-
8/3/2019 Vas Si Oncology Po
1/6
277Volume 6, N umber 6
July /A ugust 2008 .Suppo t Oncology.n t
J Support Oncol 2008;6:277282 2008 Elsevier Inc. All rights
reserved.
r e v i e w
Abstract Assessment o quality o li e (QOL) in cancer clinical
trials isimportant when comparing treatments, especially when
prolonged sur-vival is not expected. QOL scores may re ect physical
or psychosocialunctioning or distress. The choice o QOL instrument
depends uponthe defnition, research hypothesis, cancer population,
depth and sen-sitivity o in ormation required, and requency o
measurement. A visualanalogue scale (VAS) is commonly used to rate
various subjective ex-
periences. Potential advantages o these scales include their
wide scorerange and high sensitivity; disadvantages include lower
completionrates than other rating scales. Single-item VASs are
validated or cancerQOL, reliable, and responsive to change. These
scales may best representan individuals global QOL without the
constraints o predetermined do-mains. Single items are use ul or
requent measurements in palliativeor advanced populations and when
in ormation about domains is lessimportant. Multi-item VAS QOL
instruments vary in length and domains;they are use ul in clinical
trials enrolling patients with good per ormancestatus, but some are
long and disease-specifc.
aluat ng sp c c th ap s should nclud thl ant ad s cts ( g, naus
a/ om t ng, ha
loss, s xual unct on, ndoc n symptoms). in pa-t nts th ad anc d
canc , mpo tant doma nsmay d ( g, sp tual ty, s ns o bu d n). Thl
ngth, numb o qu st ons, and at ng scal allnfu nc th as o a scal s
compl t on. A b nst um nt may b mo l ant n cl n cal s tua-t ons and
ad anc d d s as . in s a ch, a balancmust b st uck b t n compl t n
ss o n o ma-t on and sk o m ss ng data.
Subj ct xp nc s such as QOL and symp-toms can b aluat d by d nt
at ng scal s,
nclud ng num cal ( g, 010), cat go cal ( g,m ld, mod at , s ), o
sual ( , sual ana-logu scal ; vAS). A vAS s a l n , usually m a-su
ng 10 cm, th d sc pto s at ach nd ( g,good to bad, non to s ). r
spond nts placa ma k along th l n nd cat ng th subj ctxp nc . Th
sco s m asu d as th d stanco th ma k om on nd o th l n . Usually,
thl n do s not ha ma k ngs, o ds, o numb salong t. vASs ha b n d sc
b d as s mpl ,
Manusc pt subm tt d Ma ch 29, 2007;acc pt d Ma ch 16, 2008.
Co spond nc to: D clan walsh, MSc, FACP, FrCP, D -cto , Th Ha y
r. Ho tz C nt o Pall at M d c n ,
Th Cl land Cl n c Foundat on, 9500 eucl d A nu , M76,Cl land, OH
44195; t l phon : (216) 444-7793; ax: (216)445-5090; -ma l:
[email protected] g
D . Haus s a r s a chF llo and D . walsh sP o sso and D ctoat Th
Ha y r. Ho tzC nt o Pall atM d c n , Cl landCl n c Tauss g CancC nt
, Cl land, Oh o.
Visual Analogue Scales and Assessment
o Quality o Li e in CancerKatherine Hauser, MD, and Declan
Walsh, MSc, FACP, FRCP (Edin)
Qual ty-o -l (QOL) ass ssm nt s m-po tant n canc cl n cal t als,
sp -c ally h n p olongat on o su al snot xp ct d ( g, th ad anc d d
s aso symptomat c t atm nts). QOL m asu s mayd st ngu sh b t n t
atm nts o s m la cacybut d nt t atm nt bu d n o tox c t s. QOLass
ssm nt may also ha a ol n cl n cal p act c ,
nclud ng n sc n ng o phys cal and psychosoc ald st ss and aluat
on o pall at t atm nt. 1
Th s no s ngl acc pt d QOL d n t on. 2 QOL s g n ally acc pt d
to ncompass th holo l , nclud ng h alth; sat s act on; happ n
ss;and nanc al, soc al, and n onm ntal conc ns.H alth- lat d QOL
(HrQOL) s to th m-pact o lln ss o t atm nt on QOL. H alth- lat dQOL
s mult d m ns onal ( nclud ng phys cal, psy-cholog cal, soc al, and
unct onal doma ns). 2,3 QOLmay also b d n d by th nd dual. Th gap
th -o y d n s QOL as th gap b t n an nd dualsxp ctat on o l and h s
o h al ty. 4 P opl npoo h alth may d sc b good QOL b caus thxp nc m
ts xp ctat ons. Doma ns such asam ly, lat onsh ps, sp tual ty, s ns
o cont ol,and autonomy may b mo mpo tant to pat ntsthan a phys cal
xp nc s. 5
Assessing QOLTh s no gold standa d o QOL ass ssm nt.
Th cho c o nst um nt s nfu nc d by th s t-uat on (cl n cal o s a
ch), th stag o d s as( a ly, ad anc d, su o ), and th t atm nt(cu
at , pall at ). Canc stag and t atm nt
nfu nc l ant doma ns. QOL nst um nts o
-
8/3/2019 Vas Si Oncology Po
2/6
278 .Suppo t Oncology.n t t he JourNAl of s upportiVe o
Ncology
vASs ha sho n mp o d QOL th pa n l , 15,16 stablQOL n pat nts n
hosp c ca , 17 and spons to st uctu dnt nt on du ng ad oth apy.
