Embed Size (px)
Citation preview

AFLACMEDICARE SUPPLEMENTYou lead a strong, active, healthy life …
Make sure a gap in your Medicare coverage
doesn’t slow you down.
NEW ME X ICO | 2012IC(10/12)A19MS75NM

AflAC MEdICArE SupplEMENt INSurANCEPolicy Series A19MS MSI
uNdErStANd INg thE fACtS CAN hElp yOu uNdErStANd Why Af lAC MEd ICArE SupplEMENt INSurANCE pOl IC IES MAkE SENSE fOr yOu.
60(SUPERIOR) by A.M. bEST.1 Of ThE WORld’S MOST EThIcAl
cOMPAnIES fOR ThE SIXTh yEAR.2
AflAc hAS nEARly 50
REcOgnIzEd In 2012 by EthisphErE MAgAzInE AS1
AflAc IS A fORTUnE 500 cOMPAny RATEd
yEARS Of PROvIdIng A STROng And lASTIng SAfETy nET fOR fAMIlIES.
MORE ThAn
MIllIOn PEOPlE WORldWIdE ARE InSUREd by AflAc.3
A+
Like most people, you’ve probably given some serious thought to planning for your retirement. And without a doubt, you have in mind some pretty specific ways of spending your time when you do retire. Whether it’s turning a hobby into a business or traveling the world, a wide-open road of possibilities lies ahead of you.
At Aflac, we want to make sure you have the right amount of health care coverage to keep you moving according to plan. That’s where the Aflac Medicare supplement insurance plans step in.
Aflac policies strengthen your overall coverage because they’ve been created to help pay for medical expenses not covered by Medicare, such as deductibles, copayments, and noncovered services.
With Aflac Medicare supplement insurance plans, you not only enhance your coverage, but you can also see any doctor who accepts Medicare—wherever and whenever you want.
We know you’ve spent a lot of time thinking about the future. We’re here to help make sure your plans stay on track.
Not connected with or endorsed by the U.S. government or the federal Medicare program. Aflac herein means American Family Life Assurance Company of Columbus. This is a solicitation of insurance and an agent may contact you.
1 Aflac’s A+ (Superior) rating for financial strength was affirmed by A.M. Best on May 27, 2011. The A+ rating is the second highest (of 16 levels) given by A.M. Best with the highest being A++ (Superior).2“World’s Most Ethical Companies,” Ethisphere magazine, Q1 2012 (quarterly).3Aflac annual report: 2011 Year in Review.
Aflac helps remove some of the guesswork about health care costs during your retirement.
MEdICArE pAySMEdICArE
SupplEMENt plANS pAy
plAN A
PlAn c
plAN d
PlAn f
plAN g
PlAn n
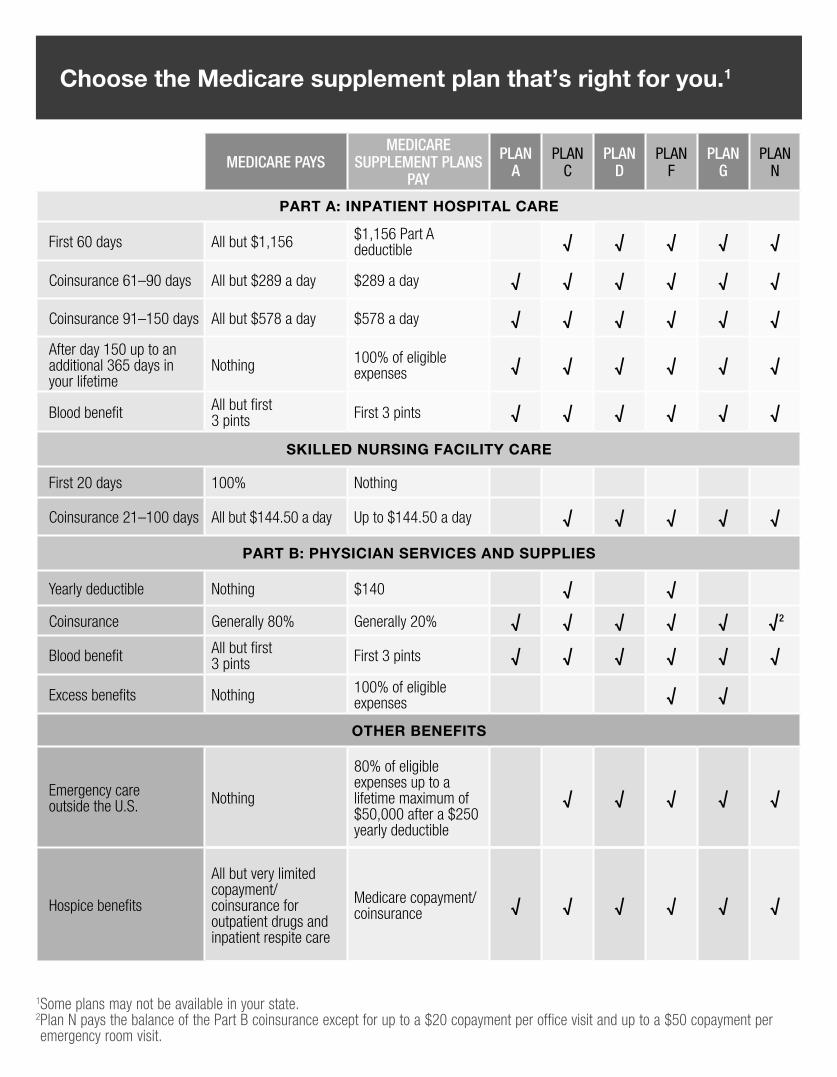
PArt A: InPAtIent HosPItAl CAre
First 60 days All but $1,156 $1,156 Part A deductible √ √ √ √ √
Coinsurance 61–90 days All but $289 a day $289 a day √ √ √ √ √ √
Coinsurance 91–150 days All but $578 a day $578 a day √ √ √ √ √ √
After day 150 up to an additional 365 days in your lifetime
Nothing 100% of eligible expenses √ √ √ √ √ √
Blood benefit All but first 3 pints First 3 pints √ √ √ √ √ √
skIlled nursIng FACIlIty CAre
First 20 days 100% Nothing
Coinsurance 21–100 days All but $144.50 a day Up to $144.50 a day √ √ √ √ √
PArt B: PHysICIAn servICes And suPPlIes
Yearly deductible Nothing $140 √ √
Coinsurance Generally 80% Generally 20% √ √ √ √ √ √2
Blood benefit All but first3 pints First 3 pints √ √ √ √ √ √
Excess benefits Nothing 100% of eligible expenses √ √
otHer BeneFIts
Emergency care outside the U.S. Nothing
80% of eligible expenses up to a lifetime maximum of $50,000 after a $250 yearly deductible
√ √ √ √ √
Hospice benefits
All but very limited copayment/coinsurance for outpatient drugs and inpatient respite care
Medicare copayment/coinsurance √ √ √ √ √ √
Choose the Medicare supplement plan that’s right for you.1
1Some plans may not be available in your state. 2 Plan N pays the balance of the Part B coinsurance except for up to a $20 copayment per office visit and up to a $50 copayment per emergency room visit.
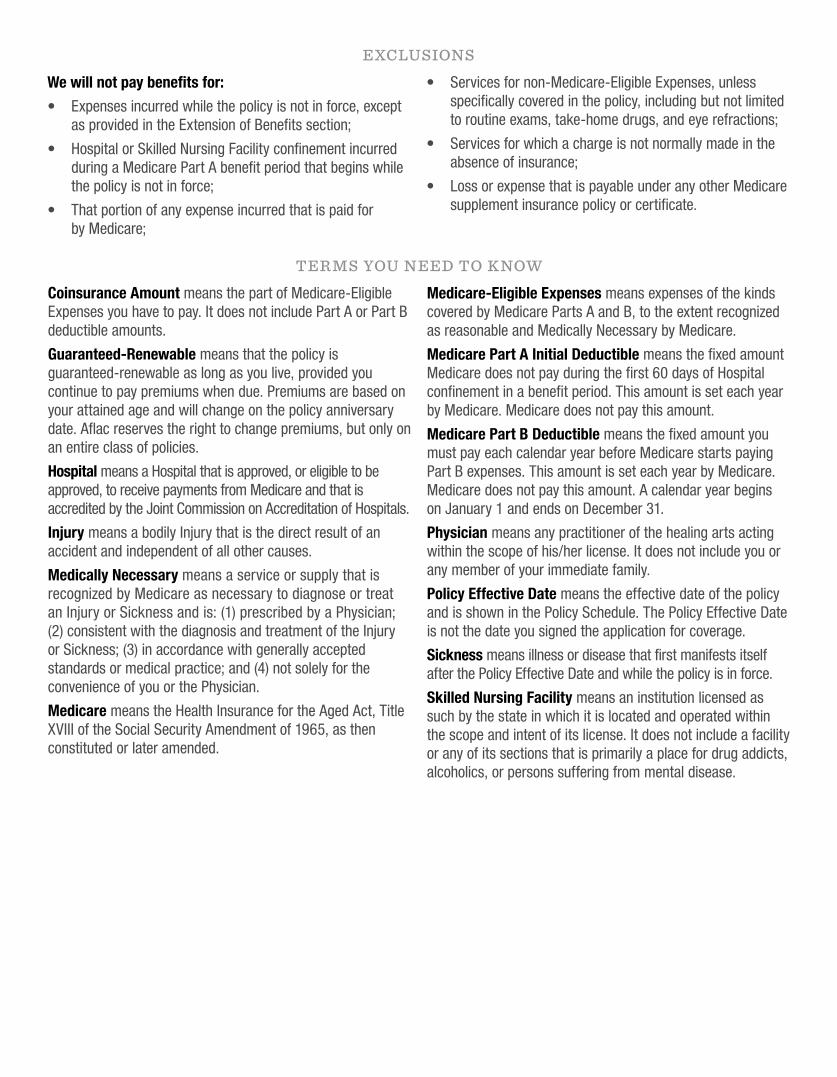
EXCLUSIONS
We will not pay benefits for:
• Expenses incurred while the policy is not in force, except as provided in the Extension of benefits section;
• hospital or Skilled nursing facility confinement incurred during a Medicare Part A benefit period that begins while the policy is not in force;
• That portion of any expense incurred that is paid for by Medicare;
• Services for non-Medicare-Eligible Expenses, unless specifically covered in the policy, including but not limited to routine exams, take-home drugs, and eye refractions;
• Services for which a charge is not normally made in the absence of insurance;
• loss or expense that is payable under any other Medicare supplement insurance policy or certificate.
TEr mS YOU NEEd TO KNOw
Coinsurance Amount means the part of Medicare-Eligible Expenses you have to pay. It does not include Part A or Part b deductible amounts.
Guaranteed-Renewable means that the policy is guaranteed-renewable as long as you live, provided you continue to pay premiums when due. Premiums are based on your attained age and will change on the policy anniversary date. Aflac reserves the right to change premiums, but only on an entire class of policies.
Hospital means a hospital that is approved, or eligible to be approved, to receive payments from Medicare and that is accredited by the Joint commission on Accreditation of hospitals.
Injury means a bodily Injury that is the direct result of an accident and independent of all other causes.
Medically Necessary means a service or supply that is recognized by Medicare as necessary to diagnose or treat an Injury or Sickness and is: (1) prescribed by a Physician; (2) consistent with the diagnosis and treatment of the Injury or Sickness; (3) in accordance with generally accepted standards or medical practice; and (4) not solely for the convenience of you or the Physician.
Medicare means the health Insurance for the Aged Act, Title XvIII of the Social Security Amendment of 1965, as then constituted or later amended.
Medicare-Eligible Expenses means expenses of the kinds covered by Medicare Parts A and b, to the extent recognized as reasonable and Medically necessary by Medicare.
Medicare Part A Initial Deductible means the fixed amount Medicare does not pay during the first 60 days of hospital confinement in a benefit period. This amount is set each year by Medicare. Medicare does not pay this amount.
Medicare Part B Deductible means the fixed amount you must pay each calendar year before Medicare starts paying Part b expenses. This amount is set each year by Medicare. Medicare does not pay this amount. A calendar year begins on January 1 and ends on december 31.
Physician means any practitioner of the healing arts acting within the scope of his/her license. It does not include you or any member of your immediate family.
Policy Effective Date means the effective date of the policy and is shown in the Policy Schedule. The Policy Effective date is not the date you signed the application for coverage.
Sickness means illness or disease that first manifests itself after the Policy Effective date and while the policy is in force.
Skilled Nursing Facility means an institution licensed as such by the state in which it is located and operated within the scope and intent of its license. It does not include a facility or any of its sections that is primarily a place for drug addicts, alcoholics, or persons suffering from mental disease.

ACOCRNM Page 1 of 24 ACOCRNM.1 Effective Date 09-28-2012
AMERICAN FAMILY LIFE ASSURANCE COMPANY OF COLUMBUS Outline of Medicare Supplement Coverage
Benefit Plans A, C, D, F, G and N Benefit Chart of Medicare Supplement Plans Sold for Effective Dates on or After June 1, 2010
This chart shows the benefits included in each of the standard Medicare supplement plans. Every company must make Plan “A” available. Some plans may not be available in your state. Basic Benefits:
Hospitalization – Part A coinsurance plus coverage for 365 additional days after Medicare benefits end. Medical Expenses – Part B coinsurance (generally 20% of Medicare-approved expenses) or copayments for hospital outpatient
services. Plans K, L, and N require insureds to pay a portion of Part B coinsurance or copayments. Blood – First three pints of blood each year. Hospice – Part A coinsurance
A B C D F F* G K L M N Basic, including 100% Part B coinsurance
Basic, including 100% Part B coinsurance
Basic, including 100% Part B coinsurance
Basic, including 100% Part B coinsurance
Basic, including 100% Part B coinsurance*
Basic, including 100% Part B coinsurance
Hospitalization and preventive care paid at 100%; other basic benefits paid at 50%
Hospitalization and preventive care paid at 100%; other basic benefits paid at 75%
Basic, including 100% Part B coinsurance
Basic, including 100 % Part B coinsurance except up to $20 copayment for office visit, and up to $50 copayment for ER
Skilled Nursing Facility Coinsurance
Skilled Nursing Facility Coinsurance
Skilled Nursing Facility Coinsurance
Skilled Nursing Facility Coinsurance
50% Skilled Nursing Facility Coinsurance
75% Skilled Nursing Facility Coinsurance
Skilled Nursing Facility Coinsurance
Skilled Nursing Facility Coinsurance
Part A Deductible
Part A Deductible
Part A Deductible
Part A Deductible
Part A Deductible
50% Part A Deductible
75% Part A Deductible
50% Part A Deductible
Part A Deductible
Part B Deductible
Part B Deductible
Part B Excess (100 %)
Part B Excess (100%)
Foreign Travel Emergency
Foreign Travel Emergency
Foreign Travel Emergency
Foreign Travel Emergency
Foreign Travel Emergency
Foreign Travel Emergency
Out- of-pocket limit $4660 paid at 100% after limit reached
Out-of -Pocket limit $2330 paid at 100% after limit reached
*Plan F also has an option called a high deductible Plan F. This high deductible plan pays the same benefits as Plan F after one has paid a calendar year $2070 deductible. Benefits from high deductible plan F will not begin until out-of-pocket expenses exceed $2070. Out-of-pocket expenses for this deductible are expenses that would ordinarily be paid by the Policy. These expenses include the Medicare deductibles for Part A and Part B, but do not include the plan’s separate foreign travel emergency deductible.

