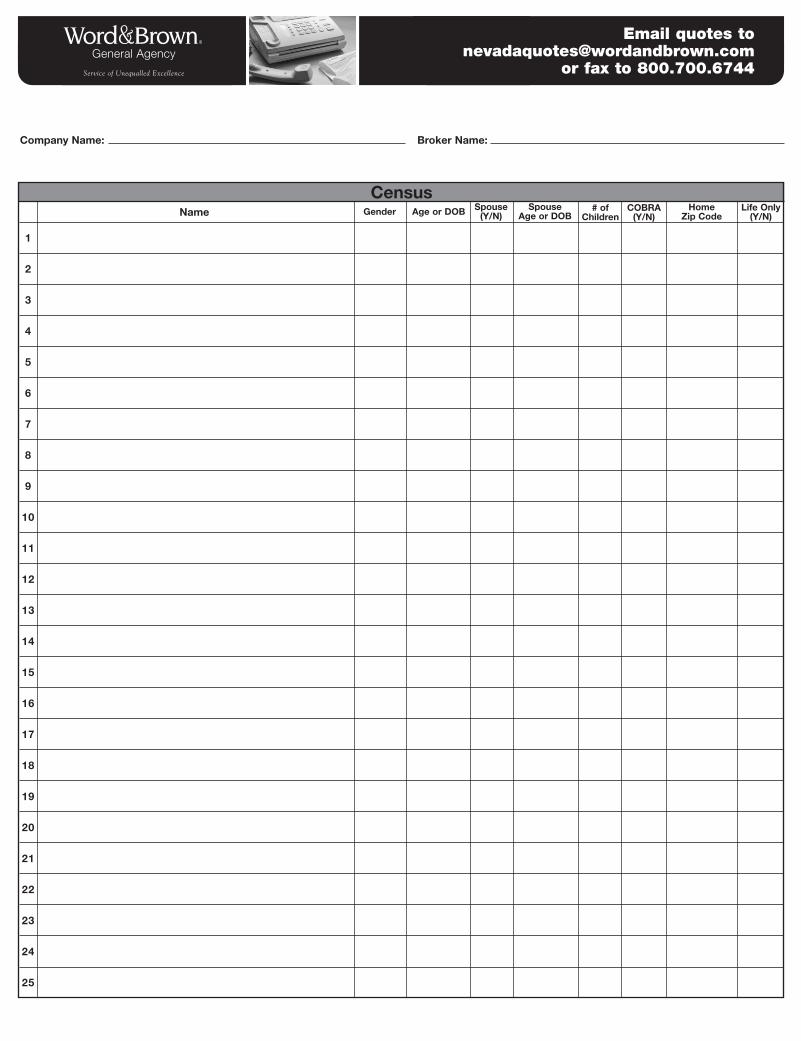
Email quotes to [email protected]
or fax to 800.700.6744
Company Name:
Name Age or DOBGender Spouse(Y/N)
# ofChildren
COBRA(Y/N)
Home Zip Code
Life Only(Y/N)
Broker Name:
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
CensusSpouse
Age or DOB
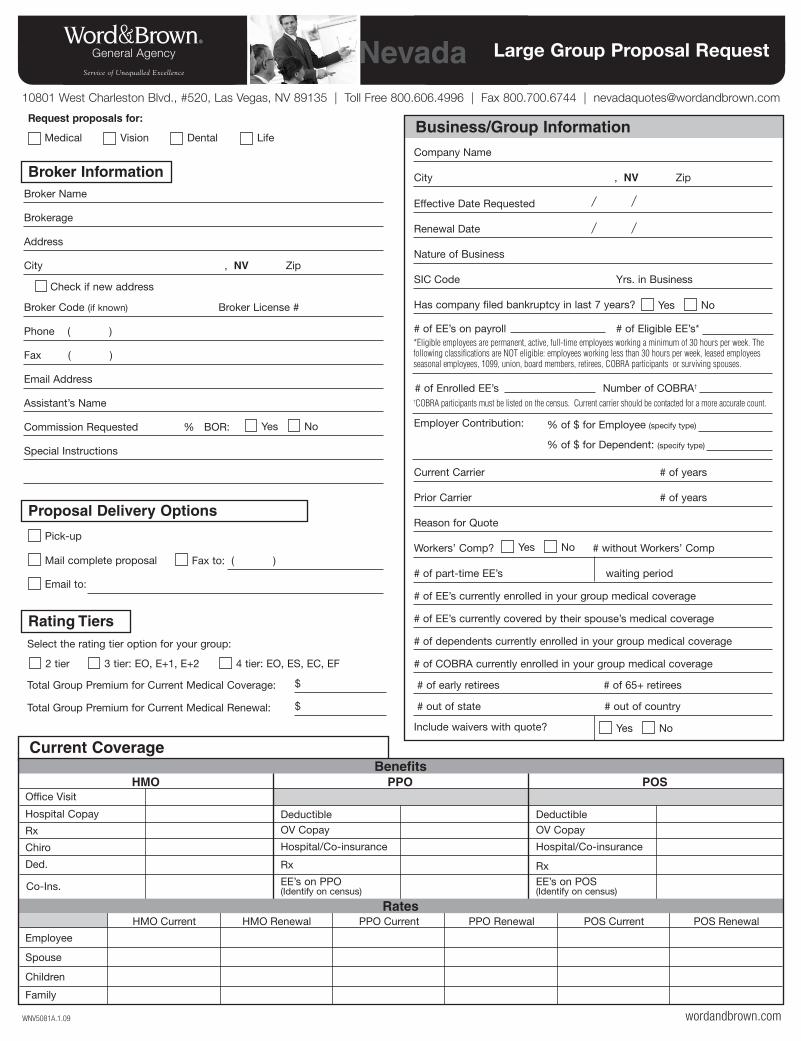
Benefits
wordandbrown.comWNV5081A.1.09
Current Coverage
Hospital Copay
Office Visit
Rx
Chiro
Employee
Spouse
Children
Family
Ded.
