Embed Size (px)
Citation preview

Please see Important Safety Information throughout and on pages 10 and 11, and accompanying full Prescribing Information, including BOXED WARNING for embryo-fetal toxicity.
WHO=World Health Organization.
INDICATION
OPSUMIT is an endothelin receptor antagonist (ERA) indicated for the treatment of pulmonary arterial hypertension (PAH, WHO Group I) to reduce the risks of disease progression and hospitalization for PAH.
Effectiveness was established in a long-term study in PAH patients with predominantly WHO Functional Class II-III symptoms treated for an average of 2 years. Patients had idiopathic and heritable PAH (57%), PAH caused by connective tissue disorders (31%), and PAH caused by congenital heart disease with repaired shunts (8%).
IMPORTANT SAFETY INFORMATION
BOXED WARNING: EMBRYO-FETAL TOXICITY Do not administer OPSUMIT to a pregnant female because it may cause fetal harm. Females of reproductive potential: Exclude pregnancy before the start of treatment, monthly during
treatment, and 1 month after stopping treatment. Prevent pregnancy during treatment and for one month after stopping treatment by using acceptable methods of contraception.
For all female patients, OPSUMIT is available only through a restricted program called the OPSUMIT Risk Evaluation and Mitigation Strategy (REMS).
In the treatment of pulmonary arterial hypertension (PAH, WHO Group I)
WHAT YOU START WITH...
Key milestones for OPSUMIT® (macitentan): from study results to continued commitment

742PATIENTS WERERANDOMIZED
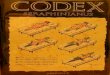
36%were not using PAH-speci�cbackground therapy atbaseline
64%were also using backgroundtherapy with PDE-5is or inhaled/oral prostanoids at baseline
OPSUMIT10 mg:n=242
Macitentan3 mg:n=250
Placebo:n=250
Macitentan 3 mg is not an approved dose.
61%PDE-5is,n=454
6%Inhaled or oralprostanoids,*
n=41
2 3
CONTRAINDICATIONS
Pregnancy: OPSUMIT may cause fetal harm when administered to a pregnant woman. OPSUMIT is contraindicated in females who are pregnant. If OPSUMIT is used during pregnancy, advise the patient of the potential risk to a fetus.
...CAN CHANGE THE OUTCOME Create a foundation based on clinical results
Trial design2-4
The effect of OPSUMIT® (macitentan) on disease progression in patients with PAH (WHO Group I) was studied in SERAPHIN, a large (N=742), event-driven, multicenter, long-term (average treatment duration 2 years), randomized, double-blind, placebo-controlled phase 3 trial. At study baseline, 36% of patients were not using PAH-specific background therapy and 64% were using background therapy with PDE-5is or inhaled/oral prostanoids.*
TRIAL DEMOGRAPHICS2
MONOTHERAPY AND COMBINATION THERAPY2,3
Trial demographics2-4
• Patients had predominantly WHO FC II (52%) and FC III (46%) symptoms
• Etiologies included IPAH/HPAH (57%), PAH-CTD (31%), PAH-CHD with repaired shunts (8%), PAH associated with drugs and toxins (3%), and PAH-HIV (1%)
• Mean patient age was 46 years, and 77% of patients were female
• 25% of patients were recently diagnosed (<6 months) and 75% were previously diagnosed (≥6 months)
Please see Important Safety Information throughout and on pages 10 and 11, and accompanying full Prescribing Information, including BOXED WARNING for embryo-fetal toxicity.
*OPSUMIT is approved in combination with PDE-5is or inhaled prostanoids, but not oral prostanoids.
FC=functional class; HPAH=heritable PAH; IPAH=idiopathic PAH; PAH-CHD=PAH associated with congenital heart disease; PAH-CTD=PAH associated with connective tissue disorders; PAH-HIV=PAH associated with human immunodeficiency virus; PDE-5i=phosphodiesterase type 5 inhibitor; SERAPHIN=Study with an Endothelin Receptor Antagonist in Pulmonary Arterial Hypertension to Improve CliNical Outcome.
WARNINGS AND PRECAUTIONSEmbryo-fetal Toxicity and OPSUMIT REMS Program
Due to the risk of embryo-fetal toxicity, OPSUMIT is available for females only through a restricted program called the OPSUMIT REMS Program. For females of reproductive potential, exclude pregnancy prior to initiation of therapy, ensure use of acceptable contraceptive methods, and obtain monthly pregnancy tests.
