-
Utero-placental Doppler ultrasound for improving pregnancy
outcome (Review)
Stampalija T, Gyte GML, Alfirevic Z
This is a reprint of a Cochrane review, prepared and maintained
by The Cochrane Collaboration and published in The Cochrane
Library2010, Issue 9
http://www.thecochranelibrary.com
Utero-placental Doppler ultrasound for improving pregnancy
outcome (Review)
Copyright 2010 The Cochrane Collaboration. Published by John
Wiley & Sons, Ltd.
-
T A B L E O F C O N T E N T S
1HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . .
1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . .
2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . .
2BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . .
4OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . .
4METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . .
7RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . .
Figure 1. . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . 8
10DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . .
11AUTHORS CONCLUSIONS . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . .
11ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . .
11REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . .
16CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . .
. . . . . . . . . . .
25DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . .
Analysis 2.1. Comparison 2 Uterine artery Doppler ultrasound
versus no Doppler ultrasound, 2nd trimester, Outcome 1
Any perinatal death after randomisation. . . . . . . . . . . . .
. . . . . . . . . . . . 33
Analysis 2.2. Comparison 2 Uterine artery Doppler ultrasound
versus no Doppler ultrasound, 2nd trimester, Outcome 2
Hypertensive disorders. . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . 34
Analysis 2.3. Comparison 2 Uterine artery Doppler ultrasound
versus no Doppler ultrasound, 2nd trimester, Outcome 3
Stillbirth. . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . 35
Analysis 2.4. Comparison 2 Uterine artery Doppler ultrasound
versus no Doppler ultrasound, 2nd trimester, Outcome 4
Neonatal death. . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . 36
Analysis 2.5. Comparison 2 Uterine artery Doppler ultrasound
versus no Doppler ultrasound, 2nd trimester, Outcome 5
Any potentially preventable perinatal death after randomisation.
. . . . . . . . . . . . . . . . 37
Analysis 2.7. Comparison 2 Uterine artery Doppler ultrasound
versus no Doppler ultrasound, 2nd trimester, Outcome 7
Intrauterine growth restriction. . . . . . . . . . . . . . . . .
. . . . . . . . . . . . 38
Analysis 2.9. Comparison 2 Uterine artery Doppler ultrasound
versus no Doppler ultrasound, 2nd trimester, Outcome 9
Neonatal resuscitation. . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . 39
Analysis 2.12. Comparison 2 Uterine artery Doppler ultrasound
versus no Doppler ultrasound, 2nd trimester, Outcome 12
Apgar score < 7 at 5 min. . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . 40
Analysis 2.13. Comparison 2 Uterine artery Doppler ultrasound
versus no Doppler ultrasound, 2nd trimester, Outcome 13
Neonatal admission to SCBU or NICU. . . . . . . . . . . . . . .
. . . . . . . . . . 41
Analysis 2.15. Comparison 2 Uterine artery Doppler ultrasound
versus no Doppler ultrasound, 2nd trimester, Outcome 15
Iatrogenic preterm birth (< 37 weeks). . . . . . . . . . . .
. . . . . . . . . . . . . . 42
Analysis 2.16. Comparison 2 Uterine artery Doppler ultrasound
versus no Doppler ultrasound, 2nd trimester, Outcome 16
Caesarean section (both elective and emergency). . . . . . . . .
. . . . . . . . . . . . . 43
Analysis 2.17. Comparison 2 Uterine artery Doppler ultrasound
versus no Doppler ultrasound, 2nd trimester, Outcome 17
Elective caesarean section. . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . 44
Analysis 2.18. Comparison 2 Uterine artery Doppler ultrasound
versus no Doppler ultrasound, 2nd trimester, Outcome 18
Emergency caesarean section. . . . . . . . . . . . . . . . . . .
. . . . . . . . . . 45
Analysis 2.21. Comparison 2 Uterine artery Doppler ultrasound
versus no Doppler ultrasound, 2nd trimester, Outcome 21
Gestational age at birth. . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . 46
Analysis 2.22. Comparison 2 Uterine artery Doppler ultrasound
versus no Doppler ultrasound, 2nd trimester, Outcome 22
Infant birthweight. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . 47
47HISTORY . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . .
47CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . .
. . . . . . . . . .
48DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . .
48SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . .
48DIFFERENCES BETWEEN PROTOCOL AND REVIEW . . . . . . . . . . .
. . . . . . . . . .
48INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . .
iUtero-placental Doppler ultrasound for improving pregnancy
outcome (Review)
Copyright 2010 The Cochrane Collaboration. Published by John
Wiley & Sons, Ltd.
-
[Intervention Review]
Utero-placental Doppler ultrasound for improving
pregnancyoutcome
Tamara Stampalija1, Gillian ML Gyte2, Zarko Alfirevic3
1Department of Obstetrics and Gynaecology, Childrens Hospital V.
Buzzi, Milano, Italy. 2Cochrane Pregnancy and Childbirth
Group, School of Reproductive and Developmental Medicine,
Division of Perinatal and Reproductive Medicine, The University
of
Liverpool, Liverpool, UK. 3School of Reproductive and
Developmental Medicine, Division of Perinatal and Reproductive
Medicine,
The University of Liverpool, Liverpool, UK
Contact address: Tamara Stampalija, Department of Obstetrics and
Gynaecology, Childrens Hospital V. Buzzi, Via Castelvetro 32,
Milano, 20154, Italy. [email protected].
Editorial group: Cochrane Pregnancy and Childbirth Group.
Publication status and date: New, published in Issue 9,
2010.
Review content assessed as up-to-date: 15 July 2010.
Citation: Stampalija T, Gyte GML, Alfirevic Z. Utero-placental
Doppler ultrasound for improving pregnancy outcome.
CochraneDatabase of Systematic Reviews 2010, Issue 9. Art. No.:
CD008363. DOI: 10.1002/14651858.CD008363.pub2.
Copyright 2010 The Cochrane Collaboration. Published by John
Wiley & Sons, Ltd.
A B S T R A C T
Background
Impaired placentation can cause some of the most important
obstetrical complications such as pre-eclampsia and intrauterine
growth
restriction and has been linked to increased fetal morbidity and
mortality. The failure to undergo physiological trophoblastic
vascular
changes is reflected by the high impedance to the blood flow at
the level of the uterine arteries. Doppler ultrasound study of
utero-
placental blood vessels, using waveform indices or notching, may
help to identify the at-risk women in the first and second
trimester
of pregnancy, such that interventions might be used to reduce
maternal and fetal morbidity and/or mortality.
Objectives
To assess the effects on pregnancy outcome, and obstetric
practice, of routine utero-placental Doppler ultrasound in first
and second
trimester of pregnancy in pregnant women at high and low risk of
hypertensive complications.
Search methods
We searched the Cochrane Pregnancy and Childbirth Groups Trials
Register (June 2010) and the reference lists of identified
studies.
Selection criteria
Randomised and quasi-randomised controlled trials of Doppler
ultrasound for the investigation of utero-placental vessel
waveforms in
first and second trimester compared with no Doppler ultrasound.
We have excluded studies where uterine vessels have been
assessed
together with fetal and umbilical vessels.
Data collection and analysis
Two authors independently assessed the studies for inclusion,
assessed risk of bias and carried out data extraction. We checked
data
entry.
1Utero-placental Doppler ultrasound for improving pregnancy
outcome (Review)
Copyright 2010 The Cochrane Collaboration. Published by John
Wiley & Sons, Ltd.
-
Main results
We found two studies involving 4993 participants. The
methodological quality of the trials was good. Both studies
included women
at low risk for hypertensive disorders, with Doppler ultrasound
of the uterine arteries performed in the second trimester of
pregnancy.
In both studies, pathological finding of uterine arteries was
followed by low-dose aspirin administration.
We identified no difference in short-term maternal and fetal
clinical outcomes.
We identified no randomised studies assessing the
utero-placental vessels in the first trimester or in women at high
risk for hypertensive
disorders.
Authors conclusions
Present evidence failed to show any benefit to either the baby
or the mother when utero-placental Doppler ultrasound was used
in
the second trimester of pregnancy in women at low risk for
hypertensive disorders. Nevertheless, this evidence cannot be
considered
conclusive with only two studies included. There were no
randomised studies in the first trimester, or in women at high
risk. More
research is needed to investigate whether the use of
utero-placental Doppler ultrasound may improve pregnancy
outcome.
P L A I N L A N G U A G E S U M M A R Y
Doppler ultrasound of blood vessels in the placenta and uterus
of pregnant women as a way of improving outcome for babies
and their mothers
One of the main aims of routine antenatal care is to identify
mothers or babies at risk of adverse outcomes. Doppler
ultrasound
uses sound waves to detect the movement of blood in blood
vessels. It is used in pregnancy to study blood circulation in the
baby,
the mothers uterus and the placenta. If abnormal blood
circulation is identified, then it is possible that medical
interventions might
improve outcomes. We set out to assess the value of using
Doppler ultrasound of the mothers uterus or placenta
(utero-placental
Doppler ultrasound) as a screening tool. Other reviews have
looked at the use of Doppler ultrasound on the babies vessels
(fetal and
umbilical Doppler ultrasound). We also choose to look at women
with low-risk and high-risk pregnancies, and in their first or
second
trimesters. This screening offers a potential for benefit, but
also a possibility of unnecessary interventions and adverse
effects. The
review of randomised controlled trials of routine Doppler
ultrasound of the uterus or placenta identified two studies
involving 4993
women. All the women were in the second trimester of pregnancy
and at low risk for hypertensive disorders. The studies were of
good
quality but small in size. We identified no improvements for the
baby or the mother. However, more data would be needed to show
whether maternal Doppler is effective, or not, for improving
outcomes. We did not find any studies in the first trimester of
pregnancy
or in women at risk of high blood pressure disorders. More
research is needed on this important aspect of care.