DeductibleOV Copay
Hospital/Co-insurance
Rx
EE’s on PPO (Identify on census)Co-Ins.
DeductibleOV Copay
Hospital/Co-insurance
RxEE’s on POS(Identify on census)
HMO Current HMO Renewal PPO Current PPO Renewal POS Current POS Renewal
HMO PPO POS
Rates
Large Group Proposal RequestNevada
Broker Code (if known) Broker License #
Phone ( )
Fax ( )
Email Address
Assistant’s Name
Commission Requested % BOR:
Special Instructions
Broker Name
Brokerage
Address
City , NV Zip
Check if new address
Pick-up
Mail complete proposal Fax to: ( )
Medical
Request proposals for:
Vision Dental Life
Email to:
Broker Information
Proposal Delivery Options
Select the rating tier option for your group:
Total Group Premium for Current Medical Coverage:
Total Group Premium for Current Medical Renewal:
2 tier 3 tier: EO, E+1, E+2
$
$
4 tier: EO, ES, EC, EF
Rating Tiers
Yes No
10801 West Charleston Blvd., #520, Las Vegas, NV 89135 | Toll Free 800.606.4996 | Fax 800.700.6744 | [email protected]
Business/Group Information
Effective Date Requested
Renewal Date
Nature of Business
SIC Code Yrs. in Business
Has company filed bankruptcy in last 7 years?
# of EE’s on payroll # of Eligible EE’s*
Employer Contribution:
Current Carrier # of years
Prior Carrier # of years
Reason for Quote
Workers’ Comp? # without Workers’ Comp
# of part-time EE’s waiting period
# of EE’s currently enrolled in your group medical coverage
# of EE’s currently covered by their spouse’s medical coverage
# of dependents currently enrolled in your group medical coverage
# of COBRA currently enrolled in your group medical coverage
# of early retirees # of 65+ retirees
# out of state # out of country
Company Name
City , NV Zip
Yes No
% of $ for Employee (specify type)
% of $ for Dependent: (specify type)
Include waivers with quote?
Yes No
Yes No
†COBRA participants must be listed on the census. Current carrier should be contacted for a more accurate count.
# of Enrolled EE’s Number of COBRA†
*Eligible employees are permanent, active, full-time employees working a minimum of 30 hours per week. Thefollowing classifications are NOT eligible: employees working less than 30 hours per week, leased employeesseasonal employees, 1099, union, board members, retirees, COBRA participants or surviving spouses.
