Embed Size (px)
Citation preview

Journal of Neuroimaging Vol 14 No 2 April 2004Alexandrov et al:CLOTBUST: Phase I Data
Ultrasound-Enhanced Thrombolysisfor Acute Ischemic Stroke:Phase I. Findings ofthe CLOTBUST Trial
Andrei V. Alexandrov, MD
Andrew M. Demchuk, MD, FRCPC
W. Scott Burgin, MD
David J. Robinson, MD
James C. Grotta, MD
for the CLOTBUST Investigators
A B S T R A C T
Background. Tissue plasminogen activator (TPA) activity maybe enhanced with ultrasound, potentially 2 MHz transcranialDoppler (TCD). The authors present Phase I data of theCLOTBUST (Combined Lysis of Thrombus in Brain ischemiausing transcranial Ultrasound and Systemic TPA). Subjects andMethods. Nonrandomized stroke patients with proximal arterialocclusion on a prebolus TCD receiving intravenous 0.9 mg/kgTPA within 3 hours after stroke onset were monitored with por-table diagnostic TCD equipment and a standard headframe.Complete recanalization was defined as thrombolysis in brainischemia (TIBI) flow grades 4-5. Results. 55 patients (mean age69 ± 15 years, median baseline NIH Stroke Scale [NIHSS] 18,range 4–29, 90% with ³ 9 points) were treated at 125 ± 36 min-utes from symptom onset. TCD monitoring began at 117 ± 39minutes. Complete recanalization on TCD within 2 hours afterbolus was found in 20 patients (36%). Dramatic recovery(NIHSS score ≤ 3) occurred in 20% at 2 hours and in 24% at 24hours. Overall improvement by ≥ 4 NIHSS points was found in49% at 24 hours. Improvement was associated withrecanalization during or shortly after TPA infusion (Φ r2 = .5, P =.03); however, in 6/20 patients with complete recanalization(30%), no immediate clinical change was noticed within 2 hours.Overall symptomatic hemorrhage rate was 5.5%. Conclusions.Continuous TCD insonation for up to 2 hours at maximum inten-sities allowed by current bio-safety guidelines is safe. Dramatic
recovery and complete recanalization shortly after TPA bolusare feasible goals for thrombolysis given with TCD monitoring.
Key words: TPA, transcranial Doppler, stroke, outcomes
Alexandrov AV, Demchuk AM,Burgin WS, Robinson DJ, Grotta JC.
Ultrasound enhanced thrombolysis for acute ischemicstroke: phase I. findings of the CLOTBUST trial.
J Neuroimaging 2004;14:113-117DOI: 10.1177/1051228403261462
Patients with myocardial ischemia had pain relief andchanges on ECG during thrombolytic therapy. However,early clinical improvement after ischemic stroke has notbeen demonstrated in pilot clinical studies1 and in subse-quent trials of tissue plasminogen activator (TPA) withprespecified end-points.2 The lack of early benefit fromthrombolysis and the increased risk of hemorrhage leadto skepticism toward its use in stroke patients.3
Arterial recanalization precedes early improvement instroke patients4-7; however, recanalization was measuredonly in a pilot angiographic study of TPA therapy forstroke1 but not in the NINDS rt-PA Stroke Study.2 A posthoc analysis of the NINDS trial showed that by 24 hours,27% of TPA-treated patients improved by ≥ 10 points onthe National Institutes of Health Stroke Scale (NIHSS) orresolved their neurological deficit completely comparedto 12% in the placebo group (P = .002).3 Since earlyrecanalization can lead to dramatic recovery,4-7 any addi-tional enhancement of TPA-associated thrombus dissolu-tion, in theory, should produce even higher early recov-ery rates among patients with ischemic stroke.
Enhancement of thrombolysis with externally appliedultrasound has been proposed previously8,9 and con-firmed by many in experimental models.10-14 Althoughlow KHz frequencies may better potentiate TPA effects,15
these systems have safety concerns for clinical practiceand are unable to diagnose assessment of cerebral vesselsusing this frequency/wavelength range. Meanwhile, 1–
Copyright © 2004 by the American Society of Neuroimaging 113
Received May 13, 2003, and in revised form July 30,2003. Accepted for publication September 10, 2003.
From the Center for Noninvasive Brain Perfusion Studies,Stroke Treatment Team, The University of Texas-Hous-ton Medical School, Houston, TX; Department of Clini-cal Neurosciences, University of Calgary, Alberta,Canada; Department of Neurology, University of Roch-ester, Rochester, NY; Department of Emergency Medi-cine, The University of Texas-Houston Medical School,Houston, TX.
