Embed Size (px)
Citation preview

Understanding Success and FailureHealing vs. Persistent Pathosis
by David B. Rosenberg, DDS, FICD, FACD

Why retreat?
Implants have eliminated the need for nonsurgicalendodontic retreatment.
Implants have eliminated the need for apicoectomies.
As the saying goes, “if you only have a hammer,everything is a nail.”
As endodontists we have a complete set of tools,along with the knowledge and experience to use themto our patient’s advantage. We perform osseous sur-gery, soft tissue surgery, and internal nonsurgicalrestorative endodontic procedures. If we need to puta post in a tooth we can do that. If we need to put atitanium post in the bone we can do that also.
So why retreat a tooth? If it is in the patient’s bestinterests why not retreat it? Unless retreatment is aservice that one can not provide.
In deciding whether to extract or retain a tooth whois more qualified than an endodontist? Endodontistssuccessfully treat teeth that other practitioners con-demn. Only endodontists have the skills and experi-ence necessary for successful endodontic treatmentof complex cases. If the only treatment option adentist or dental specialist can offer requires extract-ing the tooth, is the patient being offered a treatmentplan in their best interests or the providers?
Of course the converse is also true. If the only ser-vice you can offer for a failing tooth is a heroic at-tempt at retreatment, are you able to provide for thepatients best interests? Not every tooth should havean attempt made at saving it when more predictableoptions exist.
Endodontists perform some of the most complexdental procedures. From conventional endo wherewe work within _ to 1/2mm tolerances, to placingretrogrades in roots near vital structures in smallspaces with challenging access requirements. Re-placing a tooth with a titanium screw is a lot lesscomplicated than providing an endodontic service.
The specialty of endodontics is fortunate to be ableto offer our patients the best that dentistry can pro-vide for them. We can predictably save teeth, andwithout any conflict of interest provide implant ser-vices when appropriate. No other branch of den-tistry can make this claim.
When considering endodontic treatment orretreatment versus an extraction some factors to con-sider include:Is the tooth restorable?
What function does this tooth provide?
What is the expected functional lifetime of the re-sultant restoration?
Are the patient’s desires and expectations realistic?What are the number, types, and duration of the pro-cedures required?
What are the surgical risks and potential complica-tions?
Of course no treatment can claim 100% success.Endodontics has its limitations. Vertically fracturedroots, nonrestorable teeth, and hopeless periodontalyinvolved teeth should be extracted. Teeth that if re-tained may interfere with long term outcomes shouldalso be removed even if they can be treated. Anexample of this would be trying to save a singlemandibular incisor where implants are being usedto restore the mandibular dentition.
Implants also have their limitations. Treatment in theesthetic zone (the esthetic zone being wherever thepatient says it is) is a major concern. Often the im-plant site needs to be developed with bone, or softtissue grafting for optimal esthetic results. Withouta good recipient site for the implant, esthetics willbe compromised.
Implants used to restore adjacent tooth extractionsites often present an esthetic challenge. Estheticresults are significantly related to preservation of thepapilla and its supporting bone. The papilla is present
Retreatment: Why and When

