Embed Size (px)
Citation preview

UvA-DARE is a service provided by the library of the University of Amsterdam (http://dare.uva.nl)
UvA-DARE (Digital Academic Repository)
Fecal volatile organic compound analysis and intestinal microbiota profiling in healthy anddiseased infants
Berkhout, D.J.C.
Link to publication
Creative Commons License (see https://creativecommons.org/use-remix/cc-licenses):Other
Citation for published version (APA):Berkhout, D. J. C. (2019). Fecal volatile organic compound analysis and intestinal microbiota profiling in healthyand diseased infants.
General rightsIt is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s),other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons).
Disclaimer/Complaints regulationsIf you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, statingyour reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Askthe Library: https://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam,The Netherlands. You will be contacted as soon as possible.
Download date: 29 Aug 2020

Late-onset sepsis in preterm infants can be detected preclinically by fecal volatile organic compound analysis: a prospective, multicenter cohort study
Chapter 6
Daniel BerkhoutBritt van Keulen
Hendrik J. NiemarktJet R Bessem
Willem P. de BoodeVeerle Cossey
Neil HoogenesChristiaan V. Hulzebos
Ellen KlaverPeter Andriessen
Anton H. van KaamBoris W. Kramer
Richard A. van LingenAaron Schouten
Johannes B. van GoudoeverDaniel C. Vijlbrief
Mirjam M. van WeissenbruchAlfian N. WicaksonoJames A. Covington
Marc A. BenningaNanne K.H. de Boer
Tim G.J. de Meij
Clin Infect Dis. 2018 Jun 21. [Epub ahead of print]

Chapter 6
132
ABSTRACT
Introduction: The intestinal microbiota has increasingly been considered to play a role in the etiology of late-onset sepsis (LOS). We hypothesize that early alterations in fecal volatile organic compounds (VOCs), reflecting intestinal microbiota composition and function, allow for discrimination between infants developing LOS and controls in a preclinical stage.
Methods: In nine neonatal intensive care units in the Netherlands and Belgium, fecal samples of preterm infants born at a gestational age ≤30 weeks were collected daily, up to the postnatal age of 28 days. Fecal VOC were measured by High-Field Asymmetric Waveform Ion Mobility Spectrometry (FAIMS). VOC profiles of LOS infants, up to three days prior to clinical LOS onset, were compared with profiles from matched controls.
Results: In total, 843 preterm born infants (gestational age ≤30 weeks) were included. From 127 LOS cases and 127 matched controls, fecal samples were analyzed by means of FAIMS. Fecal VOCs allowed for preclinical discrimination between LOS and control infants. Focusing on individual pathogens, fecal VOCs differed significantly between LOS cases and controls at all predefined time points. Highest accuracy rates were obtained for sepsis caused by Escherichia
coli, followed by sepsis caused by Staphylococcus aureus and Staphylococcus epidermidis.
Conclusions: Fecal VOC analysis allowed for preclinical discrimination between infants developing LOS and matched controls. Early detection of LOS may provide clinicians a window of opportunity for timely initiation of individualized therapeutic strategies aimed at prevention of sepsis, possibly improving LOS-related morbidity and mortality.

6
LOS detection by fecal VOC analysis II
133
INTRODUCTION
Despite a decrease in the incidence of late-onset sepsis (LOS) over the past decade, still 34% of all extremely low birth weight and preterm infants, born at a gestational age <29 weeks, experience at least one episode of LOS1. Unfortunately, this decline in incidence is not accompanied with a decrease in either LOS associated mortality (12%) or length of hospital stay1.
Although extensively studied, the exact biological mechanisms of LOS are still poorly understood. Next to indwelling devices, the intestinal microbiota has increasingly been considered to play a pivotal role in LOS etiology. Bacterial dysbiosis, combined with an immature intestinal epithelial barrier and naïve immune system, may increase the risk of transmucosal bacterial translocation, ultimately leading to ‘gut-derived sepsis’. Several microbiota studies have demonstrated microbial alterations preceding the clinical onset of LOS, as compared to controls2-9. However, a key feature of these studies is the lack of a consistent LOS-specific microbial signature. Furthermore, implementation of intestinal microbiota analysis in daily clinical practice as an early diagnostic biomarker for LOS is not feasible because of high costs and the complexity to generate and interpret microbiota results in a clinically acceptable fashion.
Fecal volatile organic compound (VOC) analysis may serve as alternative test to monitor changes in microbiota and its metabolic activity. VOCs are carbon-based volatiles, which are considered to reflect microbial composition and function, as they provide insight into the interaction between gut microbiota and host10,11. Fecal VOCs have previously been described to hold potential as noninvasive diagnostic biomarker of diseases that are associated with alterations in intestinal microbiota composition12,13. Recently, in a small proof of principle study, we have shown that fecal VOCs allow for differentiation between preterm infants with and without LOS, up to three days prior to clinical onset of LOS14. Since all bacterial species exhibit a unique, metabolic signature10 and provoke species-specific host-pathogen interactions, fecal VOCs may hypothetically allow for identification of LOS-provoking pathogens at species level. Primary aim of this study was to investigate whether fecal VOC analysis could discriminate preterm infants developing LOS from controls before the onset of symptoms of LOS, in a large multi-center cohort. The secondary aim was to evaluate whether the discriminative accuracy would increase when focusing on specific causative LOS pathogens.
METHODS
Subjects
Between October 2014 and January 2017, infants born at a gestational age ≤30 weeks were consecutively included in this prospective cohort study performed at nine neonatal

Chapter 6
134
intensive care units (NICUs) located in the Netherlands and Belgium. Exclusion criteria were congenital intestinal anomalies, NEC (Bells stage ≥IIA) or spontaneous intestinal perforation (SIP) during the period of stool collection (the first 28 postnatal days), gastro-intestinal surgery within this period, missing or incomplete medical file. During the study period, none of the participating NICUs administered probiotics routinely. Data on delivery mode, center of birth, gestational age, birth weight, sex, Apgar scores, preterm premature rupture of membranes (PPROM) (≥24 hours before delivery), presence of peripheral and central catheters, enteral and parenteral feeding practices, red blood cell transfusions, administered medication (including antibiotics), treatment of a hemodynamically significant persistent ductus arteriosus (PDA), and diagnosis of NEC or sepsis, including causative agent (defined as the pathogen isolated from blood culture), were prospectively collected from all included infants during the period of stool collection. The study was approved by all local Institutional Review Boards (protocol A2016.363) and written parental informed consent was obtained from all included patients.
Patient cohort and sample selection
Included preterm infants were identified as LOS cases if all three Vermont Oxford criteria for LOS were met: 1) presence of clinical signs of generalized infection; 2) isolation of a bacterial pathogen from blood-culture obtained ≥72 hours after birth; 3) and initiation of adequate antibiotic therapy with the intention to treat for a minimal of 5 days15. In case a coagulase-negative Staphylococcus (CoNS) bacteria was isolated from blood culture, infants were allocated to the LOS group only if C-reactive protein (CRP) level was at least once ≥10 mg/L within one week after clinical onset of LOS, in order to minimize the risk of including infants with contaminated blood cultures16. Fecal samples obtained at three (t
-3), two (t
-2) and one (t
-1)
day(s) prior to clinical LOS onset were used for further VOC analysis.
Each LOS case was strictly matched to one non-LOS control based on the following criteria: center of birth, gestational age, postnatal age, birth weight, days exposed to antibiotics prior to t
0 and enteral feeding type (breastmilk versus formula feeding). Preterm infants not meeting
the criteria for LOS and without a significant clinical infection, defined as CRP < 10 mg/L within three days adjacent to t
0 and a maximum CRP <50 mg/L during the entire period of stool
collection, were eligible to participate as control.
VOC comparisons
Fecal VOC profiles from cases and controls were compared at each pre-defined time point in days (t
-3, t
-2 and t
-1) and, as extremely preterm infants may not pass stool daily, in an analysis
including the last obtained sample prior to t0. Multiple VOC profile comparisons were
performed at these measurement points:

