Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Vascular endothelial growth factor corrected for platelet countand hematocrit is associated with the clinical course of aplasticanemia in children
Yuichi Kodama • Yasuhiro Okamoto • Teruto Hashiguchi •
Yuichi Shinkoda • Takuro Nishikawa • Takayuki Tanabe •
Yoshifumi Kawano
Received: 21 October 2011 / Revised: 4 April 2012 / Accepted: 5 April 2012 / Published online: 22 April 2012
� The Japanese Society of Hematology 2012
Abstract The wide variety of clinical courses that lead to
the development of severe aplastic anemia (AA) makes it
difficult to speculate whether treatment for AA is required in
the early phase. The objective of this study was to identify a
method for predicting the clinical course of AA at the onset of
the disease. First, in healthy adults, vascular endothelial
growth factor (VEGF) released per platelet was measured by
the activation of platelet-rich plasma (PRP) and platelet-poor
plasma (PPP). Serum concentration of VEGF, serum con-
centration of VEGF corrected for platelet count, and serum
concentration of VEGF corrected for both platelet count and
hematocrit (corrected VEGF) were then compared to VEGF
released per platelet. Corrected VEGF showed the best cor-
relation with VEGF released per platelet by the activation of
PRP in healthy subjects (R2 = in a single 0.806, p = 0.001).
Next, corrected VEGF was assayed in 11 pediatric patients
with AA at the time of diagnosis. Corrected VEGF in AA
patients was significantly greater than that in age-matched
control subjects [1.32 9 10-6 pg (range 0.36–1.85) vs.
0.18 9 10-6 pg (range 0.12–0.94)] (p = 0.002). Moreover,
corrected VEGF in AA patients who did not require treatment
for more than 2 years was significantly greater than that in
AA patients who required earlier treatment [1.67 9 10-6 pg
(range 1.32–1.85) vs. 0.87 9 10-6 pg (0.36–1.34)]
(p = 0.011). These data indicate that a compensatory
mechanism for increasing VEGF and preventing disease
progression might play a role in AA. Corrected VEGF may be
useful for predicting the clinical course of AA.
Keywords Aplastic anemia � VEGF � Clinical course �Biomarker
Introduction
Most patients with aplastic anemia (AA) deteriorate to
severe AA and require transfusions. However, some cases
of AA show stable disease or resolve spontaneously [1–3].
Treatment is often begun after the patient has become
transfusion dependent or their disease has met the criteria
of severe AA because it can be difficult to decide whether
to initiate immunosuppressive therapy (IST) or hemato-
poietic stem cell transplantation (HSCT), which are asso-
ciated with many adverse effects and a risk of therapy-
related mortality [4]. For physicians, the wide variety of
clinical courses that lead to the development of severe AA
makes it difficult to judge if treatment for AA is required in
the early phase [2]. Therefore, a procedure should be
established for predicting the clinical course at the onset of
AA, especially mild and moderate AA.
Based on an immunohistochemical analysis, it has been
reported that AA is associated with the reduced expression
of vascular endothelial growth factor (VEGF) in mega-
karyocyte and immature myeloid progenitor cells and with
a reduced serum concentration of VEGF levels compared
to those in normal controls [5]. The report also noted that
VEGF expression recovered after the treatment of AA.
Since VEGF in serum is known to be exclusively released
from platelets [6], it is reasonable that the serum
Y. Kodama � Y. Okamoto (&) � Y. Shinkoda � T. Nishikawa �T. Tanabe � Y. Kawano
Department of Pediatrics, Kagoshima University Graduate
School of Medical and Dental Sciences,
8-35-1 Sakuragaoka, Kagoshima 890-8520, Japan
e-mail: [email protected]
T. Hashiguchi
Laboratory and Vascular Medicine, Kagoshima University
Graduate School of Medical and Dental Sciences,
Kagoshima, Japan
123
Int J Hematol (2012) 95:494–499
DOI 10.1007/s12185-012-1074-1

concentration of VEGF is low in AA patients. To under-
stand the significance of low VEGF in AA, VEGF released
per platelet, rather than simply VEGF in the serum, should
be measured to exclude the effect of a low platelet count in
AA patients. The most accurate and physiological method
for assessing VEGF released per platelet is to measure
VEGF by the activation of platelet-rich plasma (PRP) and
platelet-poor plasma (PPP) [7]. However, the activation of
PRP and PPP is time-consuming and requires a large
amount of blood, which is not feasible in children with AA.