ACOCRNM Page 2 of 24 ACOCRNM.1 Effective: 09-28-2012
American Family Life Assurance Company of Columbus (Aflac) State of New Mexico
Plan A
Attained Age
Non-Tobacco User Tobacco User
Female Male Female Male
0-64 N/A N/A N/A N/A
65 1,244.88 1,408.68 1,431.60 1,620.00
66 1,288.56 1,452.36 1,481.88 1,670.16
67 1,332.24 1,496.04 1,532.04 1,720.44
68 1,375.92 1,550.64 1,582.32 1,783.20
69 1,419.60 1,594.32 1,632.48 1,833.48
70 1,474.20 1,648.92 1,695.36 1,896.24
71 1,488.24 1,670.28 1,711.44 1,920.84
72 1,528.92 1,720.08 1,758.24 1,978.08
73 1,565.76 1,754.88 1,800.60 2,018.16
74 1,603.08 1,800.84 1,843.44 2,070.96
75 1,630.44 1,826.52 1,875.00 2,100.48
76 1,634.76 1,837.80 1,879.92 2,113.44
77 1,641.60 1,851.84 1,887.84 2,129.64
78 1,671.60 1,881.84 1,922.40 2,164.08
79 1,691.64 1,901.88 1,945.44 2,187.12
80 1,711.68 1,921.92 1,968.48 2,210.16
81 1,721.64 1,941.96 1,980.00 2,233.20
82 1,731.72 1,941.96 1,991.52 2,233.20
83 1,731.72 1,941.96 1,991.52 2,233.20
84 1,731.72 1,941.96 1,991.52 2,233.20
85 1,731.72 1,951.92 1,991.52 2,244.72
86 1,731.72 1,951.92 1,991.52 2,244.72
87 1,731.72 1,951.92 1,991.52 2,244.72
88 1,731.72 1,951.92 1,991.52 2,244.72
89 1,731.72 1,951.92 1,991.52 2,244.72
90 1,731.72 1,951.92 1,991.52 2,244.72
91 1,731.72 1,951.92 1,991.52 2,244.72
92 1,731.72 1,951.92 1,991.52 2,244.72
93 1,731.72 1,951.92 1,991.52 2,244.72
94 1,731.72 1,951.92 1,991.52 2,244.72
95 1,731.72 1,951.92 1,991.52 2,244.72
96 1,731.72 1,951.92 1,991.52 2,244.72
97 1,731.72 1,951.92 1,991.52 2,244.72
98 1,731.72 1,951.92 1,991.52 2,244.72
99 1,731.72 1,951.92 1,991.52 2,244.72
1. The above rates do not include a one-time $20 policy fee at time of issue.
2. If the insured qualifies for household discount, the 7% discount will be applied. 3. For payment made on monthly EBT, there is an additional $2 discount per month.
Area Factors
Modal Factors
3-Digit Zip Code Factor
Mode Factor 871 0.91
Annual 1.00000
870, 872-885 0.82
Semi-Annual 0.50000 Rest of State 0.91
Quarterly 0.25000
Monthly 0.08333
ACOCRNM Page 3 of 24 ACOCRNM.1 Effective: 09-28-2012
American Family Life Assurance Company of Columbus (Aflac)
State of New Mexico Plan C
Attained Age
Non-Tobacco User Tobacco User
Female Male Female Male
0-64 N/A N/A N/A N/A
65 1,501.92 1,683.00 1,727.16 1,935.48
66 1,555.20 1,746.96 1,788.48 2,008.92
67 1,619.04 1,821.48 1,861.92 2,094.72
68 1,683.00 1,885.44 1,935.48 2,168.16
69 1,746.96 1,959.96 2,008.92 2,253.96
70 1,810.80 2,034.48 2,082.48 2,339.76
71 1,848.60 2,078.40 2,125.92 2,390.16
72 1,905.72 2,143.92 2,191.56 2,465.52
73 1,968.12 2,214.12 2,263.32 2,546.28
74 2,030.76 2,274.48 2,335.44 2,615.64
75 2,083.68 2,345.40 2,396.28 2,697.24
76 2,119.56 2,377.08 2,437.44 2,733.60
77 2,157.96 2,421.60 2,481.60 2,784.72
78 2,216.52 2,489.88 2,548.92 2,863.32
79 2,284.80 2,568.00 2,627.52 2,953.20
80 2,343.48 2,636.40 2,694.96 3,031.80
81 2,411.76 2,704.68 2,773.56 3,110.40
82 2,470.32 2,773.08 2,840.88 3,189.00
83 2,529.00 2,841.36 2,908.32 3,267.60
84 2,587.56 2,909.76 2,975.64 3,346.20
85 2,636.40 2,968.32 3,031.80 3,413.64
86 2,694.84 3,037.08 3,099.00 3,492.72
87 2,753.28 3,105.84 3,166.32 3,571.80
88 2,792.88 3,146.76 3,211.80 3,618.84
89 2,831.40 3,186.60 3,256.08 3,664.56
90 2,868.84 3,225.12 3,299.16 3,708.96
91 2,905.08 3,262.32 3,340.80 3,751.68
92 2,939.76 3,297.84 3,380.76 3,792.60
93 2,972.16 3,331.08 3,417.96 3,830.76
94 3,002.88 3,362.40 3,453.24 3,866.76
95 3,031.68 3,391.68 3,486.48 3,900.48
96 3,058.68 3,418.92 3,517.44 3,931.80
97 3,083.64 3,444.12 3,546.24 3,960.72
98 3,106.56 3,466.92 3,572.52 3,986.88
99 3,127.20 3,487.44 3,596.28 4,010.52
1. The above rates do not include a one-time $20 policy fee at time of issue.
2. If the insured qualifies for household discount, the 7% discount will be applied. 3. For payment made on monthly EBT, there is an additional $2 discount per month.
Area Factors
Modal Factors 3-Digit Zip Code Factor
Mode Factor
871 0.91
Annual 1.00000 870, 872-885 0.82
Semi-Annual 0.50000
Rest of State 0.91
Quarterly 0.25000
Monthly 0.08333
ACOCRNM Page 2 of 24 ACOCRNM.1 Effective: 09-28-2012
American Family Life Assurance Company of Columbus (Aflac) State of New Mexico
Plan A
Attained Age
Non-Tobacco User Tobacco User
Female Male Female Male
0-64 N/A N/A N/A N/A
65 1,244.88 1,408.68 1,431.60 1,620.00
66 1,288.56 1,452.36 1,481.88 1,670.16
67 1,332.24 1,496.04 1,532.04 1,720.44
68 1,375.92 1,550.64 1,582.32 1,783.20
69 1,419.60 1,594.32 1,632.48 1,833.48
70 1,474.20 1,648.92 1,695.36 1,896.24
71 1,488.24 1,670.28 1,711.44 1,920.84
72 1,528.92 1,720.08 1,758.24 1,978.08
73 1,565.76 1,754.88 1,800.60 2,018.16
74 1,603.08 1,800.84 1,843.44 2,070.96
75 1,630.44 1,826.52 1,875.00 2,100.48
76 1,634.76 1,837.80 1,879.92 2,113.44
77 1,641.60 1,851.84 1,887.84 2,129.64
78 1,671.60 1,881.84 1,922.40 2,164.08
79 1,691.64 1,901.88 1,945.44 2,187.12
80 1,711.68 1,921.92 1,968.48 2,210.16
81 1,721.64 1,941.96 1,980.00 2,233.20
82 1,731.72 1,941.96 1,991.52 2,233.20
83 1,731.72 1,941.96 1,991.52 2,233.20
84 1,731.72 1,941.96 1,991.52 2,233.20
85 1,731.72 1,951.92 1,991.52 2,244.72
86 1,731.72 1,951.92 1,991.52 2,244.72
87 1,731.72 1,951.92 1,991.52 2,244.72
88 1,731.72 1,951.92 1,991.52 2,244.72
89 1,731.72 1,951.92 1,991.52 2,244.72
90 1,731.72 1,951.92 1,991.52 2,244.72
91 1,731.72 1,951.92 1,991.52 2,244.72
92 1,731.72 1,951.92 1,991.52 2,244.72
93 1,731.72 1,951.92 1,991.52 2,244.72
94 1,731.72 1,951.92 1,991.52 2,244.72
95 1,731.72 1,951.92 1,991.52 2,244.72
96 1,731.72 1,951.92 1,991.52 2,244.72
97 1,731.72 1,951.92 1,991.52 2,244.72
98 1,731.72 1,951.92 1,991.52 2,244.72
99 1,731.72 1,951.92 1,991.52 2,244.72
1. The above rates do not include a one-time $20 policy fee at time of issue.
2. If the insured qualifies for household discount, the 7% discount will be applied. 3. For payment made on monthly EBT, there is an additional $2 discount per month.
Area Factors
Modal Factors
3-Digit Zip Code Factor
Mode Factor 871 0.91
Annual 1.00000
870, 872-885 0.82
Semi-Annual 0.50000 Rest of State 0.91
Quarterly 0.25000
Monthly 0.08333

ACOCRNM Page 2 of 24 ACOCRNM.1 Effective: 09-28-2012
American Family Life Assurance Company of Columbus (Aflac) State of New Mexico
Plan A
Attained Age
Non-Tobacco User Tobacco User
Female Male Female Male
0-64 N/A N/A N/A N/A
65 1,244.88 1,408.68 1,431.60 1,620.00
66 1,288.56 1,452.36 1,481.88 1,670.16
67 1,332.24 1,496.04 1,532.04 1,720.44
68 1,375.92 1,550.64 1,582.32 1,783.20
69 1,419.60 1,594.32 1,632.48 1,833.48
70 1,474.20 1,648.92 1,695.36 1,896.24
71 1,488.24 1,670.28 1,711.44 1,920.84
72 1,528.92 1,720.08 1,758.24 1,978.08
73 1,565.76 1,754.88 1,800.60 2,018.16
74 1,603.08 1,800.84 1,843.44 2,070.96
75 1,630.44 1,826.52 1,875.00 2,100.48
76 1,634.76 1,837.80 1,879.92 2,113.44
77 1,641.60 1,851.84 1,887.84 2,129.64
78 1,671.60 1,881.84 1,922.40 2,164.08
79 1,691.64 1,901.88 1,945.44 2,187.12
80 1,711.68 1,921.92 1,968.48 2,210.16
81 1,721.64 1,941.96 1,980.00 2,233.20
82 1,731.72 1,941.96 1,991.52 2,233.20
83 1,731.72 1,941.96 1,991.52 2,233.20
84 1,731.72 1,941.96 1,991.52 2,233.20
85 1,731.72 1,951.92 1,991.52 2,244.72
86 1,731.72 1,951.92 1,991.52 2,244.72
87 1,731.72 1,951.92 1,991.52 2,244.72
88 1,731.72 1,951.92 1,991.52 2,244.72
89 1,731.72 1,951.92 1,991.52 2,244.72
90 1,731.72 1,951.92 1,991.52 2,244.72
91 1,731.72 1,951.92 1,991.52 2,244.72
92 1,731.72 1,951.92 1,991.52 2,244.72
93 1,731.72 1,951.92 1,991.52 2,244.72
94 1,731.72 1,951.92 1,991.52 2,244.72
95 1,731.72 1,951.92 1,991.52 2,244.72
96 1,731.72 1,951.92 1,991.52 2,244.72
97 1,731.72 1,951.92 1,991.52 2,244.72
98 1,731.72 1,951.92 1,991.52 2,244.72
99 1,731.72 1,951.92 1,991.52 2,244.72
1. The above rates do not include a one-time $20 policy fee at time of issue.
2. If the insured qualifies for household discount, the 7% discount will be applied. 3. For payment made on monthly EBT, there is an additional $2 discount per month.
Area Factors
Modal Factors
3-Digit Zip Code Factor
Mode Factor 871 0.91
Annual 1.00000
870, 872-885 0.82
Semi-Annual 0.50000 Rest of State 0.91
Quarterly 0.25000
Monthly 0.08333
ACOCRNM Page 3 of 24 ACOCRNM.1 Effective: 09-28-2012
American Family Life Assurance Company of Columbus (Aflac)
State of New Mexico Plan C
Attained Age
Non-Tobacco User Tobacco User
Female Male Female Male
0-64 N/A N/A N/A N/A
65 1,501.92 1,683.00 1,727.16 1,935.48
66 1,555.20 1,746.96 1,788.48 2,008.92
67 1,619.04 1,821.48 1,861.92 2,094.72
68 1,683.00 1,885.44 1,935.48 2,168.16
69 1,746.96 1,959.96 2,008.92 2,253.96
70 1,810.80 2,034.48 2,082.48 2,339.76
71 1,848.60 2,078.40 2,125.92 2,390.16
72 1,905.72 2,143.92 2,191.56 2,465.52
73 1,968.12 2,214.12 2,263.32 2,546.28
74 2,030.76 2,274.48 2,335.44 2,615.64
75 2,083.68 2,345.40 2,396.28 2,697.24
76 2,119.56 2,377.08 2,437.44 2,733.60
77 2,157.96 2,421.60 2,481.60 2,784.72
78 2,216.52 2,489.88 2,548.92 2,863.32
79 2,284.80 2,568.00 2,627.52 2,953.20
80 2,343.48 2,636.40 2,694.96 3,031.80
81 2,411.76 2,704.68 2,773.56 3,110.40
82 2,470.32 2,773.08 2,840.88 3,189.00
83 2,529.00 2,841.36 2,908.32 3,267.60
84 2,587.56 2,909.76 2,975.64 3,346.20
85 2,636.40 2,968.32 3,031.80 3,413.64
86 2,694.84 3,037.08 3,099.00 3,492.72
87 2,753.28 3,105.84 3,166.32 3,571.80
88 2,792.88 3,146.76 3,211.80 3,618.84
89 2,831.40 3,186.60 3,256.08 3,664.56
90 2,868.84 3,225.12 3,299.16 3,708.96
91 2,905.08 3,262.32 3,340.80 3,751.68
92 2,939.76 3,297.84 3,380.76 3,792.60
93 2,972.16 3,331.08 3,417.96 3,830.76
94 3,002.88 3,362.40 3,453.24 3,866.76
95 3,031.68 3,391.68 3,486.48 3,900.48
96 3,058.68 3,418.92 3,517.44 3,931.80
97 3,083.64 3,444.12 3,546.24 3,960.72
98 3,106.56 3,466.92 3,572.52 3,986.88
99 3,127.20 3,487.44 3,596.28 4,010.52
1. The above rates do not include a one-time $20 policy fee at time of issue.
2. If the insured qualifies for household discount, the 7% discount will be applied. 3. For payment made on monthly EBT, there is an additional $2 discount per month.
Area Factors
Modal Factors 3-Digit Zip Code Factor
Mode Factor
871 0.91
Annual 1.00000 870, 872-885 0.82
Semi-Annual 0.50000
Rest of State 0.91
Quarterly 0.25000
Monthly 0.08333
ACOCRNM Page 2 of 24 ACOCRNM.1 Effective: 09-28-2012
American Family Life Assurance Company of Columbus (Aflac) State of New Mexico
Plan A
Attained Age
Non-Tobacco User Tobacco User
Female Male Female Male
0-64 N/A N/A N/A N/A
65 1,244.88 1,408.68 1,431.60 1,620.00
66 1,288.56 1,452.36 1,481.88 1,670.16
67 1,332.24 1,496.04 1,532.04 1,720.44
68 1,375.92 1,550.64 1,582.32 1,783.20
69 1,419.60 1,594.32 1,632.48 1,833.48
70 1,474.20 1,648.92 1,695.36 1,896.24
71 1,488.24 1,670.28 1,711.44 1,920.84
72 1,528.92 1,720.08 1,758.24 1,978.08
73 1,565.76 1,754.88 1,800.60 2,018.16
74 1,603.08 1,800.84 1,843.44 2,070.96
75 1,630.44 1,826.52 1,875.00 2,100.48
76 1,634.76 1,837.80 1,879.92 2,113.44
77 1,641.60 1,851.84 1,887.84 2,129.64
78 1,671.60 1,881.84 1,922.40 2,164.08
79 1,691.64 1,901.88 1,945.44 2,187.12
80 1,711.68 1,921.92 1,968.48 2,210.16
81 1,721.64 1,941.96 1,980.00 2,233.20
82 1,731.72 1,941.96 1,991.52 2,233.20
83 1,731.72 1,941.96 1,991.52 2,233.20
84 1,731.72 1,941.96 1,991.52 2,233.20
85 1,731.72 1,951.92 1,991.52 2,244.72
86 1,731.72 1,951.92 1,991.52 2,244.72
87 1,731.72 1,951.92 1,991.52 2,244.72
88 1,731.72 1,951.92 1,991.52 2,244.72
89 1,731.72 1,951.92 1,991.52 2,244.72
90 1,731.72 1,951.92 1,991.52 2,244.72
91 1,731.72 1,951.92 1,991.52 2,244.72
92 1,731.72 1,951.92 1,991.52 2,244.72
93 1,731.72 1,951.92 1,991.52 2,244.72
94 1,731.72 1,951.92 1,991.52 2,244.72
95 1,731.72 1,951.92 1,991.52 2,244.72
96 1,731.72 1,951.92 1,991.52 2,244.72
97 1,731.72 1,951.92 1,991.52 2,244.72
98 1,731.72 1,951.92 1,991.52 2,244.72
99 1,731.72 1,951.92 1,991.52 2,244.72
1. The above rates do not include a one-time $20 policy fee at time of issue.
2. If the insured qualifies for household discount, the 7% discount will be applied. 3. For payment made on monthly EBT, there is an additional $2 discount per month.
Area Factors
Modal Factors
3-Digit Zip Code Factor
Mode Factor 871 0.91
Annual 1.00000
870, 872-885 0.82
Semi-Annual 0.50000 Rest of State 0.91
Quarterly 0.25000
Monthly 0.08333