6
LOS detection by fecal VOC analysis II
135
In the first analysis, the most frequently cultured species of Gram-positive (except CoNS) (Staphylococcus aureus), Gram-negative (Escherichia coli) and CoNS (Staphylococcus epidermidis) were identified. Fecal samples from cases and controls were compared at the predefined time points and in an analysis including only the last sample obtained prior to LOS onset. In case both CoNS and a non-CoNS species were obtained from one single blood culture, the LOS case was allocated to the non-CoNS group15. Cultures containing two different CoNS species or multiple non-CoNS species in one single blood culture were excluded from further VOC analysis.
For the second analysis, pathogens were allocated to either the Gram-positive (except CoNS), Gram-negative or CoNS group, comparing VOC profiles from the last obtained sample prior to t
0 with their corresponding matched control sample. Here, if both Gram-positive
and Gram-negative bacteria were obtained from the blood culture, cases were included in both Gram-negative and Gram-positive analysis. Cultures containing CoNS and non-CoNS pathogens were excluded from the CoNS analysis, since CoNS is often considered to be a contaminant in these cases15.
The third analysis included VOC profiles from all LOS pathogens combined and were compared with their matched controls to assess whether the overall VOC signal in LOS differed from controls. Both cross-sectional analysis per time interval (t
-3, t
-2 and t
-1) and an
analysis including only the VOC profile of the last fecal sample produced prior to LOS onset was performed.
Fourth, to assess the potential influence of center of birth on fecal VOC outcome, we performed three further analyses. Each analysis included only those VOC profiles of the last fecal sample obtained prior to LOS from infants born at one of the three centers who included the highest rates of LOS cases (center 1, 2 and 3). Since blood cultures containing more than one different pathogen are often considered to be contaminated, an additional analysis was performed including only cases with monocultures and compared them with their matched controls.
VOC analysis by FAIMS technique
Fecal samples were analyzed using the FAIMS technique (Lonestar®, Owlstone, Cambridge, England)13,17. In this particular study, a commercially available FAIMS apparatus was used (Lonestar®, Owlstone, Cambridge, England). In this device, the VOCs present in a gaseous mixture are first ionized using a NI-63 radiation source before subsequently being transported using a carrier gas (compressed air 0.1 MPa) at a rate a flowrate of 2L/min. While entering an asymmetric electrical field waveform these ionized fecal molecules pass two metal plates. The applied voltage (Dispersion Field (DF)) varies during the measurement and has a proportionate effect on the mobility of ionized molecules. Since this electric field is modulated between a

Chapter 6
136
short high electrical voltage alternated by moments of long low electrical voltage, ions drift in a ‘zigzag-like’ pattern through the metal plates towards the sensor. In the current study, the DF varied between 0% and 100% in 51 different steps. Since ions lose their electrical charge if they come in contact with a metal plate, a compensation voltage (CV) ranging between -6V and +6V is applied over these plates in 512 steps per DF, preventing ions to be left undetected by the sensor. Concluding, a complex gaseous mixture consisting of a wide variety of different ionized molecules can be separated by (ion-specific) differences in mobility by stepwise altering the strengths of both the DF and the CV. Ultimately, a 3D map of the mobility of all the molecules within a sample is generated, consisting of 52,224 different data points13,17.
All samples were analyzed in random order using www.random.org. Per sample, 0.1 gram fecal material was thawed to room temperature (20°C) and subsequently mixed with 3 mL tap water before being placed in a clean glass jar. The following temperatures were used during the analysis; 35°C, 70°C and 100 °C for the bottle holder (where the sample sits), the lid and the filter region respectively. The latter two ensure that molecules to no adhere to any of the VOC transfer lines). Cleaned and compressed air (0.1MPa) was used as carrier gas to transport fecal VOCs into the Lonestar® with a flow rate of 2.4 L/min. All samples were run three times in sequence, producing three three-dimensional matrixes, each matrix taking 180 seconds to complete. Since the second produced matrix is considered to be the most stable and least influenced by environmental factors17,18, this matrix was used in the analysis. After each fecal sample measurement, the Lonestar® was cleaned by running three matrixes deriving from the headspace of 3 mL tap water.
Statistical analysis
Demographic and clinical variables were compared using a chi-square, independent t-test or nonparametric test where appropriate. A p-value of <.05 was considered statistically significant. For the VOC-profile analyses, after reduction of the raw data using 2D discrete wavelet transform (a common form of data compression), a Wilcoxon rank-sum test was used to calculate p-values18. Subsequently, four classification algorithms, Random Forest, Sparse Logistic Regression, Support Vector Machine, and Gaussian Process Classifier, were used to produce class prediction inside a 10-fold cross validation with 90% of the data as a training set and the remaining 10% as a test set19. Random Forest is a classification method operating by constructing a multitude of decision trees based on random selection of data and variables. Randomly combining hundreds of individual decision trees (random forest) in this training phase eventually leads to an ensemble that contains higher precision, performs more stable predictions and is robust against overfitting20. Support Vector Machine is a supervised learning model performing classification by segregating two classes using a hyperplane. A robust classification model is created by constructing a higher dimensional space. By increasing the margin between the hyperplane and extreme cases, the risk of misclassification is decreased21.

6
LOS detection by fecal VOC analysis II
137
The third performed classification model is Gaussian Process Classifier, a nonparametric classification method based on Bayesian methodology22. Sparse Logistic Regression classifier is a version of logistic regression that imposes feature sparsity. By excluding non-informative features from the analysis, a small subset of features with the most discriminative power remain included, ultimately improving the quality of the analysis23.ROC curves with corresponding area under the curves (AUCs), sensitivity, specificity, positive predictive value and negative predictive value were produced for each model, selecting the most significant model for notation.
RESULTS
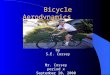
A total of 843 preterm infants were enrolled in this study, of whom 127 both met the criteria for LOS and had sufficient fecal material available for VOC analysis (Figure 1). Patient characteristics and cultured pathogens from the infants excluded based on unavailability of fecal material were similar to the characteristics and pathogens of the current study. In the present study, the sepsis and control groups did not differ with respect to demographic and clinical variables (Table 1).
† These cases depicted similar patient characteristics as the current population.
Assessed for eligibility (n=843)
Excluded (n=81) Missing or incomplete medical file (n=14) Necrotizing enterocolitis (n=56) Spontaneous intestinal perforation (n=11)
Control infants included in the study (n=127)
Infants meeting the criteria for control (n=571)
LOS infants included in the study (n=127)
Infants meeting the criteria for LOS (n=191)
Presence of LOS criteria verified (n=752)
Excluded (n=64) Insufficient material available due to
previous analyses † (n=60) Lack of fecal material at predefined
time points (n=4)
Excluded (n=444) Not matched to a
case (n=444)
Figure 1. Flow-chart of participants of the study

