Embed Size (px)
Citation preview

WHY DO SUBPERIOSTEAL IMPLANTS IN 2016
Severe maxillary and mandibular bone atrophies arenowadays successfully treated with bone regenerationtechniques and bone grafting techniques.However there are clinical cases in which such tech-niques cannot be performed for a number of differentclinical reasons such as severe diabetes1, other meta-bolic disorders, cancer, etc., or more simply becausethe patients reject this type of surgical approach forstrictly personal reasons such as significant budgetproblems2 or an untreatable terror to face a very in-vasive surgery.All such patients should not be abandoned to their to-tally unstable removable dentures.Their human casemust not be forgotten: as DDS we should constantlylook for a valid alternative option to solve their clinicalproblems.It is self evident that a leg amputee can barely movewith an old wood type leg, while he can even run,jump, dance, or ski, if equipped with the latest bio-mechatronic artificial leg. These sophisticated prosthe-ses in fact do allow amputees to regain a totallynormal life, getting rid of any physical and/or psycho-logical inability.It should be just as evident that people wearing den-
tures totally unstable because of a severe bone atro-phy do live an amputee syndrome, having lost thefunction of a basic organ : their mouth.This type of physical inability causes progressivespeech and food-chewing problems, with nutritionaldeficiences and loss of body weight. These conditionsoften cause psychic depression and/or permanentanxiety requiring specialized medical care.This type of inability is unrecognised or underesti-mated when it affects very old people, and given forgranted because of the age of the patients. This is in-deed a poor cultural heritage of past centuries stillcommonly diffused within our society today. On thecontrary this inability becomes dramatically evidentwhen it affects middle aged people or much youngerpeople. The common every day life, the family life,and the working social relations, all become dramat-ically problematic for these patients.In this article some clinical cases of severe bone atro-phy were selected, which were all affected by theabove stated amputee syndrome. None of thesecases could be treated with bone grafts. On the con-trary, these patients were all surgically treated withsubperiosteal implants supporting full arch dentures
WHY DOSUBPERIOSTEAL IMPLANTS IN 2016
by Giancarlo Cortese, MD, DDS
which proved to be perfectly stable in any conditionand circumstance since the very beginning. All thesepatients recovered very rapidly from the psychic de-pression and progressivly regained normal physicalconditions.A brief panoramic overview of these clinical cases isthe aim of this article to provide evidence that fullarch dentures firmly anchored and supported by sub-periosteal implants represent today a valid “lastshore” treatment option to let these patients regainthe function of their mouth with a 360 degree per-spective: chewing function, speech, smile, and facialaesthetics.Evidence will be provided that all such patients werebrought back to normal life standards with a mini-mally invasive surgery if compared to any full-archbone graft surgical approach, at lower costs for bothpatient and dentist, with totally predictable and rap-idly achieved final results which entirely fulfilled thefunctional and aesthetic demands of the patients.
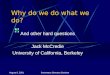
Case 1.Female patient, age 52, looking indeed much older(fig.1). Heavy smoker since decades, she wears a to-tally unstable full palate upper denture. She refers tohave lost several implants over the last years, and thatrecently she had received bilateral great sinus lift andimplants which both failed immediately after the ce-
ramic bridges had been loaded. The patient also re-ports that soon after the implants and bridges hadbeen removed, she have received bilateral huge bonegrafts which also failed and had to be removed.The patient appears to be evidently depressed, ex-plaining that at present she observes a strictly self-confined life, away from any social contact, becauseof her totally unstable and thick upper denture. In factthe patient must remove the denture in order to per-form perform an intelligible speech. She firmly rejectsany additional surgery based on bone regeneration orbone grafts. CAT scans and a stereolithographyc modelreveal the extent of the disastrous bone atrophy ofthe patient’s maxilla (fig. 2): the red line on the totallyflat palatal vault indicates where the centric occlusionshould be “if” she had an alveolar bone left where toput screw type implants.The patient accepts to receive a subperiosteal implantsurgery as her “last shore” to wear a stable implantsupported upper denture. Two separate subperiosteal
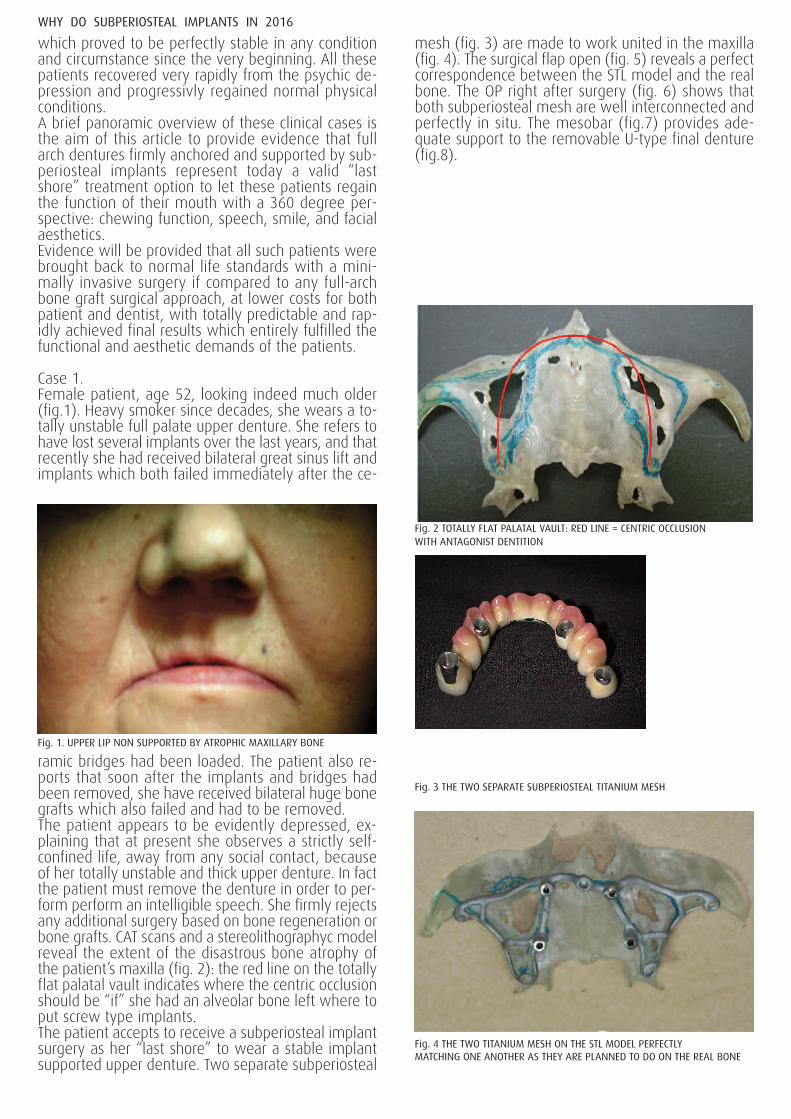
mesh (fig. 3) are made to work united in the maxilla(fig. 4). The surgical flap open (fig. 5) reveals a perfectcorrespondence between the STL model and the realbone. The OP right after surgery (fig. 6) shows thatboth subperiosteal mesh are well interconnected andperfectly in situ. The mesobar (fig.7) provides ade-quate support to the removable U-type final denture(fig.8).
