Embed Size (px)
Citation preview

1
Master Class for OncologistsWelcome to
Miami, FL
December 19, 2009
7:30 AM - 8:15 AMSession 1:
Update on Esophagogastric Cancers:Weighing the Therapeutic Options
Peter C. Enzinger, MDDana-Farber Cancer Institute
& Harvard Medical School
Presenter Disclosure Information
The following relationships exist related to this presentation:
• Dr Enzinger serves as a speaker/consultant for sanofi-aventis U.S., Pfizer Inc., Roche, Genentech, and ImClone/Bristol-Myers Squibb.
Off Label/Investigational Discussion:Use of irinotecan, oxaliplatin, and capecitabine for metastatic esophagogastric cancer
Brown LM, et al. J Natl Cancer Inst. 2008; 100:1184-1187.
Incidence of Esophageal Cancer: 16,470 new cases and 14,530 deaths in 2009
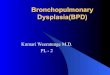
++++ > 8-fold risk+++ 4-8-fold risk++ 2-4-fold risk+ < 2-fold risk+/- Conflicting studies--- No proven risk
R isk F a cto r S C C AD C To b acco +++ ++ ETOH +++ --- Barre t t’s Es o p h ag u s --- ++++ W eekly Reflu x Sy mp to ms --- +++ Ob es ity --- ++ Po v erty ++ --- A ch alas ia ++++ Cau s tic in ju ry to es o p h ag u s ++++ --- Ty lo s is (NEPPK) ++++ --- Plu mmer-Vin s o n s y n d ro me ++++ --- His to ry o f h ead & n eck can cer ++++ --- H/o b reas t ca t reated with rad io th erap y +++ ++ Freq u en t co n s u mp tio n o f h o t b ev erag es + --- HPV (Ch in a , Jap an , So u th A frica) +/- --- Beta b lo cker --- + /- A n tich o lin erg ics --- + /- A min o p h y lin es --- + /-
Risk Factors: Esophageal CA
Enzinger PC. N Engl J Med. 2003;349:2241-2252.0
2
4
6
8
10
12
14
16
18
0 20-29 30-39 40 + 0 3.5 11 14.5 25 28.5 36+
AdenocarcinomaSquamous Cell CarcinomaAdenocarcinomaSquamous Cell Carcinoma
Cigarettes per Day Drinks per WeekData from Takezaki 2000, Wu 2001 and Brown 2001
Odds Ratio
Tobacco/Alcohol and Esophageal Cancer
1-19

2
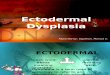
Squamousepithelium Metaplasia
Low-Grade
Dysplasia
High-Grade
DysplasiaADC METS
Oxidative stressInflammation
G1&G2COX-2BCL-2
4%/yr
0.5%/yr1%/yr
5%/yr10%
GERD1:7 Americans
0.005%/yr
Early Genetic Events:17pLOH p53; 9pLOH p16
cyclin D12nd Tier Genetic Events:
p53 mutation; p16 mutation/methylationEGF(R), telomerase RNA
Late Genetic Events:4 N (G2) aneuploidy of 5q/13q
and LOH of 5q/13q(Rb)/18q
?
c-erbB2
E-cadherin-catenin
85+%
Neoplastic Progression of Barrett’s Esophagus 2003 AJCC Classification of Esophageal Carcinoma
AJCC. AJCC Cancer Staging Manual. 6th ed. 2002.
Males in USAFemales in USA
Incidence of Gastric Adenocarcinoma
• No longer a “top ten” cause of cancer death in USA• 2009: 21,130 new cases and 10,620 deaths• Still the 4th leading cause of cancer death in Europe
CA Cancer J Clin ‘09
Risk Factors for Gastric Adenocarcinoma
• Nutritional– Low fat or protein consumption– Salted meat or fish– High nitrate consumption
• Environmental– Poor food preparation (smoked)– Lack of refrigeration– Poor drinking water (well water)– Occupation (rubber, coal workers)– Smoking (1.6x)– Low social class
• Medical– Prior gastric surgery– Helicobacter pylori infection (2x)– Gastric atrophy and gastritis
Helicobacter pylori
N=0mutagens
Higher pH
Bacterial growth + nitrate
Gastric ascorbic acid
B-carotene
Proposed Cascade of Pathologic Events inGastric Adenocarcinoma
Salt
Normal Superficialgastritis
Atrophicgastritis Metaplasia Dysplasia Carcinoma
Salt N-nitroso Chronic inflammationcarcinogens and reactive oxygen species
inhibition
promotion
Adapted from Correa
1997 AJCC Classification of Gastric Carcinoma
AJCC2003
T2a: a tumor that invades the muscularis propriaT2b: a tumor that invades into the subserosa
a/b
a/b
a/b
AJCC. AJCC Cancer Staging Manual. 6th ed. 2002.