Recruitment for the SERAPHIN clinical trial begins1 2008
SERAPHIN: The largest long-term, outcomes-based pivotal trial of an ERA in PAH2

100
90
80
70
60
50
40
30
20
10
00 6 12 18
MonthsPatients at risk242 208 187 171 155 91 41 OPSUMIT 10 mg250 188 160 135 122 64 23 Placebo
Eve
nt-f
ree
pati
ents
(%)
24 30 36
47Placebo%
63OPSUMIT 10 mg%
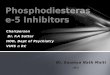
45%RISK REDUCTION
P<0.0001
HR 0.55; 97.5% CI, 0.39-0.76
OPSUMIT 10 mg(n=242), n (%)
Placebo(n=250), n (%)
Patients with primary endpoint event* 76 (31.4) 116 (46.4)
Component as �rst event
59 (24.4) 93 (37.2)Worsening PAH
16 (6.6) 17 (6.8)Death
Initiation of IV/SC prostanoids
1 (0.4) 6 (2.4)
100
90
80
70
60
50
40
30
20
10
00 6 12 18
MonthsPatients at risk154 134 119 107 97 53 24 OPSUMIT 10 mg154 122 106 90 80 40 10 Placebo
Eve
nt-
free
pat
ien
ts (%
)
24 30 36
49Placebo + background therapy%
63OPSUMIT + background therapy%
HR 0.62; 95% CI, 0.43-0.89
INCREMENTAL RISK REDUCTION OVER BACKGROUND THERAPY
38%
4 5
2013 FDA approves OPSUMIT as the first oral once-daily ERA with long-term (average treatment duration 2 years) outcomes data2
Start with OPSUMIT® (macitentan) in monotherapy or in combination therapy2
Primary endpoint in overall population: OPSUMIT significantly reduced the risk of disease progression by 45% vs placebo2
The primary endpoint in the SERAPHIN trial was time to the first occurrence of death or a significant morbidity event, defined as atrial septostomy, lung transplantation, initiation of IV or SC prostanoids, or clinical worsening of PAH (decrease in 6MWD of at least 15%, worsened PAH symptoms, and need for additional PAH treatment).2,3
Kaplan-Meier estimates of risk of first primary endpoint event in SERAPHIN2,3 Summary of primary endpoint events2
The beneficial effect of OPSUMIT was primarily attributable to a reduction in clinical worsening events (decrease in 6MWD of at least 15%, worsened PAH symptoms, and need for additional PAH treatment).
* No patients experienced an event of lung transplantation or atrial septostomy in the placebo or OPSUMIT 10 mg treatment groups.
WARNINGS AND PRECAUTIONS (continued)Embryo-fetal Toxicity and OPSUMIT REMS Program (continued)Notable requirements of the OPSUMIT REMS Program include:■ Prescribers must be certified with the program by enrolling and completing training.■ All females, regardless of reproductive potential, must enroll in the OPSUMIT REMS Program prior to initiating OPSUMIT.
Male patients are not enrolled in the REMS.■ Females of reproductive potential must comply with the pregnancy testing and contraception requirements.■ Pharmacies must be certified with the program and must only dispense to patients who are authorized to receive OPSUMIT.
Please see Important Safety Information throughout and on pages 10 and 11, and accompanying full Prescribing Information, including BOXED WARNING for embryo-fetal toxicity.
*OPSUMIT is approved in combination with PDE-5is or inhaled prostanoids, but not oral prostanoids.
Hepatotoxicity■ ERAs have caused elevations of aminotransferases, hepatotoxicity, and liver failure. The incidence of elevated
aminotransferases in the SERAPHIN study >3 x ULN was 3.4% for OPSUMIT vs 4.5% for placebo, and >8 x ULN was 2.1% vs 0.4%, respectively. Discontinuations for hepatic adverse events were 3.3% for OPSUMIT vs 1.6% for placebo.
■ Obtain liver enzyme tests prior to initiation of OPSUMIT and repeat during treatment as clinically indicated.■ Advise patients to report symptoms suggesting hepatic injury (nausea, vomiting, right upper quadrant pain, fatigue,
anorexia, jaundice, dark urine, fever, or itching).
At baseline, 64% of enrolled patients were treated with a stable dose of PAH-specific background therapy (61% PDE-5is; 6% inhaled or oral prostanoids).2*
The combination therapy data on this page represent an exploratory analysis. Results should be interpreted with caution.
Exploratory subgroup analysis: Patients experienced a 38% incremental risk reduction when OPSUMIT was added to stable PAH-specific background therapy2,4
Kaplan-Meier estimates of risk of first primary endpoint event2,4,5
6MWD=6-minute walk distance; CI=confidence interval; HR=hazard ratio; IV=intravenous; SC=subcutaneous.