18
On ssu th s ngl - t m vASs s h th a mult d -m ns onal conc pt l
k QOL can b captu d n a s ngl l n .S ngl - t m scal s do not aluat
th doma ns cont but ngto QOL and thus p o d no n o mat on xpla n ng
th o -all at ng. Ho , many mult d m ns onal nst um nts lyon xp ts
to d t m n doma ns and th ght ng; th ymay not t uly p s nt doma ns
mpo tant to an nd dual.S ngl - t m scal s l a th d n t on o QOL to
th nd -dual spond nt.
in hosp c ca , s ngl - t m QOL co lat d ll th cog-n t , phys
cal, and sp tual ll-b ng and soc al act ty butnot th soc al suppo
t. 18 S m la ly, th eOrTC (eu op anO gan zat on o r s a ch and T
atm nt o Canc ) QLQ-C30 (Qual ty-o -L Qu st onna Co 30) global
QOLsubscal (num cal) co lat d mod at ly th phys cal, ol ,cogn t ,
mot onal, and soc al unct on ng; at gu ; and pa ndoma ns but l ss
th naus a and om t ng. 19 Th m an ng
o th t m QOL may a y by ag , cultu , ducat on, andlanguag .
Global nd cato s ( g, t atm nt bu d n) may alloa compa son b t n d
nt t atm nts ac oss t als. 20,21
The Spitzer Uniscale.Th Sp tz Un scal s a s ngl qu s-t on: Pl as
at you o all QOL. 22,23 O g nally d s gn do phys c an at ng, t s no
us d o both pat nt and obsQOL at ngs. 23 Th Sp tz Un scal s al d,
th mod at toh gh co lat ons th mult d m ns onal QOL m asu s; t ss
ns t to chang s n p o manc status, symptoms, and p o-g ss d s as
and co lat s th su al. 23 Phys c an sco sag mod at ly th pat nts
sco s, although th y t nd tound st mat QOL. Th compl t on at s abo
90%.
r spond nts ma k an X n a box th ancho s lo stqual ty to h gh st
qual ty. Th o g nal Un scal d sc pt ond d not sp c y th l ngth o th
box, no h on th X thsco as m asu d. Sco ng has b n d sc b d as th
014o 0100. Som autho s adapt d t to a s ngl -l n vAS thth sam ancho
s.
MULTI-ITEM VASS FOR QOL
Mult pl - t m vASs o canc QOL st d sc b d n1976.7 T n ho zontal
vASs ass ss d phys cal and psycholog -cal symptoms, act ty, soc al
and ol act t s, and ll-b -ng. Sco s spons to t atm nt and tox c ty.
S almult d m ns onal vAS QOL nst um nts ha b t n 8 and
53 t ms. Th y may b g n al ( g, GLQ824
) o d s as -sp c c(Lung Canc Symptom Scal [LCSS] 25,26 o th P
ostat Can-c Sp c c QOL inst um nt [PrOSQOLi]). 2729 Althoughdoma ns
a y, th y all ass ss pa n and app t t but l ss o t nnaus a and at
gu . Many a l ngthy, l m t ng th us uln ssto cl n cal t als, and a
not l ant o ad anc d canc opall at populat ons. Compl t on at s a n
qu ntly -po t d. wh n po t d, th y a h gh (80%90%). 24,30 Fam lys
mpo tant n th QOL o canc pat nts but n qu ntlyass ss d. S m la ly,
sp tual ty s ass ss d n only on mult -
h ghly s ns t , and l abl at ng scal s o subj ct x-p nc s. 6 Th
ma n ad antag o a vAS s that spond ntsmay nd cat any plac along th
l n ath than b st ct dby cat go s o numb s.
vASs ha b n us d to ass ss canc QOL s nc 1976. 7 Th s a t cl a
ms to th ol o vASs n th aluat ono canc QOL and th m thodolog c ssu
s assoc at d thth us .
VASs for QOL of Cancer PatientsvASs o QOL o canc pat nts may b s
ngl - t m, global
qu st ons ( g, ho s you QOL?) o mult - t m scal s. Mult -t m
scal s nclud nd dual qu st ons about many doma ns o QOL ( g,
symptoms, unct on, lat onsh ps) and may also n-clud a global scal .
Th s scal s o t n ha a summat d scop s nt ng o all QOL and may ha s
al subscal sco s.
S ngl - t m vASs o QOL ha b n sugg st d to b st p -s nt nd dual
QOL b caus th y do not const a n spons s toth doma ns d t m n d by
h alth ca p o d s. 5
SINGLE-ITEM VASs FOR QOL
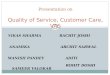
S al s ngl - t m vASs o QOL ha b n al dat dn oncology. Th y a y
n d s gn (F gu 1), th d sc pto snclud ng g n al ll-b ng, 8 l not o
th l ng, 9 phys calll-b ng, 10 cop ng, 11 and QOL. 12,13 S ngl - t
m QOL vASs
co lat ll th mult d m ns onal qu st onna s. 8,9,1114 T st- t st
8,12 and nt at 13 l ab l ty ha also b n d m-onst at d. vASs a spons
to ch moth apy- lat dchang s o t m and global at ngs o chang .
