Embed Size (px)
DESCRIPTION
public health practive
Citation preview

Introduction
12: Public Health
Public health takes an overview of the health of populations, rather than focusing on individuals, with the aim of protecting and improving overall health. It is important for those working in health and social care to understand how public health policy affects services and the provision of health care so that they are able to contribute to improving health and well-being for the public.
In this unit, you will consider the origins of public health and its relevance for current health and social care strategies, including how health and illness is monitored to determine patterns of ill health and disease, together with the influences on the development of health policy and the different ways in which the public’s health is protected and promoted.
Learning outcomes:
On completion of this unit, you should:
1 Know the origins of public health policy and current public health strategies
2 Understand the factors that affect health status and patterns of ill health
3 Understand how public health is promoted and protected.
1a Know the origins of public health policy It is helpful to know how public health gradually developed as a discipline alongside increasing scientific and technical knowledge, in order to understand the links between disease, environ-mental conditions and poverty or economic deprivation. Whilst these links are still present, it is clear that public health policies have made a major contribution to increasing life expectancy and improving health.
Historical perspectives of public health systemsBefore the eighteenth century, the population of Britain was relatively small, as it was limited by both famine and regular outbreaks of the bubonic plague. Bad weather resulted in poor harvests with the production of food also limited by manual farming methods. Most of this population lived in the countryside, on villages and in farms. Whilst famine and plague were both deadly, they were not regular and, in between, people had access to fresh food and were able to grow food, although they were poor.

2 BTEC Level 3 National Health and Social Care
Key termsUrbanisation – the movement of people away from the countryside to live in the towns.Mortality rate – the number of people who die of a particular disease or condition compared with those who could be expected to die of all other causes.
Throughout the eighteenth and nineteenth centuries, though, the Industrial Revolution caused major changes in the British lifestyle. With the development of the manufacturing industry came new agricultural techniques, such as crop rotation and the seed drill, which meant that more food was produced, reducing famine, and that fewer farm labourers were required. As a result, the population not only increased to about 30 million by 1901, but also began to migrate from rural areas to larger towns and cities, such as London, Manchester and Edinburgh.
Unfortunately, urbanisation and the rapid increase in population occurred more quickly than the towns and cities could cope with, so there was not enough accommodation, with many families sharing living quarters in cramped conditions. Because there was no transport, factory owners built houses for their workers close to the factory and deducted the rent from their wages. The lack of any formal administrative organisations meant that the community lacked facilities, such as a sewage system, drainage and a constant water supply. Along with the absence of any building regulations, this meant that houses were often without natural light, air, running water and sanitation; one toilet could be shared between three houses, and waste was often dispensed into the local river – this particular practice caused ‘The Great Stink’ in London when the Thames was full of raw sewage.
Due to these living conditions, infectious diseases were common and spread rapidly, underlining the relationship between economic development and public health. Most notable were the frequent epidemics of cholera (especially in 1831, 1848 and 1866), typhus, and tuberculosis (TB), which may have accounted for a third of all deaths. There was, therefore, a high mortality rate, which means there were a high number of deaths per year in every 1,000 of the population.
The highest mortality rates were in larger cities,
amongst the elderly, women and children, and men who had been disabled by industrial accidents. Death rates were especially high in the areas where the poorest citizens lived, due to overcrowding, poor facilities and the malnourishment associated with a lack of money. Ill health was more common among working people than wealthier people because the latter were able to pay for private water and drainage systems and had better quality food and living conditions. However, the death of Prince Albert as a result of typhoid in 1861 meant that the upper classes had just as much reason to be concerned; they were forced to recognise that infectious diseases do not discriminate. After this, a number of influential people initiated social, environmental and health reforms.
Environmental reformsEdwin Chadwick was secretary and administrator of the Poor Law Commission, which controlled the systematic financial support of those who were worse off by taxing the better off. Chadwick recognised the connections between poverty, environment and infectious diseases, and was anxious about the rise in the economic costs of administering the Poor Law in a society so affected by epidemics. He decided that it would be more cost-effective to prevent disease instead by environmental action. Therefore, there was a concerted effort to collect statistical evidence proving the need for environmental reform to restrict the spread of disease and thus minimise the cost of providing the Poor Law relief. The Poor Law Commission asked for an investigation into the link between disease, sanitation and poverty in London. Three doctors undertook the study: James Kay, James Arnott and Southwood Smith, who demonstrated the link conclusively. This persuaded the government that environmental reform would be cost-effective. The conclusions that Chadwick
Key termIndustrial Revolution – the development of the machine-based manufacturing industry.

3Unit 12: Public Health
offered, which eventually helped change legis-lation, included recommending the responsible, water-borne disposal of sewage through glazed pipes, a system used to this day.
John Snow
Before John Snow’s work on cholera, many people recognised that other diseases like smallpox, measles and syphilis were infectious, but failed to realise the same of epidemics like typhoid and cholera, which were widely believed to be caused by polluted air or ‘miasma’. This explained why the poor suffered more than the wealthy. Some people, however, were beginning to believe in ‘germ theory’ – i.e. that infection could be caused by living organisms – and this paved the way for the use of antibiotics and surgical advancements.
John Snow was an anaesthetist who, in 1854, mapped the cholera epidemic in London and discovered an infected water pump in Broad Street as the source. He found that all those who had died had used this water pump, but that a brewery on the same street was unaffected because it received water from a different supply. The result of this discovery was that cholera was identified as a water-borne disease and Snow became recog-nised as a pioneer of epidemiology.
Edward Jenner and Louis Pasteur
In 1796, Edward Jenner conducted the first experi-ments in the development of immunisation, an important development in disease prevention. He inoculated a young boy against smallpox using cowpox, a milder form of the bacteria. Meanwhile, Louis Pasteur had proven that bacteria in the air caused liquids such as milk to ferment and become sour. As a result, he invented the process of Pasteurisation, wherein liquids are boiled to kill the bacteria and then allowed to cool, a method that is still used in the manufacture of dairy products in the modern age. In 1822, Jenner and Pasteur united to develop the vaccination process and this, along with the invention of antibiotics like penicillin, heralded the beginning of the usage of scientific methods in medicine.
Key termsWelfare state – in the UK, this is the system for providing health care for all and basic financial assistance for those who are sick or unable to work.Epidemiology – the study of the origin and spread of disease.
Health reformsIn the eighteenth and nineteenth centuries, a number of discoveries increased our under-standing of health and disease and influenced government action, eventually resulting in the formation in the twentieth century of what we now call the welfare state.
In the late eighteenth century, several surveys were conducted exploring the impact of the environment on health, disease and mortality in local populations. This became known as epidemi-ology, and some important examples include John Haygarth’s 1764 study of population and disease in Chester, Charles Turner Thackeray’s exploration of occupations, illness and life expectancy in Leeds and Robert Baker’s survey of the impact of cholera in Leeds, wherein he mapped the spread of the disease. Furthermore, Richard Miller analysed the incidence of typhus in Glasgow, and James Kay wrote on ‘The Moral and Physical Condition of the Working Classes’ in Manchester in 1832.
Key termImmunisation – vaccination or inoculation against disease by introducing a harmless form of the disease to stimulate the individual’s immune system defence.
Sir Edwin Chadwick© London Stereoscopic Company/Getty Images