Chapter 6
138
Table 1. Subject characteristics of cases and controls
Sepsis(n=127)
Controls(n=127) p-value
Gestational age (median [IQR]),
weeks + days [days]
26 + 6 [19] 27 + 0 [14] .384
Birth weight (median [IQR]), g 920 [365] 964 [280] .280
Sex
Male (n=[%]) 66 [52.0] 70 [55.1] .615
Delivery mode Vaginal delivery (n=[%]) 67 [52.8] 62 [48.8] .530
Multiple births (n=[%]) 57 [44.9] 48 [37.8] .251
Postnatal age at t0 (median [IQR]), days 9 [7] n.a. n.a.
Antibiotic exposure prior t0 (n=[%])
Antibiotic days (median [IQR])
118 [92.9]
4 [3]
119 [93.7]
4 [3]
.802
.911
Enteral feeding type prior t0 † (n=[%])
Breast milk fed
Formula fed
Combination
53 [45.7]
31 [26.7]
32 [27.6]
57 [49.1]
30 [25.9]
29 [25.0]
.857
Mortality (n=[%])
Age of death (median [IQR]), days
8 [6.3]
15.5 [7.8]
2 [1.6]
9.5
.053
.711Abbreviations: CI = Confidence Interval; IQR = interquartile range; n.a.= not applicable. † variables were not retrievable from the medical records in one participating center (n=22).
Table 2. Isolated pathogens (n=[%]) from blood cultures in 127 sepsis patients
(n=) [%]
Monomicrobial cultures 113 [89]
CoNSStaphylococcus epidermidis
Staphylococcus capitis
Staphylococcus haemolyticus
Staphylococcus warneri
Staphylococcus hominis
Coagulase negative Staphylococcus
42
17
4
2
1
1
[33.1]
[13.4]
[3.1]
[1.6]
[0.8]
[0.8]
Gram positive pathogens†
Staphylococcus aureus
Bacillus cereus
Enterococcus faecalis
Group B Streptococcus
Group C Streptococcus
19
2
1
1
1
[15.0]
[1.6]
[0.8]
[0.8]
[0.8]

6
LOS detection by fecal VOC analysis II
139
Gram negative pathogensEscherichia coli
Enterobacter cloacae
Serratia marcescens
Enterobacter aerogenes
Klebsiella pneumoniae
Serratia liquefaciens
11
4
3
1
1
1
[8.7]
[3.1]
[2.4]
[0.8]
[0.8]
[0.8]
Fungal pathogensCandida Albicans 1 [0.8]
Cultures with ≥2 different pathogens 14 [11.0]
Gram negative pathogens + Gram positive pathogens† + CoNSKlebsiella ornithinolytica + Enterococcus faecalis + Staphylococcus epidermidis 1 [0.8]
Gram negative pathogens + Gram positive pathogens†
Klebsiella pneumoniae + Staphylococcus aureus 1 [0.8]
Gram negative pathogens + CoNSEscherichia coli + Staphylococcus epidermidis
Enterobacter cloacae + Staphylococcus epidermidis
3
1
[2.4]
[0.8]
Gram positive pathogens† + CoNSStaphylococcus aureus + Staphylococcus epidermidis 2 [1.6]
CoNS + CoNSStaphylococcus capitis + Staphylococcus epidermidis
Staphylococcus epidermidis + Staphylococcus haemolyticus
Staphylococcus capitis + Staphylococcus haemolyticus + Staphylococcus warneri
3
2
1
[2.4]
[1.6]
[0.8]
†Not including coagulase negative Staphylococcus. Abbreviations: CoNS = Coagulase negative Staphylococcus
Variation in initial empirical antibiotic treatment between centers is depicted in Supplemental Table 1. In 14/127 (11%) cases, more than one different pathogen was isolated from the blood culture. Focusing on monocultures, Staphylococcus epidermidis was the most frequently isolated pathogen (n=42), followed by Staphylococcus capitis (n=17), Staphylococcus aureus (n=19) and Escherichia coli (n=11) (Table 2).
Fecal volatile organic compound analysis
An overview of the fecal VOC outcomes is depicted in Table 3, Supplemental Table 2 and Supplemental Figure 1. The median date of birth with corresponding interquartile range [IQR] was 5-May-2016 [427 days] for cases and 17-May-2016 [311 days] for controls and could be considered as a reflection of the median sample storage time per study group. Summarized, we observed that fecal VOC profiles of infants with LOS caused by Staphylococcus aureus and Escherichia coli, differed significantly from matched controls infants at all three predefined time points. Corresponding area under the curves (AUCs) in the analysis including only

Chapter 6
140
Staphylococcus aureus were .85;.70;.80, and in the analysis including Escherichia coli .88;.99;.86 at t
-3, t
-2 and t
-1 respectively. Pooling the samples obtained most adjacent to t
0 from all Gram-
negative (AUC =.77) or Gram-positive pathogens allowed for discrimination between cases and controls. In the subgroup analysis including VOC profiles of all CoNS together, and the analysis focusing on the last obtained sample prior onset from the most frequently cultured species within this CoNS subgroup (Staphylococcus epidermidis), fecal VOCs did not allow for discrimination between LOS cases and controls. In contrast, separating these samples based on the time points they were obtained, fecal VOCs allowed for discrimination between cases and controls with corresponding AUC of .90;.78;.63 at t
-3, t
-2 and t
-1 respectively.
If all LOS infants were included, irrespective of the cultured pathogen, fecal VOC analysis only allowed for a statistically significant discrimination at t
-1. If only the last produced
fecal sample prior t0 was included in the analysis, fecal VOC analysis remained statistically
significantly different.
Three additional analyses were performed including infants born at one of the three centers, which included the largest number of LOS cases (n=39, n=25, n=16 respectively). Fecal VOCs allowed for statistically significant discrimination in center 1 (AUC[±95% confidence interval (CI)],p-value, sensitivity, specificity;.76[.63-.90],.0005,.76,.72) and center 2 (.86[.71-1],.0001,.88,.88), but not in center three (.62[.50-.75],.9693,.74,.59). At least one CoNS was isolated in 33 of 39 (85%) sepsis cases born in center 3, whereas CoNS was identified in 13/25 (52%) cases and 11/16 (69%) cases in respectively center 1 and center 2.
DISCUSSION
In this prospective multicenter cohort study, we investigated the diagnostic potential of fecal VOCs in the preclinical detection of LOS. In general, VOC profiles of 127 infants with LOS could be discriminated from controls before the clinical diagnosis was established. Specifically, LOS caused by Escherichia coli, Staphylococcus aureus and Staphylococcus epidermidis could be differentiated from their matched controls with high predictive value, up to three days before the clinical onset of LOS.
Previously, we have demonstrated that fecal VOCs allowed for differentiation between infants developing LOS and matched controls with AUCs of 70.2, 77.7 and 70.4 at respectively three, two and one day prior to LOS onset, but not earlier14. However, that study was limited by a wide variety of pathogens and a small sample size (n=36 cases). In addition, VOC analyses in that study were performed by a Cyranose320® eNose (Cyranose320®, Sensigent, US) harboring 32 unique conducting sensors, whereas the currently applied FAIMS technique allows for over 52.000 individual data points18, 24, based on the mobility of ionized molecules in an electrical field.