10,12 S ngl - t m
Visual Analogue Scales and Assessment of Quality of Life in
Cancer
Life is not worth living
Life could not be better
Worst imaginablequality of life
Perfectquality of life
How are you doing overall today?Worst possible Best possible
How would you rate your well-being today?Very low Very high
How would you rate your quality of li fe today?Very low Very
high
Figure 1 Examples o Global Quality-o -Li eVisual Analogue
Scale
-
8/3/2019 Vas Si Oncology Po
3/6
279Volume 6, N umber 6
July /A ugust 2008 .Suppo t Oncology.n t
d m ns onal qu st onna (th QOL-rTi [QOL-rad at on
Th apy inst um nt], h ch has subs qu ntly chang d to anum cal o
mat). 31 General scales. G n al vAS nst um nts a d sc b d n
Tabl 1. 7,2426,2840 Many nclud a s ngl - t m o all QOLscal o a
summat d sco .
Lung cancer. Th s l - po t d LCSS has s x symptom (ap-p t t
loss, cough, dyspn a, at gu , h moptys s, pa n) and thsumma y scal
s (symptom d st ss, no mal act ty, and o allQOL). 25,26,39,40 An
obs scal at s th s x symptoms on o -d nal scal s. it s ll al dat d
by co lat ons th oth n-
st um nts and p o manc status and has nt nal cons st ncy
as ll as t st- t st and nt at l ab l ty. r spons n sshas not b n
t st d. Num cal and m soth l oma scal s hab n al dat d. 41,42 Th m
an compl t on t m s 8 m nut s opat nts and 2 m nut s o obs s. Th
LCSS f ct d thb n t o doc tax l (Taxot ) ch moth apy o no lb no b
st suppo t ca n ad anc d lung canc 43,44 and b t-t QOL n non smok
s. 45 Th app t t and at gu subscal snd p nd ntly p d ct su al. 46
Th LCSS s comput z d ohand-h ld d c s, s asy to us , and s abl to
nhanc com-mun cat on and sat s act on th cl n c s ts. 47
Hauser and Walsh
Table 1
Multi-item Quality-o -Li e Visual Analogue ScaleAUTHOR
ORINSTRUMENT DESIGN DOMAINS PSYCHOMETRICS
Priestman and Baum 7,32 10 horizontal VASs Well-being, mood,
activity, pain, nausea, Responsive to change with
chemotherapy,(1976, 1983) appetite, housework, social activities,
endocrine therapy
anxiety, treatment response Test-retest reliability at 24
hours
Padilla et al33
14 horizontal VASs General physical condition (pain, appetite,
Discriminates inpatient/outpatient,(1983) nausea, strength)
analgesic useImportant activities Internal consistencyOverall QOL
Test-retest reliability
Selby et al 3436 29 horizontal VASs 5- actor structure: physical
activities, Correlations with SIP, KPS(1984, 1988, 1992) emotional,
alimentary, appearance, Discriminates metastatic disease/early,
and concentration and language chemotherapy or notInternal
consistency Test-retest reliability at 912 hoursInterrater
reliability
Holmes and Dickerson 37 26 horizontal VASs Symptoms, 11 items
Discriminates inpatient vs outpatient(1987) Activities o daily
living, 15 items Internal reliability
Test-retest reliability at 1 hourCoates et al 8 horizontal VASs
Physical symptoms: pain, atigue, Correlations with FLIC, PACIS,
PACGLQ824 appetite/sense o taste, nausea/vomiting, Discriminates
chemotherapy and
(1990) hair loss numbness/pins and needles per ormance
statusAnxiety, depression, sexual interest Test-retest reliability
at 1 and 24 hours Thought o having treatmentGlobal QOL
Ballatori et al 38 49 items, 10 cm horizontal 3 actors:
psychological, relationship to Discriminates per ormance status
(1993) VASs hospital, and appetite Test-retest reliability at 24
hoursHollen et al Patient scale: 9 horizontal 6 symptoms: appeti te
loss, cough, dyspnea, Correlates with KPS, SIP, POMSLCSS25,26,39,40
VASs atigue, hemoptysis, pain Discriminates per ormance status,
cancer(1993, 1994, 1999) Observer scale: 6 symptoms 3 summary
scales: symptom distress, stage
(ordinal scale) normal activity, and overall QOL Internal
reliabilityEach item on a separate card Test-retest reliability at
1 hour
Modifed and validated or mesothelioma 41 Numerical orm validated
42
Johnson et al 24 horizontal VASs 4 domains: unctional/health,
Correlates with FPQLIQOL-RTI31 socioeconomic/ amily, general QOL,
Internal consistency
(1994) emotional/psychological Test-retest reliability at 1 week
Subsequently, scaling changed to
numerical 010, and head and neck module added
Tannock et al, 9 horizontal VASs Physical symptoms (appetite,
constipation, Correlates with EORTC QLQ-C30Stockler et al atigue,
pain, passing urine, physical Discriminates per ormance
status,PROSQOLI2830 activity), mood, amily, and global hemoglobin
level, analgesic score, and(1996, 1998, 1999) well-being
survival
Responsive to treatment
Abbreviations: EORTC QLQ-C30 = European Organization or Research
and Treatment o Cancer Quality-o -Li e Questionnaire C30; FLIC =
Functional Living IndexCancer; FPQLI = Ferrans andPowers Quality o
Li e Index; KPS = K arno sky Per ormance Status; LCSS = Lung Cancer
Symptom Scale; PAC = Psychological Adjustment to Cancer Scale;
PACIS = Perceived Adjustment to ChronicIllness Scale; POMS = Profle
o Mood States; PROSQOLI = Prostate Cancer Specifc Quality o Li e
Instrument; QOL = quality o li e; QOL-RTI = Quality o Li
e-Radiation Therapy Instrument; SIP =Sickness Impact Profle; VAS =
visual analogue scale
-
8/3/2019 Vas Si Oncology Po
4/6
280 .Suppo t Oncology.n t t he JourNAl of s upportiVe o
Ncology
At th s t m , ho , only th LCSS has po t d sults than l ct on c
s on. 47
Cons nsus s lack ng about th stat st cal analys s o vASdata.