B A C K G R O U N D
Description of the condition
The blood supply to the uterus is provided mainly by the
uterine
arteries and also by the ovarian arteries. Once the arterial
vessels
reach myometrium, they divide into arcuate arteries, then
into
the radial arteries which ultimately branch into the spiral
arteries.
During the first and second trimester of pregnancy,
trophoblast
invades the spiral arteries - a process that is fundamental for
normal
placentation. The most important change, but not the only
one,
is replacement of the muscular and elastic arterial layer by
collagen
(Espinoza 2006). As the trophoblastic invasion continues
during
the first half of pregnancy, the resistance to the blood flow in
the
uterine arteries progressively decreases.
The failure to undergo these physiologic vascular changes
has
been associated not just with pre-eclampsia (Brosens 1972;
Khong
1991; Sibai 2005; Von Dadelszen 2002) and intrauterine
growth
restriction (IUGR) (Bernstein 2000; Fisk 2001; Khong 1991),
but
also with other maternal diseases such as diabetes mellitus
(Khong
1991), lupus erythematosus (Nayar 1996), antiphospholipid
an-
tibody syndrome (Levy 1998) and others (Barker 2004).
2Utero-placental Doppler ultrasound for improving pregnancy
outcome (Review)
Copyright 2010 The Cochrane Collaboration. Published by John
Wiley & Sons, Ltd.
-
Description of the intervention
Doppler ultrasound velocimetry uses the Doppler principle to
analyse the properties of the blood flow in a vessel of
interest. This
physical principle explains the observed change in wave
frequency
relative to the speed of a moving object. In case of Doppler
ul-
trasound, the emitted ultrasound frequency will change when
ul-
trasound beam encounters moving blood. The principle can be
applied using different ultrasound modalities such as
continuous-
wave Doppler, pulsed-wave Doppler, colour and power Doppler
wave (Burns 1993; Chen 1996; Owen 2001). While colour and
power Doppler provide visualisation of the blood flow and its
di-
rection, pulsed Doppler allows reproducible measurements of
the
blood velocities. The measurements obtained will reflect, in
any
vessel studied, the cardiac contraction force, density of the
blood,
vessel wall elasticity, but more importantly peripheral and
down-
stream resistance (Owen 2001).
Physiological process of the trophoblastic invasion of spiral
arter-
ies takes place between six and 24 weeks of gestation in
normal
pregnancies. The blood flow from the uterine arteries to the
pla-
centa will progressively increase during that time. By studying
the
uterine arteries with pulse Doppler ultrasound, it is possible
to as-
sess the progressive decrease in resistance to blood flow. The
ratio-
nale of using the Doppler velocimetry of uterine arteries to
assess
the failure of the placentation is related to fact that the lack
of
physiological transformation of the spiral arteries will cause
high
resistance to blood flow within uterus and subsequently in
uterine
arteries.
At least 15 different uterine artery Doppler indices have been
used
to quantify the uterine arteries perfusion and predict
pre-eclamp-
sia and IUGR (Cnossen 2008). The most commonly used indices
are the pulsatility and resistant index (PI and RI) which
showed
the highest predictive value (Cnossen 2008). The qualitative
de-
scription focuses on the presence or absence of early diastolic
notch
that could be either unilateral or bilateral.
The abnormal findings in uterine arteries are usually defined as
PI
or RI above the 95 percentile at a given gestational age
(Albaiges
2000; Bower 1993) and the presence of notching (a qualitative
as-
sessment of flow velocity waveform - Harrington 1996).
Numer-
ous studies have linked the high impedance and bilateral
notching
in uterine arteries to early onset pre-eclampsia, IUGR and
higher
perinatal mortality (Aardema 2001; Albaiges 2000; Bower
1993;
Harrington 1996; Olofsson 1993).
Reported sensitivity and detection rate of the uterine
artery
Doppler to predict pre-eclampsia in unselected population
range
from 50% to 60%, meaning that only half of the women that
subsequently develop the disease will be correctly identified by
the
increased resistance in uterine arteries. On the other hand the
re-
ported specificity is around 95%, which means that most
women
with normal uterine artery Doppler will not develop
pre-eclamp-
sia. The performance of uterine artery Doppler as a screening
test
is higher when pre-eclampsia is divided in severe or early onset
and
mild or late onset pre-eclampsia. In that case, the sensitivity
rises
from 80% to 85% for severe pre-eclampsia, requiring delivery
be-
fore 34 weeks (Papageorghiou 2001; Yu 2005) and 90% for
severe
pre-eclampsia indicating delivery before 32 weeks
(Papageorghiou
2001).
More recently, the interest for uterine artery measurements
has
moved from the second to the first trimester of pregnancy
(13+6
to 11+0 weeks of gestation). The rationale of measuring the
uter-
ine artery Doppler in the first trimester is the possibility to
in-
tervene with some prophylactic therapy such as
antithrombotic
drugs while the trophoblastic invasion is still ongoing. The
uterine
arteryDoppler has been found tobe less predictivewhen
compared
with the second trimester examination. Reported detection
rate
for uterine artery Doppler alone in the first trimester ranged
from
40% to 67% for early onset pre-eclampsia and 15% to 20% for
late
onset pre-eclampsia (Martin 2001; Parra 2005). In the attempt
to
improve the performance of the uterine artery as a screening
test,
new algorithms that take into account thematernal
characteristics,
history and/or biochemical markers have been proposed. In
fact,
uterine artery Doppler in the first and second trimester, in
com-
bination with several biochemical markers, has been
extensively
tested as a predictive test for pre-eclampsia and IUGR, and the
first
results are encouraging (Nicolaides 2006; Parra 2005;
Plasencia
2007; Spencer 2007; Zhong 2010). Nevertheless, at present
the
literature comprises several large uncontrolled cohort studies
and
as yet there are no randomised studies in this field, and the
cost-
effectiveness remains to be proven.
How the intervention might work
It is hoped that early detection of abnormal placental
vascula-
ture, before maternal and fetal complications develop, would
al-
low preventative interventions and more targeted maternal
and
fetal surveillance. Low-dose aspirin is an example of a
preventative
intervention that could be targeted to those with abnormal
utero-
placental Doppler (Askie 2007).
Why it is important to do this review
Doppler ultrasound has become an integral part of obstetric
care
(Alfirevic 2010a) and more clinicians are being trained to use
it.
Using a non-invasive and relatively easy screening tool such
as
Doppler ultrasound of the uterine arteries to predict
pre-eclamp-
sia and IUGR is undoubtedly appealing. Early recognition of
pre-
eclampsia and IUGR could improve maternal and perinatal out-
come by administration antiplatelet therapy, appropriate
antihy-
pertensive therapy, medication for fetal lung maturation and
early
delivery. Nevertheless, labelling woman as at risk could cause
sig-
nificant anxiety and increase the number of unnecessary
examina-
tions and interventions (blood tests, hospital admission and
pos-
sibly early delivery).
3Utero-placental Doppler ultrasound for improving pregnancy
outcome (Review)
Copyright 2010 The Cochrane Collaboration. Published by John
Wiley & Sons, Ltd.
-
This review will complement two other Cochrane reviews that
focus on the fetal and umbilical Doppler ultrasound in high-
risk populations (Alfirevic 2010a), and in low-risk
populations
(Alfirevic 2010b).
O B J E C T I V E S
To assess whether the use of utero-placental Doppler
ultrasound
(uterine arteries and placental vessels) improves the outcome
of
low- and high-risk pregnancies.
M E T H O D S
Criteria for considering studies for this review
Types of studies
All randomised trials and quasi-randomised studies comparing
utero-placental Doppler ultrasound (uterine, arcuate, radial
and
spiral arteries) in low- and high-risk pregnancies. We planned
to
perform sensitivity analysis by trial quality. We included
study
abstracts.Wehave considered cluster trials, thoughwe
foundnone,
but we did not think cross-over trials would be suitable for
this
topic.
Types of participants
Pregnant women, considered to be either low- or high-risk,
who
had utero-placental Doppler ultrasound performed at first or
sec-
ond trimester of pregnancy. We planned to include twin preg-
nancies and to perform subgroup analysis for that population
but
there were insufficient data.
Types of interventions
Doppler ultrasound of the utero-placental circulation
(uterine,
arcuate, radial and spiral arteries) in pregnancies at low and
high
risk. We did not include studies that considered the
combination
of utero-placental Doppler and fetal or umbilical Doppler in
this
review, but did include them in fetal andumbilicalDoppler
reviews
(Alfirevic 2010a; Alfirevic 2010b).
Comparisons
1. Doppler ultrasound of utero-placental vessels versus no
Doppler ultrasound of utero-placental vessels (including
comparisons of Doppler ultrasound of utero-placental vessels
revealed versus Doppler of utero-placental vessels concealed)
in
first trimester of pregnancy.
2. Doppler ultrasound of utero-placental vessels versus no
Doppler ultrasound of utero-placental vessels (including
comparisons of Doppler ultrasound of utero-placental vessels
revealed versus Doppler of utero-placental vessels concealed)
in
second trimester of pregnancy.
3. Comparison of different forms of Doppler ultrasound of
utero-placental vessels versus other types of Doppler
ultrasound
of utero-placental vessels in first trimester of pregnancy.
4. Comparison of different forms of Doppler ultrasound of
utero-placental vessels versus other types of Doppler
ultrasound
of utero-placental vessels in second trimester of pregnancy.
5. Comparison of different methods of Doppler ultrasound
measurements of utero-placental vessels in first trimester
of
pregnancy.
6. Comparison of different methods of Doppler ultrasound
measurements of utero-placental vessels in second trimester
of
pregnancy.
Types of outcome measures
Primary outcomes
1. Any perinatal death after randomisation.
2. Hypertensive disorders (pre-eclampsia, eclampsia,
haemolysis elevated liver enzymes and low platelets, chronic
hypertension).