4 BTEC Level 3 National Health and Social Care
Many Quakers such as Rowntree were prominent social reformers. The Rowntree family’s legacy continues into the modern age in the Joseph Rowntree Charitable Trust, which still investigates various social issues and provides charitable assistance. See www.jrct.org.uk.
Did you know... ?
Social reformsSocial reforms were important in the development of public health because of society’s attitudes towards poverty and the lack of formal, statistical knowledge of its real extent. Many assumed that illness, unemployment and old age should be anticipated and that people who did not prepare for them were ‘morally deficient’. The first national census was conducted in 1801 and, in the late 1800s, charitable and friendly societies began to provide help. Many people expected these societies and the Poor Law to be able to combat poverty, but its real extent went unrecognised.
Charles Booth
Charles Booth was a rich merchant from Liverpool who concerned himself with the reports he heard of working-class life. He looked into many different factors of the lives of the working class, such as where and how they were employed, their pastimes, their religion and the conditions in which they lived. Between 1889 and 1903, he published a work in three parts, entitled the ‘Life and Labour of the People in London’, pioneering social inquiry, inventing the idea of the poverty line, and aiming to identify the reasons for poverty. He concluded that 30 per cent of people in London were living in poverty, more than had been previ-ously thought and more than society’s established mechanisms could cope with.
Key termPoverty line – the financial level below which people were considered poor.
Seebhom Rowntree
Seebhom Rowntree was a member of the prominent Quaker family, who owned the Rowntree’s Cocoa works in York and devoted a great deal of their time to public work. Rowntree read Charles Booth’s survey on poverty in London and decided to conduct a similar experiment in York for comparison. He too found that 30 per cent of the population of York was living in poverty, so it follows that, at that time, about one third of the entire population of the country was in poverty. Rowntree was also pioneering in that he distinguished between different types of poverty:
primary poverty and secondary poverty. Primary poverty means that a family’s earnings are insuf-ficient to live on, and secondary poverty means that their income is sufficient but not spent most wisely. These are similar to the ideas of absolute poverty and relative poverty (see definitions in the ‘Did you know?’ box on page 17).
He also recognised that there were certain stages in a working-class person’s lifetime in which they were most susceptible to poverty. This is known as the cycle of poverty and the stages at which poverty is most likely to be a problem are in childhood, early marriage and childrearing, and old age. Overall, Rowntree’s studies demonstrated that poverty was caused by economic and social factors that individuals themselves could not necessarily control and, as a result, the government could intervene.
Booth and Rowntree were pioneers of the use of statistics and evidence to map the extent of poverty and provide explanations for what we now call deprivation.
The Boer War (1899–1902)
It was found that up to a third of recruits for the Boer War were not fit to serve in the war due to their poor health. The government was anxious about ‘national inefficiency’ and how to defend the Empire. After the war, child services such as the School Health Service and screening programmes were introduced.
William Beveridge
William Beveridge was a government adviser to the Liberal government of 1906–1914 on pensions for the elderly and National Insurance. By this time, the basic legislative framework had been created to better the population’s health, for which the government had accepted some responsibility.

5Unit 12: Public Health
During the Second World War, in 1942, Beveridge reported on how Britain ought to be rebuilt and he advised the government to combat the five ‘Great Evils’, which he considered to be ‘Want, Disease, Ignorance, Squalor and Idleness’. His report was instrumental in the creation of the welfare state.
The welfare state
When the government changed in 1945, the welfare state was formed, aiming to provide free
medical treatment and social security so that the people could be protected ‘from the cradle to the grave’. The government had now accepted respon-sibility for protecting and promoting the health of the public.
Table 12.1 shows how the government gradually accepted responsibility for public health and some of the drivers that were instrumental in making this happen.
Table 12.1 Milestones in public health and public health acts
Date What happened
1764–1774
John Haygarth’s study of disease in Chester, demonstrating that people were becoming aware of patterns of disease.
1795 Local men in Manchester establish a Board of Health, as the effects of industrialisation began to take hold.
1831–1832
13,000 people die of cholera in the first epidemic of the nineteenth century, causing some towns to set up Boards of Health.
1834 The Poor Law Amendment Act happens, meaning that Poor Law medical officers are appointed.
1838 The Poor Law Commission’s fourth report, including those of Arnott, Kay and Smith on disease in the slums of London.
1842 Edwin Chadwick’s report on the ‘Sanitary Condition of the Labouring Population of Great Britain’, which emphasises the need for national action by showing the social and economic costs of slum living.
1846 The first of numerous acts targeting unfit housing and living conditions, known as ‘nuisances’. The act, therefore, is referred to as the Nuisance Removals Act.
1848 Another cholera epidemic causes 21,000 deaths and fills the country’s burial grounds.
1848 The first national measure is passed, a Public Health Act which allows Local Health Boards to be started if requested by ten per cent of ratepayers or where the mortality rate is higher than 23 per 1,000. The act has a somewhat limited scope but results in the General Board of Health being established in London.
1854 The beginning of germ theory, with John Snow’s work, which links cholera to a polluted well in London’s Broad Street, identifying the links between poor sanitation, living bacterial organisms and disease.
1858 As a result of Londoners disposing of their faecal waste in the Thames, the river becomes an open sewer. The overpowering smell permeates Westminster and Parliament has to be adjourned. The incident becomes known as ‘The Great Stink’ of London.
1861 The death of Prince Albert from typhoid, a major killer in the nineteenth century, proves that the wealthy, too, could be susceptible to infectious diseases.
1864 Octavia Hill begins her campaign to improve the housing of working people to a decent standard, something which was effectively the first stage in the development of social housing.

6 BTEC Level 3 National Health and Social Care
During the twentieth century, overall health improved in the years following the growth of the NHS, together with technological and medical developments. For example, between 1945 and the 1970s, there was a mass immunisation programme against the major infectious diseases, such as polio (poliomyelitis), diphtheria and tetanus, which had been responsible for many childhood deaths and much disability. The last recorded case of polio in the UK was in 1982 and it was finally eradicated in Europe in 2002. Tuberculosis, however, has never been fully eradicated in the UK; the lowest number of recorded cases was 5,086 in 1987, and numbers have steadily risen since then.
Similarly, following the initial success of penicillin, different antibiotics have been developed and have been used to treat a wide range of previ-ously lethal infections. Improvements in antenatal, midwifery and neonatal care have significantly improved infant and maternal mortality.
Despite the medical and technological advances, it has been argued that the greatest contribution to health has been due to environmental advances, as the mortality rate began coming down before antibiotics and immunisation improved the chances of surviving infectious diseases. This was due, in particular, to the supply of clean water and the collection and treatment of sewage, together with clean air and improved living conditions, such as the provision of social housing after the Second World War, during which much of the housing stock had been destroyed.
1b Current public health strategies Governments are interested in public health because it directly affects the economic performance of the country. The more people who become unfit for work, either temporarily
or permanently – for example, as a result of disability – the lower the productivity of the country and the greater the cost to the welfare state, both in direct cost to the health services for treatment and indirectly through social insurance (unemployment or disability benefits, housing support, etc.). However, it is not only for economic reasons that governments support health; there are considerable social and ethical benefits. The attention that governments pay to the health of all members of the population, particularly the more vulnerable, is the mark of a civilised society.
The primary purpose of public health is therefore to reduce current and future risks to health. To do this, the government develops policies on public health, creating strategies to prevent ill health that are delivered through a range of different programmes at both national and local level. These programmes involve individuals and communities, as well as the health services and local authorities, recognising that the causes of ill health continue to include the environmental and social factors, as well as individual health and susceptibility to disease. However, the extent to which the government should try to prevent people from unhealthy choices or behaviour that is harmful to health continues to be controversial.
Public health strategies Key aspects of public health strategies include the need to monitor the health of people and communities, to develop plans to improve the health of the population and to prevent illness. Governments and health agencies need to have information in order to identify issues affecting health so that appropriate action can be taken. This usually involves carrying out research to establish patterns and trends in health and illness and encouraging action on health issues by individuals as well as at national and local level. The extent to which governments should intervene
Date What happened
1866 A fourth cholera epidemic causes 6,000 deaths. The Sanitary Act makes Sanitary Inspectors compulsory in cities and demands that local governments provide fresh water. Overcrowding, a major cause of disease, becomes classified as a ‘nuisance’.
1869 The Peabody Trust builds cheap flats that provide good living conditions and are of a good quality in London, buildings which are used to this day.