6
LOS detection by fecal VOC analysis II
141
Tabl
e 3.
Per
form
ance
cha
ract
eris
tics f
or th
e di
scrim
inat
ion
of la
te-o
nset
sep
sis a
nd m
atch
ed c
ontr
ols u
sing
feca
l VO
Cs.
Cor
resp
ondi
ng a
rea
unde
r the
cur
ves,
sens
itivi
ty, s
pec
ifici
ty, p
ositi
ve a
nd n
egat
ive
pred
ictiv
e va
lues
are
dis
play
ed.
Ana
lysi
s
Seps
is
sam
ples
† (n
=)p
-val
ueA
UC
(±
95%
CI)
Sens
itiv
ity
(±
95%
CI)
Spec
ifici
ty
(± 9
5% C
I)PP
VN
PVA
pplie
d m
etho
d
Esch
eric
hia
coli‡
14.0
002
0.87
(0.7
4 - 1
)0.
93 (0
.66
- 1)
0.71
(0.4
2 - 0
.92)
0.76
0.91
Gau
ssia
n Pr
oces
s
Esch
eric
hia
coli
t-113
.000
60.
86 (0
.71-
1)0.
92 (0
.64-
1)0.
77 (0
.46-
0.95
)0.
80.
91Su
ppor
t Vec
tor M
achi
ne
Esch
eric
hia
coli
t-29
<.0
001
0.99
(0.9
5-1.
0)1
(0.6
6-1)
0.89
(0.5
2-1.
0)0.
91
Gau
ssia
n Pr
oces
s
Esch
eric
hia
coli
t-311
.001
30.
88 (0
.72-
1)0.
91 (0
.59-
1.0)
0.82
(0.4
8-0.
98)
0.83
0.9
Rand
om F
ores
t
S. a
ureu
s‡21
.019
10.
69 (0
.52-
0.85
)0.
76 (0
.53-
0.92
)0.
62 (0
.38-
0.82
)0.
670.
72G
auss
ian
Proc
ess
S. a
ureu
s t-1
15.0
016
0.8
(0.6
4 - 0
.96)
0.73
(0.4
5 - 0
.92)
0.8
(0.5
2 - 0
.96)
0.79
0.75
Supp
ort V
ecto
r Mac
hine
S. a
ureu
s t-2
13.0
406
0.7
(0.5
- 0.
91)
0.85
(0.5
5 - 0
.98)
0.62
(0.3
2 - 0
.86)
0.69
0.8
Rand
om F
ores
t
S. a
ureu
s t-3
16.0
002
0.85
(0.7
- 1)
0.88
(0.6
2 - 0
.98)
0.81
(0.5
4 - 0
.96)
0.82
0.87
Gau
ssia
n Pr
oces
s
S. e
pide
rmid
is‡
42.9
823
0.63
(0.5
1 - 0
.75)
0.74
(0.5
8 - 0
.86)
0.55
(0.3
9 - 0
.7)
0.62
0.68
Supp
ort V
ecto
r Mac
hine
S. e
pide
rmid
is t-1
35.0
308
0.63
(0.5
-0.7
6)0.
54 (0
.37-
0.71
)0.
71 (0
.54-
0.85
)0.
660.
61G
auss
ian
Proc
ess
S. e
pide
rmid
is t-2
22.0
006
0.78
(0.6
4-0.
92)
0.82
(0.6
0-0.
95)
0.68
(0.4
5-0.
86)
0.72
0.79
Spar
se L
ogis
tic R
egre
ssio
n
S. e
pide
rmid
is t-3
19<
.000
10.
90 (0
.79-
1.0)
0.84
(0.6
-0.9
7)0.
89 (0
.67-
0.99
)0.
890.
85Ra
ndom
For
est
Gra
m-n
egat
ive
bac
teria
‡27
.003
00.
77 (0
.63
- 0.9
)0.
78 (0
.58
- 0.9
1)0.
81 (0
.62
- 0.9
4)0.
810.
79Su
ppor
t Vec
tor M
achi
ne
Gra
m-p
ositi
ve b
acte
ria‡
28.0
007
0.74
(0.6
1 - 0
.88)
0.75
(0.5
5 - 0
.89)
0.75
(0.5
5 - 0
.89)
.75
.75
Spar
se L
ogis
tic R
egre
ssio
n
CoN
S‡73
.107
70.
56 (0
.47
- 0.6
5)0.
56 (0
.44
- 0.6
8)0.
6 (0
.48
- 0.7
2)0.
590.
58Ra
ndom
For
est
t -1 to
t -3‡
127
.043
70.
56 (0
.49
- 0.6
3)0.
69 (0
.6 -
0.76
)0.
44 (0
.35
- 0.5
3)0.
550.
58Ra
ndom
For
est
t -110
5.0
249
0.58
(0.5
- 0.
66)
0.61
(0.5
1 - 0
.7)
0.55
(0.4
5 - 0
.65)
0.58
0.59
Rand
om F
ores
t
t -278
.989
80.
61 (0
.52
- 0.7
)0.
91 (0
.82
- 0.9
6)0.
29 (0
.2 -
0.41
)0.
560.
77G
auss
ian
Proc
ess
t -378
.979
10.
59 (0
.51
- 0.6
8)0.
55 (0
.43
- 0.6
6)0.
62 (0
.5 -
0.72
)0.
590.
58Ra
ndom
For
est
Mon
o-cu
lture
s‡11
3.0
079
0.59
(0.5
2 - 0
.67)
0.81
(0.7
2 - 0
.87)
0.4
(0.3
1 - 0
.49)
0.57
0.67
Rand
om F
ores
t
† co
rres
pon
ding
num
ber
of f
ecal
sam
ples
from
con
trol
s w
ere
anal
yzed
, ‡ for t
his
anal
ysis
onl
y th
e la
st fe
cal s
ampl
e pr
oduc
ed p
rior t
o la
te-o
nset
sep
sis
was
use
dA
bbre
viat
ions
: AU
C ±
95%
CI,
area
und
er t
he c
urve
with
95%
con
fiden
ce in
terv
al; C
oNS
= c
oagu
lase
neg
ativ
e St
aphy
loco
ccus
; NPV
= n
egat
ive
pred
ictiv
e va
lue;
PPV
=
pos
itive
pre
dict
ive
valu
e; S
= S
taph
yloc
occu
s; VO
Cs=
Vol
atile
org
anic
com
pou
nds

Chapter 6
142
In the present study, including a larger number of LOS cases, discriminative accuracies improved compared to the results obtained in the previous study, in case of Escherichia coli (n=14) and Staphylococcus aureus (n=21) LOS. This suggests the presence of a unique, species-specific fecal VOC profile in LOS. It has been demonstrated, mainly in in-vitro studies, that individual bacterial species are characterized by production of a unique VOC fingerprint10,25. We therefore hypothesized that changes in the composition of the microbiota prior to LOS onset may have largely contributed to the detected alterations in fecal VOC profiles. To date, the intestinal microbiota has increasingly been recognized as an important factor in LOS etiology in preterm infants. Interestingly, an increased abundance of the LOS causing pathogen preceding onset, including Escherichia coli2,7,8 and Staphylococcus aureus5,7, has been demonstrated in several studies.
By pooling both gram-negative pathogens (n=27) and gram-positive pathogens (n=28), discriminative accuracy slightly decreased compared to the analysis involving unique species. This finding may be explained by the observation that gram-positive and gram-negative pathogens depict specific metabolic processes, allowing for discrimination between both subgroups by VOC analysis26.
As expected, including fecal samples obtained most adjacent to t0
from all included LOS infants (n=127) in the analysis, discriminative accuracy decreased even further. This may be explained by the wide variety of different LOS pathogens in this study, each pathogen exhibiting a distinct VOC profile. Presumably, the presence of discriminative VOCs in septic infants resulting from production of local and systemic inflammatory biomarkers allowed for the discrimination between LOS and control infants. Another possible explanation is that absence of VOCs originating from commensals characterizing healthy state in controls, including anaerobic bacteria of the genus Bifidobacterium4,7, allowed for the discrimination in this specific analysis.
In the current study, focusing on the last sample obtained prior to disease onset, fecal VOCs did not allow for discrimination between sepsis caused by either Staphylococcus epidermidis (n=42) or CoNS (n=73) in general, and strictly matched controls. Since CoNS species are considered predominant components of both dermal27 and intestinal microbiome28, we hypothesize that, in at least a part of the cases, not intestinal mucosal translocation but skin invasive procedures may have been the source of CoNS bacteremia. Consequently, bacterial dysbiosis in the intestines preceding a LOS episode may not have occurred, hampering discrimination between cases and controls based on fecal VOCs in this particular group. This hypothesis is underlined by a recent study, demonstrating the gastrointestinal tract to be dominated by the LOS causing pathogen prior to onset, except for Staphylococcus epidermis7. Interestingly, separating these samples based on the time points they were obtained, fecal VOCs allowed for discrimination between cases with Staphylococcus epidermidis sepsis and