Address correspondence to Dr A. Alexandrov, MSB7.044 6431 Fannin St, University of Texas, Houston, TX77030. E-mail: [email protected].

2.2 MHz frequencies can also enhance TPA-inducedthrombus dissolution,16-17 and this frequency range issafely used for diagnostic and monitoring procedures.
Physicians involved in evaluation of stroke patientscan efficiently use portable diagnostic ultrasound equip-ment in the emergency room.18 With prior training andexperience in interpretation of transcranial Doppler(TCD) studies, this test can yield high degrees of accuracyfor rapid bedside detection and localization of arterialocclusion as well as continuous assessment of recanaliza-tion process.19-20 Moreover, a relatively narrow ultra-sound beam can be steadily focused at presumed intra-cranial thrombus location, and arterial recanalization canbe monitored in real time.18 Even though 2 MHz fre-quency and power settings of standard TCD monitoringcan only transmit low amounts of energy through theskull, we have observed higher early recanalization anddramatic recovery rates18 than could have been expectedfrom the pilot study and a post hoc analysis of thrombo-lytic trials.1-3 This nonrandomized study of patientstreated with different TPA doses18 suggested potentialtherapeutic effect of TCD, subject to a prospective ran-domized trial. We previously reported findings in 30patients treated with 0.9 mg dose of TPA,18 and these datawere included in the extended study presented below. Toavoid errors associated with small numbers of patients,we extended pilot phase I observations in patients treatedwith standard 0.9 mg/kg TPA dose to demonstrate safetyof TCD monitoring and to assess rates of early arterialrecanalization and dramatic recovery.
Subjects and Methods
A pilot phase I of the CLOTBUST (combined lysis ofthrombus in brain ischemia using transcranial ultrasoundand systemic TPA) trial included consecutive patientswho were treated with intravenous TPA and receivedcontinuous TCD monitoring between 01/99 and 09/00.TPA was given in a standard 0.9 mg/kg dose (10% bolus,90% continuous infusion over 1 hour) to patients present-ing within the first 3 hours after symptom onset. Ourmultidisciplinary stroke treatment team routinely per-forms diagnostic TCD examination in the emergencyroom before TPA bolus. The CLOTBUST proceduresare performed under informed consent MSC-MS-00-107approved by the local ethics committee, the University ofTexas Committee for Protection of Human Subjects. Weused a single channel portable unit (Multigon 500M, Yon-kers, NY; EZ-Dop, MultiDop-T, DWL, Sterling, VA). AsTCD testing can be interrupted to perform CT scan orchest x-ray, no delay in TPA administration was experi-
enced as a result of the ultrasound examination at bedsideand obtaining informed consent.
TCD was used to identify the site of intracranial occlu-sion following previously published and validated diag-nostic criteria.19 Once the occlusion was diagnosed byhandheld examination, the presumed thrombus locationand residual flow around it was determined by the pres-ence of abnormal flow signals (minimal, blunted, ordampened waveforms).19,20
The sample volume (gate) was set at 11.8 mm(Multigon) or 15 mm (DWL). The power was set at a 100%level (Multigon) or ≥ 128 mW (DWL) for the duration ofmonitoring. For patients with MCA occlusion, the probeposition was tightly fixed using a standard headframe(Marc series, Spencer Technologies, Seattle, WA) to maxi-mize sound energy transmission and to maintain a con-stant angle of insonation. If the basilar artery wasoccluded, handheld monitoring was performed via thetransforaminal window.
TCD monitoring was performed during the entire TPAinfusion under direct visual control of the investigators.Any flow signal changes were interpreted in real time, andthe timing of change was documented. The flow signalswere documented at the end of TPA infusion in allpatients, and TCD monitoring was extended up to 2 hourswhen feasible to determine if recanalization continues upto 2 hours after TPA bolus. TCD monitoring was contin-ued for specified time intervals whether recanalizationoccurred or not.