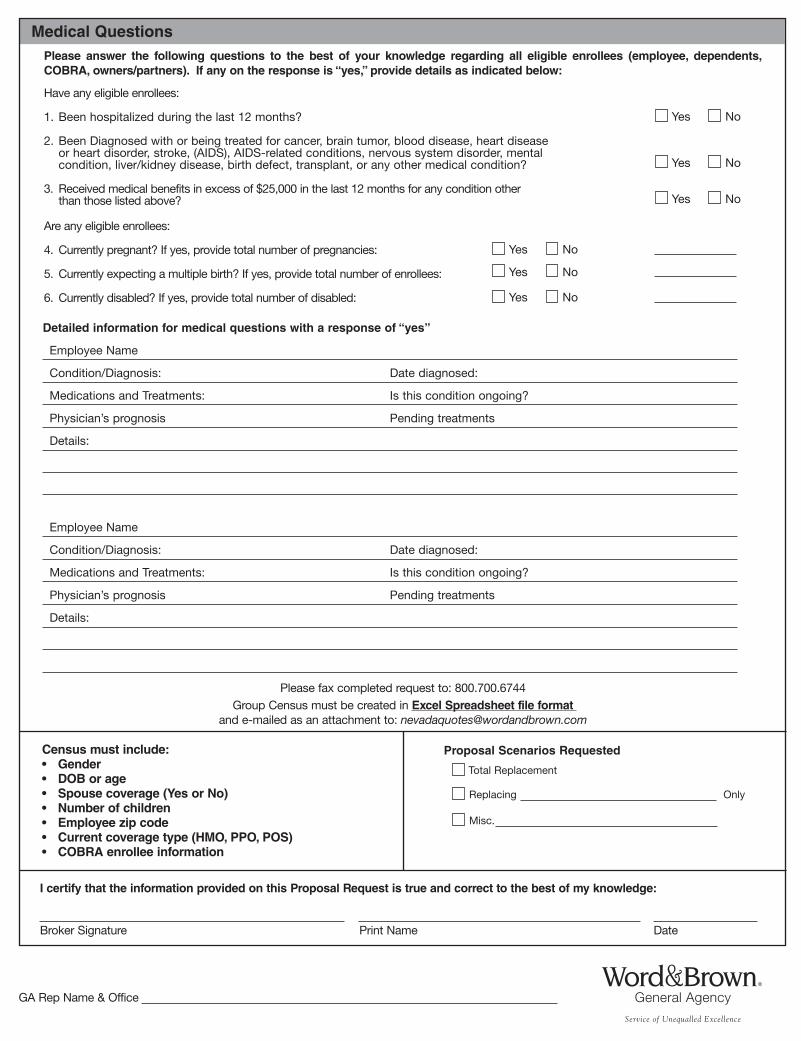
Detailed information for medical questions with a response of “yes”
Employee Name
Condition/Diagnosis: Date diagnosed:
Medications and Treatments: Is this condition ongoing?
Physician’s prognosis Pending treatments
Details:
Employee Name
Condition/Diagnosis: Date diagnosed:
Medications and Treatments: Is this condition ongoing?
Physician’s prognosis Pending treatments
Details:
Have any eligible enrollees:
1. Been hospitalized during the last 12 months?
2. Been Diagnosed with or being treated for cancer, brain tumor, blood disease, heart disease or heart disorder, stroke, (AIDS), AIDS-related conditions, nervous system disorder, mentalcondition, liver/kidney disease, birth defect, transplant, or any other medical condition?
3. Received medical benefits in excess of $25,000 in the last 12 months for any condition other than those listed above?
Are any eligible enrollees:
4. Currently pregnant? If yes, provide total number of pregnancies:
5. Currently expecting a multiple birth? If yes, provide total number of enrollees:
6. Currently disabled? If yes, provide total number of disabled:
Please answer the following questions to the best of your knowledge regarding all eligible enrollees (employee, dependents,COBRA, owners/partners). If any on the response is “yes,” provide details as indicated below:
Medical Questions
Yes No
Please fax completed request to: 800.700.6744Group Census must be created in Excel Spreadsheet file format
and e-mailed as an attachment to: [email protected]
I certify that the information provided on this Proposal Request is true and correct to the best of my knowledge:
Broker Signature Print Name Date
Yes No
Yes No
Yes No
Yes No
Yes No
Census must include:• Gender• DOB or age• Spouse coverage (Yes or No) • Number of children • Employee zip code • Current coverage type (HMO, PPO, POS)• COBRA enrollee information
Total Replacement
Replacing
Misc.
Proposal Scenarios Requested
Only
GA Rep Name & Office

Ever get the feeling new businessis passing you by?
FREE!
Stay organized
Fewer underwriting headaches
Get rates fastAgencyWow helps you track your progress with prospects and get quotes immediately to stay ahead of the competition. And with the new improved features you can:
• quicklybuildenrollmentformswithpre-filled employer and employee data
• trackcommissionsonacasebyanycarrier
• seeanyclientrecordfromanycomputerwithinternetaccess
• createe-blastsformarketingcampaignstosecuremoresales
With everything you have to do to manage your agency, who’sgottimetoworryaboutgettingnewbusiness?
Now there’s a way you can spend less time tracking and managing and more time doing what’s good for you – gettingnewcustomersandwritingnewbusiness.
AgencyWowisaWeb-basedagencymanagementsystemthatmanagesallyouractivitiesinoneeasy-to-useprogram. AgencyWowhelpsyoubuildyourbookofbusinessfromanycomputer-orphone–withinternetaccessbymakingiteasyto:
➤ Manage sales and agency activities
➤ Track appointments, contacts, prospects and commissions
➤ Produce quotes and solutions in minutes www.agencywow.com





