Secondary outcomes
1. Stillbirth (as defined by trialists).
2. Neonatal death (as defined by trialists).
3. Any potentially preventable perinatal death.*
4. Serious neonatal morbidity - composite outcome including
hypoxic Ischaemic encephalopathy, intraventricular
haemorrhage, bronchopulmonary dysplasia, necrotising
enterocolitis.
5. IUGR (as defined by the trialists).
6. Fetal distress (as defined by the study authors).
7. Neonatal resuscitation required (as defined by
trialists).
8. Infant requiring intubation/ventilation.
9. Infant respiratory distress syndrome.
10. Apgar score less than seven at five minutes.
11. Neonatal admission to special care or intensive care unit,
or
both.
12. Preterm birth (birth before 37 completed weeks of
pregnancy):
i) spontaneous preterm birth;
ii) iatrogenic preterm birth.
13. Caesarean section (elective and emergency).
14. Caesarean section - elective.
4Utero-placental Doppler ultrasound for improving pregnancy
outcome (Review)
Copyright 2010 The Cochrane Collaboration. Published by John
Wiley & Sons, Ltd.
-
15. Caesarean section - emergency.
16. Serious maternal morbidity and mortality (composite
outcome with death of a woman while pregnant or within 42
days of termination of pregnancy).
17. Mothers admission to special care or intensive care unit,
or
both.
18. Gestational age at birth.
19. Infant birthweight.
20. Length of infant hospital stay.
21. Length of maternal hospital stay.
* Perinatal death excluding chromosomal abnormalities,
termina-
tion of pregnancies, birth before fetal viability (as defined by
tri-
alists) and fetal death before use of the intervention.
Search methods for identification of studies
Electronic searches
We contacted the Trials Search Co-ordinator to search the
Cochrane Pregnancy and Childbirth Groups Trials Register
(June
2010).
The Cochrane Pregnancy and Childbirth Groups Trials Register
is maintained by the Trials Search Co-ordinator and contains
trials
identified from:
1. quarterly searches of the Cochrane Central Register of
Controlled Trials (CENTRAL);
2. weekly searches of MEDLINE;
3. handsearches of 30 journals and the proceedings of major
conferences;
4. weekly current awareness alerts for a further 44 journals
plus monthly BioMed Central email alerts.
Details of the search strategies for CENTRAL and MEDLINE,
the list of handsearched journals and conference proceedings,
and
the list of journals reviewed via the current awareness service
can
be found in the Specialized Register section within the
edito-
rial information about the Cochrane Pregnancy and Childbirth
Group.
Trials identified through the searching activities described
above
are each assigned to a review topic (or topics). The Trials
Search
Co-ordinator searches the register for each review using the
topic
list rather than keywords.
Searching other resources
We searched the reference lists at the end of papers for
further
studies.
We did not apply any language restrictions.
Data collection and analysis
Themethodology for data collection and analysis was based on
the
Cochrane Handbook of Systematic Reviews of Interventions
(Higgins2008).
Selection of studies
Two review authors (TS,GG) independently assessed for
inclusion
all potential studies we identified as a result of the search
strategy.
We resolved any disagreement through discussion or, if
required,
we consulted the third author (ZA).
Data extraction and management
We designed a form to extract data. For eligible studies, two
re-
view authors (TS, GG) extracted the data using the agreed
form,
with additional help at times (Stephania Livio). We resolved
dis-
crepancies through discussion or, if required, we consulted
the
third author (ZA).We entered data into ReviewManager
software
(RevMan 2008) (TS) and checked for accuracy (GG).
When information regarding any of the above was unclear, we
attempted to contact authors of the original reports to
provide
further details.
Assessment of risk of bias in included studies
Two review authors (TS, GG) independently assessed risk of
bias
for each study using the criteria outlined in
theCochraneHandbookfor Systematic Reviews of Interventions (Higgins
2008).We resolvedany disagreement by discussion or by involving the
third author
(ZA).
(1) Sequence generation (checking for possible selection
bias)
We describe for each included study the method used to
generate
the allocation sequence in sufficient detail to allow an
assessment
of whether it should produce comparable groups.
We assessed the method as:
adequate (any truly random process, e.g. random number
table; computer random-number generator);
inadequate (any non-random process, e.g. odd or even date
of birth; hospital or clinic record number);
unclear.
(2) Allocation concealment (checking for possible selection
bias)
We describe for each included study the method used to
conceal
the allocation sequence in sufficient detail and determine
whether
intervention allocation could have been foreseen in advance of,
or
during recruitment, or changed after assignment.
5Utero-placental Doppler ultrasound for improving pregnancy
outcome (Review)
Copyright 2010 The Cochrane Collaboration. Published by John
Wiley & Sons, Ltd.
-
We assessed the methods as:
adequate (e.g. telephone or central randomisation;
consecutively numbered sealed opaque envelopes);
inadequate (open random allocation; unsealed or non-
opaque envelopes, alternation; date of birth);
unclear.
(3) Blinding (checking for possible performance bias)
We describe for each included study the methods used, if any,
to
blind study participants and personnel from knowledge of
which
intervention a participant received. We judged studies at low
risk
of bias if theywere blinded, or if we judged that the lack of
blinding
could not have affected the results. We assessed blinding
separately
for different outcomes or classes of outcomes.
We assessed the methods as:
adequate, inadequate or unclear for participants;
adequate, inadequate or unclear for personnel;
adequate, inadequate or unclear for outcome assessors.
(4) Incomplete outcome data (checking for possible attrition
bias through withdrawals, dropouts, protocol deviations)
We describe for each included study, and for each outcome or
class
of outcomes, the completeness of data including attrition and
ex-
clusions from the analysis. We state whether attrition and
exclu-
sions were reported, the numbers included in the analysis at
each
stage (compared with the total randomised participants),
reasons
for attrition or exclusionwhere reported, andwhethermissing
data
were balanced across groups or were related to outcomes.
Where
sufficient information was reported, or was supplied by the
trial
authors, we have re-included missing data in the analyses
which
we undertook. We assessed methods as:
adequate;
inadequate:
unclear.
We were to discuss whether missing data greater than 20%
might
impact on outcomes, acknowledging that with long-term follow
up, complete data are difficult to attain. However, none of
the
included studies had greater than 20% missing data.
(5) Selective reporting bias
We describe for each included study how we investigated the
pos-
sibility of selective outcome reporting bias and what we
found.
We assessed the methods as:
adequate (where it was clear that all of the studys pre-
specified outcomes and all expected outcomes of interest to
the
review have been reported);
inadequate (where not all the studys pre-specified outcomes
have been reported; one or more reported primary outcomes
were not pre-specified; outcomes of interest were reported
incompletely and so cannot be used; study fails to include
results
of a key outcome that would have been expected to have been
reported);
unclear.
(6) Other sources of bias
We describe for each included study any important concerns
we
have about other possible sources of bias.
We assessed whether each study was free of other problems
that
could put it at risk of bias:
yes;
no;
unclear.
(7) Overall risk of bias
We made explicit judgements about whether studies were at
high
risk of bias, according to the criteria given in the Cochrane
Hand-book for Systematic Reviews of Interventions (Higgins 2008).
Withreference to (1) to (6) above, we assessed the likely magnitude
and
direction of the bias and whether we considered it is likely to
im-
pact on the findings. We explored the impact of the level of
bias
through undertaking sensitivity analyses - see Sensitivity
analysis.
Measures of treatment effect
Dichotomous data
For dichotomous data, we present results as summary risk
ratio
with 95% confidence intervals.
Continuous data
For continuous data, we used the mean difference if outcomes
are
measured in the sameway between trials.We used the
standardised
mean difference to combine trials that measure the same
outcome,
but used different methods.
Unit of analysis issues
Cluster-randomised trials
We would have included cluster-randomised trials in the
analyses
along with individually randomised trials, had we identified
any.
We would have make adjustments using the methods described
in the Cochrane Handbook for Systematic Reviews of
Interventions(Higgins 2008) using an estimate of the intracluster
correlation co-
efficient (ICC) derived from the trial (if possible), or from
another
source. If ICCs from other sources had been used, we would
have
reported this and conducted sensitivity analyses to investigate
the
6Utero-placental Doppler ultrasound for improving pregnancy
outcome (Review)
Copyright 2010 The Cochrane Collaboration. Published by John
Wiley & Sons, Ltd.
-
effect of variation in the ICC. If we had identified both
cluster-
randomised trials and individually-randomised trials, we
would
have planned to synthesise the relevant information. We
would
have considered it reasonable to combine the results from both
if
there was little heterogeneity between the study designs and
the
interaction between the effect of intervention and the choice
of
randomisation unit were considered to be unlikely.
We would also have acknowledged any heterogeneity in the
ran-
domisation unit and perform a separate meta-analysis.
Cross-over trials
We considered cross-over designs inappropriate for this
research
question.
Dealing with missing data
For included studies, we noted levels of attrition. We would
have
explored the impact of including studies with high levels of
miss-
ing data in the overall assessment of treatment effect by using
sen-
sitivity analysis.
For all outcomes, we carried out analyses, as far as possible,
on an
intention-to-treat basis, i.e. we attempted to include all
partici-
pants randomised to each group in the analyses. The
denominator
for each outcome in each trial is the number randomised
minus
any participants whose outcomes were known to be missing. We
would have excluded data on outcomes where there was greater
than 20% missing data on short term outcomes had we encoun-
tered such data.
Assessment of heterogeneity
We assessed statistical heterogeneity in each meta-analysis
using
the T (tau-squared), I and Chi statistics. We regarded
hetero-
geneity as substantial if T was greater than zero and either I
was
greater than 30% or there was a low P-value (less than 0.10) in
the
Chi test for heterogeneity. Where we found heterogeneity and
random-effects was used, we have reported the average risk
ratio,
or average mean difference or average standard mean
difference.