ACOCRNM Page 4 of 24 ACOCRNM.1 Effective: 09-28-2012
American Family Life Assurance Company of Columbus (Aflac)
State of New Mexico Plan D
Attained Age
Non-Tobacco User Tobacco User
Female Male Female Male
0-64 N/A N/A N/A N/A
65 1,353.00 1,514.04 1,555.92 1,741.08
66 1,395.84 1,578.48 1,605.24 1,815.24
67 1,449.60 1,632.12 1,667.04 1,876.92
68 1,514.04 1,696.56 1,741.08 1,951.08
69 1,567.68 1,761.00 1,802.88 2,025.12
70 1,632.12 1,825.44 1,876.92 2,099.16
71 1,663.44 1,874.04 1,912.92 2,155.08
72 1,722.72 1,931.52 1,981.08 2,221.20
73 1,777.32 1,994.28 2,043.84 2,293.44
74 1,832.16 2,057.40 2,106.96 2,365.92
75 1,887.36 2,120.76 2,170.44 2,438.88
76 1,916.88 2,156.52 2,204.52 2,480.04
77 1,958.76 2,194.92 2,252.52 2,524.20
78 2,017.80 2,263.80 2,320.44 2,603.40
79 2,076.84 2,332.80 2,388.36 2,682.72
80 2,135.88 2,401.68 2,456.28 2,761.92
81 2,194.92 2,470.56 2,524.20 2,841.12
82 2,263.80 2,539.44 2,603.40 2,920.32
83 2,322.96 2,608.32 2,671.32 2,999.64
84 2,382.00 2,677.20 2,739.24 3,078.84
85 2,431.20 2,736.36 2,795.88 3,146.76
86 2,492.64 2,806.44 2,866.44 3,227.40
87 2,553.96 2,876.52 2,937.12 3,307.92
88 2,593.32 2,917.32 2,982.36 3,354.96
89 2,631.60 2,957.16 3,026.40 3,400.80
90 2,668.92 2,995.68 3,069.24 3,445.08
91 2,704.80 3,032.88 3,110.52 3,487.80
92 2,739.36 3,068.40 3,150.36 3,528.72
93 2,771.52 3,101.64 3,187.32 3,566.88
94 2,802.00 3,132.96 3,222.36 3,602.88
95 2,830.80 3,162.24 3,255.36 3,636.60
96 2,857.56 3,189.48 3,286.20 3,667.92
97 2,882.40 3,214.56 3,314.76 3,696.72
98 2,905.08 3,237.36 3,340.92 3,723.00
99 2,925.72 3,257.88 3,364.56 3,746.64
1. The above rates do not include a one-time $20 policy fee at time of issue.
2. If the insured qualifies for household discount, the 7% discount will be applied. 3. For payment made on monthly EBT, there is an additional $2 discount per month.
Area Factors
Modal Factors 3-Digit Zip Code Factor
Mode Factor
871 0.91
Annual 1.00000 870, 872-885 0.82
Semi-Annual 0.50000
Rest of State 0.91
Quarterly 0.25000
Monthly 0.08333
ACOCRNM Page 5 of 24 ACOCRNM.1 Effective: 09-28-2012
American Family Life Assurance Company of Columbus (Aflac)
State of New Mexico Plan F
Attained Age
Non-Tobacco User Tobacco User
Female Male Female Male
0-64 N/A N/A N/A N/A
65 1,534.56 1,726.44 1,764.72 1,985.40
66 1,598.52 1,790.28 1,838.28 2,058.84
67 1,651.80 1,864.92 1,899.60 2,144.64
68 1,715.76 1,928.88 1,973.04 2,218.20
69 1,779.72 2,003.40 2,046.60 2,304.00
70 1,854.24 2,078.04 2,132.40 2,389.80
71 1,891.20 2,121.12 2,174.88 2,439.24
72 1,958.40 2,196.72 2,252.16 2,526.24
73 2,010.00 2,266.32 2,311.44 2,606.28
74 2,072.28 2,336.40 2,383.20 2,686.92
75 2,134.92 2,396.76 2,455.20 2,756.28
76 2,169.96 2,437.56 2,495.52 2,803.20
77 2,207.76 2,481.24 2,538.84 2,853.36
78 2,276.04 2,549.64 2,617.56 2,932.08
79 2,334.72 2,627.76 2,684.88 3,021.96
80 2,403.12 2,696.16 2,763.60 3,100.56
81 2,461.68 2,764.56 2,830.92 3,179.16
82 2,520.36 2,832.96 2,898.36 3,257.88
83 2,588.64 2,901.24 2,976.96 3,336.48
84 2,647.32 2,969.64 3,044.40 3,415.08
85 2,696.16 3,038.04 3,100.56 3,493.80
86 2,755.80 3,108.24 3,169.08 3,574.56
87 2,815.44 3,178.56 3,237.72 3,655.32
88 2,855.76 3,220.32 3,284.16 3,703.32
89 2,895.12 3,261.00 3,329.40 3,750.12
90 2,933.28 3,300.36 3,373.32 3,795.48
91 2,970.24 3,338.40 3,415.80 3,839.16
92 3,005.76 3,374.76 3,456.60 3,880.92
93 3,038.76 3,408.60 3,494.64 3,919.92
94 3,070.08 3,440.64 3,530.64 3,956.64
95 3,099.60 3,470.52 3,564.48 3,991.20
96 3,127.08 3,498.48 3,596.16 4,023.24
97 3,152.52 3,524.04 3,625.44 4,052.64
98 3,175.92 3,547.44 3,652.32 4,079.52
99 3,197.04 3,568.32 3,676.56 4,103.64
1. The above rates do not include a one-time $20 policy fee at time of issue.
2. If the insured qualifies for household discount, the 7% discount will be applied. 3. For payment made on monthly EBT, there is an additional $2 discount per month.
Area Factors
Modal Factors 3-Digit Zip Code Factor
Mode Factor
871 0.91
Annual 1.00000 870, 872-885 0.82
Semi-Annual 0.50000
Rest of State 0.91
Quarterly 0.25000
Monthly 0.08333

ACOCRNM Page 4 of 24 ACOCRNM.1 Effective: 09-28-2012
American Family Life Assurance Company of Columbus (Aflac)
State of New Mexico Plan D
Attained Age
Non-Tobacco User Tobacco User
Female Male Female Male
0-64 N/A N/A N/A N/A
65 1,353.00 1,514.04 1,555.92 1,741.08
66 1,395.84 1,578.48 1,605.24 1,815.24
67 1,449.60 1,632.12 1,667.04 1,876.92
68 1,514.04 1,696.56 1,741.08 1,951.08
69 1,567.68 1,761.00 1,802.88 2,025.12
70 1,632.12 1,825.44 1,876.92 2,099.16
71 1,663.44 1,874.04 1,912.92 2,155.08
72 1,722.72 1,931.52 1,981.08 2,221.20
73 1,777.32 1,994.28 2,043.84 2,293.44
74 1,832.16 2,057.40 2,106.96 2,365.92
75 1,887.36 2,120.76 2,170.44 2,438.88
76 1,916.88 2,156.52 2,204.52 2,480.04
77 1,958.76 2,194.92 2,252.52 2,524.20
78 2,017.80 2,263.80 2,320.44 2,603.40
79 2,076.84 2,332.80 2,388.36 2,682.72
80 2,135.88 2,401.68 2,456.28 2,761.92
81 2,194.92 2,470.56 2,524.20 2,841.12
82 2,263.80 2,539.44 2,603.40 2,920.32
83 2,322.96 2,608.32 2,671.32 2,999.64
84 2,382.00 2,677.20 2,739.24 3,078.84
85 2,431.20 2,736.36 2,795.88 3,146.76
86 2,492.64 2,806.44 2,866.44 3,227.40
87 2,553.96 2,876.52 2,937.12 3,307.92
88 2,593.32 2,917.32 2,982.36 3,354.96
89 2,631.60 2,957.16 3,026.40 3,400.80
90 2,668.92 2,995.68 3,069.24 3,445.08
91 2,704.80 3,032.88 3,110.52 3,487.80
92 2,739.36 3,068.40 3,150.36 3,528.72
93 2,771.52 3,101.64 3,187.32 3,566.88
94 2,802.00 3,132.96 3,222.36 3,602.88
95 2,830.80 3,162.24 3,255.36 3,636.60
96 2,857.56 3,189.48 3,286.20 3,667.92
97 2,882.40 3,214.56 3,314.76 3,696.72
98 2,905.08 3,237.36 3,340.92 3,723.00
99 2,925.72 3,257.88 3,364.56 3,746.64
1. The above rates do not include a one-time $20 policy fee at time of issue.
2. If the insured qualifies for household discount, the 7% discount will be applied. 3. For payment made on monthly EBT, there is an additional $2 discount per month.
Area Factors
Modal Factors 3-Digit Zip Code Factor
Mode Factor
871 0.91
Annual 1.00000 870, 872-885 0.82
Semi-Annual 0.50000
Rest of State 0.91
Quarterly 0.25000
Monthly 0.08333
ACOCRNM Page 5 of 24 ACOCRNM.1 Effective: 09-28-2012
American Family Life Assurance Company of Columbus (Aflac)
State of New Mexico Plan F
Attained Age
Non-Tobacco User Tobacco User
Female Male Female Male
0-64 N/A N/A N/A N/A
65 1,534.56 1,726.44 1,764.72 1,985.40
66 1,598.52 1,790.28 1,838.28 2,058.84
67 1,651.80 1,864.92 1,899.60 2,144.64
68 1,715.76 1,928.88 1,973.04 2,218.20
69 1,779.72 2,003.40 2,046.60 2,304.00
70 1,854.24 2,078.04 2,132.40 2,389.80
71 1,891.20 2,121.12 2,174.88 2,439.24
72 1,958.40 2,196.72 2,252.16 2,526.24
73 2,010.00 2,266.32 2,311.44 2,606.28
74 2,072.28 2,336.40 2,383.20 2,686.92
75 2,134.92 2,396.76 2,455.20 2,756.28
76 2,169.96 2,437.56 2,495.52 2,803.20
77 2,207.76 2,481.24 2,538.84 2,853.36
78 2,276.04 2,549.64 2,617.56 2,932.08
79 2,334.72 2,627.76 2,684.88 3,021.96
80 2,403.12 2,696.16 2,763.60 3,100.56
81 2,461.68 2,764.56 2,830.92 3,179.16
82 2,520.36 2,832.96 2,898.36 3,257.88
83 2,588.64 2,901.24 2,976.96 3,336.48
84 2,647.32 2,969.64 3,044.40 3,415.08
85 2,696.16 3,038.04 3,100.56 3,493.80
86 2,755.80 3,108.24 3,169.08 3,574.56
87 2,815.44 3,178.56 3,237.72 3,655.32
88 2,855.76 3,220.32 3,284.16 3,703.32
89 2,895.12 3,261.00 3,329.40 3,750.12
90 2,933.28 3,300.36 3,373.32 3,795.48
91 2,970.24 3,338.40 3,415.80 3,839.16
92 3,005.76 3,374.76 3,456.60 3,880.92
93 3,038.76 3,408.60 3,494.64 3,919.92
94 3,070.08 3,440.64 3,530.64 3,956.64
95 3,099.60 3,470.52 3,564.48 3,991.20
96 3,127.08 3,498.48 3,596.16 4,023.24
97 3,152.52 3,524.04 3,625.44 4,052.64
98 3,175.92 3,547.44 3,652.32 4,079.52
99 3,197.04 3,568.32 3,676.56 4,103.64
1. The above rates do not include a one-time $20 policy fee at time of issue.
2. If the insured qualifies for household discount, the 7% discount will be applied. 3. For payment made on monthly EBT, there is an additional $2 discount per month.
Area Factors
Modal Factors 3-Digit Zip Code Factor
Mode Factor
871 0.91
Annual 1.00000 870, 872-885 0.82
Semi-Annual 0.50000
Rest of State 0.91
Quarterly 0.25000
Monthly 0.08333

ACOCRNM Page 6 of 24 ACOCRNM.1 Effective: 09-28-2012
American Family Life Assurance Company of Columbus (Aflac)
State of New Mexico Plan G
Attained Age
Non-Tobacco User Tobacco User
Female Male Female Male
0-64 N/A N/A N/A N/A
65 1,375.08 1,546.92 1,581.36 1,779.00
66 1,428.72 1,611.36 1,643.04 1,853.16
67 1,493.28 1,675.92 1,717.20 1,927.20
68 1,546.92 1,740.36 1,779.00 2,001.36
69 1,600.68 1,804.80 1,840.80 2,075.52
70 1,665.12 1,869.24 1,914.84 2,149.56
71 1,706.40 1,917.00 1,962.36 2,204.64
72 1,765.32 1,984.68 2,030.04 2,282.28
73 1,819.44 2,046.84 2,092.32 2,353.92
74 1,874.04 2,109.48 2,155.08 2,425.92
75 1,928.88 2,172.48 2,218.20 2,498.40
76 1,967.76 2,207.52 2,262.96 2,538.60
77 1,999.08 2,245.20 2,298.84 2,582.04
78 2,058.12 2,314.20 2,366.88 2,661.24
79 2,127.00 2,383.08 2,446.08 2,740.56
80 2,186.16 2,452.08 2,514.00 2,819.88
81 2,245.20 2,530.80 2,582.04 2,910.48
82 2,314.20 2,599.68 2,661.24 2,989.68
83 2,373.24 2,668.68 2,729.28 3,069.00
84 2,432.28 2,737.56 2,797.20 3,148.20
85 2,491.44 2,796.72 2,865.12 3,216.24
86 2,554.20 2,868.12 2,937.24 3,298.32
87 2,616.84 2,939.64 3,009.48 3,380.52
88 2,657.04 2,981.40 3,055.68 3,428.52
89 2,696.28 3,021.96 3,100.68 3,475.20
90 2,734.32 3,061.32 3,144.48 3,520.44
91 2,771.16 3,099.12 3,186.84 3,564.00
92 2,806.44 3,135.48 3,227.40 3,605.76
93 2,839.32 3,169.32 3,265.32 3,644.64
94 2,870.52 3,201.24 3,301.08 3,681.36
95 2,899.92 3,231.12 3,334.92 3,715.80
96 2,927.28 3,258.96 3,366.36 3,747.84
97 2,952.72 3,284.52 3,395.52 3,777.24
98 2,975.88 3,307.80 3,422.28 3,804.00
99 2,997.00 3,328.80 3,446.52 3,828.12
1. The above rates do not include a one-time $20 policy fee at time of issue.
2. If the insured qualifies for household discount, the 7% discount will be applied. 3. For payment made on monthly EBT, there is an additional $2 discount per month.
Area Factors
Modal Factors 3-Digit Zip Code Factor
Mode Factor
871 0.91
Annual 1.00000 870, 872-885 0.82
Semi-Annual 0.50000
Rest of State 0.91
Quarterly 0.25000
Monthly 0.08333
ACOCRNM Page 7 of 24 ACOCRNM.1 Effective: 09-28-2012
American Family Life Assurance Company of Columbus (Aflac)
State of New Mexico Plan N
Attained Age
Non-Tobacco User Tobacco User
Female Male Female Male
0-64 N/A N/A N/A N/A
65 1,054.56 1,192.92 1,212.72 1,371.96
66 1,097.16 1,235.52 1,261.68 1,420.92
67 1,139.76 1,278.24 1,310.64 1,469.88
68 1,182.36 1,331.40 1,359.72 1,531.20
69 1,235.52 1,384.68 1,420.92 1,592.40
70 1,278.24 1,437.96 1,469.88 1,653.60
71 1,305.48 1,472.52 1,501.32 1,693.44
72 1,356.72 1,522.44 1,560.24 1,750.80
73 1,394.04 1,568.28 1,603.08 1,803.48
74 1,441.80 1,624.56 1,658.04 1,868.28
75 1,489.68 1,670.88 1,713.12 1,921.56
76 1,515.36 1,703.52 1,742.64 1,959.00
77 1,542.72 1,737.96 1,774.08 1,998.72
78 1,591.56 1,786.80 1,830.24 2,054.76
79 1,640.28 1,845.36 1,886.40 2,122.20
80 1,698.96 1,903.92 1,953.72 2,189.52
81 1,747.80 1,962.60 2,009.88 2,256.96
82 1,796.52 2,021.16 2,066.04 2,324.28
83 1,855.20 2,079.72 2,133.36 2,391.72
84 1,903.92 2,138.28 2,189.52 2,459.04
85 1,952.76 2,187.12 2,245.68 2,515.20
86 2,007.12 2,247.36 2,308.08 2,584.44
87 2,061.36 2,307.60 2,370.60 2,653.68
88 2,094.96 2,342.28 2,409.24 2,693.64
89 2,127.72 2,376.00 2,446.92 2,732.40
90 2,159.64 2,408.76 2,483.52 2,770.08
91 2,190.36 2,440.20 2,518.92 2,806.20
92 2,219.88 2,470.32 2,552.88 2,840.88
93 2,247.48 2,498.40 2,584.56 2,873.16
94 2,273.52 2,524.92 2,614.56 2,903.64
95 2,298.00 2,549.64 2,642.76 2,932.20
96 2,321.04 2,572.68 2,669.16 2,958.60
97 2,342.16 2,593.80 2,693.52 2,982.96
98 2,361.60 2,613.12 2,715.84 3,005.04
99 2,379.24 2,630.28 2,736.12 3,024.84
1. The above rates do not include a one-time $20 policy fee at time of issue.
2. If the insured qualifies for household discount, the 7% discount will be applied. 3. For payment made on monthly EBT, there is an additional $2 discount per month.
Area Factors
Modal Factors 3-Digit Zip Code Factor
Mode Factor
871 0.91
Annual 1.00000 870, 872-885 0.82
Semi-Annual 0.50000
Rest of State 0.91
Quarterly 0.25000
Monthly 0.08333

