Embed Size (px)
Citation preview

L.NL.MA.09.2015.0058
Where are we
now in the long-
term management
of PAH and
CTEPH?
Hits and misses of
medical treatment Hap Farber
Boston University School of
Medicine, Boston, USA
ERS International
Congress 2015
Monday, 28 September

L.NL.MA.09.2015.0058
Disclosures
Honoraria:
– Actelion, Bayer HealthCare, Gilead
Consultancy:
– Actelion, Bayer HealthCare, Bristol Myers Squibb, Gilead, Ikaria,
United Therapeutics
Research grants:
– Gilead, United Therapeutics

L.NL.MA.09.2015.0058
Long-term management of PH
Issues in CTEPH
Issues in PAH

L.NL.MA.09.2015.0058
● Chronic
thromboembolic
pulmonary
hypertension
● Other pulmonary
artery obstructions
● Hematological
disorders
● Systemic disorders
● Metabolic disorders
● Others
Pulmonary hypertension is classified into five
main categories, based on etiology
BMPR2, bone morphogenetic protein 2.
Galie N et al. Eur Heart J 2015: doi:10.1093/eurheartj/ehv317.
● Idiopathic (IPAH)
● Heritable (BMPR2
and other mutations)
● Drug- and toxin-
induced
● Associated with
other conditions
(APAH)
WHO Group 1′
● Pulmonary veno-
occlusive disease
● Pulmonary capillary
hemangiomatosis
WHO Group 1′′
● Persistent pulmonary
hypertension of the
newborn (PPHN)
● Left ventricular
systolic dysfunction
● Left ventricular
diastolic dysfunction
● Valvular disease
● Congenital/acquired
left heart inflow/
outflow tract
obstruction and
congenital
cardiomyopathies
● Congenital/acquired
pulmonary veins
stenosis
● Chronic obstructive
pulmonary disease
● Interstitial lung
disease
● Other pulmonary
diseases with mixed
restrictive and
obstructive pattern
● Sleep-disordered
breathing
● Alveolar
hypoventilation
disorders
● Chronic exposure to
high altitude
● Developmental lung
diseases
GROUP 1 PAH
GROUP 2 Left-heart related
GROUP 3 Lung/hypoxia related
GROUP 4 CTEPH and other
PA obstructions
GROUP 5 Unclear multifactorial
Pulmonary hypertension
(ESC/ERS classification 2015)

