Embed Size (px)
Citation preview

Updates in NOAC Reversal, What Have We Learned?Interim Outcomes Report (as of February 4, 2020)
Portola Pharmaceuticals Grant ID: 53174365

Activity Description In this video commentary, Dr. Gregory Piazza and Dr. Christian Ruff presented recent clinical data, guideline recommendations and updates on navigating the use of newly approved and emerging NOAC reversal agents. The webcast includes clinical case reviews and discussions about strategies to navigate the complexities of reversing anticoagulant effects of NOACs across diverse patient populations in emergent medical situations.
Availability August 30, 2019 – August 30, 2020
Credit 1.0 AMA PRA Category 1 Credit™
Sponsored by Academy for Continued Healthcare Learning (ACHL)
Supported by an educational grant from Portola Pharmaceuticals, Inc.
Intended Audience hospitalists, cardiologists, primary care physicians, nurses and others with an interest in NOAC reversal.
Distribution• ACHLcme.org: https://www.achlcme.org/ReversingNOACs• myCME.com: https://www.mycme.com/updates-in-noac-reversal-what-have-we-learned/activity/6102/• Direct Access: https://www.achlcme.org/digital/NOAC190/index.html
Overview

Participation (as of February 6, 2020)823 Participants (1,200 learners guaranteed); 322 Certificates Issued
Practicing Type23% Physicians, 41% NPs/PAs; 13% Nurses, 2% Pharmacists, 21% Other HCPs
Objectivity & BalanceObjectivity and balance rated as good/excellent by 98% of learners
Learning Objectives
99% of learners strongly agree or agree that all learning objectives were met, with an average rating of 3.56/4.0.
Faculty
Christian Ruff, MD & Gregory Piazza, MD were highly rated by 98% of learners.
Executive Summary

Executive SummaryAn effect size of 0.97 indicates that cardiology learners are now ~54.26% more knowledgeable of the content assessed than prior to participating in this education.
An effect size of 0.85 indicates that non-cardiology learners are now ~49.5% more knowledgeable of the content assessed than prior to participating in this education.
62% of learners intend to change their practice. Among other changes, 51% plan to change the management and/or treatment of their patients with use of NOACs when appropriate.
Cardiology learners demonstrated improved knowledge and competence on five of five pre/posttest questions with an average educational gain of 54%.
Changes will impact 3,901 to more than 6,947 patients taking NOACs per month.
There was a 95% increase in cardiology learners and a 336% increase in non-cardiology learners’ self-reported familiarity with agents that specifically reverse NOAC activity.

Activity Screenshots

Outcomes Reporting Methodology• First-attempt posttest scores are reported throughout:
• Initial answer choices for the posttest provide insight into the learners’ ability to immediately recall and apply the education.
• Pre- and posttest responses have been paired/matched. Non-completer data has been omitted from the analysis to ensure comparison groups are equivalent.
• Participant: term used to describe an HCP who reviewed CME front matter and took action to begin the education.
• Learner: Term used to describe an HCP who engaged in the core educational content/intervention.
• Cardiology learner: self-identified physician, nurse practitioner, or physician assistant specializing in cardiology.

Participation
23%
31%10%
13%
2%
21%
Participation by Clinician Type
Physician
Physician Assistant
Nurse Practitioner
Nurse
Pharmacist
Other HCP
Participants Learners Certificates 823 463 322
37%
21%
11%
9%
2%
2%
19%
Participation by Specialty
CardiologyEmergency Medicine/Critical CareFamily/General PracticeSugeryOrthopedicsRadiologyOther

Learning Objectives & Faculty
99% of learners would recommend this activity to a colleague.
Please rate the following objectives to indicate if you are better able to:
Analysis of RespondentsRating scale:
4=Strongly Agree; 1=Strongly Disagree
Review current approaches to the management of bleeding in patients receiving NOACs, as well as unmet needs with current practices 3.56
Compare and contrast approved and emerging reversal agents for NOACs, including their mechanisms of action and available data 3.56
Discuss clinical strategies for NOAC reversal in emergent patient scenarios 3.56
N=315
Please rate the faculty on the criteria listedChristian Ruff, MD & Gregory Piazza, MD
Analysis of RespondentsRating scale: 4=Excellent; 1=Poor
Ability to effectively convey the subject matter 3.57
Ability to present scientifically rigorous information 3.56

Objectivity & Balance
Activity was perceived as objective, balanced and non-biased.
60%
38%
2%0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Excellent Good Fair Poor
Objectivity & Balance
N=316
99%
Was the activity free of commercial bias?
Yes No