ACOCRNM Page 6 of 24 ACOCRNM.1 Effective: 09-28-2012
American Family Life Assurance Company of Columbus (Aflac)
State of New Mexico Plan G
Attained Age
Non-Tobacco User Tobacco User
Female Male Female Male
0-64 N/A N/A N/A N/A
65 1,375.08 1,546.92 1,581.36 1,779.00
66 1,428.72 1,611.36 1,643.04 1,853.16
67 1,493.28 1,675.92 1,717.20 1,927.20
68 1,546.92 1,740.36 1,779.00 2,001.36
69 1,600.68 1,804.80 1,840.80 2,075.52
70 1,665.12 1,869.24 1,914.84 2,149.56
71 1,706.40 1,917.00 1,962.36 2,204.64
72 1,765.32 1,984.68 2,030.04 2,282.28
73 1,819.44 2,046.84 2,092.32 2,353.92
74 1,874.04 2,109.48 2,155.08 2,425.92
75 1,928.88 2,172.48 2,218.20 2,498.40
76 1,967.76 2,207.52 2,262.96 2,538.60
77 1,999.08 2,245.20 2,298.84 2,582.04
78 2,058.12 2,314.20 2,366.88 2,661.24
79 2,127.00 2,383.08 2,446.08 2,740.56
80 2,186.16 2,452.08 2,514.00 2,819.88
81 2,245.20 2,530.80 2,582.04 2,910.48
82 2,314.20 2,599.68 2,661.24 2,989.68
83 2,373.24 2,668.68 2,729.28 3,069.00
84 2,432.28 2,737.56 2,797.20 3,148.20
85 2,491.44 2,796.72 2,865.12 3,216.24
86 2,554.20 2,868.12 2,937.24 3,298.32
87 2,616.84 2,939.64 3,009.48 3,380.52
88 2,657.04 2,981.40 3,055.68 3,428.52
89 2,696.28 3,021.96 3,100.68 3,475.20
90 2,734.32 3,061.32 3,144.48 3,520.44
91 2,771.16 3,099.12 3,186.84 3,564.00
92 2,806.44 3,135.48 3,227.40 3,605.76
93 2,839.32 3,169.32 3,265.32 3,644.64
94 2,870.52 3,201.24 3,301.08 3,681.36
95 2,899.92 3,231.12 3,334.92 3,715.80
96 2,927.28 3,258.96 3,366.36 3,747.84
97 2,952.72 3,284.52 3,395.52 3,777.24
98 2,975.88 3,307.80 3,422.28 3,804.00
99 2,997.00 3,328.80 3,446.52 3,828.12
1. The above rates do not include a one-time $20 policy fee at time of issue.
2. If the insured qualifies for household discount, the 7% discount will be applied. 3. For payment made on monthly EBT, there is an additional $2 discount per month.
Area Factors
Modal Factors 3-Digit Zip Code Factor
Mode Factor
871 0.91
Annual 1.00000 870, 872-885 0.82
Semi-Annual 0.50000
Rest of State 0.91
Quarterly 0.25000
Monthly 0.08333
ACOCRNM Page 7 of 24 ACOCRNM.1 Effective: 09-28-2012
American Family Life Assurance Company of Columbus (Aflac)
State of New Mexico Plan N
Attained Age
Non-Tobacco User Tobacco User
Female Male Female Male
0-64 N/A N/A N/A N/A
65 1,054.56 1,192.92 1,212.72 1,371.96
66 1,097.16 1,235.52 1,261.68 1,420.92
67 1,139.76 1,278.24 1,310.64 1,469.88
68 1,182.36 1,331.40 1,359.72 1,531.20
69 1,235.52 1,384.68 1,420.92 1,592.40
70 1,278.24 1,437.96 1,469.88 1,653.60
71 1,305.48 1,472.52 1,501.32 1,693.44
72 1,356.72 1,522.44 1,560.24 1,750.80
73 1,394.04 1,568.28 1,603.08 1,803.48
74 1,441.80 1,624.56 1,658.04 1,868.28
75 1,489.68 1,670.88 1,713.12 1,921.56
76 1,515.36 1,703.52 1,742.64 1,959.00
77 1,542.72 1,737.96 1,774.08 1,998.72
78 1,591.56 1,786.80 1,830.24 2,054.76
79 1,640.28 1,845.36 1,886.40 2,122.20
80 1,698.96 1,903.92 1,953.72 2,189.52
81 1,747.80 1,962.60 2,009.88 2,256.96
82 1,796.52 2,021.16 2,066.04 2,324.28
83 1,855.20 2,079.72 2,133.36 2,391.72
84 1,903.92 2,138.28 2,189.52 2,459.04
85 1,952.76 2,187.12 2,245.68 2,515.20
86 2,007.12 2,247.36 2,308.08 2,584.44
87 2,061.36 2,307.60 2,370.60 2,653.68
88 2,094.96 2,342.28 2,409.24 2,693.64
89 2,127.72 2,376.00 2,446.92 2,732.40
90 2,159.64 2,408.76 2,483.52 2,770.08
91 2,190.36 2,440.20 2,518.92 2,806.20
92 2,219.88 2,470.32 2,552.88 2,840.88
93 2,247.48 2,498.40 2,584.56 2,873.16
94 2,273.52 2,524.92 2,614.56 2,903.64
95 2,298.00 2,549.64 2,642.76 2,932.20
96 2,321.04 2,572.68 2,669.16 2,958.60
97 2,342.16 2,593.80 2,693.52 2,982.96
98 2,361.60 2,613.12 2,715.84 3,005.04
99 2,379.24 2,630.28 2,736.12 3,024.84
1. The above rates do not include a one-time $20 policy fee at time of issue.
2. If the insured qualifies for household discount, the 7% discount will be applied. 3. For payment made on monthly EBT, there is an additional $2 discount per month.
Area Factors
Modal Factors 3-Digit Zip Code Factor
Mode Factor
871 0.91
Annual 1.00000 870, 872-885 0.82
Semi-Annual 0.50000
Rest of State 0.91
Quarterly 0.25000
Monthly 0.08333
ACOCRNM Page 8 of 24 ACOCRNM.1 Effective: 09-28-2012
PREMIUM INFORMATION American Family Life Assurance Company of Columbus may change your premium on any premium due date if a new table of rates is applicable to the policy. The change in the table of rates will apply to all covered persons in the same class. Class is defined as attained age, sex, underwriting class, state of issue, and your most recent ZIP code of residence.
Premiums are based on your attained age and will change on your policy anniversary date. We will give you at least 60 days advance written notice if a new table of rates is applicable to the policy.
DISCLOSURES Use this outline to compare benefits and premiums among policies.
READ YOUR POLICY VERY CAREFULLY This is only an outline describing your Policy’s most important features. The Policy is your insurance contract. You must read the Policy itself to understand all of the rights and duties of both you and American Family Life Assurance Company of Columbus.
RIGHT TO RETURN POLICY If you find that you are not satisfied with your Policy, you may return it to: American Family Life Assurance Company of Columbus, Medicare Supplement Administration, P.O. Box 1553, Pensacola, Florida 32591. If you send the Policy back to us within 30 days after you receive it, we will treat the Policy as if it had never been issued and return all of your payments.
POLICY REPLACEMENT If you are replacing another health insurance policy, do NOT cancel it until you have actually received your new policy and are sure you want to keep it.
NOTICE This Policy may not fully cover all of your medical costs. Neither American Family Life Assurance Company of Columbus nor its agents are connected with Medicare. This outline of coverage does not give all the details of Medicare coverage. Contact your local Social Security Office or consult Medicare and You for more details.
COMPLETE ANSWERS ARE VERY IMPORTANT When you fill out the application for the new Policy, be sure to answer truthfully and completely all questions about your medical and health history. American Family Life Assurance Company of Columbus may cancel your Policy and refuse to pay any claims if you leave out or falsify important medical information.
Review the application carefully before you sign it. Be certain that all information has been properly recorded.
Please refer to your Policy for details.
ACOCRNM Page 9 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN A MEDICARE (PART A) – HOSPITAL SERVICES – PER BENEFIT PERIOD
*A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and have not received skilled care in any other facility for 60 days in a row.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY
HOSPITALIZATION* Semiprivate room and board, general nursing and miscellaneous services and supplies
First 60 days All but $1156 $0 $1156 (Part A deductible)
61st thru 90th day All but $289 a day $289 a day $0 91st day and after: — While using 60 lifetime reserve
days All but $578 a day $578 a day $0 — Once lifetime reserve days are
used:
— Additional 365 days $0 100% of Medicare-eligible expenses
$0**
— Beyond the additional 365 days $0 $0 All costs
SKILLED NURSING FACILITY CARE*
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts $0 $0 21st thru 100th day All but $144.50 a day $0 Up to $144.50 a day 101st day and after $0 $0 All costs
BLOOD
First 3 pints $0 3 pints $0 Additional amounts 100% $0 $0
HOSPICE CARE
You must meet Medicare’s requirements, including a doctor’s certification of terminal illness.
All but very limited co-payment/ coinsurance for out-patient drugs and inpatient respite care
Medicare copayment/coinsurance
$0
**NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy’s “Core Benefits.” During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.
ACOCRNM Page 9 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN A MEDICARE (PART A) – HOSPITAL SERVICES – PER BENEFIT PERIOD
*A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and have not received skilled care in any other facility for 60 days in a row.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY
HOSPITALIZATION* Semiprivate room and board, general nursing and miscellaneous services and supplies
First 60 days All but $1156 $0 $1156 (Part A deductible)
61st thru 90th day All but $289 a day $289 a day $0 91st day and after: — While using 60 lifetime reserve
days All but $578 a day $578 a day $0 — Once lifetime reserve days are
used:
— Additional 365 days $0 100% of Medicare-eligible expenses
$0**
— Beyond the additional 365 days $0 $0 All costs
SKILLED NURSING FACILITY CARE*
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts $0 $0 21st thru 100th day All but $144.50 a day $0 Up to $144.50 a day 101st day and after $0 $0 All costs
BLOOD
First 3 pints $0 3 pints $0 Additional amounts 100% $0 $0
HOSPICE CARE
You must meet Medicare’s requirements, including a doctor’s certification of terminal illness.
All but very limited co-payment/ coinsurance for out-patient drugs and inpatient respite care
Medicare copayment/coinsurance
$0
**NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy’s “Core Benefits.” During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.