Assessment of reporting biases
If there had been 10 or more studies in a meta-analysis we
would
have investigated reporting biases (such as publication bias)
using
funnel plots. We would have assessed funnel plot asymmetry
vi-
sually, and use formal tests for funnel plot asymmetry. For
contin-
uous outcomes, we would have used the test proposed by Egger
1997, and for dichotomous outcomes we would have used the
tests proposed by Harbord 2006. If asymmetry had been
detected
by any of these tests or was suggested by a visual assessment,
we
would have performed exploratory analyses to investigate it.
We
would seek statistical help if necessary.
Data synthesis
We carried out statistical analysis using the Review Manager
soft-
ware (RevMan 2008).We used fixed-effect meta-analysis for
com-
bining data where it was reasonable to assume that studies
were
estimating the same underlying treatment effect: i.e. where
trials
were examining the same intervention, and the trials
populations
and methods were judged sufficiently similar. If there was
clinical
heterogeneity sufficient to expect that the underlying treatment
ef-
fects differ between trials, or if substantial statistical
heterogeneity
was detected, we would have used random-effects analysis to
pro-
duce an overall summary, if this was considered clinically
mean-
ingful. If an average treatment effect across trials was not
clinically
meaningful, we would not have combined heterogeneous trials.
If
we used random-effects analyses, the results have been
presented
as the average treatment effect and its 95% confidence
interval,
the 95% prediction interval for the underlying treatment
effect,
and the estimates of T and I (Higgins 2009).
Subgroup analysis and investigation of heterogeneity
We had planned to carry out the following subgroup analyses
on
all outcomes:
1. measurements in high-risk population, low-risk population
and unselected population;
2. in singleton and twin pregnancies.
However, there were insufficient data to perform any
subgroup
analyses. We had also planned to pull together the three
subgroups
for the overall estimation.
For fixed-effect meta-analyses, we had planned to conduct
the
planned subgroup analyses classifying whole trials by
interaction
tests as described by Deeks 2001. For random-effects
meta-analy-
ses, we would have assessed differences between subgroups by
in-
spection of the subgroups confidence intervals;
non-overlapping
confidence intervals indicate a statistically significant
difference in
treatment effect between the subgroups.
Sensitivity analysis
We would have performed sensitivity analysis on the primary
out-
comes based on trial quality, separating high-quality trials
from
trials of lower quality. High quality would, for the purposes
of
this sensitivity analysis, have been defined as a trial having
ade-
quate sequence generation and allocation concealment.
R E S U L T S
Description of studies
See:Characteristics of included studies; Characteristics of
excluded
studies; Characteristics of studies awaiting classification.
7Utero-placental Doppler ultrasound for improving pregnancy
outcome (Review)
Copyright 2010 The Cochrane Collaboration. Published by John
Wiley & Sons, Ltd.
-
Results of the search
The searchwas designed to identify all randomised controlled
trials
on assessing the effectiveness of Doppler ultrasound, whether
us-
ing fetal-umbilical or utero-placental (maternal) vessels. We
iden-
tified 58 publications from 34 studies, of which we have
included
two in this review, involving data on 4993 women and 5009
neonates (Goffinet 2001; Subtil 2003).
We have excluded 30 studies, mainly because they assessed both
fe-
tal and umbilical vessels. For further details of trial
characteristics,
please refer to the tables of Characteristics of included
studies and
Characteristics of excluded studies. Two studies are awaiting
classi-
fication as we are trying to locate the authors but they both
appear
to remain unpublished (Ellwood 1997; Snaith 2006). The large
number of excluded studies reflects the fact that the search
was
designed for all Doppler ultrasound studies, including both
utero-
placental vessels and fetal-umbilical vessels. Most of the
studies
identified focused on fetal-umbilical vessels and are included
by
two other Doppler ultrasound reviews (Alfirevic 2010a;
Alfirevic
2010b).
Included studies
Included studies compared uterine artery Doppler assessments
in
the experimental group with no uterine artery Doppler
performed
in the control groups (Goffinet 2001; Subtil 2003). In both
stud-
ies, low-dose aspirin was administrated in cases of abnormal
uter-
ine artery Doppler findings (Goffinet 2001; Subtil 2003).
Both studies were of assessments of women in the second
trimester,
around time for fetal anomaly scan, and both included women
at
low risk for hypertensive disorders (Goffinet 2001; Subtil
2003).
One of the studies involved a mixture of singleton and twin
preg-
nancies (Subtil 2003), while the other did not state
specifically if
it included multiple pregnancies, although reported numbers
sug-
gest only singleton pregnancies were included (Goffinet
2001).
Excluded studies
We excluded 30 studies, mostly because they assessed
umbilical
arteryDoppler ultrasound. SeeCharacteristics of excluded
studies.
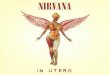
Risk of bias in included studies
The quality of the three included studies was reasonable,
although
blinding was not possible (Figure 1).
Figure 1. Methodological quality summary: review authors
judgements about each methodological quality
item for each included study.
8Utero-placental Doppler ultrasound for improving pregnancy
outcome (Review)
Copyright 2010 The Cochrane Collaboration. Published by John
Wiley & Sons, Ltd.
-
Allocation
Both studies had adequate sequence generation and
concealment
allocation (Goffinet 2001; Subtil 2003).
Blinding
Blinding women and/or staff in these trials was not generally
fea-
sible. Some outcomes like induction of labour and caesarean
sec-
tion may be influenced by the knowledge of Doppler results,
but
it may be possible to avoid bias in neonatal assessment.
Unfortu-
nately, the information on the attempts to protect against
biased
assessment was not available.
Incomplete outcome data
The two studies had adequate outcomedata (Goffinet 2001;
Subtil
2003). One of the studies awaiting classification (Ellwood
1997)
aimed to recruit 524 women, but undertook the analysis after
364
women had entered the trial, though data were available on
only
164. As this was not a block randomisation, we cannot be
sure
these are randomised groups being compared so we are
awaiting
the full study to be reported before including any data.
Selective reporting
We assessed both included studies as unclear because we did
not
assess the trial protocols.
Other potential sources of bias
One study appeared free of other biases (Subtil 2003), whilst
for
the other this was unclear (Goffinet 2001).
Sensitivity analyses
For sensitivity analyses by quality of studies, we have used
both ad-
equate labelled sequence generation and adequate allocation
con-
cealment as essential criteria for high quality. Two of three
stud-
ies met these criteria (Goffinet 2001; Subtil 2003), see Figure
1.However, we feel there are insufficient data to perform a
sensitivity
analysis by quality.
Effects of interventions
1. Uterine artery Doppler ultrasound versus no
Doppler ultrasound, 1st trimester (no studies)
We found no studies assessing uterine artery Doppler
ultrasound
in the first trimester.
2. Uterine artery Doppler ultrasound versus no
Doppler ultrasound, 2nd trimester (two studies, 4993
women)
We identified two studies assessing uterine artery Doppler
ultra-
sound in the second trimester in women at low risk for
hyperten-
sive disorders (Goffinet 2001; Subtil 2003). Both were full
pub-
lications (Goffinet 2001; Subtil 2003). Overall the quality of
the
included studies was good for the main criteria of
randomisa-
tion, allocation concealment and low percentage of missing
data
(Goffinet 2001; Subtil 2003), see Figure 1.
Primary outcomes
It is important to emphasise that this review remains
underpow-
ered to detect clinically important differences in serious
maternal
and neonatal morbidity.
Any perinatal death after randomisation
The difference in perinatal mortality between two groups was
not
statistically significant (average risk ratio (RR) 1.61, 95%
confi-
dence interval (CI) 0.48 to 5.39, two studies, 5009 babies,
Analysis
2.1). The heterogeneity was high (T = 0.55, Chi P = 0.06, I
= 72%) and therefore, we used the random-effects model for
the
analysis. We were unable to calculate the prediction interval
as
there were only two studies.
Subtil 2003 reported significantly fewer deaths in the
control
group (RR 3.14, 95% CI 1.10 to 8.98). This difference was
con-
tributed to by 17 abortions or medically indicated terminations
of
pregnancy in the 1253 women in the Doppler group (1.4%) com-
pared with three out of 617 in the control group (0.5%). In
addi-
tion, 78 of the 1253 women randomised toDoppler group (6.2%)
did not receive their allocated treatment. The reason was
termina-
tion of pregnancies for medical or social reasons in 15 women
and
perinatal deaths in two babies, but the reasons for the
remainder
of the women not receiving the Doppler ultrasound were not
doc-
umented. The analysis for Any potentially preventable
perinatal
death after randomisation which excluded all terminations
and
perinatal deaths for chromosomal abnormalities is more
clinically
relevant and showed no detectable difference (see below).
9Utero-placental Doppler ultrasound for improving pregnancy
outcome (Review)
Copyright 2010 The Cochrane Collaboration. Published by John
Wiley & Sons, Ltd.
-
Hypertensive disorders
There was no difference identified in maternal hypertensive
dis-
orders between two groups (RR 1.08, 95% CI 0.87 to 1.33, two
studies, 4987 women, Analysis 2.2).
Secondary outcomes
We found no significant difference in the pooled estimate of the
in-
tervention effect for the range of secondary outcomeswith
lowhet-
erogeneity where a fixed-effect meta-analysis was used. Most
pre-
specified secondary outcomes had high heterogeneity and
there-
fore an intervention effect estimate across studies was
calculated
using random-effects.
There was no significant difference in stillbirths (average RR
1.44,
95% CI 0.38 to 5.49, two studies, 5003 babies,
random-effects
T = 0.70, Chi P = 0.04, I = 75%, Analysis 2.3), or for
neonatal
deaths (RR 2.39, 95%CI 0.39 to 14.83, two studies, 5009
babies,
Analysis 2.4). Similarly for Any potentially preventable
perinatal
death after randomisation (average RR1.29, 95%CI 0.21 to
7.94,
two studies, 5009babies, random-effectsT 1.09,Chi P = 0.11,
I
= 60%, Analysis 2.5). These data should be interpreted
cautiously
because the numbers are small and heterogeneity is high.
