Embed Size (px)
Citation preview

1
Thrombolysis in ischemic stroke
- a clinical challenge
Grethe AndersenDepartment of NeurologyÅrhus University Hospital
Ischemic stroke – worst case!
Left-sided hemiplegia, sensory deficits, hemianopia and neglect.
Komplications: depression, centrale pain, epilepsy.
Survivors: 3-6 months of rehabilitation/nursing home.

2
Facts about stroke
• Incidence: 2 pr 1000 first ever strokes in Scandinavian countries. – 50% symptom remission within 1 week– 25% disabled with need of rehabilitation for 1-3
months– 25% severe disabled or dead within 3 months
• The most severe strokes are admitted earliest• The effect of thrombolysis declines with time
from symptom onset
Prove of thrombolysis (2002) was conditioned - SITS-MOST and ECASS-3 were requiered
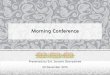
mRS 0-1 at day 90
Adjusted odds ratio with 95 % confidence interval by stroke onset to treatment time (OTT)
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
Adj
ust e
dod
dsra
tio
Stroke onset to treatment time (OTT) [min]
60 90 120 150 180 210 240 270 300 330 360
< 3 hSITS-MOST
3-4 hRCT
ECASS III
> 4,5h
except selected patients
Brott TG. International Stroke Conference 2002; abstract.

3
Meta-analysis of rt-PA studies ECASS, NINDS, ATLANTIS2.775 randomized patients < 6 h
Lancet 2004;363:768-74.
3 months follow-up
Good outcome (mRS 0-1) vs. poor outcome (mRS 2-6)
Region Midt
1,2 mill. inhabitants (20% of DK)2.400 ischemic strokes per year
Organisation:Acute stroke admission directly in neurological department Århus
- first 2 years in day-time- from 01.04.06 round-the clock
- 01.11.06 telestroke service in
Holstebro

4
Before arrival at Århus University Hospital
On call thombolysis neurologist8949 4444
”Ambulance-criteria”Inclusion criteria:• Onset time < 3 hours• age 18 – 80 • Independent ADL• Paresis and/or
dysphasia or other symptoms suggesting stroke
General Practitioner
Casuality department
Ambulance param.
Call First priority ambulance transport
Department of neurology
+1.5T MRIEvaluation
Pre-hospital phase
Highest priority ambulance transport to Department of neurology – stroke ward
Admission
•Neurological examination – NIHSS
•Exclusion criteria
•ECG, BP, Tp., Lab. -tests
AcuteMRI
ICH
DWI lesion and 1<NIHSS<25
DWI > ½ ofMCA area
Thrombolysis(SITS-MOST)
0-3 hours
3-4 hours
AcuteCT
Thrombolysis(RCT: ECASS 3)
DWI > 1/3 of MCA areaand = PWI
•Transfer to regional stroke department/ Dept. of Neurology
•Inclusion in scientific studies or RCT
•Further cerebrovascular exam. (Ecco, US etc.) and rehabilitation
MRI/ CT
•Symptom progression
•24 hours
Patient admission

5
The Acute Stroke StudyResults from the first 100 cases (80% MRI)
46%
26%
14%
2%
12% ischemicinfarctTIA
ICH
Tumors
Other
ThrombolysisÅrhus: April 2004 - Oktober 2006
47
9 97
10 11 11
27
32
0
5
10
15
20
25
30
35
40
2. kv
artal
3. kv
artal
4.kva
rtal
1.kva
rtal
2. kv
artal
3. kv
artal
4.kva
rtal
1.kva
rtal
2. kv
artal
3. kv
artal
2004 2005 2006
5%
10%

6
Thrombolysisjan. – okt. 2006
• 1170 patients admitted for stroke– 703 stroke (60%)
• 460 ischemic stroke• 153 TCI• 90 ICH, SAH, SDH, EDH
• 187 patients admitted for acute thrombolysis – 70 treated with thrombolysis
• 6% of all patients admitted for stroke• 10% of all stroke patients• 15% of all patients with ischemic stroke• 37% of all patients admitted for acute thrombolysis
Time delay (minutes)
145153MedianOnset to
treatment/needle time
6668MedianDoor to needle
DNT
524MedianImaging study to report
time
2528MedianDoor to imaging study
time
6585MedianOnset to treating
hospital/door time
SITS-MOSTÅrhus