ACOCRNM Page 8 of 24 ACOCRNM.1 Effective: 09-28-2012
PREMIUM INFORMATION American Family Life Assurance Company of Columbus may change your premium on any premium due date if a new table of rates is applicable to the policy. The change in the table of rates will apply to all covered persons in the same class. Class is defined as attained age, sex, underwriting class, state of issue, and your most recent ZIP code of residence.
Premiums are based on your attained age and will change on your policy anniversary date. We will give you at least 60 days advance written notice if a new table of rates is applicable to the policy.
DISCLOSURES Use this outline to compare benefits and premiums among policies.
READ YOUR POLICY VERY CAREFULLY This is only an outline describing your Policy’s most important features. The Policy is your insurance contract. You must read the Policy itself to understand all of the rights and duties of both you and American Family Life Assurance Company of Columbus.
RIGHT TO RETURN POLICY If you find that you are not satisfied with your Policy, you may return it to: American Family Life Assurance Company of Columbus, Medicare Supplement Administration, P.O. Box 1553, Pensacola, Florida 32591. If you send the Policy back to us within 30 days after you receive it, we will treat the Policy as if it had never been issued and return all of your payments.
POLICY REPLACEMENT If you are replacing another health insurance policy, do NOT cancel it until you have actually received your new policy and are sure you want to keep it.
NOTICE This Policy may not fully cover all of your medical costs. Neither American Family Life Assurance Company of Columbus nor its agents are connected with Medicare. This outline of coverage does not give all the details of Medicare coverage. Contact your local Social Security Office or consult Medicare and You for more details.
COMPLETE ANSWERS ARE VERY IMPORTANT When you fill out the application for the new Policy, be sure to answer truthfully and completely all questions about your medical and health history. American Family Life Assurance Company of Columbus may cancel your Policy and refuse to pay any claims if you leave out or falsify important medical information.
Review the application carefully before you sign it. Be certain that all information has been properly recorded.
Please refer to your Policy for details.
ACOCRNM Page 9 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN A MEDICARE (PART A) – HOSPITAL SERVICES – PER BENEFIT PERIOD
*A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and have not received skilled care in any other facility for 60 days in a row.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY
HOSPITALIZATION* Semiprivate room and board, general nursing and miscellaneous services and supplies
First 60 days All but $1156 $0 $1156 (Part A deductible)
61st thru 90th day All but $289 a day $289 a day $0 91st day and after: — While using 60 lifetime reserve
days All but $578 a day $578 a day $0 — Once lifetime reserve days are
used:
— Additional 365 days $0 100% of Medicare-eligible expenses
$0**
— Beyond the additional 365 days $0 $0 All costs
SKILLED NURSING FACILITY CARE*
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts $0 $0 21st thru 100th day All but $144.50 a day $0 Up to $144.50 a day 101st day and after $0 $0 All costs
BLOOD
First 3 pints $0 3 pints $0 Additional amounts 100% $0 $0
HOSPICE CARE
You must meet Medicare’s requirements, including a doctor’s certification of terminal illness.
All but very limited co-payment/ coinsurance for out-patient drugs and inpatient respite care
Medicare copayment/coinsurance
$0
**NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy’s “Core Benefits.” During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.
ACOCRNM Page 9 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN A MEDICARE (PART A) – HOSPITAL SERVICES – PER BENEFIT PERIOD
*A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and have not received skilled care in any other facility for 60 days in a row.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY
HOSPITALIZATION* Semiprivate room and board, general nursing and miscellaneous services and supplies
First 60 days All but $1156 $0 $1156 (Part A deductible)
61st thru 90th day All but $289 a day $289 a day $0 91st day and after: — While using 60 lifetime reserve
days All but $578 a day $578 a day $0 — Once lifetime reserve days are
used:
— Additional 365 days $0 100% of Medicare-eligible expenses
$0**
— Beyond the additional 365 days $0 $0 All costs
SKILLED NURSING FACILITY CARE*
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts $0 $0 21st thru 100th day All but $144.50 a day $0 Up to $144.50 a day 101st day and after $0 $0 All costs
BLOOD
First 3 pints $0 3 pints $0 Additional amounts 100% $0 $0
HOSPICE CARE
You must meet Medicare’s requirements, including a doctor’s certification of terminal illness.
All but very limited co-payment/ coinsurance for out-patient drugs and inpatient respite care
Medicare copayment/coinsurance
$0
**NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy’s “Core Benefits.” During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.
ACOCRNM Page 10 of 24 ACOCRNM.1 Effective: 09-28-2012
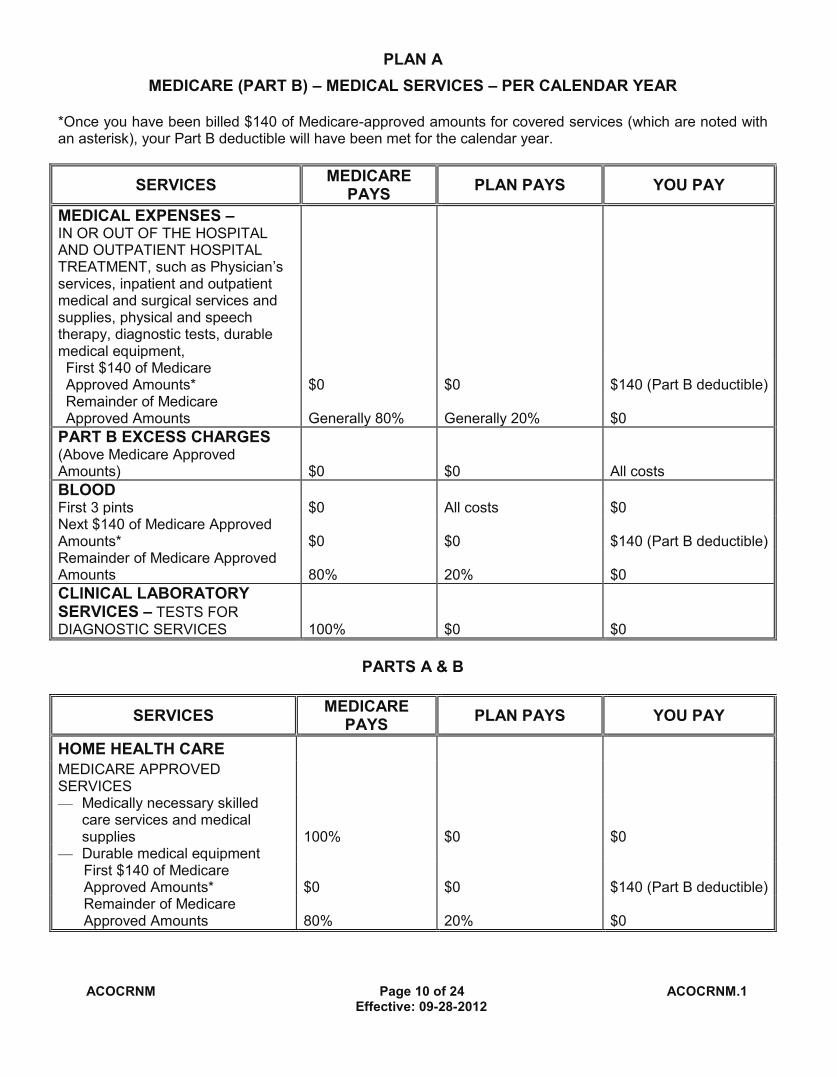
PLAN A MEDICARE (PART B) – MEDICAL SERVICES – PER CALENDAR YEAR
*Once you have been billed $140 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible will have been met for the calendar year.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY
MEDICAL EXPENSES – IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as Physician’s services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment,
First $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts Generally 80% Generally 20% $0
PART B EXCESS CHARGES (Above Medicare Approved Amounts) $0 $0 All costs BLOOD First 3 pints $0 All costs $0 Next $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0 CLINICAL LABORATORY SERVICES – TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0
PARTS A & B
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY
HOME HEALTH CARE MEDICARE APPROVED SERVICES
— Medically necessary skilled care services and medical supplies 100% $0 $0
— Durable medical equipment First $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0
ACOCRNM Page 11 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN C MEDICARE (PART A) – HOSPITAL SERVICES – PER BENEFIT PERIOD
*A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and have not received skilled care in any other facility for 60 days in a row.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY
HOSPITALIZATION* Semiprivate room and board, general nursing and miscellaneous services and supplies
First 60 days All but $1156 $1156 (Part A deductible) $0 61st thru 90th day All but $289 a day $289 a day $0 91st day and after: — While using 60 lifetime
reserve days All but $578 a day $578 a day $0 — Once lifetime reserve days
are used:
— Additional 365 days $0 100% of Medicare-eligible expenses
$0**
— Beyond the additional 365 days $0 $0 All costs
SKILLED NURSING FACILITY CARE*
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts
$0 $0
21st thru 100th day All but $144.50 a day
Up to $144.50 a day $0
101st day and after $0 $0 All costs
BLOOD
First 3 pints $0 3 pints $0 Additional amounts 100% $0 $0
HOSPICE CARE
You must meet Medicare’s requirements, including a doctor’s certification of terminal illness.
All but very limited co-payment/ coinsurance for out-patient drugs and inpatient respite care
Medicare co-payment/coinsurance
$0
**NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy’s “Core Benefits.” During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.
ACOCRNM Page 10 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN A MEDICARE (PART B) – MEDICAL SERVICES – PER CALENDAR YEAR
*Once you have been billed $140 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible will have been met for the calendar year.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY
MEDICAL EXPENSES – IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as Physician’s services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment,
First $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts Generally 80% Generally 20% $0
PART B EXCESS CHARGES (Above Medicare Approved Amounts) $0 $0 All costs BLOOD First 3 pints $0 All costs $0 Next $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0 CLINICAL LABORATORY SERVICES – TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0
PARTS A & B
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY
HOME HEALTH CARE MEDICARE APPROVED SERVICES
— Medically necessary skilled care services and medical supplies 100% $0 $0
— Durable medical equipment First $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0
ACOCRNM Page 11 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN C MEDICARE (PART A) – HOSPITAL SERVICES – PER BENEFIT PERIOD
*A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and have not received skilled care in any other facility for 60 days in a row.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY
HOSPITALIZATION* Semiprivate room and board, general nursing and miscellaneous services and supplies
First 60 days All but $1156 $1156 (Part A deductible) $0 61st thru 90th day All but $289 a day $289 a day $0 91st day and after: — While using 60 lifetime
reserve days All but $578 a day $578 a day $0 — Once lifetime reserve days
are used:
— Additional 365 days $0 100% of Medicare-eligible expenses
$0**
— Beyond the additional 365 days $0 $0 All costs
SKILLED NURSING FACILITY CARE*
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts
$0 $0
21st thru 100th day All but $144.50 a day
Up to $144.50 a day $0
101st day and after $0 $0 All costs
BLOOD
First 3 pints $0 3 pints $0 Additional amounts 100% $0 $0
HOSPICE CARE
You must meet Medicare’s requirements, including a doctor’s certification of terminal illness.
All but very limited co-payment/ coinsurance for out-patient drugs and inpatient respite care
Medicare co-payment/coinsurance
$0
**NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy’s “Core Benefits.” During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.

ACOCRNM Page 10 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN A MEDICARE (PART B) – MEDICAL SERVICES – PER CALENDAR YEAR
*Once you have been billed $140 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible will have been met for the calendar year.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY
MEDICAL EXPENSES – IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as Physician’s services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment,
First $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts Generally 80% Generally 20% $0
PART B EXCESS CHARGES (Above Medicare Approved Amounts) $0 $0 All costs BLOOD First 3 pints $0 All costs $0 Next $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0 CLINICAL LABORATORY SERVICES – TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0
PARTS A & B
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY
HOME HEALTH CARE MEDICARE APPROVED SERVICES
— Medically necessary skilled care services and medical supplies 100% $0 $0
— Durable medical equipment First $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0
ACOCRNM Page 11 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN C MEDICARE (PART A) – HOSPITAL SERVICES – PER BENEFIT PERIOD
*A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and have not received skilled care in any other facility for 60 days in a row.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY
HOSPITALIZATION* Semiprivate room and board, general nursing and miscellaneous services and supplies
First 60 days All but $1156 $1156 (Part A deductible) $0 61st thru 90th day All but $289 a day $289 a day $0 91st day and after: — While using 60 lifetime
reserve days All but $578 a day $578 a day $0 — Once lifetime reserve days
are used:
— Additional 365 days $0 100% of Medicare-eligible expenses
$0**
— Beyond the additional 365 days $0 $0 All costs
SKILLED NURSING FACILITY CARE*
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts
$0 $0
21st thru 100th day All but $144.50 a day
Up to $144.50 a day $0
101st day and after $0 $0 All costs
BLOOD
First 3 pints $0 3 pints $0 Additional amounts 100% $0 $0
HOSPICE CARE
You must meet Medicare’s requirements, including a doctor’s certification of terminal illness.
All but very limited co-payment/ coinsurance for out-patient drugs and inpatient respite care
Medicare co-payment/coinsurance
$0
**NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy’s “Core Benefits.” During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.
ACOCRNM Page 10 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN A MEDICARE (PART B) – MEDICAL SERVICES – PER CALENDAR YEAR
*Once you have been billed $140 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible will have been met for the calendar year.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY
MEDICAL EXPENSES – IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as Physician’s services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment,
First $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts Generally 80% Generally 20% $0
PART B EXCESS CHARGES (Above Medicare Approved Amounts) $0 $0 All costs BLOOD First 3 pints $0 All costs $0 Next $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0 CLINICAL LABORATORY SERVICES – TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0
PARTS A & B
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY
HOME HEALTH CARE MEDICARE APPROVED SERVICES
— Medically necessary skilled care services and medical supplies 100% $0 $0
— Durable medical equipment First $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0
ACOCRNM Page 11 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN C MEDICARE (PART A) – HOSPITAL SERVICES – PER BENEFIT PERIOD
*A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and have not received skilled care in any other facility for 60 days in a row.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY
HOSPITALIZATION* Semiprivate room and board, general nursing and miscellaneous services and supplies
First 60 days All but $1156 $1156 (Part A deductible) $0 61st thru 90th day All but $289 a day $289 a day $0 91st day and after: — While using 60 lifetime
reserve days All but $578 a day $578 a day $0 — Once lifetime reserve days
are used:
— Additional 365 days $0 100% of Medicare-eligible expenses
$0**
— Beyond the additional 365 days $0 $0 All costs
SKILLED NURSING FACILITY CARE*
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts
$0 $0
21st thru 100th day All but $144.50 a day
Up to $144.50 a day $0
101st day and after $0 $0 All costs
BLOOD
First 3 pints $0 3 pints $0 Additional amounts 100% $0 $0
HOSPICE CARE
You must meet Medicare’s requirements, including a doctor’s certification of terminal illness.
All but very limited co-payment/ coinsurance for out-patient drugs and inpatient respite care
Medicare co-payment/coinsurance
$0
**NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy’s “Core Benefits.” During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.

ACOCRNM Page 12 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN C MEDICARE (PART B) – MEDICAL SERVICES – PER CALENDAR YEAR
*Once you have been billed $140 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible will have been met for the calendar year.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY MEDICAL EXPENSES – IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as Physician’s services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment,
First $140 of Medicare Approved Amounts* $0 $140 (Part B deductible) $0 Remainder of Medicare Approved Amounts Generally 80% Generally 20% $0
PART B EXCESS CHARGES (Above Medicare Approved Amounts) $0 $0 All costs BLOOD First 3 pints $0 All costs $0 Next $140 of Medicare Approved Amounts* $0 $140 (Part B deductible) $0 Remainder of Medicare Approved Amounts 80% 20% $0 CLINICAL LABORATORY SERVICES – TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0
PARTS A & B HOME HEALTH CARE MEDICARE APPROVED SERVICES
— Medically necessary skilled care services and medical supplies 100% $0 $0
— Durable medical equipment First $140 of Medicare Approved Amounts* $0 $140 (Part B deductible) $0 Remainder of Medicare Approved Amounts 80% 20% $0
OTHER BENEFITS – NOT COVERED BY MEDICARE FOREIGN TRAVEL – NOT COVERED BY MEDICARE
Medically necessary emergency care services beginning during the first 60 days of each trip outside the USA
First $250 each calendar year $0 $0 $250 Remainder of charges $0 80% to a lifetime
maximum benefit of $50,000.
20% and amounts over the $50,000 lifetime maximum.
ACOCRNM Page 13 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN D MEDICARE (PART A) – HOSPITAL SERVICES – PER BENEFIT PERIOD
*A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and have not received skilled care in any other facility for 60 days in a row.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY
HOSPITALIZATION*
Semiprivate room and board, general nursing and miscellaneous services and supplies
First 60 days All but $1156 $1156 (Part A deductible)
$0
61st thru 90th day All but $289 a day $289 a day $0 91st day and after: — While using 60 lifetime
reserve days All but $578 a day $578 a day $0 — Once lifetime reserve days
are used:
Additional 365 days $0 100% of Medicare-eligible expenses
$0**
— Beyond the additional 365 days $0 $0 All costs
SKILLED NURSING FACILITY CARE*
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts
$0 $0
21st thru 100th day All but $144.50 a day Up to $144.50 a day $0 101st day and after $0 $0 All costs
BLOOD
First 3 pints $0 3 pints $0 Additional amounts 100% $0 $0
HOSPICE CARE
You must meet Medicare’s requirements, including a doctor’s certification of terminal illness.
All but very limited co-payment/ coinsurance for out-patient drugs and inpatient respite care
Medicare co-payment/coinsurance
$0
**NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy’s “Core Benefits.” During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.
ACOCRNM Page 12 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN C MEDICARE (PART B) – MEDICAL SERVICES – PER CALENDAR YEAR
*Once you have been billed $140 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible will have been met for the calendar year.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY MEDICAL EXPENSES – IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as Physician’s services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment,
First $140 of Medicare Approved Amounts* $0 $140 (Part B deductible) $0 Remainder of Medicare Approved Amounts Generally 80% Generally 20% $0
PART B EXCESS CHARGES (Above Medicare Approved Amounts) $0 $0 All costs BLOOD First 3 pints $0 All costs $0 Next $140 of Medicare Approved Amounts* $0 $140 (Part B deductible) $0 Remainder of Medicare Approved Amounts 80% 20% $0 CLINICAL LABORATORY SERVICES – TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0
PARTS A & B HOME HEALTH CARE MEDICARE APPROVED SERVICES
— Medically necessary skilled care services and medical supplies 100% $0 $0
— Durable medical equipment First $140 of Medicare Approved Amounts* $0 $140 (Part B deductible) $0 Remainder of Medicare Approved Amounts 80% 20% $0
OTHER BENEFITS – NOT COVERED BY MEDICARE FOREIGN TRAVEL – NOT COVERED BY MEDICARE
Medically necessary emergency care services beginning during the first 60 days of each trip outside the USA
First $250 each calendar year $0 $0 $250 Remainder of charges $0 80% to a lifetime
maximum benefit of $50,000.
20% and amounts over the $50,000 lifetime maximum.
ACOCRNM Page 13 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN D MEDICARE (PART A) – HOSPITAL SERVICES – PER BENEFIT PERIOD
*A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and have not received skilled care in any other facility for 60 days in a row.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY
HOSPITALIZATION*
Semiprivate room and board, general nursing and miscellaneous services and supplies
First 60 days All but $1156 $1156 (Part A deductible)
$0
61st thru 90th day All but $289 a day $289 a day $0 91st day and after: — While using 60 lifetime
reserve days All but $578 a day $578 a day $0 — Once lifetime reserve days
are used:
Additional 365 days $0 100% of Medicare-eligible expenses
$0**
— Beyond the additional 365 days $0 $0 All costs
SKILLED NURSING FACILITY CARE*
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts
$0 $0
21st thru 100th day All but $144.50 a day Up to $144.50 a day $0 101st day and after $0 $0 All costs
BLOOD
First 3 pints $0 3 pints $0 Additional amounts 100% $0 $0
HOSPICE CARE
You must meet Medicare’s requirements, including a doctor’s certification of terminal illness.
All but very limited co-payment/ coinsurance for out-patient drugs and inpatient respite care
Medicare co-payment/coinsurance
$0
**NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy’s “Core Benefits.” During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.