7Unit 12: Public Health
in the choices and behaviour of individuals has always been controversial, however.
Public health programmes have traditionally been delivered through the health services, particu-larly primary care services that are available to everyone.
Health servicesPrimary care services are so called because they are preventive services – an aspect of public health. They also include general practitioners, the first point of contact for most people. Primary care services are generally based in the community or other non-hospital settings. Primary care provides universal health services (i.e. services for everyone). These include:
●● immunisation – provided by GP or practice nurse
●● baby and child welfare services, including baby and child health clinics and child health and development checks (Child Health Promotion Programme)
●● school health services●● community midwifery and health-visiting
services, providing home visiting, health advice and support
●● general health and well-being clinics – well man and well woman clinics, which provide screening services (e.g. cervical and breast
cancer screening, heart health, smoking cessation).
All of these services are aimed at preventing ill health through monitoring, early detection and treatment of disease. However, despite the success of the National Health Service (NHS) in tackling acute and life-threatening conditions, the improvements in antenatal and postnatal maternity care, midwifery and neonatal care, which reduced infant and maternal mortality, and the virtual eradication of infectious diseases thanks to the programme of childhood immunisation and antibiotics, it was clear by the late 1970s that not everyone was benefiting equally from improved health and increased life expectancy.
Local authorities As a result, successive legislation financially encouraged and supported closer working between local health services and local author-ities to try and address the wider causes of health and health inequalities. Examples include the Healthy Schools Programme, school meals initia-tives, improvements to social housing stock and access to leisure facilities, such as swimming, walking and gym use, which people were actively encouraged to use. Targets were introduced to measure progress and actively monitored through joint inspection processes.
Table 12.2 Contemporary public health
Date Document Comment
1965 Tobacco advertising banned on TV
One of the first initiatives by government to regulate for harm rather than leaving it to individual choice.
1967 Alcohol driving limits introduced
Aiming to reduce death and injury by drink-driving, followed by compulsory fitting of seatbelts in new cars. However, it was not compulsory to wear them until 1983 when legislation was eventually passed after several failed attempts (see ROSPA, www.rospa.com).
1980 Black Report: Inequalities in Health
Documented increasing socio-economic (social class) differences in health. Identified a key factor as material deprivation. Called for a holistic approach and re-distribution of resources within health and associated services.
1986 The Health Divide: Margaret Whitehead
Commissioned by the Health Education Council (HEC) to update the evidence on health inequalities, the report found that the wealth gap was increasing and the link between material factors and lifelong health outcomes was strong. HEC disbanded by government.

8 BTEC Level 3 National Health and Social Care
Date Document Comment
1992 Health of the Nation (white paper)
From 1992 to 1997, the Health of the Nation (HOTN) strategy was the central plank of health policy in England and formed the context for the planning of services provided by the NHS. It was the first explicit attempt by government to provide a strategic approach to improving the overall health of the population. Identified five key areas – cancer, coronary heart disease (CHD) and stroke, mental illness, sexual health and HIV/AIDS and accidents, with 27 targets altogether.
1998 Acheson Report: Independent Inquiry into Inequalities in Health
Found that despite overall fall in mortality rates, these declined more rapidly for the better off (higher socio-economic classes). Recommended priority given to families with children.
1998 Sure Start launched
In response to government goal of reducing child poverty, provided services tailored to meet the particular deprivation issues in local areas. Initially for children 0–4 years, then 0–14 or 16 if disabled.
1999 Saving Lives: Our Healthier Nation (white paper)
First comprehensive action plan with targets to improve health for all but in particular for the worse off. Focused on preventable disease – cancer, CHD, stroke, accidents and mental illness – to be reduced by 2010. Emphasis on both individual behaviour and wider determinants, e.g. Health Action Zones in poorer areas. Health Development Agency created (transferred to National Institute for Clinical Excellence, NICE, in 2005).
2000 NHS Plan Investment in and reform of the NHS. National Service Frameworks introduced, NHS Direct, core national targets, including a national health inequalities reduction target, especially in child health. Cross-departmental strategy to abolish child poverty. Development of a Health Poverty Index to provide information about health status.
2001 National Strategy for Neighbourhood Renewal and UK Fuel Poverty Strategy
Initiative to reduce ‘postcode poverty’ through cross-sector action on energy-efficient homes (Local Authority Decent Homes programmes), winter fuel/cold weather payments and pressure on energy companies to keep prices down and deal fairly with low-income groups.
2002 Wanless Report: Securing our Future Health
Highlighted the cost of poor health on the NHS and recommended increased spending on health as a proportion of gross domestic product (GDP).
2003 Tackling Health Inequalities: A Programme for Action (white paper)
A three-year plan with a raft of initiatives with the emphasis on prevention and early detection of disease and commitment to reduce child poverty. Aims to reduce smoking, increase screening and improve access to treatment for cancer and CHD. Initiatives to increase Sure Start, increase breastfeeding, increase nursery placements, improve and reform welfare food programme, improve preventive action on children’s dental health and implement multi-disciplinary family support teams.

9Unit 12: Public Health
Date Document Comment
2004 Wanless Report: Securing Good Health for the Whole Population
Recommended evidence-based interventions to improve health, value for money and the right of individuals to choose.
2004 NHS Improvement Plan
Aim was faster, better quality care, safer and more effective treatment. Investment in NHS to counter health inequalities, focus on health and well-being by devolving decision making to local primary care trusts.
2004 Choosing Health (white paper)
Aimed to support the public to make healthier choices, especially diet. Three core principles:●● Informed choice – clear, honest information for people to make
their own health decisions.●● Personalisation – tailored personal support for individuals and
deprived groups. ●● Encouraging people to adopt healthy behaviours.
Implemented Local Health Improvement Partnerships between communities, groups, business and government and cross-government cooperation.
2010 Marmot Review: Fair Society, Healthy Lives
Revealed continuing social gradient in health between groups with best socio-economic advantage and those with the worst, not only in relation to life expectancy, but also to disability-free life expectancy. Recommended developing standards for a minimum income for healthy living.
2010 Child Poverty Act Defines child poverty and aims to set targets relating to the reduction in child poverty. Enables a Child Poverty Commission and local authorities to make arrangements to cooperate with partner authorities (e.g. police, transport, Strategic Health Authorities, PCTs and Youth Offending Teams).
Activity 1
Research and examine the public health document by Sir Liam Donaldson (the Chief Medical Officer, 1998–2010) ‘150 Years of the Annual Report of the Chief Medical Officer: On the State of Public Health 2008’. In particular, you should look at the chapter ‘1858: The First Annual Report of the Chief Medical Officer’ (www.dh.gov.uk).
Write a report identifying the development of public health and the similarities and differences between public health in 1858 and 2008?
What key aspects of public health strategies have been effective in improving health?
P1 P2 M1