7
Door-to-needle is inversely related to prehospital delay (onset-door)
Imaging details
788775869276Infarcts%
22122311719
No infarcts %
Follow-up24 timer
218715729315Infarcts%
7312 77307 82
No infarcts %
Akut skanning
CT or MR
99 %MR
10 %CT
93%
CT or MR
100%MR
73 % CT
30 %
SITS-MOSTÅrhus

8
Stroke subgroups
12%10%I63.9 None of the above ( can be multiple causes)
5%7%I63.8 Other/unusual cause
9%16%I63.5 Small vessel disease (lacunar)
37%23%I63.4 Cardiac source of emboli
24%28%I63.3 Large vessel disease, other
13%17%I63.0 Large vessel disease with sign. Carotidpathology
SITS-MOST
Århus
Distribution of stroke severity in different studies
0-7 mild
8-14 moderate
NIHSS>14 severe

9
Outcome after 3 monthsModified Rankin Scale 0(no symptoms) – 6(dead).
pooled analysis (Hacke W, Donnan G, Fieschi C, Kaste M, von Kummer R, Broderick JP, Brott T, Frankel M, Grotta JC, Haley EC, Jr., Kwiatkowski T, Levine SR, Lewandowski C, Lu M, Lyden P, Marler JR, Patel S, Tilley BC, Albers G, Bluhmki E, Wilhelm M, Hamilton S. Association of outcome with early stroke treatment: pooled analysis of ATLANTIS, ECASS, and NINDS rt-PA stroke trials)
mRS 0
mRS 0
mRS 0
1
1
1
2
2
2
3
3
3
4
4
4
5
5
5
Døde
Døde
Døde
0% 20% 40% 60% 80% 100%
Århus
pooled analysis
SITS-MOST
All
Moderate
Mild
Severe
Responder analysis of outcome.
For mild stroke (NIHSS 0-7)good outcome is mRS 0
For moderate (NIHSS 8-14)good outc is mRS 0-1
For severe stroke (NIHSS >14)good outc is mRS 0-2

10
ThrombolysisComplications:
2% Quinckes oedema1-5% Hypotension1-2% Epistaksis1-2% Symptomatic ICH
Safety Outcome Reports
11%11%Significant deterioration
14%8%Death within 3 month
1,7%1,4%SICH user defined
SITS-MOST
Århus

11
Clinical dilemmasexamples
• Visitation• Indication• Medication• Follow up
clinical dilemmaVisitation
Case IPhone call from a regional hospital -Randers, emergency room60 year old man, former healthy, no medicationSudden left-sided hemiplegia while driving his car. Onset as a TIA, paramedics found the patient in his car unconscious ?

12
Case I
Case I

13
Clinical dilemmaIndication
Case II60 year old man
bypassop., hypertension, hyperkolesterolæmiaSudden onset of
DysphasiaRight sided facial paresis and dysartriaRight-sided senso-motor disability in arm
At admissionallmost complet recovery, NIHSS 0-1 (asymetric smile)
Case II
T2

14
Case II
DWI
Case II
MR-angio

15
Case II
PWI
Klinisk dilemmaIndikation
Case II• 5 minutes after MRI – symptoms starts
again (NIHSS 6)• It is now 3 hours and 10 minutes after
onset• What can we do?