L.NL.MA.09.2015.0058
Consider left heart disease and lung diseases by
symptoms, signs, risk factors, ECG, PFT + DLCO, chest
radiograph and HRCT, arterial blood gases
High or intermediate
Symptoms, signs, history suggestive of PH
Echocardiographic probability of PH
Consider other causes and/or follow-up
Low
V/Q scana
Mismatched perfusion defects?
No
Treat underlying disease
Diagnosis of left heart diseases or lung
diseases confirmed?
No signs of severe PH/RV dysfunction Signs of severe PH/RV dysfunction
Yes Yes
Refer to PH expert center
No
RHC
mPAP ≥25 mmHg, PWAP
≤15 mmHg, PVR >3 Wood units
Refer to PH expert center
CTEPH possible?
CT pulmonary angiography,
RHC +/- pulmonary angiography
PAH likely
Specific diagnostic tests
Yes
Heritable PAH Heritable
PVOD/PCH
CTD
Drugs - toxin
Schistosomiasis HIV
CHD
Portopulmonary
Idiopathic
PVOD/PCH Idiopathic PAH
A complete diagnostic work-up for PH should
always be performed to ensure the correct
diagnosis is made
CHD, congenital heart disease; CT, computed tomography; CTD, connective tissue disease; DLCO, diffusion capacity of the lung for carbon dioxide; ECG, electrocardiogram; HIV, human immunodeficiency virus; HRCT, high-resolution computed tomography; mPAP, mean pulmonary arterial pressure; PAWP, pulmonary artery wedge pressure; PFT, pulmonary function tests; PVOD/PCH, pulmonary veno-occlusive disease or pulmonary capillary hemangiomatosis; PVR, pulmonary vascular resistance; RHC, right heart catheterization; RV, right ventricular, V/Q, ventilation/perfusion.
Galiè N et al. Eur Heart J 2015:doi:10.1093/eurheart/ehv317.
aCT pulmonary angiography alone
may miss diagnosis of CTEPH.
Copyright protected content.
Please view original content in the following reference:
Galiè N et al. Eur Heart J 2015:doi:10.1093/eurheart/ehv317
Differential diagnosis is important because
the prognosis and treatment approaches
vary for different PH groups
L.NL.MA.09.2015.0058
ESC/ERS 2015 diagnostic guidelines
for CTEPH
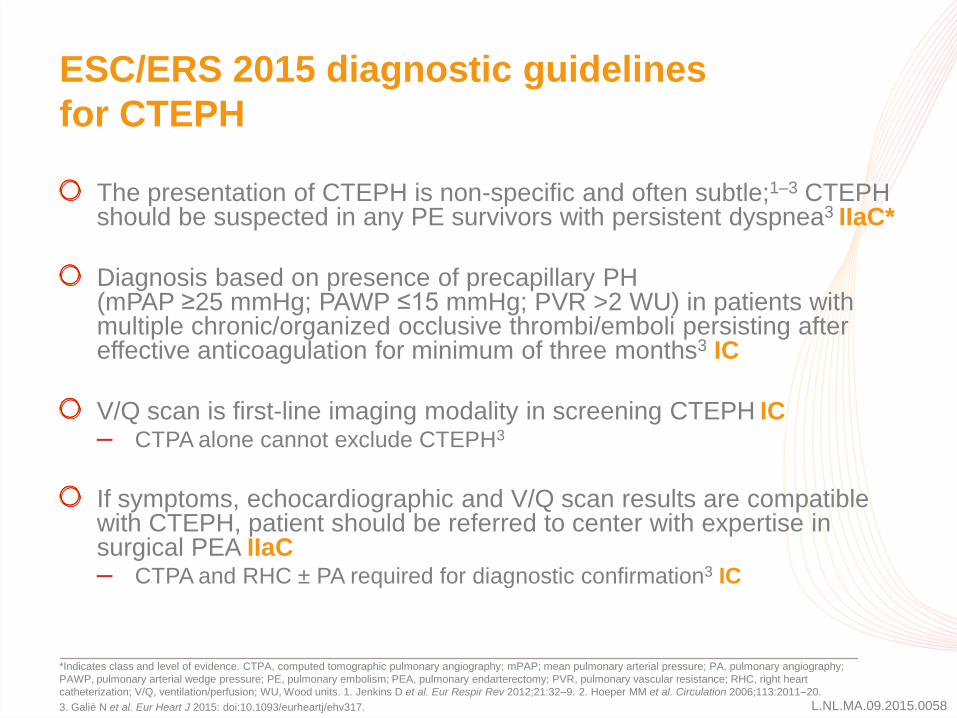
The presentation of CTEPH is non-specific and often subtle;1–3 CTEPH should be suspected in any PE survivors with persistent dyspnea3 IIaC*
Diagnosis based on presence of precapillary PH (mPAP ≥25 mmHg; PAWP ≤15 mmHg; PVR >2 WU) in patients with multiple chronic/organized occlusive thrombi/emboli persisting after effective anticoagulation for minimum of three months3 IC
V/Q scan is first-line imaging modality in screening CTEPH IC – CTPA alone cannot exclude CTEPH3
If symptoms, echocardiographic and V/Q scan results are compatible with CTEPH, patient should be referred to center with expertise in surgical PEA IIaC – CTPA and RHC ± PA required for diagnostic confirmation3 IC
*Indicates class and level of evidence. CTPA, computed tomographic pulmonary angiography; mPAP; mean pulmonary arterial pressure; PA. pulmonary angiography;
PAWP, pulmonary arterial wedge pressure; PE, pulmonary embolism; PEA, pulmonary endarterectomy; PVR, pulmonary vascular resistance; RHC, right heart
catheterization; V/Q, ventilation/perfusion; WU, Wood units. 1. Jenkins D et al. Eur Respir Rev 2012;21:32–9. 2. Hoeper MM et al. Circulation 2006;113:2011–20.
3. Galiè N et al. Eur Heart J 2015: doi:10.1093/eurheartj/ehv317.