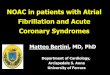
Familiarity Assessment: NOAC-reversals
Surprisingly, cardiology and non-cardiology learners reported similar levels of familiarity with NOAC reversal agents at baseline. Post-activity reports of familiarity increased by 29% and 23% among cardiology and non-cardiology learners, respectively.
How aware are you of agents that specifically reverse NOAC activity?A. Very awareB. Somewhat awareC. Not at all aware
Cardiology Learner Responses Non-cardiology Learner Responses
19%
54%
27%37%
57%
6%
A B C0%
20%
40%
60%
80%
100%
Pre (n=137) Post (n=137)
11%
69%
20%
48% 50%
2%
A B C0%
20%
40%
60%
80%
100%Pre (n=215) Post (n=215)

15%
55%
30%
40%
56%
4%
A B C0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Pre (n=215) Post (n=215)
Confidence Assessment: Bleeding Control
An increase in non-cardiology confidence with respect to bleeding control on NOAC treatment was observed postactivity.
How confident are you in controlling bleeding of a patient on NOAC treatment in an emergent situation?
Non-cardiology Learner Responses
A. Very confidentB. Somewhat confidentC. Not at all confident

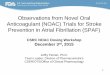
Pretest vs. Posttest Summary
Cardiology learners demonstrated improved knowledge and competence on five of five pre/posttest questions.
61% 60% 56% 58%
40%
85% 82%87%
80% 80%
0%
20%
40%
60%
80%
100%
Reluctance Bleeding Guidelines Efficacy MOAs
Pre Post
Topic % Change*
NOAC Reluctance 40%
NOACs and Bleeding 37%
Application of Guidelines 55%
Efficacy Data 38%
MOAs 100%
Cardiology Learners: Overview of Correct Responses
54% average
educational gain

Effect Size: Cardiology Learners
An effect size of 0.97 indicates that cardiology learners are now ~54.26% more knowledgeable of the content assessed than prior to participating in this education.
Pretest Posttest
55%Mean
0.296Standard Deviation
137Sample Size
83%Mean
0.281Standard Deviation
137Sample Size
Cohen’s d Effect Size = 0.97
This Effect Size calculation includes all cardiology learner completers and encompasses all pre/post-test questions. First-attempt posttest and paired data was used to calculate mean and standard deviation.
Cohen (1988): .2 = small, .5 = medium, .8 = largeWolf (1986): .25 = educationally significant, .50 = clinically significant

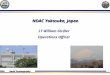
Pretest vs. Posttest Summary
Non-cardiology learners demonstrated improved knowledge and competence on four of four pre/posttest
questions.
62%
74%
56%
38%
87% 88%83%
72%
0%
20%
40%
60%
80%
100%
Guidelines Reversal Efficacy MOAs
Pre Post
Topic % Change*
Application of Guidelines 40%
NOAC Reversal 19%
Efficacy Data 48%
MOAs 89%
Non-cardiology Learners: Overview of Correct Responses49%
average educational
gain

Effect Size: Non-cardiology Learners
An effect size of 0.85 indicates that non-cardiology learners are now ~49.5% more knowledgeable of the content assessed than prior to participating in this education.
Pretest Posttest
58%Mean
0.289Standard Deviation
215Sample Size
82%Mean
0.274Standard Deviation
215Sample Size
Cohen’s d Effect Size = 0.85
This Effect Size calculation includes all non-cardiology learner completers and encompasses all pre/post-test questions. First-attempt posttest and paired data was used to calculate mean and standard deviation.
Cohen (1988): .2 = small, .5 = medium, .8 = largeWolf (1986): .25 = educationally significant, .50 = clinically significant

12% 15% 12%
61%
8%3% 4%
85%
33%
67%
A B C D0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Pre (n=137) Post (n=137) Follow-up (n=3)
Knowledge Acquisition: NOAC Reluctance
Many physicians and patients have been reluctant to embrace NOACs despite considerable data demonstrating that NOACs cause less serious
bleeding than VKAs, and that patients who experience a bleed while taking a NOAC have similar or better outcomes in comparison with patients on
warfarin. Cardiology learners in this activity demonstrated awareness of this challenge along with increased awareness postactivity. Increased
understanding of available reversal agents should quell concerns about effectively managing patients who present with serious bleeding or who
require urgent procedures.
Reluctance by clinicians to prescribe NOACs to patients may most commonly result from which of the following concerns?
Cardiology Learner Performance
A. The belief that warfarin is more effective than NOACs B. The clinical efficacy of NOACs is restricted to specific patient populationsC. Low compliance to NOAC useD. The concern of bleeding in certain populations, as well as potential
uncontrolled bleeding