The data for neonatal admission to special care baby unit
(SCBU)
or neonatal intensive care unit (NICU) (RR 1.12, 95% CI 0.92
to 1.37, two studies, 5001 babies, Analysis 2.13) and
iatrogenic
pretermbirth (average RR 0.92, 95%CI 0.51 to 1.65, two
studies,
4982 women, random-effects T = 0.09, Chi P = 0.15, I = 51%,
Analysis 2.15) are consistent with the overall picture showing
no
significant difference in two groups. The meta-analysis also
failed
to identify any difference in IUGR (average RR 0.98, 95% CI
0.64 to 1.50, two studies, 5006 babies, random-effects T =
0.08,
Chi P = 0.02, I = 82%, Analysis 2.7), although there was
high
heterogeneity, so it is also possible that there are different
effects
in the different studies, for unknown reasons.
Only one study assessed neonatal resuscitation (RR 0.94, 95%
CI
0.75 to 1.19, 3133 babies, Analysis 2.9), Apgar score less
than
seven at fiveminutes (RR 1.08, 95%CI 0.48 to 2.45, 3133
babies)
(Analysis 2.12) and caesarean sections (emergency plus
elective)
(RR 1.09, 95% CI 0.91 to 1.29, 3133 women) (Analysis 2.16).
We found no significant difference for any of these
outcomes.
None of the studies assessed the following outcomes: Serious
neonatal morbidity, Fetal distress, Infant requiring
intubation/
ventilation, Infant respiratory distress syndrome,
Spontaneous
preterm birth, Serious maternal morbidity and Maternal
admis-
sion to special care.
Non-prespecified outcomes
We did not include any non-prespecified outcomes.
Sensitivity analysis
Since we assessed both studies as adequate for sequence
generation
and allocation concealment (Goffinet 2001; Subtil 2003), we
did
not undertake sensitivity analysis by quality.
D I S C U S S I O N
Increasing interest in maternal Doppler in first and second
trimester led us to undertake this review which completes a
trio
of reviews on Doppler ultrasound in pregnancy. The other two
reviews focused on the use of fetal-umbilical Doppler
ultrasound
in high risk (Alfirevic 2010a) and normal pregnancies
(Alfirevic
2010a).
Despite wide use of uterine artery Doppler ultrasound in
clinical
practice, we identified just two randomised studies assessing
this
intervention in the second trimester of pregnancy involving
4993
women at low risk of hypertensive disorders (Goffinet 2001;
Subtil
2003) and found no difference in any perinatal or maternal
out-
comes. Considering that both included studies involved women
at
low risk for hypertensive disorders, this could possibly explain
the
lack of benefit identified for uterine artery Doppler
application
as incidence of adverse outcomes was low (any potentially
pre-
ventable perinatal death 0.4%, hypertensive disorders 7%,
IUGR
11%).
In both studies (Goffinet 2001; Subtil 2003), the finding of
patho-
logical uterine artery Doppler was followed by low-dose
aspirin
administration. When interpreting these data, it is important
to
highlight the presence of heterogeneity and small number of
par-
ticipants that makes our review underpowered rare events such
as
perinatal mortality and severe maternal outcomes.
Suprisingly, lower perinatal mortality was observed in the
con-
trol group in one study (Subtil 2003: risk ratio 3.14, 95%
confi-
dence interval 1.10 to 8.98, Analysis 2.1). This could be
possibly
explained by a higher percentage of women with termination
of
pregnancy or perinatal death that occurred in the Doppler
group
by chance before the Doppler ultrasound was carried out.
Summary of main results
We found no differences in any of the perinatal and maternal
outcomes when comparing uterine artery Doppler ultrasound in
the second trimester in women at low risk for hypertensive
disor-
ders versus controls. There were no studies of women in the
first
trimester.
Overall completeness and applicability ofevidence
10Utero-placental Doppler ultrasound for improving pregnancy
outcome (Review)
Copyright 2010 The Cochrane Collaboration. Published by John
Wiley & Sons, Ltd.
-
There were only two studies involving 4993 women, and
clearly
the meta-analysis remains underpowered to show clinically
im-
portant differences in primary outcomes. The identification of
an
abnormal results also needs an effective intervention before
the
screening test can be said to be helpful.
Quality of the evidence
The studies were of reasonable quality, but involved
insufficient
numbers of women overall to assess the rare outcomes of
perinatal
death and morbidity.
Potential biases in the review process
We attempted to minimise bias in a number of ways; two
review
authors assessed eligibility for inclusion, carried out data
extraction
and assessed risk of bias. Eachworked
independently.Nevertheless,
the process of assessing risk of bias, for example, is not an
exact
science and includes many personal judgements.
Agreements and disagreements with otherstudies or reviews
Findings from this meta-analysis are not in disagreement
with
other non-randomised studies that examined the role of
uterine
arteries in low-risk population in second trimester of
pregnancy.
A U T H O R S C O N C L U S I O N S
Implications for practice
Data in this meta-analysis failed to show that the use of
uterine
artery Doppler in second trimester in low-risk population for
hy-
pertensive disorders provides benefit for the baby or
mother.
Uterine arteryDoppler ultrasound is widely used in high-risk
preg-
nancy and progressively its use is spreading into the first
trimester,
although there are no randomised studies to show clear benefit
in
this population of women. Futher research is needed to prove
the
appropriateness of this clinical practice application.
Implications for research
As previously highlighted, larger studies are needed with
enough
power to show clearly the presence or absence of benefit
when
using uterine artery Doppler ultrasound in second trimester
in
low-riskwomen for hypertensive disorders.Moreover,
randomised
controlled trials of uterine artery Doppler in the first and
second
trimester, in combination with womans history and/or
biochemi-
cal serummarkers, are needed to evaluate the benefit of
combined
models.
A C K N OW L E D G E M E N T S
We would also like to thank Stefania Livio, who helped with
some
of the data extractions, and Eugenie Ong, who translated the
de
Rochambeau 1992 study.
As part of the pre-publication editorial process, this reviewhas
been
commented on by two peers (an editor and referee who is
external
to the editorial team), a member of the Pregnancy and
Childbirth
Groups international panel of consumers and the Groups
Statis-
tical Adviser.
R E F E R E N C E S
References to studies included in this review
Goffinet 2001 {published data only}
Goffinet F, Aboulker D, Paris-Llado J, Bucourt M, Uzan
M, Papiernik E, et al.Screening with a uterine doppler in
low risk pregnant women followed by low dose aspirin in
women with abnormal results: a multicenter randomised
controlled trial. British Journal of Obstetrics and
Gynaecology2001;108:5108.
Subtil 2003 {published data only} Subtil D, Goeusse P,
Houfflin-Debarge V, Puech F,
Lequien P, Breart G, et al.Randomised comparison of
uterine artery doppler and aspirin (100 mg) with placebo
in nulliparous women: the Essai Regional Aspirine Mere-
Enfant study (part 2). BJOG: an International Journal of
Obstetrics & Gynaecology 2003;110(5):48591.Subtil D,
Truffert P, Goeusse P, Dufour P, Uzan S, Breart
G, et al.Value of systematic doppler +/- low dose aspirin
to prevent vascular complications in primigravidae.
Hypertension in Pregnancy 2000;19(Suppl 1):9.
References to studies excluded from this review
Almstrom 1992 {published data only} Almstrom H, Axelsson O,
Cnattingius S, Ekman G,
Maesel A, Ulmsten U, et al.Comparison of umbilical-artery
velocimetry and cardiotocography for surveillance of small-
for-gestational-age fetuses. Lancet 1992;340:93640.
Almstrom H, Axelsson O, Ekman G, Ingemarsson I,
Maesel A, Arstrom K, et al.Umbilical artery velocimetry
may influence clinical interpretation of intrapartum
11Utero-placental Doppler ultrasound for improving pregnancy
outcome (Review)
Copyright 2010 The Cochrane Collaboration. Published by John
Wiley & Sons, Ltd.
-
cardiotocograms. Acta Obstetricia et Gynecologica
Scandinavica 1995;74:5269.Marsal K, Almstrom H, Axelsson O,
Cnattingius S, Ekman
G, Maesel A, et al.Umbilical artery velocimetry is more
effective than cardiotocography for surveillance of growth
retarded fetuses. Journal of Perinatal Medicine 1991;19(Suppl
2):84.
Ben-Ami 1995 {published data only}
Ben-Ami M, Battino S, Geslevich Y, Shalev E. A random
single Doppler study of the umbilical artery in the
evaluation
of pregnancies complicated by diabetes. American Journal of
Perinatology 1995;12(6):4378.
Biljan 1992 {published data only} Biljan M, Haddad N, McVey K,
Williams J. Efficiency of
continuous-wave Doppler in screening high risk pregnancies
in a district general hospital (a prospective randomized
study on 674 singleton pregnancies). Proceedings of 26th
British Congress of Obstetrics and Gynaecology; 1992 July
7-10; Manchester, UK. 1992:6.
Biljan MM, McVey KP, Haddad NG. The value of
continuous wave doppler assessment of fetal umbilical artery
in management of at risk pregnancies. Proceedings of 2nd
European Congress on Prostaglandins in Reproduction;
1991 April 30-May 3; The Hague, Netherlands. 1991:189.
Burke 1992 {published data only} Burke G, Stuart B, Crowley P,
Ni Scanaill S, Drumm J.
Does Doppler ultrasound alter the management of high-risk
pregnancy?. Care concern and cure in perinatal medicine.
13th European Congress of Perinatal Medicine; 1992 May;
Amsterdam, The Netherlands. Parthenon, 1992:597604.
Burke G, Stuart B, Crowley P, Ni Scanaill S, Drumm J.
Does Doppler ultrasound alter the management of high-risk
pregnancy?. Journal of Perinatal Medicine
1992;20(Suppl1):266.
Davies 1992 {published data only}
Breart G, Uzan S, Uzan M. Doppler ultrasound screening
during pregnancy [Letter; comment]. Lancet
1993;341(8843):5012.