L.NL.MA.09.2015.0058
Issues in CTEPH
Underdiagnosis or misdiagnosis results in many patients with
CTEPH being overlooked for potentially curative treatment with
PEA1,2
– Late diagnosis contributes to poor prognosis3
Widespread use of PAH-targeted medical therapies in CTEPH
– No robust evidence to support the efficacy of unapproved therapies in
patients with inoperable CTEPH and persistent/recurrent CTEPH
post-PEA
– Only riociguat has proven efficacy in these indications, based on robust
evidence from the CHEST studies4,5
PEA, pulmonary endarterectomy.
1. Jenkins D et al. Eur Respir Rev 2012;21:32–9. 2. Panduranga P, Mukhaini M. Ann Thorac Med 2011;6:43–5. 3. Olsson KM et al. Dtsch Arztebl Int
2014;111:856–62. 4. Ghofrani HA et al. N Engl J Med 2013;369:319–29. 5. Simonneau G et al. Eur Respir J 2014;44(Suppl.58):1802.

L.NL.MA.09.2015.0058
CTEPH: Pathophysiological similarities
with PAH
Controversy whether in situ thrombosis or embolic phenomenon
responsible for CTEPH1
Microscopic similarities between CTEPH and forms of PAH,
including plexogenic lesions2,3
Difficult to distinguish whether CTEPH leads to vasculopathic
pathology of PAH, or PAH leads to CTEPH4
1. Peacock A et al. Proc Am Thorac Soc 2006;608–14. 2. Pepke-Zaba J et al. Eur Respir J 2013;41:985–90. 3. Yi ES et al. Am J Respir Crit Care Med
2000;162:1577–86. 4. Berger G et al. IMAJ 2011;13:106–10.

L.NL.MA.09.2015.0058
Acute PE: Role in CTEPH?
~600,000 cases in US/year; up to 200,000 deaths/year1
Without treatment, mortality 30%; accurate diagnosis and appropriate
treatment reduces mortality to 2–8%2,3
PE prevalence and associated mortality
DVT, deep vein thrombosis; PE, pulmonary embolism.
1. Tapson V et al. Proc Am Thorac Soc 2006;3:564–7. 2. Fedullo P et al. Am J Respir Crit Care Med 2011;183:1605–13. 3. Vuylsteke A. PH and RV failure.
In Cardiovascular Critical Care, Griffiths M, Cordingley J, Price S (Eds). Wiley-Blackwell 2010; pp 367–82. 4. Lang I. Eur Respir Rev 2015;24:246–52.
5. Humbert M. Eur Respir Rev 2010;19:59–63.
Proportion of patients with PE-associated CTEPH Unclear why some patients with PE develop CTEPH2
– Most patients return to baseline functional status and normal hemodynamics
Occurrence is not precisely known:
– 0.4–9.1% of patients after acute PE4
– Thus, ~2400–54,600 CTEPH patients in US annually
Not all patients with CTEPH have a history of PE/DVT5

L.NL.MA.09.2015.0058
Follow-up testing for PH in PE survivors is inadequate
PE cases from national health claims database covering 70 million lives1
55%
7%
47%
20%
1% 0%
90%
16%
87%
34%
4% 2%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Any test V/Q scan Echo CTPA scan RHC PA
All patients (n=7,068)
PH subset (n=538)
V/Q scan is underutilized as a screening
modality P
rop
ort
ion
o
f p
op
ula
tio
n (
%)
a
(1-year incidence of PH = 7.6%)
V/Q scan performed during PH diagnostic workup in separate US QuERI
database:2
– 64.2% (n=433) in academic center
– 48.7% (n=353) in community center aComprising those listed on X-axis: CTPA, computed tomographic pulmonary angiography; Echo, echocardiography; PA, pulmonary angiogram; QuERI, Quality Enhancement
Research Initiative; RHC; right heart catheterization; V/Q, ventilation/perfusion.
1. Channick RN et al. Am J Respir Crit Care Med 2015;191:A4831. 2. McLaughlin VV et al. Chest 2013;143:324–32. 3. Zhang C et al. CJNMMI 2013;33:254–257.
100
80
60
40
20
0