In this study, we first attempted to identify a more fea-
sible, alternative method for assessing VEGF released per
platelet in healthy controls. Next, we examined the asso-
ciation between VEGF measured at the onset of AA by this
new method and the clinical course.
Methods
Blood samples
Platelet-rich plasma, PPP and serum samples were taken
from healthy adult donors. In contrast, only serum samples
were taken from AA patients and control subjects. Plasma
samples were collected in sterile tubes containing sodium
citrate as an anticoagulant. PRP was obtained by centri-
fugation (120 g for 5 min). PPP and serum samples were
also obtained by centrifugation (2,000 g for 20 min).
Plasma samples and serum samples were stored at -40 �C
(Sanyo, Tokyo, Japan) until the time of assay.
Measurement of VEGF
The VEGF concentration in serum or plasma was measured
in duplicate with a commercially available human VEGF
quantitative enzyme-linked immunosorbent assay (ELISA:
Catalogue No. DVE00, R&D Systems, Minneapolis, MN).
This system can measure as little as 9 pg/ml and does not
cross-react with platelet-derived growth factor or other
homologous cytokines. The optical density at 450 nm was
measured on an ImmunoMini NJ-2300 (Nippon Inter Med,
Tokyo, Japan) and the VEGF concentration was determined
by linear regression from a standard curve that was con-
structed using the VEGF supplied with the kit as a standard.
VEGF released per platelet by the activation of PRP
and PPP (VEGF per platelet) and serum concentration
of VEGF corrected for both the platelet count
and hematocrit (corrected VEGF)
Platelet-rich plasma and PPP were activated by the addition
of human thrombin (Sigma Chemical Co., St. Louis,
MO)/calcium chloride solution to a final concentration of
5 U/ml/10 mM to ensure maximal clotting (PRP VEGF and
PPP VEGF, respectively). After being allowed to stand at
room temperature for 30 min, samples were centrifuged at
750 g at 4 �C for 20 min, and the supernatants were trans-
ferred for measurement of the VEGF concentration. VEGF
per platelet was calculated as {PRP VEGF (pg/ml) - PPP
VEGF (pg/ml)}/platelet count in PRP (/ll) 9 1,000, as
described previously [7]. Since the measurement of VEGF
per platelet is time-consuming and requires a large amount
of blood as described above, the serum concentration of
VEGF was also measured. The serum concentration of
VEGF corrected for platelet count was calculated as the
serum concentration of VEGF (pg/ml)/platelet count (/ll) 9
1,000 to exclude the effect of the platelet count. Corrected
VEGF was calculated as the serum concentration of VEGF
(pg/ml) 9 {1-hematocrit}/platelet count (/ll) 9 1,000 to
exclude the effects of both the platelet count and hematocrit.
Subjects for the examination of VEGF per platelet
Eight healthy adult subjects were examined to evaluate the
correlation between VEGF per platelet, the serum con-
centration of VEGF, the serum concentration of VEGF
corrected for platelet count and corrected VEGF.
Patients and control subjects
Eleven AA patients (5 male and 6 female) diagnosed at
Kagoshima University Hospital between 2001 and 2007
whose serum at the onset was available were evaluated.
The median age of the patients was 10 years (range
8–14 years). All patients were diagnosed with acquired AA
and none had a family history or any physical malforma-
tions. None were post-hepatitis. Myelodysplastic syndrome
and paroxysmal nocturnal hemoglobinuria were excluded
by cytology and chromosome analysis, and/or by flow
cytometry using anti-CD55/59 [8]. None of the patients
showed an abnormal physical examination that would
indicate Fanconi anemia or chromosome fragility. Two
patients were classified with mild, 6 with moderate and 3
with severe AA, according to currently used criteria [2].