when the interproximal crest of alveolar bone ex-ists. This alveolar bone is resorbed when adjacentteeth are missing. Between adjacent implants thereis often no interproximal crest of alveolar bone thatprovides for the scalloped appearance of the peri-odontal tissues that form a papilla. Natural rootscan have an esthetic advantage due to their ability topreserve the natural papilla.
Rationale for RetreatmentWhen considering treating teeth with failing endo-dontic therapy, several options exist. They includeendodontic surgery, extraction, no treatment, or en-dodontic retreatment.
The patient’s chief complaint needs to be investi-gated. Postendodontic treatment complaints mayinclude, sensitivity to; temperature, biting, pressure,palpation, and recurrent sinus tracts.
When a patient complains of temperature sensitiv-ity after endodontic therapy, their complaint is oftendismissed. Thermal testing should be performed tosee if their complaint is reproduced. If it is the endo-dontic treated tooth that responds, the presence ofuntreated pulp is suspected.
When an endodontic treated and restored tooth thathas been asymptomatic for years begins to becomesensitive to biting, pressure, or palpation, endodon-tic failure should be suspected. This is especially trueif no recent dentistry or trauma has taken place. Oc-clusal adjustment and antibiotics will temporarilyabate the symptoms but they will usually return re-peatedly. As with virgin teeth exhibiting these symp-toms an endodontic abscess should be suspected.(Figures 1, 2)
Patients are often aware of a “gum boil” that comesand goes. When presenting for an exam the sinustract may be difficult to see. Palpation in an apicalto coronal direction on the buccal and lingual mayresult in exudate being expressed through the mu-cosa. The sinus tract may now be traced to its source.
Evaluation of the Existing Treatment: Radiographinterpretation in evaluation for retreatmentWhen retreatment is being considered the quality ofthe previous endodontic therapy and subsequent res-
toration must also be evaluated. This is a subjectiveevaluation based in part on experience.
A thorough radiographic examination can makeevaluation of existing conditions more objective.Radiographs angulated from the mesial and distal,as well as straight on, are needed. Furcations can beevaluated with a bitewing film. The bitewing filmscan also be taken from more coronal and apical di-rections. These different angles can help identifymissed canals, fractures, perforations, while alsoevaluating the quality of the existing endodontics.
Most causes of endodontic failure are related to con-taminated root canal spaces. There are several cat-egories of endodontic failure for which retreatmentis promising. They include:� Missed canals (Figures 3, 4)� Incomplete obturation (Figures 5, 6, 7)� Perforations (Figures 8, 9)� Coronal leakage (Figures 10, 11)
Missed CanalsAngled radiographs can show missed canals in sev-eral ways:� By observing that the obturation is not centered
in the canal. Since the root forms around thecentrally located pulp, an eccentrically locatedobturation may indicate additional untreated ca-nal space. (Figures 12, 13)
� Observing the radiographic apex having a bi-convex shape. Maxillary molar MB roots andmandibular molar distal roots with two canalsoften exhibit this anatomical marker. (Figures14, 15, 16)
� Angled radiographs project superimposed rootsonto the film as described with the cone shiftrule, also called the buccal object rule, or theSLOB rule. The result of angling the radiographis the identification of these otherwise superim-posed roots. (Figures 17, 18)
Incomplete ObturationIncomplete obturation is suspected when radiographsshow:� The radiopacity of the obturation is similar to
dentin. When pulpal and dentinal debris are left

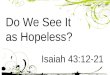
Figure 3 The second premolar has aradiolucency that extends from theapex to the CEJ along the distal rootsurface.
Figure 4 This tooth was found to havethree separate canals.
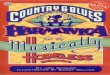
Figures 5-7 Without the use of the surgical operating microscope, retreatment of this central incisor would be extremely difficult.With the microscope the apical bifurcation can be seen and managed.
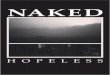
Figure 1 Upon a quick inspection theendodontics in the first molar appearsadequate to outstanding. The patientwas persistently symptomatic.
Figure 2 The patient’s symptoms wererelieved after retreatment of thepreviously under-treated canals, andtreatment of a previously missedsecond MB canal. Almost all maxillarymolars have four canals.

Figure 10 Endodontic surgery hasfailed to resolve this extensivelytreated first molar. The margins on thecrown are suspect. The leaking crownneeds to be addressed if endodonticretreatment is to succeed.
Figure 11 Healing has occurred afterpost removal, silver point removal,gutta percha removal, endodonticretreatment, and a new crown.
Figure 8-9 A perforation with no communication to the oral cavity has a goodprognosis today. The post was removed and the perforation was repaired with MTA.A new post and crown were placed and healing has occurred.
Figure 12-13 The obturation of the MB root on this first molar is eccentricallypositioned. When the root was retreated, a second MB canal was found.