L.NL.MA.09.2015.0058
Follow-up testing for PH in PE survivors is inadequate
PE cases from national health claims database covering 70 million lives1
55%
7%
47%
20%
1% 0%
90%
16%
87%
34%
4% 2%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Any test V/Q scan Echo CTPA scan RHC PA
All patients (n=7,068)
PH subset (n=538)
V/Q scan is underutilized as a screening
modality P
rop
ort
ion
o
f p
op
ula
tio
n (
%)
a
(1-year incidence of PH = 7.6%)
V/Q scan performed during PH diagnostic workup in separate US QuERI
database:2
– 64.2% (n=433) in academic center
– 48.7% (n=353) in community center aComprising those listed on X-axis: CTPA, computed tomographic pulmonary angiography; Echo, echocardiography; PA, pulmonary angiogram; QuERI, Quality Enhancement
Research Initiative; RHC; right heart catheterization; V/Q, ventilation/perfusion.
1. Channick RN et al. Am J Respir Crit Care Med 2015;191:A4831. 2. McLaughlin VV et al. Chest 2013;143:324–32. 3. Zhang C et al. CJNMMI 2013;33:254–257.
100
80
60
40
20
0
Utility as a screening modality3 V/Q scan
Multidetector CTPA
Sensitivity (%) 96.9 78.7
Specificity (%) 86.2 93.1
Accuracy (%) 93.4 84.2
Negative predictive value (%) 96.2 73.0

L.NL.MA.09.2015.0058
Treatment algorithm for CTEPH
BPA, balloon pulmonary angioplasty.
Galiè N et al. Eur Heart J 2015:doi:10.1093/eurheart/ehv317.
aTechnically operable patients with non-acceptable risk/benefit ratio can be considered also for BPA. bIn some centers medical therapy and BPA are initiated concurrently.
Diagnosis confirmed by
CTEPH expert center
Lifelong anticoagulation
Operability assessment by a
multidisciplinary CTEPH team
Technically operable Technically non-operable
Targeted medical
therapy
Consider BPA in
expert centerb
Persistent severe
symptomatic PH
Consider lung
transplantation
Persistent
symptomatic PH
Non-acceptable
risk:benefit ratioa
Acceptable
risk:benefit ratio
Pulmonary
endarterectomy
IC
IB
IIbC
Copyright protected content.
Please view original content in the following reference:
Galiè N et al. Eur Heart J 2015:doi:10.1093/eurheart/ehv317

