Embed Size (px)
DESCRIPTION
Teaching presentation on diagnosis and management of varicose veins.
Citation preview

Sarantos [email protected]
Airedale General HospitalAiredale General Hospital
Department of Surgery Teaching SessionDepartment of Surgery Teaching Session
27 August 200927 August 2009

“In A Surgeon's Gown (Good) Physicians May Make Some Progress”
Incidence Age Sex Geography Genetics Predisposing factors Macroscopic appearance Microscopic appearance Spread Prognosis: mortality and complications

25-50% of adult women 15-30% of adult men
Is it an industrialized country disease? UK: 45 000 hospital admissions per yearPatrick H. Carpentier, Hildegard R. Maricq, Christine Biro, Claire O. Poncot-Makinen, Alain Franco, Prevalence,
risk factors, and clinical patterns of chronic venous disorders of lower limbs: A population-based study in France, Journal of Vascular Surgery, Volume 40, Issue 4, October 2004, Pages 650-659, ISSN 0741-5214, DOI: 10.1016/j.jvs.2004.07.025.
Coon WW, Willis PW III, Keller JB. Venous thromboembolism and other venous disease in the Tecumseh community health study. Circulation 1973; 48: 839–846.
Franks PJ, Wright DD, Moffatt CJ, Stirling J, Fletcher AE, Bulpitt CJ et al. Prevalence of venous disease: a community study in west London. Eur J Surg 1992; 158: 143–147.
Bradbury A, Evans C, Allan P, Lee A, Ruckley CV, Fowkes FG. What are the symptoms of varicose veins? Edinburgh vein study cross sectional population survey. BMJ 1999; 318: 353–356

Family history of varicose veins (current hypothesis: autosomal dominant with variable penetrance mode of genetic transmission)
History of thromboembolic disease Number of pregnancies Activity (prolonged sitting or standing) Unskilled work Exercise less than once a week Height ObesityCornu-Thenard A, Boivin P, Baud MM, et al: Importance of the familial factor in varicose disease: Clinical study of
134 families. J Derm Surg Oncol 20:318-326, 1994Patrick H. Carpentier, Hildegard R. Maricq, Christine Biro, Claire O. Poncot-Makinen, Alain Franco, Prevalence, risk
factors, and clinical patterns of chronic venous disorders of lower limbs: A population-based study in France, Journal of Vascular Surgery, Volume 40, Issue 4, October 2004, Pages 650-659, ISSN 0741-5214, DOI: 10.1016/j.jvs.2004.07.025.

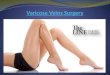
Dilated, tortuous, elongated superficial veins – Possible venous eczema – possible venous ulcers
Venous eczema
Images: Mr Neeraj Bhasin

Anatomy of the venous system of the leg▪ Deep veins▪ Posterior tibial▪ Anterior tibial▪ Peroneal▪ Soleal▪ Gastrocnemius▪ Popliteal▪ Femoral▪ Iliac
▪ Superficial veins▪ Long saphenous (LSV)▪ Short saphenous (SSV)


It was previously thought that axial destruction of venous valves led to transmission of ambulatory venous hypertension, causing reflux and varix formation.
However, Labropoulos and associates reported that the most common location for initial varicose vein formation was in the below-knee great saphenous vein (GSV) and its tributaries, followed by the above-knee GSV, and the saphenofemoral junction.
Their study clearly indicates that vein wall degeneration with subsequent varix formation can occur in any segment of the superficial and deep systems at any time and suggests a genetic component to the disease.
Labropoulos N, Giannoukas AD, Delis K, et al: Where does the venous reflux start? J Vasc Surg 26:736-742, 1997.

Asymptomatic Unsightly cutaneous veins Itching Corona phlebectatica (ankle/malleolar
flare) Lipodermatosclerosis Atrophie blanche Varicose eczema Edema Hemorrhage Chronic ulceration


Presenting Complaint: Varicosities, abdominal/groin lump – saphena varix
Symptoms Localized discomfort in the leg, Pain, Swelling,
Venous claudication, Itching “Risk” factors
Female, age, ethnicity, occupation, pregnancy, obesity, smoking
ASK about history of abdominal complaints/cancer, DVT, previous & other venous complaints

General OSCE tips: ICEPP Introduce – be polite and friendly Consent to examination Expose (adequately!) Position (standing initially) Pain – ask before examining the patient
Wash hands before examining the patient Cover and thank patient, present findings

Look at the legs whilst patient is standing Examine around the medial malleolus
‘gaiter area’ VVV LAPS
Varicose veins – distribution (LSV, SSV)Venous ulcers/eczemaVenous starsLipodermatosclerosisAtrophy blanchePitting oedemaScars