WHY DO SUBPERIOSTEAL IMPLANTS IN 2016
Fig. 1. UPPER LIP NON SUPPORTED BY ATROPHIC MAXILLARY BONE
Fig. 2 TOTALLY FLAT PALATAL VAULT: RED LINE = CENTRIC OCCLUSIONWITH ANTAGONIST DENTITION
Fig. 3 THE TWO SEPARATE SUBPERIOSTEAL TITANIUM MESH
Fig. 4 THE TWO TITANIUM MESH ON THE STL MODEL PERFECTLYMATCHING ONE ANOTHER AS THEY ARE PLANNED TO DO ON THE REAL BONE
Case 2.Female patient, age 58. She declares to possess ananxious and insecure personality, to be very jalous ofher much younger and handsome husband, bank di-rector, who is daily surrounded by young andnicelooking female secretaries.She refers to wear a totally unstable upper denturewhich is the main cause of her unhappiness. Sherefers that due to the bone atrophy affecting herupper maxilla, three different surgeons have all pro-posed to give her a fixed full arch bridge, first by in-
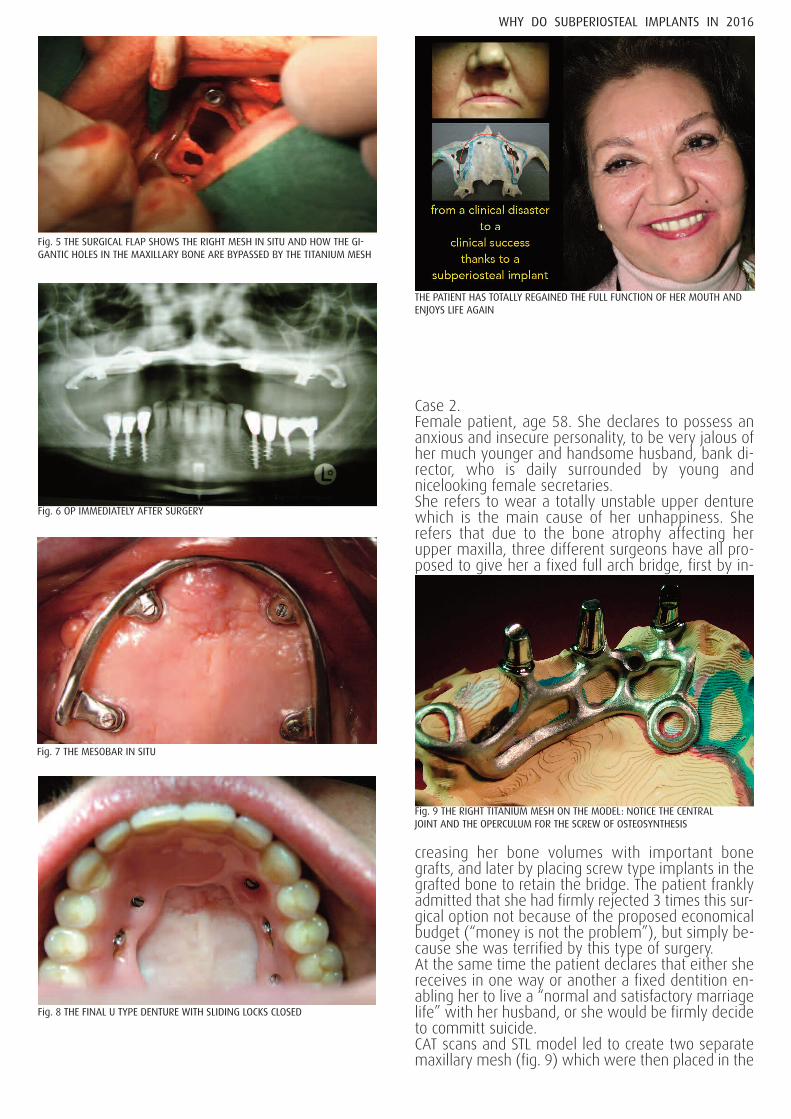
creasing her bone volumes with important bonegrafts, and later by placing screw type implants in thegrafted bone to retain the bridge. The patient franklyadmitted that she had firmly rejected 3 times this sur-gical option not because of the proposed economicalbudget (“money is not the problem”), but simply be-cause she was terrified by this type of surgery.At the same time the patient declares that either shereceives in one way or another a fixed dentition en-abling her to live a “normal and satisfactory marriagelife” with her husband, or she would be firmly decide to committ suicide.CAT scans and STL model led to create two separatemaxillary mesh (fig. 9) which were then placed in the
WHY DO SUBPERIOSTEAL IMPLANTS IN 2016
Fig. 5 THE SURGICAL FLAP SHOWS THE RIGHT MESH IN SITU AND HOW THE GI-GANTIC HOLES IN THE MAXILLARY BONE ARE BYPASSED BY THE TITANIUM MESH
Fig. 6 OP IMMEDIATELY AFTER SURGERY
Fig. 7 THE MESOBAR IN SITU
Fig. 8 THE FINAL U TYPE DENTURE WITH SLIDING LOCKS CLOSED
THE PATIENT HAS TOTALLY REGAINED THE FULL FUNCTION OF HER MOUTH ANDENJOYS LIFE AGAIN