Recanalization was graded on TCD as complete, par-tial, or none using previously validated classification pre-dictive of the thrombolysis in myocardial ischemia(TIMI) flow grades at angiography. Specific TCD flowfindings were previously validated in our laboratory forthis purpose.20 Complete recanalization was diagnosedwhen a normal waveform or a low resistance stenotic sig-nal appeared at the selected depth of insonation, suggest-ing low resistance in distal circulatory bed that correlateswith unobstructed passage of contrast (TIMI grade IIIflow). If the abnormal signals (high resistance dampenedsignals or flattening of systolic upstroke with “blunted”waveform) were still seen at the distal portion, partialrecanalization was diagnosed (TIMI grade II flow equiva-lent). No change in the abnormal flow signals indicatedthat no recanalization has occurred with minimal flow sig-nal or absent flow corresponding to TIMI grades 0-I. OurTCD criteria for thrombolysis in the middle cerebralartery (MCA) to predict TIMI grade III recanalization onangiography had 91% sensitivity and 93% specificity.20
The NIHSS scores were obtained before and afterTPA infusion by a neurologist not involved in TCD. Out-
114 Journal of Neuroimaging Vol 14 No 2 April 2004

come measurements included the NIHSS scores at 2hours after TPA bolus, and at 24 hours. We used the fol-lowing measures of clinical recovery reported in previousstudies.2-4 “Recovery” was defined as decrease of the totalNIHSS score to 3 points within 2 hours after TPA bolus.4
“Improvement” was defined as reduction by 10 points inthe total NIHSS score.3 The NIHSS scores are reportedfor 2 hours after TPA bolus and 24 hours after symptomsonset. Statistical analysis included the Phi test to establishan association between recanalization and clinicalrecovery.
Results
We screened a total of 75 acute stroke patients: 5 were ex-cluded because they had no temporal window for trans-cranial insonation, 5 patients had no proximalintracranial arterial occlusion on pre-TPA TCD, and 10presented outside of the conventional 3-hour window forTPA.
The remaining 55 patients were treated within the first3 hours after stroke onset, and all of them had an occlu-sion on pre-TPA TCD. Occlusions were located in the M2MCA in 12/55 (21.8%), M1 MCA in 26/55 (47.2%), com-bined MCA/ICA in 9/55 (16.4%), TICA in 4/55 (7.3%),and in the vertebro-basilar system in 4/55 (7.3%) patients.The mean age was 68 ± 15 years, median baseline NIHSSscore was 18 (range 4–29), and 49 patients (89%) hadNIHSS score ≥ 10 points. The TPA bolus was given at 125± 36 minutes from symptom onset.
TCD monitoring started at 117 ± 39 minutes, continuedfor the duration of TPA infusion in all patients, andextended up to 2 hours in 13 patients. The cumulative rateof complete recanalization on TCD during the first 2hours after bolus was observed in 20 patients (36%).
Recovery to the total NIHSS score of ≤ 3 pointsoccurred in 11 (20%) of the patients at the end of TPA infu-sion. At 24 hours, this degree of recovery was seen in 13(24%) of the patients (Table 1). Improvement by ≥ 10NIHSS points was found in an additional 4 (7%) patientsat 2 hours and 4 (7%) patients at 24 hours (Table 1). Thisrecovery or improvement occurred during TPA infusionin 13 of these 17 patients (76%), and in 2 additionalpatients during the second hour after TPA bolus (15/17, or88%). Finally, 2 more patients had recovered to the totalNIHSS score of ≤ 3 points between 2 and 24 hours (Fig-ure 1). Of 24 patients with NIHSS scores ≤ 8 at 24 hours,22 (92%) patients achieved this score by 2 hours afterbolus.
Overall improvement by ≥ 4 NIHSS points was foundin 49% at 24 hours. This improvement was associatedwith complete recanalization during or shortly after TPAinfusion (Φ r2 = .5, P = .03). However, 6 of 20 patients(30%) had recanalization during or shortly after TPA infu-sion without any clinical improvement within 24 hours.
Three patients suffered symptomatic intracerebralhemorrhage (overall rate of 5.5%), and all of these 3patients died during their hospital stay. One patient had ahemorrhagic transformation without progression of thebaseline neurological deficit (NIHSS 13 points on admis-sion and at 72 hours).
Discussion
Our study showed that continuous monitoring for 2 hoursusing standard TCD equipment set at maximum allow-able intensities is safe and does not lead to increasedintracranial hemorrhage rates. Furthermore, our datasuggest that complete recanalization, clinical recovery, orsignificant improvement within 2 hours of TPA therapyare feasible goals when TPA infusion is monitored with 2MHz pulsed wave ultrasound. We confirmed observa-
Alexandrov et al: CLOTBUST: Phase I Data 115
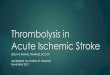
Table 1. Neurological Improvement and Recanalization in Pa-tients Treated With 0.9 mg/kg Dose TPA and Moni-tored With 2 MHz TCD
TPA Dose 0.9 mg/kg (n = 55)
End-Points End of TPA Infusion At 24 Hours
Recovery (to the totalNIHSS score of ≤ 3 points) 20% 24%
Improvement(by ≥ 10 NIHSS points) 7% 7%
Complete recanalization 36% n/aCombined: CompleteRecanalization + Recovery +Improvement 42% n/a
Note that 12 of 15 patients with recovery or improvement also had earlycomplete recanalization.