L.NL.MA.09.2015.0058
Do you currently use riociguat in
treating CTEPH?
1. Yes
2. No
3. I do not treat CTEPH patients, I refer them
VOTE NOW!
L.NL.MA.09.2015.0058
Summary: CTEPH
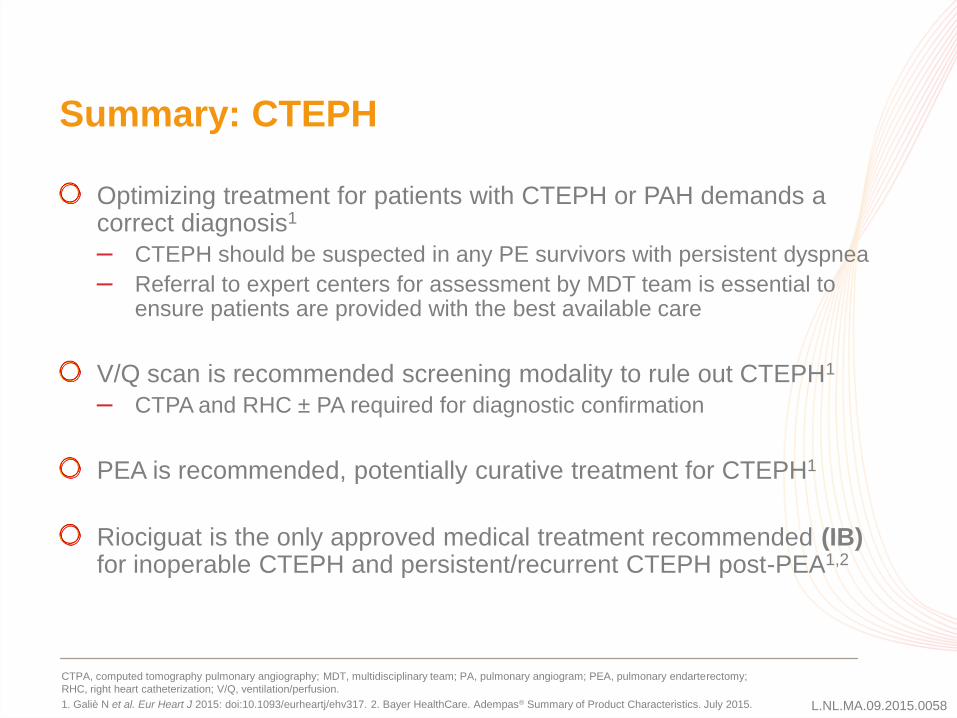
Optimizing treatment for patients with CTEPH or PAH demands a correct diagnosis1
– CTEPH should be suspected in any PE survivors with persistent dyspnea
– Referral to expert centers for assessment by MDT team is essential to ensure patients are provided with the best available care
V/Q scan is recommended screening modality to rule out CTEPH1
– CTPA and RHC ± PA required for diagnostic confirmation
PEA is recommended, potentially curative treatment for CTEPH1
Riociguat is the only approved medical treatment recommended (IB) for inoperable CTEPH and persistent/recurrent CTEPH post-PEA1,2
CTPA, computed tomography pulmonary angiography; MDT, multidisciplinary team; PA, pulmonary angiogram; PEA, pulmonary endarterectomy;
RHC, right heart catheterization; V/Q, ventilation/perfusion.
1. Galiè N et al. Eur Heart J 2015: doi:10.1093/eurheartj/ehv317. 2. Bayer HealthCare. Adempas® Summary of Product Characteristics. July 2015.

L.NL.MA.09.2015.0058
Long-term management of PH
Issues in CTEPH
Issues in PAH

L.NL.MA.09.2015.0058
Issues in PAH
Many patients do not achieve treatment goals,1 requiring escalation or change of therapy
Which treatment regimen?
– Monotherapy
– Dual combination therapy
– Triple combination therapy
When and how?
– Upfront
– Add-on
– Transition
Which drugs, and in what order?
Inefficacy, treatment
failure, adverse events
1. Badesch DB et al. Chest 2010;137:376–87.

L.NL.MA.09.2015.0058
Treatment algorithm for PAH
CCB, calcium channel blocker; DPAH, drug-induced pulmonary arterial hypertension; HPAH, hereditary pulmonary arterial hypertension; IPAH, idiopathic
pulmonary arterial hypertension; i.v., intravenous; PCA, prostacyclin analog; WHO FC, World Health Organization functional class.
Galiè N et al. Eur Heart J 2015:doi:10.1093/eurheart/ehv317.
aSome WHO-FC III patients may be considered high risk. bInitial combination with ambrisentan+tadalafil has proven to be superior to initial monotherapy with ambrisentan or tadalafil in delaying clinical failure. cIntravenous epoprostenol should be prioritized as it has reduced 3-month mortality in high-risk PAH patients also as monotherapy. dConsider also balloon atrial septostomy.
General measures
Supportive therapy
PAH confirmed by
expert center
Treatment-
naïve patient
Acute vasoreactivity test
(IPAH/HPAH/DPAH only)
Non-vasoreactive
Low or intermediate risk
(WHO FC II‒III)a
Initial monotherapyb Initial oral combinationb Initial oral combination
including i.v. PCAc
High risk
(WHO FC IV)a
Inadequate clinical response Patient already
on treatment
Vasoreactive
CCB
therapy
Consider referral for
lung transplantation
Double or triple sequential combination
Consider listing for lung transplantationd
Inadequate clinical response
Copyright protected content.
Please view original content in the following reference:
Galiè N et al. Eur Heart J 2015:doi:10.1093/eurheart/ehv317