Figure 14-16 This first premolar case illustrates the value of multiple angled preoperative views and the significance of lateralcanals. The outline of a second untreated canal can be seen on the second view. After the silver point is removed and the toothretreated, the anatomical complexity of this root canal is revealed.
Figure 17 The radiograph of thelateral incisor reveals a deep concavityon the root surface. The presence ofthis concavity is often indicative ofmultiple canals within the root.
Figure 18 The presence of two canalsis demonstrated on the postoperativeradiograph.
Figure 19 Indistinct obturation asseen in this molar is cause forconcern. After the crown was placed,symptoms developed, necessitatingendodontic retreatement.
Figure 20-21 The original treatment terminated at a ledge that was created when the original path of the canal was not followed.Upon retreatment the ledge was bypassed, allowing access and treatment of the original canal, which terminates with its foramencentrally located in the periapical radiolucency.

in the canal during obturation, the volume thatthe more radiopaque obturation materials canoccupy is limited. The result is a diminished ra-diopacity of the obturated canal.
� The radiopacity of the obturation becomes lessdistinct in an apical direction. This is anotherindication that significant debris may remain inthe canal. (Figure 19)
� The obturation does not reach the PDL. Mesial,distal, and straight on radiographs will show themost apical obturation level. If none of the ra-diographs show obturation to the PDL it is rea-sonable to assume that the obturation is short ofthe cavosurface of the canal. (Figures 20, 21)
� A vertical void (a black line) visible betweenthe obturation material and the canal wall. Thecanal may be filled in terms of length, but in-completely filled in three dimensions. This blackline could also indicate a vertical fracture.
� Evidence of endodontic surgery without retro-grade placement
� Evidence of endodontic surgery with retrogradeplacement in the root, but not the canal. (Figure22)
� The obturation does not seem to follow the curveof the root, or terminate in the center of the ra-diolucency. This could indicate a ledge or per-foration. (Again, see Figures 20, 21)
� The presence of silver points.
� The presence of separated instruments.
PerforationsPerforations create areas of persistent inflammation,and resolution of perforations depends to a largeextent on where they are located. The amount ofsupportive tooth structure remaining is also a criti-cal factor in the long-term success or failure of per-foration repair efforts.
Perforations should be suspected when radiographsreveal:� A radiolucency at the apical extent of a post.
� A furcal radiolucency exists adjacent to mini-mally remaining furcal tooth structure.
� A sinus tract that traces to the furcation, or tothe mid root area where the external root sur-face is concave (a strip perforation).
The Coronal SealThe quality of the coronal seal can be evaluated ra-diographically by examining for the following, asthey can provide avenues for micro leakage:� Open margins
� Recurrent decay
� Voids parallel to posts
If the etiology of the failure can be assigned to oneof these four categories there is reason to exploreretreatment as an option for the patient.
Root FracturesFractures also create areas of persistent inflamma-tion that may necessitate extraction. Fractures areoften difficult to see on radiographs. Sometimes theirpresence is indicated when radiographs show:� A vertical black line between the obturation
material and the root
� A “halo” shaped radiolucency surrounding aroot. (Not the typical circumscribed radiolucencyassociated with a chronic apical abscess.)
� Changing the vertical angulation of the centralray may allow detection of horizontal fractures(usually caused by trauma). A radiograph shouldbe taken at a right angle to the long axis of theroot, along with two additional views, one at 45degrees toward the apex and one at 45 degreestoward the crown.

Figure 22 These retrogrades may haveesthetic value but are not sealing thecanals, as evidenced by the filesextending past them.
Figure 23 The preoperative radio-graph of the second premolar sug-gested the presence of a vertical rootfracture on the distal side of the root.
Figure 24 The apex locator readingswere suggestive of a perforation orfracture. The radiograph shows the filein the fracture line. Irrigating this withNaOCl would have been a majoriatrogenic mistake. When the apexlocator reading is aberrant, investigatethe cause before proceeding.
Figure 25 The second molar has silverpoints perforating both mesial canals.The first molar is fractured through thefurcation and decayed. The patient hasbeen asymptomatic for more than 20years. Regaining access to the calcifiedmesial canals apical to the perforationis a challenge. Surgery or extractionare more predictable treatment optionsfor the second molar.