In our institution, treatments including HSCT or IST were
initiated if the patient became transfusion dependent or was
classified as severe AA. HSCT was performed if the patient
had a human leukocyte antigen (HLA)-matched/HLA one-
locus-mismatched sibling or an HLA-matched unrelated
donor. IST was performed for the remaining patients. If the
patient did not respond to IST, an HLA one-locus-mis-
matched unrelated donor was used as an alternative donor.
In this study, acute AA was defined as when the patient
required treatment within 2 years after diagnosis. Chronic
AA was defined as when the patient did not require treat-
ment more than 2 years after diagnosis.
Corrected VEGF is associated with the clinical course of AA 495
123
The control subjects consisted of 7 age-matched children
who did not have AA. They were not obese and their median
body mass index was 17.1 (range 16.5–21.7). Basically, they
were afebrile and the median C-reactive protein was 0.02
(range 0.02–0.05). The clinical protocols for measuring
serum VEGF were approved by the Institutional Review
Board at Kagoshima University Hospital. Written informed
consent was obtained from the respective parents.
Statistical analysis
Data are presented as medians (ranges). Paired data were
compared using the Mann–Whitney U test. A simple linear
regression analysis was used to evaluate the correlation
between two parameters. All statistical analyses were
performed using SPSS statistical software (SPSS Co.,
Tokyo, Japan), and p \ 0.05 was considered to be statis-
tically significant.
Results
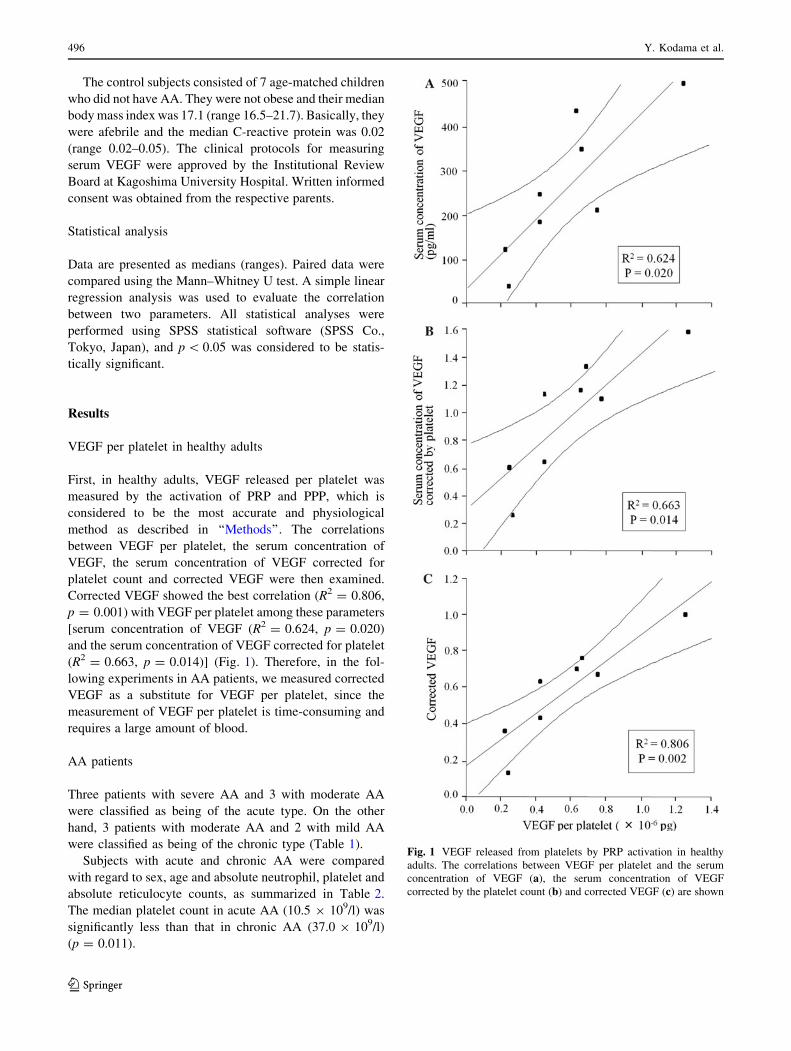
VEGF per platelet in healthy adults
First, in healthy adults, VEGF released per platelet was
measured by the activation of PRP and PPP, which is
considered to be the most accurate and physiological
method as described in ‘‘Methods’’. The correlations
between VEGF per platelet, the serum concentration of
VEGF, the serum concentration of VEGF corrected for
platelet count and corrected VEGF were then examined.