NO. OF EVENTS/NO. OF PATIENTSOPSUMIT 50/154Placebo 68/154

PVR
Mean PVR at BL for OPSUMIT:924 ± 532 dyn•sec/cm5†
37%median reductionin PVR vs placebo
Cardiac Index
Mean cardiac index at BL for OPSUMIT:2.55 ± 0.85 L/min/m2†
0.6L/min/m2
median increasein cardiac index vs placebo
NO. OF EVENTS/NO. OF PATIENTS 50%RISK REDUCTION
P<0.0001
OPSUMIT 50/242Placebo 84/250
HR 0.50; 97.5% CI, 0.34-0.75
OPSUMIT 37/154Placebo 49/154
HR 0.65; 95% CI, 0.42-0.99
NO. OF EVENTS/NO. OF PATIENTS35%INCREMENTAL
RISK REDUCTIONOVER BACKGROUND
THERAPY
6 7
2015ESC/ERS Guidelines recommend OPSUMIT added to sildenafil as an option for sequential combination therapy in PAH (WHO Group I) FC II-III patients6
OPSUMIT: Additional endpoints from the SERAPHIN trial
OPSUMIT® (macitentan) reduced the risk of PAH-related hospitalization in monotherapy and combination therapy2,3
Secondary endpoints in the overall populationSignificant improvement from baseline in 6MWD at Month 62,3
At Month 6, 6MWD had increased by a mean of 12.5 m in the group receiving OPSUMIT 10 mg (n=242); 6MWD decreased by a mean of 9.4 m in the placebo group (n=249) (placebo-corrected mean increase of 22.0 m; 97.5% CI, 3-41; P=0.0078).
Significant improvement from baseline in WHO FC at Month 62,3
At Month 6, 22% of patients in the OPSUMIT 10 mg group (n=242) experienced improvement of at least 1 WHO FC vs 13% of patients in the placebo group (n=249).*
Exploratory hemodynamic substudy within SERAPHIN
Improvement from baseline in key measures of hemodynamics at Month 6 (OPSUMIT: n=57, placebo: n=67)2,3,7
Please see Important Safety Information throughout and on pages 10 and 11, and accompanying full Prescribing Information, including BOXED WARNING for embryo-fetal toxicity.
*P=0.006.3
†Plus-minus values are mean ± standard deviation.
BL=baseline; ERS=European Respiratory Society; ESC=European Society of Cardiology; PVR=pulmonary vascular resistance.
Fluid Retention■ Peripheral edema and fluid retention are known consequences of PAH and ERAs. In the pivotal PAH study SERAPHIN, edema
was reported in 21.9% of the OPSUMIT group vs 20.5% for placebo.■ Patients with underlying left ventricular dysfunction may be at particular risk for developing significant fluid retention after
initiation of ERA treatment. In a small study of pulmonary hypertension due to left ventricular dysfunction, more patients in the OPSUMIT group developed significant fluid retention and had more hospitalizations due to worsening heart failure compared to placebo. Postmarketing cases of edema and fluid retention occurring within weeks of starting OPSUMIT, some requiring intervention with a diuretic or hospitalization for decompensated heart failure, have been reported.
Analysis of death due to PAH or PAH-related hospitalization2,3,5
A key secondary endpoint in SERAPHIN was death due to PAH or PAH-related hospitalizationThere was a 50% reduction in risk of PAH-related hospitalization vs placebo in the overall population (P<0.0001).
OVERALL POPULATIONSUBGROUP OF PATIENTS ON
COMBINATION THERAPY*
Combination therapy data represent an exploratory analysis and do not appear in the OPSUMIT full Prescribing Information. Results should be interpreted with caution.
Summary of death due to PAH and hospitalization due to PAH2
Fifty patients (20.7%) receiving OPSUMIT 10 mg experienced an event of hospitalization for PAH or death due to PAH vs 84 patients (33.6%) receiving placebo. The components were hospitalization for PAH (OPSUMIT, 45 [18.6%]; placebo, 79 [31.6%]) and death due to PAH (OPSUMIT, 5 [2.1%]; placebo, 5 [2.0%]).
* Combination therapy: Patients were also using background therapy with PDE-5is (61%) or inhaled/oral prostanoids (6%) at baseline. OPSUMIT is approved in combination with PDE-5is or inhaled prostanoids, but not oral prostanoids.
WARNINGS AND PRECAUTIONS (continued)Hepatotoxicity (continued)
■ If clinically relevant aminotransferase elevations occur, or if elevations are accompanied by an increase in bilirubin >2 x ULN, or by clinical symptoms of hepatotoxicity, discontinue OPSUMIT. Consider re-initiation of OPSUMIT when hepatic enzyme levels normalize in patients who have not experienced clinical symptoms of hepatotoxicity.