Fig. 9 THE RIGHT TITANIUM MESH ON THE MODEL: NOTICE THE CENTRALJOINT AND THE OPERCULUM FOR THE SCREW OF OSTEOSYNTHESIS
WHY DO SUBPERIOSTEAL IMPLANTS IN 2016
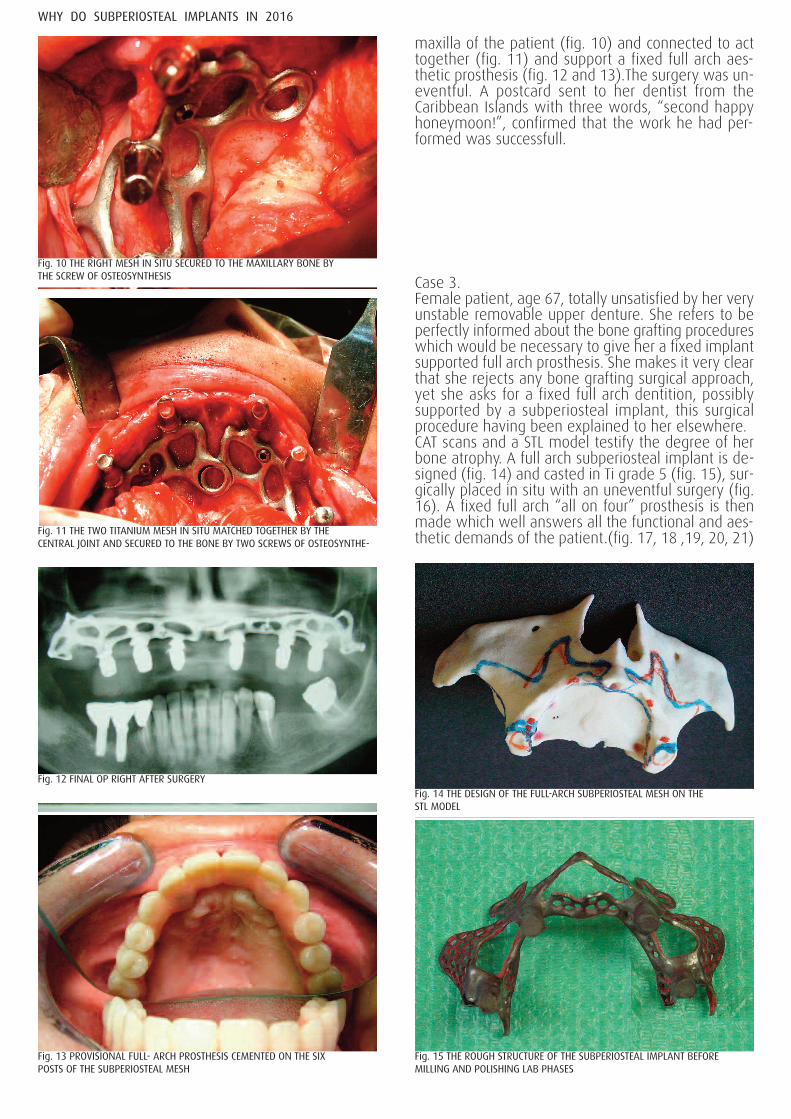
maxilla of the patient (fig. 10) and connected to acttogether (fig. 11) and support a fixed full arch aes-thetic prosthesis (fig. 12 and 13).The surgery was un-eventful. A postcard sent to her dentist from theCaribbean Islands with three words, “second happyhoneymoon!”, confirmed that the work he had per-formed was successfull.
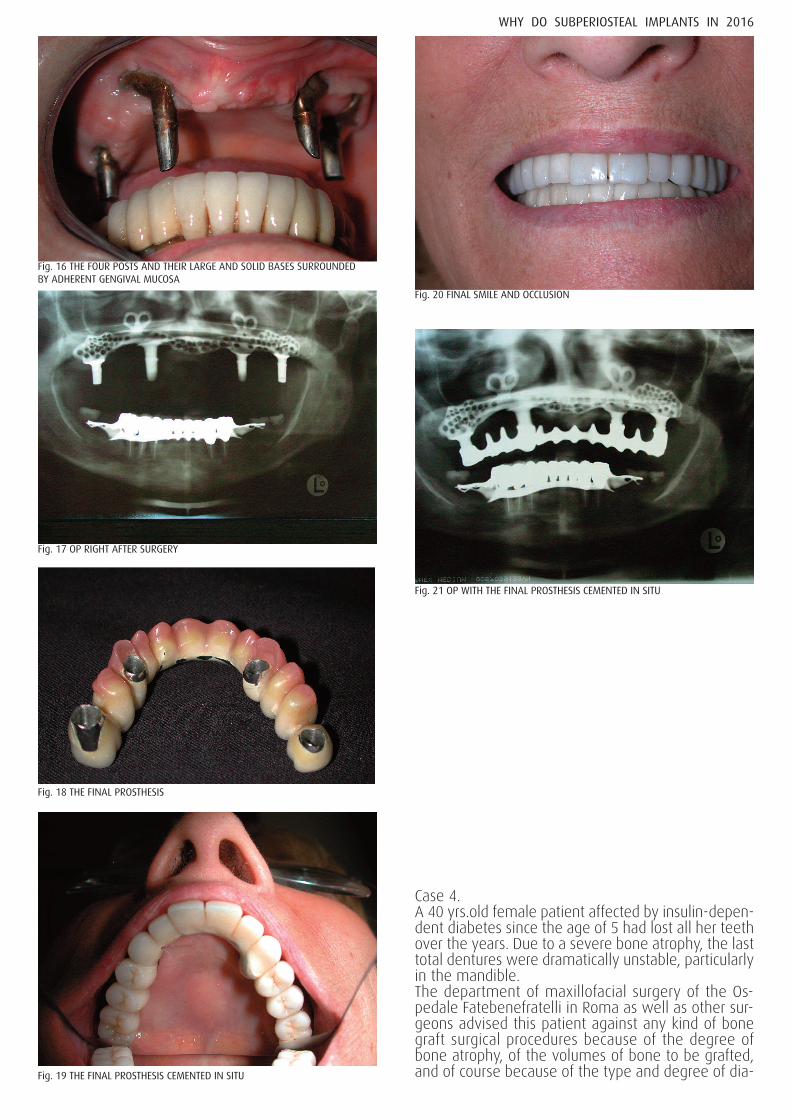
Case 3.Female patient, age 67, totally unsatisfied by her veryunstable removable upper denture. She refers to beperfectly informed about the bone grafting procedureswhich would be necessary to give her a fixed implantsupported full arch prosthesis. She makes it very clearthat she rejects any bone grafting surgical approach,yet she asks for a fixed full arch dentition, possiblysupported by a subperiosteal implant, this surgicalprocedure having been explained to her elsewhere.CAT scans and a STL model testify the degree of herbone atrophy. A full arch subperiosteal implant is de-signed (fig. 14) and casted in Ti grade 5 (fig. 15), sur-gically placed in situ with an uneventful surgery (fig.16). A fixed full arch “all on four” prosthesis is thenmade which well answers all the functional and aes-thetic demands of the patient.(fig. 17, 18 ,19, 20, 21)
Fig. 10 THE RIGHT MESH IN SITU SECURED TO THE MAXILLARY BONE BYTHE SCREW OF OSTEOSYNTHESIS
Fig. 11 THE TWO TITANIUM MESH IN SITU MATCHED TOGETHER BY THECENTRAL JOINT AND SECURED TO THE BONE BY TWO SCREWS OF OSTEOSYNTHE-
Fig. 12 FINAL OP RIGHT AFTER SURGERY
Fig. 13 PROVISIONAL FULL- ARCH PROSTHESIS CEMENTED ON THE SIXPOSTS OF THE SUBPERIOSTEAL MESH
Fig. 14 THE DESIGN OF THE FULL-ARCH SUBPERIOSTEAL MESH ON THESTL MODEL
Fig. 15 THE ROUGH STRUCTURE OF THE SUBPERIOSTEAL IMPLANT BEFOREMILLING AND POLISHING LAB PHASES