Corrected VEGF showed the best correlation (R2 = 0.806,
p = 0.001) with VEGF per platelet among these parameters
[serum concentration of VEGF (R2 = 0.624, p = 0.020)
and the serum concentration of VEGF corrected for platelet
(R2 = 0.663, p = 0.014)] (Fig. 1). Therefore, in the fol-
lowing experiments in AA patients, we measured corrected
VEGF as a substitute for VEGF per platelet, since the
measurement of VEGF per platelet is time-consuming and
requires a large amount of blood.
AA patients
Three patients with severe AA and 3 with moderate AA
were classified as being of the acute type. On the other
hand, 3 patients with moderate AA and 2 with mild AA
were classified as being of the chronic type (Table 1).
Subjects with acute and chronic AA were compared
with regard to sex, age and absolute neutrophil, platelet and
absolute reticulocyte counts, as summarized in Table 2.
The median platelet count in acute AA (10.5 9 109/l) was
significantly less than that in chronic AA (37.0 9 109/l)
(p = 0.011).
Fig. 1 VEGF released from platelets by PRP activation in healthy
adults. The correlations between VEGF per platelet and the serum
concentration of VEGF (a), the serum concentration of VEGF
corrected by the platelet count (b) and corrected VEGF (c) are shown
496 Y. Kodama et al.
123
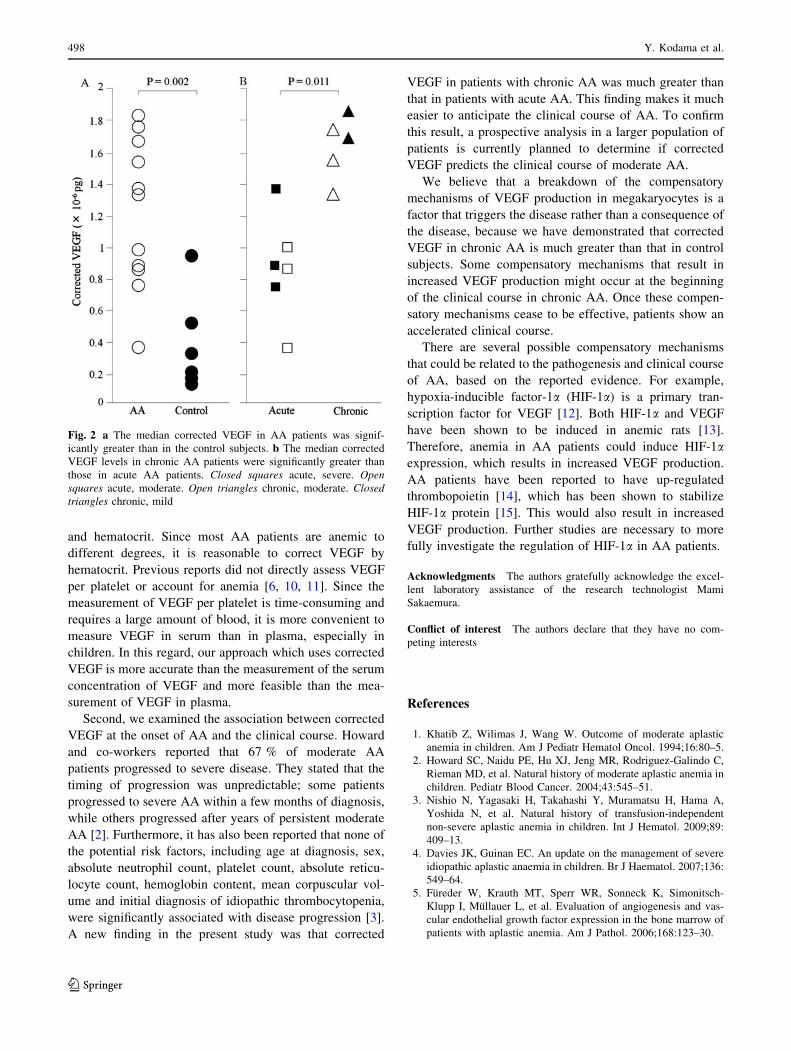
Corrected VEGF in AA patients and control subjects
The median corrected VEGF in AA patients [1.32 9
10-6 pg (range 0.36–1.85)] was significantly greater
(p = 0.002) than that in control subjects [0.18 9 10-6 pg
(range 0.12–0.94)] (Fig. 2a). The median corrected VEGF
levels in chronic AA patients [1.67 9 10-6 pg (range
1.32–1.85)] were significantly greater (p = 0.011) than
those in acute AA patients [0.87 9 10-6 pg (0.36–1.34)]
(Fig. 2b).
Corrected VEGF in moderate AA patients
To exclude the effect of the severity of the disease, we
compared corrected VEGF only in moderate AA patients.
The corrected VEGF values in 3 moderate/acute and 3
moderate/chronic AA patients were 0.36, 0.98 and
0.86 9 10-6 pg and 1.76, 1.32 and 1.54 9 10-6 pg,
respectively (Fig. 2b). The corrected VEGF in moderate/
chronic AA patients was higher than that in moderate/acute
AA patients.
Discussion
Vascular endothelial growth factor in platelets is derived
from the megakaryocytes in bone marrow [9]. Therefore,
we believe that VEGF could reflect bone marrow function.
Another group reported that AA was associated with the
reduced expression of VEGF in megakaryocyte and
immature myeloid progenitor cells, and with a low serum
concentration of VEGF compared with normal controls [5].
They also reported that VEGF expression recovered after
the treatment of AA. We presume that a low serum con-