59,60 issu s n ol h th th data a o d nal o at oand h th sco s a no
mally d st but d and thus appl -cabl o pa am t c analys s. Compa
son o pa am t c ( thand thout t ans o mat on) and nonpa am t c
analys s o vAS pa n sco s sugg st d that pa am t c t sts accu-at
and had th g at st po to d t ct a d nc , d sp ta lack o no mal d st
but on o th data. 61
COMPLETION RATES
Compl t on o a vAS qu s conc ptual zat on o a com-pl x xp nc to
a s ngl l n . vAS pa n scal s ha locompl t on at s than num cal o
cat go cal scal s. 62,63 rat s a ad s ly a ct d by nc as ng ag , h
gh op o ddos , and th p s nc o con us on. 62,63 Ta n ng n vAS t
ch-n qu s mo t m -consum ng than o oth at ng scal s. 64 in QOL stud
s, th Un scal has a s m la compl t on at tooth mult - t m nst um
nts. 23 Both th PrOSQOLi 28 and
LCSS43
ha h gh compl t on at s (> 80%) n cl n cal t als.Th eSAS
compl t on at d cl n s th ad anc ng d s as .
SENSITIVITY
vASs a sa d to b mo s ns t to subj ct chang sthan a num cal o
cat go cal scal s. Ho , t s uncl ah th such h gh s ns t ty s cl n
cally l ant. Stud s o QOL n ca d ac and sp ato y a lu ha d monst at
da 7-po nt bal d sc pto scal had qual s ns t ty to avAS. 64,65 val
dat on o a 010 num cal LCSS d monst at-d good ag m nt th a vAS. 42
Compa son o a vAS nth PrOSQOLi th qu al nt L k t scal s o th
eOrTCQLQ-C30 d monst at d sup o s ns t ty o th vAS opa n and oth
phys cal symptoms. 28 All scal s d nt at dt atm nt g oups, but th
vAS as l ss s ns t n compl xdoma ns l k am ly and mot onal unct
on.
CLINICAL SIGNIFICANCE
Small chang s on a vAS ( g, 05 mm) may b stat st callys gn cant
but cl n cally l ant. Th cl n cal s gn canccan b aluat d by compa
ng vAS sco s th a globalchang scal ( g, om much b tt to much o s ).
Fo acutpa n, th m n mal cl n cally s gn cant vAS chang s 13mm.66
ind ct LCSS analys s suppo t d cl n cally s gn cantchang s o 1025
mm. 67 Cl n cally s gn cant chang has b n
sugg st d as 50% o th scal s standa d d at on ( , 810mm on a
100-mm vAS). 21 Th s sult ould b qu al nt toa chang o 1 on an 11-po
nt num cal scal .
Instrument SelectionS al acto s a ct th s l ct on o an nst um
nt. Popu-
lat on cha act st cs ( nclud ng ag , d agnos s, and p o -manc
status) a ct compl t on at s and h th a d s as -sp c c o g n al qu
st onna s app op at . in s a ch,th d n t on and hypoth s s nfu nc
th s cho c , pa t cu-
Prostate cancer. Th PrOSQOLi has n n vASs ass ss-ng phys cal
symptoms (app t t , const pat on, at gu , pa n,pass ng u n , phys
cal act ty), mood, am ly, and globalll-b ng. 29,30 it ms co lat mod
at ly th th eOrTC
QLQ-C30. it d sc m nat s pat nts by p o manc status,h moglob n l
l, analg s c sco , and su al. it has d mon-st at d mp o d o all QOL
n ad anc d ho mon - ac-to y p ostat canc pat nts ho spond d to m
toxant onand p dn solon . 30
PROXY MEASURES OF QOL
A vAS may also b us d to aluat sp c c doma ns o QOL ( g, nd dual
symptoms o psycholog cal conc ns).