3
Which one of the following strategies has NOT been shown in the setting of a randomized trial to extend
survival in a 68 yo man (PS 0, no significant comorbidities) with locally advanced GE junction
adenocarcinoma?
Localized Gastroesophageal Junction Cancer ?
1.1. Chemotherapy Chemotherapy surgery surgery chemoradiationchemoradiation therapytherapy2.2. Chemotherapy Chemotherapy surgery surgery chemotherapychemotherapy3.3. ChemoradiationChemoradiation therapy therapy surgerysurgery4.4. Surgery Surgery chemotherapy chemotherapy chemoradiationchemoradiation chemotherapychemotherapy
What Can Surgery Accomplish?
Localized Esophageal Cancer
Wijnhoven BP, et al. Ann Surg. 2007;245:717-725.
Esophageal Cancer Treated With Surgery
Does Adjuvant Chemotherapy Improve Surgery Outcomes?
Localized Esophageal Cancer
Neoadjuvant Chemotherapy Compared with Surgery Alone for Localized Esophageal Cancer
Thirion. ASCO 2007
FP (*) x 2/3 every 28 days
Resection
Within 4 weeks
4 - 6 weeks
Resection
4 – 6 weeks
FP x 3/4 or no treatment
Follow-up
Randomization
CT + S S
FNLCC ACCORD 07-FFCD 9703 Trial: Schema
(*) FP = 5FU: 800 mg/m² CI x 5 days - CDDP: 100 mg/m² at d1 or d2, 1-hr infusion Boige. ASCO 2007
Stage II-IVA75% distal esophagusor GEJ ADC

4
S CT + S P-valuen = 85 n = 98
Tumor stage
T0 0% 3%T1, T2 32% 39%T3, T4 68% 58% 0.16
Nodal status (%)
N- 20% 33%N+ 80% 67% 0.054
Nb nodes removed
Median 19 19Range (2 - 82) (1 - 49)
Boige. ASCO 2007
ACCORD 07: Pathological Results
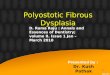
713162738537911114172741536593113
0,00
0,20
0,40
0,60
0,80
1,00
0 1 2 3 4 5 6 7A risque
logrank : p = 0,021
___ S___ CT + S
years
ACCORD 07: Overall Survival
At risk
5-year OS: 24% (95% CI, 16%-33%) vs 38% (95% CI, 28%-47%)
Logrank P-value = 0.021Hazard Ratio, 0.69 (95% CI, 0.50-0.95)
Boige. ASCO 2007
Does NeoadjuvantChemoradiation
Therapy Improve Surgery Outcomes?
Localized Esophageal Cancer All-Cause Mortality Estimates for Neoadjuvant C/RT Compared with Surgery Alone
Gebski V, et al. Lancet Oncol. 2007;8:226-234.
POET: Schema
Arm A
Week
Arm B
PLF I PLF III (3 weeks)
15 x 2 Gy in 3 weeks
PE (1 week)
Surgery
Surgery
1 1314 17 20-21
PLF: Cisplatin 50mg/m2, 1h, d 1,15,29. Leukovorin/5-FU 500mg/m2 2h / 2g/m2 24h, d1,8,15,22,29,36PE: Cisplatin 50 mg/m2, 1h, d 2+8. Etoposide 80 mg/m2, 1h, d 3-5
PLF II
6 7
PLF I PLF II
Stahl M, et al. J Clin Oncol.2009;27:851-856.
POET: Downstaging
Arm A Arm B P-value(n = 49) (n = 45)
Path CR 2% 16% 0.03T1-4N0M0 35% 49%Node neg. 37% 64% 0.01T0-4N+M0 55% 31%T1-4N+M1 8% 4%
Stahl M, et al. J Clin Oncol.2009;27:851-856.