100
90
80
70
60
50
40
30
20
10
00 1 2 3
Time from treatment start (years)Patients at risk242 230 225 221 210 189 171 152 145 129 105 91 79 73 47 OPSUMIT 10 mg
Even
t-fr
ee p
atie
nts
(%)
4 5 6 7
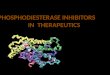
95.0%(91.3, 97.1) 89.1%
(84.4, 92.4)
73.3%(66.6, 78.9)
62.6%(54.6, 69.6)
PATIENTS TAKING OPSUMIT HAD A 63% ESTIMATE OF SURVIVAL AT 7 YEARS2,8
OPSUMIT 10 mg(n=242)
Placebo(n=249)
Anemia 13% 3%
Nasopharyngitis/pharyngitis 20% 13%
Bronchitis
Headache
In�uenza
Urinary tract infection
12%
14%
6%
9%
6%
9%
2%
6%
Adverse reactions more frequentwith OPSUMIT 10 mg vs placeboby ≥3%
OPSUMIT 10 mg(n=242)
Placebo(n=249)
ALT/AST elevations >3 x ULN 3.4% 4.5%
ALT/AST elevations >8 x ULN 2.1% 0.4%
Patients with Hgb <10 g/dL 8.7% 3.4%
OPSUMIT 10 mg(n=242)
Placebo(n=249)
Hypotension 7.0% 4.4%
Edema 21.9% 20.5%
Peripheraledema 18.2% 18.1%
MEDICATION EFFECT
Strong inducers of CYP3A4(eg, rifampin)
• Signi�cantly reduce macitentan exposure• Concomitant use of OPSUMIT with strong CYP3A4 inducers should be avoided
Strong inhibitors of CYP3A4(eg, ketoconazole)
• Approximately double macitentan exposure• Concomitant use of OPSUMIT with strong CYP3A4 inhibitors should be avoided• Use other PAH treatment options when strong CYP3A4 inhibitors are needed as part of HIV treatment (eg, ritonavir)
BCRP substrate drugs(riociguat and rosuvastatin)Cyclosporine AHormonal contraceptives (norethisterone and ethinyl estradiol)Sildena�lWarfarin
No clinically relevant interaction
8 9
OPSUMIT® (macitentan) has a well-studied safety and tolerability profile The only ERA with 7-year survival estimates2,8
Open-label extension data add to the understanding of the long-term use of OPSUMIT 2,82017
Incidence of elevated aminotransferases/ decreases in hemoglobin2
Postmarketing experience with OPSUMIT2
Because these adverse reactions are reported voluntarily during postapproval use of OPSUMIT from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.• Hypersensitivity reactions (angioedema, pruritus, and rash)• Nasal congestion• Elevations of liver aminotransferases (ALT, AST) and liver
injury; in most cases alternative causes could be identified (heart failure, hepatic congestion, autoimmune hepatitis). Endothelin receptor antagonists have been associated with elevations of aminotransferases, hepatotoxicity, and cases of liver failure
• Edema/fluid retention. Cases of edema and fluid retention occurred within weeks of starting OPSUMIT, some requiring intervention with a diuretic, fluid management, or hospitalization for decompensated heart failure
• Symptomatic hypotension
ALT=alanine aminotransferase; AST=aspartate aminotransferase; BCRP=breast cancer resistance protein; CYP=cytochrome P450; Hgb=hemoglobin; HIV=human immunodeficiency virus; ULN=upper limit of normal.
In long-term follow-up of patients who were treated with OPSUMIT 10 mg in the placebo-controlled study (n=242) and the open-label extension study (n=182), Kaplan-Meier estimates of survival at 1, 2, 5, and 7 years were 95%, 89%, 73%, and 63%, respectively. The median exposure to OPSUMIT was 4.6 years.2,8
Overall survival Kaplan-Meier curve for patients randomized to OPSUMIT 10 mg in SERAPHIN and entered into the open-label extension study 8
These data are from long-term follow-up and an open-label extension study. These uncontrolled observations do not allow comparison with a group not given OPSUMIT and cannot be used to determine the long-term effect of OPSUMIT on mortality.
Please see Important Safety Information throughout and on pages 10 and 11, and accompanying full Prescribing Information, including BOXED WARNING for embryo-fetal toxicity.
The incidence of peripheral edema was similar in OPSUMIT- and placebo-treated patients (18.2% and 18.1%, respectively).3
The overall incidence of treatment discontinuations due to adverse events with OPSUMIT was similar to placebo (approximately 11%).2
WARNINGS AND PRECAUTIONS (continued)
Fluid Retention (continued)■ Monitor for signs of fluid retention after OPSUMIT initiation. If clinically significant fluid retention develops, evaluate the
patient to determine the cause and the possible need to discontinue OPSUMIT.
Hemoglobin Decrease■ Decreases in hemoglobin concentration and hematocrit have occurred following administration of other ERAs and in clinical
studies with OPSUMIT. These decreases occurred early and stabilized thereafter. ■ In the SERAPHIN study, OPSUMIT caused a mean decrease in hemoglobin (from baseline to 18 months) of about 1.0 g/dL vs
no change in the placebo group. A decrease in hemoglobin to below 10.0 g/dL was reported in 8.7% of the OPSUMIT group vs 3.4% for placebo. Decreases in hemoglobin seldom require transfusion.
Adapted from Souza R et al. Poster presented at: American Thoracic Society Congress; May 19-24, 2017; Washington, DC, USA. Data presented are Kaplan-Meier survival estimates (95% CI).