Single-item VASs.S ngl - t m vASs a al d o ass ssm nto pa n and
d p ss on n canc . 48,49 Th y a us ul n cl n calt als h n chang n
nd dual symptoms s xp ct d. Th ymay b pa d th a s ngl - t m QOL
scal to n st gat thmpact o symptoms on o all QOL. 15
Edmonton Symptom Assessment Scale (ESAS). Th eSASas d s gn d o
pall at populat ons. N n vASs aluat
symptoms (act ty, anx ty, app t t , d p ss on, d o s n ss,pa n,
naus a, sho tn ss o b ath, and ll-b ng); sco s asummat d to a d st
ss sco . 50 it s al d th nt nal cons s-t ncy and t st- t st l ab l
ty. 51 int at stud s al ano st mat on o symptoms by ca g s and an
und st -mat on o symptoms by phys c ans. 50,52 Th compl t on at sa
y by stag o d s as . Most g n al oncology pat nts cancompl t t on
hosp tal adm ss on, compa d th 63%84%o pall at m d c n canc pat nts
and only 15% o t -m nal pat nts. 50,51,53 rout n us o eSAS on adm
ss on to apall at m d c n un t has sho n s gn cant und ass ss-m nt
and docum ntat on o symptoms, sp c ally nact ty,mpa d ll-b ng, and
anx ty. 54
The Distress Thermometer. Th D st ss Th mom t s amod d vAS: a t
cal th mom t numb d 010 thth o ds no d st ss, mod at d st ss, and s
d st ssalong th scal . 5557 it has a 34- t m p obl m ch ckl st,
n-clud ng phys cal and psychosoc al conc ns. it s al dat dn canc
populat ons and ad ocat d o out n sc n ng. 58 Sco s o at l ast 4 a
comm nd d as th t gg o u thaluat on and nt nt on. Th s no d nc as
to th
assoc at on b t n D st ss Th mom t sco s and QOLo cl n cal
outcom s om out n sc n ng.
Methodologic Issues
Many stud s al dat ng QOL nst um nts a con n nco cl n cal t al
sampl s. Th s act pot nt ally l m ts th l-anc o th s nst um nts to
s l ct d populat ons. Oth
m thodolog c ssu s nclud th pot nt al o m asu m nto and th unsu
tab l ty o t l phon ollo -up. Sco ng
a vAS qu s m asu m nt ath than s mply ad ng oma pap , pot nt
ally add ng a sou c o o . vAS qu st on-na s must b p nt d nd
dually, as photocopy ng can d s-to t th l ngth o th l n , l ad ng
to ncons st nt sco ng. AvAS can b comput z d, th by a o d ng such d
cult s.
Visual Analogue Scales and Assessment of Quality of Life in
Cancer
-
8/3/2019 Vas Si Oncology Po
5/6
281Volume 6, N umber 6
July /A ugust 2008 .Suppo t Oncology.n t
la ly h th global QOL o sp c c doma ns a mpo tanto l k ly to
chang th nt nt on.
Th cho c o scal (vAS, num cal, o cat go cal) d -p nds upon th
data s ns t ty qu d and th d s dcompl t on at s. inst um nts that
app a to b l ant tocl n cal p act c nclud s ngl - t m global scal s
(QOL, t at-m nt bu d n), th eSAS, th D st ss Th mom t , and thLCSS.
inst um nts th num cal o cat go cal scal s mayb as to compl t and
sco , and chang s may b mol ant to cl n cal p act c . M asu m nt qu
ncy s mpo -
tant; s ngl - t m vASs may b us ul o qu nt m asu sand may a o d
pat nt bu d n. S ngl - t m QOL nst um ntsmay b o th h l n cl n cal
t als ( sp c ally long tud nalon s) o cl n cal sc n ng (pa n, d p
ss on, ad anc d can-c ) and o global QOL. 13 in symptom l t als,
comb n ngsymptom and s ngl - t m QOL vASs ass ss s th mpact o
symptoms on QOL. S ngl t ms a l ant and may b stp s nt hat th pat
nt s xp nc ng. wh th th scoang 0100 s n c ssa y s d batabl ; p haps
a sco ang o only 010 s n d d.
Future ResearchCla cat on o th d al at ng scal s o QOL s n c
s-
sa y. D lopm nt and us o pat nt- ocus d nst um ntsmay balanc th
bu d n on spond nts and cl n cally l-ant data. Compl t on at s n d
to b docum nt d n
uns l ct d cl n cal populat ons. Cl n cally s gn cant cuto po
nts and sco d nc s should b d t m n d o globaland mult - t m nst um
nts. in add t on, n o mat on aboutth most app op at QOL nst um nts
o cl n cal p act cand d nc o mp o d outcom s as a sult o th ou-t n
us a n c ssa y.
ConclusionS ngl - t m QOL vASs ac l tat an nd dual d n -
t on o QOL and a us ul n ad anc d o pall at pop-ulat ons and
long tud nal stud s. Th y a s ns t andspons to chang th t m and t
atm nt. Mult - t m
vAS nst um nts a o t n l ngthy and d s as -sp c c;th y a us ul n
s a ch stud s, g n pat nts haa good p o manc status. vASs a mo d
cult tocompl t than a oth at ng scal s and ha th po-t nt al o m asu
m nt o . Th vAS sco ang may
not t anslat nto cl n cal s gn canc . Fu th s a ch sn d d to d t
m n h th QOL vASs a app op ato cl n cal p act c .
References
1. Sloan JA, Frost MH, Berzon R, et al. The clinicalsignifcance
o quality o li e assessments in oncol-ogy: a summary or clinicians.
Support Care Cancer2006;14:988998. [1679481]
2. Ferrans CE. Defnitions and conceptual modelso quality o li e.
In: Lipscomb J, Gotay C, Snyder C, eds.Outcomes Assessment in
Cancer. Measures, Methodsand Applications. Cambridge, UK:
CambridgeUniversity Press; 2005:1430.
