Embed Size (px)
Citation preview

Dr.Omneya Nagy ElmakhzangySpecial Fetal Care UnitAin Shams University
DOPPLER IN DIAGNOSIS OF PLACENTAL INVASION

• Christian Andreas Doppler ( 29 November 1803 – 17 March 1853) was an Austrian mathematician and physicist. He is celebrated for his principle — known as the Doppler effect — that the observed frequency of a wave depends on the relative speed of the source and the observer.
DOPPLER IN DIAGNOSIS OF PLACENTAL INVASION

DEFINITION AND TYPES • Placenta accreta refers to an abnormality of placental
implantation in which the anchoring placental villi attach to myometrium rather than decidua, resulting in a morbidly adherent placenta.
• Placenta increta (chorionic villi penetrate into the myometrium) and placenta percreta (chorionic villi penetrate through the myometrium to the uterine serosa or adjacent organs..
• The pathogenesis is primarily attributed to defective decidualization of the implantation site

IS IT IMPORTANT TO DIAGNOSE?• In 1950, placenta accreta was rare, occurring in 1 in
30,000 deliveries in the United States . During the 1980s and 1990s, the incidence markedly increased, ranging from 1 in 533 to 1 in 2510 deliveries . The marked increase has been attributed to the increasing prevalence of cesarean delivery in recent yeas (uptodate sep.2014).
• Placenta accreta is undoubtedly a challenge, but with proper diagnosis and preparation, the goal is to decrease the morbidity of this rapidly increasing obstetric complication.
• In other words Proper Diagnosis gives a chance for a well prepared and well planned management

DIAGNOSTIC PERFORMANCE OF DIFFERENT ULTRASOUND MODALITIES
Sensitivity (%) Specificity (%) Positive predictive value (%)
Risk
Grey scale 95 76 82 93
Colour Doppler 92 68 76 89
Three-dimensional power Doppler
100 85 88 100
RCOG Green–top Guideline No. 27 , January 2011

1ST TRIMESTER PLACENTA ACCRETA
• Placenta accreta (and percreta) does occur in the first trimester. It is usually discovered during dilatation and curettage when massive bleeding occurs due to placental invasion of the myometrium by placenta (H¨ opker M, 2002)
• Individuals who are at risk for placenta accreta at term are also at risk for placenta accreta in the first trimester.
• This type of pregnancy, in which a sac is abnormally attached in the lower uterus, needs to be differentiated from ‘Cesarean scar pregnancy’ because in the latter, the pregnancy is entirely contained within the myometrial confines of the scar, with no part within the cavity itself.

Placenta Percreta in a patient with five previous Cesarean sections. The sac is low in the uterus and appears to be attached to the bladder wall.
Reproduced with permission of AIUM, J Ultrasound Med 2003

Placenta accreta at 8 weeks. This pregnancy progressed to term. Note that there is little myometrium between the sac and the bladder (arrow).
Reproduced with permission of AIUM, J Ultrasound Med 2003

Placenta increta at 6 weeks. Note almost no myometrium between the sac and bladder wall (arrow).
Reproduced with permission of AIUM, J Ultrasound Med 2003

SIGNS SUGGESTIVE OF PLACENTAL INVASION ON GRAYSCALE ULTRASOUND:
• Loss of the retroplacental sonolucent zone
• Irregular retroplacental sonolucent zone
• Thinning or disruption of the hyperechoic serosa–bladder interface
• Presence of focal exophytic masses invading the urinary bladder
• Abnormal intraplacental lacunae.

ABNORMAL PLACENTAL LACUNAE
• Visualization of lacunae had the highest sensitivity (79%) in the 15–20-week range and a sensitivity of 93% in the 15–40-week gestational age time frame (ISUOG 2005).
• They usually, but not always, have turbulent flow within them, and they appear irregular, often more linear rather than rounded and smooth bordered. They do not have the highly echogenic border that standard venous sinuses have.(Tornado-shaped flow)
• To predict placenta accreta the lacunae have to be highly vascular intraplacental rather than well defined extraplacental low flow blood vessels

Gray-scale image of a tornado-shaped sinus (moth Eaten) Color Doppler image showing placenta accreta with many sinuses.