10 BTEC Level 3 National Health and Social Care
Sources of information for determining patterns of ill healthAll of the historical studies and investigations relied upon analysing statistical data (numbers, facts and figures) to provide information to support their findings and present their arguments, partic-ularly about the relationship between deprivation (poverty) and ill health. This is called intelligence.
establish how many obstetricians and midwives will be needed. It is also important to determine, when taken together with the mortality rate, whether the population is growing, remaining stable or declining.
In many Western European countries, the birth rate is declining and is not high enough to ensure the population remains stable. This means that the demographic profile is getting older and there are more old people than young people. This has implications for economic competitiveness if there are not enough people of working age to pay into the welfare system to support those who have retired after paying in during their working lives. This is called social insurance and everyone in the UK who is working pays into the system through National Insurance contributions to finance services like the NHS.
Mortality rateThis is the number of people who die each year measured as a percentage of the population. The mortality rate of particular fatal diseases and conditions (causes of death) – for example, cancer of the lung – is also measured and compared with all other deaths, so there will be a mortality rate for each condition, as well as an overall mortality rate. The calculation is done per 100,000 of a population for each year. The standard mortality rate (SMR) assumes the average risk of death for those aged 16–65 years to be 100. Those with an SMR of 100+ have a higher risk of an early death.
Two types of mortality rate are considered very important as a general guide to the overall health of a population: infant mortality rate and maternal mortality rate. Infant mortality is the number of infants dying before their first birthday per 1,000 live births. It has been steadily dropping in the UK, and in 2008 was 4.5 per 1,000 live births, down from 12 per 1,000 in 1980 (Office for National Statistics, ONS).
Maternal mortality is the number of women dying during pregnancy or within 42 days of delivery. In the UK, this rate is now so low that statistics are only calculated every three years. For example, during the period 2003–2005, two million women gave birth in the UK and only 295 died from causes directly or indirectly related to pregnancy. The maternal mortality rate from 2003 to 2005
Key termsData – numerical information (e.g. how many deaths), usually expressed as a percentage. Intelligence – comes from analysing data and identifying what it means (e.g. by comparing two sets of data you can tell if something has improved or not).
Prior to the 1999 Acheson Report, information on health was not aligned with information on deprivation, which made it statistically difficult to establish the link between poor health and deprivation. However, following the NHS Plan in 2000, there was a major change in the type and volume of data available to provide information on the health of the UK population. In order to assess patterns of ill health and develop strat-egies that can improve health, action needs to be taken at both national and local level. This means information must be collected at national and local level to identify health differences. The government needs to know the following as a baseline for action.
Population and demographic profileThis means not only how many people there are in the UK, but also the age, sex and ethnicity of the population; some diseases, such as thalassemia (a genetic blood disorder), are more common in some ethnic groups, for example. Similarly, an older population will have quite different health needs from one with a younger profile.
Birth rateThis is used to plan maternity services and

11Unit 12: Public Health
was 14 per 100,000 (Centre for Maternal and Child Enquiries, CMACE: Saving Mothers’ Lives 2003–2005).
Morbidity ratesThis is a measure of the rate of ill health, whether temporary (acute), long term (chronic) or without cure (terminal). Some diseases are notifiable in law to the authorities because they pose a threat to public health and doctors must report incidences of these diseases to the local authority. Examples include tuberculosis and meningitis. Morbidity statistics examine the frequency and prevalence of diseases within population groups.
Social Trends is also published by the ONS, collecting and analysing data from a range of different government agencies and departments to identify changes in British society over time. Social Trends provides information on topics such as household spending, income and lifestyle.
Health Statistics Quarterly is another publication by the ONS that provides specific national infor-mation on health topics, including public health, health services provided by the NHS (not private providers) and social care. Health information is collected four times a year from health authorities and primary care trusts. It includes:
●● the number of patients in hospital (beds), their age and sex
●● the number of outpatients treated, including accident and emergency figures
●● the number of GP consultations●● the number of communicable diseases
reported●● the number of immunisations given●● the number and type of conditions treated●● the number of people who have been
discharged from hospital or outpatient treatment (finished consultant episodes)
●● the number and cause of death.
Registrar of Births, Marriages and Deaths (www.ips.gov.uk)The Registrar of Births, Marriages and Deaths collects information locally on behalf of the government. The Registrar General is responsible for these and the General Register Office is now part of the Home Office’s Identity and Passport Service.
The Association of Public Health Observatories (www.apho.org.uk)Public health observatories (PHOs) were developed in every NHS region and country in the UK, following ‘Saving Lives: Our Healthier Nation’ in 1999. The Association of Public Health Observatories (APHO) is an umbrella body repre-senting and coordinating the work of the 12 PHOs, working with universities, government and health organisations at local and national level to collect and gather facts and data about health. Each regional PHO provides intelligence
Key termStandard mortality rate – this calculation is based on the number of actual deaths compared with the expected number of deaths in a particular group.
Office for National Statistics (www.ons.gov.uk)The Office for National Statistics (ONS) is the main source of statistical data and information, it is part of the UK Statistics Authority, which is an aspect of government. The ONS is responsible for collecting, analysing and publishing much of the data that is regularly collected from a range of sources. The information is arranged into topic areas and there is a specific section of the website devoted to health issues.
The ONS carries out a census of the population every ten years, the next being due in 2011. The Census has been carried out since 1801 and is a count of every person and household in Britain and provides population statistics at neighbourhood, regional and national level for governments, local authorities, businesses and communities.
Explore the website at www.ons.gov.uk/census. The Census is a key source of information.
Regional information is collected and published annually, based on a particular theme each year. In 2010, for example, Regional Trends 42 examined ageing, comparing two different regions of the UK to identify trends.

12 BTEC Level 3 National Health and Social Care
for policy makers and practitioners in their own region (or country) by:
●● monitoring trends in health status and disease●● showing how health inequalities are being
tackled
●● assessing the effects of healthcare interventions and providing evidence needed to reduce health inequalities.
The PHOs have developed a set of information and intelligence tools, accessible via the internet,
Table 12.3 History of the Office for National Statistics
1086 First census in England and Wales carried out by William the Conqueror and published in the Domesday Book.
1500s Elizabeth I carried out an early census by asking bishops to count the number of families in their dioceses.
1600s James I (James VI of Scotland) asked bishops to provide numbers of families in the diocese to gauge the population.
1801 First regular population census for Great Britain held.
1837 General Register Office (GRO) for England and Wales established.
1841 First population census conducted by the General Register Office.
1855 General Register Office (Scotland) established.
1864 General Register Office (Ireland) established.
1939 National register created for entire population and identity cards issued.
1940 The Government Social Survey, which began as the Wartime Social Survey, created.
1941 The only decade in which a census was not held since 1801. Central Statistical Office (CSO) established.
1952 National Health Service Central Register formed from National Registration records.
1968 Claus Moser, now Lord Moser, established the Government Statistical Service.
1969 Business Statistics Office created.
1970 General Register Office and Government Social Survey merged to create the Office of Population Censuses and Surveys (OPCS).
1989 Business Statistics Office merged with the CSO.
1996 Office for National Statistics formed by merging CSO, OPCS and the statistics division of the Department of Employment
1997 Family Record Centre established at Myddelton Street, Islington.
2000 Statistics Commission and ‘National Statistics’ established.
2005 Announcement made by the Chancellor of the Exchequer of his intention to legislate for independence in statistics.
2007 Bill introduced in Lords and Royal Assent given.
2008 UK Statistics Authority established (Statistics Commission abolished).
Source: www.ons.gov.uk