3. Wilson IB, Cleary PD. Linking clinical vari ableswith
health-related quality o li e: a conceptualmodel o patient
outcomes. JAMA 1995;273:5965.[7996652]
4. Calman KC. Quality o li e in cancer patientsan hypothesis. J
Med Ethics 1984;10:124127.[6334159]
5. McCabe C, Begley C, Collier S, McCann S.Methodological issues
related to assessing andmeasuring quality o li e in patients with
cancer:implications or patient care. Eur J Cancer Care
(Engl)2008;17:5664. [18181892]
6. McCormack HM, Horne DJ, Sheather S. Clinicalapplications o
visual analogue scales: a critical review.
Psychol Med 1988;18:10071019. [3078045]7. Priestman TJ, Baum M.
Evaluation o quality
o li e in patients receiving treatment or advancedbreast cancer.
Lancet 1976;1:899900. [58161]
8. Gough IR, Furnival CM, Schilder L, Grove W.Assessment o the
quality o li e o patients with ad-vanced cancer. Eur J Cancer Clin
Oncol 1983;19:11611165. [6684561]
9. Khalil HS, Feldman M, Bridger MW. A simpleassessment o
quality o li e in head and neck cancerpatients: what can it tell
us? Rev Laryngol Otol Rhinol(Bord) 2003;124:211214. [15038562]
10. Bernhard J, Sullivan M, Hrny C, Coates AS,Rudenstam CM.
Clinical relevance o single itemquality o li e indicators in cancer
clinical trials. Br JCancer 2001;84:11561165. [11336464]
11. Hrny C, Bernhard J, Bacchi M, et al. ThePerceived Adjustment
to Chronic Illness Scale (PACIS):a global indicator o coping or
operable breast can-cer patients in clinical trials. Swiss Group or
ClinicalCancer Research (SAKK) and the International BreastCancer
Study Group (IBCSG). Support Care Cancer1993;1:200208.
[8193882]
12. de Boer AG, van Lanschot JJ, Stalmeier PF,et al. Is a
single-item visual analogue scale as valid,reliable and responsive
as multi-item scales in mea-suring quality o li e? Qual Li e Res
2004;13:311320.[15085903]
13. Sloan JA, Aaronson N, Cappelleri JC, FaircloughDL,
Varricchio C; Clinical Signi icance ConsensusMeeting Group.
Assessing the clinical signifcance o single items relative to
summated scores. Mayo ClinProc 2002;77:479487. [12004998]
14. Donnelly S, Walsh D. Quality o li e assessmentin advanced
cancer. Palliat Med 1996;10:275283.
[8931062]15. Stockler M, Vardy J , Pi l la i A, Warr D.
Acetaminophen (paracetamol) improves pain andwell-being in
people with advanced cancer alreadyreceiving a strong opioid
regimen: a randomized,double-blind, placebo-controlled cross-over
trial. JClin Oncol 2004;22:33893394. [15310785]
16. Chang VT, Hwang SS, Kasimis B. Longitudinaldocumentation o
cancer pain management out-comes: a pilot study at a VA medical
center. J PainSymptom Manage 2002;24:494505. [12547049]
17. Bretscher M, Rummans T, Sloan J, et al. Quality o
li e in hospice patients: a pilot study.
Psychosomatics1999;40:309313. [10402876]
18. Rummans TA, Clark MM, Sloan JA, et al.Impacting quality o li
e or patients with advancedcancer with a structured
multidisciplinary interven-tion: a randomized controlled trial. J
Clin Oncol2006;24:635642. [16446335]
19. Aaronson NK, Ahmedzai S, Bergman B, et al. TheEuropean
Organization or Research and Treatmento Cancer QLQ-C30: a quality-o
-li e instrument oruse in international clinical trials in
oncology. J NatlCancer Inst 1993;85:365376. [8433390]
20. Bernhard J, Maibach R, Thrlimann B, Sessa C,Aapro MS; Swiss
Group or Clinical Cancer Research.Patients estimation o overall
treatment burden: whynot ask the obvious? J Clin Oncol
2002;20:6572.[11773155]
21. Sloan J. Asking the obvious quest ions re-garding patient
burden. J Clin Oncol 2002;20:46.[11773146]
22. Spitzer WO, Dobson AJ, Hall J, et al. Measur ingthe quality
o li e o cancer patients: a concise QL-in-dex or use by physicians.
J Chronic Dis 1981;34:585
597. [7309824]23. Sloan JA, Loprinzi CL, Kuross SA, et al.
Randomized comparison o our tools measuringoverall quality o li
e in patients with advanced cancer.J Clin Oncol 1998;16:36623673.