Vascular sinuses in patients without placenta accreta. -Vascular areas lie between the placenta and myometrium ratherthan within the placenta; they have low flow. - Large well-defined vessels with low flow at the edge of the placenta

MYOMETRIAL THICKNESS
• Measurement of the thickness of the lower uterine segment in women who had had a previous Cesarean section and had a low-lying anterior placenta or placenta previa by measuring between the bladder wall and the retroplacental vessels, as seen by color Doppler.
• All patients later proven to have placenta accreta had myometrium of less than 1 mm, which was as predictive of accreta as lacunae.

Normal ‘clear’ or echolucent space between theplacenta and myometrial wall .
Lack of the clear zone in a normal anterior placenta
The area near the arrow appears to be abnormal, possibly due in part to drop-out. Thetransducer should be perpendicular to the bladder wall during evaluation of its integrity
Translucency zone

SIGNS SUGGESTIVE OF PLACENTAL INVASION ON COLOR DOPPLER
• Diffuse or focal lacunar flow
• Vascular lakes with turbulent flow (peak systolic velocity over 15 cm/s)
• Hypervascularity of serosa–bladder interface
• Markedly dilated vessels over peripheral subplacental zone.

Color Doppler images showing diffuse dilated intraplacental vasculature and marked periplacental vascularity between bladder anduterine serosa , compared with a normal placenta at the same gestational age

Color Doppler image of a tornado-shaped sinus
Am J Obstet Gynecol 2004

Color Doppler of placenta percreta with invasion of bladder wall

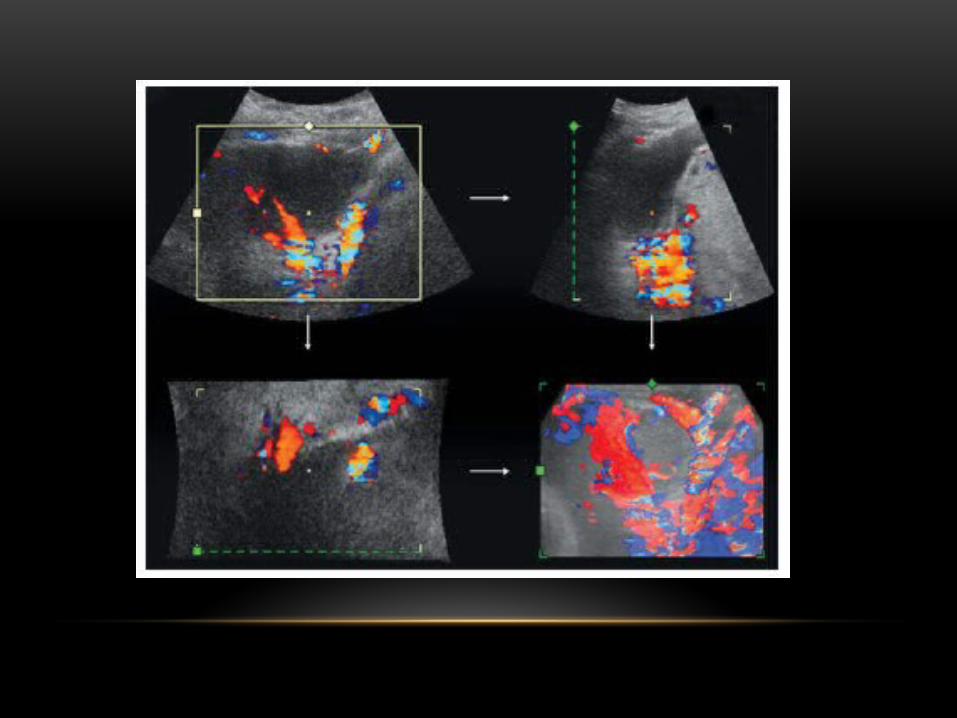
SIGNS SUGGESTIVE OF PLACENTAL INVASION BY 3D POWER DOPPLER
• Numerous coherent vessels involving the whole uterine serosa–bladder junction (basal view)
• Hypervascularity (lateral view)
• Inseparable cotyledonal and intervillous circulations, chaotic branching, detour vessels (lateral view).


FOR FURTHER INFORMATION ON DIAGNOSIS AND MANAGEMENT OF PLACENTAL INVASION
• http://www.uptodate.com.search.sti.sci.eg:2048/contents/clinical-features-and-diagnosis-of-placenta-accreta-increta-and-percreta?source=search_result&search=placenta+accreta&selectedTitle=1~38
• RCOG Green-top Guideline No. 27






