13Unit 12: Public Health
that show detailed information about the health of people in a region, using key indicators for measuring health, such as the level of heart disease, teen pregnancy, education levels, income and employment, and comparing them with the national profile. These are:
●● health profiles – information about the health of people in 386 local authority areas, comparing issues such as levels of obesity, or binge drinking
●● indications reports – measure progress in reducing health inequalities and use European comparisons
●● health poverty index – an interactive tool used to compare different groups and populations in different regions
●● local basket of inequalities indicators – allow monitoring and measurement of interventions (programmes, etc.) designed to improve health.
All the interactive tools can be accessed from the APHO website (www.apho.org.uk) – have a go and see if you can compare your region with another.
National Centre for Health Outcomes Development (www.nchod.nhs.uk)The National Centre for Health Outcomes Development (NCHOD) collects all the infor-mation on health outcomes, including comparative information for health and local government organisations in England. It also shows how to measure health and the impact of health interven-tions and health care.
The Health Development AgencyThe Health Development Agency was a national authority providing evidence-based information on what works to improve health and reduce health inequalities. These responsibilities have now been transferred to the National Institute for Clinical Excellence (NICE), at www.nice.org.uk.
The World Health Organisation (www.who.int) The World Health Organisation has a great deal of information available which allows comparisons to be made with countries all over the world about health, mortality rates, income equality
and inequality, access to health services, etc. In addition, comparisons with specific European countries can be found through Eurostat (see http://epp.eurostat.ec.europa.eu).
Key groups in setting and influencing public health policyGovernment policy on health and well-being is influenced by a whole range of factors, not least of which is the cost to the NHS of treating people who become ill, as well as the economic costs from loss of productivity. At the same time, there are a number of organisations and groups who wish to bring health and well-being issues to the attention of the government to demand action, or who have an interest in influencing government for commercial ends.
Academic researchAcademic research is funded by various organisa-tions – for example, Research Councils UK, which uses public money to invest in research that helps the UK to have a ‘healthy society, a productive economy and contribute to a sustainable world’. It is a partnership between the previously separate research councils. Research in health and well-being looks at areas such as:
●● the development of a vaccine for influenza●● air pollution and health●● the immune system●● independent living support (sensing systems,
for example).
Research on happiness and well-being influenced government policy initiatives such as the New Deal Programme and Working Families Tax Credit scheme. Other key funding agencies include the Economic and Social Research Council, the Leverhulme Trust and the British Academy. The research is usually, but not always, carried out through universities.
Academic research can also be commissioned and funded from charitable and independent organisations. For example, the Joseph Rowntree Foundation continues to commission and report on poverty and health, carrying on the tradition started by Seebohm Rowntree.
Professionals and professional organisations such as the Royal Colleges (Surgeons, Obstetricians and

14 BTEC Level 3 National Health and Social Care
Gynaecologists, Medicine, General Practitioners, etc.), the Institute of Child Health, the Royal College of Midwives, the Royal College of Nursing and the British Medical Association all carry out research, often with academic institutions, to inform and influence health policy for the benefit of the population. The Department of Health and the NHS also fund research.
Research into clinical efficiency and evidence-based medicine is important, particularly for influencing professional practice, but it also influ-ences government spending decisions. For example, the National Institute for Clinical Excellence (NICE) looks at the efficacy not only of drugs, but also of surgical procedures and of areas of medical and nursing practice; the government will only fund drugs and treatments that have been shown to be effective through NICE research. The Social Care Institute for Excellence (SCIE) performs a similar role for social care professionals.
Other influences on government policy-making include representatives from the food and drinks industry and the pharmaceutical industry, who work with government on various initiatives aimed at helping individuals make healthier choices by, for example, food and drink labelling.
International influencesInternational influences are important because the government wants the UK to remain compet-itive and to ensure that health and well-being is comparable with other affluent and developed nations. The European Parliament influences government policies across the EU in a number of areas that are important to wider health, such as working hours. Similarly, groups that promote health and safety in the workplace, such as the Health and Safety Executive (HSE) and the Institute of Personnel and Development, have influenced policy in relation to working practice and employment law – for example, reducing stress in the workplace and enhancing parental leave.
2 Understand the factors that affect health status and patterns of ill health
Patterns of ill healthThe link between social class and health, evident from the historical perspectives, was similarly well-documented in the extremely influential Black Report 1980 (Townsend and Davidson, 1982). The report was commissioned in 1977 and was asked to examine available information about differences in health and longevity within the population and consider the factors contrib-uting to these.
The report examined the differences in mortality and morbidity according to social class and used the Registrar General’s five occupational categories, as used by government at the time. They found that there was an inverse relationship between social class (socio-economic status) and health; in other words, the higher the social
Key termEfficacy – usefulness and effectiveness; value.
Independent organisations such as Bandolier also produce evidence-based information. Bandolier is web-based information produced by a group of Oxford scientists and sponsored by various organisations, including the University of Oxford and private medical organisations. They develop evidence-based intelligence from searching and analysing recently published medical research papers and studies. The information is available on the website (www.medicine.ox.ac.uk/bandolier) and they have published books on specific topics. They have a dedicated Healthy Living Zone.
Pressure groupsPressure groups usually have a particular interest and will lobby the government on behalf of their group. Most pressure groups are charitable organisations, such as Age UK and the Child Poverty Action Group, who campaign to ensure the most vulnerable in society are treated fairly. Greenpeace and Friends of the Earth campaign on environmental issues that are harmful to health.

15Unit 12: Public Health
class, the lower the mortality rate. They offered a number of explanations, including possible statis-tical inaccuracy, social selection through upward social mobility of healthier people, the unhealthy lifestyles linked to working-class culture and economic differences.
Subsequent reports, particularly the Acheson Report and the more recent Marmot Review, show that, despite increases in health overall, health inequalities between the better off and the more deprived persisted and got wider in the late 1980s and early 1990s.
Health inequalities parallel income inequalities. Gender and ethnicity as explanations of health inequalities fail to address the income inequalities within these groups. All health inequalities can be explained by economic differences, which are linked to socio-economic status. Socio-economic status is defined by factors such as level of education, type of economic activity, income and place of residence. So, for example, average life expectancy at birth in England rose for men from 75.1 in 1997–1999 to 75.4 in 1998–2000 and for women the figures were 80.0 to 80.2 years,
respect ively. However, the gap in life expectancy between those living in the health authority (HA) area with the highest life expectancy (Kensington, Chelsea and Westminster HA) and those in the HA with the lowest life expectancy (Manchester HA) increased from 7.3 to 7.7 years for men and 5.9 to 6.6 years for women. A similar pattern was shown for infant mortality.
Table 12.4 shows the overall life expectancy between the years 1981 and 2002.
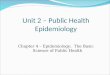
The graph on the next page shows the current life expectancy at birth by social class.
As a result of the social class differences in life expectancy, the government developed targets to reduce the gap in infant mortality and life expectancy between the highest performing areas and the lowest, developing indicators to support the national targets (a ‘basket of indicators’). The targets were formulated to take into account socio-economic groups and geographical areas, as well as access to health care. You can access infor-mation on your local area through the interactive tool on the APHO website (www.apho.org.uk).
Table 12.4 Life expectancy and health expectancies at birth: by sex, 1981 and 2002
Males Females
1981 2002 Absolute change (2002–1981)
1981 2002 Absolute change (2002–1981)
Life expectancy (years)
70.9 76.0 5.1 76.8 80.5 3.7
Healthy life expectancy (years)
64.4 67.2 2.8 66.7 69.9 3.2
Ill health (years) 6.4 8.8 2.4 10.1 10.6 0.5
% of life healthy 90.9 88.4 –2.5 86.9 86.8 –0.0
Disability-free life expectancy
58.1 60.9 2.8 60.8 63.0 2.2
Limited (years) 12.8 15.1 2.4 16.0 17.5 1.5
% of life without disability
82.0 80.1 –1.9 79.1 78.3 –0.9
Source: Office for National Statistics, Government Actuary’s Department