WHY DO SUBPERIOSTEAL IMPLANTS IN 2016
Case 4.A 40 yrs.old female patient affected by insulin-depen-dent diabetes since the age of 5 had lost all her teethover the years. Due to a severe bone atrophy, the lasttotal dentures were dramatically unstable, particularlyin the mandible.The department of maxillofacial surgery of the Os-pedale Fatebenefratelli in Roma as well as other sur-geons advised this patient against any kind of bonegraft surgical procedures because of the degree ofbone atrophy, of the volumes of bone to be grafted,and of course because of the type and degree of dia-
Fig. 16 THE FOUR POSTS AND THEIR LARGE AND SOLID BASES SURROUNDEDBY ADHERENT GENGIVAL MUCOSA
Fig. 17 OP RIGHT AFTER SURGERY
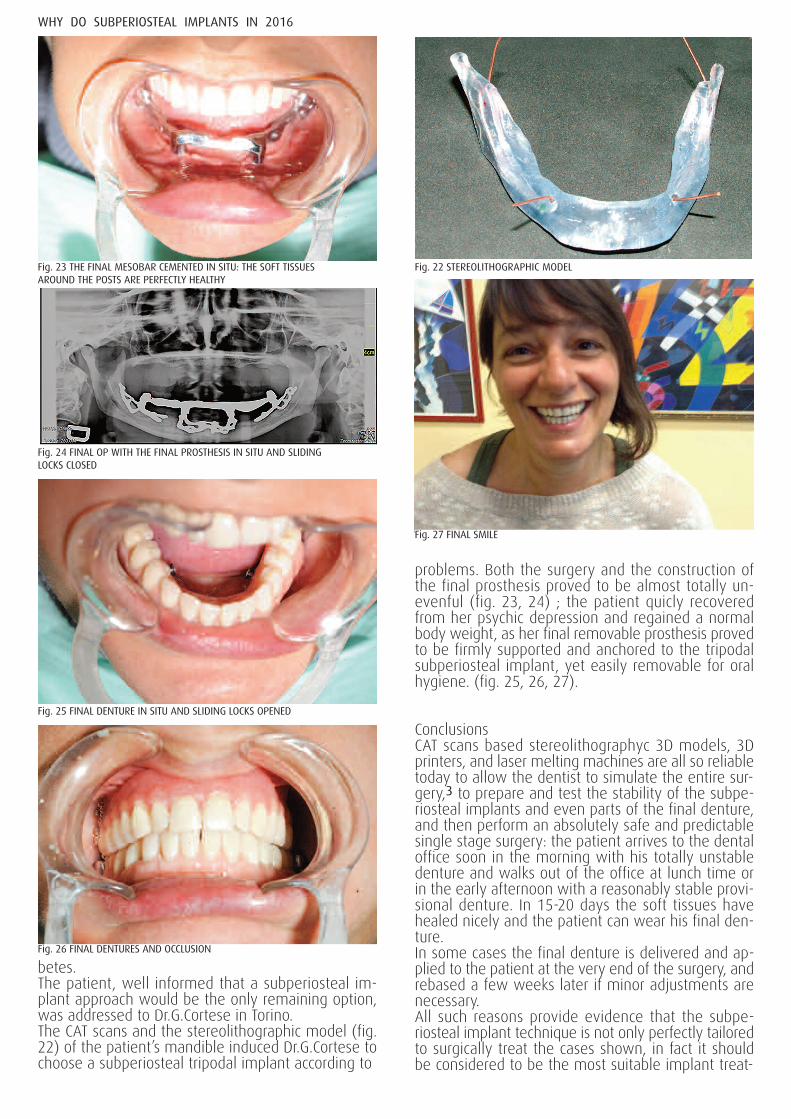
Fig. 18 THE FINAL PROSTHESIS
Fig. 19 THE FINAL PROSTHESIS CEMENTED IN SITU
Fig. 20 FINAL SMILE AND OCCLUSION
Fig. 21 OP WITH THE FINAL PROSTHESIS CEMENTED IN SITU
betes.The patient, well informed that a subperiosteal im-plant approach would be the only remaining option,was addressed to Dr.G.Cortese in Torino.The CAT scans and the stereolithographic model (fig.22) of the patient’s mandible induced Dr.G.Cortese tochoose a subperiosteal tripodal implant according to
L.I.Linkow as the most adequate implant to solve her-
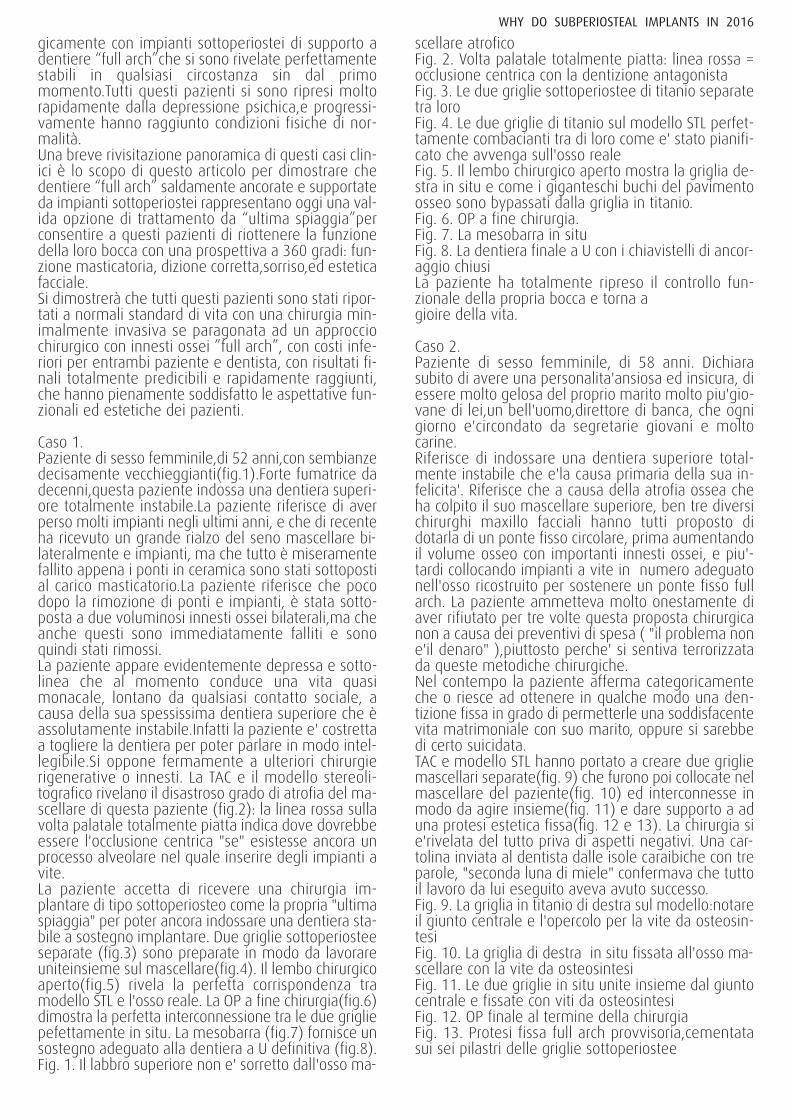
problems. Both the surgery and the construction ofthe final prosthesis proved to be almost totally un-evenful (fig. 23, 24) ; the patient quicly recoveredfrom her psychic depression and regained a normalbody weight, as her final removable prosthesis provedto be firmly supported and anchored to the tripodalsubperiosteal implant, yet easily removable for oralhygiene. (fig. 25, 26, 27).