16
Case II
CT 3 hours and 20 minutes after onset
NIHSS: 6
Case II
CT 24 hours after onset
NIHSS: 3
MRS at 3 months: 0

17
• The most common reason for exclusion from treatment is a: few symptoms or b: rapidly improvement of symptoms (58%)• Patients with more than 4 point recovery on NIHSS before rt-PA decision of no-treatment have significant worse outcome• Patients with stable symptoms were more likely to have small vessel infarction• 27% of those not treated were not discharged to home
Poor Outcomes in Patients Who Do Not Receive Intravenous Tissue Plasminogen Activator
Because of Mild or Improving Ischemic Stroke
Stroke 36(11), November 2005, pp 2497-2499
Clinical dilemmaMedication
Case III• 65 year old man with atrial fibrilation, not
treated with warferin• Sudden symptoms at 14.15.
– Left-sided hemiplegia and lower facialparesis. No forsed eye deviation
• Admitted 1 hour later: NIHSS 14 (severe stroke)

18
Case III
DWI ADC
Case III
FlairDVI

19
Case III
• Actilyse is started at kl. 16.20 (2 hours and 5 minutes after onset)
• BP rises during treatment (>150 mmHg systolisk)
• Thrombolysis is temporary stopped (iv. labetalol)
• 80% of full dose was given
Case III
8 hours after onset

20
Case III
19 hoursafter onset
Bleeding complicationsSymptomatic bleedings – definitions RCT: • RCT: Parenchymal haematoma exceeding more than
30% of the infarct volume with significant space occupying effect
• SITS-MOST: Parenchymal haematoma and a significant woresning of symptoms or dead (increase in NIHSS of 4 points or more)

21
Parenchymal haematoma 0-6 h. 1. Meta-analysis of rtPA studies: 2.775 ptt. < 6 h
2. SITS-MOST registre: 6.000 patients < 3 timer
symptomatic parenchymal bleeding: 1.7%
Klinisk dilemmaMedication
Case IV• 73 årig woman, DM type 2, hypertension• Sudden onset of:
– Dysphasia– Right-sided hemiplegia– NIHSS 11– BP > 230/110 mmHg

22
Case IV
T2 DWI ADC
2 hours and 42 minutes after onset
Case IV
PWI

23
Case IV
15 hoursafter onset
Case IV
19 hours after onset

24
Case IV
• Audit– Start of treatment were 3 hours 15 minutes– 105 mg Actilyse (max dose is 90 mg)– Blodtryk 230/110 mmHg not sufficiently
treated before and after actilyse treatment.
Clinical dilemmaFollow up
• Case V• 63 year old former healthy male• Sudden onset of
– Dysphasia– Right-sided hemiplegia
• NIHSS 16

25
Case V
CT 150 minutes after onset
Case V
• Actilyse treatment starts at 3 hours after onset
• Dramatic recovery after about 1 hour• No complications• NIHSS: 5 after 24 hours• Aspirin was started and the patient
discharged to his regional hospital

26
Case V
MR 24 hours after thrombolysis
Case V
MR-angio before treatment

27
Case V2 days later
Admitted again with severe stroke i left MCA (NIHSS ~18)
Conclusion• Treatment must be performed by a physician trained in
neurological care and experienced in the use of thrombolytic treatment (NICE guidelines)
• Thrombolysis requiers careful– Visitation– Indication– Medication– Follow up

28
Future• MRI mismatch will probably replace “clinical” onset-to-
treatment window (DIAS, DEFUSE, EPITET).– Age limit 80 years ? (1/3 of stroke patients)
• I.a. thrombolysis +/- thrombectomi are advancing technologies.
• Clot lysis facilitation with transcranial ultrasound.• Other acute treatments for stroke e.g. Novo-7 for ICH.• In a modern society the stroke patient will demand acute
stroke settings with a hyperacute diagnostic setup and treatment on individual basis.
Time is Brain
Imaging delay in patients with suspected stroke (ending with other diagnoses)
After the introduction of thrombolysis (stage II) a larer proportion of patients are scanned within the very early hours of hospitalization

29
Length of stay in SU for patients with suspected stroke (ending with non-stroke diagnoses)
LOS significantlyshortened after intro of rtPA (stage II)
Fast triage of non-stroke patients to appropriate departments or to discharge.
Total length of hospitalization for patients with suspected stroke (ending with non-stroke diagnoses)
Total LOS was shortened from stage I-III.
Fast triage of non-stroke patients to appropriate departments or to discharge.