ACOCRNM Page 12 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN C MEDICARE (PART B) – MEDICAL SERVICES – PER CALENDAR YEAR
*Once you have been billed $140 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible will have been met for the calendar year.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY MEDICAL EXPENSES – IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as Physician’s services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment,
First $140 of Medicare Approved Amounts* $0 $140 (Part B deductible) $0 Remainder of Medicare Approved Amounts Generally 80% Generally 20% $0
PART B EXCESS CHARGES (Above Medicare Approved Amounts) $0 $0 All costs BLOOD First 3 pints $0 All costs $0 Next $140 of Medicare Approved Amounts* $0 $140 (Part B deductible) $0 Remainder of Medicare Approved Amounts 80% 20% $0 CLINICAL LABORATORY SERVICES – TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0
PARTS A & B HOME HEALTH CARE MEDICARE APPROVED SERVICES
— Medically necessary skilled care services and medical supplies 100% $0 $0
— Durable medical equipment First $140 of Medicare Approved Amounts* $0 $140 (Part B deductible) $0 Remainder of Medicare Approved Amounts 80% 20% $0
OTHER BENEFITS – NOT COVERED BY MEDICARE FOREIGN TRAVEL – NOT COVERED BY MEDICARE
Medically necessary emergency care services beginning during the first 60 days of each trip outside the USA
First $250 each calendar year $0 $0 $250 Remainder of charges $0 80% to a lifetime
maximum benefit of $50,000.
20% and amounts over the $50,000 lifetime maximum.
ACOCRNM Page 13 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN D MEDICARE (PART A) – HOSPITAL SERVICES – PER BENEFIT PERIOD
*A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and have not received skilled care in any other facility for 60 days in a row.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY
HOSPITALIZATION*
Semiprivate room and board, general nursing and miscellaneous services and supplies
First 60 days All but $1156 $1156 (Part A deductible)
$0
61st thru 90th day All but $289 a day $289 a day $0 91st day and after: — While using 60 lifetime
reserve days All but $578 a day $578 a day $0 — Once lifetime reserve days
are used:
Additional 365 days $0 100% of Medicare-eligible expenses
$0**
— Beyond the additional 365 days $0 $0 All costs
SKILLED NURSING FACILITY CARE*
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts
$0 $0
21st thru 100th day All but $144.50 a day Up to $144.50 a day $0 101st day and after $0 $0 All costs
BLOOD
First 3 pints $0 3 pints $0 Additional amounts 100% $0 $0
HOSPICE CARE
You must meet Medicare’s requirements, including a doctor’s certification of terminal illness.
All but very limited co-payment/ coinsurance for out-patient drugs and inpatient respite care
Medicare co-payment/coinsurance
$0
**NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy’s “Core Benefits.” During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.
ACOCRNM Page 12 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN C MEDICARE (PART B) – MEDICAL SERVICES – PER CALENDAR YEAR
*Once you have been billed $140 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible will have been met for the calendar year.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY MEDICAL EXPENSES – IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as Physician’s services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment,
First $140 of Medicare Approved Amounts* $0 $140 (Part B deductible) $0 Remainder of Medicare Approved Amounts Generally 80% Generally 20% $0
PART B EXCESS CHARGES (Above Medicare Approved Amounts) $0 $0 All costs BLOOD First 3 pints $0 All costs $0 Next $140 of Medicare Approved Amounts* $0 $140 (Part B deductible) $0 Remainder of Medicare Approved Amounts 80% 20% $0 CLINICAL LABORATORY SERVICES – TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0
PARTS A & B HOME HEALTH CARE MEDICARE APPROVED SERVICES
— Medically necessary skilled care services and medical supplies 100% $0 $0
— Durable medical equipment First $140 of Medicare Approved Amounts* $0 $140 (Part B deductible) $0 Remainder of Medicare Approved Amounts 80% 20% $0
OTHER BENEFITS – NOT COVERED BY MEDICARE FOREIGN TRAVEL – NOT COVERED BY MEDICARE
Medically necessary emergency care services beginning during the first 60 days of each trip outside the USA
First $250 each calendar year $0 $0 $250 Remainder of charges $0 80% to a lifetime
maximum benefit of $50,000.
20% and amounts over the $50,000 lifetime maximum.
ACOCRNM Page 13 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN D MEDICARE (PART A) – HOSPITAL SERVICES – PER BENEFIT PERIOD
*A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and have not received skilled care in any other facility for 60 days in a row.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY
HOSPITALIZATION*
Semiprivate room and board, general nursing and miscellaneous services and supplies
First 60 days All but $1156 $1156 (Part A deductible)
$0
61st thru 90th day All but $289 a day $289 a day $0 91st day and after: — While using 60 lifetime
reserve days All but $578 a day $578 a day $0 — Once lifetime reserve days
are used:
Additional 365 days $0 100% of Medicare-eligible expenses
$0**
— Beyond the additional 365 days $0 $0 All costs
SKILLED NURSING FACILITY CARE*
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts
$0 $0
21st thru 100th day All but $144.50 a day Up to $144.50 a day $0 101st day and after $0 $0 All costs
BLOOD
First 3 pints $0 3 pints $0 Additional amounts 100% $0 $0
HOSPICE CARE
You must meet Medicare’s requirements, including a doctor’s certification of terminal illness.
All but very limited co-payment/ coinsurance for out-patient drugs and inpatient respite care
Medicare co-payment/coinsurance
$0
**NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy’s “Core Benefits.” During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.
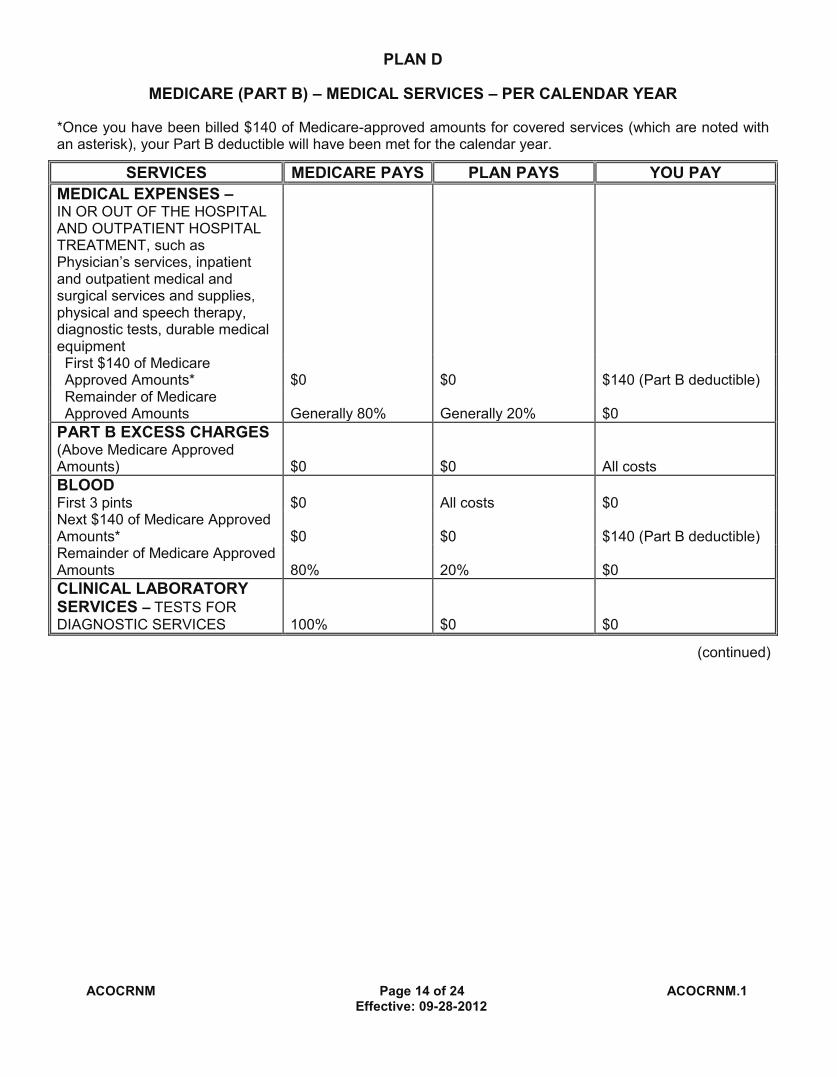
ACOCRNM Page 14 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN D
MEDICARE (PART B) – MEDICAL SERVICES – PER CALENDAR YEAR
*Once you have been billed $140 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible will have been met for the calendar year.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY MEDICAL EXPENSES – IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as Physician’s services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment
First $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts Generally 80% Generally 20% $0
PART B EXCESS CHARGES (Above Medicare Approved Amounts) $0 $0 All costs BLOOD First 3 pints $0 All costs $0 Next $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0 CLINICAL LABORATORY SERVICES – TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0
(continued)
ACOCRNM Page 15 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN D PARTS A & B
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY HOME HEALTH CARE MEDICARE APPROVED SERVICES
— Medically necessary skilled care services and medical supplies 100% $0 $0
— Durable medical equipment First $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0
OTHER BENEFITS – NOT COVERED BY MEDICARE
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY FOREIGN TRAVEL – NOT COVERED BY MEDICARE Medically necessary emergency care services beginning during the first 60 days of each trip outside the USA
First $250 each calendar year $0 $0 $250 Remainder of charges $0 80% to a lifetime
maximum benefit of $50,000.
20% and amounts over the $50,000 lifetime maximum.
ACOCRNM Page 14 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN D
MEDICARE (PART B) – MEDICAL SERVICES – PER CALENDAR YEAR
*Once you have been billed $140 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible will have been met for the calendar year.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY MEDICAL EXPENSES – IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as Physician’s services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment
First $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts Generally 80% Generally 20% $0
PART B EXCESS CHARGES (Above Medicare Approved Amounts) $0 $0 All costs BLOOD First 3 pints $0 All costs $0 Next $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0 CLINICAL LABORATORY SERVICES – TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0
(continued)
ACOCRNM Page 15 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN D PARTS A & B
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY HOME HEALTH CARE MEDICARE APPROVED SERVICES
— Medically necessary skilled care services and medical supplies 100% $0 $0
— Durable medical equipment First $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0
OTHER BENEFITS – NOT COVERED BY MEDICARE
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY FOREIGN TRAVEL – NOT COVERED BY MEDICARE Medically necessary emergency care services beginning during the first 60 days of each trip outside the USA
First $250 each calendar year $0 $0 $250 Remainder of charges $0 80% to a lifetime
maximum benefit of $50,000.
20% and amounts over the $50,000 lifetime maximum.

ACOCRNM Page 14 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN D
MEDICARE (PART B) – MEDICAL SERVICES – PER CALENDAR YEAR
*Once you have been billed $140 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible will have been met for the calendar year.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY MEDICAL EXPENSES – IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as Physician’s services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment
First $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts Generally 80% Generally 20% $0
PART B EXCESS CHARGES (Above Medicare Approved Amounts) $0 $0 All costs BLOOD First 3 pints $0 All costs $0 Next $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0 CLINICAL LABORATORY SERVICES – TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0
(continued)
ACOCRNM Page 15 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN D PARTS A & B
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY HOME HEALTH CARE MEDICARE APPROVED SERVICES
— Medically necessary skilled care services and medical supplies 100% $0 $0
— Durable medical equipment First $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0
OTHER BENEFITS – NOT COVERED BY MEDICARE
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY FOREIGN TRAVEL – NOT COVERED BY MEDICARE Medically necessary emergency care services beginning during the first 60 days of each trip outside the USA
First $250 each calendar year $0 $0 $250 Remainder of charges $0 80% to a lifetime
maximum benefit of $50,000.
20% and amounts over the $50,000 lifetime maximum.
ACOCRNM Page 14 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN D
MEDICARE (PART B) – MEDICAL SERVICES – PER CALENDAR YEAR
*Once you have been billed $140 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible will have been met for the calendar year.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY MEDICAL EXPENSES – IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as Physician’s services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment
First $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts Generally 80% Generally 20% $0
PART B EXCESS CHARGES (Above Medicare Approved Amounts) $0 $0 All costs BLOOD First 3 pints $0 All costs $0 Next $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0 CLINICAL LABORATORY SERVICES – TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0
(continued)
ACOCRNM Page 15 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN D PARTS A & B
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY HOME HEALTH CARE MEDICARE APPROVED SERVICES
— Medically necessary skilled care services and medical supplies 100% $0 $0
— Durable medical equipment First $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0
OTHER BENEFITS – NOT COVERED BY MEDICARE
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY FOREIGN TRAVEL – NOT COVERED BY MEDICARE Medically necessary emergency care services beginning during the first 60 days of each trip outside the USA
First $250 each calendar year $0 $0 $250 Remainder of charges $0 80% to a lifetime
maximum benefit of $50,000.
20% and amounts over the $50,000 lifetime maximum.
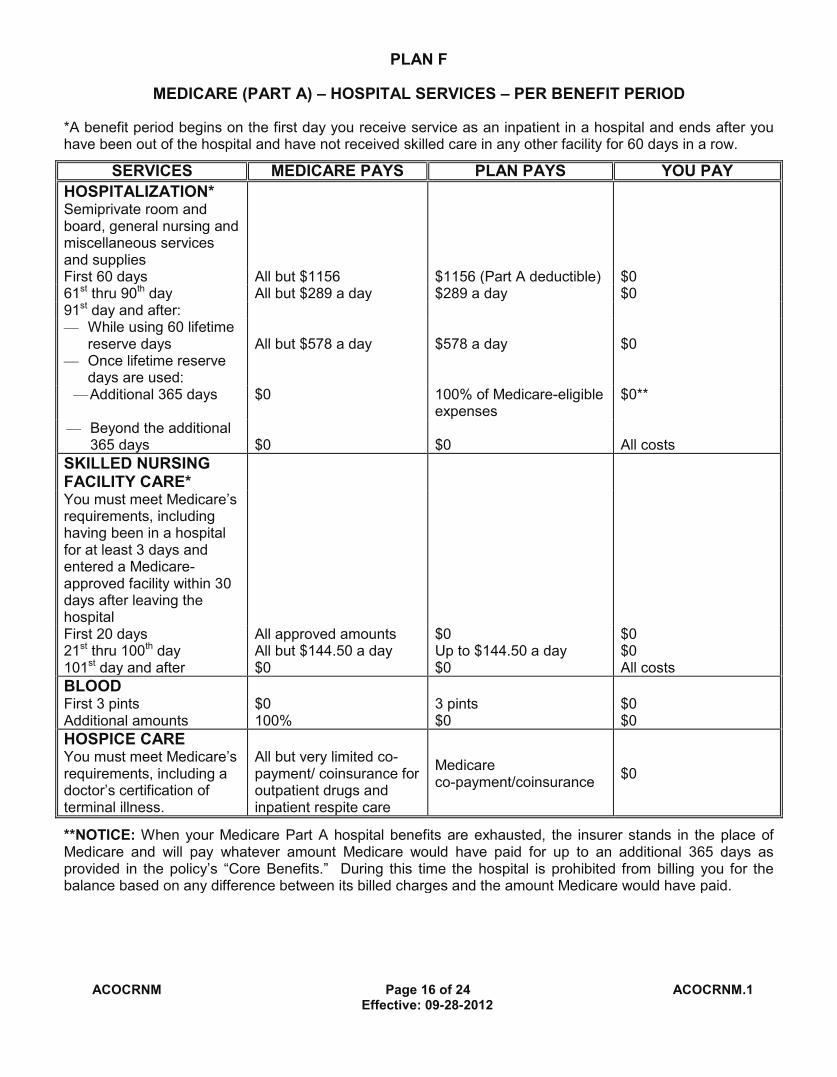
ACOCRNM Page 16 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN F
MEDICARE (PART A) – HOSPITAL SERVICES – PER BENEFIT PERIOD
*A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and have not received skilled care in any other facility for 60 days in a row.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY HOSPITALIZATION* Semiprivate room and board, general nursing and miscellaneous services and supplies
First 60 days All but $1156 $1156 (Part A deductible) $0 61st thru 90th day All but $289 a day $289 a day $0 91st day and after: — While using 60 lifetime
reserve days All but $578 a day $578 a day $0 — Once lifetime reserve
days are used:
— Additional 365 days $0 100% of Medicare-eligible expenses
$0**
— Beyond the additional 365 days $0 $0 All costs
SKILLED NURSING FACILITY CARE*
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts $0 $0 21st thru 100th day All but $144.50 a day Up to $144.50 a day $0 101st day and after $0 $0 All costs BLOOD First 3 pints $0 3 pints $0 Additional amounts 100% $0 $0 HOSPICE CARE You must meet Medicare’s requirements, including a doctor’s certification of terminal illness.
All but very limited co-payment/ coinsurance for outpatient drugs and inpatient respite care
Medicare co-payment/coinsurance
$0
**NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy’s “Core Benefits.” During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.
ACOCRNM Page 17 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN F
MEDICARE (PART B) – MEDICAL SERVICES – PER CALENDAR YEAR
*Once you have been billed $140 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible will have been met for the calendar year.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY MEDICAL EXPENSES – IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as Physician’s services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment,
First $140 of Medicare Approved Amounts* $0 $140 (Part B deductible) $0 Remainder of Medicare Approved Amounts Generally 80% Generally 20% $0
PART B EXCESS CHARGES (Above Medicare Approved Amounts) $0 100% $0 BLOOD First 3 pints $0 All costs $0 Next $140 of Medicare Approved amounts* $0 $140 (Part B deductible) $0 Remainder of Medicare Approved amounts 80% 20% $0 CLINICAL LABORATORY SERVICES – TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0
(continued)
ACOCRNM Page 16 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN F
MEDICARE (PART A) – HOSPITAL SERVICES – PER BENEFIT PERIOD
*A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and have not received skilled care in any other facility for 60 days in a row.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY HOSPITALIZATION* Semiprivate room and board, general nursing and miscellaneous services and supplies
First 60 days All but $1156 $1156 (Part A deductible) $0 61st thru 90th day All but $289 a day $289 a day $0 91st day and after: — While using 60 lifetime
reserve days All but $578 a day $578 a day $0 — Once lifetime reserve
days are used:
— Additional 365 days $0 100% of Medicare-eligible expenses
$0**
— Beyond the additional 365 days $0 $0 All costs
SKILLED NURSING FACILITY CARE*
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts $0 $0 21st thru 100th day All but $144.50 a day Up to $144.50 a day $0 101st day and after $0 $0 All costs BLOOD First 3 pints $0 3 pints $0 Additional amounts 100% $0 $0 HOSPICE CARE You must meet Medicare’s requirements, including a doctor’s certification of terminal illness.
All but very limited co-payment/ coinsurance for outpatient drugs and inpatient respite care
Medicare co-payment/coinsurance
$0
**NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy’s “Core Benefits.” During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.
ACOCRNM Page 17 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN F
MEDICARE (PART B) – MEDICAL SERVICES – PER CALENDAR YEAR
*Once you have been billed $140 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible will have been met for the calendar year.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY MEDICAL EXPENSES – IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as Physician’s services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment,
First $140 of Medicare Approved Amounts* $0 $140 (Part B deductible) $0 Remainder of Medicare Approved Amounts Generally 80% Generally 20% $0
PART B EXCESS CHARGES (Above Medicare Approved Amounts) $0 100% $0 BLOOD First 3 pints $0 All costs $0 Next $140 of Medicare Approved amounts* $0 $140 (Part B deductible) $0 Remainder of Medicare Approved amounts 80% 20% $0 CLINICAL LABORATORY SERVICES – TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0
(continued)