6
LOS detection by fecal VOC analysis II
143
controls at each individual time-point. It has previously been described that the center of birth has a significant influence on fecal VOC profiles, possibly resulting from center-specific protocols on feeding patterns and choice of antibiotics29. This finding was confirmed in the present study, since focusing on VOC profiles of infants from the same center of birth resulted in an increased discriminative accuracy between LOS and controls, the only exception being center 3. We hypothesized that this apparent discrepancy resulted from the presence of CoNS in the vast majority of the sepsis cases (85%) in that particular center, whereas CoNS species were less frequently isolated from blood culture in the remaining two centers. As described previously, detection of CoNS by fecal VOC analysis seems to be less feasible than other pathogens, possibly by a different site of entry.
In the current study, observations are highly dependent on the selected statistical analytical supervised method. Since the performance of various prediction models have been shown to vary considerably, it has been questioned whether a certain classifier model may have universal applicability in different populations19. Further studies are needed to assess which model provides optimal accuracy in different research and clinical settings.
Strengths of the current study are the large number of included cases in this multicenter, prospective designed study with daily collection of samples and detailed collection on clinical variables, allowing for applying a matching procedure of cases and controls. This study also has several limitations. Firstly, differences in storage time existed between the first collected samples and the samples collected at the end of the study period. This difference in storage time may have caused degradation of volatiles and consequently has influenced VOC outcome. However, we believe that these potential effects on presented results are limited, since this accounted for both cases and controls30. Secondly, microbiota analyses were not performed in the current study. Consequently, study design did not provide prove for our hypothesis that the LOS causing pathogens is abundantly present in the intestines preceding clinical onset. Third, based on our previous study14, we have only analyzed fecal samples obtained within three days prior to LOS onset. Possibly, VOC differences are present already more than three days prior to LOS onset, providing a larger window of opportunity to prevent LOS. Fourth, although the eNose instrument allows for bedside and relative inexpensive VOC analysis of complex gaseous mixtures, they do not allow for the identification of individual VOCs. Identification of individual, LOS-specific volatiles by means of chemical analytical techniques could allow for development of a tailor-made eNose instrument, with increased accuracy compared to the non-primed eNose in the present study. Since the currently applied eNose focuses on the entire spectrum of VOCs and is not specifically designed to detect LOS in a preclinical phase, we hypothesize that including more subjects in the analysis would result in an increase in the number of confounding VOCs, deriving from non-relevant and non-avoidable environmental and host-specific sources. Potentially, this may have caused the decrease in discriminative accuracy in the analysis comparing the last obtained fecal samples

Chapter 6
144
prior to t0 from infants with a Staphylococcus aureus sepsis, compared to the analysis including
the t -1 samples. Future studies should focus on identification of discriminative and species-
specific VOCs by means of chemical analytical techniques. This may allow for development of LOS-specific eNose sensors to be applied as a diagnostic tool for preclinical detection of LOS in clinical practice, simultaneously providing information about the causative agent. Daily analysis of fecal samples obtained from the diaper would ultimately allow for the early detection and consequently timely intervention of LOS in preterm infants, eventually resulting in a decrease in LOS-related morbidity and mortality. Hypothetically, these sensors could also be incorporated in an incubator, continuously analyzing the VOCs deriving from the infants. In conclusion, we demonstrated that fecal VOC analysis allowed for the preclinical discrimination between infants developing LOS and matched controls, up to three days prior to LOS onset. In particular, the highly pathogenic Escherichia coli and Staphylococcus aureus were detectable pre-clinically with high accuracy. Preclinical detection of LOS may provide clinicians a window of opportunity for timely initiation of individualized therapeutic strategies, for example narrow spectrum antibiotics, aimed at prevention of sepsis and might ultimately decrease overall morbidity and mortality in preterm born infants.

6
LOS detection by fecal VOC analysis II
145
REFERENCES
1. Greenberg RG, Kandefer S, Do BT, Smith PB, Stoll BJ, Bell EF, et al. Late-onset Sepsis in Extremely Premature Infants: 2000-2011. Pediatr Infect Dis J. 2017;36(8):774-9.
2. Carl MA, Ndao IM, Springman AC, Manning SD, Johnson JR, Johnston BD, et al. Sepsis from the gut: the enteric habitat of bacteria that cause late-onset neonatal bloodstream infections. Clin Infect Dis. 2014;58(9):1211-8.
3. Madan JC, Salari RC, Saxena D, Davidson L, O’Toole GA, Moore JH, et al. Gut microbial colonisation in premature neonates predicts neonatal sepsis. Arch Dis Child Fetal Neonatal Ed. 2012;97(6):F456-62.
4. Mai V, Torrazza RM, Ukhanova M, Wang X, Sun Y, Li N, et al. Distortions in development of intestinal microbiota associated with late onset sepsis in preterm infants. PLoS One. 2013;8(1):e52876.
5. Shaw AG, Sim K, Randell P, Cox MJ, McClure ZE, Li MS, et al. Late-Onset Bloodstream Infection and Perturbed Maturation of the Gastrointestinal Microbiota in Premature Infants. PLoS One. 2015;10(7):e0132923.
6. Soeorg H, Huik K, Parm U, Ilmoja ML, Metelskaja N, Metsvaht T, et al. Genetic relatedness of coagulase-negative Staphylococci from gastrointestinal tract and blood of preterm neonates with late-onset sepsis. Pediatr Infect Dis J. 2013;32(4):389-93.
7. Stewart CJ, Embleton ND, Marrs ECL, Smith DP, Fofanova T, Nelson A, et al. Longitudinal development of the gut microbiome and metabolome in preterm neonates with late onset sepsis and healthy controls. Microbiome. 2017;5(1):75.
8. Taft DH, Ambalavanan N, Schibler KR, Yu Z, Newburg DS, Deshmukh H, et al. Center Variation in Intestinal Microbiota Prior to Late-Onset Sepsis in Preterm Infants. PLoS One. 2015;10(6):e0130604.
9. Tarr PI, Warner BB. Gut bacteria and late-onset neonatal bloodstream infections in preterm infants. Semin Fetal Neonatal Med. 2016;21(6):388-93.
10. Bos LD, Sterk PJ, Schultz MJ. Volatile metabolites of pathogens: a systematic review. PLoS Pathog. 2013;9(5):e1003311.
11. Raman M, Ahmed I, Gillevet PM, Probert CS, Ratcliffe NM, Smith S, et al. Fecal microbiome and volatile organic compound metabolome in obese humans with nonalcoholic fatty liver disease. Clin Gastroenterol Hepatol. 2013;11(7):868-75 e1-3.
12. de Meij TG, van der Schee MP, Berkhout DJ, van de Velde ME, Jansen AE, Kramer BW, et al. Early Detection of Necrotizing Enterocolitis by Fecal Volatile Organic Compounds Analysis. J Pediatr. 2015;167(3):562-7 e1.
13. van Gaal N, Lakenman R, Covington J, Savage R, de Groot E, Bomers M, et al. Fecal volatile organic compounds analysis using field asymmetric ion mobility spectrometry: non-invasive diagnostics in pediatric inflammatory bowel disease. J Breath Res. 2017.
14. Berkhout DJ, Niemarkt HJ, Buijck M, van Weissenbruch MM, Brinkman P, Benninga MA, et al. Detection of Sepsis in Preterm Infants by Fecal Volatile Organic Compounds Analysis: A Proof of Principle Study. J Pediatr Gastroenterol Nutr. 2016.
15. Manual of Operations: Part 2 Data Definitions & Infant Data Forms [Internet]. Vermont Oxford Network. 2016 [cited 12-10-2016].
16. Hofer N, Zacharias E, Muller W, Resch B. An update on the use of C-reactive protein in early-onset neonatal sepsis: current insights and new tasks. Neonatology. 2012;102(1):25-36.