The Clinical ExamThe Coronal SealThe integrity of the coronal restoration needs to beevaluated clinically and visually, as coronal leakageis a factor in endodontic failure.
Open margins on coronal restorations can be revealedby the production of bubbles when apical pressureis applied to the occlusal surface. Use of an explorerand mobility testing is also required.
Periodontal Evaluation.Periodontal disease may be misdiagnosed as an en-dodontic failure. The opposite is also true. The clini-cal exam needs to include periodontal probing of theentire tooth including any furcations. Ideally theentire quadrant should be probed. When the generalperiodontal health is good, finding an isolated deepperiodontal defect that is narrow in a horizontal di-rection may actually be a draining sinus tract. Peri-odontal defects that are wider coronally than apicalyare more indicative of fractures or periodontal pa-thosis.
PerforationsPerforations that can be probed through the sulcushave an unfavorable prognosis. This is because re-attachment of the periodontal fibers and regenera-tion of the alveolar bone is compromised. Due tosalivary contamination a persistent supraosseous,subgingival inflamed pocket will remain.
Perforations that are in 5 or 6 walled bony defectshave an excellent prognosis when repaired withMTA.
Fracture IdentificationFiber optic transillumination when applicable is anexcellent diagnostic aide for fracture identification.A fracture is indicated when the light transmissionis halted at a darkened interface. This interface iswhere the fracture line exists. Crowns and large res-torations can limit the usefulness of fiber optic tran-sillumination.
Staining with a dye such as methylene blue will alsohelp elucidate the fracture. The stain can be used inconjunction with transillumination. When the tooth
is extensively restored, the dye can be placed in thegingival sulcus. A spoon excavator or similar instru-ment may than be used to reflect the soft tissue awayfrom the root. The root can be examined for a frac-ture with magnification and fiber optics.
Apex locator readings that are aberrantly short shouldbe compared with a measurement film. The apexlocator reading could be due to a fracture or perfora-tion. (Figures 23, 24)
Observation of multiple sinus tracts that trace to thesame root often occurs when the fracture separatesthe root in half, creating buccal and lingual sinustracts.
Past History of the ToothInformation on the technique used during the initialendodontic treatment may be difficult to obtain. Itcould be useful to know if irrigants were used. Thetype of irrigants and how they were used could alsobe useful. The importance of using NaOCl and EDTAto produce as clean a canal as possible has been wellestablished. If a less than ideal protocol was fol-lowed during the original treatment, retreatment mayresult in healing.
PrognosisWhen all the information required to diagnose theetiology of the endodontic failure is analyzed a prog-nosis for retreatment can be offered.
A Poor prognosis is given for:� Vertical root fractures with probing depths that
are markedly greater than immediately adjacentsites. This indicates that the fracture, in additionto being subgingival extends infraosseously. Thisbone is expected to eventually be lost due tobacterial infection of the fracture.
� Furcation perforations with a sulcular commu-nication.
� Apical third perforations in roots with abruptapical curvature. It can be very difficult to re-enter the natural canal to complete the endodon-tics in this situation. Surgery is usually a morepredictable approach here. (Figure 25)

A Good prognosis can be given failures with an eti-ology of:� Separated instruments
� Silver points
� Perforations coronal to the periodontal attach-ment
� Root perforations in the coronal to middle thirdwithout sulcular communication (5 or 6 walleddefects)
� Apicoectomies without retrogrades placed
� Retrogrades placed in the root but not in the ca-nal
� Missed canals
� Incomplete obturation
� Coronal leakage
Deciding Upon Endodontic RetreatmentAs described previously, there are several factors thatmake endodontic retreatment the preferred methodfor treating endodontic failures, they include:
� When the natural root and the bone it preservesis the best option.
� When the decision is made to retain the tooth,retreatment addresses more of the apicalanatomy than surgery.
� Infraosseous perforations that don’t communi-cate through the sulcus can be addressed in amore conservative fashion from a coronal ap-proach than a surgical approach.
When discussing a comprehensive treatment plan,patients should be made aware of the status of theirexisting endodontic treatments. Asymptomatic teethwith questionable endodontics should be consideredfor retreatment prior to completion of their compre-hensive treatment plan. Before proceeding withretreatment, the potential need for additional proce-dures needs to be assessed. New restorations, crownlengthening or other periodontal needs should beexplained to the patient in order for an informeddecision to be made. When pre-existing endodonticpathosis or teeth with questionable endodontic treat-ment become symptomatic shortly after overall treat-ment has been completed, patient doctor relationscan be strained. This is especially true if the patientswere not informed ahead of time of the findings fromtheir comprehensive exams.