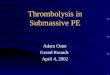
0% 20% 40% 60% 80% 100%
24 hrs
2 hrs
Pre-TPA
3 or less4 to 910 or more
Fig 1. NIHSS scores in nonrandomized patients treatedwith a 0.9 mg/kg dose TPA and monitored with 2 MHz TCD.

tions from our small pilot study18 that as many as 36% ofpatients had early and complete (TIMI grade III equiva-lent) recanalization leading to dramatic improvement intwo thirds of these patients. Early recovery and improve-ment occurred in 27% of all patients during or shortly af-ter treatment with 0.9 mg/kg TPA dose, and thisimprovement accounted for most of the clinical recoveryseen at 24 hours (total 31% of patients). The absolute dif-ference between our results and those seen in theNINDS-rtPA Stroke Study3 is only 4%. However, our pa-tients had more severe strokes prior to treatment (medianpretreatment NIHSS 18 vs 14), and patients with lacunarstrokes (who benefit most in the NINDS trial) were ex-cluded from our present study. These results support ourhypothesis that 2 MHz TCD monitoring may betherapeutically active.
A total of 15% of patients experienced recanalizationduring TPA infusion that could not be detected clinically.Favorable outcome (NIHSS 0-1 points at 3 months) wasfound in 37% of another cohort of similarly treatedpatients,21 and the possibility of ischemic brain stunning isa subject of another study. The end-point of completerecanalization on TCD has not been tested in a trial with-out angiographic control. Early complete recanalizationon TCD represents the primary end-point that maydirectly reflect ultrasound enhancement of thrombolysis.A 36% rate of complete recanalization in our study dose is10% higher than the rate demonstrated by del Zoppo etal.1 In contradistinction to del Zoppo et al, we excludedpartial recanalization (defined by TCD) as an endpoint forour analysis since these criteria do not have balanced sen-sitivity and specificity compared to complete recanali-zation on TCD.20 When compared to angiography, ourcriteria for complete recanalization on TCD have sensitiv-ity of 91% and specificity of 93%. Therefore, in the pres-ence of clear temporal windows, these criteria allow reli-able assessment of complete MCA recanalization inprospective studies. Since only 13 patients were moni-tored up to 2 hours, recanalization rates may be evenhigher if monitoring time is consistently extended tocover maximum TPA activity at the thrombus that occursin 90 minutes.
Most occlusions spontaneously lyse at a rate of approx-imately 6% per hour without TPA,22 and about 10% to15% per hour with TPA after its infusion.23 Delayedrecanalization may not lead to immediate clinicalimprovement23 and may also be harmful due to increasedrisk of symptomatic hemorrhage.24 The goal of ultrasound-enhanced thrombolysis should be to achieve flowimprovement within minutes of treatment initiation.25
CLOTBUST is an Investigator Sponsored Trial (A2207s, Genentech,Inc). Dr Alexandrov, principal investigator, is supported for this studyby the NIH 1 K23 NS-02229-01 Career Development Award. Dr Burginwas supported during this study by the NIH Fellowship Training Grant1-T32-NS07412-O1A1 for the Stroke Program, University of Texas –Houston Medical School. The authors gratefully acknowledge technicalsupport offered by Multigon Industries, DWL, and Spencer Technolo-gies during this project.
References
1. del Zoppo GJ, Poeck K, Pessin MS, et al. Recombinant tissueplasminogen activator in acute thrombotic and embolicstroke. Ann Neurol 1992;32:78-86.
2. The National Institutes of Neurological Disorders andStroke rt-PA Stroke Study Group. Tissue plasminogen acti-vator for acute ischemic stroke. N Engl J Med 1995;333:1581-1587.
3. Haley EC, Lewandowski C, Tilley BC. Myths regardingNINDS rt-PA Stroke Trial: setting the record straight. AnnEmerg Med 1997;30:676-682.
4. Demchuk AM, Felberg RA, Alexandrov AV. Clinical recov-ery from acute ischemic stroke after early reperfusion of thebrain with intravenous thrombolysis. N Engl J Med1999;340:894-895.
5. Grotta JC, Alexandrov AV. TPA-associated reperfusion inacute ischemic stroke demonstrated by SPECT. Stroke1998:29:429-432.
6. Heiss W-D, Grond M, Thiel A, et al. Tissue at risk of infarc-tion rescued by early reperfusion: a positron emissiontomography study in systemic recombinant tissueplasminogen activator thrombolysis of acute stroke. J CerebBlood Flow Metab 1998;18:1298-1307.