centration of VEGF level may not merely reflect bone
marrow function in AA. Therefore, in this study we tried to
appreciate the significance of a low VEGF in AA by
measuring VEGF released per platelet. VEGF assayed by
the activation of PRP and PPP should be quite accurate,
since the maximal VEGF released from platelets by the
activation of PRP and PPP is actually measured [7].
In this study, we demonstrated for the first time that
VEGF per platelet showed the best correlation with cor-
rected VEGF, which is VEGF corrected for platelet count
Table 1 Clinical features at diagnosis of 11 children with aplastic anemia
Case no. Course Age/sex Severity ANC (9109/l) Platelets (9109/l) ARC (9109/l) Treatment
Case 1 Acute 10/F Severe 1.132 6 10.20 HSCT at 1 month
Case 2 Acute 13/M Severe 0.000 8 5.60 HSCT at 1 month
Case 3 Acute 8/M Severe 0.450 10 36.30 IST at 0.5 month
Case 4 Acute 9/M Moderate 0.588 11 42.66 HSCT at 2 months
Case 5 Acute 12/M Moderate 0.398 30 31.95 HSCT at 3 months
Case 6 Acute 11/F Moderate 1.320 18 35.40 IST at 1 month, HSCT at 6 months
Case 7 Chronic 12/M Moderate 1.240 37 37.53 No therapy for 30 months
Case 8 Chronic 10/F Moderate 0.481 22 77.66 No therapy for 33 months
Case 9 Chronic 8/M Moderate 0.820 33 20.86 No therapy for 33 months
Case 10 Chronic 7/F Mild 1.835 63 52.48 No therapy for 26 months
Case 11 Chronic 14/F Mild 1.220 51 57.00 No therapy for 28 months
ANC absolute neutrophil count, ARC absolute reticulocyte count, M male, F female, HSCT hematopoietic stem cell transplantation, ISTimmunosuppressive therapy
Table 2 Comparison of acute and chronic aplastic anemia with regard to sex, age, ANC, platelet count and ARC
Acute Chronic p value
Sex (male:female) 3:3 2:3
Median age at diagnosis 10.5 (8–13) 10.0 (7–14) 0.783
Median ANC for each patient (9109/l) 0.59 (0.40–1.38) 1.22 (0.48–1.84) 0.251
Median ARC for each patient (9109/l) 33.7 (5.6–42.6) 52.5 (20.9–77.7) 0.068
Median platelet count for each patient (9109/l) 10.5 (6–30) 37.0 (22–63) 0.011
Median time to require treatment (months) 1 (0.5–3) 30 (26–33) 0.006
The results are presented as median values (ranges)
ANC absolute neutrophil count, ARC absolute reticulocyte count
Corrected VEGF is associated with the clinical course of AA 497
123
and hematocrit. Since most AA patients are anemic to
different degrees, it is reasonable to correct VEGF by
hematocrit. Previous reports did not directly assess VEGF
per platelet or account for anemia [6, 10, 11]. Since the
measurement of VEGF per platelet is time-consuming and
requires a large amount of blood, it is more convenient to
measure VEGF in serum than in plasma, especially in