16 BTEC Level 3 National Health and Social Care
Life expectancy at birth by social class, a) males and b) females, England and Wales, 1972–2005
++
1972–76 1977–81 1982–86 1987–91 1992–96 1997–2001 2002–2005
1972–76
Social Class
I
II
IIIN
I
V
AII
IIIM
IV
1977–81 1982–86 1987–91 1992–96 1997–2001 2002–2005
Years
(a) Males90
85
80
75
70
Years
(b) Females
Source: Of�ce for National StatisticsLongitudinal Study
90
85
80
75
70
+
+
++
++
+++
+++
++
+++
+++
+
+
+
+
++++

17Unit 12: Public Health
Not only are there differences in life expectancy, it is clear that major life-limiting diseases and conditions such as cancer, heart disease, stroke and diabetes are more prevalent in people living in the most deprived areas, so not only do they suffer from lower life expectancy, they have poorer health during their later years – their healthy life expectancy is reduced, by about 17 years for the poorest (Marmot Review: Fair Society, Healthy Lives, 2010). At the same time, their access to health care can be uneven, since GPs and other services are not distributed evenly across the country. The introduction of targets for waiting times was intended to address this.
Following the ‘Choosing Health’ white paper, public service agreements were introduced between local authorities and primary care trusts (PCTs) in the areas with the worst health depri-vation indicators, with the intention that they would reduce their health inequalities faster than average. This became known as the ‘Spearhead’ group and was made up of 70 local authorities and
88 PCTs in the bottom fifth nationally for three or more of these indicators:
●● male life expectancy at birth●● female life expectancy at birth●● cancer mortality rate in under 75s●● cardio-vascular (heart) disease mortality rate
in under 75s●● Index of Multiple Deprivation average score
(covers economic, social and housing factors – for more information, see Communities and Local Government website: www.communities.gov.uk).
As well as reducing the gap in life expectancy, the targets cover reducing cardio-vascular disease and cancer, reducing smoking, improving educational achievement and unemployment, tackling crime and neighbourhood renewal. The government has targeted funding at the Spearhead areas to support these initiatives. The Spearhead areas are primarily in the North East, North West, the West Midlands and parts of East and South London. Progress towards these targets will be monitored through the PHOs.
According to the United Nations declaration at the World Summit on Social Development in Copenhagen in 1995, absolute poverty is:
‘a condition characterised by severe deprivation of basic human needs, including food, safe drinking water, sanitation facilities, health, shelter, education and information. Absolute poverty depends not only on income, but also on access to services.’
Relative poverty is defined by being below an agreed threshold, considered adequate for an acceptable standard of living. The European Union defined relative poverty as:
‘if income and resources are so inadequate as to preclude them from having a standard of living considered acceptable in the society in which they live. Because of their poverty they may experience multiple disadvantage through unemployment, low income, poor housing, inadequate health care and barriers to lifelong learning, culture, sport and recreation. They are often excluded and marginalised from participating in activities (economic, social and cultural) that are the norm for other people and their access to fundamental rights may be restricted.’
Source: European Commission, Joint Report on Social Inclusion, 2004
In the EU, people falling below 60 per cent of median (the middle point) income are said to be at risk of poverty. Most people in developed countries suffer from relative rather than absolute poverty.
Did you know... ?

18 BTEC Level 3 National Health and Social Care
It is important to monitor progress against targets to ensure that public health programmes and initiatives are effective. Patterns of disease and ill health can be monitored, differences noted and targeted action taken. For example, some South Asian communities have a greater risk of high cholesterol, whereas some Caribbean communities are at higher risk of diabetes. It may therefore be cost effective to introduce screening programmes to identify those at risk before they become ill so that preventive measures can be taken (e.g. encour-aging changes to diet and patterns of exercise). This will prevent later hospital admissions.
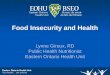
Factors affecting healthResearch has shown that the factors affecting health are remarkably consistent over time and that they fall broadly into the three categories identified historically – environmental factors, social factors and biological/health factors.
As a result, inequalities have been examined at neighbourhood level so that the social and environmental factors affecting health can be
more easily identified and local authorities can take action to improve health.
Environmental factors ●● Adequate housing: a place to live that is
structurally sound, has sufficient space for the number of people living there, has heating and utilities (gas, water, electricity, etc.) that are affordable.
●● Transport: access to affordable transport which enables travel to, for example, out-of-town shopping areas for cheaper, bulk purchases or access to health care. This can be difficult in some instances, e.g. in rural areas for non-car owners or older people.
●● Pollution: this has direct and negative effects on health – for example, car fumes causing respiratory problems (e.g. asthma).
●● Nutrition: healthy eating depends on knowledge of how food affects health, access to affordable healthy food and basic cooking skills. If any of these are lacking, nutrition is likely to be poor and health impaired over the
Age standardised mortality rates by socio-economic classification (NS-SEC) and region, men aged 25–64, 2001–2003
Eng
land
&W
ales
Routine
Semi-routine
Lower supervisory and technical
Small employers, own account workers
Semi-routine
Lower supervisory and technical
Small employers, own account workers
English Health Regions
Source: Of�ce for National Statistics
Eas
tern
Sou
thW
este
rn
Sou
thE
aste
rn
Eas
tM
idla
nds
Wes
tM
idla
nds
Yor
kshi
re &
Hum
ber
Lond
on
Nor
thW
est
Nor
thE
ast
Mor
talit
y ra
te p
er 1
00,0
00
800
700
600
500
400
300
200
100
0