ConclusionsCAT scans based stereolithographyc 3D models, 3Dprinters, and laser melting machines are all so reliabletoday to allow the dentist to simulate the entire sur-gery,3 to prepare and test the stability of the subpe-riosteal implants and even parts of the final denture,and then perform an absolutely safe and predictablesingle stage surgery: the patient arrives to the dentaloffice soon in the morning with his totally unstabledenture and walks out of the office at lunch time orin the early afternoon with a reasonably stable provi-sional denture. In 15-20 days the soft tissues havehealed nicely and the patient can wear his final den-ture.In some cases the final denture is delivered and ap-plied to the patient at the very end of the surgery, andrebased a few weeks later if minor adjustments arenecessary.All such reasons provide evidence that the subpe-riosteal implant technique is not only perfectly tailoredto surgically treat the cases shown, in fact it shouldbe considered to be the most suitable implant treat-
WHY DO SUBPERIOSTEAL IMPLANTS IN 2016
Fig. 23 THE FINAL MESOBAR CEMENTED IN SITU: THE SOFT TISSUESAROUND THE POSTS ARE PERFECTLY HEALTHY
Fig. 24 FINAL OP WITH THE FINAL PROSTHESIS IN SITU AND SLIDINGLOCKS CLOSED
Fig. 25 FINAL DENTURE IN SITU AND SLIDING LOCKS OPENED
Fig. 26 FINAL DENTURES AND OCCLUSION
Fig. 27 FINAL SMILE
Fig. 22 STEREOLITHOGRAPHIC MODEL

ment today in all cases of severe full arch bone atro-phy.Predictability, minor costs for both patient and dentist,rapidly achieved final results, immediate functionalload of the prosthesis, patient comfort right after sur-gery, single stage surgical session, no hospital recov-ery: indeed a sum of positive factors for all kinds ofpatients regardless of the age.Last but not least, the millions of aged people withmaxillary and/or mandibular bone atrophy within thegrowing number of the elderly population of any so-cially and culturally advanced country, from the U.S.A.to Europe, from Far East countries to Japan and China,are themselves a strong argument to highlight thecrucial importance to finance and promote further re-search on subperiosteal implant materials and de-vices, and surgical technique.