5
POET: Overall Survival
Log rank P = 0.07
HR Arm B vs A0.67; 95% CI, 0.41-1.07)
Arm B
Arm A
47.4%
27.7%
Arm A Arm B
Median survival 21.1 mo 33.1 mo
Median follow-up 45.2 mo 46.2 moStahl M, et al. J Clin Oncol.2009;27:851-856.
Can Surgery Improve the Outcomes of Chemoradiation?
Localized Esophageal Cancer
Prospective Randomized Intergroup Study:Radiation Therapy vs Chemotherapy + Radiation Therapy
for Localized SCC or ADC of the Esophagus
Schema
tumor size
histology
weight loss
2 x Cisplatin (75 mg/m2) + 5-fluorouracil (1000 mg/m2/d CI x 4d) + radiation therapy (5000 cGy)
R
A
N
D
O
M
I
Z
E
radiation therapy (6400 cGy)
Herskovic A, et al. N Engl J Med. 1992;326:1593-1598.al-Sarraf M, et al. J Clin Oncol. 1997;15:277-284.
Intergroup Study
Herskovic A, et al. N Engl J Med. 1992;326:1593-1598. al-Sarraf M, et al. J Clin Oncol. 1997;15:277-284.
• A total of 455 patients with localized esophageal cancer were given 2 courses of 5-FU/cisplatin plus radiation therapy.
• 259/455 patients experienced a “partial response”, were considered operative candidates, and entered the randomized component of the trial.
Chemoradiation Therapy With or Without Surgery: French Phase III Trial
Bedenne. J Clin Oncol. 2007;25:1160-1168.
Chemoradiation Therapy With or Without Surgery: French Phase III Trial
Survival
3-month mortality median 2-year
5-FU/CDDP x 3 +
1% Radiation
therapy
19.3
months
40%
P=0.56
Surgery 9% 17.7 months
34%
Partial Response
R A N D O M I Z E
(259 pts)
Bedenne. J Clin Oncol. 2007;25:1160-1168.

6
Patients:(N = 177)
uT3-4,N0-1, M0with SCC
Chemoradiation Therapy With or Without Surgery:German Phase III Trial (Schema)
RANDOMIZE
3 cycles:5-FU/LV + Cisplatin + Etoposide
Chemoradiation:Cisplatin+Etoposide
+ 40 Gy RTSurgery
Chemoradiation:Cisplatin+Etoposide
+ > 60 Gy RT
Stahl. J Clin Oncol. 2005;23:2310-2317.
Chemoradiation Therapy With or Without Surgery: German Phase III Trial (Results)
Arm CompletedTreatment
TreatmentMortality
3-yr LocalRecurrence
MedianSurvival
3-Year SurvivalInduction Chemo
All Responder
Arm A:C/RT S 62% 12.8% 41% 16 mo. 31% 54%
Arm B:C/RT 85% 3.5%
(P = 0.03)64%
(P = 0.004)15 mo. 24%
(P = 0.02)54%
Stahl. J Clin Oncol. 2005;23:2310-2317.
C/RT +/- Surgery for Esophageal SCC
Stahl. J Clin Oncol. 2005;23:2310-2317.
Median survival (N=172):Arm A (C/RT S) -16.4 monthsArm B (C/RT only)-14.9 months
31.3% (P = 0.02)
24.4%
Conclusions from these Results
Localized Esophageal
Pre-operative cisplatin/5-FU chemotherapy offers a small survival advantage in distal esophageal and GE junction cancer.
Neoadjuvant cisplatin-based chemoradiation offers a greater survival advantage with better local control but increased surgical morbidity.
Surgery may not be needed in patients who have a clinical response to chemoradiation.
What Can Surgery Accomplish?
Localized Gastric Cancer
Survival in 633 patients, according to 1997 TNM stage
Gastric Cancer Kranenberg. Br. J Cancer 2001
42%
66%
82%
20%
12%

7
5-Year Survival %
Authors n DST TG
Gouzi 1989 169 48 48
Bozzetti 1999 648 64 62
Randomized Controlled Trials
Prospective Studies of Total Gastrectomy (TG) vsSubtotal Gastrectomy (DST) for Distal Gastric Cancer What Is the Ideal Extent of Lymphadenectomy?
D0 - removes less than all relevant N1 nodes
D1 - requires the dissection of the N1 nodes (1 - 6)*
D2 - includes the N1 and N2 nodes (7–11)
D3 – includes the N1, N2, and N3 nodes (12-15)
D4 – includes the N1, N2, N3 and N4 nodes (16)
*nodes 2, 4 remain if distal subtotal gastrectomy
4d6 4d
4d4sb
533
12 4sa
4sb
1616
1616
Japanese Data
Marujama. Semin Oncol 1996
Randomized Study of D1 and D2 Dissection for Gastric Cancer
711 patients undergoing curative resection of gastric cancer
Peri-Op Morbidity
Peri-OpMortality
Median Hospital Stay
(days)5-Year
Survival
11-YearSurvival(P = 0.53)
D1Dissection 25% 4% 14 45% 30%
D2Dissection 43% 10% 16 47% 35%
Bonenkamp JJ, et al. N Engl J Med. 1999;340:908-914.Hartgrink HH, et al. J Clin Oncol. 2004;22:2069-2077.
What are Proven Strategies to Enhance Outcomes for Surgical
Resection?
Localized Gastric Cancer Intergroup Protocol 0116Adjuvant Therapy for Gastric Cancer
Stratify
depth of tumor penetration 5-FU/leucovorin x 1
5-FU/leucovorin +
4500 cGy radiation
5-FU/leucovorin x 2
number involved nodes
location of tumor observation
extent of surgery
R
A
N
D
O
M I
Z
E
Macdonald. N Engl J Med 2001