14%22%
60%
4%5%9%
82%
4%
A B C D0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Pre (n=137) Post (n=137)
Clinical Competence: NOACs and Bleeding
Cardiology learners demonstrated increased recognition that specific reversal agents should be used sparingly after their participation in the activity. These data suggest that learners understand that the majority
of bleeds can be managed conservatively with temporary discontinuation of NOACs and supportive measures; time is the only
antidote required in most cases.
A 72-year old man with a history of hypertension, atrial fibrillation, and peptic ulcer disease takes apixaban 5 mg twice daily. He presents with dark, tarry stools and found to have a gastrointestinal bleed. He is transfused one unit of blood and has stable vital signs. This patient should be managed with which of the following?
Cardiology Learner Performance
A. Platelet substitution B. Use of a specific NOAC reversal agentC. Discontinuation or delay of apixabanD. Use of rFVIIa

14%
56%
10%
20%
3%
87%
4%6%
100%
A B C D0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Pre (n=137) Post (n=137) Follow-up (n=3)
Clinical Competence: Guidelines
A 55% increase in application of the AHA/ACC/HRS guidelines was observed for cardiology learners. These findings indicate that learners are familiar with the use of reversal agents in line with recent data and
guideline updates.
Around noon, a 65-year-old woman fell from stairs while at home and presented with persistent left hip pain. She takes apixaban for AF (last dose was in the morning). She has a left femoral neck fracture and internal bleeding. Recent 2019 guidelines issued by the AHA/ACC/HRS noted which of the following recommendations in terms of reversing this patient’s NOAC treatment resulting from uncontrolled bleeding?
Cardiology Learner Performance
A. There is insufficient evidence to warrant the recommended use of specific NOAC reversal agents
B. Andexanet alfa is recommended for the reversal of rivaroxaban and apixaban and idarucizumab for dabigatran in the event of life-threatening or uncontrolled bleeding
C. Perform a laboratory coagulation test on patients with uncontrolled bleeding before stopping anticoagulation and using supportive measures
D. Discontinuation or delay of drug as well as platelet substitution are adequate approaches to manage the bleeding events of patients on NOACs

Knowledge Acquisition: Guidelines
Non-cardiology learners demonstrated increased familiarity with the AHA/ACC/HRS guidance and available reversal agents.
Recent 2019 guideline recommendations issued by the AHA/ACC/HRS noted which of the following in terms of reversing NOAC treatment in the case of life-threatening or uncontrolled bleeding?
A. There is insufficient evidence to warrant the recommended use of specific NOAC reversal agents
B. Andexanet alfa is recommended for the reversal of rivaroxaban and apixaban and idarucizumab for dabigatran in the event of life-threatening or uncontrolled bleeding
C. Perform a laboratory coagulation test on patients with uncontrolled bleeding before stopping anticoagulation and using supportive measures
D. Discontinuation or delay of drug as well as platelet substitution are adequate approaches to manage the bleeding events of patients on NOACs
Non-cardiology Learner Performance
13%
62%
13% 12%6%
87%
3% 4%
14%
72%
14%
A B C D0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Pre (n=215) Post (n=215) Follow-up (n=7)

Clinical Competence: NOAC Reversal
Similar to what was observed for cardiology learners (slide 19), these learners also demonstrated increased competency with application of reversal agents and guideline recommendations in a theoretical case patient requiring an emergent procedure. However, follow-up survey
data indicate a lack of knowledge and competence retention, reinforcing the need for continued education on interruption and
bridging of anticoagulation in the event of life-threatening or uncontrolled bleeding.
Around noon, a 65-year-old woman fell from stairs while at home and presented with persistent left hip pain. She takes apixaban for AF (last dose was in the morning). She has a left femoral neck fracture requiring urgent surgery. Which of the following FDA approved NOAC reversal agents would be necessary for this patient prior to performing surgery?
A. Andexanet alfaB. CiraparantagC. Idarucizumab
Non-cardiology Learner Performance
74%
16%10%
88%
8%4%
71%
29%
A B C0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Pre (n=215) Post (n=215) Follow-up (n=7)