Key words amputee syndrome - severe bone atrophy - bonegrafts - subperiosteal mesh - CAT scans -stereolitho-graphic models - 3D printers - laser melting machines-immediate functional load.
References
1 Giancarlo Cortese,Enrico Moglioni,Paolo Diotallevi;A Tripodal Mandibular Subperiosteal Implant; Spec-trum Implants-Vol.6 N°2,summer 20015,46-51,Palmeri Publishing Co.
2 Cosimo Loperfido, Juan Mesquida, Jaime Lozada;Severe Mandibular Atrophy Treated With a Subpe-riosteal Implant and Simultaneous Graft With 2hBMP-2 and Mineralized Allograft: A case Report. Journal ofOral Implantology,Vol XL/No.SIX/2014
3 Peckitt N.S.; Stereoscopic Lithography and the man-ifacture of customized titanium implants in orofacialreconstruction; BJOMS 1999, 37, 353-369
Correspondence to:Dr.Giancarlo Cortese MD.,DDS.Corso Sommeiller 23, 10128 Torino (I)[email protected]@icloud.comwww.giancarlocortese.itoffice: 0039 011591732mobile: 0039 3381461208
TESTO ITALIANOPerchè fare impianti sottoperiosteinel 2016Giancarlo Cortese, MD,DDS
Le atrofie ossee gravi del mascellare o della mandi-bola vengono oggi trattate con successo utilizzandotecniche di osteo rigenerazione e tecniche di innestoosseo.Ci sono però casi clinici nei quali queste tecniche nonpossono essere utilizzate a causa di diverse ragionicliniche come ad esempio il diabete, altri disordinimetabolici, cancro etc., o più semplicemente perché ipazienti rifiutano questo tipo di approccio chirurgicoper motivi strettamente personali come significativiproblemi di budget o un vero e proprio terrore invin-cibile a sottoporsi a queste chirurgie molto invasive.Tutti questi pazienti non possono essere semplice-mente abbandonati alle loro dentiere assolutamenteinstabili.Il loro caso umano non può essere dimenti-cato: come DDS dobbiamo sempre cercare una validascelta alternativa per risolvere i loro problemi clinici.E’del tutto evidente che un individuo che ha subìto laamputazione di una gamba può appena muoversi conuna vecchia gamba di legno, mentre può addiritturacorrere, saltare, danzare,o sciare, se equipaggiato conuna delle più recenti gambe artificiali di tipo biomec-catronico.Infatti queste sofisticate protesi permettonoagli amputati di ritornare ad una vita totalmente nor-male, liberandosi da qualsiasi inabilità fisica e/opsichica.Dovrebbe essere altrettanto evidente che individuiche indossano dentiere totalmente instabili a causa diuna grave atrofia ossea, vivono una condizione di am-putato, avendo perso la funzione di un organo basi-lare: la loro bocca.Questo tipo di inabilità fisica genera problemi progres-sivi di fonazione e masticazione, con deficienze nu-trizionali e perdita di peso corporeo. Queste condizionispesso causano depressione psichica e/o ansia per-manente che finiscono per richiedere assistenza med-ica specializzata.Questo tipo di inabilità viene spesso sottostimato onon riconosciuto quando colpisce persone moltoanziane, e quindi dato per scontato a causa dell’etàdei pazienti. Ciò è veramente un pessimo retaggio cul-turale tipico dei secoli passati,che purtroppo è ancoradiffuso oggi nella nostra società. Al contrario, questotipo di inabilità diventa drammaticamente evidentequando colpisce persone di mezza età o anche per-sone più giovani.La normale routine quotidiana, lastessa vita di famiglia, e le relazioni sociali di lavorodiventano tutte drammaticamente problematiche perquesti pazienti.In questo articolo sono stati selezionati alcuni casi clin-ici tutti affetti da grave atrofia ossea, e tutti colpitidalla suddetta sindrome da amputazione. Nessuno diquesti casi poteva essere trattato con innesti ossei. Alcontrario questi pazienti sono tutti stati trattati chirur-
WHY DO SUBPERIOSTEAL IMPLANTS IN 2016
gicamente con impianti sottoperiostei di supporto adentiere “full arch”che si sono rivelate perfettamentestabili in qualsiasi circostanza sin dal primomomento.Tutti questi pazienti si sono ripresi moltorapidamente dalla depressione psichica,e progressi-vamente hanno raggiunto condizioni fisiche di nor-malità.Una breve rivisitazione panoramica di questi casi clin-ici è lo scopo di questo articolo per dimostrare chedentiere “full arch” saldamente ancorate e supportateda impianti sottoperiostei rappresentano oggi una val-ida opzione di trattamento da “ultima spiaggia”perconsentire a questi pazienti di riottenere la funzionedella loro bocca con una prospettiva a 360 gradi: fun-zione masticatoria, dizione corretta,sorriso,ed esteticafacciale.Si dimostrerà che tutti questi pazienti sono stati ripor-tati a normali standard di vita con una chirurgia min-imalmente invasiva se paragonata ad un approcciochirurgico con innesti ossei ”full arch”, con costi infe-riori per entrambi paziente e dentista, con risultati fi-nali totalmente predicibili e rapidamente raggiunti,che hanno pienamente soddisfatto le aspettative fun-zionali ed estetiche dei pazienti.