children. In this regard, our approach which uses corrected
VEGF is more accurate than the measurement of the serum
concentration of VEGF and more feasible than the mea-
surement of VEGF in plasma.
Second, we examined the association between corrected
VEGF at the onset of AA and the clinical course. Howard
and co-workers reported that 67 % of moderate AA
patients progressed to severe disease. They stated that the
timing of progression was unpredictable; some patients
progressed to severe AA within a few months of diagnosis,
while others progressed after years of persistent moderate
AA [2]. Furthermore, it has also been reported that none of
the potential risk factors, including age at diagnosis, sex,
absolute neutrophil count, platelet count, absolute reticu-
locyte count, hemoglobin content, mean corpuscular vol-
ume and initial diagnosis of idiopathic thrombocytopenia,
were significantly associated with disease progression [3].
A new finding in the present study was that corrected
VEGF in patients with chronic AA was much greater than
that in patients with acute AA. This finding makes it much
easier to anticipate the clinical course of AA. To confirm
this result, a prospective analysis in a larger population of
patients is currently planned to determine if corrected
VEGF predicts the clinical course of moderate AA.
We believe that a breakdown of the compensatory
mechanisms of VEGF production in megakaryocytes is a
factor that triggers the disease rather than a consequence of
the disease, because we have demonstrated that corrected
VEGF in chronic AA is much greater than that in control
subjects. Some compensatory mechanisms that result in
increased VEGF production might occur at the beginning
of the clinical course in chronic AA. Once these compen-
satory mechanisms cease to be effective, patients show an
accelerated clinical course.
There are several possible compensatory mechanisms
that could be related to the pathogenesis and clinical course
of AA, based on the reported evidence. For example,
hypoxia-inducible factor-1a (HIF-1a) is a primary tran-
scription factor for VEGF [12]. Both HIF-1a and VEGF
have been shown to be induced in anemic rats [13].
Therefore, anemia in AA patients could induce HIF-1aexpression, which results in increased VEGF production.
AA patients have been reported to have up-regulated
thrombopoietin [14], which has been shown to stabilize
HIF-1a protein [15]. This would also result in increased
VEGF production. Further studies are necessary to more
fully investigate the regulation of HIF-1a in AA patients.
Acknowledgments The authors gratefully acknowledge the excel-
lent laboratory assistance of the research technologist Mami
Sakaemura.