Adverse reactions in the SERAPHIN study2 Additional adverse events of special interest3,4
Drug-drug interactions2

10 11
OPSUMIT® (macitentan) Important Safety Information
Please see accompanying full Prescribing Information, including BOXED WARNING for embryo-fetal toxicity.
INDICATION
OPSUMIT is an endothelin receptor antagonist (ERA) indicated for the treatment of pulmonary arterial hypertension (PAH, WHO Group I) to reduce the risks of disease progression and hospitalization for PAH.Effectiveness was established in a long-term study in PAH patients with predominantly WHO Functional Class II-III symptoms treated for an average of 2 years. Patients had idiopathic and heritable PAH (57%), PAH caused by connective tissue disorders (31%), and PAH caused by congenital heart disease with repaired shunts (8%).
IMPORTANT SAFETY INFORMATION
CONTRAINDICATIONS
Pregnancy: OPSUMIT may cause fetal harm when administered to a pregnant woman. OPSUMIT is contraindicated in females who are pregnant. If OPSUMIT is used during pregnancy, advise the patient of the potential risk to a fetus.
WARNINGS AND PRECAUTIONS
Embryo-fetal Toxicity and OPSUMIT REMS Program
Due to the risk of embryo-fetal toxicity, OPSUMIT is available for females only through a restricted program called the OPSUMIT REMS Program. For females of reproductive potential, exclude pregnancy prior to initiation of therapy, ensure use of acceptable contraceptive methods, and obtain monthly pregnancy tests.Notable requirements of the OPSUMIT REMS Program include: Prescribers must be certified with the program by
enrolling and completing training. All females, regardless of reproductive potential, must
enroll in the OPSUMIT REMS Program prior to initiating OPSUMIT. Male patients are not enrolled in the REMS.
Females of reproductive potential must comply with the pregnancy testing and contraception requirements.
Pharmacies must be certified with the program and must only dispense to patients who are authorized to receive OPSUMIT.
Hepatotoxicity ERAs have caused elevations of aminotransferases,
hepatotoxicity, and liver failure. The incidence of elevated aminotransferases in the SERAPHIN study >3 x ULN was 3.4% for OPSUMIT vs 4.5% for placebo, and >8 x ULN was 2.1% vs 0.4%, respectively. Discontinuations for hepatic adverse events were 3.3% for OPSUMIT vs 1.6% for placebo.
Obtain liver enzyme tests prior to initiation of OPSUMIT and repeat during treatment as clinically indicated.
Advise patients to report symptoms suggesting hepatic injury (nausea, vomiting, right upper quadrant pain, fatigue, anorexia, jaundice, dark urine, fever, or itching).
If clinically relevant aminotransferase elevations occur, or if elevations are accompanied by an increase in bilirubin >2 x ULN, or by clinical symptoms of hepatotoxicity,
discontinue OPSUMIT. Consider re-initiation of OPSUMIT when hepatic enzyme levels normalize in patients who have not experienced clinical symptoms of hepatotoxicity.
Fluid Retention Peripheral edema and fluid retention are known
consequences of PAH and ERAs. In the pivotal PAH study SERAPHIN, edema was reported in 21.9% of the OPSUMIT group vs 20.5% for placebo.
Patients with underlying left ventricular dysfunction may be at particular risk for developing significant fluid retention after initiation of ERA treatment. In a small study of pulmonary hypertension due to left ventricular dysfunction, more patients in the OPSUMIT group developed significant fluid retention and had more hospitalizations due to worsening heart failure compared to placebo. Postmarketing cases of edema and fluid retention occurring within weeks of starting OPSUMIT, some requiring intervention with a diuretic or hospitalization for decompensated heart failure, have been reported.
Monitor for signs of fluid retention after OPSUMIT initiation. If clinically significant fluid retention develops, evaluate the patient to determine the cause and the possible need to discontinue OPSUMIT.
Hemoglobin Decrease Decreases in hemoglobin concentration and hematocrit
have occurred following administration of other ERAs and in clinical studies with OPSUMIT. These decreases occurred early and stabilized thereafter.
In the SERAPHIN study, OPSUMIT caused a mean decrease in hemoglobin (from baseline to 18 months) of about 1.0 g/dL vs no change in the placebo group. A decrease in hemoglobin to below 10.0 g/dL was reported in 8.7% of the OPSUMIT group vs 3.4% for placebo. Decreases in hemoglobin seldom require transfusion.
Initiation of OPSUMIT is not recommended in patients with severe anemia. Measure hemoglobin prior to initiation of treatment and repeat during treatment as clinically indicated.
Pulmonary Edema with Pulmonary Veno-occlusive Disease (PVOD)
Should signs of pulmonary edema occur, consider the possibility of associated PVOD. If confirmed, discontinue OPSUMIT.
Decreased Sperm Counts
OPSUMIT, like other ERAs, may have an adverse effect on spermatogenesis. Counsel men about potential effects on fertility.