8
Intergroup Protocol 0116
Macdonald JS, et al. N Engl J Med. 2001;345:725-730.
Chemoradiotherapy
Surgery Only
50%
41%
P = 0.005
3 years
MAGIC Trial: Schema
ECF x 3 q3/523-6 weeks
Resection
ECF x 3 q3/52
6-12 weeks
CSC S
Follow-up
Within 6 weeks
Resection
Cunningham D, et al. N Engl J Med. 2006;355:11-20. 503 Patients:15% Lower Third12% GE Junction
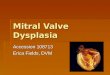
MAGIC: Survival
Patients at risk
Logrank P-value = 0.009Hazard Ratio = 0.75 (95% CI, 0.60 - 0.93)
CSCS
250 168 111 79 52 38 27253 155 80 50 31 18 9
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Months from randomization0 12 24 36 48 60 72
149 250
170 253
Events TotalCSC
S
Sur
viva
l rat
e
36%
23%
50%
41%
Cunningham. N Engl J Med 2006 Which one of the following strategies has NOT been
shown in the setting of a randomized trial to extend survival in a 68 yo man (PS 0, no significant
comorbidities) with locally advanced GE junction adenocarcinoma?
Localized Gastroesophageal Junction Cancer ?
1.1. Chemotherapy Chemotherapy surgery surgery chemoradiationchemoradiation therapytherapy
2.2. Chemotherapy Chemotherapy surgery surgery chemotherapychemotherapy
3.3. ChemoradiationChemoradiation therapy therapy surgerysurgery
4.4. Surgery Surgery chemotherapy chemotherapy chemoradiationchemoradiation chemotherapychemotherapy
Conclusions from these Results
Localized Gastric:
Post-operative 5-FU-based chemoradiation therapy remains the standard of care for muscle-invasive or LN positive disease.
The MAGIC trial demonstrates that pre- and post-operative ECF improves survival. It may be particularly beneficial for downstaging extensive local disease.
What are the Active Agents and Combinations for this Disease?
Metastatic Esophagogastric Cancer