19Unit 12: Public Health
long term due to conditions such as obesity, which can lead to heart disease and diabetes.
Social factors●● Child development: children from poorer
homes lag behind their wealthier peers in their development, including cognitive development. Their less bright but wealthier peers overtake bright children from poorer homes by the age of three, affecting educational achievement. Parenting, infant nutrition and home safety are also key factors affecting child development.
●● Education: people with good educational outcomes, currently five GCSEs at A* to C are more likely to go on to higher education and better paid jobs.
●● Employment: provides sufficient money for necessities. Research by the Rowntree Foundation found there was broad agreement within the population on what were considered necessities for a minimum standard of living, including playing a full part in society. Based on these views, in 2008, a single person in Britain needed to earn £13,000 before tax to afford such a lifestyle and a couple with two children needed £27,600. A person in full-time work on the national minimum wage cannot achieve this minimum income standard and neither do those on benefits (sources: A Minimum Income Standard for Britain in 2009; Centre for Research in Social Policy, Loughborough University for the Joseph Rowntree Trust, 2009). Income inequality has remained stable since 2005/6 after rising during the late 1980s and early 1990s.
●● Lifestyle factors: these are the factors most likely to be within the individual’s control. They include things like the amount of physical exercise, smoking, use of alcohol and drugs, risk-taking behaviour and peer pressure to engage in this.
●● Social and community factors: social isolation has a negative impact on mental health because those who lack social support can find it more difficult to manage everyday stresses and strains, particularly if they have low income and childcare responsibilities. The level of crime in an area and the general condition of the local area (e.g. litter, graffiti,
anti-social behaviour) is important for feelings of security.
●● Media influences: these can affect purchasing choices through advertising as well as lifestyle and behaviour by influencing what is considered normal or acceptable behaviour (e.g. portrayals of violence and sex).
Health factors●● Genetic factors: these make some individuals
more susceptible to certain diseases, such as breast cancer, or there may be a directly inherited condition that makes periods of ill health more likely, e.g. sickle cell anaemia. Illness has a direct effect on individuals and an indirect effect through missed school and educational achievement or time off work, affecting job security.
●● Accidents and injury: these factors are more likely for people who are fatalistic about their health or indulge in risk-taking behaviour. They can cause long-term ill health and disability.
●● Access to health care: The number of GPs in a particular area and the distance required to travel to receive health care affect health outcomes.
●● Disability: this may have a genetic cause or may be acquired. Nevertheless, disability of any type may have an effect on educational achievement (depending on the type and severity of the disability) and employment chances.
Over time, these influences interact with each other to impact on an individual’s health and overall well-being. The Health Poverty Index (web-based tool) shows how these interact at local level (see APHO, www.apho.org.uk). Many of these influences are rooted in income inequality, which varies across England, with the North having broadly less than the South, which is clear from looking at the Spearhead group.
Key termSocio-economic factors – these include income inequality and are key factors that affect longevity, health and well-being.

20 BTEC Level 3 National Health and Social Care
According to the World Health Organisation, the UK spends a smaller proportion of its income (gross domestic product) on health than Denmark, yet average life expectancy in the UK in 2007 was 80 years compared to 78 years in Denmark. Also, the UK’s health system was rated second out of seven countries for efficiency in a report by the Commonwealth Fund in 2010, behind the Netherlands but in front of Australia, Germany, New Zealand, Canada and the United States.
Did you know... ? Activity 2
Research one of the Spearhead areas and find out the main health issues for people living there. How are they monitored? What are the main factors affecting health in your chosen area?
Compare your findings with another person from your group and identify similarities and differences.
Prepare a presentation to your class identifying two things the government has done in these areas to improve health. How effective do you think they have been? Use statistics to provide evidence for your view.
P3 P4 M2
D1
3 Understand how public health is promoted and protected
AimsThe aims and purpose of public health policy and practice is to develop initiatives that will improve people’s health overall and particularly of those most at risk of ill health, in order to reduce health inequalities and current and future risks to health. Public health policies are developed from health indicators in order to target areas and commu-nities most at risk of ill health and take preventive action.
Health educationThese are initiatives aimed at individuals, groups and communities, intended to encourage and help people to lead healthier lives. Health education programmes will usually look at one aspect of health (e.g. diet, exercise, smoking) and target groups that would benefit most. Examples include: encouraging children to eat more fruit as part of a
‘5 a day’ campaign, research having demonstrated that five portions of fruit and vegetables a day will help to prevent some cancers and heart disease; and helping pregnant women, or those intending to become pregnant, to give up smoking, which is a cause of low birth weight, a risk factor for infant mortality.
It is important that health education programmes do not make people feel guilty about their behaviour, so a number of different approaches have been taken, such as the introduction of health trainers who are specially trained in techniques that help people change their behaviour.
Disease prevention and protectionProtecting the public’s health is the primary responsibility of the Health Protection Agency (HPA), a government agency (www.hpa.org.uk) set up to protect the public from threats to health caused by infectious diseases and environmental hazards, such as Legionnaires’ disease or Weil’s disease. There are plenty of precautions that individuals can take to protect themselves from viruses, bacteria and other transferable diseases,

21Unit 12: Public Health
such as regular hand-washing and making sure you cover your nose and mouth and use disposable tissues when sneezing. The HPA provides infor-mation, advice and guidance to professionals and the public, working at regional and local level, as well as national, to deal with communicable diseases that need to be notified and outbreaks of infectious diseases (e.g. influenza, salmonella). The HPA works with other government depart-ments such as the Department for Environment, Food and Rural Affairs (DEFRA) to ensure that animal diseases don’t pose a threat to human health (e.g. E.coli) and to predict epidemics and take preventive action.
In addition to the HPA, there are a number of specific programmes designed to protect vulnerable sections of the population, such as the Child Health Promotion Programme (see Table 12.5) and the flu vaccination programme. Adult screening programmes are offered for detectable diseases that can be treated; it is unethical to screen for a disease or condition for which there is no effective treatment. Currently, breast and cervical cancer are routinely screened and prostate cancer screening is on request, as is cholesterol and blood pressure, although these will be checked at well man or well woman clinics, run by GPs and practice nurses.
Table 12.5 Child Health Promotion Programme – a universal programme developed as a strategy for improving the health of children from before birth up until secondary school.
Age Intervention
Antenatal Antenatal screening and a preliminary assessment of child and family needs, including past medical history. Advice on breastfeeding and general health and well-being is provided, including healthy eating and help to stop smoking if appropriate. Includes advice on eligibility for welfare foods and maternity benefits. Arrangements put in place to ensure a smooth transition from midwifery to health-visiting service, including the sharing of information.
Post delivery/soon after birth
General physical examination of baby, particularly heart, eyes and hips. Vitamin K injection given (to prevent bleeding as some babies have a deficiency). BCG vaccination given to babies who are at risk of tuberculosis (TB). Hepatitis B vaccine is given to babies who may have been infected by their mother or close family member. Baby weighed and measured for baseline assessment.
5–6 days old Blood spot test for hypothyroidism and phenylketonuria (both metabolic diseases). Screening for sickle cell disease and cystic fibrosis from the same blood spot if baby is at high risk.
Within first month
Newborn hearing test. Second dose of Hepatitis B if baby has already had first. Baby weighed to check feeding progress.
Newborn home visit within 12 days of birth
Midwife or health visitor assesses the child to provide a baseline for future development and assesses the family’s health needs, including identifying any mental health needs (e.g. signs of postnatal depression). Gives ‘Birth to Five’ guidance booklet and Personal Child Health Record to parent. Provides information on key health issues and services available. Gives advice and support on breastfeeding, infant routines, feeding, safety and general care.
6–8 weeks General physical examination of baby, particularly heart, eyes and hips and developmental progress. First immunisations – polio, diphtheria, tetanus, whooping cough (pertussis), Hib (influenza) and meningitis C. General review of progress and key parenting and health messages reinforced. Identification of possible problems (e.g. postnatal depression). Third dose of Hepatitis B at eight weeks if required.