Knowledge Competence: Efficacy Data
Both learner types demonstrated gains in knowledge of the ANNEXA-4 clinical trial results, indicating an understanding of the MOA and efficacy of andexanet. This may translate into appropriate use of this reversal agent in eligible patients.
Based on the results of the ANNEXA-4 clinical trial, which of the following statements is correct?A. Reduction in anti–factor Xa activity via use of andexanet alfa was not overall predictive of hemostatic efficacy B. Reversal of NOACs can only be attained with factors that act non-specificallyC. Andexanet alfa administration led to a 92% decrease of median anti–FXa activity among patients receiving rivaroxaban or apixabanD. A high rate of mortality and thrombotic events are associated with NOAC reversal and restarting of therapy
Cardiology Learner Performance Non-cardiology Learner Performance
16% 18%
58%
8%6% 10%
80%
4%
A B C D0%
20%
40%
60%
80%
100%Pre (n=137) Post (n=137)
18% 15%
56%
11%8% 6%
83%
3%
A B C D0%
20%
40%
60%
80%
100%Pre (n=215) Post (n=215)

Knowledge Competence: Reversal Agent MOAs
Both learner types demonstrated marked improvement in their understanding of the MOAs of these available and emerging reversal agents for direct (apixaban, rivaroxaban, and edoxaban) and indirect (low-molecular-weight heparins and fondaparinux) FXa inhibitors.
In particular, learners demonstrated increased awareness that an additional reversal agent may be available in the near future.
Which of the following anticoagulation reversal agents target both direct and indirect parenteral FXa inhibitors?A. IdarucizumabB. Andexanet alfaC. CiraparantagD. Both Andexanet alfa and ciraparantag
Cardiology Learner Performance Non-cardiology Learner Performance
18%34%
8%
40%
8% 8% 4%
80%100%
A B C D0%
20%
40%
60%
80%
100%Pre (n=137) Post (n=137) Follow-up (n=2)
20%33%
8%
39%
10% 10% 8%
72%
17%33%
50%
A B C D0%
20%
40%
60%
80%
100%Pre (n=215) Post (n=215) Follow-up (n=6)

Practice Change: Cardiology Learners
68% of cardiology learners intend to change their practice. Among other changes, 44% plan to change the management and/or treatment of their patients with use of NOACs when appropriate.
50%
50%
42%
10%
3%
8%
44%
0% 10% 20% 30% 40% 50% 60% 70% 80%
This activity validated my current practice; no changes will be made
Other change
Create/revise protocols, policies, and/or procedures for patient selectionfor NOAC reversal
Increase utilization of NOAC reversal agents in appropriate patients
Change the management and/or treatment of my patients with the use ofNOACs when appropriate
Post (n=118)Follow-up (n=2)
Multiple responses allowed

Practice Change: Non-cardiology Learners
64% of non-cardiology learners intend to change their practice such as changing the treatment of their patients on NOACs or increasing utilization of NOAC reversal agents when appropriate.
71%
14%
14%
36%
3%
8%
13%
55%
0% 10% 20% 30% 40% 50% 60% 70% 80%
This activity validated my current practice; no changes will be made
Other change
Create/revise protocols, policies, and/or procedures for patient selectionfor NOAC reversal
Increase utilization of NOAC reversal agents in appropriate patients
Change the management and/or treatment of my patients with the use ofNOACs when appropriate
Post (n=192)Follow-up (n=7)
Multiple responses allowed

Barriers to Planned Change
41%
3%
3%
2%
10%
12%
9%
24%
16%
12%
12%
0% 10% 20% 30% 40% 50% 60%
No barriers
Other
Lack of consensus or professional guidelines
Lack of supporting evidece in the literature
Patient adherence/compliance issues
Organizational/institutional culture
Do not have an implementation strategy
Cost
Insurance/reimbursement issues
Lack of equipment or necessary resources
Lack of staff time to implement change
Post (n=309)
Participants indicated cost (24%) as the most common barrier to implementing changes in their practice, followed by insurance/reimbursement issues (16%). Of those who identified barriers, 87% will attempt to address the
perceived barrier(s) in order to affect change.
Multiple responses allowed

Patient Care Impact
17%
22%
20%
24%
17%
01-1011-2021-50>50
Changes in approach to NOAC use and greater understanding of guideline recommendations made by cardiology learners has the potential to impact 1,856 to more than 3,105 patients each month. This assumes data in the first chart above is representative of all
cardiology learners, who indicated they would change their practice as a result of their participation in this activity (68%). Furthermore, another 2,186 to 4,111 patients seen by other healthcare professionals may benefit from NOAC reversal agents.
N=123
Number of patients seen per month taking NOACs?
Cardiology Learner Performance Non-cardiology Learner Performance
20%
30%20%
20%
10%
01-1011-2021-50>50
N=192