Chapter 6
146
17. Bomers MK, Menke FP, Savage RS, Vandenbroucke-Grauls CM, van Agtmael MA, Covington JA, et al. Rapid, accurate, and on-site detection of C. difficile in stool samples. Am J Gastroenterol. 2015;110(4):588-94.
18. Covington JA, van der Schee MP, Edge AS, Boyle B, Savage RS, Arasaradnam RP. The application of FAIMS gas analysis in medical diagnostics. Analyst. 2015;140(20):6775-81.
19. Ai L, Tian H, Chen Z, Chen H, Xu J, Fang JY. Systematic evaluation of supervised classifiers for fecal microbiota-based prediction of colorectal cancer. Oncotarget. 2017;8(6):9546-56.
20. Liaw A, Wiener M. Classification and regression by randomForest. R news. 2002;2(3):18-22.
21. Adankon MM, Cheriet M. Support vector machine. Encyclopedia of biometrics: Springer; 2009. p. 1303-8.
22. Rasmussen CE. Gaussian processes in machine learning. Advanced lectures on machine learning: Springer; 2004. p. 63-71.
23. Arasaradnam RP, Westenbrink E, McFarlane MJ, Harbord R, Chambers S, O’Connell N, et al. Differentiating coeliac disease from irritable bowel syndrome by urinary volatile organic compound analysis--a pilot study. PLoS One. 2014;9(10):e107312.
24. Arasaradnam RP, Ouaret N, Thomas MG, Gold P, Quraishi MN, Nwokolo CU, et al. Evaluation of gut bacterial populations using an electronic e-nose and field asymmetric ion mobility spectrometry: further insights into ‘fermentonomics’. J Med Eng Technol. 2012;36(7):333-7.
25. Palma S, Traguedo AP, Porteira AR, Frias MJ, Gamboa H, Roque ACA. Machine learning for the meta-analyses of microbial pathogens’ volatile signatures. Sci Rep. 2018;8(1):3360.
26. Dolch ME, Janitza S, Boulesteix AL, Grassmann-Lichtenauer C, Praun S, Denzer W, et al. Gram-negative and -positive bacteria differentiation in blood culture samples by headspace volatile compound analysis. J Biol Res (Thessalon). 2016;23:3.
27. Bialkowska-Hobrzanska H, Jaskot D, Hammerberg O. Molecular characterization of the coagulase-negative staphylococcal surface flora of premature neonates. J Gen Microbiol. 1993;139(12):2939-44.
28. Jacquot A, Neveu D, Aujoulat F, Mercier G, Marchandin H, Jumas-Bilak E, et al. Dynamics and clinical evolution of bacterial gut microflora in extremely premature patients. J Pediatr. 2011;158(3):390-6.
29. Berkhout DJ, Benninga MA, van Stein RM, Brinkman P, Niemarkt HJ, de Boer NK, et al. Effects of Sampling Conditions and Environmental Factors on Fecal Volatile Organic Compound Analysis by an Electronic Nose Device. Sensors (Basel). 2016;16(11).
30. Forbes SL, Rust L, Trebilcock K, Perrault KA, McGrath LT. Effect of age and storage conditions on the volatile organic compound profile of blood. Forensic Sci Med Pathol. 2014;10(4):570-82.

6
LOS detection by fecal VOC analysis II
147

Chapter 6
148

6
LOS detection by fecal VOC analysis II
149

Chapter 6
150

6
LOS detection by fecal VOC analysis II
151

Chapter 6
152
Supplemental Figures 1 a-w. Best available receiver operating curve of fecal volatile organic compound analysis for the discrimination of late-onset sepsis and matched controls per analysis
‡ for these analyses only the last fecal sample produced prior to late-onset sepsis were used
Abbreviations: AUC ± 95% CI, area under the curve with 95% confidence interval, CoNS = coagulase negative Staphylococcus

6
LOS detection by fecal VOC analysis II
153
Supplemental Table 1. Initial empirical antibiotic treatment variation between centers
Hospital Initial empirical antibiotic treatment
Emma children’s hospital Benzyl penicillin
Gentamicin
Vrije universiteit medical center Benzyl penicillin
Amikacin
Máxima medical center Amoxicillin
Gentamicin
Amalia children’s hospital Zwolle Amoxicillin
Ceftazidime
University hospitals Leuven Amoxicillin
Amikacin
Beatrix children’s hospital Amoxicillin Gentamicin
Maastricht university medical center Amoxicillin
Gentamicin
Amalia children’s center Nijmegen Amoxicillin
Gentamicin
Wilhelmina children’s hospital Amoxicillin clavulanate acid
Gentamicin

Chapter 6
154
Supplemental Table 2. Different classification algorithms with corresponding area under the curve, sensitivity, specificity, positive and negative predictive value of fecal volatile organic compound analysis for the discrimination of late-onset sepsis and matched controls
Classification algorithm p-value AUC (± 95% CI)
Escherichia coli‡
Sparse Logistic Regression .0685 0.66 (0.45 - 0.87)
Random Forest .0065 0.77 (0.58 - 0.97)
Gaussian Process .0002 0.87 (0.74 - 1)
Support Vector Machine .0015 0.82 (0.64 - 0.99)
Escherichia coli t-1
Sparse Logistic Regression .0082 0.78 (0.58 - 0.97)
Random Forest .0363 0.71 (0.51 - 0.91)
Gaussian Process .0284 0.72 (0.52 - 0.92)
Support Vector Machine .0006 0.86 (0.71 - 1)
Escherichia coli t-2
Sparse Logistic Regression .0028 0.86 (0.7 - 1)
Random Forest .0094 0.81 (0.6 - 1)
Gaussian Process <.0001 0.99 (0.95 - 1)
Support Vector Machine .0028 0.86 (0.68 - 1)
Escherichia coli t-3
Sparse Logistic Regression .3032 0.56 (0.31 - 0.82)
Random Forest .0013 0.88 (0.72 - 1)
Gaussian Process .0016 0.85 (0.67 - 1)
Support Vector Machine .0326 0.73 (0.51 - 0.95)
Staphylococcus aureus‡
Sparse Logistic Regression .3005 0.55 (0.37 - 0.73)
Random Forest .6471 0.47 (0.29 - 0.65)
Gaussian Process .0191 0.69 (0.52 - 0.85)
Support Vector Machine .7652 0.56 (0.39 - 0.74)
Staphylococcus aureus t-1
Sparse Logistic Regression .0064 0.76 (0.59 - 0.93)
Random Forest .0045 0.78 (0.6 - 0.96)
Gaussian Process .0147 0.73 (0.54 - 0.92)
Support Vector Machine .0016 0.8 (0.64 - 0.96)
Staphylococcus aureus t-2
Sparse Logistic Regression .0844 0.66 (0.44 - 0.88)
Random Forest .0406 0.7 (0.5 - 0.91)
Gaussian Process .0627 0.68 (0.46 - 0.9)
Support Vector Machine .0565 0.69 (0.47 - 0.91)
Staphylococcus aureus t-3
Sparse Logistic Regression .0010 0.88 (0.76 - 1)
Random Forest .0014 0.81 (0.65 - 0.96)
Gaussian Process .0002 0.85 (0.7 - 1)
Support Vector Machine .005 0.83 (0.67 - 0.98)
Staphylococcus epidermidis‡
Sparse Logistic Regression .9911 0.65 (0.53 - 0.77)
Random Forest .9945 0.66 (0.54 - 0.78)
Gaussian Process .9999 0.73 (0.62 - 0.84)
Support Vector Machine .9823 0.63 (0.51 - 0.75)
Staphylococcus epidermidis t-1
Sparse Logistic Regression .5695 0.51 (0.37 - 0.65)
Random Forest .6200 0.48 (0.34 - 0.62)
Gaussian Process .0308 0.63 (0.5 - 0.76)
Support Vector Machine .8538 0.57 (0.44 - 0.71)