ACOCRNM Page 16 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN F
MEDICARE (PART A) – HOSPITAL SERVICES – PER BENEFIT PERIOD
*A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and have not received skilled care in any other facility for 60 days in a row.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY HOSPITALIZATION* Semiprivate room and board, general nursing and miscellaneous services and supplies
First 60 days All but $1156 $1156 (Part A deductible) $0 61st thru 90th day All but $289 a day $289 a day $0 91st day and after: — While using 60 lifetime
reserve days All but $578 a day $578 a day $0 — Once lifetime reserve
days are used:
— Additional 365 days $0 100% of Medicare-eligible expenses
$0**
— Beyond the additional 365 days $0 $0 All costs
SKILLED NURSING FACILITY CARE*
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts $0 $0 21st thru 100th day All but $144.50 a day Up to $144.50 a day $0 101st day and after $0 $0 All costs BLOOD First 3 pints $0 3 pints $0 Additional amounts 100% $0 $0 HOSPICE CARE You must meet Medicare’s requirements, including a doctor’s certification of terminal illness.
All but very limited co-payment/ coinsurance for outpatient drugs and inpatient respite care
Medicare co-payment/coinsurance
$0
**NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy’s “Core Benefits.” During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.
ACOCRNM Page 17 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN F
MEDICARE (PART B) – MEDICAL SERVICES – PER CALENDAR YEAR
*Once you have been billed $140 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible will have been met for the calendar year.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY MEDICAL EXPENSES – IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as Physician’s services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment,
First $140 of Medicare Approved Amounts* $0 $140 (Part B deductible) $0 Remainder of Medicare Approved Amounts Generally 80% Generally 20% $0
PART B EXCESS CHARGES (Above Medicare Approved Amounts) $0 100% $0 BLOOD First 3 pints $0 All costs $0 Next $140 of Medicare Approved amounts* $0 $140 (Part B deductible) $0 Remainder of Medicare Approved amounts 80% 20% $0 CLINICAL LABORATORY SERVICES – TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0
(continued)
ACOCRNM Page 16 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN F
MEDICARE (PART A) – HOSPITAL SERVICES – PER BENEFIT PERIOD
*A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and have not received skilled care in any other facility for 60 days in a row.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY HOSPITALIZATION* Semiprivate room and board, general nursing and miscellaneous services and supplies
First 60 days All but $1156 $1156 (Part A deductible) $0 61st thru 90th day All but $289 a day $289 a day $0 91st day and after: — While using 60 lifetime
reserve days All but $578 a day $578 a day $0 — Once lifetime reserve
days are used:
— Additional 365 days $0 100% of Medicare-eligible expenses
$0**
— Beyond the additional 365 days $0 $0 All costs
SKILLED NURSING FACILITY CARE*
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts $0 $0 21st thru 100th day All but $144.50 a day Up to $144.50 a day $0 101st day and after $0 $0 All costs BLOOD First 3 pints $0 3 pints $0 Additional amounts 100% $0 $0 HOSPICE CARE You must meet Medicare’s requirements, including a doctor’s certification of terminal illness.
All but very limited co-payment/ coinsurance for outpatient drugs and inpatient respite care
Medicare co-payment/coinsurance
$0
**NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy’s “Core Benefits.” During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.
ACOCRNM Page 17 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN F
MEDICARE (PART B) – MEDICAL SERVICES – PER CALENDAR YEAR
*Once you have been billed $140 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible will have been met for the calendar year.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY MEDICAL EXPENSES – IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as Physician’s services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment,
First $140 of Medicare Approved Amounts* $0 $140 (Part B deductible) $0 Remainder of Medicare Approved Amounts Generally 80% Generally 20% $0
PART B EXCESS CHARGES (Above Medicare Approved Amounts) $0 100% $0 BLOOD First 3 pints $0 All costs $0 Next $140 of Medicare Approved amounts* $0 $140 (Part B deductible) $0 Remainder of Medicare Approved amounts 80% 20% $0 CLINICAL LABORATORY SERVICES – TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0
(continued)

ACOCRNM Page 18 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN F
PARTS A & B
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY HOME HEALTH CARE MEDICARE APPROVED SERVICES
— Medically necessary skilled care services and medical supplies 100% $0 $0
— Durable medical equipment First $140 of Medicare Approved Amounts* $0 $140 (Part B deductible) $0 Remainder of Medicare Approved Amounts 80% 20% $0
OTHER SERVICES – NOT COVERED BY MEDICARE
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY FOREIGN TRAVEL – NOT COVERED BY MEDICARE Medically necessary emergency care services beginning during the first 60 days of each trip outside the USA
First $250 each calendar year $0 $0 $250
Remainder of charges $0 80% to a lifetime maximum benefit of $50,000
20% and amounts over the $50,000 lifetime maximum
ACOCRNM Page 19 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN G
MEDICARE (PART A) – HOSPITAL SERVICES – PER BENEFIT PERIOD
*A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and have not received skilled care in any other facility for 60 days in a row.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY
HOSPITALIZATION* Semiprivate room and board, general nursing and miscellaneous services and supplies
First 60 days All but $1156 $1156 (Part A deductible) $0 61st thru 90th day All but $289 a day $289 a day $0 91st day and after: — While using 60 lifetime
reserve days All but $578 a day $578 a day $0 — Once lifetime reserve days
are used:
— Additional 365 days $0 100% of Medicare-eligible expenses
$0**
— Beyond the additional 365 days $0 $0 All costs
SKILLED NURSING FACILITY CARE*
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts $0 $0 21st thru 100th day All but $144.50 a day Up to $144.50 a day $0 101st day and after $0 $0 All costs
BLOOD First 3 pints $0 3 pints $0 Additional amounts 100% $0 $0
HOSPICE CARE
You must meet Medicare’s requirements, including a doctor’s certification of terminal illness.
All but very limited co-payment/ coinsurance for out-patient drugs and inpatient respite care
Medicare co-payment/coinsurance
$0
**NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy’s “Core Benefits.” During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.
ACOCRNM Page 18 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN F
PARTS A & B
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY HOME HEALTH CARE MEDICARE APPROVED SERVICES
— Medically necessary skilled care services and medical supplies 100% $0 $0
— Durable medical equipment First $140 of Medicare Approved Amounts* $0 $140 (Part B deductible) $0 Remainder of Medicare Approved Amounts 80% 20% $0
OTHER SERVICES – NOT COVERED BY MEDICARE
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY FOREIGN TRAVEL – NOT COVERED BY MEDICARE Medically necessary emergency care services beginning during the first 60 days of each trip outside the USA
First $250 each calendar year $0 $0 $250
Remainder of charges $0 80% to a lifetime maximum benefit of $50,000
20% and amounts over the $50,000 lifetime maximum
ACOCRNM Page 19 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN G
MEDICARE (PART A) – HOSPITAL SERVICES – PER BENEFIT PERIOD
*A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and have not received skilled care in any other facility for 60 days in a row.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY
HOSPITALIZATION* Semiprivate room and board, general nursing and miscellaneous services and supplies
First 60 days All but $1156 $1156 (Part A deductible) $0 61st thru 90th day All but $289 a day $289 a day $0 91st day and after: — While using 60 lifetime
reserve days All but $578 a day $578 a day $0 — Once lifetime reserve days
are used:
— Additional 365 days $0 100% of Medicare-eligible expenses
$0**
— Beyond the additional 365 days $0 $0 All costs
SKILLED NURSING FACILITY CARE*
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts $0 $0 21st thru 100th day All but $144.50 a day Up to $144.50 a day $0 101st day and after $0 $0 All costs
BLOOD First 3 pints $0 3 pints $0 Additional amounts 100% $0 $0
HOSPICE CARE
You must meet Medicare’s requirements, including a doctor’s certification of terminal illness.
All but very limited co-payment/ coinsurance for out-patient drugs and inpatient respite care
Medicare co-payment/coinsurance
$0
**NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy’s “Core Benefits.” During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.
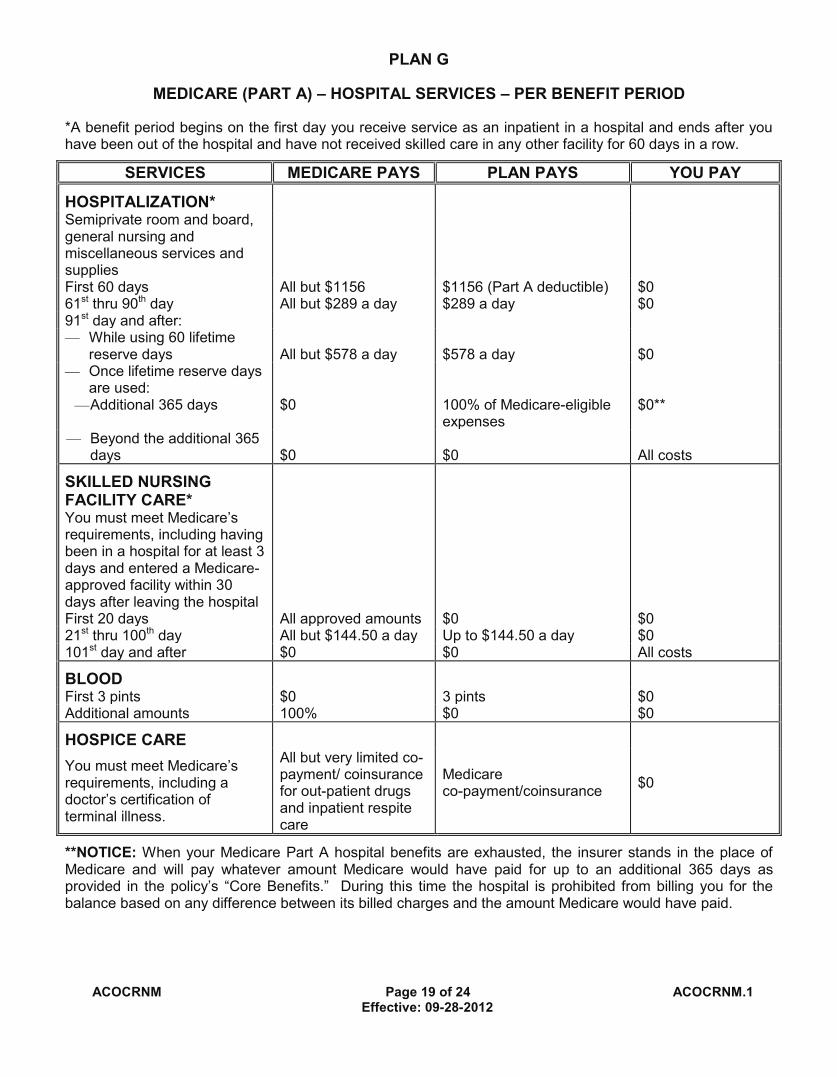
ACOCRNM Page 18 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN F
PARTS A & B
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY HOME HEALTH CARE MEDICARE APPROVED SERVICES
— Medically necessary skilled care services and medical supplies 100% $0 $0
— Durable medical equipment First $140 of Medicare Approved Amounts* $0 $140 (Part B deductible) $0 Remainder of Medicare Approved Amounts 80% 20% $0
OTHER SERVICES – NOT COVERED BY MEDICARE
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY FOREIGN TRAVEL – NOT COVERED BY MEDICARE Medically necessary emergency care services beginning during the first 60 days of each trip outside the USA
First $250 each calendar year $0 $0 $250
Remainder of charges $0 80% to a lifetime maximum benefit of $50,000
20% and amounts over the $50,000 lifetime maximum
ACOCRNM Page 19 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN G
MEDICARE (PART A) – HOSPITAL SERVICES – PER BENEFIT PERIOD
*A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and have not received skilled care in any other facility for 60 days in a row.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY
HOSPITALIZATION* Semiprivate room and board, general nursing and miscellaneous services and supplies
First 60 days All but $1156 $1156 (Part A deductible) $0 61st thru 90th day All but $289 a day $289 a day $0 91st day and after: — While using 60 lifetime
reserve days All but $578 a day $578 a day $0 — Once lifetime reserve days
are used:
— Additional 365 days $0 100% of Medicare-eligible expenses
$0**
— Beyond the additional 365 days $0 $0 All costs
SKILLED NURSING FACILITY CARE*
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts $0 $0 21st thru 100th day All but $144.50 a day Up to $144.50 a day $0 101st day and after $0 $0 All costs
BLOOD First 3 pints $0 3 pints $0 Additional amounts 100% $0 $0
HOSPICE CARE
You must meet Medicare’s requirements, including a doctor’s certification of terminal illness.
All but very limited co-payment/ coinsurance for out-patient drugs and inpatient respite care
Medicare co-payment/coinsurance
$0
**NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy’s “Core Benefits.” During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.
ACOCRNM Page 18 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN F
PARTS A & B
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY HOME HEALTH CARE MEDICARE APPROVED SERVICES
— Medically necessary skilled care services and medical supplies 100% $0 $0
— Durable medical equipment First $140 of Medicare Approved Amounts* $0 $140 (Part B deductible) $0 Remainder of Medicare Approved Amounts 80% 20% $0
OTHER SERVICES – NOT COVERED BY MEDICARE
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY FOREIGN TRAVEL – NOT COVERED BY MEDICARE Medically necessary emergency care services beginning during the first 60 days of each trip outside the USA
First $250 each calendar year $0 $0 $250
Remainder of charges $0 80% to a lifetime maximum benefit of $50,000
20% and amounts over the $50,000 lifetime maximum
ACOCRNM Page 19 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN G
MEDICARE (PART A) – HOSPITAL SERVICES – PER BENEFIT PERIOD
*A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and have not received skilled care in any other facility for 60 days in a row.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY
HOSPITALIZATION* Semiprivate room and board, general nursing and miscellaneous services and supplies
First 60 days All but $1156 $1156 (Part A deductible) $0 61st thru 90th day All but $289 a day $289 a day $0 91st day and after: — While using 60 lifetime
reserve days All but $578 a day $578 a day $0 — Once lifetime reserve days
are used:
— Additional 365 days $0 100% of Medicare-eligible expenses
$0**
— Beyond the additional 365 days $0 $0 All costs
SKILLED NURSING FACILITY CARE*
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts $0 $0 21st thru 100th day All but $144.50 a day Up to $144.50 a day $0 101st day and after $0 $0 All costs
BLOOD First 3 pints $0 3 pints $0 Additional amounts 100% $0 $0
HOSPICE CARE
You must meet Medicare’s requirements, including a doctor’s certification of terminal illness.
All but very limited co-payment/ coinsurance for out-patient drugs and inpatient respite care
Medicare co-payment/coinsurance
$0
**NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy’s “Core Benefits.” During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.