Davies J, Spencer J, Gallivan S. Randomised trial of Doppler
screening in a general obstetric population. Proceedings of
26th British Congress of Obstetrics and Gynaecology; 1992
July 7-10; Manchester, UK. 1992:316. Davies JA, Gallivan S,
Spencer JAD. Randomised
controlled trial of doppler ultrasound screening of
placental
perfusion during pregnancy. Lancet 1992;340:1299303.Spencer JAD,
Davies JA, Gallivan S. Randomised trial of
routine Doppler screening during pregnancy. Journal ofMaternal
Fetal Investigation 1992;1:126.
de Rochambeau 1992 {published data only}
de Rochambeau B, Jabbour N, Mellier G. Umbilical doppler
velocimetry in prolonged pregnancies [La velocimetrie
Doppler ombilicale dans les grossesses prolongees.].
RevueFrancaise de Gynecologie et d Obstetrique 1992;87(5):
28994.
Doppler 1997 {published data only}
Doppler French Study Group. A randomised controlled
trial of Doppler ultrasound velocimetry of the umbilical
artery in low risk pregnancies Doppler French Study Group.
British Journal of Obstetrics and Gynaecology 1997;104(4):
41924.
Giles 2003 {published data only}
Giles W, Bisits A, OCallaghan S. The doppler assessment
in multiple pregnancy study (damp) and metaanalyses
of doppler and twins. American Journal of Obstetrics
andGynecology 2000;182(1 Pt 2):S17. Giles W, Bisits A, OCallaghan
S, Gill A. The doppler
assessment in multiple pregnancy randomised controlled
trial of ultrasound biometry versus umbilical artery doppler
ultrasound and biometry in twin pregnancy. BJOG: an
international journal of obstetrics and gynaecology
2003;110(6):5937.
Gonsoulin 1991 {published data only}
Gonsoulin W. Umbilical artery Doppler waveform analysis:
a randomized study on effect on outcome. American Journal
of Obstetrics and Gynecology 1991;164:370.
Haley 1997 {published data only}
Haley J, Tuffnell DJ, Johnson N. Randomised controlled
trial of cardiotocography versus umbilical artery Doppler in
the management of small for gestational age fetuses.
BritishJournal of Obstetrics and Gynaecology 1997;104(4):4315.
Hofmeyr 1991 {published data only}
Hofmeyr GJ, Pattinson R, Buckley D, Jennings J, Redman
CWG. Umbilical artery resistance index as a screening
test for fetal well-being. II. Randomized feasibility study.
Obstetrics & Gynecology 1991;78:35962.
Johnstone 1993 {published data only}
Johnstone FD, Prescott R, Hoskins P, Greer IA, McGlew
T, Compton M. The effect of introduction of umbilical
Doppler recordings to obstetric practice. British Journal of
Obstetrics and Gynaecology 1993;100:73341.
Mason 1993 {published data only}
Mason GC, Lilford RJ, Porter J, Nelson E, Tyrell S.
Randomised comparison of routine vs highly selective use of
Doppler ultrasound in low risk pregnancies. British Journal
of Obstetrics and Gynaecology 1993;100:1303.
McCowan 1996 {published data only}
McCowan LME, Harding J, Roberts AB, Barker S,
Townend K. Perinatal morbidity in small for gestational age
fetuses in relation to umbilical doppler. Proceedings of the
14th Annual Congress of the Australian Perinatal Society in
conjunction with the New Zealand Perinatal Society; 1996
March 24-27; Adelaide, Australia. 1996:P10.
McParland 1988 {published data only}
McParland P, Pearce JM. Doppler blood flow in pregnancy.
Placenta 1988;9:42750.
Neales 1994 {published data only}
Neales K. A randomised controlled study to assess the use
of Doppler ultrasound in the management of patients with
intrauterine growth retardation. Personal communication
1994.
12Utero-placental Doppler ultrasound for improving pregnancy
outcome (Review)
Copyright 2010 The Cochrane Collaboration. Published by John
Wiley & Sons, Ltd.
-
Newnham 1991 {published data only}
Newnham JP, ODea MRA, Reid KP, Diepeveen DA.
Doppler flow velocity waveform analysis in high risk
pregnancies: a randomized controlled trial. British Journalof
Obstetrics and Gynaecology 1991;98:95663.
Newnham 1993 {published data only}
Evans S, Newnham J, MacDonald W, Hall C.
Characterisation of the possible effect on birthweight
following frequent prenatal ultrasound examinations. EarlyHuman
Development 1996;45(3):20314.
Newnham J, Macdonald W, Gurrin L, Evans S, Landau L,
Stanley F. The effect of frequent prenatal ultrasound on
birthweight: follow-up at one year of age. Proceedings
of the 14th Annual Congress of the Australian Perinatal
Society in conjunction with the New Zealand Perinatal
Society; 1996 March 24-27; Adelaide, Australia. 1996:A26.
Newnham JP, Doherty DA, Kendall GE, Zubrick SR,
Landau LL, Stanley FJ. Effects of repeated prenatal
ultrasound examinations on childhood outcome up to 8
years of age: follow-up of a randomised controlled trial.
Lancet 2004;364:203844. Newnham JP, Evans SF, Michael CA,
Stanley FJ, Landau
LI. Effects of frequent ultrasound during pregnancy: a
randomised controlled trial. Lancet 1993;342:88791.
Nienhuis 1997 {published data only}
Nienhuis SJ. Costs and effects of Doppler ultrasound
measurements in suspected intrauterine growth retardation.
A randomised clinical trial. Thesis. Maastricht:
UniversitairePers Maastricht, 1995.
Nienhuis SJ, Ruissen CJ, Hoogland HJ, Gerver JW, Vles
J, de Haan J. Cost-effectiveness of a doppler policy in
suspected intrauterine growth retardation - a randomized
controlled trial. International Journal of Gynecology and
Obstetrics 1991;36 Suppl:32. Nienhuis SJ, Vles JS, Gerver WJ,
Hoogland HJ.
Doppler ultrasonography in suspected intrauterine growth
retardation: a randomized clinical trial. Ultrasound in
Obstetrics & Gynecology 1997;9(1):613.Ruissen CJ, Nienhuis
SJ, Hoogland HJ, Vles JFH, Gerver
WJ, De Haan J. Cost-effectiveness of a Doppler based policy
of suspected intrauterine growth retardation - a randomised
controlled trial. Journal of Maternal Fetal Investigation
1992;1:126.
Nimrod 1992 {published data only}
Nimrod C, Yee J, Hopkins C, Pierce P, Lange I, Fick G, et
al.The utility of pulsed Doppler studies in the evaluation
of
postdate pregnancies. Journal of Maternal Fetal
Investigation
1992;1:127.
Norman 1992 {published data only}
Norman K, Pattinson RC, Carstens E. Doppler velocimetry
in recurrent pregnancy loss: is there a role?. Proceedings
of
11th Conference on Priorities in Perinatal Care in South
Africa; 1992 March; Caledon, South Africa. 1992:714.
Omtzigt 1994 {published data only}
Omtzigt AWJ. Clinical value of umbilical doppler
velocimetry.Utrecht: University of Utrecht, 1990.
Omtzigt AWJ, Bruinse HW, Reuwer PJHM. A randomized
controlled trial on the clinical value of umbilical Doppler
velocimetry: neonatal outcome. Proceedings of 12th
European Congress of Perinatal Medicine; 1990 Sept 11-
14; Lyon, France. 1990:189.
Omtzigt AWJ, Bruinse HW, Reuwer PJHM. A randomized
controlled trial on the clinical value of umbilical Doppler
velocimetry. I. Obstetrical management. Proceedings of
12th European Congress of Perinatal Medicine; 1990 Sept
11-14; Lyon, France. 1990:210. Omtzigt AWJ, Reuwer PJHM,
BruinseHW. A randomized
controlled trial on the clinical value of umbilical Doppler
velocimetry in antenatal care. American Journal of Obstetricsand
Gynecology 1994;170:62534.
Pattinson 1994 {published data only}
Pattinson R, Norman K, Odendaal HJ. Management of
fetuses suspected of IUGR but with EDVs of the umbilical
artery: a randomised controlled trial. Proceedings of 26th
British Congress of Obstetrics and Gynaecology; 1992 July
7-10; Manchester, UK. 1992:5. Pattinson RC, Norman K, Odendaal
HJ. The role of
Doppler velocimetry in the management of high risk
pregnancies. British Journal of Obstetrics and
Gynaecology1994;101:11420.
Pattinson RC, Norman K, Odendaal HJ. The role of
doppler velocimetry in the management of pregnancies:
a randomized controlled trial. Proceedings of 11th
Conference on Priorities in Perinatal Care in South Africa;
1992 March; Caledon, South Africa. 1992:5963.
Pearce 1992 {published data only}
Pearce JM. The application of uteroplacental waveforms to
complicated pregnancies. In: Pearce JMP editor(s).
Dopplerultrasound in perinatal medicine. Oxford: Oxford
University
Press, 1992:15977.
Schneider 1992 {published data only}
Schneider KT, Amberg-Wendland D, Renz S, Furstenau
U. Prospective randomized study of the clinical value
of Doppler sonography as a screening procedure
[Prospektiv randomisierte Untersuchung zum klinischen
Wert der Dopplersonographie als Screeningverfahren].
Gynakologische Rundschau 1991;31(Suppl 1):13940.
Schneider KTM, Renz S, Furstenau U, Amberg-Wendland
D, Prochaska D, Graeff H. Doppler flow measurements as a
screening method during pregnancy: is it worth the effort?.
Journal of Maternal Fetal Investigation 1992;1:125.
Scholler 1993 {published data only}
Scholler J, Putz M, Sainz HG, Altrichter R, Philipp
K. Value of Doppler sonography in management of
non-risk pregnancies at term [Der Stellenwert der
Dopplersonographie bei der Betreuung von Nicht
Risikoschwangerschaften amGeburtstermin]. Gynakologisch
Geburtshilfliche Rundschau 1993;33(1 Suppl):1189.