6
LOS detection by fecal VOC analysis II
155
Sensitivity (± 95% CI) Specificity (± 95% CI) PPV NPV
1 (0.77 - 1) 0.36 (0.13 - 0.65) .61 1
0.93 (0.66 - 1) 0.57 (0.29 - 0.82) .68 .89
0.93 (0.66 - 1) 0.71 (0.42 - 0.92) .76 .91
0.93 (0.66 - 1) 0.79 (0.49 - 0.95) .81 .92
0.77 (0.46 - 0.95) 0.77 (0.46 - 0.95) .77 .77
0.54 (0.25 - 0.81) 0.85 (0.55 - 0.98) .78 .65
1 (0.75 - 1) 0.38 (0.14 - 0.68) .62 1
0.92 (0.64 - 1) 0.77 (0.46 - 0.95) .80 .91
1 (0.66 - 1) 0.56 (0.21 - 0.86) .59 1
0.67 (0.3 - 0.93) 1 (0.66 - 1) 1 .75
1 (0.66 - 1) 0.89 (0.52 - 1) .90 1
0.78 (0.4 - 0.97) 0.89 (0.52 - 1) .88 .80
0.82 (0.48 - 0.98) 0.36 (0.11 - 0.69) .56 .67
0.91 (0.59 - 1) 0.82 (0.48 - 0.98) .83 .90
0.91 (0.59 - 1) 0.82 (0.48 - 0.98) .83 .90
0.82 (0.48 - 0.98) 0.64 (0.31 - 0.89) .69 .78
1 (0.84 - 1) 0.19 (0.054 - 0.42) .55 1
0.62 (0.38 - 0.82) 0.48 (0.26 - 0.7) .54 .56
0.76 (0.53 - 0.92) 0.62 (0.38 - 0.82) .67 .72
0.52 (0.3 - 0.74) 0.71 (0.48 - 0.89) .65 .60
0.93 (0.68 - 1) 0.53 (0.27 - 0.79) .67 .89
0.67 (0.38 - 0.88) 0.93 (0.68 - 1) .91 .74
0.87 (0.6 - 0.98) 0.67 (0.38 - 0.88) .72 .83
0.73 (0.45 - 0.92) 0.8 (0.52 - 0.96) .79 .75
0.92 (0.64 - 1) 0.46 (0.19 - 0.75) .63 .86
0.85 (0.55 - 0.98) 0.62 (0.32 - 0.86) .69 .80
0.92 (0.64 - 1) 0.54 (0.25 - 0.81) .67 .88
0.92 (0.64 - 1) 0.54 (0.25 - 0.81) .67 .88
0.75 (0.48 - 0.93) 0.94 (0.7 - 1) .92 .79
0.75 (0.48 - 0.93) 0.81 (0.54 - 0.96) .80 .76
0.88 (0.62 - 0.98) 0.81 (0.54 - 0.96) .82 .87
0.88 (0.62 - 0.98) 0.81 (0.54 - 0.96) .82 .87
0.71 (0.55 - 0.84) 0.6 (0.43 - 0.74) .64 .68
0.86 (0.71 - 0.95) 0.45 (0.3 - 0.61) .61 .76
0.88 (0.74 - 0.96) 0.52 (0.36 - 0.68) .65 .81
0.74 (0.58 - 0.86) 0.55 (0.39 - 0.7) .62 .68
0.77 (0.6 - 0.9) 0.34 (0.19 - 0.52) .54 .60
0.97 (0.85 - 1) 0.11 (0.032 - 0.27) .52 .80
0.54 (0.37 - 0.71) 0.71 (0.54 - 0.85) .66 .61
0.74 (0.57 - 0.88) 0.43 (0.26 - 0.61) .57 .62

Chapter 6
156
Staphylococcus epidermidis t-2
Sparse Logistic Regression .0006 0.78 (0.64 - 0.92)
Random Forest .0271 0.67 (0.51 - 0.83)
Gaussian Process .2924 0.55 (0.37 - 0.73)
Support Vector Machine .2462 0.44 (0.26 - 0.61)
Staphylococcus epidermidis t -3
Sparse Logistic Regression .0099 0.72 (0.55 - 0.89)
Random Forest <.0001 0.9 (0.79 - 1)
Gaussian Process <.0001 0.89 (0.78 - 0.99)
Support Vector Machine .0005 0.8 (0.65 - 0.95)
Gram-negative bacteria‡
Sparse Logistic Regression .0040 0.76 (0.63 - 0.9)
Random Forest .0040 0.76 (0.63 - 0.9)
Gaussian Process .0211 0.66 (0.51 - 0.81)
Support Vector Machine .0030 0.77 (0.63 - 0.9)
Gram-positive bacteria‡
Sparse Logistic Regression .0007 0.74 (0.61 - 0.88)
Random Forest .0097 0.68 (0.54 - 0.82)
Gaussian Process .0021 0.72 (0.59 - 0.86)
Support Vector Machine .0023 0.72 (0.58 - 0.85)
CoNS‡
Sparse Logistic Regression .2381 0.53 (0.44 - 0.63)
Random Forest .1077 0.56 (0.47 - 0.65)
Gaussian Process .2986 0.53 (0.43 - 0.62)
Support Vector Machine .3786 0.49 (0.39 - 0.58)
t-1 to t
-3‡
Sparse Logistic Regression .3825 0.51 (0.44 - 0.58)
Random Forest .0437 0.56 (0.49 - 0.63)
Gaussian Process .8304 0.53 (0.46 - 0.61)
Support Vector Machine .3334 0.52 (0.44 - 0.59)
t-1
Sparse Logistic Regression .2323 0.53 (0.45 - 0.61)
Random Forest .0249 0.58 (0.5 - 0.66)
Gaussian Process .8028 0.53 (0.46 - 0.61)
Support Vector Machine .1583 0.54 (0..46 - 0.62)
t-2
Sparse Logistic Regression .9942 0.62 (0.53 - 0.71)
Random Forest .9978 0.63 (0.54 - 0.72)
Gaussian Process .9898 0.61 (0.52 - 0.7)
Support Vector Machine .9934 0.61 (0.53 - 0.7)
t-3
Sparse Logistic Regression .9961 0.62 (0.54 - 0.71)
Random Forest .9791 0.59 (0.51 - 0.68)
Gaussian Process .9968 0.63 (0.54 - 0.71)
Support Vector Machine .9903 0.61 (0.52 - 0.7)
Mono-cultures‡
Sparse Logistic Regression .6113 0.51 (0.43 - 0.59)
Random Forest .0079 0.59 (0.52 - 0.67)
Gaussian Process .3127 0.48 (0.41 - 0.56)
Support Vector Machine .6168 0.49 (0.41 - 0.56)
Classification algorithm p-value AUC (± 95% CI)
Supplemental Table 2. (continued)