ACOCRNM Page 20 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN G
MEDICARE (PART B) – MEDICAL SERVICES-PER – CALENDAR YEAR
*Once you have been billed $140 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible will have been met for the calendar year.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY MEDICAL EXPENSES – IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as Physician’s services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment
First $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts Generally 80% Generally 20% $0
PART B EXCESS CHARGES (Above Medicare Approved Amounts) $0 100% $0 BLOOD First 3 pints $0 All costs $0 Next $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0 CLINICAL LABORATORY SERVICES – TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0
(continued)
ACOCRNM Page 21 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN G PARTS A & B
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY HOME HEALTH CARE MEDICARE APPROVED SERVICES
— Medically necessary skilled care services and medical supplies 100% $0 $0
— Durable medical equipment First $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0
OTHER BENEFITS – NOT COVERED BY MEDICARE
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY FOREIGN TRAVEL – NOT COVERED BY MEDICARE
Medically necessary emergency care services beginning during the first 60 days of each trip outside the USA
First $250 each calendar year $0 $0 $250
Remainder of Charges $0 80% to a lifetime maximum benefit of $50,000.
20% and amounts over the $50,000 lifetime maximum
ACOCRNM Page 21 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN G PARTS A & B
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY HOME HEALTH CARE MEDICARE APPROVED SERVICES
— Medically necessary skilled care services and medical supplies 100% $0 $0
— Durable medical equipment First $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0
OTHER BENEFITS – NOT COVERED BY MEDICARE
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY FOREIGN TRAVEL – NOT COVERED BY MEDICARE
Medically necessary emergency care services beginning during the first 60 days of each trip outside the USA
First $250 each calendar year $0 $0 $250
Remainder of Charges $0 80% to a lifetime maximum benefit of $50,000.
20% and amounts over the $50,000 lifetime maximum

ACOCRNM Page 20 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN G
MEDICARE (PART B) – MEDICAL SERVICES-PER – CALENDAR YEAR
*Once you have been billed $140 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible will have been met for the calendar year.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY MEDICAL EXPENSES – IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as Physician’s services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment
First $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts Generally 80% Generally 20% $0
PART B EXCESS CHARGES (Above Medicare Approved Amounts) $0 100% $0 BLOOD First 3 pints $0 All costs $0 Next $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0 CLINICAL LABORATORY SERVICES – TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0
(continued)
ACOCRNM Page 21 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN G PARTS A & B
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY HOME HEALTH CARE MEDICARE APPROVED SERVICES
— Medically necessary skilled care services and medical supplies 100% $0 $0
— Durable medical equipment First $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0
OTHER BENEFITS – NOT COVERED BY MEDICARE
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY FOREIGN TRAVEL – NOT COVERED BY MEDICARE
Medically necessary emergency care services beginning during the first 60 days of each trip outside the USA
First $250 each calendar year $0 $0 $250
Remainder of Charges $0 80% to a lifetime maximum benefit of $50,000.
20% and amounts over the $50,000 lifetime maximum
ACOCRNM Page 21 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN G PARTS A & B
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY HOME HEALTH CARE MEDICARE APPROVED SERVICES
— Medically necessary skilled care services and medical supplies 100% $0 $0
— Durable medical equipment First $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0
OTHER BENEFITS – NOT COVERED BY MEDICARE
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY FOREIGN TRAVEL – NOT COVERED BY MEDICARE
Medically necessary emergency care services beginning during the first 60 days of each trip outside the USA
First $250 each calendar year $0 $0 $250
Remainder of Charges $0 80% to a lifetime maximum benefit of $50,000.
20% and amounts over the $50,000 lifetime maximum

ACOCRNM Page 22 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN N
MEDICARE (PART A) – HOSPITAL SERVICES – PER BENEFIT PERIOD *A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and have not received skilled care in any other facility for 60 days in a row.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY
HOSPITALIZATION*
Semiprivate room and board, general nursing and miscellaneous services and supplies
First 60 days All but $1156 $1156 (Part A deductible)
$0
61st thru 90th day All but $289 a day $289 a day $0 91st day and after: — While using 60 lifetime
reserve days All but $578 a day $578 a day $0 — Once lifetime reserve days
are used:
— Additional 365 days $0 100% of Medicare-eligible expenses
$0**
— Beyond the additional 365 days $0 $0 All costs
SKILLED NURSING FACILITY CARE*
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts $0 $0 21st thru 100th day All but $144.50 a day Up to $144.50 a day $0 101st day and after $0 $0 All costs
BLOOD
First 3 pints $0 3 pints $0 Additional amounts 100% $0 $0
HOSPICE CARE
You must meet Medicare’s requirements, including a doctor’s certification of terminal illness.
All but very limited co-payment/ coinsurance for outpatient drugs and inpatient respite care
Medicare co-payment/coinsurance
$0
**NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy’s “Core Benefits.” During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.
ACOCRNM Page 23 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN N
MEDICARE (PART B) – MEDICAL SERVICES – PER CALENDAR YEAR
*Once you have been billed $140 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible will have been met for the calendar year.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY MEDICAL EXPENSES – IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as Physician’s services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment,
First $140 of Medicare Approved Amounts*
$0 $0 $140 (Part B deductible)
Remainder of Medicare Approved Amounts
Generally 80% Balance, other than up to $20 per office visit and up to $50 per emergency room visit. The co-payment of up to $50 is waived if the insured is admitted to any hospital and the emergency visit is covered as a Medicare Part A expense.
Up to $20 per office visit and up to $50 per emergency room visit. The co-payment of up to $50 is waived if the insured is admitted to any hospital and the emergency visit is covered as a Medicare Part A expense.
PART B EXCESS CHARGES (Above Medicare Approved Amounts) $0 $0 All costs BLOOD First 3 pints $0 All costs $0 Next $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0 CLINICAL LABORATORY SERVICES – TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0
(continued)
ACOCRNM Page 23 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN N
MEDICARE (PART B) – MEDICAL SERVICES – PER CALENDAR YEAR
*Once you have been billed $140 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible will have been met for the calendar year.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY MEDICAL EXPENSES – IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as Physician’s services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment,
First $140 of Medicare Approved Amounts*
$0 $0 $140 (Part B deductible)
Remainder of Medicare Approved Amounts
Generally 80% Balance, other than up to $20 per office visit and up to $50 per emergency room visit. The co-payment of up to $50 is waived if the insured is admitted to any hospital and the emergency visit is covered as a Medicare Part A expense.
Up to $20 per office visit and up to $50 per emergency room visit. The co-payment of up to $50 is waived if the insured is admitted to any hospital and the emergency visit is covered as a Medicare Part A expense.
PART B EXCESS CHARGES (Above Medicare Approved Amounts) $0 $0 All costs BLOOD First 3 pints $0 All costs $0 Next $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0 CLINICAL LABORATORY SERVICES – TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0
(continued)

ACOCRNM Page 22 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN N
MEDICARE (PART A) – HOSPITAL SERVICES – PER BENEFIT PERIOD *A benefit period begins on the first day you receive service as an inpatient in a hospital and ends after you have been out of the hospital and have not received skilled care in any other facility for 60 days in a row.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY
HOSPITALIZATION*
Semiprivate room and board, general nursing and miscellaneous services and supplies
First 60 days All but $1156 $1156 (Part A deductible)
$0
61st thru 90th day All but $289 a day $289 a day $0 91st day and after: — While using 60 lifetime
reserve days All but $578 a day $578 a day $0 — Once lifetime reserve days
are used:
— Additional 365 days $0 100% of Medicare-eligible expenses
$0**
— Beyond the additional 365 days $0 $0 All costs
SKILLED NURSING FACILITY CARE*
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts $0 $0 21st thru 100th day All but $144.50 a day Up to $144.50 a day $0 101st day and after $0 $0 All costs
BLOOD
First 3 pints $0 3 pints $0 Additional amounts 100% $0 $0
HOSPICE CARE
You must meet Medicare’s requirements, including a doctor’s certification of terminal illness.
All but very limited co-payment/ coinsurance for outpatient drugs and inpatient respite care
Medicare co-payment/coinsurance
$0
**NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy’s “Core Benefits.” During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.
ACOCRNM Page 23 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN N
MEDICARE (PART B) – MEDICAL SERVICES – PER CALENDAR YEAR
*Once you have been billed $140 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible will have been met for the calendar year.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY MEDICAL EXPENSES – IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as Physician’s services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment,
First $140 of Medicare Approved Amounts*
$0 $0 $140 (Part B deductible)
Remainder of Medicare Approved Amounts
Generally 80% Balance, other than up to $20 per office visit and up to $50 per emergency room visit. The co-payment of up to $50 is waived if the insured is admitted to any hospital and the emergency visit is covered as a Medicare Part A expense.
Up to $20 per office visit and up to $50 per emergency room visit. The co-payment of up to $50 is waived if the insured is admitted to any hospital and the emergency visit is covered as a Medicare Part A expense.
PART B EXCESS CHARGES (Above Medicare Approved Amounts) $0 $0 All costs BLOOD First 3 pints $0 All costs $0 Next $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0 CLINICAL LABORATORY SERVICES – TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0
(continued)
ACOCRNM Page 23 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN N
MEDICARE (PART B) – MEDICAL SERVICES – PER CALENDAR YEAR
*Once you have been billed $140 of Medicare-approved amounts for covered services (which are noted with an asterisk), your Part B deductible will have been met for the calendar year.
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY MEDICAL EXPENSES – IN OR OUT OF THE HOSPITAL AND OUTPATIENT HOSPITAL TREATMENT, such as Physician’s services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment,
First $140 of Medicare Approved Amounts*
$0 $0 $140 (Part B deductible)
Remainder of Medicare Approved Amounts
Generally 80% Balance, other than up to $20 per office visit and up to $50 per emergency room visit. The co-payment of up to $50 is waived if the insured is admitted to any hospital and the emergency visit is covered as a Medicare Part A expense.
Up to $20 per office visit and up to $50 per emergency room visit. The co-payment of up to $50 is waived if the insured is admitted to any hospital and the emergency visit is covered as a Medicare Part A expense.
PART B EXCESS CHARGES (Above Medicare Approved Amounts) $0 $0 All costs BLOOD First 3 pints $0 All costs $0 Next $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0 CLINICAL LABORATORY SERVICES – TESTS FOR DIAGNOSTIC SERVICES 100% $0 $0
(continued)
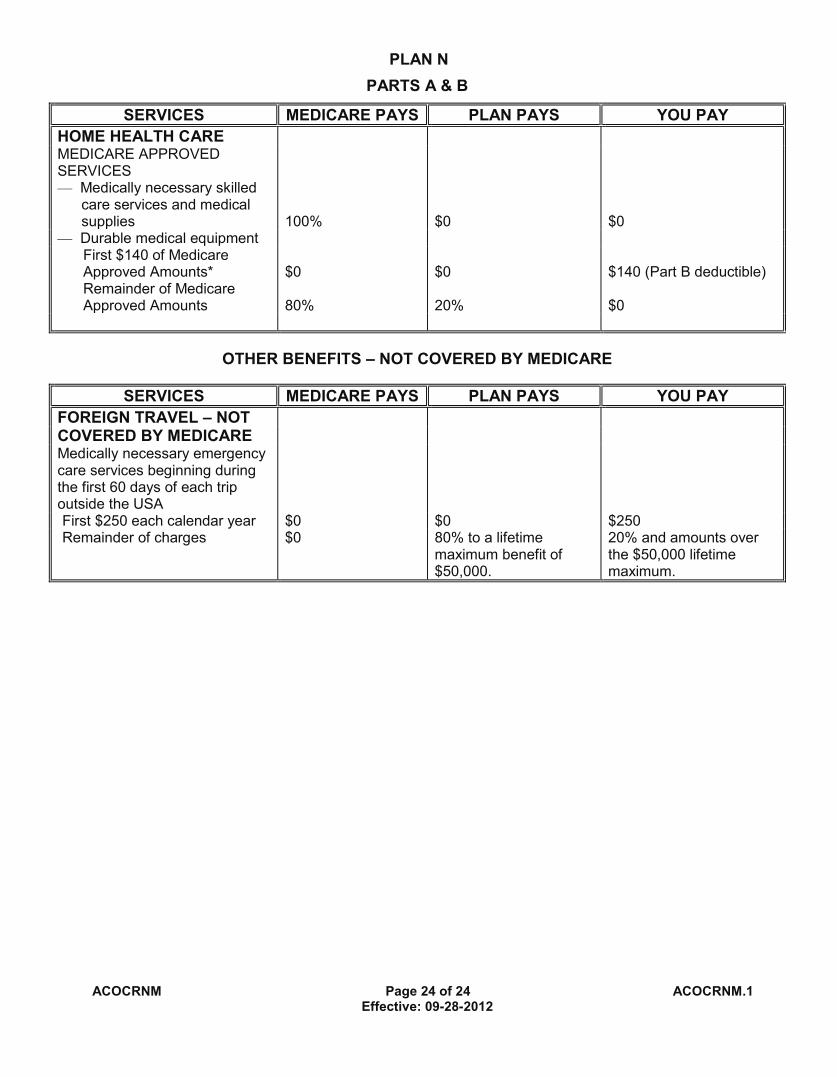
ACOCRNM Page 24 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN N PARTS A & B
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY HOME HEALTH CARE MEDICARE APPROVED SERVICES
— Medically necessary skilled care services and medical supplies 100% $0 $0
— Durable medical equipment First $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0
OTHER BENEFITS – NOT COVERED BY MEDICARE
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY FOREIGN TRAVEL – NOT COVERED BY MEDICARE Medically necessary emergency care services beginning during the first 60 days of each trip outside the USA
First $250 each calendar year $0 $0 $250 Remainder of charges $0 80% to a lifetime
maximum benefit of $50,000.
20% and amounts over the $50,000 lifetime maximum.
ACOCRNM Page 24 of 24 ACOCRNM.1 Effective: 09-28-2012
PLAN N PARTS A & B
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY HOME HEALTH CARE MEDICARE APPROVED SERVICES
— Medically necessary skilled care services and medical supplies 100% $0 $0
— Durable medical equipment First $140 of Medicare Approved Amounts* $0 $0 $140 (Part B deductible) Remainder of Medicare Approved Amounts 80% 20% $0
OTHER BENEFITS – NOT COVERED BY MEDICARE
SERVICES MEDICARE PAYS PLAN PAYS YOU PAY FOREIGN TRAVEL – NOT COVERED BY MEDICARE Medically necessary emergency care services beginning during the first 60 days of each trip outside the USA
First $250 each calendar year $0 $0 $250 Remainder of charges $0 80% to a lifetime
maximum benefit of $50,000.
20% and amounts over the $50,000 lifetime maximum.