Trudinger 1987 {published data only}
Trudinger BJ, Cook CM, Giles WB, Connelly AJ,
Thompson RS. Umbilical artery flow velocity waveforms in
high-risk pregnancy: randomised controlled trial. Lancet
1987;1:18890.
13Utero-placental Doppler ultrasound for improving pregnancy
outcome (Review)
Copyright 2010 The Cochrane Collaboration. Published by John
Wiley & Sons, Ltd.
-
Tyrrell 1990 {published data only}
Lilford RJ. Fetal assessment in laboratory vs standard
management of high risk pregnancy. Personal
communication 1989. Tyrrell SN, Lilford RJ, MacDonald HN, Nelson
EJ,
Porter J, Gupta JK. Randomized comparison of routine vs
highly selective use of Doppler ultrasound and biophysical
scoring to investigate high risk pregnancies. British Journalof
Obstetrics and Gynaecology 1990;97:90916.
Whittle 1994 {published data only}
Hanretty KP. Randomized study of doppler waveforms in
umbilical and uterine arteries as a screening method to
identify the compromised fetus. Personal communication
1988.
Whittle MJ, Hanretty KP, Primrose MH, Neilson JP.
Screening for the compromised fetus: a randomized trial
of umbilical artery velocimetry in unselected pregnancies.
American Journal of Obstetrics and Gynecology 1994;170:5559.
Williams 2003 {published data only}
Williams K, Farquharson D, Bebbington M, Dansereau J,
Galerneau F, Wilson RD, et al.A randomized controlled
clinical trial comparing non stress testing versus doppler
velocimetry as a screening test in a high risk population
[abstract]. American Journal of Obstetrics and Gynecology
2000;182(1 Pt 2):S109. Williams KP, Farquharson DF, Bebbington
M, Dansereau
J, Galerneau F, Wilson RD, et al.Screening for fetal well-
being in a high-risk pregnant population comparing the
nonstress test with umbilical artery doppler velocimetry: a
randomized controlled clinical trial. American Journal of
Obstetrics and Gynecology 2003;188(5):136671.
References to studies awaiting assessment
Ellwood 1997 {published data only}
Ellwood D. Predicting adverse pregnancy outcomes with
ultrasound. Personal communication 1997.
Snaith 2006 {published data only}
Snaith V. Support and reassurance in antenatal care (ongoing
trial). Current Controlled Trials (http://controlled-
trials.com/mrct) (accessed 21 March 2006).
Additional references
Aardema 2001
Aardema MW, Oosterhof H, Timmer A, van Rooy
I, Aarnoudse JG. Uterine artery Doppler flow and
uteroplacental vascular pathology in normal pregnancies
and pregnancies complicated by pre-eclampsia and small for
gestational age fetuses. Placenta 2001;22(5):40511.
Albaiges 2000
Albaiges G, Missfelder-Lobos H, Lees C, Parra M,
Nicolaides KH. One-stage screening for pregnancy
complications by color Doppler assessment of the uterine
arteries at 23 weeks gestation. Obstetrics &
Gynecology2000;96(4):55964.
Alfirevic 2010a
Alfirevic Z, Stampalija T, Gyte GML, Neilson JP. Fetal and
umbilical Doppler ultrasound in high risk pregnancies.
Cochrane Database of Systematic Reviews 2010, Issue 1.[DOI:
10.1002/14651858.CD007529.pub2]
Alfirevic 2010b
Alfirevic Z, Stampalija T, Gyte GML. Fetal and umbilical
Doppler ultrasound in normal pregnancy. Cochrane
Database of Systematic Reviews 2010, Issue 8.
[DOI:10.1002/14651858.CD001450.pub3]
Askie 2007
Askie LM, Duley L, Henderson-Smart DJ, Stewart LA.
Antiplatelet agents for prevention of pre-eclampsia: a meta-
analysis of individual patient data. Lancet 2007;369:
17918.
Barker 2004
Barker DJ. The developmental origins of chronic adult
disease. Acta Paediatrica. Supplement 2004;93(446):2633.
Bernstein 2000
Bernstein IM, Horbar JD, Badger GJ, Ohlsson A, Golan
A. Morbidity and mortality among very-low-birth neonates
with intrauterine growth restriction. The Vermont Oxford
Network. American Journal of Obstetrics and
Gynecology2000;182:198206.
BJOG 1995
Anonymous. Retraction of articles. British Journal ofObstetrics
and Gynaecology 1995;102(11):853.
Bower 1993
Bower S, Schuchter K, Campbell S. Doppler ultrasound
screening as part of routine antenatal screening: prediction
of pre-eclampsia and intrauterine growth retardation.
British Journal of Obstetrics and Gynaecology 1993;100(11):
98994.
Brosens 1972
Brosens IA, Robertson WB, Dixon HG. The role of the
spiral arteries in the pathogenesis of preeclampsia.
Obstetrics
and Gynecology Annual 1972;1:17791.
Burns 1993
Burns PN. Principles of Doppler and colour flow. Radiology
in Medicine 1993;85:316.
Chen 1996
Chen JF, Fowlkes JB, Carson PL, Rubin JM, Adler RS.
Autocorrelation of integrated power Doppler signals and its
application. Ultrasound in Medicine and Biology
1996;22:10537.
Cnossen 2008
Cnossen JS, Morris RK, ter Riet G, Mol BW, van der Post
JA, Coomarasamy A, et al.Use of uterine artery Doppler
ultrasonography to predict pre-eclampsia and intrauterine
growth restriction: a systematic review and bivariable meta-
analysis. Canadian Medical Association Journal 2008;178
(6):70111.
Deeks 2001
Deeks JJ, Altman DG, Bradburn MJ. Statistical methods
for examining heterogeneity and combining results from
14Utero-placental Doppler ultrasound for improving pregnancy
outcome (Review)
Copyright 2010 The Cochrane Collaboration. Published by John
Wiley & Sons, Ltd.
-
several studies in meta-analysis. In: Egger M, Davey Smith
G, Altman DG editor(s). Systematic reviews in health
care:meta-analysis in context. London: BMJ Books, 2001.
Egger 1997
Egger M, Smith GD, Schneider M, Minder C. Bias in
meta-analysis detected by a simple, graphical test.
BMJ1997;315:62934.
Espinoza 2006
Espinoza J, Romero R, Kim YM, Kusanovic JP, Hassan
S, Erez O, et al.Normal and abnormal transformation of
the spiral arteries during pregnancy. Journal of Perinatal
Medicine 2006;34:44758.
Fisk 2001
Fisk NM, Smith RP. Fetal growth restriction; small for
gestational age. In: Chamberlain G, Steer P editor(s).
Turnbulls obstetrics. 3rd Edition. Edinburgh: Churchill
Livingstone, 2001:197209.
Harbord 2006
Harbord RM, Egger M, Sterne JA. A modified test for
small-study effects in meta-analyses of controlled trials
with binary endpoints. Statistics in Medicine
2006;25(20):344357.
Harrington 1996
Harrington K, Cooper D, Lees C, Hecher K, Campbell S.
Doppler ultrasound of the uterine arteries: the importance
of bilateral notching in the prediction of pre-eclampsia,
placental abruption or delivery of small-for-gestational-age
baby. Ultrasound in Obstetrics and Gynecology 1996;7(3):
1828.
Higgins 2008
Higgins JPT, Green S, editors. Cochrane Handbook for
Systematic Reviews of Interventions Version 5.0.1 [updated
September 2008]. The Cochrane Collaboration, 2008.
Available from www.cochrane-handbook.org.
Higgins 2009
Higgins JP, Thompson SG, Spiegelhalter DJ. A re-
evaluation of random-effects meta-analysis. Journal of the
Royal Statistical Society, Series A, (Statistics in Society)
2009;172(1):13759.
Khong 1991
Khong TY. Acute atherosis in pregnancies complicated by
hypertension, small-for-gestational-age infants, and
diabetes
mellitus. Archives of Pathology and Laboratory Medicine
1991;115(7):7225.
Levy 1998
Levy RA, Avvad E, Oliviera J, Porto LC. Placental pathology
in antiphospholipid syndrome. Lupus 1998;7(Suppl 2):S81.
Martin 2001
Martin AM, Bindra R, Curcio P, Cicero S, Nicolaides KH.
Screening for pre-eclampsia and fetal growth restriction
by uterine artery Doppler at 11-14 weeks of gestation.
Ultrasound in Obstetrics and Gynecology 2001;18:5836.
Nayar 1996
Nayar R, Lage JM. Placental changes in a first trimester
missed abortion in maternal systemic lupus erythematosus
with antiphospholipid syndrome; a case report and review
of the literature. Human Pathology 1996;27(2):2016.
Nicolaides 2006
Nicolaides KH, Bindra R, Turan OM, Chefetz I, Sammar
M, Meiri H, et al.A novel approach to first trimester
screening for early pre-eclampsia combining serum PP-
13 and Doppler ultrasound. Ultrasound in Obstetrics and
Gynecology 2006;27(1):137.
Olofsson 1993
Olofsson P, Laurini RN, Marsal K. A high uterine artery
pulsatility index reflects a defective development of
placental bed spiral arteries in pregnancies complicated by
hypertension and fetal growth retardation. European Journal
of Obstetrics & Gynecology and Reproductive Biology
1993;49(3):1618.
Owen 2001
Owen P. Fetal assessment in the third trimester: fetal
growth
and biophysical methods. In: Chamberlain G, Steer P
editor(s). Turnbulls obstetrics. 3rd Edition. Edinburgh:
Churchill Livingstone, 2001.
Papageorghiou 2001
Papageorghiou AT, Yu CK, Bindra R, Pandis G, Nicolaides
KH: Fetal Medicine Foundation Second Trimester
Screening Group. Multicenter screening for pre-eclampsia
and fetal growth restriction by transvaginal uterine artery
Doppler at 23 weeks of gestation. Ultrasound Obstetrics
andGynecology 2001;18:4419.