6
LOS detection by fecal VOC analysis II
157
0.82 (0.6 - 0.95) 0.68 (0.45 - 0.86) .72 .79
0.82 (0.6 - 0.95) 0.5 (0.28 - 0.72) .62 .73
0.59 (0.36 - 0.79) 0.59 (0.36 - 0.79) .59 .59
1 (0.85 - 1) 0.045 (0.0012 - 0.23) .51 1
0.53 (0.29 - 0.76) 1 (0.82 - 1) 1 .68
0.84 (0.6 - 0.97) 0.89 (0.67 - 0.99) .89 .85
0.89 (0.67 - 0.99) 0.79 (0.54 - 0.94) .81 .88
0.74 (0.49 - 0.91) 0.79 (0.54 - 0.94) .78 .75
0.78 (0.58 - 0.91) 0.78 (0.58 - 0.91) .78 .78
0.7 (0.5 - 0.86) 0.85 (0.66 - 0.96) .83 .74
0.93 (0.76 - 0.99) 0.44 (0.25 - 0.65) .62 .86
0.78 (0.58 - 0.91) 0.81 (0.62 - 0.94) .81 .79
0.75 (0.55 - 0.89) 0.75 (0.55 - 0.89) .75 .75
0.68 (0.48 - 0.84) 0.64 (0.44 - 0.81) .66 .67
0.68 (0.48 - 0.84) 0.75 (0.55 - 0.89) .73 .70
0.39 (0.22 - 0.59) 0.96 (0.82 - 1) .92 .61
0.9 (0.81 - 0.96) 0.25 (0.15 - 0.36) .55 .72
0.56 (0.44 - 0.68) 0.6 (0.48 - 0.72) .59 .58
0.96 (0.88 - 0.99) 0.14 (0.068 - 0.24) .53 .77
0.58 (0.45 - 0.69) 0.49 (0.37 - 0.61) .53 .54
0.76 (0.68 - 0.83) 0.33 (0.25 - 0.42) .53 .58
0.69 (0.6 - 0.76) 0.44 (0.35 - 0.53) .55 .58
0.6 (0.51 - 0.68) 0.49 (0.4 - 0.58) .54 .55
0.68 (0.59 - 0.76) 0.45 (0.36 - 0.54) .55 .58
0.75 (0.66 - 0.83) 0.37 (0.28 - 0.47) .54 .60
0.61 (0.51 - 0.7) 0.55 (0.45 - 0.65) .58 .59
0.58 (0.48 - 0.68) 0.58 (0.48 - 0.68) .56 .56
0.65 (0.55 - 0.74) 0.48 (0.38 - 0.58) .55 .57
0.72 (0.6 - 0.81) 0.54 (0.42 - 0.65) .61 .66
0.73 (0.62 - 0.82) 0.53 (0.41 - 0.64) .61 .66
0.91 (0.82 - 0.96) 0.29 (0.2 - 0.41) .56 .77
0.86 (0.76 - 0.93) 0.38 (0.28 - 0.5) .58 .73
0.67 (0.55 - 0.77) 0.55 (0.43 - 0.66) .60 .62
0.55 (0.43 - 0.66) 0.62 (0.5 - 0.72) .59 .58
0.72 (0.6 - 0.81) 0.5 (0.38 - 0.62) .59 .64
0.44 (0.32 - 0.55) 0.79 (0.69 - 0.88) .68 .58
0.67 (0.58 - 0.76) 0.43 (0.34 - 0.53) .54 .57
0.81 (0.72 - 0.87) 0.4 (0.31 - 0.49) .57 .67
0.53 (0.43 - 0.63) 0.52 (0.43 - 0.62) .53 .53
0.59 (0.5 - 0.68) 0.47 (0.37 - 0.57) .53 .54
Sensitivity (± 95% CI) Specificity (± 95% CI) PPV NPV

Chapter 6
158
Center 1‡
Sparse Logistic Regression .0339 0.65 (0.49 - 0.81)
Random Forest .0547 0.63 (0.47 - 0.79)
Gaussian Process .0005 0.76 (0.63 - 0.9)
Support Vector Machine .0247 0.66 (0.51 - 0.82)
Center 2‡
Sparse Logistic Regression .0026 0.78 (0.61 - 0.95)
Random Forest .0001 0.86 (0.71 - 1)
Gaussian Process .0213 0.71 (0.52 - 0.89)
Support Vector Machine .0006 0.82 (0.67 - 0.97)
Center 3‡
Sparse Logistic Regression .9985 0.69 (0.57 - 0.81)
Random Forest .9983 0.69 (0.57 - 0.81)
Gaussian Process .9693 0.62 (0.5 - 0.75)
Support Vector Machine .9960 0.67 (0.55 - 0.79)
† corresponding number of fecal samples from controls were analyzed, ‡ for this analysis only the last fecal sample produced prior to late-onset sepsis were usedAbbreviations: AUC ± 95% CI, area under the curve with 95% confidence interval; CoNS = coagulase negative Staphylococcus; NPV = negative predictive value; PPV = positive predictive value; S = Staphylococcus
Classification algorithm p-value AUC (± 95% CI)
Supplemental Table 2. (continued)

6
LOS detection by fecal VOC analysis II
159
0.64 (0.43 - 0.82) 0.76 (0.55 - 0.91) .73 .68
0.88 (0.69 - 0.97) 0.44 (0.24 - 0.65) .61 .79
0.76 (0.55 - 0.91) 0.72 (0.51 - 0.88) .73 .75
0.68 (0.46 - 0.85) 0.72 (0.51 - 0.88) .71 .69
0.69 (0.41 - 0.89) 0.88 (0.62 - 0.98) .85 .74
0.88 (0.62 - 0.98) 0.88 (0.62 - 0.98) .88 .88
0.94 (0.7 - 1) 0.44 (0.2 - 0.7) .62 .88
0.81 (0.54 - 0.96) 0.75 (0.48 - 0.93) .76 .80
0.56 (0.4 - 0.72) 0.79 (0.64 - 0.91) .73 .65
0.54 (0.37 - 0.7) 0.82 (0.66 - 0.92) .75 .64
0.74 (0.58 - 0.87) 0.59 (0.42 - 0.74) .64 .70
0.56 (0.4 - 0.72) 0.77 (0.61 - 0.89) .71 .64
Sensitivity (± 95% CI) Specificity (± 95% CI) PPV NPV

















![LEARNING TO LISTEN [OUR PHILOSOPHY]phd… · A presentation for the NCMEA Professional Development Conference Saturday, November 5th, 2:00 pm Alyssa Cossey & Becky Marsh, presenters](https://img.pdfslide.us/doc/110x75/5fb1c88505da1141cf25834a/learning-to-listen-our-philosophy-phd-a-presentation-for-the-ncmea-professional.jpg)