Conflict of interest The authors declare that they have no com-
peting interests
References
1. Khatib Z, Wilimas J, Wang W. Outcome of moderate aplastic
anemia in children. Am J Pediatr Hematol Oncol. 1994;16:80–5.
2. Howard SC, Naidu PE, Hu XJ, Jeng MR, Rodriguez-Galindo C,
Rieman MD, et al. Natural history of moderate aplastic anemia in
children. Pediatr Blood Cancer. 2004;43:545–51.
3. Nishio N, Yagasaki H, Takahashi Y, Muramatsu H, Hama A,
Yoshida N, et al. Natural history of transfusion-independent
non-severe aplastic anemia in children. Int J Hematol. 2009;89:
409–13.
4. Davies JK, Guinan EC. An update on the management of severe
idiopathic aplastic anaemia in children. Br J Haematol. 2007;136:
549–64.
5. Fureder W, Krauth MT, Sperr WR, Sonneck K, Simonitsch-
Klupp I, Mullauer L, et al. Evaluation of angiogenesis and vas-
cular endothelial growth factor expression in the bone marrow of
patients with aplastic anemia. Am J Pathol. 2006;168:123–30.
Fig. 2 a The median corrected VEGF in AA patients was signif-
icantly greater than in the control subjects. b The median corrected
VEGF levels in chronic AA patients were significantly greater than
those in acute AA patients. Closed squares acute, severe. Opensquares acute, moderate. Open triangles chronic, moderate. Closedtriangles chronic, mild
498 Y. Kodama et al.
123

6. Gunsilius E, Petzer AL, Gastl G. Correspondence re: P. Salven
et al. Leukocytes and platelets with cancer contain high levels of
vascular endothelial growth factor. Clin Cancer Res. 1999;5:
487–1. Clin Cancer Res. 1999; 5: 2978–9.
7. Hashiguchi T, Arimura K, Matsumuro K, Otsuka R, Watanabe O,
Jonosono M, et al. Highly concentrated vascular endothelial
growth factors in platelets in Crow-Fukase syndrome. Muscle
Nerve. 2000;23:1051–6.
8. Hall SE, Rosse WF. The use of monoclonal antibodies and flow
cytometry in the diagnosis of paroxysmal nocturnal hemoglo-
binuria. Blood. 1996;87:5332–40.
9. Mohle R, Green D, Moore MAS, Nachman RL, Rafii S. Con-
stitutive production and thrombin-induced release of vascular
endothelial growth factor by human megakaryocytes and plate-
lets. Proc Natl Acad Sci USA. 1997;94:663–8.
10. George ML, Eccles SA, Tutton MG, Abulafi AM, Swift RI.
Correlation of plasma and serum vascular endothelial growth
factor levels with platelet count in colorectal cancer: clinical
evidence of platelet scavenging? Clin Cancer Res. 2000;6:
3147–52.
11. Gunsilius E, Gastl G. Platelet and VEGF blood levels in cancer
patients. Br J Cancer. 1999;81:184–6.
12. Semenza GL. Regulation of mammalian O2 homeostasis by
hypoxia-inducible factor 1. Annu Rev Cell Dev Biol. 1999;15:
551–78.
13. McLaren AT, Marsden PA, Mazer CD, Baker AJ, Stewart DJ,
Tsui AK, et al. Increased expression of HIF-1a, nNOS, and
VEGF in the cerebral cortex of anemic rats. Am J Physiol Regul
Integr Comp Physiol. 2007;292:R403–14.
14. Marsh JC, Gibson FM, Prue RL, Bowen A, Dunn VT, Hornkohl
AC, et al. Serum thrombopoietin levels in patients with aplastic
anaemia. Br J Haematol. 1996;95:605–10.
15. Kirito K, Fox N, Komatsu N, Kaushansky K. Thrombopoietin
enhances expression of vascular endothelial growth factor
(VEGF) in primitive hematopoietic cells through induction of
HIF-1a. Blood. 2005;105:4258–63.
Corrected VEGF is associated with the clinical course of AA 499
123