[9817289]
24. Coates A, Glasziou P, McNeil D. On the receiv-ing endIII.
measurement o quality o li e duringcancer chemotherapy. Ann Oncol
1990;1:213217.[2261367]
25. Hollen PJ, Gralla RJ, Kris MG, Cox C. Quality o li e during
clinical trials: conceptual model or theLung Cancer Symptom Scale
(LCSS). Support Care
PubMed ID in brackets
Hauser and Walsh
-
8/3/2019 Vas Si Oncology Po
6/6
282 .Suppo t Oncology.n t t he JourNAl of s upportiVe o
Ncology
Cancer 1994;2:213222. [8087439]26. Hollen PJ, Gralla RJ, Kris
MG, et al. Measurement
o quality o li e in patients with lung cancer inmulticenter
trials o new therapies: psychometric as-sessment o the Lung Cancer
Symptom Scale. Cancer1994;73:20872098. [8156514]
27. Tannoc k I, Gospodarowicz M, Meakin W,Panzarella T, Stewart
L, Rider W. Treatment o meta-static prostatic cancer with low-dose
prednisone:evaluation o pain and quality o li e as pragmatic
indices o response. J Clin Oncol 1989;7:590597.[2709088]
28. Stock ler MR, Osoba D, Goodwin P, Corey P, Tannock IF.
Responsiveness to change in health-related quality o li e in a
randomized clinical trial: acomparison o the Prostate Cancer
Specifc Qualityo Li e Instrument (PROSQOLI) with analogousscales
rom the EORTC QLQ-C30 and a trial specifcmodule. European
Organization or Research and Treatment o Cancer. J Clin Epidemiol
1998;51:137145. [9474074]
29. Stockler MR, Osoba D, Corey P, Goodwin PJ, Tannock IF.
Convergent discriminitive, and predictivevalidity o the Prostate
Cancer Specifc Quality o Li eInstrument (PROSQOLI) assessment and
comparisonwith analogous scales rom the EORTC QLQ-C30 and
a trial-specifc module. European Organisation orResearch and
Treatment o Cancer. Core Quality o Li e Questionnaire. J Clin
Epidemiol 1999;52:653666.[10391659]
30. Tannock IF, Osoba D, Stockler MR, et al.Chemotherapy with
mitoxantrone plus prednisone orprednisone alone or symptomatic
hormone-resistantprostate cancer: a Canadian randomized trial
withpalliative end points. J Clin Oncol
1996;14:17561764.[8656243]
31. Johnson DJ, Casey L, Noriega B. A pilot study o patient
quality o li e during radiation therapy treat-ment. Qual Li e Res
1994;3:267272. [7812279]
32. Coates A, Dillenbeck CF, McNeil DR, et al. On thereceiving
endII. Linear Analogue Sel -Assessment(LASA) in evaluation o
aspects o the quality o li e
o cancer patients receiving therapy. Eur J Cancer ClinOncol
1983;19:16331637. [6315445]33. Padilla GV, Presant C, Grant MM,
Metter G,
Lipsett J, Heide F. Quality o li e index or patients withcancer.
Res Nurs Health 1983;6:117126. [6556698]
34. Selby PJ, Chapman JA, Etazadi-Amoli J, DalleyD, Boyd NF. The
development o a method or a ssess-ing the quality o li e o cancer
patients. Br J Cancer1984;50:1322. [6743512]
35. Boyd NF, Selby PJ, Sutherland HJ, Hogg S.Measurement o the
clinical status o patients withbreast cancer: evidence or the
validity o sel assess-ment with linear analogue scales. J Clin
Epidemiol1988;41:243250. [3339377]
36. Bliss JM, Selby PJ, Robertson B, Powles TJ. Amethod or
assessing the quality o li e o cancerpatients: replication o the
actor structure. Br J Cancer1992;65:961966. [1616871]
37. Holmes S, Dickerson J. The quality o li e:design and
evaluation o a sel -assessment instru-ment or use with cancer
patients. Int J Nurs Stud1987;24:1524. [3644797]
38. Ballatori E, Roila F, Basurto C, et al. Reliabilityand
validity o a quality o li e questionnaire in cancerpatients. Eur J
Cancer 1993;29A(suppl 1):S63S69.
[8427728]39. Hollen PJ, Gralla RJ, Kris MG, Potanovich LM.
Quality o li e assessment in individuals with lung can-cer:
testing the Lung Cancer Symptom Scale (LCSS).Eur J Cancer
1993;29A(suppl 1):S51S58. [8381294]
40. Hollen PJ, Gralla RJ, Kris MG, Eberly SW, Cox C.Normative
data and trends in quality o li e rom theLung Cancer Symptom Scale
(LCSS). Support CareCancer 1999;7:140148. [10335932]
41. Hollen PJ, Gralla RJ, Liepa AM, Symanowski JT,
Rusthoven JJ. Adapting the Lung Cancer SymptomScale (LCSS) to
mesothelioma: using the LCSS-Meso conceptual model or validation.
Cancer2004;101:587595. [15274072]
42. Hollen PJ, Gralla RJ, Kris MG, McCoy S,Donaldson GW,
Moinpour CM. A comparison o vi-sual analogue and numerical rating
scale ormats orthe Lung Cancer Symptom Scale (LCSS): does ormata
ect patient ratings o symptoms and quality o li e?Qual Li e Res
2005;14:837847. [16022076]
43. Belani CP, Pereira JR, von Pawel J, et al. E ect o
chemotherapy or advanced non-small cell lung can-cer on patients
quality o li e: a randomized controlledtrial. Lung Cancer
2006;53:231239. [16787687]
44. Dancey J, Shepherd FA, Gralla RJ, Kim YS. Qualityo li e
assessment o second-line docetaxel versus
best supportive care in patients with non-small-celllung cancer
previously treated with platinum-basedchemotherapy: results o a
prospective, random-ized phase III trial. Lung Cancer
2004;43:183194.[14739039]
45. Garces YI, Yang P, Parkinson J, et al. The relation-ship
between cigarette smoking and quality o li e a -ter lung cancer
diagnosis. Chest 2004;126:17331741.[15596667]
46. Martin s SJ, Ho N, Cavamura SO, Harada CM,Yamamoto CA,
Takagaki TY. Lung cancer symptomsand pulse oximetry in the
prognostic assessmento patients with lung cancer. BMC Cancer
2005;5:72.[16000170]
47. Welch A, De Yoe N, Hollen P, Gralla R. How dopatients,
physicians and nurses using a computer-
assisted quality o li e instrument (LCSS-QL) in a pro-spective
multicenter clinical trial in non-small celllung cancer (NSCLC)
rate the scale? Poster presentedat the 18th Annual International
Symposium o theMultinational Association o Supportive Care
inCancer. June 2224, 2006. Toronto Canada.