L.NL.MA.09.2015.0058
ESC/ERS 2015 recommendations for monotherapy in PAH
APAH, associated pulmonary arterial hypertension; EMA, European Medicines Agency; IP, prostacyclin receptor; IPAH, idiopathic pulmonary arterial hypertension; RCT, randomized controlled trial; s.c., subcutaneous; WHO FC, World Health Organization functional class.Galiè N et al. Eur Heart J 2015:doi:10.1093/eurheart/ehv317.
Copyright protected content. Please view original content in the following reference:
Galiè N et al. Eur Heart J 2015:doi:10.1093/eurheart/ehv317
L.NL.MA.09.2015.0058
ESC/ERS 2015 recommendations for upfront
and sequential combination therapy in PAH
Upfront Sequential
Consideration: Dose adjustments and potential side effects may be simpler
to manage with sequential administration of combination partners
aClass of recommendation. bLevel of evidence. cSupporting references. dTime to clinical worsening as RCT primary endpoint, or drugs reducing all-cause mortality. eNo EMA
approval at time of publication.
EMA, European Medicines Agency; ERA, endothelin receptor antagonist; i.v. intravenous; PDE5i, phosphodiesterase type 5 inhibitor; s.c. subcutaneous; WHO FC, World Health Organization functional class. Galiè N et al. Eur Heart J 2015:doi:10.1093/eurheart/ehv317.
Copyright protected content.
Please view original content in the following reference:
Galiè N et al. Eur Heart J 2015:doi:10.1093/eurheart/ehv317

L.NL.MA.09.2015.0058
What do the majority of your PAH patients
receive?
1. Monotherapy
2. Dual combination therapy (upfront or sequential combination)
3. Triple combination therapy (upfront or sequential combination)
4. I refer my PAH patients
VOTE NOW!

L.NL.MA.09.2015.0058
18.5% 17.1% 11.1%
0.9%
21.1% 24.4%
16.1%
5.8% 7.4% 7.5% 4.8% 3.0%
0%
20%
40%
60%
80%
100%
ERA* PDE5 inhibitor* i.v./s.c. prostacyclin* Inhaled prostacyclin*
Pro
po
rtio
n o
f p
ati
en
tsc (%
)
Monotherapy Dual combinationa Triple combinationb
48% of patients (n=2438) were receiving monotherapy at time of study enrollment
REVEAL: Majority of patients with PAH receive
dual combination therapy
ERA, endothelin receptor antagonist; i.v., intravenous; PDE5, phosphodiesterase type 5; s.c., subcutaneous.
Badesch DB et al. Chest 2010;137;376–87.
Enrollment prior to approval of riociguat in 2014
*Percentages for each drug class add up to proportion of patients receiving that class in total population, e.g. 47% of patients received ERA. aCombination with one oral therapy or one prostanoid; bCombination with more than one other therapy; cProportion of overall population. Oral therapy defined as bosentan, sildenafil, ambrisentan, sitaxsentan, or tadalafil.
100
80
60
40
20
0

L.NL.MA.09.2015.0058
0
25
50
75
100
Pro
po
rtio
n o
f p
ati
en
ts
eve
nt-
fre
e (
%)
Time (weeks)
0 24 48 72 96 120 144 168 192
1 year
75.5%
Combination therapy
Pooled monotherapy*
2 years
63.2% 56.1%
3 years
AMBITION: Ambrisentan + tadalafil upfront
combination therapy improved time to clinical
worsening vs monotherapy1
*Pooled ambrisentan and tadalafil monotherapy arms of study. WHO FC, World Health Organization functional class.
1. Galiè G et al. Eur Respir J 2014;44(Suppl 58):2916. 2. Frost A et al. Am J Respir Crit Care Med 2015;191:A4781.
88.9%
79.7%
67.6%
Additional observations:
– Earlier initiation of upfront ambrisentan + tadalafil (WHO FC II) is more effective
than later initiation (WHO FC III) vs monotherapy2
Copyright protected content.
Please view original content in the following reference:
Galiè N et al. Eur Respir J 2014;44(Suppl 58):2916