Topics of Interest
3%
28%
46%
34%
35%
0% 20% 40% 60%
Other
Review of case scenarios for use of NOAC reversal agents
Clinical considerations for restarting anticoagulation afterNOAC reversal
Dosing considerations for NOAC reversal agents
Formulary approval of NOAC reversal agents
Clinical considerations for restarting anticoagulation after NOAC reversal was rated with highest interest for future education.
N=149; multiple responses allowed

Anticipated Practice ChangesPlease list what you will do differently as a result of participating in this activity:• More often consider use of specific reversal agents available• Able to manage life threatening bleeding on patients with NOACs,
able to evaluate and manage pts on NOACS• Advocate for use of NOAC reversal agents as appropriate,
educate colleagues on use of these agents.• Apply concepts to current practice; understand how NOAC affects
each patient differently• Ask hospital to have agents available and be very open to patients
who have bleeding of all levels on noacs• Be aware of the reversal agents and to utilize them as necessary• Be careful when reversing and for how long• Be more conscious of when patients are on NOACs• Be more informative of these conditions, test results and treatment
medications.• Better be able to understand the indications and dosing of
anticoagulation reversal agents.• better knowledge on reversal agents, NOAC• Better pt education and work to prevent clot events• Consider reversal agents for severe bleeding. Investigate
availability of reversal agents in my facility.• Consider specific reversals if available. Be more likely to restart AC
post bleed.• Consider using NOACs more frequently in elderly frail pts, explain
to others how monitoring PT Apt for Noacs is not appropriate
• Create approp. Protocols to use and consider use of approved NOAC agents
• Educate my patients better and better understand care of pts on NOAC with bleeding
• Educate on bleeding risk, will reduce underdosing if possible• Educate patients about warning signs of bleeds and that if they
go to ER; can be safely resolved, and educate patients about importance of taking medications.
• Encourage implementation of NOAC reversal agents• Evaluate reversal of agents more and evaluating patients on a
case by case• Feel more comfortable with noac reversal• Have reversal agents available, identify reversal agents for
emergency situations.• I have more understanding regarding the factors which affect
decision making in bleeding cases. Need to re-evaluate for under medicated patients
• Increase my assertiveness in restarting NOAC after bleeding event
• increase the use of Noacs• Know better which reversal agents are appropriate in which
situations• Know when to use reversal agents and which ones

Anticipated Practice ChangesPlease list what you will do differently as a result of participating in this activity:• Knowing that there are reversal agents for the NOACs and
implementing them prior to emergent surgical intervention if necessary. Educating patients that there are reversal agents prior to initiation of a NOAC.
• Less fearful treatment, know when to restart• Manage bleeds in NOAC pts, rethink restart of anticoagulation• Management of urgent surgery and restarting anticoagulation• Monitoring NOAC potential side effects more closely. Considering
reversal agents for emergent procedures.• More accurate and more interest with this topic• More aggressive reversal in emergent cases• More aware of IIa and Xa drugs, see if reversal agents are on
formulary here• More prepared to use medications as they become available,
review if patients are on the appropriate dosing• Not be as hesitant with NOACs in patients that need them. Start
using NOAC reversal agents.• Not obtain laboratory studies prior to using NOAC reversal agents
when reversal is indicated. Promptly restart NOAC agents in patients with GI bleeding after addressing cause of bleeding.
• Patient management in the OR• Prescribe more noac; Prescribe less warfarin• Prescribe reversal agents
• Provide better patient education and try to implement NOAC reversal agents into my practice
• Reassure patients that reversal agents are available• Restart AC sooner, speak to other providers regarding reversal
possibilities• Restart NOAC when appropriate after GI bleed• Reversal agents, when indicated• Stop inappropriate dosage lowering and more confidence in
prescribing NOACs now with reversal agents available• This improved my understanding. I will be able to explain this
better to patients• Treat patient with specific medications rather than non specific
procoagulants• Use DOACs more often; Know how to reverse them sensibly.
Excellent education session!!• Use NOAC reversal agents when appropriate.• Use reversal agents when appropriate. Discuss with patients
when starting NOACs• Will be able to confidently administer appropriate reversals in
emergency situations. Conversely, in stable pts it is multifactorial and requires more thought, which I now am aware of.

Contact InformationRichard KeenanVP, Education DevelopmentAcademy for Continued Healthcare Learning (ACHL)
E: [email protected]: 773-714-0705 ext. 215C: 610-742-0749