Venous ulcers/eczema
Venous stars (spider veins)
Atrophy blanche Ulceration: active and healed Leaves a white patch
Pitting oedema

Lipodermatosclerosis Literally "scarring of the skin and fat“ A slow process that occurs over a number
of years and has 2 phases:1. Acute
Venous pooling →chronic venous hypertension
RBC forced into surrounding tissue Haemoglobin broken down into brown
haemosiderin2. Chronic
Chronic haemosiderin formation leads to fibrin deposition
Skin becomes thickened and shiny Skin around ankle constricts and the
inverted champagne-bottle shape is seen

Temperature Feel with back of hand,
should be warm If cold, arterial disease
may co-exist Palpate the vein
Feel the course of the vein
Cough impulse Locate the
saphenofemoral junction (SFJ)
Feel for the smooth swelling and palpable thrill of a saphena varix (cause of groin lump)
If present, cough test +ve
Tap Test Place finger at any point along the
varicose vein Tap the vein proximally (above the
finger) Incompetent valves allow the
transmission of a fluid thrill to the finger below
Direction Test Empty a short section of the vein (place
one finger on the vein and slide another finger firmly upwards).
If the valves are incompetent, the vein will refill when you release the top finger.
Auscultation• Over a large group of veins may indicate
a bruit• Rare – indicates an underlying
arteriovenous malformation

1. The Trendelenburg test Used to assess the competence of SFJ Patient lies flat Elevate the leg and gently empty the veins Palpate the SFJ and ask the patient to stand whilst
maintaining pressure
Findings: If the veins do not refill→ SFJ is incompetent If the veins do refill →SFJ may or may not be
incompetent, presence of distal incompetent perforators

2. Tourniquet test Uses a tourniquet to control the junction rather than
fingers Advantage of moving the tourniquet lower (mid-
thigh region) Test is unreliable below the knee
3. Perthes Test Empty the vein as above, place a tourniquet around
the thigh, stand the patient up. Ask them to rapidly stand up and down on their toes
– filling of the veins indicated deep venous incompetence. This is a painful and rarely used test.

Use a Doppler ultrasound
Examine the abdomen for masses (+ DRE) to ascertain whether the varicose veins are primary or secondary
Complete a peripheral vascular exam for arterial supply of the lower limb, including ABPI

Conservative/Medical Graded compression
bandaging, Compression hosiery
Paste Gauze (Unna) Boots Diuretics? Zinc?
Phlebotrophic/Hemorheologic agents? Aspirin/NSAIDs etc
Robert B. Rutherford (editor). Vascular surgery 6th ed. 2005. Elsevier Saunders. ISBN 0-7216-0299-1 (set)
J. A. Michaels, J. E. Brazier, W. B. Campbell, J. B.MacIntyre, S. J. Palfreyman and J. Ratcliffe. Randomized clinical trial comparing surgery with conservative treatment for uncomplicated varicose veins. British Journal of Surgery 2006; 93: 175–181
Surgical Ankle-to-groin saphenous vein
stripping (with stab avulsion) Segmental saphenous vein
stripping (with stab avulsion) Saphenous vein ligation: high,
low, or both Saphenous vein ligation and
sclerotherapy Saphenous vein ligation (with
stab avulsion) Stab avulsion of varices without
saphenous vein stripping (phlebectomy)
Endoluminal occlusion of the saphenous vein by radiofrequency (RF) or laser energy


Images: Mr Neeraj Bhasin

Day case procedureOral paracetamol as analgesiaElastic bandaging for 2-3 daysMobilization: Walking for 2-3 miles
daily (ideally for 5 minutes every hour)
Compression stockings?
J.P. Houtermans-Auckel a, E. van Rossum b, J.A.W. Teijink c, A.A.H.R. Dahlmans a, E.F.B. Eussen a, S.P.A. Nicolaı¨a, R.J.Th.J. Welten. To Wear or not to Wear Compression Stockings after Varicose Vein Stripping: A Randomised Controlled Trial. Eur J Vasc Endovasc Surg (2009) 38, 387-391

Major complications following VV surgery are relatively rare
Up to 20% morbidity Infection Hematoma Pain Nerve damage
▪ Saphenous nerve (LSV surgery)▪ Sural, peroneal nerve (SSV surgery)
Lymphatic leak - Venous thrombosis - Vascular injury
Recurrence
W. B. Campbell, F. France & H.M. Goodwin, Medicolegal claims in vascular surgery. Annals of the Royal College of Surgeons of England, 84 (2002), 181–4.
W.G. Tennant, Medicolegal action following treatment for varicose veins. British Journal of Surgery, 8 (1996), 291–2.

Any Questions?