L.NL.MA.09.2015.0058
Upfront triple combination therapy in PAH was
favorable in a small study population
Solid squares represent mean; boxes and diamonds represent SD; whiskers represent range. Enrollment between Dec 2007 and July 2012; observational
period ended in July 2013. Final follow-up: time-point of complete evaluation including right heart catheterization. 6MWD, 6-minute walking distance;
i.v., intravenous; PAP, pulmonary arterial pressure; PVR pulmonary vascular resistance. Sitbon O et al. Eur Respir J 2014;43:1691–7.
Improvements (p<0.01) in 6MWD and hemodynamics after 4 months’ therapy in
18 out of 19 patients who initiated the regimen
Retrospective pilot study of bosentan + sildenafil + i.v. epoprostenol
Copyright protected content.
Please view original content in the following reference:
Sitbon O et al. Eur Respir J 2014;43:1691–7.

L.NL.MA.09.2015.0058
Riociguat: a PH-targeted therapy with proven
long-term efficacy in both PAH and CTEPH
1. Ghofrani HA et al. N Engl J Med 2013;369:330–40. 2 Rubin LJ et al. Eur Respir J 2015 May;45:1303–13. 3. Simonneau G et al. Eur Respir J 2014;44(Suppl.58):P1802. 4 Ghofrani HA et al. N Engl J Med 2013;369:319–29. 5. Simonneau G et al. Eur Respir J 2015 ;45:1293–302. 6 Simonneau G et al. Eur Respir J 2014;44(Suppl.58):P1803. 7. Barst RJ et al. N Engl J Med 1996;334:296–301. 8. Simonneau G et al. Am J Respir Crit Care Med 2002;165:800–4. 9. Olschewski H et al. N Engl J Med 2002;347:322–9. 10. McLaughlin VV et al. J Am Coll Cardiol 2015;65(10S):A1538. 11. Rubin LJ et al. N Engl J Med 2002;346:896–903.12. Jaïs X et al. J Am Coll Cardiol 2008;52:2127–34. 13. Galiè N et al. Circulation 2008;117:3010–9. 14.GlaxoSmithKline. AMBER I. Available at: https://clinicaltrials.gov/ct2/show/NCT01884675 (accessed Aug 2015). 15. Pulido T et al. N Engl J Med 2013;369:809–1. 16. Actelion. MERIT-1. Available at: https://clinicaltrials.gov/ct2/show/NCT02021292 (accessed Aug 2015). 17. Galiè N et al. N Engl J Med 2005 353:2148–57. 18. Galiè N et al. Circulation 2009;119:2894–903.
Class Drug Randomized pivotal clinical trials in specific PH groups
PAH CTEPH
sGC stimulator Riociguat
PATENT-1 and -21–3
CHEST-1 and -24–6
Prostanoid
Epoprostenol
Barst (1996)7 –
Treprostinil
Simonneau (2002)8 –
Iloprost
AIR9 –
Selexipaga
GRIPHON10 –
ERA
Bosentan
BREATHE-111
BENEFiT12
Ambrisentan
ARIES-1 and -213 completed AMBER I14
Macitentan
SERAPHIN15
recruiting MERIT-116
PDE5 inhibitor
Sildenafil
SUPER-117 –
Tadalafil
PHIRST18 –
= Met primary endpoint
= Failed to meet primary endpoint
aNot currently approved. by European Medicines Agency.
ERA, endothelin receptor antagonist; PDE5, phosphodiesterase type 5; sGC, soluble guanylate cyclase.

L.NL.MA.09.2015.0058
Summary: PAH
Many patients with PAH do not achieve treatment goals, requiring escalation or change of therapy: – Increase dose or transition
– Combination of two or more drugs
Referral to expert centers for assessment by MDT team is essential to ensure patients are provided with the best available care
Initial monotherapy is recommended in treatment naïve, low or intermediate risk patients in WHO FC II−III
Combination therapy is an attractive option for patients in WHO FC II–IV: – Upfront dual therapy in WHO FC II–III
– Triple therapy in WHO FC III–IV
– Sequential add-on dual or triple therapy in patients with inadequate treatment response to initial approaches
MDT, multidisciplinary team; WHO FC, World Health Organization functional class.
Galiè N et al. Eur Heart J 2015: doi:10.1093/eurheartj/ehv317.

Thanks