9
Prior to selecting systemic treatment, which of the following molecular studies should be performed on tumor tissue from a 73 yo man with gastric cancer
metastatic to liver and lungs?
Metastatic Esophagogastric Cancer ?
1.1. EGFREGFR2.2. KK--rasras3.3. HERHER--2/neu2/neu4.4. MSIMSI5.5. cc--KITKIT
Advanced Esophagogastric Cancer:Older Single Agents
Class Agent Mechanism Of Action ResponseAntimetabolite 5-Fluorouracil Inhibits thymidylate synthase 21%
Methotrexate Inhibits purine nucleotide and thymidylatesynthesis 11%
Pemetrexed Inhibits thymidylate synthase 21%
Gemcitabine Inhibits ribonucleotide reductase 0%
Antibiotic Mitomycin-C Produces interstrand DNA cross-links 30%
Anthracycline Doxorubicin Intercalates into DNA and interactswith topoisomerase II
17%
Epirubicin 18%
Heavy Metal Cisplatin Produces intrastrand and interstrand DNA cross-links
21%
Carboplatin 9%
TopoisomeraseInhibitor Etoposide Binds to and inhibits topoisomerase II 8%
National Cancer Institute. http://www.cancer.gov/drugdictionary/
Chemotherapy for Advanced Gastric Cancer:Important Randomized Studies
Study Regimen n Response (%) OS (months) P-value
Ohtsu et al. 20031
FCF
UFTM
10510570
11349
7.17.36.0
NS
Vanhoefer et al. 20002
FAMTXELFCF
133132134
129
20
6.77.27.2
NS
Webb et al. 19973ECF
FAMTX111108
4521
8.95.7
0.0009
Ross et al. 20024ECFMCF
289285
4244
9.4 +QOL8.7 -QOL
NS
F = 5FU; A = doxorubicin; M = mitomycin; MTX = methotrexate; C = cisplatin; U = uracil; FT = tegafur;E = etoposide (in ELF) or epirubicin (in ECF); L = leucovorin; NS = not significant.
1. Ohtsu et al. J Clin Oncol. 2003;21:54; 2. Vanhoefer et al. J Clin Oncol. 2000;18:2648;. 3. Webb et al. J ClinOncol. 1997;15:261; 4. Ross et al. J Clin Oncol. 2002;20:1996.
ToGA - Schema
HER2-positiveadvanced GC
(n = 584)
5-FU or capecitabine+ cisplatin(n = 290)
R
aChosen at investigator’s discretion GEJ, gastroesophageal junction
5-FU or capecitabinea
+ cisplatin+ trastuzumab
(n = 294)Stratification factors− advanced vs metastatic − GC vs GEJ− measurable vs non-measurable− ECOG PS 0-1 vs 2− capecitabine vs 5-FU
Phase III, randomized, open-label, international, multicenter study
Van Cutsem. ASCO 2009
3807 patients screened1
810 HER2-positive (22.1%)
0
10
20
30
40
50
60
ToGA: Response Rate
2.4%5.4%
32.1%
41.8%
34.5%
47.3%
Intent to treat
ORR= CR + PR; CR, complete response; PR, partial response
P = 0.0599
P = 0.0145
F+C + trastuzumabF+C
P = 0.0017Patients (%)
CR PR ORR
Van Cutsem. ASCO 2009
ToGA: Overall Survival
Time (months)
294290
277266
246223
209185
173143
147117
11390
9064
7147
5632
4324
3016
2114
137
126
65
40
10
00
No. at risk
11.1 13.8
0.00.10.20.30.40.50.60.70.80.91.0
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
Event
FC + TFC
Events
167182
HR
0.74
95% CI
0.60, 0.91
P-value
0.0046
MedianOS
13.811.1
T= trastuzumab Van Cutsem. ASCO 2009

10
Advanced Esophagogastric Cancer:Newer Agents
Class Agent MOA1 Response2,3
AntimetaboliteCapecitabine Reduces thymidine production and competes with uridine
triphosphate for incorporation into RNA 30%
S-1 Inhibits thymidylate synthase and CDHP, and competes with uridine triphosphate for incorporation into RNA 26%
Heavy Metal Oxaliplatin Produces intrastrand and interstrand platinum-DNA cross-links na
Taxane Paclitaxel Binds to and stabilizes tubulin inhibiting microtubule disassembly
13%
Docetaxel 21%
TopoisomeraseInhibitor Irinotecan Inhibits topoisomerase I 21%
1. National Cancer Institute. http://www.cancer.gov/drugdictionary/;2. Schöffski P. Ann Oncol. 2002;13:13-22. Ajani JA. Oncologist. 2005.10;49-58.
CDHP = 5-chloro-2,4-dihydroxypyridine; na = not available.
REAL-2: Schema
Previously untreated patients
with locally advanced or metastatic
oesophago-gastric cancer
RANDOMISATION
EpirubicinCisplatinFluorouracil
EpirubicinCisplatinXeloda (capecitabine)
EpirubicinOxaliplatinFluorouracil
EpirubicinOxaliplatinXeloda (capecitabine)Stratified for:
- Centre (63 centres mainly UK, 2 Aus) - Locally advanced versus metastatic - PS 0/1 versus 2
2 x 2 design
Cunningham D, et al. N Engl J Med. 2008;358:36-46.
REAL-2: Survival (ITT)
0
20
40
60
80
100
0 1 2 3Time since randomisation (years)
Prob
abili
ty o
f sur
viva
l (%
)
ECF EOF ECX EOX
Arm OS (m) 1-year survival (95% CI)
P-value HR(95% CI)
ECFEOFECXEOX
9.99.39.9
11.2
37.7 (31.8-43.6)40.4 (34.2-46.5)40.8 (34.7-46.9)46.8 (40.4-52.9)
0.6120.3890.020
10.96 (0.79-1.15)0.92 (0.76-1.11)0.80 (0.66-0.97)
Cunningham D, et al. N Engl J Med. 2008;358:36-46.
EOX
ECF
Capecitabine / Cisplatin vs. 5-FU / CisplatinSchema
Previously untreated advanced gastric cancer
XP - Capecitabine 1000/m2 twice daily d1-14 Cisplatin 80/m2 d1 q3 weeks
N=160
N=156
FP - 5-FU 800 mg/m2 d1-5 Cisplatin 80 mg/m2 d1 q3 weeks
Primary endpoint: Non-inferiority in PFS, HR <1.4
Secondary endpoints: Response rate (RR), time to response (TTR), overall survival (OS), safety
R
Kang. ASCO 2006
• ORR: FP (29%) XP (41%)• MS: FP (9.3 mo) XP (10.5 mo)• Toxicity: Similar• Conclusions: XP is non-inferior to FP (HR, 0.8; 95% CI, 0.6-.0)
Kang. ASCO 2006
Estimated probability
XP (n=139) 5.6 (4.9—7.3)FP (n=137) 5.0 (4.2—6.3)
Median PFSMonths (95% Cl)
HR = 0.81 (95% Cl, 0.63—1.04)Compared to HR upper limit 1.25, P = 0.0008
MonthsPer protocol analysis
0 2 4 6 8 10 12 14 16 18 20 22 24 26
1.0
0.8
0.6
0.4
0.2
0.0
Capecitabine/Cisplatin vs 5-FU/CisplatinProgression-Free Survival
5-FU/LV + Oxaliplatin vs 5-FU/LV + CisplatinSchema
Previously untreated advanced gastric cancer
FLO - 5-FU 2600 mg/m2 24-hr CILeucovorin 200 mg/m2
Oxaliplatin 85 mg/m2 d1q2 w
N = 112
N = 106
FLP - 5-FU 2000 mg/m2 24-hr Leucovorin 200 mg/m2
q1 wCisplatin 50 mg/m2 d1q2 w
Primary endpoint: Superiority for TTP
Secondary endpoints: Response rate (RR), time to treatment failure (TTF), overall survival (OS), safety
R
Al-Batran SE, et al. J Clin Oncol. 2008;26:1435-1442.