22 BTEC Level 3 National Health and Social Care
Age Intervention
Three months Second set of immunisations against polio, diphtheria, tetanus, whooping cough, Hib and meningitis C. Review of progress and key parenting and health messages, including weaning, e.g. the dangers of early weaning and suitable foods.
Four months Third set of immunisations against polio, diphtheria, tetanus, whooping cough, Hib and meningitis C. Give health promotion advice, check parents concerns and provide general health and well-being advice, especially safety and play.
By first birthday Systematic assessment by the health-visiting team of the child’s physical, emotional and social development, including family needs and action to address these. Agree future contact with service.
13 months Immunisation against measles, mumps and rubella (MMR). Review of general progress and provision of health promotion and general health advice to parents. If Hepatitis B was given, a booster dose and blood test to ensure immunity are given.
2–3 years The health-visiting team is responsible for reviewing the child’s progress and ensuring health and development needs are being addressed. The health visitor exercises professional judgment and agrees with the parents how the review is carried out, e.g. in clinic, at a children’s centre or Sure Start centre, at the GP surgery or at home. Use is made of other contacts with the primary care team.
3–5 years Immunisation against measles, mumps and rubella plus polio, diphtheria, tetanus and whooping cough booster. Review of progress and reinforcement of health messages and parenting advice.
4–5 years A review at school entry provides an opportunity to check that immunisations are up to date, children have access to primary care (GP) and dental care and appropriate interventions are available to address any issues with physical, developmental or emotional problems newly arising, previously missed or not addressed. Information provided to children, parents and school staff about specific health issues. Child’s height and weight checked (BMI calculated), sweep test of hearing administered. Orthoptist-led programme for vision screening carried out. Foundation Stage profile – teacher assessment of: ●● personal, social and emotional development●● communication, language and literacy●● creative development.
Ongoing support in primary and secondary schools
Access to school nursing service through open sessions/drop-in clinics through self-referral or via teachers or parents. Provision for referral to specialists available for children giving cause for concern. Children and young people with additional needs or disabilities may receive nursing care in the school environment depending on their needs.
Secondary school
Heaf test for TB between 10 and 14 years; BCG vaccine given if needed. Tetanus, diphtheria and polio booster given between 13 and 18 years. HPV (human papilloma virus) vaccination for girls between 12 and 13. Check other immunisations are up to date.

23Unit 12: Public Health
Environmental protectionFavourable and less favourable environmental conditions include, for example, river water quality, air quality, green space, habitat favourable to bio-diversity, flood risk, litter and rubbish, housing conditions, road accidents and regulated sites such as landfill and industry. Environmental measures to protect public health include both external (outdoor) and internal hazards. The main types of hazard include:
●● physical hazards, such as the structure of buildings and materials, land use and the quality of air and water, road traffic
●● biological hazards, such as vermin, animal-borne diseases such as anthrax or CJD, poisonous plants and dangerous animals
●● social–environmental hazards, such as noise pollution, littering and graffiti.
Local authorities are responsible not only for reducing environmental harm, but also for contributing to a sustainable economy, which is why they have targets for reducing landfill and have implemented doorstep recycling schemes. Road traffic schemes such as speed limits, traffic calming measures and controlled parking schemes are all aimed at improving the environment by controlling car use to limit the environmental pollution caused by motor vehicles.
Local authorities control housing, planning and building regulations and they have been given targets to encourage ‘affordable housing’ and social housing. This is especially important in places such as London where housing costs are among the highest in the country. Housing costs have a knock-on effect on the overall cost of living
and it is estimated it costs up to one-third more to live in London than anywhere else in the UK. As a result, the Mayor of London has been actively encouraging the idea of a ‘living wage for London’ and getting businesses to sign up to this.
Socio-economic supportFinancial support is provided through welfare benefits to vulnerable people and groups – for example, families on low incomes and disabled people. These benefits have had various names over time – for example, income support and working families tax credit – but essentially the principles remain the same. There are also specific benefits and initiatives designed to reduce child poverty, such as child benefit and the Sure Start programme for children and families. Disabled people and the unemployed are also entitled to financial support. However, the value of these benefits is low so that it does not act as a disin-centive to work. These issues are discussed in more detail in Unit 47: Social Policy for Health and Social Care.
Age Intervention
This schedule is underpinned by a health promotion programme, based on best evidence, focusing on healthy eating, physical activity, safety, smoking, sexual health and mental health. It is delivered by all practitioners who come into contact with children and young people and in all settings used by this age group.
The National Institute for Clinical Excellence (NICE) has estimated that many lives would be saved if major changes were made to processed food, including introducing the ‘traffic light’ system of labelling, which shows the level of fat, sugar and salt in food, and ensuring that low-fat and low-salt foods are cheaper than less healthy versions.
Did you know... ?

24 BTEC Level 3 National Health and Social Care
Activity 3
You are part of the health-visiting team and have called on Suzy to give her advice on keeping healthy during her pregnancy and to tell her of any potential hazards to her health and that of her baby.
Identify one communicable and one non-communicable disease Suzy or her baby may face. Explain how you would promote and protect Suzy’s health. Make a list of the things you need to tell Suzy and advise her how to protect her baby.
You will need to carry out research to identify likely diseases that Suzy or her baby may get and what health services are available to protect their health. You will also need to provide health promotion advice to support Suzy’s pregnancy.
Write a storyboard saying how you approached the task, what advice you gave to Suzy and, using statistical evidence, say how effective the health promotion and health protection measures are.
P5 P6 M3 D2
Case Study
Suzy is expecting her first child. She lives on a farm in a rural area and has two cats as well as an old sheepdog living in the house. She usually helps the dairyman milk the cows in the morning before going off to her part-time job as an administrator at the local village school.
SummaryPublic health is important to governments, groups and individuals. It is as much a matter for social justice as health, since civilised societies should protect the most vulnerable in society.
Responsibility for health is down to individual choices. However, governments and public sector employees have a responsibility to facilitate and encourage people to make healthy choices through legislation, research and planned health education and health promotion initiatives.
Whilst health has improved and life expectancy has increased, inequalities in health remain. The reasons for this are complex and inter-related. However, income inequality is a major determinant of health status. As a result, the NHS, whilst having a role to play, cannot impact on health inequalities without initiatives in other areas, such as the environment, housing and welfare support, which are beyond its remit.

25Unit 12: Public Health
Assessment and grading criteriaIn order to pass this unit, the evidence that the learner presents for assessment needs to
demonstrate that they can meet all the learning outcomes for the unit. The assessment criteria for a pass grade describe the level of achievement required to pass this unit.
To achieve a pass grade the evidence must show that the learner is able to:
To achieve a merit grade the evidence must show that, in addition to the pass criteria, the learner is able to:
To achieve a distinction grade the evidence must show that, in addition to the pass and merit criteria, the learner is able to:
P1 describe key aspects of public health strategies
M1 compare historical and current features of public health
P2 describe the origins of public health policy in the UK from the nineteenth century to the present day
P3 describe current patterns of ill health and how they are monitored
P4 explain the main factors affecting current patterns of health in the UK
M2 discuss the factors likely to influence current and future patterns of health in the UK
D1 evaluate the influence of government on factors that contribute to the current patterns of health and illness in the UK
P5 explain health promotion and protection
M3 assess the different methods that can be used for promoting and protecting public health.
P6 explain appropriate methods of prevention/control for a named communicable and a named non-communicable disease.
D2 evaluate the effectiveness of methods used to promote and protect public health for the two named diseases.

26 BTEC Level 3 National Health and Social Care
Health Services Journal Supplement (2010) Health Intelligence (in partnership with APHO, www.apho.org.uk).
MacInnes, T., Kenway, P. and Parekh, A. (2009) Monitoring Poverty and Social Exclusion, Joseph Rowntree Foundation and the New Policy Institute.
Marmot Review (2010) Fair Society, Healthy Lives. A Strategic Review of Health Inequalities in England post 2010.
Townsend, P. and Davidson, N. (1982) Inequalities in Health: The Black Report 1980, London: Pelican.
Resources