7. Ringelstein EB, Biniek R, Weiller C, Ammeling B, NoltePN, Thron A. Type and extent of hemispheric braininfarctions and clinical outcome in early and delayed mid-dle cerebral artery recanalization. Neurology 1992;42:289-298.
8. Trubestein R, Bernard HR, Etzel F, Sobbe A, Cremer A,Stumpff U. Thrombolysis by ultrasound. Clin Sci Mol Med1976;51:697-698.
9. Tachibana K, Tachibana S. Ultrasonic vibration for boostingfibrinolytic effects of urokinase in vivo. Thromb Haemost1981;46:211 [abstract].
10. Lauer CG, Burge R, Tang DB, Bass BG, Gomez ER, AlvingBM. Effect of ultrasound on tissue-type plasminogenactivator-induced thrombolysis. Circulation 1992;86:1257-1264.
11. Kimura M, Iijima S, Kobayashi K, Furuhata H. Evaluationof the thrombolytic effect of tissue-type plasminogen activa-tor with ultrasound irradiation: in vitro experiment involv-ing assay of the fibrin degradation products from the clot.Biol Pharm Bull 1994;17:126-130.
12. Akiyama M, Ishibashi T, Yamada T, Furuhata H. Low-frequency ultrasound penetrates the cranium and enhancesthrombolysis in vitro. Neurosurgery 1998;43:828-832.
13. Suchkova V, Siddiqi FN, Carstensen EL, Dalecki D, ChildS, Francis CW. Enhancement of fibrinolysis with 40-kHzultrasound. Circulation 1998;98:1030-1035.
116 Journal of Neuroimaging Vol 14 No 2 April 2004

14. Behrens S, Daffertshoffer M, Spiegel D, Hennerici M. Low-frequency, low-intensi ty ultrasound acceleratesthrombolysis through the skull. Ultrasound Med Biol1999;25:269-273.
15. Spengos K, Behrens S, Daffertshofer M, Dempfle CE,Hennerici M. Acceleration of thrombolysis with ultrasoundthrough the cranium in a flow model. Ultrasound Med Biol2000;26(5):889-895.
16. Behrens S, Spengos K, Daffertshofer M, Schroeck H,Dempfle CE, Hennerici M. Transcranial ultrasound-improved thrombolysis: diagnostic vs. therapeutic ultra-sound. Ultrasound Med Biol 2001;27(12):1683-1689.
17. Blinc A, Francis CW, Trudnowski JL, Carstensen EL. Char-acterization of ultrasound-potentiated fibrinolysis in vitro.Blood 1993;81:2636-2643.
18. Alexandrov AV, Demchuk AM, Felberg RA, et al. High rateof complete recanalization and dramatic clinical recoveryduring TPA infusion when continuously monitored by 2MHz transcranial Doppler monitoring. Stroke 2000:31:610-614.
19. Demchuk AM, Christou I, Wein TH, et al. Accuracy and cri-teria for localizing arterial occlusion with transcranial Dopp-ler. J Neuroimaging 2000;10:1-12.
20. Burgin WS, Malkoff M, Felberg RA, et al. TranscranialDoppler ultrasound criteria for recanalization afterthrombolysis for middle cerebral artery stroke. Stroke2000;31:1128-1132.
21. Alexandrov AV, Hall CE, Labiche LA, Wojner AW, GrottaJC. Ischemic stunning of the brain: early recanalizationwithout immediate clinical improvement in acute ischemicstroke. Stroke 2004 (in press).
22. Alexandrov AV, Bladin CF, Norris JW. Intracranial bloodflow velocities in acute ischemic stroke. Stroke 1994;25:1378-1383.
23. Christou I, Alexandrov AV, Burgin WS, et al. Timing ofrecanalization after TPA therapy determined bytranscranial Doppler correlates with clinical recovery fromischemic stroke. Stroke 2000;31:1812-1816.
24. Molina CA, Demchuk AM, Saqqur M, et al. Timing ofrecanalization and risk of symptomatic intracranial hemor-rhage after iv TPA. The CLOTBUST Collaboration StudyGroup. Cerebrovasc Dis 2003;16(suppl 4):114.
25. Alexandrov AV, Burgin WS, Demchuk AM, El-Mitwalli A,Grotta JC. Speed of intracranial clot lysis with intravenousTPA therapy: sonographic classification and short termimprovement. Circulation 2001;103:2897-2902.
Alexandrov et al: CLOTBUST: Phase I Data 117