ADVERSE REACTIONS
Most common adverse reactions (more frequent than placebo by ≥3%) were anemia (13% vs 3%), nasopharyngitis/pharyngitis (20% vs 13%), bronchitis (12% vs 6%), headache (14% vs 9%), influenza (6% vs 2%), and urinary tract infection (9% vs 6%).
DRUG INTERACTIONS Strong inducers of CYP3A4 such as rifampin significantly
reduce macitentan exposure. Concomitant use of OPSUMIT with strong CYP3A4 inducers should be avoided.
Strong inhibitors of CYP3A4 like ketoconazole approximately double macitentan exposure. Many HIV drugs like ritonavir are strong inhibitors of CYP3A4. Avoid concomitant use of OPSUMIT with strong CYP3A4 inhibitors. Use other PAH treatment options when strong CYP3A4 inhibitors are needed as part of HIV treatment.
cp-113979
BOXED WARNING: EMBRYO-FETAL TOXICITY Do not administer OPSUMIT to a pregnant female
because it may cause fetal harm. Females of reproductive potential: Exclude
pregnancy before the start of treatment, monthly during treatment, and 1 month after stopping treatment. Prevent pregnancy during treatment and for one month after stopping treatment by using acceptable methods of contraception.
� For all female patients, OPSUMIT is available only through a restricted program called the OPSUMIT Risk Evaluation and Mitigation Strategy (REMS).

12
WARNINGS AND PRECAUTIONS (continued)
Hemoglobin Decrease (continued)■ Initiation of OPSUMIT is not recommended in patients with severe anemia. Measure hemoglobin prior to initiation of
treatment and repeat during treatment as clinically indicated.
Pulmonary Edema with Pulmonary Veno-occlusive Disease (PVOD)
Should signs of pulmonary edema occur, consider the possibility of associated PVOD. If confirmed, discontinue OPSUMIT.
Decreased Sperm Counts
OPSUMIT, like other ERAs, may have an adverse effect on spermatogenesis. Counsel men about potential effects on fertility.
Janssen is committed to supporting your patients
2020
Janssen CarePath is your one source for access, affordability, and treatment support for your patients
Access support to help navigate payer processes
Janssen CarePath helps verify insurance coverage for your patients taking OPSUMIT® (macitentan) and
provides reimbursement information
Affordability support to help your patients start and stay
on the treatment you prescribe
Janssen CarePath can help you find out what affordability
assistance may be available for your patients taking OPSUMIT®
Treatment support to help your patients get
informed and stay on OPSUMIT®
Janssen CarePath provides additional support to your patients,
including patient education and web-based resources
Call a Janssen CarePath Care Coordinator at 866-228-3546, Monday-Friday, 8:00 am to 8:00 pm ET.
Multilingual phone support available.
Visit JanssenCarePath.com/hcp/Opsumit
2008 2013 2015 2017 2020Recruitment for the SERAPHIN
clinical trial begins1
FDA approves OPSUMIT as the
first oral once-daily ERA with long-term (average treatment
duration 2 years) outcomes data2
ESC/ERS Guidelines recommend OPSUMIT
added to sildenafil as an option
for sequential combination therapy in PAH (WHO Group I)
FC II-III patients6
Open-label extension data
add to the understanding of the long-term use
of OPSUMIT2,8
More than 32,000 patients prescribed
OPSUMIT in the US since approval
in 20135*
OngoingContinued commitment
to PAH through:
• Patient support
• Clinical research including 7 ongoing phase 2 and 3 clinical trials through 2023
The ongoing commitment of Janssen to advancing the treatment of PAH
OPSUMIT® (macitentan) milestones from the past, present, and future
References: 1. Study of Macitentan (ACT-064992) on Morbidity and Mortality in Patients With Symptomatic Pulmonary Arterial Hypertension (SERAPHIN). National Institutes of Health, U.S. National Library of Medicine. https://clinicaltrials.gov/ct2/show/NCT00660179. Accessed April 22, 2019. 2. OPSUMIT [prescribing information]. South San Francisco, CA: Actelion Pharmaceuticals US, Inc. 3. Pulido T, Adzerikho I, Channick RN, et al; for the SERAPHIN Investigators. Macitentan and morbidity and mortality in pulmonary arterial hypertension. N Engl J Med. 2013;369:809-818 and Suppl 1-21. 4. Center for Drug Evaluation and Research, US Food and Drug Administration. Opsumit (macitentan) NDA 204410. http://www.accessdata.fda.gov/drugsatfda_docs/nda/2013/204410Orig1s000MedR.pdf. Accessed April 17, 2019. 5. Data on file, Janssen Pharmaceuticals, Inc. 6. Galiè N, Humbert M, Vachiery J-L, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS). Eur Respir J. 2015;46(4):903-975. 7. Galiè N, Jansa P, Pulido T, et al. SERAPHIN haemodynamic substudy: the effect of the dual endothelin receptor antagonist macitentan on haemodynamic parameters and NT-proBNP levels and their association with disease progression in patients with pulmonary arterial hypertension. Eur Heart J. 2017;38(15):1147-1155. 8. Souza R, Pulido T, Channick RN, et al. Long-term survival and safety with macitentan in patients with pulmonary arterial hypertension: results from the SERAPHIN study and its open-label extension. Poster presented at: American Thoracic Society Congress; May 19-24, 2017; Washington, DC, USA.