Caso 1.Paziente di sesso femminile,di 52 anni,con sembianzedecisamente vecchieggianti(fig.1).Forte fumatrice dadecenni,questa paziente indossa una dentiera superi-ore totalmente instabile.La paziente riferisce di averperso molti impianti negli ultimi anni, e che di recenteha ricevuto un grande rialzo del seno mascellare bi-lateralmente e impianti, ma che tutto è miseramentefallito appena i ponti in ceramica sono stati sottopostial carico masticatorio.La paziente riferisce che pocodopo la rimozione di ponti e impianti, è stata sotto-posta a due voluminosi innesti ossei bilaterali,ma cheanche questi sono immediatamente falliti e sonoquindi stati rimossi.La paziente appare evidentemente depressa e sotto-linea che al momento conduce una vita quasimonacale, lontano da qualsiasi contatto sociale, acausa della sua spessissima dentiera superiore che èassolutamente instabile.Infatti la paziente e' costrettaa togliere la dentiera per poter parlare in modo intel-legibile.Si oppone fermamente a ulteriori chirurgierigenerative o innesti. La TAC e il modello stereoli-tografico rivelano il disastroso grado di atrofia del ma-scellare di questa paziente (fig.2): la linea rossa sullavolta palatale totalmente piatta indica dove dovrebbeessere l'occlusione centrica "se" esistesse ancora unprocesso alveolare nel quale inserire degli impianti avite.La paziente accetta di ricevere una chirurgia im-plantare di tipo sottoperiosteo come la propria "ultimaspiaggia" per poter ancora indossare una dentiera sta-bile a sostegno implantare. Due griglie sottoperiosteeseparate (fig.3) sono preparate in modo da lavorareuniteinsieme sul mascellare(fig.4). Il lembo chirurgicoaperto(fig.5) rivela la perfetta corrispondenza tramodello STL e l'osso reale. La OP a fine chirurgia(fig.6)dimostra la perfetta interconnessione tra le due grigliepefettamente in situ. La mesobarra (fig.7) fornisce unsostegno adeguato alla dentiera a U definitiva (fig.8).Fig. 1. Il labbro superiore non e' sorretto dall'osso ma-
scellare atroficoFig. 2. Volta palatale totalmente piatta: linea rossa =occlusione centrica con la dentizione antagonistaFig. 3. Le due griglie sottoperiostee di titanio separatetra loroFig. 4. Le due griglie di titanio sul modello STL perfet-tamente combacianti tra di loro come e' stato pianifi-cato che avvenga sull'osso realeFig. 5. Il lembo chirurgico aperto mostra la griglia de-stra in situ e come i giganteschi buchi del pavimentoosseo sono bypassati dalla griglia in titanio.Fig. 6. OP a fine chirurgia.Fig. 7. La mesobarra in situFig. 8. La dentiera finale a U con i chiavistelli di ancor-aggio chiusiLa paziente ha totalmente ripreso il controllo fun-zionale della propria bocca e torna a gioire della vita.
Caso 2.Paziente di sesso femminile, di 58 anni. Dichiarasubito di avere una personalita'ansiosa ed insicura, diessere molto gelosa del proprio marito molto piu'gio-vane di lei,un bell'uomo,direttore di banca, che ognigiorno e'circondato da segretarie giovani e moltocarine.Riferisce di indossare una dentiera superiore total-mente instabile che e'la causa primaria della sua in-felicita'. Riferisce che a causa della atrofia ossea cheha colpito il suo mascellare superiore, ben tre diversichirurghi maxillo facciali hanno tutti proposto didotarla di un ponte fisso circolare, prima aumentandoil volume osseo con importanti innesti ossei, e piu'-tardi collocando impianti a vite in numero adeguatonell'osso ricostruito per sostenere un ponte fisso fullarch. La paziente ammetteva molto onestamente diaver rifiutato per tre volte questa proposta chirurgicanon a causa dei preventivi di spesa ( "il problema none'il denaro" ),piuttosto perche' si sentiva terrorizzatada queste metodiche chirurgiche.Nel contempo la paziente afferma categoricamenteche o riesce ad ottenere in qualche modo una den-tizione fissa in grado di permetterle una soddisfacentevita matrimoniale con suo marito, oppure si sarebbedi certo suicidata.TAC e modello STL hanno portato a creare due grigliemascellari separate(fig. 9) che furono poi collocate nelmascellare del paziente(fig. 10) ed interconnesse inmodo da agire insieme(fig. 11) e dare supporto a aduna protesi estetica fissa(fig. 12 e 13). La chirurgia sie'rivelata del tutto priva di aspetti negativi. Una car-tolina inviata al dentista dalle isole caraibiche con treparole, "seconda luna di miele" confermava che tuttoil lavoro da lui eseguito aveva avuto successo.Fig. 9. La griglia in titanio di destra sul modello:notareil giunto centrale e l'opercolo per la vite da osteosin-tesiFig. 10. La griglia di destra in situ fissata all'osso ma-scellare con la vite da osteosintesiFig. 11. Le due griglie in situ unite insieme dal giuntocentrale e fissate con viti da osteosintesiFig. 12. OP finale al termine della chirurgiaFig. 13. Protesi fissa full arch provvisoria,cementatasui sei pilastri delle griglie sottoperiostee
WHY DO SUBPERIOSTEAL IMPLANTS IN 2016
Caso 3.Paziente di sesso femminile,di 67 anni, totalmente in-soddisfatta della sua dentiera full arch superiore che,lei riferisce, e'assolutamente instabile. Riferisce di es-sere perfettamente informata circa le procedurechirurgiche di innesti ossei che sarebbero necessariper poterla dotare di una protesi fissa full archsostenuta da impianti a vite. Dichiara subito moltochiaramente che rifiuta qualsiasi approccio chirurgicocon innesti ossei. Al contrario richiede espressamenteun impianto sottoperiosteo che possa sostenere unaprotesi fissa full arch, questa tecnica chirurgica es-sendole stata dettagliatamente spiegata altrove.La TAC e il modello STL testimoniano il grado di atrofiadel suo mascellare superiore.Si disegna pertanto un impianto sottoperiosteo fullarch (fig. 14), fuso in titanio di grado 5 (fig. 15), cheviene poi collocato chirurgicamente in situ con unachirurgia del tutto priva di problemi (fig. 16). Unaprotesi fissa full arch "all on four" viene infine realiz-zata e indossata dalla paziente, che risponde pien-amente a tutte le sue aspettative estetiche efunzionali.(fig. 17,18,19,20,21)Fig. 14. Il disegno della griglia sottoperiostea sul mod-ello STLFig. 15. La struttura ancora grezza dell'impianto sot-toperiosteo prima di tutte le fasi di laboratorio di fre-saggio e rifinituraFig. 16. I 4 pilastri e le loro solide basi circondate damucosa gengivale aderente sanaFig. 17. OP a fine chirurgiaFig. 18. La protesi definitivaFig. 19. La protesi definitiva cementata in situFig. 20. Il sorriso finale e l'occlusioneFig. 21. OP della protesi finale cementata in situ.