48. Ahles TA, Ruckde schel JC, Blanchard EB.Cancer-related
painII. assessment with visualanalogue scales. J Psychosom Res
1984;28:121124.[6737324]
49. Fishman B, Pasternak S, Wallenstein SL,Houde RW, Holland JC,
Foley KM. The MemorialPain Assessment Card: a valid instrument or
theevaluation o cancer pain. Cancer 1987;60:11511158.[3300951]
50. Bruer a E, Kuehn N, Miller MJ, Selmser P,Macmillan K. The
Edmonton Symptom AssessmentSystem (ESAS): a simple method or the
assessmento palliative care patients. J Palliat Care
1991;7:69.[1714502]
51. Chang VT, Hwang SS, Feuerman M. Validationo the Edmonton
Symptom Assessment Scale. Cancer2000;88:21642171. [10813730]
52. Nekolaichuk CL, Bruera E, Spachynski K,MacEachern T, Hanson
J, Maguire TO. A comparison
o patient and proxy symptom assessments in ad-vanced cancer
patients. Palliat Med 1999;13:311323.[10659100]
53. Rees E, Hardy J, Ling J, Bradley K, AHern R. Theuse o the
Edmonton Symptom Assessment Scale(ESAS) within a palliative care
unit in the UK. PalliatMed 1998;12:7582. [9616443]
54. Strmgren AS, Groenvold M, Pedersen L,Olsen AK, Spile M,
Sjgren P. Does the medical recordcover the symptoms experienced by
cancer patients
receiving palliative care? A comparison o the recordand patient
sel -rating. J Pain Symptom Manage2001;21:189196. [11239737]
55. Akiz uki N, Akechi T, Nakani shi T, et al.Development o a
brie screening interview or adjust-ment disorders and major
depression in patients withcancer. Cancer 2003;97:26052613.
[12733160]
56. Gil F, Grassi L, Travado L, Tomamichel M,Gonzalez JR;
Southern European Psycho-OncologyStudy Group. Use o distress and
depression ther-mometers to measure psychosocial morbidity
amongsouthern European cancer patients. Support CareCancer
2005;13:600606. [15761700]
57. Jacobsen PB, Donovan KA, Trask PC, et al.Screening or
psychologic distress in ambula-tory cancer patients. Cancer
2005;103:14941502.
[15726544]58. National Comprehensive Cancer Network Clinical
Practice Guidelines in Oncology. DistressManagement. V.1.2008.
Available at: http://www.nccn.org/pro
essionals/physician_gls/PDF/distress.pd . Accessed May 22,
2008.
59. Wewe rs ME, Lowe NK. A critica l review o visual analogue
scales in the measurement o clini-cal phenomena. Res Nurs Health
1990;13:227236.[2197679]
60. Butler PV. Linear analogue sel -assessment andprocrustean
measurement: a critical review o visualanalogue scaling in pain
assessment. J Clin PsycholMed Settings 1997;4:111129.
61. Dexter F, Chestnut DH. Analysis o statisticaltests to
compare visual analog scale measurements
among groups. Anesthesiology 1995;82:896902.[7717561]62. Kremer
E, Atkinson JH, Ignelzi RJ. Measurement
o pain: patient pre erence does not con ound painmeasurement.
Pain 1981;10:241248. [7267140]
63. Paice JA, Cohen FL. Validity o a verbally admin-istered
numeric rating scale to measure cancer painintensity. Cancer Nurs
1997;20:8893. [9145556]
64. Guyatt GH, Townsend M, Berman LB, Keller JL.A comparison o
Likert and visual analogue scalesor measuring change in unction. J
Chronic Dis
1987;40:11291133. [3680471]65. Jaeschke R, Singer J, Guyatt GH.
Measurement
o health status: ascertaining the minimal clinicallyimportant di
erence. Control Clin Trials 1989;10:407415. [2691207]
66. Gallagher EJ, Liebman M, Bijur PE. Prospectivevalidation o
clinically important changes in pain se-verity measured on a visual
analog scale. Ann EmergMed 2001;38:633638. [11719741]
67. Hollen P, Gralla R. Clinical vs statistical signif-cance:
using the LCSS quality o li e instrument andKarno sky Per ormance
Status (KPS) to approach theproblem in patients with non-small cell
lung cancer(NSCLC). Proc Am Soc Clin Oncol 2000;19:2510.
Visual Analogue Scales and Assessment of Quality of Life in
Cancer