©2020 Actelion Pharmaceuticals US, Inc. All rights reserved. cp-115809v3 1220
Please see Important Safety Information throughout and on pages 10 and 11, and accompanying full Prescribing Information, including BOXED WARNING for embryo-fetal toxicity.
*As of April 2020.
13
ADVERSE REACTIONS
Most common adverse reactions (more frequent than placebo by ≥3%) were anemia (13% vs 3%), nasopharyngitis/pharyngitis (20% vs 13%), bronchitis (12% vs 6%), headache (14% vs 9%), influenza (6% vs 2%), and urinary tract infection (9% vs 6%).
DRUG INTERACTIONS■ Strong inducers of CYP3A4 such as rifampin significantly reduce macitentan exposure. Concomitant use of OPSUMIT with
strong CYP3A4 inducers should be avoided.■ Strong inhibitors of CYP3A4 like ketoconazole approximately double macitentan exposure. Many HIV drugs like ritonavir
are strong inhibitors of CYP3A4. Avoid concomitant use of OPSUMIT with strong CYP3A4 inhibitors. Use other PAH treatment options when strong CYP3A4 inhibitors are needed as part of HIV treatment.
OPSUMIT® (macitentan) is covered for Commercial and Medicare Part D Patients: 97% covered lives5†‡
OPSUMIT Voucher ProgramA free 30-day trial offer is available for eligible patients to help them become familiar with OPSUMIT®. At the conclusion of the program, you and your patient decide if it is appropriate to continue treatment.
Subject to 1 (one) use per product, per lifetime. Terms expire at the end of each calendar year and may change. This Voucher Program is open to patients who have commercial insurance, government coverage, or no insurance coverage; however, there is no guarantee of continuous accessibility after the program ends.
Support for patients using commercial or private insurance to pay for medicationJanssen CarePath Oral PAH Savings Program can help eligible patients save on their out-of-pocket medication costs for OPSUMIT®. Depending on their health insurance plan, savings may apply toward co-pay, co-insurance, or deductible. Your eligible patients will pay $5 per prescription fill with a $20,000 maximum program benefit per calendar year across all oral PAH therapies in the program. Not valid for patients using Medicare, Medicaid, or other government-funded programs to pay for their medications. Terms expire at the end of each calendar year and may change. There is no income requirement. See full eligibility requirements at Opsumit.JanssenCarePathSavings.com.
prescribed OPSUMIT® (macitentan)
Please see Important Safety Information throughout and on pages 10 and 11, and accompanying full Prescribing Information, including BOXED WARNING for embryo-fetal toxicity.
*As of April 2020.† 97.3% as of February 2020 in the US for all Commercial and Medicare Part D lives.‡ Collected on February 2020, and subject to change. This percentage may not represent 100% of formulary lives due to data limitations.
BOXED WARNING: EMBRYO-FETAL TOXICITY Do not administer OPSUMIT to a pregnant female because it may cause fetal harm. Females of reproductive potential: Exclude pregnancy before the start of treatment, monthly during
treatment, and 1 month after stopping treatment. Prevent pregnancy during treatment and for one month after stopping treatment by using acceptable methods of contraception.
For all female patients, OPSUMIT is available only through a restricted program called the OPSUMIT Risk Evaluation and Mitigation Strategy (REMS).