Caso 4.Una paziente di sesso femminile di 40 anni affetta dadiabete insulino-dipendente sin dall'eta' di 5, avevaperso tutti i suoi denti nel corso degli anni. A causa diuna grave atrofia ossea le ultime dentiere eranodrammaticamente instabili, particolarmente sullamandibola.Il dipartimento di chirurgia maxillofacciale del-l'Ospedale Fatebenefratelli di Roma,cosi come altrichirurghi, aveva sconsigliato la paziente dal sottoporsia qualsiasi tipo di chirurgia con innesti ossei a causadel grado della sua atrofia ossea, dei volumi di ossoda innestare,e ovviamente del tipo e grado di diabete.La paziente, ben informata che un approccio chirurgicosottoperiosteo sarebbe stato la sua ultima opzione ri-masta, fu indirizzata al dr.G.Cortese in Torino.La TAC e il modello STL (fig. 22) della mandibola dellapaziente hanno indotto il dr.G.Cortese a scegliere unimpianto sottoperiosteo tripodale secondo L.I.Linkowcome l'impianto piu' adatto in assoluto per risolvere i prob-lemi della paziente. Entrambi la chirurgia e lacostruzione della protesi finale si sono svolti senzaproblemi particolari (fig. 23,24); la paziente si e' rap-idamente ristabilita dalla sua depressione psichica ri-tornando rapidamente ad un peso corporeo normale,la sua protesi finale rimovibile essendosi dimostrata saldamente ancorata esostenuta dall'impianto sottoperiosteo tripodale, e
contemporaneamente facilmente rimovibile perl'igiene orale.(fig.25,26,27)Fig. 22. Modello STL che evidenzia il grado di atrofiadella mandibolaFig. 23. La mesobarra definitiva cementata in situ: legengive attorno ai pilastri sono perfettamente saneFig. 24. OP finale con la protesi definitiva in situ e chi-avistelli di fissaggio chiusiFig. 25. Dentiera finale in situ e chiavistelli di fissaggioapertiFig. 26. Le dentiere definitive e l'occlusione finaleFig. 27. Sorriso finale della paziente
ConclusioniLe TAC e i modelli STL in 3D, le stampanti a 3D, e lemacchine per il laser melting sono nel complesso tutticosi affidabili oggigiorno da consentire al dentista disimulare l'intera chirurgia, di preparare e testare lastabilita' degli impianti sottoperiostei e anche partidella dentiera definitiva, e poi attuare una chirurgiamonofasica assolutamente sicura e predicibile: ilpaziente arriva allo studio dentistico presto in matti-nata con la sua dentiera totalmente instabile, ed escedallo studio circa per l'ora di pranzo o nelle prime oredel pomeriggio con una protesi provvisoria ragionevol-mente stabile. In 15-20 giorni i tessuti molli sono ben guariti ed il pazientepuo' indossare la sua protesi definitiva.In taluni casi la protesi finale viene consegnata alpaziente al termine della chirurgia, e ribasata dopoqualche settimana qualora piccoli aggiustamenti fos-sero necessari.Tutte queste ragioni comprovano l'evidenza che la tec-nica implantare sottoperiostea non e' solo "confezion-ata su misura" per trattare chirurgicamente i casimostrati, infatti dovrebbe essere considerata la migliore tecnica chirur-gica implantare disponibile oggi in tutti i casi di graveatrofia ossea full arch.Predicibilita', costi minori per entrambi dentista epaziente, risultati finali raggiungibili rapidamente,carico funzionale immediato della protesi, il confortgenerale del paziente a fine chirurgia, una singola ses-sione chirurgica, nessun ricovero ospedaliero : davverouna somma di fattori positivi per tutti i tipi di pazientiindipendentemente dall'eta'.Infine,ma non meno importante, i milioni di anzianicon atrofie ossee mascellari e/o mandibolari che sonoparte del crescente numero della popolazione anzianadi tutte le societa' culturalmente e socialmente avan-zate, dagli USA all'Europa, dai paesi del Sud Est Asi-atico al Giappone e alla Cina, sono essi stessi un forteargomento per evidenziare l'importanza cruciale di fi-nanziare e promuovere la ricerca sugli impianti sot-toperiostei, sui materiali sui mezzi e sulle tecnichechirurgiche ad essi correlati.
Parole chiaveSindrome da amputazione-grave atrofia ossea-innestiossei-griglie sottoperiostee-TAC-modelli stereoli-tografici-stampanti 3D-macchine per laser melting-carico funzionale immediato
WHY DO SUBPERIOSTEAL IMPLANTS IN 2016

![Subperiosteal bone proliferation at the tibia in ... · who have neurofibromatosis also have a congenital pseudarthrosis of the tibia [1]. is a subperiosteal haematoma which may lead](https://img.pdfslide.us/doc/110x75/604103a2383053274b34db04/subperiosteal-bone-proliferation-at-the-tibia-in-who-have-neurofibromatosis.jpg)