Embed Size (px)
Citation preview

108 CLINICAL RADIOLOGY
there is no doubt that the structure arrowed in Fig. lb is the duodenum. To describe it as an inflammatory mass is unkind in the extreme. I do hope that the authors can be persuaded to retract this libellous comment; if they decide to plead guilty they may also wish for a similar but less clear cut offence (Fig. 4) to be taken into account.
P. J. ROBINSON St James's University Hospital Leeds
diatrizoate) during an IV-DSA examination. The patient, a previously healthy adult male with no history of allergy or of hypersensitivity to iodinated contrast, underwent an IV-DSA examination in order to demonstrate the carotid arterial ana tomy following a bullet injury to the neck. A 5 French high-flow pigtail catheter was placed in the right atrium and the position checked by the injection of 4 ml of contrast medium. Following this injection he had no complaints but 10 min later, immediately after injecting the first bolus of Urografin 76 % (25 ml at 20 ml/s), he complained of a pulsating sensation in the left eye and soon afterwards was noted to have developed oedema of the left orbit. There was no skin rash. He also complained of a dry cough but had no respiratory difficulty. Examination revealed a regular, good volume radial pulse, a blood pressure of 120/80 mmHg, and normal chest and heart sounds. He was treated with intravenous hydrocortisone and phenylamine malleate and the study was abandoned. The orbital oedema had disappeared 6 h later.
Adverse reactions to intravascular contrast media occur in approxi- mately 5% of patients and are probably not related to the age, sex or weight of the patient except for a slight variance in the lower age and weight groups (Shehadi and Toniolo, 1980). The majority are minor reactions and usually subside without treatment (Lodge and Steiner, 1975). Although a wide variety of contrast-induced adverse reactions have been described (Lodge and Steiner, 1975; Shehadi and Toniolo, 1980; Shehadi 1982), we found no previous report of isolated unilateral orbital oedema following the intravascular injection of iodinated contrast medium. In our patient oedema was certainly related to the contrast administration as it appeared immediately after the injection and was probably an allergic response as it responded well to treatment with steroid and anti-histamine.
S. S H A R M A S. A G G A R W A L
Department of Radio-diagnosis All India Institute of Medical Sciences
New Delhi India
References
Lodge, T & Steiner, RE (1975). Recent Advances in Radiology, pp 340. Churchill Livingstone, New York,
Shehadi, WH (1982). Contrast media adverse reactions: Occurrence, recurrence and distribution patterns. Radiology 143, 11 17.
Shehadi, WH & Toniolo, G (1980). Adverse reactions to contrast media. Radiology, 137, 299 302.
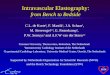
Fig. I - (a) Post-contrast CT scan through the lower part of the kidneys discloses contrast leak within the left perirenal space (arrows) extending towards the midline anterior to the aorta (A). V, Inferior vena cava. (b) CT scan 7 cm below (a) discloses continued downward extension of contrast leak into the retroperitoneal space (arrows) anterior to the left psoas muscle. This space is not the perirenal space as the lower pole of the left kidney is 6 cm above this level. C, Descending colon; U, Left ureter.
References
Fitzgerald, EJ & Blackett, RL (1988). ' Inf lammatory ' abdominal aortic aneurysms. Clinical Radiology 39, 247-25 l.
SIR - I am grateful to Dr Robinson for his interest in and comments on the paper on inflammatory aneurysms. If guilty the charge should be of diagnosis by serendipity or of judging the duodenum by the company he(she) kept, as there was an inflammatory mass involving the duodenum, proximal aorta and inferior vena cava present at surgery in this patient. As regards the second charge, this scan was taken about 6 cm below where the duodenum was clearly seen to cross the midline; the mass continued in a caudal direction for a further 4 cm.
Again I would like to thank Dr. Robinson for his comments particularly in pointing out the error in Fig. lb.
E. J. F I T Z G E R A L D St James's Hospital Dublin
UNILATERAL ORBITAL O E D E M A F O L L O W I N G THE INTRAVASCULAR INJECTION OF C O N T R A S T M E D I U M
SIR We recently witnessed an unusual adverse reaction following intravascular injection of Urografin 76% (Sodium and meglumine
RELAPSING P O L Y C H O N D R I T I S
SIR- We read with interest the recent paper by Crockford and Kerr (1988), reporting their experience with four cases of relapsing polychon- dritis (RP).
Coincidental with publication of their cases, we had the opportunity to investigate a patient with RP. A 14-year-old schoolgirl presented with a 2-month history of illness and over the course of 6 months exhibited features of recurrent polychondritis of both ears, which was biopsy proven, polychondritis of nasal cartilages, inflammation of ocular structures (episcleritis) and cochlear/vestibular damage with complex neurosensory loss.
In addition, and most worryingly, she has more recently complained of hoarseness. As Crockford and Kerr (1988) emphasised in their paper, respiratory tract involvement is the main cause of death from RP and larger studies have in the past recommended that the search for possible respiratory tract involvement should be made at regular intervals in all affected patients. Serial tracheal tomography and contrast pharyngo- tracheograms have been suggested (McAdam et al., 1976).
With the wider availability of computed tomographic scanning facilities, the next question must be the place of computed tomography in this follow-up. It has been claimed that CT is a safe and accurate method for assessment of the upper airways (Mendelson et al., 1985). However, we would like to emphasise the limitations of CT, particularly in the assessment of short segment stenoses which can occur in this condition. Such stenoses can go completely undetected and CT is more likely to be inaccurate at predicting stricture length.
We agree with Crockford and Kerr (1988) that good quality radiographs and conventional tomograms should remain the imaging techniques of choice.
G. N E E D H A M E. M. ROBERTSON
Aberdeen Royal Infirmary Foresthill Aberdeen