Parra 2005
Parra M, Rodrigo R, Barja P, Bosco C, Fernndez V, Muoz
H, et al.Screening tests for preeclampsia through assessment
of uteroplacental blood flow and biochemical markers of
oxidative stress and endothelial dysfunction. American
Journal of Obstetrics and Gynecology 2005;193:148691.
Plasencia 2007
Plasencia W, Maiz N, Bonino S, Kaihura C, Nicolaides
KH. Uterine artery Doppler at 11+0 to 13+6 weeks in the
prediction of pre-eclampsia. Ultrasound in Obstetrics
andGynecology 2007;30:7429.
RevMan 2008
The Nordic Cochrane Centre, The Cochrane Collaboration.
Review Manager (RevMan). 5.0. Copenhagen: The Nordic
Cochrane Centre, The Cochrane Collaboration, 2008.
Sibai 2005
Sibai B, Dekker G, Kupferminc M. Pre-eclampsia.
Lancet2005;365:78599.
Spencer 2007
Spencer K, Cowans NJ, Chefetz I, Tal J, Meiri H. First
trimester maternal serum PP-13, PAPP-A and second
trimester uterine artery Doppler pulsatility index as marker
of pre-eclampsia. Ultrasound Obstetrics and
Gynecology2007;29:12834.
Von Dadelszen 2002
Von Dadelszen P, Magee LA. Could an infectious trigger
explain the differential maternal response to the shared
placental pathology of preeclampsia and normotensive
15Utero-placental Doppler ultrasound for improving pregnancy
outcome (Review)
Copyright 2010 The Cochrane Collaboration. Published by John
Wiley & Sons, Ltd.
-
intrauterine growth restriction?. Acta Obstetricia et
Gynecologica Scandinavica 2002;81(7):6428.
Yu 2005
Yu CK, Smith GC, Papageorghiou AT, Cacho AM,
Nicolaides KH, Fetal Medicine Foundation Second
Trimester Screening Group. An integrated model for the
prediction of pre-eclampsia using maternal factors and
uterine artery Doppler velocimetry in unselected low-risk
women. American Journal of Obstetrics and Gynecology
2005;193(2):42936.
Zhong 2010
Zhong Y, Tuuli M, Odibo AO. First trimester assessment of
placental function and the prediction of pre-eclampsia and
intrauterine growth restriction. Prenatal Diagnosis
2010;30:293308.
Indicates the major publication for the study
16Utero-placental Doppler ultrasound for improving pregnancy
outcome (Review)
Copyright 2010 The Cochrane Collaboration. Published by John
Wiley & Sons, Ltd.
-
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Goffinet 2001
Methods Multicentre randomised trial. Stratified by centre and
parity (nulliparous ormultiparous)
. Blocks of 4. Randomisatioin numbers were established using
tables of order 4 permu-
tations
Individual woman.
Participants Inclusion criteria:
All women attending for a routine antenatal visit before 24
weeks.
Nulliparaus and multiparus.
Low risk.
N = 3317, though analysis on 3133.
Exclusion criteria:
Women who had indications for UAD including chronic
hypertension, diabetes,
previous fetal death, IUGR, hypertensive disorders of
pregnancy.
Women known to be at high risk before 24 weeks did not enter the
trial.
Women with contraindications to aspirin were also excluded.
Interventions Experimental intervention: uterine artery Doppler
US
Uterine artery Doppler performed between 20 and 24. 100 mg of
aspirin daily
until the 35th week was prescribed to patients with abnormal
results.
N = 1672 randomised though 100 lost to follow up = 1572.
Control/comparison intervention: no Doppler US
Women allocated to the control group did not have a uterine
artery Doppler on
the day of the second-trimester abdominal US examination.
N = 1645 though 84 lost to follow up = 1561.
Outcomes Principal outcome: IUGR (birthweight < 10% and <
3% according to gestational age)
Pre-eclampsia, gestational hypertension.
Uterine bleeding, oligohydramnios, abnormal CTG.
Number of antenatal consultations, days of antenatal
hospitalisation, CTG
measurements, ultrasound and Doppler tests.
Peri and neonatal death, fetal distress defined by abnormal CTG
resulting in
intervention (caesarean or instrumental delivery), Apgar score,
neonatal resuscitation,
neonatal transfer.
Notes
Risk of bias
Item Authors judgement Description
Adequate sequence generation? Yes The randomisation was
stratified
according to centre and parity (nulliparae
or multiparae).
The randomisation numbers were
17Utero-placental Doppler ultrasound for improving pregnancy
outcome (Review)
Copyright 2010 The Cochrane Collaboration. Published by John
Wiley & Sons, Ltd.
-
Goffinet 2001 (Continued)
established using tables of order four
permutation.
Allocation concealment? Yes Randomisation procedure using
sealed envelopes.
The randomisation procedure was
verified by checking all unused envelopes
at the end of the trial and confirming that
envelopes had been used in ascending
order.
Blinding?
All outcomes
No Not possible to blind.
Incomplete outcome data addressed?
All outcomes
Yes Loss of participants to follow up at each
data collection point:
115 follow-up data missing.
Overall 100/1672 (6%) lost from
Doppler.
Overall 84/1765 (5%) lost from
control group.
Exclusion of participants after randomisa-
tion:
Shortly after randomisation, follow
up ceased for 69 women: 39 in Doppler
group and 30 in control group. Of those:
1. 48 (27 in Doppler and 21 in control)
follow up ended when verification of
admission criteria indicated that they
should not have been randomised.
2. 4 women refused further
participation after randomisation.
3. 6 had miscarriages before
ultrasound.
Free of selective reporting? Unclear We did not assess the trial
protocol.
Free of other bias? Unclear 2 centres stopped inclusions a few
month
after the beginning of the study and did
not send the records of 11 women they had
included
Describe any baseline in balance: none
identified.
18Utero-placental Doppler ultrasound for improving pregnancy
outcome (Review)
Copyright 2010 The Cochrane Collaboration. Published by John
Wiley & Sons, Ltd.
-
Subtil 2003
Methods Multicentre randomised controlled trial (12 centres).
Block randomisation - blocks of 8
or 16, stratified by centre
Unit of randomisation: individual woman, 2:1 ratio for
randomisation of Doppler vs
placebo
Part of a larger study (Essai Regional Aspirine Mere Enfant,
ERASME trial) which
evaluated the routine prescription of low-dose aspirin (100mg)
in nulliparous women
Participants Inclusion criteria:
Nulliparae (no previous delivery 22 weeks) between 14 and 20+6
weeks.
Singletons and twins.
N = 1870. 2491 women agreed to participate and were randomised.
621 were
excluded from the current evaluation as they were allocated to
routine aspirin leaving
1870 in the current evaluation. Data available on 1860
women.
Exclusion criteria:
No history of hypertension.
No clear indications for or contraindications to the
prescription of aspirin or
another anticoagulant during the pregnancy.
Interventions Experimental intervention: uterine artery Doppler
US
Half underwent utero-placental artery Doppler at the same time
as the second-
trimester anatomical ultrasound (22-24 weeks), with low-dose
aspirin (100 mg)
prescribed only if the findings were abnormal until 36
weeks.
N = 1253 women (22 twin pregnancies). Outcomes on 1244 women and
1249
neonates.
Control/comparison intervention: no Doppler US
The other half (1238) was further divided randomly into 2
groups:
i) daily treatment with low-dose aspirin 100 mg (N = 621)
excluded from the
current evaluation;
ii) or placebo until the end of 34 weeks (N = 617).
The group of patients receiving aspirin or placebo began
treatment the day after
randomisation (between 14+1 and 21+0 weeks) and stopped after 34
weeks.
N = 617 women (14 twin pregnancies). Outcomes on 616 women and
627
neonates.
Outcomes Pre-eclampsia, pregnancy related hypertension, very low
or low birthweight for gesta-
tional age (birthweight 3rd and 10th centile of the standard
curves used in France),
HELLP syndrome, placental abruption or a caesarean section
because of fetal indication
(uncompensated maternal hypertension, suspected IUGR, meconium
stained amniotic
fluid or placental abruption)
Notes Doppler group included 22 twin pregnancies and the control
group included 14 twin
pregnancies
Risk of bias
Item Authors judgement Description
Adequate sequence generation? Yes ...a randomisation list was
computer gen-
erated by themanufacturer of the treatment
19Utero-placental Doppler ultrasound for improving pregnancy
outcome (Review)
Copyright 2010 The Cochrane Collaboration. Published by John
Wiley & Sons, Ltd.
-
Subtil 2003 (Continued)
boxes before the study began. Treatment
randomisation was balanced in blocks of 8
and stratified by centre. Each block of eight
box numbers was then randomly mixed,
according to a random number table, with
eight boxes labelled Doppler. The ran-
domisation was thus balanced by blocks of
16 in these centres, and the box numbers
were not consecutive.
Allocation concealment? Yes ...each patient was randomly
allocated to a
group immediately after inclusion by con-
nection to an always available server.... Af-
ter verifying the inclusion criteria and the
patients consent, the server provided ei-
ther a treatment box number or the word
Doppler to the physician investigator. At
the end of prenatal consultation the physi-
cian gave the patient a numbered treatment
box (neither the physician nor the patient
knew whether this was aspirin or placebo)
or an appointment (between 22 and 24
weeks) for a utero-placental arteryDoppler.
Blinding?
All outcomes
No It was not possible to blind participants and
clinicians with regard t






![Research Article Effects of Yoga on Utero-Fetal-Placental ...subtle, pranic body, where the prana ows, and the mental body, where our thoughts are processed [ ]. e frequency ... protocol](https://img.pdfslide.us/doc/110x75/60ce42a4852bb83fc46bfdf3/research-article-effects-of-yoga-on-utero-fetal-placental-subtle-pranic-body.jpg)