More than 32,000 patients prescribed OPSUMIT in the US since approval in 20135*
IMPORTANT SAFETY INFORMATION

2008 2013 2015 2017 2020Recruitment for the SERAPHIN
clinical trial begins1
FDA approves OPSUMIT as the
first oral once-daily ERA with long-term (average treatment
duration 2 years) outcomes data2
ESC/ERS Guidelines recommend OPSUMIT
added to sildenafil as an option
for sequential combination therapy in PAH (WHO Group I)
FC II-III patients6
Open-label extension data
add to the understanding of the long-term use
of OPSUMIT2,8
More than 32,000 patients prescribed
OPSUMIT in the US since approval
in 20135*
OngoingContinued commitment
to PAH through:
• Patient support
• Clinical research including 7 ongoing phase 2 and 3 clinical trials through 2023
The ongoing commitment of Janssen to advancing the treatment of PAH
OPSUMIT® (macitentan) milestones from the past, present, and future
References: 1. Study of Macitentan (ACT-064992) on Morbidity and Mortality in Patients With Symptomatic Pulmonary Arterial Hypertension (SERAPHIN). National Institutes of Health, U.S. National Library of Medicine. https://clinicaltrials.gov/ct2/show/NCT00660179. Accessed April 22, 2019. 2. OPSUMIT [prescribing information]. South San Francisco, CA: Actelion Pharmaceuticals US, Inc. 3. Pulido T, Adzerikho I, Channick RN, et al; for the SERAPHIN Investigators. Macitentan and morbidity and mortality in pulmonary arterial hypertension. N Engl J Med. 2013;369:809-818 and Suppl 1-21. 4. Center for Drug Evaluation and Research, US Food and Drug Administration. Opsumit (macitentan) NDA 204410. http://www.accessdata.fda.gov/drugsatfda_docs/nda/2013/204410Orig1s000MedR.pdf. Accessed April 17, 2019. 5. Data on file, Janssen Pharmaceuticals, Inc. 6. Galiè N, Humbert M, Vachiery J-L, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS). Eur Respir J. 2015;46(4):903-975. 7. Galiè N, Jansa P, Pulido T, et al. SERAPHIN haemodynamic substudy: the effect of the dual endothelin receptor antagonist macitentan on haemodynamic parameters and NT-proBNP levels and their association with disease progression in patients with pulmonary arterial hypertension. Eur Heart J. 2017;38(15):1147-1155. 8. Souza R, Pulido T, Channick RN, et al. Long-term survival and safety with macitentan in patients with pulmonary arterial hypertension: results from the SERAPHIN study and its open-label extension. Poster presented at: American Thoracic Society Congress; May 19-24, 2017; Washington, DC, USA.
©2020 Actelion Pharmaceuticals US, Inc. All rights reserved. cp-115809v3 1220
Please see Important Safety Information throughout and on pages 10 and 11, and accompanying full Prescribing Information, including BOXED WARNING for embryo-fetal toxicity.
*As of April 2020.
13
ADVERSE REACTIONS
Most common adverse reactions (more frequent than placebo by ≥3%) were anemia (13% vs 3%), nasopharyngitis/pharyngitis (20% vs 13%), bronchitis (12% vs 6%), headache (14% vs 9%), influenza (6% vs 2%), and urinary tract infection (9% vs 6%).
DRUG INTERACTIONS■ Strong inducers of CYP3A4 such as rifampin significantly reduce macitentan exposure. Concomitant use of OPSUMIT with
strong CYP3A4 inducers should be avoided.■ Strong inhibitors of CYP3A4 like ketoconazole approximately double macitentan exposure. Many HIV drugs like ritonavir
are strong inhibitors of CYP3A4. Avoid concomitant use of OPSUMIT with strong CYP3A4 inhibitors. Use other PAH treatment options when strong CYP3A4 inhibitors are needed as part of HIV treatment.
OPSUMIT® (macitentan) is covered for Commercial and Medicare Part D Patients: 97% covered lives5†‡
OPSUMIT Voucher ProgramA free 30-day trial offer is available for eligible patients to help them become familiar with OPSUMIT®. At the conclusion of the program, you and your patient decide if it is appropriate to continue treatment.
Subject to 1 (one) use per product, per lifetime. Terms expire at the end of each calendar year and may change. This Voucher Program is open to patients who have commercial insurance, government coverage, or no insurance coverage; however, there is no guarantee of continuous accessibility after the program ends.
Support for patients using commercial or private insurance to pay for medicationJanssen CarePath Oral PAH Savings Program can help eligible patients save on their out-of-pocket medication costs for OPSUMIT®. Depending on their health insurance plan, savings may apply toward co-pay, co-insurance, or deductible. Your eligible patients will pay $5 per prescription fill with a $20,000 maximum program benefit per calendar year across all oral PAH therapies in the program. Not valid for patients using Medicare, Medicaid, or other government-funded programs to pay for their medications. Terms expire at the end of each calendar year and may change. There is no income requirement. See full eligibility requirements at Opsumit.JanssenCarePathSavings.com.
prescribed OPSUMIT® (macitentan)
Please see Important Safety Information throughout and on pages 10 and 11, and accompanying full Prescribing Information, including BOXED WARNING for embryo-fetal toxicity.
*As of April 2020.† 97.3% as of February 2020 in the US for all Commercial and Medicare Part D lives.‡ Collected on February 2020, and subject to change. This percentage may not represent 100% of formulary lives due to data limitations.
BOXED WARNING: EMBRYO-FETAL TOXICITY Do not administer OPSUMIT to a pregnant female because it may cause fetal harm. Females of reproductive potential: Exclude pregnancy before the start of treatment, monthly during
treatment, and 1 month after stopping treatment. Prevent pregnancy during treatment and for one month after stopping treatment by using acceptable methods of contraception.
For all female patients, OPSUMIT is available only through a restricted program called the OPSUMIT Risk Evaluation and Mitigation Strategy (REMS).
More than 32,000 patients prescribed OPSUMIT in the US since approval in 20135*
IMPORTANT SAFETY INFORMATION