11
• ORR: FLO (34%) FLP (27%); improved safety profile for FLO• Conclusions: Primary endpoint not met and survival data are pending
FLO FLPMedian TTP (months) 5.7 3.8TTP Events 80 (71.4%) 81 (76.4%)
HR, 0.8 (95% Cl, 0.58 - 1.09)
Log rank P = 0.081Wilcoxon P = 0.0179
Monthsn at riskn at risk
FLOFLP
Prob
abili
ty (%
)
1.0
0.8
0.6
0.4
0.2
0.0
0 5 10 15 20 25 30
102 52 15 4106 35 13 5
5-FU/LV + Oxaliplatin vs 5-FU/LV + CisplatinTime to Progression
Al-Batran. J Clin Oncol 2008
Irinotecan/Cisplatin–Based Tx for Esophagogastric Cancer
Author Regimen Cancer Type
# Patients Major Response
Rate
G3-4 Diarrhea
G4 ANC
Median Survival
Ilson. 1999
weekly Esoph. GE jct.
35 57% 11% 9% 14.6 mo.
Ajani. 2002
weekly GE jct. Gastric
38 58% 22% 15% 9 mo.
Ajani. 2002
weekly GE jct. Gastric
29 pretreated
31% 13% 9% 5 mo.
Satoh. 2002
weekly Gastric. 15 naive 25 pretx
53% 20%
3% 10% 9.9 mo.9.0 mo.
Enzinger.2009
weekly EsophGastric
3125
67%37%
26% 11% 14.3 mo.9 mo.
TPC: docetaxel – cisplatin - irinotecan
PC: cisplatin - irinotecan
Prior to selecting systemic treatment, which of the following molecular studies should be performed on tumor tissue from a 73 yo man with gastric cancer
metastatic to liver and lungs?
Metastatic Esophagogastric Cancer ?
1.1. EGFREGFR2.2. KK--rasras3.3. HERHER--2/neu2/neu4.4. MSIMSI5.5. cc--KITKIT
Conclusions from these Results
Metastatic Esophagogastric:
The most active single agents are the 5-fluoro-pyrimidines, platinum analogues, taxanes, and irinotecan.
Combinations of fluoropyrimidine and platinum remain the standard of care. Trastuzumab should be added for HER2/neu 2-3+ or FISH+ tumors.
Weekly irinotecan/cisplatin is most convenient. FOLFOX is best for patients with hepatic or renal insufficiency.
Thank you for attendingMaster Class for Oncologists
Questions & Answers
?